Embed Size (px)
Citation preview
7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 1/9
48 january 31 :: vol 21 no 21 :: 2007 NURSING STANDARD
learning zoneCONTINUING PROFESSIONAL DEVELOPMENT
Aim and intended learning outcomes
The aim of this article is to provide ward-basednurses with an overview of the investigation,treatment and nursing care of a patient withchronic diarrhoea. After reading this article youshould be able to:
Provide a definition of diarrhoea.
Identify the main causes of chronic diarrhoea.
Explain initial patient assessment.
Describe the investigations a patient mayundergo.
Outline medical and surgical treatment.
Discuss the nursing care of a patient withchronic diarrhoea.
Understand the psychological impact of copingwith chronic diarrhoea.
Introduction
Disorders of bowel function resulting in eitherdiarrhoea or constipation are not unusual andchronic diarrhoea is one of the most commonreasons why patients are referred to a hospitalgastroenterology clinic (Thomas et al 2003).
Several studies have indicated thatapproximately 95 per cent of the population opentheir bowels between three times per day and threetimes per week, with women being twice as likelyas men to have fewer than three bowel actions perweek (Spiller 1994). Contrary to popular belief,
the passage of a single motion once a day, at thesame time each day, is found in only one third of the population. Most people experience muchday-to-day variability in both stool frequency andconsistency. This should be regarded as part of normal physiology and not a sign of disease, assome patients believe (Spiller 1994).
A person’s personality is also intimately linkedto his or her bowel habits. For example, it hasbeen shown that extroverts produce bulkier, morefrequent stools, illustrating the complexinteraction between the mind and the gut. Mental
illness in later life is often associated with changesin bowel function. Anxiety and fear may causediarrhoea, while depressed patients are four tofive times more likely to report constipation(Spiller 1994).
NS377 Metcalf C (2007) Chronic diarrhoea: investigation, treatment and nursing care.
Nursing Standard . 21, 21, 48-56. Date of acceptance: August 17 2006.
Summary
Chronic diarrhoea is a distressing symptom of a number of
conditions. This article explains the assessment of patients at the
initial outpatient visit through the various investigations and finally
medical and surgical treatment. Emphasis is placed on the nursing
management of chronic diarrhoea, particularly the treatment of
physical effects such as dehydration and perianal skin soreness, and
the psychological aspects of care.
Author
Chris Metcalf is nurse specialist/senior nurse endoscopy, West
Hertfordshire Hospitals NHS Trust, Hertfordshire.
Email: [email protected]
Keywords
Body image; Chronic diarrhoea; Gastrointestinal system and
disorders; Patients: psychology
These keywords are based on the subject headings from the British
Nursing Index. This article has been subject to double-blind review.
For author and research article guidelines visit the Nursing Standard
home page at www.nursing-standard.co.uk. For related articles
visit our online archive and search using the keywords.
Chronic diarrhoea:investigation,treatment and nursing care
Page 58
Chronic diarrhoea multiplechoice questionnaire
Page 59
Read Jeanette Richards’s practice profile on chlamydia
Page 60
Guidelines on how to writea practice profile

7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 2/9
Diarrhoea
Diarrhoea may be defined in terms of stoolfrequency, consistency, volume or weight.Patients’ perceptions of diarrhoea often focus onstool consistency. However, quantification of stool consistency in clinical practice can provedifficult and so other criteria, such as the passageof more than three stools per day or stool weightprovide an alternative meaningful definition.However, although a stool weight of 200g/day isoften regarded as the upper limit of normal, thiscan be misleading because stool weights varygreatly and normal stool volumes can exceed thisvalue, particularly when a non-Western diet isconsumed (Thomas et al 2003).
There is further potential for confusion arisingfrom the discrepancy between medical and layconcepts of diarrhoea and these concepts need tobe clarified at a patient’s initial assessment. Forexample, faecal incontinence in particular iscommonly misinterpreted as diarrhoea whilesymptoms relating to functional bowel diseasecan be difficult to distinguish from organicpathology on the basis of history alone (Thomaset al 2003).
There is no consensus on the duration of symptoms that define chronic rather than acutediarrhoea. Most clinicians, however, wouldaccept that symptoms persisting for longer thanfour weeks suggest a non-infectious aetiology and
merit further investigation (Thomas et al 2003).
History and causes
A detailed history is essential when assessingpatients with chronic diarrhoea. It is useful todistinguish between the acute, usually self-limiting diarrhoeas, which are largely infectiveand chronic diarrhoea. It is also important todistinguish progressive persistent diarrhoea,which is usually a result of more serious medicalconditions, from the fluctuating, erratic
diarrhoea more characteristic of diverticulardisease and irritable bowel syndrome (Travis et al 1991). A patient’s previous medical history willidentify whether the diarrhoea is more likely to beof organic origin and also help direct thephysician as to what investigations should beundertaken. Significant previous medical historyincludes (Thomas et al 2003):Family history of neoplastic, inflammatory boweldisease or coeliac disease in particular.Previous surgery Extensive resections of theileum and right colon cause diarrhoea because of
lack of absorptive surfaces and hence fat andcarbohydrate malabsorption, decreased transittime, or malabsorption of bile acids. Shorterresections of the terminal ileum can lead to bileacid diarrhoea that typically occurs after
meals and usually responds to fasting andcholestyramine. Chronic diarrhoea may alsooccur in up to 10 per cent of patients aftercolycystectomy through mechanisms that includeincreased gut transit and bile acid malabsorption.Previous pancreatic disease Diseases such aschronic pancreatitis and cystic fibrosis.Systemic disease Thyrotoxicosis andparathyroid disease, diabetes mellitus or systemicsclerosis may predispose patients to diarrhoeathrough various mechanisms, includingendocrine effects, autonomic dysfunction andsmall bowel bacterial overgrowth or the use of concomitant drug therapy.Alcohol Diarrhoea is common in alcohol misuse.Mechanisms include rapid gut transit, decreasedactivity of intestinal disaccharides and decreasedpancreatic function.Drugs Up to 4 per cent of people have diarrhoeabecause of the side effects of medications they areprescribed – particularly magnesium containingproducts, antihypertensives, non-steroidalanti-inflammatories, theophyllines, antibiotics,antiarrhythmics and antineoplastic agents – andfood additives such as sorbitol and fructose.Diarrhoea is a relatively frequent adverse eventaccounting for about 7 per cent of all drugadverse effects. Certain new drugs are likely toinduce diarrhoea because of theirpharmacodynamic properties, for example,lipase inhibitors and cholinesterase inhibitors.
Antimicrobials are responsible for 25 per cent of drug-induced diarrhoea ranging from benign topotentially life-threatening pseudomembranouscolitis (Chassany et al 2000).Recent overseas travel or other potential
sources of infectious gastrointestinal
pathogensEntertoxigenic Escherichia coli is themost common cause of traveller’s diarrhoea.Other organisms that would be suspected areShigella, Salmonellaand Campylobacter.Giardiasis, amoebiasis and cryptosporidiosis arecommon particularly where water quality is not
predictably high (Spiller 1994).Recent antibiotic therapy and Clostridium
difficile infectionAntibiotic-associated diarrhoeasare much more common than pseudomembranouscolitis, occurring in about 20 per cent of patientstaking broad-spectrum antibiotics such asampicillin. The incidence is lower with amoxicillin,which is better absorbed, suggesting that it is theunabsorbed antibiotics that most disturb colonicflora (Spiller 1994).
Although a small proportion of individualscarry C. difficile without illness, broad-spectrum
antibiotic therapy is thought to allow theorganism to multiply by suppressing other entericorganisms. The onset may be early in thetreatment course or it may occur up to a monthafter cessation of antibiotics. Asymptomatic
january 31 :: vol 21 no 21 :: 2007 49NURSING STANDARD
7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 3/9
inflammatory bowel disease where persistentbleeding typically accompanies frequent bouts of diarrhoea with or without crampy abdominalpain (Sands and Daniel 1999).
Abdominal pain may be related to a variety of different conditions. Crohn’s disease or ulcerativecolitis may cause a diffuse, crampy andspasmodic pain associated with bloodydiarrhoea. Understanding and eliciting thesymptoms of abdominal pain will enable theclinician to conduct an examination to locate thesite of discomfort as well as its severity and arriveat the correct diagnosis (Sands and Daniel 1999).
The history, no matter how accurate, is nevercomplete without an adequate physicalexamination. A smooth tongue may reflectvitamin B12 or iron deficiency, while spontaneousbruising may be a feature of malabsorption arisingfrom a lack of vitamin K. The abdomen will be
learning zone gastrointestinal nursing
50 january 31 :: vol 21 no 21 :: 2007 NURSING STANDARD
ColonicColonic neoplasia
Ulcerative colitis and Crohn’s disease
Microscopic colitis
Small bowel
Coeliac disease
Crohn’s disease
Other small bowel enteropathies, for example,
Whipple’s diseaseBile acid malabsorption
Disaccharidase deficiency
Small bowel bacterial overgrowth
Mesenteric ischaemia
Radiation enteritis
Lymphoma
Giardiasis
Pancreatic
Chronic pancreatitis
Pancreatic carcinoma
Cystic fibrosis
Endocrine
Hyperthyroidism
Diabetes
Hypoparathyroidism
Addison’s disease
Hormone-secreting tumours
Other causes
Factitious diarrhoea, for example, caused bylaxative misuse
Surgical causes, for example, small bowel resectionor intestinal fistulae
Drugs
Alcohol
Autonomic neuropathy
(Thomas et al 2003)
BOX 1
Causes of chronic diarrhoea
infection is common but about one third of patients develop high fever, severe abdominalpain, leucocytosis and profuse watery diarrhoea.Occasionally blood is found in the stool and toxicmegacolon and perforation may occur. Diagnosisis made by detecting the C. difficile cytotoxin inthe stool or by sigmoidoscopy, which shows thecharacteristic white patches due to focaldisruption of the endothelium with aninflammatory exudate (Spiller 1994).Lactase deficiency Lactase, the enzymeresponsible for hydrolysis of dietary lactase, islocated in the microvilli of small intestinalenterocytes. Lactase deficiency may lead tolactose malabsorption and hence a mild osmoticdiarrhoea (Thomas et al 2003).
The common causes of chronic diarrhoea aresummarised in Box 1. Classification intoosmotic, secretory, motility and combined types(Table 1) helps when planning later investigationbut diagnosis initially depends on excludingcolonic causes and identifying commonconditions. More than one mechanism maycontribute to a patient having diarrhoea.
Enteropathogens that cause diarrhoeas affectthe physiology of the gut in different ways. Bymodifying the equilibrium of water and
electrolytes, they induce different types of diarrhoea. Thus, osmotic diarrhoeas result froman excess of non-absorbable and osmoticallyactive solutes in the lumen and secretorydiarrhoea results when the secretory activity of the mucosa exceeds its absorption capacity.Diarrhoea of a predominantly osmotic basis isusually investigated by measurement of faecalcarbohydrates; cessation of diarrhoea within 72hours of fasting is a confirmatory feature of thispathological mechanism (Castro-Rodriguezet al 1997).
Initial assessment
At the initial assessment the patient will be askedquestions about the history of the illness andthese will focus on several key symptoms. Theseinclude a change in bowel habit – that is, onset of diarrhoea, frequency of stool and consistency –whether the patient has noticed any rectalbleeding, experienced abdominal pain or noticedany abdominal swellings.
In obtaining the history of passing blood per
rectum it is important to establish both thequantity and quality of bleeding. While thepatient may fear that rectal bleeding is associatedwith colorectal neoplasm, bleeding may occur fora variety of benign reasons, for example,
7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 4/9
palpated for abdominal masses. These can be feltin association with Crohn’s disease when a painfulmass of matted ileum may be palpable in the rightiliac fossa. However, most masses that arepalpable in the abdomen are faecal. The sigmoidcolon can often be felt in the left iliac fossa andmay be tender in both diverticular disease andirritable bowel syndrome. Evidence of hepaticenlargement will also be looked for but this is avery late feature of most neoplasms (Spiller 1994).
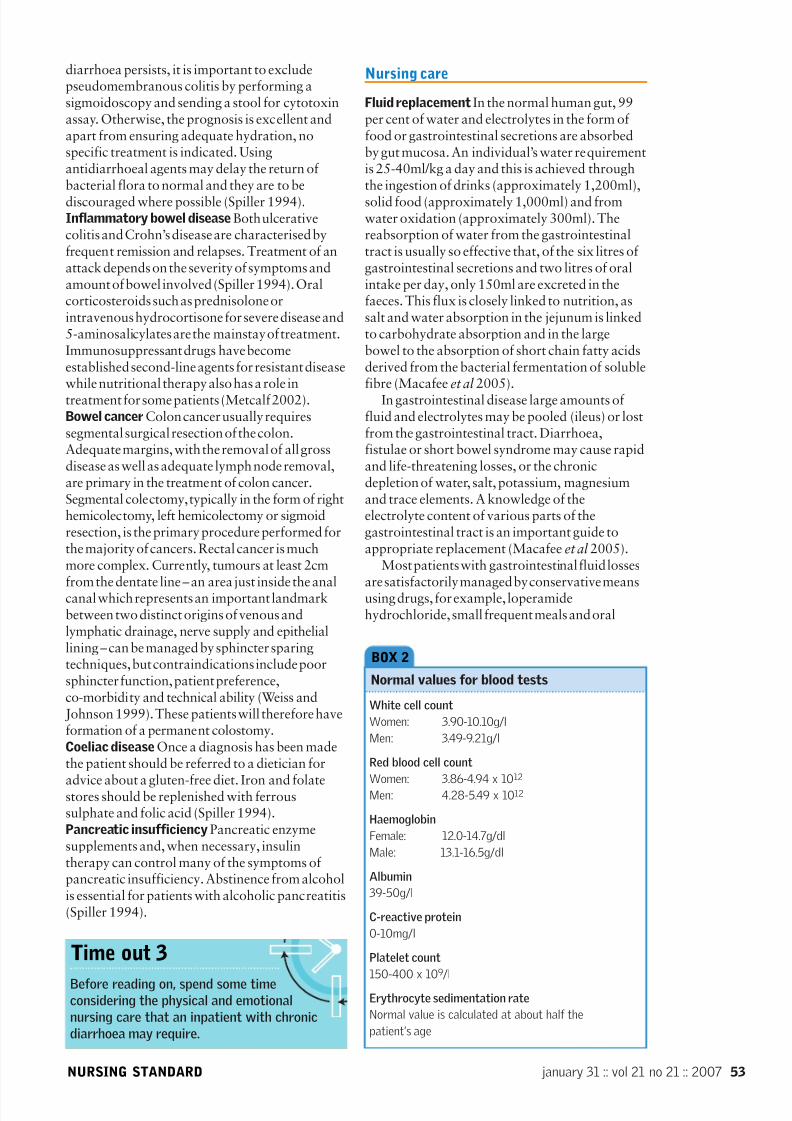
Blood tests are a routine part of initialassessment. An abnormal erythrocytesedimentation rate (ESR), anaemia or lowalbumin have a high specificity for the presence of organic disease. The presence of iron deficiencyanaemia is a sensitive indicator of small bowelenteropathy, particularly of coeliac disease. Abasic screen for evidence of malabsorption shouldinclude full blood count, urea and electrolytes,liver function tests, vitamin B12, folate, calcium,ferritin, ESR and C-reactive protein together withthyroid function test (Thomas et al 2003). Thepatient should also be weighed becausemalabsorption and inflammatory bowel diseaseoften cause weight loss (Spiller 1994).
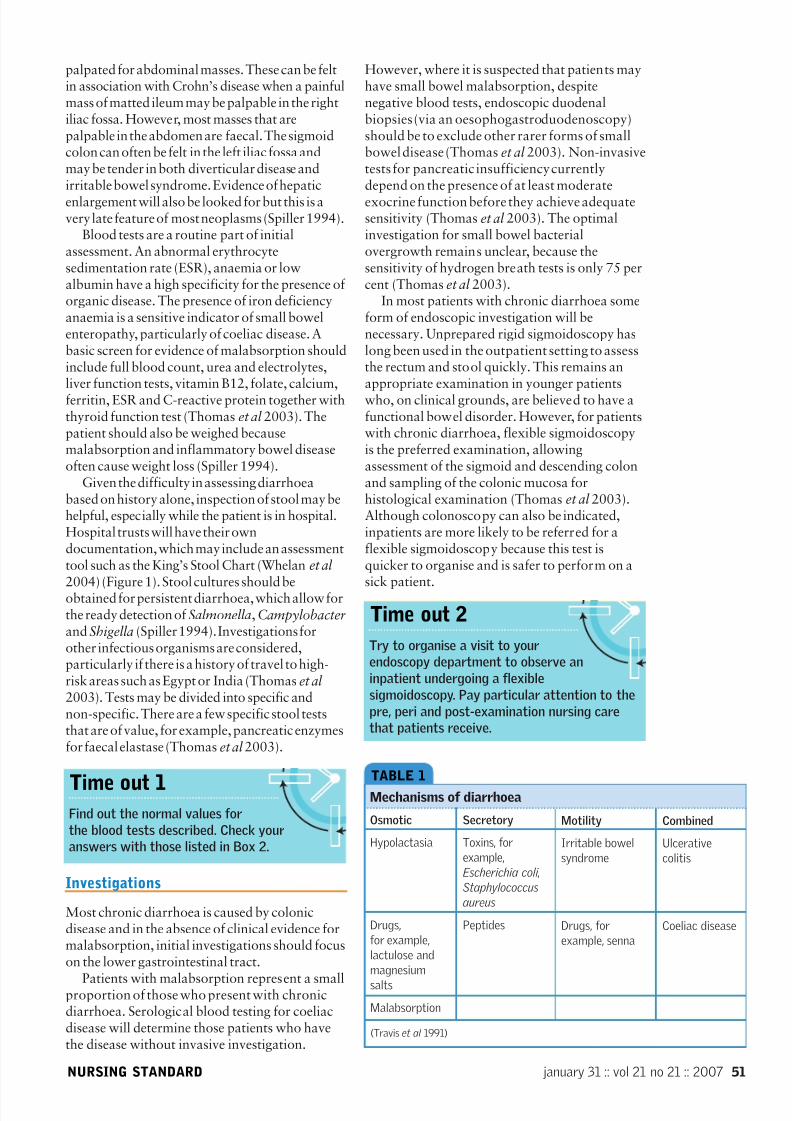
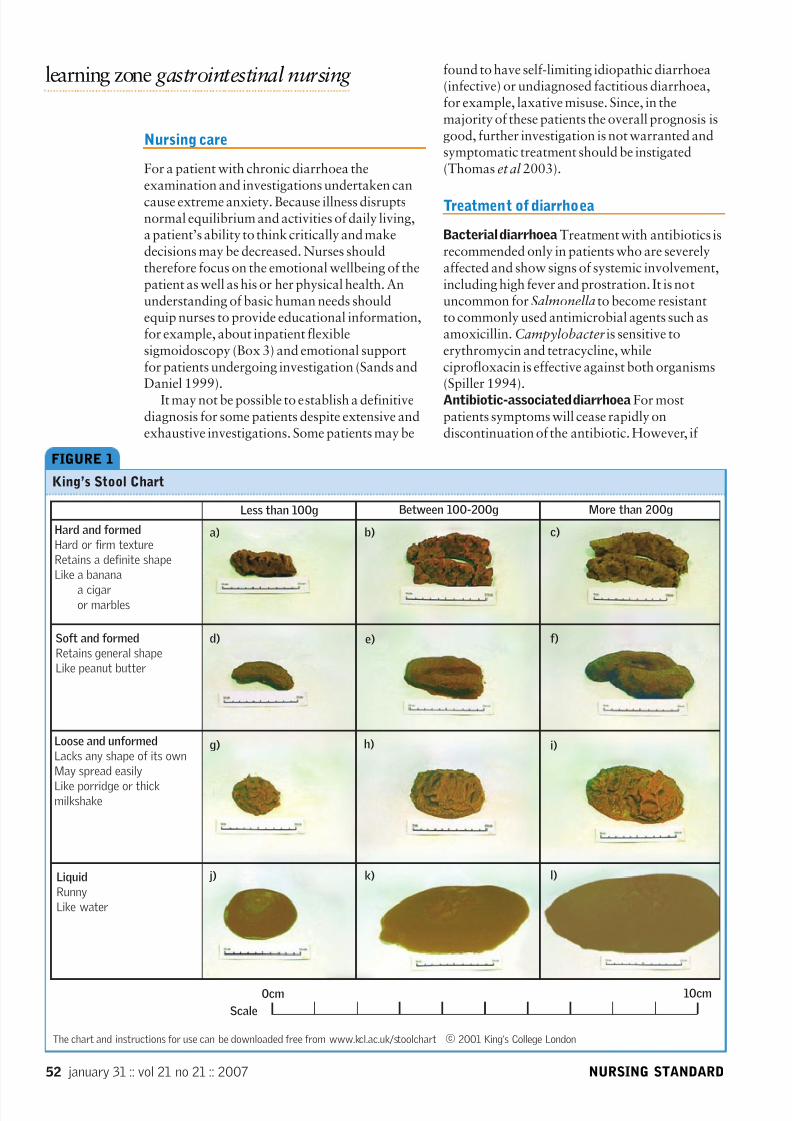
Given the difficulty in assessing diarrhoeabased on history alone, inspection of stool may behelpful, especially while the patient is in hospital.Hospital trusts will have their owndocumentation, which may include an assessmenttool such as the King’s Stool Chart (Whelan et al
2004) (Figure 1). Stool cultures should beobtained for persistent diarrhoea, which allow forthe ready detection of Salmonella, Campylobacterand Shigella (Spiller 1994). Investigations forother infectious organisms are considered,particularly if there is a history of travel to high-risk areas such as Egypt or India (Thomaset al 2003). Tests may be divided into specific andnon-specific. There are a few specific stool teststhat are of value, for example, pancreatic enzymesfor faecal elastase (Thomas et al 2003).
Investigations
Most chronic diarrhoea is caused by colonicdisease and in the absence of clinical evidence formalabsorption, initial investigations should focuson the lower gastrointestinal tract.
Patients with malabsorption represent a smallproportion of those who present with chronicdiarrhoea. Serological blood testing for coeliacdisease will determine those patients who havethe disease without invasive investigation.
However, where it is suspected that patients mayhave small bowel malabsorption, despitenegative blood tests, endoscopic duodenalbiopsies (via an oesophogastroduodenoscopy)should be to exclude other rarer forms of smallbowel disease (Thomas et al 2003). Non-invasivetests for pancreatic insufficiency currentlydepend on the presence of at least moderateexocrine function before they achieve adequatesensitivity (Thomas et al 2003). The optimalinvestigation for small bowel bacterialovergrowth remains unclear, because thesensitivity of hydrogen breath tests is only 75 percent (Thomas et al 2003).
In most patients with chronic diarrhoea someform of endoscopic investigation will benecessary. Unprepared rigid sigmoidoscopy haslong been used in the outpatient setting to assessthe rectum and stool quickly. This remains anappropriate examination in younger patientswho, on clinical grounds, are believed to have afunctional bowel disorder. However, for patientswith chronic diarrhoea, flexible sigmoidoscopyis the preferred examination, allowingassessment of the sigmoid and descending colonand sampling of the colonic mucosa forhistological examination (Thomas et al 2003).Although colonoscopy can also be indicated,inpatients are more likely to be referred for aflexible sigmoidoscopy because this test isquicker to organise and is safer to perform on a
sick patient.
january 31 :: vol 21 no 21 :: 2007 51NURSING STANDARD
TABLE 1
Mechanisms of diarrhoea
Osmotic
Hypolactasia
Drugs,
for example,
lactulose and
magnesium
salts
Malabsorption
Secretory
Toxins, for
example,
Escherichia coli ,
Staphylococcus
aureus
Peptides
Motility
Irritable bowel
syndrome
Drugs, for
example, senna
Combined
Ulcerative
colitis
Coeliac disease
(Travis et al 1991)
Time out 1Find out the normal values for
the blood tests described. Check your
answers with those listed in Box 2.
Time out 2
Try to organise a visit to your
endoscopy department to observe an
inpatient undergoing a flexible
sigmoidoscopy. Pay particular attention to the
pre, peri and post-examination nursing care
that patients receive.
7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 5/9
found to have self-limiting idiopathic diarrhoea(infective) or undiagnosed factitious diarrhoea,for example, laxative misuse. Since, in themajority of these patients the overall prognosis isgood, further investigation is not warranted andsymptomatic treatment should be instigated(Thomas et al 2003).
Treatment of diarrhoea
Bacterial diarrhoea Treatment with antibiotics isrecommended only in patients who are severelyaffected and show signs of systemic involvement,including high fever and prostration. It is notuncommon for Salmonella to become resistantto commonly used antimicrobial agents such asamoxicillin. Campylobacteris sensitive toerythromycin and tetracycline, whileciprofloxacin is effective against both organisms(Spiller 1994).Antibiotic-associated diarrhoea For mostpatients symptoms will cease rapidly ondiscontinuation of the antibiotic. However, if
Nursing care
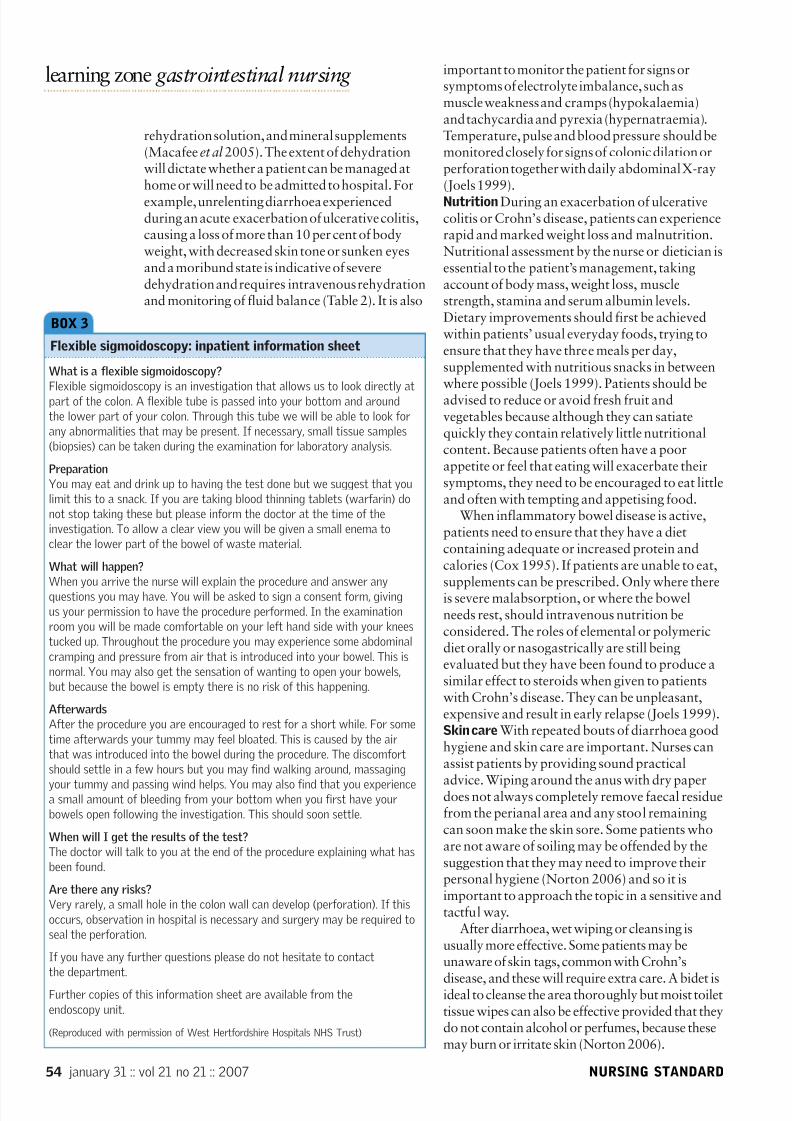
For a patient with chronic diarrhoea theexamination and investigations undertaken cancause extreme anxiety. Because illness disruptsnormal equilibrium and activities of daily living,a patient’s ability to think critically and makedecisions may be decreased. Nurses shouldtherefore focus on the emotional wellbeing of thepatient as well as his or her physical health. Anunderstanding of basic human needs shouldequip nurses to provide educational information,for example, about inpatient flexiblesigmoidoscopy (Box 3) and emotional supportfor patients undergoing investigation (Sands andDaniel 1999).
It may not be possible to establish a definitivediagnosis for some patients despite extensive andexhaustive investigations. Some patients may be
learning zone gastrointestinal nursing
52 january 31 :: vol 21 no 21 :: 2007 NURSING STANDARD
FIGURE 1
King’s Stool Chart
Hard and formed
Hard or firm texture
Retains a definite shape
Like a banana
a cigaror marbles
Soft and formed
Retains general shape
Like peanut butter
Less than 100g Between 100-200g More than 200g
The chart and instructions for use can be downloaded free from www.kcl.ac.uk/stoolchart © 2001 King’s College London
Scale
0cm 10cm
a) b) c)
d) e) f)
g) h) i)Loose and unformed
Lacks any shape of its own
May spread easily
Like porridge or thickmilkshake
Liquid
Runny
Like water
j) k) l)
7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 6/9
diarrhoea persists, it is important to excludepseudomembranous colitis by performing asigmoidoscopy and sending a stool for cytotoxinassay. Otherwise, the prognosis is excellent andapart from ensuring adequate hydration, nospecific treatment is indicated. Usingantidiarrhoeal agents may delay the return of bacterial flora to normal and they are to bediscouraged where possible (Spiller 1994).Inflammatory bowel disease Both ulcerativecolitis and Crohn’s disease are characterised byfrequent remission and relapses. Treatment of anattack depends on the severity of symptoms andamount of bowel involved (Spiller 1994). Oralcorticosteroids such as prednisolone orintravenous hydrocortisone for severe disease and5-aminosalicylates are the mainstay of treatment.Immunosuppressant drugs have becomeestablished second-line agents for resistant diseasewhile nutritional therapy also has a role intreatment for some patients (Metcalf 2002).Bowel cancer Colon cancer usually requiressegmental surgical resection of the colon.Adequate margins, with the removal of all grossdisease as well as adequate lymph node removal,are primary in the treatment of colon cancer.Segmental colectomy, typically in the form of righthemicolectomy, left hemicolectomy or sigmoidresection, is the primary procedure performed forthe majority of cancers. Rectal cancer is muchmore complex. Currently, tumours at least 2cm
from the dentate line – an area just inside the analcanal which represents an important landmarkbetween two distinct origins of venous andlymphatic drainage, nerve supply and epitheliallining – can be managed by sphincter sparingtechniques, but contraindications include poorsphincter function, patient preference,co-morbidity and technical ability (Weiss and
Johnson 1999). These patients will therefore haveformation of a permanent colostomy.Coeliac disease Once a diagnosis has been madethe patient should be referred to a dietician for
advice about a gluten-free diet. Iron and folatestores should be replenished with ferroussulphate and folic acid (Spiller 1994).Pancreatic insufficiency Pancreatic enzymesupplements and, when necessary, insulintherapy can control many of the symptoms of pancreatic insufficiency. Abstinence from alcoholis essential for patients with alcoholic pancreatitis(Spiller 1994).
Nursing care
Fluid replacement In the normal human gut, 99per cent of water and electrolytes in the form of food or gastrointestinal secretions are absorbedby gut mucosa. An individual’s water requirementis 25-40ml/kg a day and this is achieved throughthe ingestion of drinks (approximately 1,200ml),solid food (approximately 1,000ml) and fromwater oxidation (approximately 300ml). Thereabsorption of water from the gastrointestinaltract is usually so effective that, of the six litres of gastrointestinal secretions and two litres of oralintake per day, only 150ml are excreted in thefaeces. This flux is closely linked to nutrition, assalt and water absorption in the jejunum is linkedto carbohydrate absorption and in the largebowel to the absorption of short chain fatty acidsderived from the bacterial fermentation of solublefibre (Macafee et al 2005).
In gastrointestinal disease large amounts of fluid and electrolytes may be pooled (ileus) or lostfrom the gastrointestinal tract. Diarrhoea,fistulae or short bowel syndrome may cause rapidand life-threatening losses, or the chronicdepletion of water, salt, potassium, magnesiumand trace elements. A knowledge of theelectrolyte content of various parts of thegastrointestinal tract is an important guide toappropriate replacement (Macafee et al 2005).
Most patients with gastrointestinal fluid losses
are satisfactorily managed by conservative meansusing drugs, for example, loperamidehydrochloride, small frequent meals and oral
january 31 :: vol 21 no 21 :: 2007 53NURSING STANDARD
White cell count
Women: 3.90-10.10g/l
Men: 3.49-9.21g/l
Red blood cell count
Women: 3.86-4.94 x 1012
Men: 4.28-5.49 x 1012
Haemoglobin
Female: 12.0-14.7g/dl
Male: 13.1-16.5g/dl
Albumin
39-50g/l
C-reactive protein
0-10mg/l
Platelet count
150-400 x 109 /l
Erythrocyte sedimentation rate
Normal value is calculated at about half the
patient’s age
BOX 2
Normal values for blood tests
Time out 3
Before reading on, spend some timeconsidering the physical and emotional
nursing care that an inpatient with chronic
diarrhoea may require.
7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 7/9
important to monitor the patient for signs orsymptoms of electrolyte imbalance, such asmuscle weakness and cramps (hypokalaemia)and tachycardia and pyrexia (hypernatraemia).Temperature, pulse and blood pressure should bemonitored closely for signs of colonic dilation orperforation together with daily abdominal X-ray(Joels 1999).Nutrition During an exacerbation of ulcerativecolitis or Crohn’s disease, patients can experiencerapid and marked weight loss and malnutrition.Nutritional assessment by the nurse or dietician isessential to the patient’s management, takingaccount of body mass, weight loss, musclestrength, stamina and serum albumin levels.Dietary improvements should first be achievedwithin patients’ usual everyday foods, trying toensure that they have three meals per day,supplemented with nutritious snacks in betweenwhere possible (Joels 1999). Patients should beadvised to reduce or avoid fresh fruit andvegetables because although they can satiatequickly they contain relatively little nutritionalcontent. Because patients often have a poorappetite or feel that eating will exacerbate theirsymptoms, they need to be encouraged to eat littleand often with tempting and appetising food.
When inflammatory bowel disease is active,patients need to ensure that they have a dietcontaining adequate or increased protein andcalories (Cox 1995). If patients are unable to eat,
supplements can be prescribed. Only where thereis severe malabsorption, or where the bowelneeds rest, should intravenous nutrition beconsidered. The roles of elemental or polymericdiet orally or nasogastrically are still beingevaluated but they have been found to produce asimilar effect to steroids when given to patientswith Crohn’s disease. They can be unpleasant,expensive and result in early relapse (Joels 1999).Skin care With repeated bouts of diarrhoea goodhygiene and skin care are important. Nurses canassist patients by providing sound practical
advice. Wiping around the anus with dry paperdoes not always completely remove faecal residuefrom the perianal area and any stool remainingcan soon make the skin sore. Some patients whoare not aware of soiling may be offended by thesuggestion that they may need to improve theirpersonal hygiene (Norton 2006) and so it isimportant to approach the topic in a sensitive andtactful way.
After diarrhoea, wet wiping or cleansing isusually more effective. Some patients may beunaware of skin tags, common with Crohn’s
disease, and these will require extra care. A bidet isideal to cleanse the area thoroughly but moist toilettissue wipes can also be effective provided that theydo not contain alcohol or perfumes, because thesemay burn or irritate skin (Norton 2006).
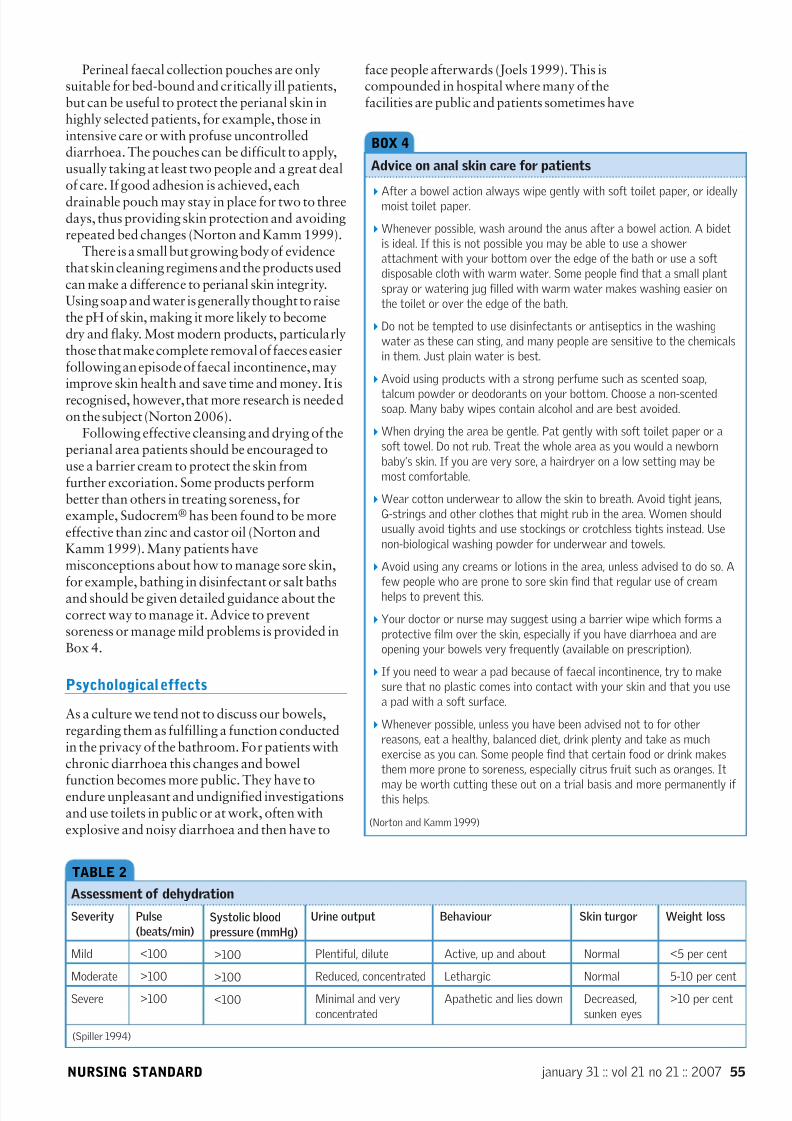
rehydration solution, and mineral supplements(Macafeeet al 2005). The extent of dehydrationwill dictate whether a patient can be managed athome or will need to be admitted to hospital. For
example, unrelenting diarrhoea experiencedduring an acute exacerbation of ulcerative colitis,causing a loss of more than 10 per cent of bodyweight, with decreased skin tone or sunken eyesand a moribund state is indicative of severedehydration and requires intravenous rehydrationand monitoring of fluid balance (Table 2). It is also
learning zone gastrointestinal nursing
54 january 31 :: vol 21 no 21 :: 2007 NURSING STANDARD
What is a flexible sigmoidoscopy?
Flexible sigmoidoscopy is an investigation that allows us to look directly atpart of the colon. A flexible tube is passed into your bottom and around
the lower part of your colon. Through this tube we will be able to look for
any abnormalities that may be present. If necessary, small tissue samples
(biopsies) can be taken during the examination for laboratory analysis.
Preparation
You may eat and drink up to having the test done but we suggest that you
limit this to a snack. If you are taking blood thinning tablets (warfarin) do
not stop taking these but please inform the doctor at the time of the
investigation. To allow a clear view you will be given a small enema to
clear the lower part of the bowel of waste material.
What will happen?
When you arrive the nurse will explain the procedure and answer any
questions you may have. You will be asked to sign a consent form, giving
us your permission to have the procedure performed. In the examination
room you will be made comfortable on your left hand side with your knees
tucked up. Throughout the procedure you may experience some abdominal
cramping and pressure from air that is introduced into your bowel. This is
normal. You may also get the sensation of wanting to open your bowels,
but because the bowel is empty there is no risk of this happening.
Afterwards
After the procedure you are encouraged to rest for a short while. For some
time afterwards your tummy may feel bloated. This is caused by the air
that was introduced into the bowel during the procedure. The discomfort
should settle in a few hours but you may find walking around, massaging
your tummy and passing wind helps. You may also find that you experiencea small amount of bleeding from your bottom when you first have your
bowels open following the investigation. This should soon settle.
When will I get the results of the test?
The doctor will talk to you at the end of the procedure explaining what has
been found.
Are there any risks?
Very rarely, a small hole in the colon wall can develop (perforation). If this
occurs, observation in hospital is necessary and surgery may be required to
seal the perforation.
If you have any further questions please do not hesitate to contact
the department.
Further copies of this information sheet are available from the
endoscopy unit.
(Reproduced with permission of West Hertfordshire Hospitals NHS Trust)
BOX 3
Flexible sigmoidoscopy: inpatient information sheet
7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 8/9
Perineal faecal collection pouches are onlysuitable for bed-bound and critically ill patients,but can be useful to protect the perianal skin inhighly selected patients, for example, those inintensive care or with profuse uncontrolleddiarrhoea. The pouches can be difficult to apply,usually taking at least two people and a great dealof care. If good adhesion is achieved, eachdrainable pouch may stay in place for two to threedays, thus providing skin protection and avoidingrepeated bed changes (Norton and Kamm 1999).
There is a small but growing body of evidencethat skin cleaning regimens and the products usedcan make a difference to perianal skin integrity.Using soap and water is generally thought to raisethe pH of skin, making it more likely to becomedry and flaky. Most modern products, particularlythose that make complete removal of faeces easierfollowing an episode of faecal incontinence, mayimprove skin health and save time and money. It isrecognised, however, that more research is neededon the subject (Norton 2006).
Following effective cleansing and drying of theperianal area patients should be encouraged touse a barrier cream to protect the skin fromfurther excoriation. Some products performbetter than others in treating soreness, forexample, Sudocrem® has been found to be moreeffective than zinc and castor oil (Norton andKamm 1999). Many patients havemisconceptions about how to manage sore skin,
for example, bathing in disinfectant or salt bathsand should be given detailed guidance about thecorrect way to manage it. Advice to preventsoreness or manage mild problems is provided inBox 4.
Psychological effects
As a culture we tend not to discuss our bowels,regarding them as fulfilling a function conductedin the privacy of the bathroom. For patients withchronic diarrhoea this changes and bowel
function becomes more public. They have toendure unpleasant and undignified investigationsand use toilets in public or at work, often withexplosive and noisy diarrhoea and then have to
face people afterwards (Joels 1999). This iscompounded in hospital where many of thefacilities are public and patients sometimes have
january 31 :: vol 21 no 21 :: 2007 55NURSING STANDARD
After a bowel action always wipe gently with soft toilet paper, or ideallymoist toilet paper.
Whenever possible, wash around the anus after a bowel action. A bidet
is ideal. If this is not possible you may be able to use a shower
attachment with your bottom over the edge of the bath or use a soft
disposable cloth with warm water. Some people find that a small plant
spray or watering jug filled with warm water makes washing easier on
the toilet or over the edge of the bath.
Do not be tempted to use disinfectants or antiseptics in the washing
water as these can sting, and many people are sensitive to the chemicals
in them. Just plain water is best.
Avoid using products with a strong perfume such as scented soap,
talcum powder or deodorants on your bottom. Choose a non-scentedsoap. Many baby wipes contain alcohol and are best avoided.
When drying the area be gentle. Pat gently with soft toilet paper or a
soft towel. Do not rub. Treat the whole area as you would a newborn
baby’s skin. If you are very sore, a hairdryer on a low setting may be
most comfortable.
Wear cotton underwear to allow the skin to breath. Avoid tight jeans,
G-strings and other clothes that might rub in the area. Women should
usually avoid tights and use stockings or crotchless tights instead. Use
non-biological washing powder for underwear and towels.
Avoid using any creams or lotions in the area, unless advised to do so. A
few people who are prone to sore skin find that regular use of cream
helps to prevent this.
Your doctor or nurse may suggest using a barrier wipe which forms a
protective film over the skin, especially if you have diarrhoea and are
opening your bowels very frequently (available on prescription).
If you need to wear a pad because of faecal incontinence, try to make
sure that no plastic comes into contact with your skin and that you use
a pad with a soft surface.
Whenever possible, unless you have been advised not to for other
reasons, eat a healthy, balanced diet, drink plenty and take as much
exercise as you can. Some people find that certain food or drink makes
them more prone to soreness, especially citrus fruit such as oranges. It
may be worth cutting these out on a trial basis and more permanently if this helps.
(Norton and Kamm 1999)
BOX 4
Advice on anal skin care for patients
TABLE 2
Assessment of dehydration
Severity
Mild
ModerateSevere
Pulse
(beats/min)
<100
>100>100
Systolic blood
pressure (mmHg)
>100
>100<100
Urine output
Plentiful, dilute
Reduced, concentratedMinimal and very
concentrated
Behaviour
Active, up and about
LethargicApathetic and lies down
Skin turgor
Normal
NormalDecreased,
sunken eyes
Weight loss
<5 per cent
5-10 per cent>10 per cent
(Spiller 1994)

7/14/2019 Chronic Diarrhoea
http://slidepdf.com/reader/full/chronic-diarrhoea-56327cd1a56af 9/9
Conclusion
Chronic diarrhoea can be a distressing symptom.This article provides an overview of the care of apatient with this condition. You should nowunderstand the importance of patients beingaccurately assessed and asked questions toidentify any significant medical history, both of which can guide the clinician as to the diagnostictests required. The most common causes of diarrhoea have been explained together with theappropriate treatments. The management of apatient has been outlined, focusing on the nursingcare with relation to fluid replacement, nutritionand skin care. Finally, the psychological impact of having diarrhoea has been discussed outliningnurses’ contribution in helping patients to copewith what can be a distressing symptom NS
to rely on commodes with only flimsy curtains toprovide privacy. It is therefore essential for nursesto be sensitive to patients’ needs by making themaware of the location of the nearest toilets or if possible providing a bed close to the bathroom ora side room with ensuite facilities.
Casati et al (2000) identified eight categoriesof concerns patients have about living and copingwith inflammatory bowel disease. Patientsstruggle to cope with the sense of loss of controland feeling dirty. Symptoms such as diarrhoea,urgency and faecal incontinence can dominate aperson’s life, making accessibility to a toilet apriority. Faecal incontinence in particular is aproblem that can have a major effect on thequality of life of those affected. Deutekom et al (2005) demonstrated that the more severe thefaecal incontinence, the greater the effect it hadon everyday activities and the more pain,discomfort, anxiety and depression it caused.
Social stigma caused by the unpredictabilityand embarrassing nature of the symptoms canaffect people psychologically. Patients can feelthat they are the only one to have the problem,which can make them feel isolated and alone.Nurses can help by encouraging patients to share
their feelings and concerns with those closest tothem (Metcalf 2002).
learning zone gastrointestinal nursing
56 january 31 :: vol 21 no 21 :: 2007 NURSING STANDARD
Casati J, Toner BB, de Rooy EC,
Drossman DA, Maunder RG(2000) Concerns of patients with
inflammatory bowel disease: a
review of emerging themes.
Digestive Diseases and Sciences.
45, 1, 26-31.
Castro-Rodriguez JA,
Salazar-Lindo E, Leon-Barua R
(1997) Differentiation of osmotic
and secretory diarrhoea by stool
carbohydrate and osmolar gap
measurements. Archives of Disease
in Childhood . 77, 3, 201-205.
Chassany O, Michaux A,
Bergmann JF (2000) Drug induced
diarrhoea. Drug Safety . 22, 1, 53-72.
Cox J (1995) Inflammatory bowel
disease: implications for the
medical-surgical nurse. Medsurg
Nursing. 4, 6, 427-437.
Deutekom M, Terra MP,
Dobben AC et al (2005) Impact of
faecal incontinence severity on
health domains. Colorectal Disease.
7, 3, 263-269.
Joels J (1999) Inflammatory bowel
disease: the nursing implications. In
Porrett T, Daniel N (Eds) Essential
Coloproctology for Nurses. Whurr,
London, 119-145.
Macafee DA, Allison SP, Lobo DN
(2005) Some interactions betweengastrointestinal function and fluid
and electrolyte homeostasis.
Current Opinion in Clinical Nutrition
and Metabolic Care. 8, 2, 197-203.
Metcalf C (2002) Crohn’s disease:
an overview. Nursing Standard . 16,31, 45-52.
Norton C (2006) Perianal skin care.
Gastrointestinal Nursing. 4, 1, 18-25.
Norton C, Kamm M (1999) Bowel
Control: Information and Practical
Advice. Beaconsfield Publishers,
Beaconsfield.
Sands LR, Daniel N (1999)
Investigation and examination of a
patient with colorectal problems. In
Porrett T, Daniel N (Eds) Essential
Coloproctology for Nurses. Whurr,
London, 52-75.
Spiller R (1994) Diarrhoea and
Constipation. Science Press, London.
Thomas PD, Forbes A, Green J
et al (2003) Guidelines for the
investigation of chronic diarrhoea.Second edition. Gut . 52, Suppl 5,
v1-15.
Travis SPL, Taylor RH, Musiewicz J
(1991) Gastroenterology . Blackwell
Science, Oxford.
Weiss EG, Johnson TE (1999)
Colorectal cancer. In Porrett T,
Daniel N (Eds) Essential
Coloproctology for Nurses. Whurr,
London, 97-118.
Whelan K, Judd PA, Taylor MA
(2004) Assessment of fecal outputin patients receiving enteral tube
feeding: validation of a novel chart.
European Journal of Clinical
Nutrition. 58, 7, 1030-1037.
References
Time out 4
Imagine that a patient complaining of
chronic diarrhoea has been admitted to
your ward. Write a nursing care plan taking
into account what has been discussed regarding
a patient’s physical and psychological needs.
Time out 5
Now that you have completed this
article you might like to write a practice
profile. Guidelines to help you are on page 60.