Embed Size (px)
Citation preview

BioMed Central
International Journal of Health Geographics
ss
Open AcceResearchDistance, rurality and the need for care: access to health services in South West EnglandHannah Jordan*1, Paul Roderick1, David Martin2 and Sarah Barnett3Address: 1Health Care Research Unit, CCS Division, School of Medicine, University of Southampton, UK, 2School of Geography, University of Southampton, UK and 3International Perinatal Care Unit, Institute of Child Health, London, UK
Email: Hannah Jordan* - [email protected]; Paul Roderick - [email protected]; David Martin - [email protected]; Sarah Barnett - [email protected]
* Corresponding author
AbstractBackground: This paper explores the geographical accessibility of health services in urban andrural areas of the South West of England, comparing two measures of geographical access andcharacterising the areas most remote from hospitals.
Straight-line distance and drive-time to the nearest general practice (GP) and acute hospital (DGH)were calculated for postcodes and aggregated to 1991 Census wards. The correlation between thetwo measures was used to identify wards where straight-line distance was not an accuratepredictor of drive-time. Wards over 25 km from a DGH were classified as 'remote', andcharacterised in terms of rurality, deprivation, age structure and health status of the population.
Results: The access measures were highly correlated (r2>0.93). The greatest differences werefound in coastal and rural wards of the far South West. Median straight-line distance to GPs was 1km (IQR = 0.6–2 km) and to DGHs, 12 km (IQR = 5–19 km). Deprivation and rates of prematurelimiting long term illness were raised in areas most distant from hospitals, but there was noevidence of higher premature mortality rates. Half of the wards remote from a DGH were notclassed as rural by the Office for National Statistics. Almost a quarter of households in the wardsfurthest from hospitals had no car, and the proportion of households with access to two or morecars fell in the most remote areas.
Conclusion: Drive-time is a more accurate measure of access for peripheral and rural areas.Geographical access to health services, especially GPs, is good, but remoteness affects both ruraland urban areas: studies concentrating purely on rural areas may underestimate geographicalbarriers to accessing health care. A sizeable minority of households still had no car in 1991, andfew had more than one car, particularly in areas very close to and very distant from hospitals.Better measures of geographical access, which integrate public and private transport availabilitywith distance and travel time, are required if an accurate reflection of the experience those withouttheir own transport is to be obtained.
BackgroundThe UK National Health Service has always aimed to pro-
vide health care for all. Although the importance of "fairaccess for all" (independent of the ability to pay, age, sex
Published: 29 September 2004
International Journal of Health Geographics 2004, 3:21 doi:10.1186/1476-072X-3-21
Received: 31 August 2004Accepted: 29 September 2004
This article is available from: http://www.ij-healthgeographics.com/content/3/1/21
© 2004 Jordan et al; licensee BioMed Central Ltd. This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Page 1 of 9(page number not for citation purposes)

International Journal of Health Geographics 2004, 3:21 http://www.ij-healthgeographics.com/content/3/1/21
or area of residence) has been highlighted in recent policydocuments [1], the meaning of 'fair access' is still debated[2]. Although there will always be variations in geograph-ical access to health services, the extent of such variationsand the relationship between distance to health servicesand the need for health care is unclear. If policy makersare to address inequities of access, more understanding isneeded both of appropriate methods for measuring accessand of the relationship between access to health servicesand health.
Although 'fair access' can be characterised simply as 'pro-viding the right service at the right time in the rightplace'[3], it is a complex concept covering the provision ofservices, the knowledge and opportunity to use them, andthe measurement of need [4]. In the UK mergers of hospi-tal trusts have highlighted tensions between the perceivedsafety, effectiveness and efficiency of larger specialist cen-tres and the demand for more geographically accessiblelocal care [5,6], revealing the lack of evidence on which tobase decisions [7]. Geographical access – the distancewhich must be travelled in order to use health services – isone aspect of access which is often overlooked [2], butwhich presents barriers of cost, time and inconvenience.
Although there is some evidence that increasing distancefrom health services inhibits the use of primary [8] andsecondary care [9], and that it is associated with a range ofpoor health outcomes, from higher than expected num-bers of deaths from asthma to lower than expected fiveyear survival from cancer [10,11], few studies haveattempted to quantify or set thresholds of poor access[12,13]. Furthermore, measures of geographical accesscan be difficult to compare. Rurality has often been usedas a proxy for inaccessibility [14], as have dichotomouscategorisations such as the presence or absence of a serviceprovider in an area [15,8]. More complex measurementssuch as the straight line distance between populations (i.edemand points) and health service providers [16,17], or'network distances' (which can include both road distanceand travel time) [8] have added complexity, but the rela-tionship between these measures is not clear.
One assumption which is commonly made is that geo-graphical inaccessibility of health services is essentially arural problem, but there is little evidence demonstratingthe differences in accessibility between rural and otherareas. In any area, the greatest disadvantage is likely to beexperienced by individuals without access to a car (includ-ing members of one-car households without daytimeaccess). With the declining availability of public transport,it is likely that a private car is the only convenient way totravel in rural Britain [18]. Although car ownership is rel-atively high in rural areas, rates for the poor, the elderlyand for women are far lower than average: the 2001 Cen-
sus reports that more than two thirds of single-pensionerhouseholds, many of which comprise single women, donot have access to a car. Distance may therefore be a fur-ther burden on groups with a particularly high need forhealth care, raising issues of inequity. Furthermore, if geo-graphical access to health services is a problem for somegroups outside of traditional rural areas, then rural poli-cies alone will not tackle the problem.
In this paper, we aim to determine the geographical acces-sibility of health services, and the demographic andhealth related factors associated with it. We compare twomeasures of geographical access: straight-line distanceand modelled drive-time along the road network to pri-mary and secondary care throughout South West England.We investigate whether the most geographically inaccessi-ble populations are in rural areas, describe the relation-ship between geographical access to hospital andpopulation health, and investigate whether the popula-tions furthest from health services have a greater need forhealth care due to age or deprivation.
The study area is the former South West Region, compris-ing the counties of Avon, Cornwall and the Isles of Scilly,Devon, Dorset, Gloucestershire, Hampshire, the Isle ofWight, Somerset and Wiltshire. As defined in 1991 thisarea has a population of about 6 million, with a low pro-portion from ethnic minorities, and a higher than averageproportion living in rural areas.
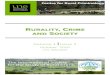
ResultsCorrelation between the access measuresThe straight-line and drive-time measures were highly cor-related for both GP and hospital services (figure 1). Areaswhere residuals from the regression analysis of straight-line distance and drive-time to DGHs are more than twostandard deviations from the norm were concentrated incoastal and rural wards of the far South West. Areas whereresiduals are negative indicate faster than expected drivetimes, wheras positive residuals indicate that drive time isslower than predicted by straight line distances (figure 2).The analysis was repeated, excluding wards along theboundary between the study area and neighbouring coun-ties to check for edge-effects, but there was no differencein results.
Distances to health servicesDistances to GPs were low, with a median distance of just1 km to the closest practice (IQR 0.6 – 2.2). The calcula-tion was repeated excluding branch surgeries (which tendto have limited opening hours), but this made little differ-ence to the outcome, with a median distance to a mainsurgery of just 1.2 km. 95% of wards (98% of the popula-tion) were under 4.4 km, or 6.3 minutes, from their clos-est GP. The maximum distance to a GP was just 9.4 km
Page 2 of 9(page number not for citation purposes)

International Journal of Health Geographics 2004, 3:21 http://www.ij-healthgeographics.com/content/3/1/21
(13.7 minutes). The median distance to a DGH was justless than 12 km (IQR 5.4 – 19.0), with a maximum of 50km, corresponding to an estimated 13 and 48 minutesdrive-time (table 1).
Remoteness and ruralityFor the purposes of this study, remoteness from healthservices was defined as over 5 km from a GP or over 25 kmfrom a DGH. Access to primary care was good, with just91 wards (6.3% of the total) remote from primary care.These areas have just 3% of the regional population. Ofthese the majority (63%) were ONS 'rural' areas. Therewere 162 wards which we classified as remote from hospi-tals (11% of the total, home to 6.5% of the region's pop-ulation). All had drive-times to hospital of over 21minutes; 81 (51%) were urban by the ONS classification,69 (43%) were rural areas and the remaining eight (5%)were rural fringe. Four wards had no ONS urban / ruralclassification (table 2).
Distance and the need for health careDeprivation scores ranged from -6.2 to 9.9, with a meanof -1.0, indicating that the study area had a slightly moreaffluent profile than the England and Wales average. Themost affluent wards were in the middle of the range ofstraight-line distances from secondary care. The mediandeprivation score was 1.0 in the decile of wards closest tohospitals, decreased to a low of -2.2 in the 5th decile, thenrose steadily to -1.0 in the decile of wards furthest fromhospitals, giving a slight 'U' shape to the relationship
between deprivation and distance from health services(figure 3).
The proportion of over 65 year olds increased slightly withstraight-line distance from hospitals: more remote wardshad a slightly higher proportion of residents over the ageof 65, but there was considerable variation within decilesof remoteness, and the observed difference was small. Theproportion of the population under five years old in 1991showed no clear trend with ward distance from hospital,but was slightly lower in more remote wards (figure 4).
The age-standardised rate of LLTI was highest in the areasclosest to hospitals. The LLTI rate decreased with increas-ing distance from hospital and then increased again in themost remote areas. Standardised rates of premature mor-tality showed no strong pattern with distance from a hos-pital, although median rates were high in areas close tohospitals and also slightly raised in the most remote areas.The proportion of households with no car was highest inthe areas closest to hospital, but increased again in thedecile of wards furthest from hospital. The same patternwas seen in the ownership of two or more cars – the low-est rates were found in areas either very close to or very farfrom hospitals (table 3).
DiscussionThe impact of distance on the use of hospitals and otherhealth care, and on health status, has not been well estab-lished. In the UK threshold distances of between 24 and
Correlation between straight line and drive-time measures to GP and hospital servicesFigure 1Correlation between straight line and drive-time measures to GP and hospital services
District general hospital General practice
r2 = 0.93 r
2 = 0.95
Straight line distance to nearest DGH (metres)
6000050000400003000020000100000
Drive
tim
eto
ne
are
stD
GH
50
40
30
20
10
0
Straight line distance to nearest GP (metres)
1000080006000400020000
Dri
ve
tim
eto
ne
are
stG
P
14
12
10
8
6
4
2
0
Page 3 of 9(page number not for citation purposes)

International Journal of Health Geographics 2004, 3:21 http://www.ij-healthgeographics.com/content/3/1/21
50 miles to specialist hospital services [19,20], 10 miles toscreening services [21], 7 km (4 miles) to family planningclinics [22] and 2.5 miles to primary care [23] have allbeen used in reporting 'poor access', but there is little con-
sensus and no strong theoretical or empirical basis forthese choices. By international standards, distances tohealth services for our study population are low, averag-ing just 12 km to the closest hospital, but drive-times to
Standardised residuals from the regression of drive time and straight-line distance to hospitalsFigure 2Standardised residuals from the regression of drive time and straight-line distance to hospitals
Table 1: Access to DGHs and GPs
25th
centilePopn (%)* Median Popn (%) 75th
centilePopn (%) 95th
centilePopn (%) Maximum
Straight line (km)
DGH 5.4 2.40 (39.3) 11.6 3.97 (65.1) 19.0 5.15 (84.3) 29.0 5.92 (97.1) 50.1
GP surgery
0.6 2.24 (36.8) 1.0 4.17 (68.3) 2.2 5.39 (88.4) 4.4 5.96 (97.7) 9.4
Drive time ('minutes')
DGH 7.1 2.38 (38.9) 13.4 3.93 (64.4) 20.5 5.17 (84.7) 31.6 5.93 (97.2) 48.3
GP surgery
1.0 2.19 (35.9) 1.7 4.00 (65.5) 3.4 5.28 (86.5) 6.3 5.89 (96.5) 13.7
*Population in millions (percent of the total population) living in wards within this distance of their closest DGH and GP
Page 4 of 9(page number not for citation purposes)

International Journal of Health Geographics 2004, 3:21 http://www.ij-healthgeographics.com/content/3/1/21
hospital of up to 50 minutes are predicted by our modeland there are groups who could be considerably disadvan-taged by the travel distances we have reported.
A variety of measures of geographic access of varying com-plexity and specificity exist and selecting an appropriatemeasure is not simple. Straight-line distances are widelyused, easy to calculate and to compare and, in this study,they are closely correlated with the more complex drive-times. However, there is some evidence that areas of lowcorrelation are concentrated in peripheral areas of therural South West. In these areas straight-line distancesunderestimate true travel distance, reflecting sparse roadnetworks and geographical barriers such as hills, riversand coastline. Access to health services in these areascould be misrepresented by the use of the simpler meas-ure, masking problems faced by these populations. Fur-thermore, neither measure used here reflects theexperience of those without access to a private car. Travelto hospital and GP appointments is already known to bea problem for some groups in rural areas of the UK.Although informal systems of 'lift-giving' and more for-mal 'voluntary taxi' schemes often exist [24] these are notavailable everywhere [25,26], and it could be argued thata measure of travel by public transport is vital in deter-
mining accessibility for the most disadvantaged popula-tions. Few studies have attempted this [27-29]., andcomposite measures, which include both public and pri-vate transport, are even less common [30]. Better meas-ures of access, which integrate private and publictransport, are required to reflect the experience of those onlow incomes, and without their own transport.
A surprising finding of this study was the relatively lowproportion of wards remote from health care which aredefined as 'rural'. Fewer than half of the wards remotefrom hospital and under two-thirds of those remote fromprimary care are classified as rural by the ONS. Analysiswhich concentrates on rural areas under the ONS defini-tion, or even stretches this to include 'rural fringe' areas,will still miss over half of the wards which are remotefrom hospitals. There has been concern over the targetingof resources in concentrations of deprivation: the majorityof deprived people live outside of these areas and are notreached by narrowly focused initiatives. Although theward-level definition of rurality used here may class as'urban' some small towns which many would consideressentially 'rural' when viewed at a larger scale (such as theLocal Authority level), we conclude that caution shouldbe exercised when evaluating and responding to pooraccess to health services, a high proportion of whichoccurs outside areas traditionally considered to be remote.
In this study, we found no clear threshold at which needbecomes greater or health status sharply declines. If any-thing, the converse is true with worse health status andgreatest need in areas close to health services. Distance tohealth care was not associated with a high proportion ofelderly or very young residents, but was related to depriva-tion. We found high deprivation in areas close to hospi-tals, relative affluence in more distant areas and anincrease in deprivation in the most remote wards. Depri-vation indices have been criticised for failing to representdeprivation in rural areas [31] and the relatively highproportion of rural areas in the most remote wards mayhide even higher need in these areas. Further researchusing different measures of need and deprivation isindicated.
Although the highest rates of morbidity and mortalitywere found in the areas closest to hospitals, there was
Table 2: ONS rurality and remoteness from hospital
N (%) Rural Rural fringe Not rural No classification Total*
Remote 69 (43%) 8 (5%) 81 (51%) 2 (1%) 162 (100%)Not remote 184 (14%) 146 (11%) 950 (74%) 6 (0.5%) 1286 (100%)
Townsend deprivation score for deciles of wards by straight-line distance from DGHFigure 3Townsend deprivation score for deciles of wards by straight-line distance from DGH
144145145145145145145145145144N =
deciles of wards by straight line distance from the nearest DGH
furthest98765432closest
To
wn
send
dep
riva
tion
sco
re
20
10
0
-10
Page 5 of 9(page number not for citation purposes)

International Journal of Health Geographics 2004, 3:21 http://www.ij-healthgeographics.com/content/3/1/21
some evidence of increasing rates in more remote areas.Rates of LLTI, particularly for those under 64, show anupwards trend in more remote areas. This supports previ-ous findings that LLTI is higher in rural wards with themost dispersed populations [31], but it is not clearwhether this reflects a true increase in morbidity or a per-ception of handicap of those living in such areas. The rela-tionship between distance and all-cause prematuremortality is less clear. The high levels of mobility whichare often reported in populations living far from serviceswere upheld by our study (expressed through high carownership), but the areas most remote from hospitalsbegin to show a decrease in levels of car ownership. It isunlikely that this indicates less need for private transport,and may indicate a less wealthy population for whomtravel is a potential problem.
There are a number of important limitations to our study.We have explored only one region of England, a relativelyaffluent area with a very small ethnic minority populationand an unusual 'peninsular' geography. Our findings needto be reproduced in other areas. We have limited our def-inition of access to simple geographical measures. Otheraspects of accessibility include the quantity and quality ofhealth services, and financial and cultural barriers to theiruse, and have not been explored here. The choice of SMRsand LLTI rates as health outcome indicators may haveresulted in our inability to observe stronger relationshipsbetween geographical access and health: even over a sixyear period absolute numbers of deaths were low. Moreresearch is needed including the young and elderly andusing a wider range of health status measures. Finally, theinter relationship between use of health care, need andaccess has been insufficiently explored.
Age structure of wards by straight-line distance from DGHFigure 4Age structure of wards by straight-line distance from DGH. average proportion of young (under 5) and elderly (over 65) population for deciles of Wards by straight line distance from DGH
Table 3: Median values for health outcomes and car ownership for deciles of ward by straight-line distance from DGH
Closest 2 3 4 5 6 7 8 9 Furthest
LLTI SMR (0–64) 1.08 1.02 0.92 0.84 0.85 0.89 0.85 0.87 0.89 1.02All-cause SMR (0–64) 1.08 0.99 0.93 0.91 0.87 0.93 0.88 0.91 0.96 0.94Proportion of households with No car
34.2 29.3 25.4 20.4 20.3 21.0 20.1 20.7 20.2 23.1
Two or more cars 20.0 23.2 27.8 32.1 33.2 32.0 32.8 32.5 31.2 27.0
144145145145145145145145145144N =
deciles of wards by straight line distance from the nearest DGH
furthest98765432closest
pro
po
rtio
no
ver
65
(%)
40
30
20
10
0
-10
144145145145145145145145145144N =
deciles of wards by straight line distance from the nearest DGH
furthest98765432closest
pro
port
ion
un
de
r5
(%)
16
14
12
10
8
6
4
2
0
Page 6 of 9(page number not for citation purposes)

International Journal of Health Geographics 2004, 3:21 http://www.ij-healthgeographics.com/content/3/1/21
ConclusionsThis paper has provided a population-based estimate foraccess to both primary and secondary health care in SouthWest England. We have shown that although geographicalaccess to health services is generally good, remotenessfrom health services is an issue which affects both urbanand rural areas. Studies concentrating purely on ruralareas are therefore likely to underestimate the extent ofgeographical barriers to accessing health care. Areas whichwere furthest from hospitals did not have an especially oldor young population, but there was some evidence ofhigher rates of LLTI and of deprivation in the most remotewards, indicating higher need for services in the areas fur-thest from them. Finally, the fact that almost a quarter ofhouseholds in the decile of wards most remote from hos-pital services had no car in 1991 indicated a large numberof people for whom travel is likely to be more difficultthan implied by current measures of geographical access.
Our understanding of the effect of distance on the use ofservices and on health outcomes is far from complete.Both the measurement of access and the understanding ofneed and deprivation require further exploration. Thedevelopment of web-based public transport informationsystems may supply the data needed to enhance currentlyavailable measures of access by adding public transporttravel times, likely to be relevant to access for the poorestand most deprived populations and the introduction ofthe Indices of Multiple Deprivation 2000 in England maypresent a clearer picture of the need for health care thantraditional census-based indices [32]. This index containsa measure of geographical access to services, which hasbeen of particular interest to rural populations and mayprovide a missing dimension to the measurement of dep-rivation. Linking geographical access with a wider range ofhealth status measures and health care use in differentpopulations is also vital if a clear picture of the impact ofaccessibility of health care is to be fully understood.
MethodsMeasuring geographical access to health servicesA Geographical Information System (Arc/Info) and cus-tom written programs were used to calculate two meas-
ures of access to health services. Access was calculatedfrom all residential postcodes to primary care services (allmain and branch General Practice (GP) surgeries) and sec-ondary care services (acute hospitals (DGHs)) in theregion. Data on main and branch GP surgeries (n = 1469)were obtained from all Family Health Services Authoritiesin 1998. Acute DGHs (n = 39) were defined as hospitalswith general medicine and general surgery facilities andan Accident and Emergency department. DGHs wereidentified using the hospital year-books (1992–97) andhospitals were contacted to clarify their status in 1997 asnecessary.
The first access measure calculated was a widely usedmeasure: the shortest straight-line distance between everyresidential postcode, the closest GP (both main andbranch) and the closest DGH. A more complex measure ofaccess was the shortest drive-time from each residentialpostcode to the closest GP and the closest DGH. This wasmodelled using estimated road-network travel speedsalong the Bartholomew digital road network and associat-ing these with residential postcode locations by the use ofa travel time (drive-time) surface model. While includingprovision for congestion and slow travel through urbanareas, this measure does not include any estimates forparking times or transfers between car and surgery or hos-pital. The methods are described in detail elsewhere [33].
The need for health careProxy measures of the need for health care were calcu-lated. The Townsend score, a widely used indicator ofmaterial deprivation, was calculated from 1991 censusdata. The variables used in the score are the percentage ofeconomically active people over the age of 16 who areunemployed; the percentage of households which areovercrowded; the percentage of households with no carand the percentage of households not owning their ownhome. A log transformation is applied to the overcrowd-ing and unemployment variables. The logged variablesand the car ownership and owner occupation variables are
Table 4: Aggregating household level access data to wards
Ward Postcode N Households from each postcode in Ward1
Time from PC to health services
Households * time
Ward1 PC1 10 10 100Ward1 PC2 7 13 91Ward1 PC3 2 11 22Ward1 PC4 6 21 126Sum (Ward1) 25 339
Population weighted average time for Ward1 ((hhds*time)/hhs)
Page 7 of 9(page number not for citation purposes)

International Journal of Health Geographics 2004, 3:21 http://www.ij-healthgeographics.com/content/3/1/21
standardised by creating z-scores for each value, and thefour z-scores are summed to provide the final Townsendscore. Scores are standardised to give a mean of zero forEngland and Wales: any scores greater than zero indicaterelative deprivation, any less than zero represent relativeaffluence. The proportions of the population over 65 andunder 5 years old – were taken from the 1991 CensusSmall Area Statistics (SAS). Health status was assessedusing indirectly standardised rates of all-cause mortalityand Limiting Long Term Illness (LLTI) for all those under65 (premature mortality and morbidity). Data on LLTIwere taken from the 1991 Census. The Office for NationalStatistics (ONS) provided data on all-cause mortality forthe years 1991–1996. Data were aggregated over the sixyears, to minimise problems due to small numbers ofcases in some wards.
Assigning data to geographical areasPostcodes were allocated to 1991 Census wards using the1991 and subsequent postcode to enumeration districtdirectories. Travel times and distances were calculated forall residential postcodes and aggregated to ward level for
analysis. The resident population of each ward was usedto weight individual postcode times and distances to cre-ate a population-weighted average, as demonstrated intable 4. ONS ward classifications were used to select 'rural'wards [34]. The ONS classifications are listed in table 5.Only two categories: 'rural areas' and 'rural fringe', areunambiguously rural under this definition and we havedefined than as rural here. All other wards were defined asurban.
AnalysesTo investigate if straight-line distance was a valid proxy forthe more complex drive-time measure, the two were com-pared using Pearson correlation coefficients and aregression analysis of drive-time against straight-line dis-tance. Areas where straight-line distance appeared tounderestimate the drive-time more than expected wereidentified and mapped to investigate the extent of geo-graphical clustering. Access to primary and secondaryhealth services was described using median distances andinter-quartile ranges for both measures.
To investigate the assumption that it is the residents ofrural areas who are most disadvantaged by poorgeographical access to health services, we first had todefine poor access. Standard estimates of 'remoteness'from health services have not been established – there isno a priori definition of the distance regarded as 'remotefrom health services' and no consensus has been estab-lished in the literature on access to health services. Theproportion of rural, rural fringe and urban wards whichwere 'remote' from health services under the definition ofa straight-line distance of three, five or seven kilometres toa GP and 20, 25, 30 or 35 km to a hospital was thereforecalculated (Table 6). We used an arbitrary cut-off point ofa straight-line distance of 5 km to a GP and 25 km to ahospital, beyond which wards were classed as 'remote'from health services. These distances classified approxi-mately 6% of the study population as remote from sec-ondary care and 3% as remote from primary care.
Table 5: The ONS ward classification
ONS group Rural / urban classification
Suburbia UrbanRural areas RuralRural fringe RuralIndustrial areas UrbanMiddling Britain UrbanProsperous areas UrbanInner city estates UrbanEstablished owner occupiers UrbanTransient populations UrbanMetropolitan professionals UrbanDeprived city areas UrbanLower status owner occupiers UrbanMature populations UrbanDeprived industrial areas Urban
Table 6: ONS rurality and remoteness from primary and secondary care
Rural Rural fringe Urban No classification Total wards
All wards 253 (18%) 154 (11%) 1031 (71%) 10 (1%) 1448 (100%)GPs
Remote (3 km) 117 (53%) 14 (6%) 84 (38%) 6 (3%) 221 (100%)Remote (5 km) 20 (53%) 4 (10%) 12 (32%) 2 (5%) 38 (100%)Remote (7 km) 5 (71%) 1 (14%) 0 (0%) 1 (14%) 7 (100%)
HospitalsRemote (20 km) 126 (39%) 36 (11%) 158 (49%) 4 (1%) 324 (100%)Remote (25 km) 69 (43%) 8 (5%) 81 (51%) 2 (1%) 162 (100%)Remote (30 km) 30 (49%) 1 (2%) 28 (46%) 2 (3%) 61 (100%)Remote (35 km) 17 (59%) 0 (0%) 12 (41%) 0 (0%) 29 (100%)
Page 8 of 9(page number not for citation purposes)

International Journal of Health Geographics 2004, 3:21 http://www.ij-healthgeographics.com/content/3/1/21
Publish with BioMed Central and every scientist can read your work free of charge
"BioMed Central will be the most significant development for disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
We then identified the proportion of remote wards thatwere rural under the ONS classification. To investigaterelationships between distance to health services and theneed for health care, straight-line distance to hospital wasused to group wards into deciles and the deprivation scoreand the age profile of the population in each decile wasdescribed. Standardised rates for premature all-cause mor-tality and LLTI were used to indicate health outcomes foreach decile of wards, and car ownership (as reported inthe 1991 census) was used to indicate how easy travelwould be for the population in each group.
Authors' contributionsHJ carried out the analyses and drafted the manuscript.HJ, PR, and DM collaborated in the formation of theresearch questions, the management of the study and thedevelopment of the paper. HJ and SB collected the dataand calculated measures of deprivation, health and acces-sibility. DM designed the drive-time access measure. Allauthors read and approved the final manuscript.
References1. The NHS Performance Assessment Framework: London: NHS
Executive; 1999. 2. Goddard M, Smith P: Equity of access to health care services:
theory and evidence from the UK. Soc Sci Med 2001,53:1149-1162.
3. Rogers A, Flowers J, Pencheon D: Improving access needs awhole systems approach. BMJ 1999, 319:866-867.
4. Gulliford M, Figueroa-Munoz J, Morgan M, Hughes D, Gibson B,Beech R, Hudson M: What does access to health care mean? JHealth Serv Res Policy 2002, 7:186-188.
5. Posnett J: Is bigger better? Concentration in the provision ofsecondary care. BMJ 1999, 319:1063-1065.
6. Smith R: Reconfiguring acute hospital services. BMJ 1999,319:797-798.
7. Baird A, Donnelly C, Miscampell N, Wemyss H: Centralisation ofcancer services in rural areas has disadvantages. BMJ 2000,320:717.
8. Jones AP, Bentham G, Harrison BD, Jarvis D, Badminton RM, Ware-ham NJ: Accessibility and health service utilization for asthmain Norfolk, England. J Public Health Med 1998, 20:312-317.
9. Haynes R, Bentham CG, Lovett A, Gale S: Effects of distances tohospital and GP surgery on hospital inpatient episodes, con-trolling for needs and provision. Soc Sci Med 1999, 49:425-433.
10. Jones AP, Bentham G: Health service accessibility and deathsfrom asthma in 401 local authority districts in England andWales, 1988–92. Thorax 1997, 52:218-222.
11. Campbell NC, Elliott AM, Sharp L, Ritchie LD, Cassidy J, Little J:Rural factors and survival from cancer: Analysis of Scottishcancer registrations. Br J Cancer 2000, 82:1863-1866.
12. Hyndman JCG, Holman CD, Dawes VP: Effect of distance andsocial disadvantage on the response to invitations to attendmammography screening. J Medical Screening 2000, 7:141-145.
13. Martin D, Roderick P, Diamond I, Clements S, Stone N: Geograph-ical aspects of the uptake of renal replacement therapy inEngland. Int J Population Geography 1998, 4:227-242.
14. Sommers I: Geographic location and mental health servicesutilization among the chronically mentally ill. Community Men-tal Health Journal 1989, 25:132-144.
15. Haynes R, Bentham CG: The effects of accessibility on generalpractitioner consultations, out-patient attendances and in-patient admissions in Norfolk, England. Soc Sci Med 1982,16:561-569.
16. Gregory PM, Malka ES, Kostis JB, Wilson AC, Arora JK, Rhoads GG:Impact of geographic proximity to cardiac revascularizationservices on service utilization. Medical Care 2000, 38:45-57.
17. McKee CM, Gleadhill DN, Watson JD: Accident and emergencyattendance rates: variation among patients from differentgeneral practices. Br J Gen Pract 1990, 40:150-153.
18. Rural Development Commission: Community and voluntarytransport in rural England. Rural Research Series 23 Salisbury:RDC; 1996.
19. Cassar K, Godden DJ, Duncan JL: Community mortality afterruptured abdominal aortic aneurysm is unrelated to the dis-tance from the surgical centre. Br J Surgery 2001, 88:1341-1343.
20. Campbell NC, Elliott AM, Sharp L, Ritchie LD, Cassidy J, Little J:Rural and urban differences in stage at diagnosis of colorec-tal and lung cancers. Br J Cancer 2001, 84:910-914.
21. Stark CR, Reay L, Shiroyama C: The effect of access factors onbreast screening attendance on two Scottish islands. HealthBull (Edinb) 1997, 55:316-321.
22. Diamond I, Clements S, Stone N, Ingham R: Spatial variation inteenage conceptions in south and west England. J R Statist SocA 2002, 162:273-289.
23. Whitehouse CR: Effect of distance from surgery on consulta-tion rate in an urban practice. BMJ 1985, 290:359-362.
24. Sherwood KB, Lewis GJ: Accessing health care in a rural area:an evaluation of a voluntary medical transport scheme in theEnglish Midlands. Health & Place 2000, 6:337-350.
25. Mosley MJ: Accessibility: the rural challenge. Methuen 1979.26. Cloke P, Milbourne P, Thomas C: Lifestyles in rural England. Rural
Research 18, Wiltshire: Rural Development Commission 1994.27. Bentham CG: Factors affecting non-response to cervical cytol-
ogy screening in Norfolk, England. Soc Sci Med 1995,40:131-135.
28. Lovett A, Haynes R, Sunnenberg G, Gale S: Car travel time andaccessibility by bus to general practitioner services: a studyusing patient registers and GIS. Soc Sci Med 2002, 55:97-111.
29. Lovett A, Haynes R, Sunnenberg G, Gale S: Accessibility of pri-mary health care services in East Anglia. Research Reports (9)Norwich: School of Health Policy and Practice, UEA 2000.
30. Knox P: The intraurban ecology of primary medical care: pat-terns of accessibility and their policy implications. Environmentand Planning A 1978, 10:415-435.
31. Barnett S, Roderick P, Martin D, Diamond I: A multilevel analysisof the effects of rurality and social deprivation on prematurelimiting long term illness. J Epidemiol Community Health 2001,55:44-51.
32. Department of Environment Transport and the Regions: Indices ofdeprivation 2000. Regeneration Research Summary 31 London:DETR; 2000.
33. Martin D, Wrigley H, Barnett S, Roderick P: Increasing the sophis-tication of access measurement in a rural healthcare study.Health & Place 2002, 8:3-13.
34. Wallace M, Charlton J, Denham C: The new OPCS areaclassifications. Population Trends 79, 15–30 London: HMSO; 1995.
Page 9 of 9(page number not for citation purposes)