Embed Size (px)
Citation preview

Disease in childhood and the impact of childcareDepartment of Epidemiology Research, Statens Serum Institut,
Copenhagen, Denmark
Mads Kamper-Jørgensen
Mad
s Kam
per-Jø
rgen
sen D
isease in ch
ildhood an
d th
e impact o
f child
care
MADS_PHD_01_BB.indd 1MADS_PHD_01_BB.indd 1 07-08-2007 22:42:5007-08-2007 22:42:50
1
Disease in childhood and the impact of childcare
PhD thesis by Mads Kamper-Jørgensen,
MSc (Public Health), 2007
Supervisors: Jan Wohlfahrt, MSc, DMSc and Christine Stabell Benn, MD, PhD
Department of Epidemiology Research,
Statens Serum Institut, Copenhagen, Denmark
Faculty of Health Sciences,
University of Copenhagen, Denmark
2
The thesis was handed in on 30 April, 2007 for evaluation at the University of Copenhagen, and accepted on 1 August 2007 for public defence of the PhD degree. The evaluators are: Freddy Karup Pedersen, Professor, Clinic of Pediatrics II, National University Hospi-tal Rigshospitalet, Copenhagen, Denmark Henrik Toft Sørensen, Professor, Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark Per Magnus, Professor, Division of Epidemiology, Institute of Public Health, Oslo, Norway The defence will take place on 30 August, 2007 at 14.00h in the lecture room ‘Foredragssalen’ at Statens Serum Institut, Artillerivej 5, Copenhagen. The thesis can be obtained upon request to the author ([email protected])
3
Acknowledgements
The present thesis contains the essence of three educational and shaping years, engaged
in epidemiological questions of disease in childhood and childcare. I am indebted to my
supervisors and colleagues, to financial contributors, and to family and friends.
My work was conducted at Department of Epidemiology Research, Statens Serum Institut,
an inspiring and thriving research environment. Jan Wohlfahrt and Christine Stabell Benn
has been been my supervisors; not only are they competent researchers, they are also
pleasant to be around. Jan Wohlfahrt has generously shared his unique scientific insight
with me and taught me the value of quantifying rather than speculating. Christine Stabell
Benn’s ability to generate inventive research ideas has been a constant source of inspira-
tion; she has also backed me up when needed. I admire the scientific curiosity, which both
Jan Wohlfahrt and Christine Stabell Benn possess.
I would like to thank Mads Melbye for advice on my professional life, Jacob Simonsen for
patience and data preparation, Peter Bager for good talks, Annemette Kristensen for proof
reading manuscripts and thesis, Helle Jørgensen for handling economic matters, and my
other colleagues at Department of Epidemiology Research for high spirits and fruitful dis-
cussions. I also thank Alistair Woodward for facilitating and supervising me during my stay
at School of Population Health, University of Auckland.
Disease in childhood and the impact of childcare
4
I acknowledge the following contributors for financing the included studies: the Health In-
surance Foundation, the Egmont Foundation, the Danish Graduate School in Public Health
Science, the Danish Foundation of Child Cancer, Rosalie Petersens Fond, Gangstedfonden,
Aase og Ejnar Danielsens Fond, and the National Union of Nursery and Childcare Assis-
tance.
Finally, I am grateful to my family for continuous support, to my friends for sharing my
passion for rock’n’roll and to Annegrete Juul Nielsen for daily inspiration.
Mads Kamper-Jørgensen
August, 2007
Disease in childhood and the impact of childcare
5
The present thesis is based on the following five original studies, referred to by their ro-
man numerals in the text. All studies were approved by the Danish Data Protection Agen-
cy (reference number 2001-41-1445).
I Kamper-Jørgensen M1, Wohlfahrt J1, Simonsen J1, Thrane N3, Benn CS2. Temporal
trend in paediatric infections in Denmark. Archives of Disease in Childhood.
2006;91:401-4
II Kamper-Jørgensen M1, Wohlfahrt J1, Simonsen J1, Benn CS2. The Childcare Database:
a valuable register-linkage. Scandinavian Journal of Public Health 2007;35(3):323-9
III Kamper-Jørgensen M1, Wohlfahrt J1, Simonsen J1, Grønbæk M4, Benn CS2. Popula-
tion-based study of the impact of childcare attendance on hospitalizations for acute
respiratory infections. Pediatrics 2006;118:1439-46
IV Kamper-Jørgensen M1, Benn CS2, Simonsen J1, Thrane N3, Wohlfahrt J1. Determinants
of clustering of acute respiratory infection hospitalizations in childcare facilities. Sub-
mitted
V Kamper-Jørgensen M1, Woodward A5, Wohlfahrt J1, Benn CS2, Simonsen J1, Hjalgrim
H1, Schmiegelow K6. Childcare in the first 2 years of life reduces the risk of childhood
acute lymphoblastic leukemia. Leukemia 2007; doi:10.1038/sj.leu.2404884
1Department of Epidemiology Research, Statens Serum Institut, Denmark 2Bandim Health Project, Statens Serum Institut, Denmark 3Department of Pediatrics, Herning Central Hospital, Denmark 4National Institute of Public Health, Denmark 5School of Population Health, University of Auckland, New Zealand 6Pediatric Clinic, The University Hospital Rigshospitalet, Denmark

Disease in childhood and the impact of childcare
6
Disease in childhood and the impact of childcare
7
Contents
1. Introduction .....................................................................................................................9
2. Background ....................................................................................................................10
2.1. Childcare attendance .............................................................................................. 10
2.2. Respiratory infection................................................................................................ 12
2.3. Childhood acute lymphoblastic leukemia................................................................. 15
3. Aims ...............................................................................................................................17
4. Material ..........................................................................................................................18
4.1. Child and family data .............................................................................................. 18
4.2. Infection hospitalization data................................................................................... 18
4.3. Childcare attendance data....................................................................................... 19
4.4. Childcare facility data .............................................................................................. 19
4.5. The Childcare Database (study II) ............................................................................ 20
4.6. Childhood leukemia data......................................................................................... 22
4.7. Birth characteristics data.......................................................................................... 22
5. Methods.........................................................................................................................23
5.1. Cohort studies (studies I, III and IV) ......................................................................... 23
5.2. Case-control study (study V).................................................................................... 24
6. Results ............................................................................................................................25
6.1. Study I .................................................................................................................... 25
6.2. Study III................................................................................................................... 26
6.3. Study IV .................................................................................................................. 27
6.4. Study V ................................................................................................................... 28
Disease in childhood and the impact of childcare
8
7. Discussion.......................................................................................................................29
7.1. The temporal trend in infection hospitalizations....................................................... 29
7.2. The short-term impact of childcare.......................................................................... 30
7.3. The long-term impact of childcare........................................................................... 33
7.4. Confounding, bias and interaction........................................................................... 35
7.5. Analytical challenges ............................................................................................... 39
8. Conclusions and perspectives..........................................................................................40
8.1. Conclusions............................................................................................................. 40
8.2. Perspectives............................................................................................................. 41
9. English summary.............................................................................................................42
10. Dansk resumé ...............................................................................................................44
11. References ....................................................................................................................46
Study I................................................................................................................................53
Study II ...............................................................................................................................59
Study III ..............................................................................................................................69
Study IV..............................................................................................................................79
Study V.............................................................................................................................103
Disease in childhood and the impact of childcare
9
1. Introduction
Since the initial studies of disease in childhood and the impact of childcare in the 1930s
by authors such as Lichtenstein (1) and Gyllenswärd (2), the area has received much at-
tention and been subject to many epidemiological studies. Reasons for this great scientific
attention are that the vast majority of children are enrolled in childcare in high-income so-
cieties (3), including Denmark (4), and that childcare attendance entails a short-term in-
creased risk of acquiring childhood infections (5-53). Moreover, because transmission of
many infections in childcare facilities is easily reduced by good hygienic measures (54-58),
the field holds a huge potential for prevention. So far, only few studies have aimed and
had a sufficient sample size to study the short-term effect of childcare attendance in dif-
ferent groups of children. Hence, very little is known about which factors might modify
the increased risk of infectious diseases associated with childcare attendance. Until recent
years, focus has been put mainly on the short-term impact of childcare attendance, such
as respiratory infections, whereas less attention has been given to possible long-term ef-
fects, such as childhood cancer. The idea that childcare attendance may have an impact
on health later in life is not new, however. Already in 1953 Hesselvik (59) asked ‘to what
extent is the later health of children […] affected by day nursery infections?’’ Conflicting an-
swers to this question have been presented (60-70), but whether the association between
childcare attendance and childhood cancer is dependent on characteristics of the child-
care facility, the child and the child’s family has not been studied.
In the present thesis the impact of childcare attendance is evaluated on a short-term
and a long-term basis, respectively. The studies of the short-term impact of childcare at-
tendance focus on acute respiratory infection, whereas the study of long-term impact fo-
cuses on childhood acute lymphoid leukemia. The included studies are based on person-
identifiable prospective Danish register data with detailed information on childcare atten-
dance, child and family characteristics and disease for each child. The material used in the
present thesis is the most comprehensive to date in the area.
- Introduction
Disease in childhood and the impact of childcare
10
2. Background
2.1. Childcare attendance
In Denmark, the entrance of women into the labor market and changing family structure
towards single rather than shared parenthood have had a tremendous impact on the
availability and organization of childcare away from the child’s home. From mainly being
offered to children from socially deprived families, publicly subsidized childcare places
were offered to all pre-school children in Denmark from the mid 1960s. By then, less than
1 out of 10 pre-school children attended childcare, whereas today more than 8 out of 10
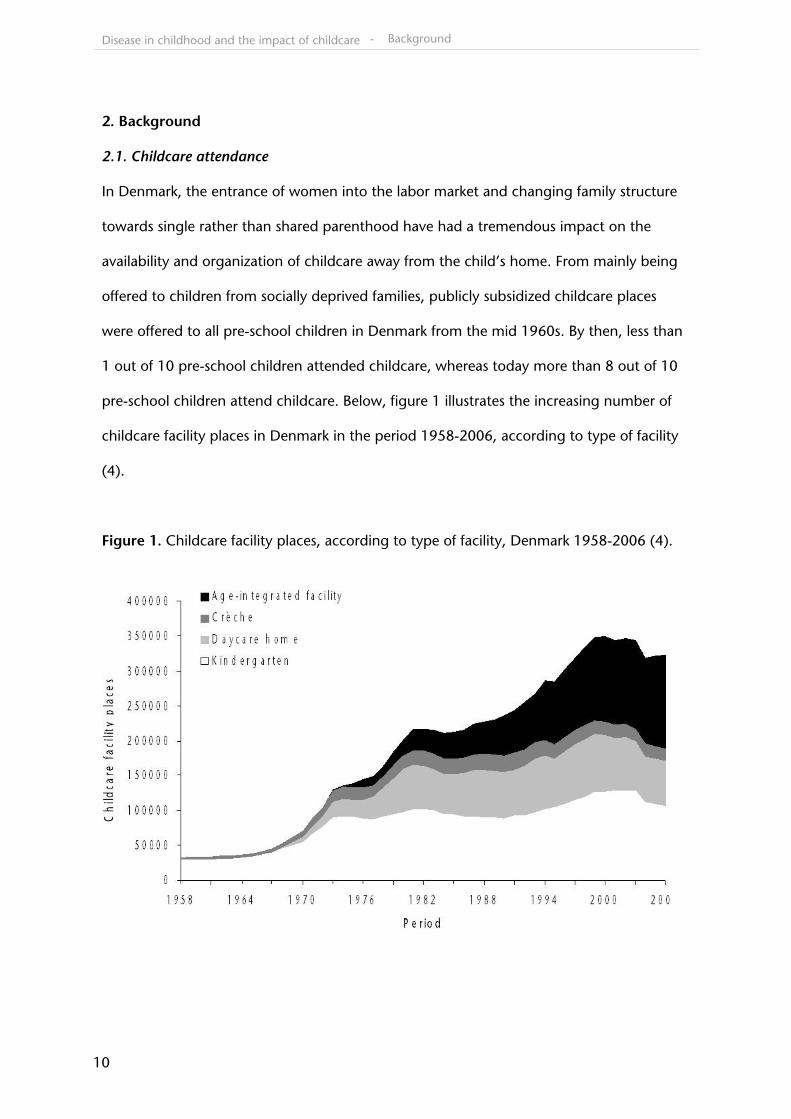
pre-school children attend childcare. Below, figure 1 illustrates the increasing number of
childcare facility places in Denmark in the period 1958-2006, according to type of facility
(4).
Figure 1. Childcare facility places, according to type of facility, Denmark 1958-2006 (4).
- Background
Disease in childhood and the impact of childcare
11
Four types of publicly subsidized childcare exist in Denmark, namely crèche, daycare
home, age-integrated facility and kindergarten. Alternatives, such as playgroups and
pooled facilities exist, but they are not publicly subsidized and very few children attend
these types. Crèches are facilities with an average of 40.8 children enrolled, targeted for
children aged 6 months to 3 years. Daycare homes are targeted for children of the same
age, but are most often run by a single child minder looking after 1-5 children. Age-
integrated facilities are targeted towards children aged 6 months to 6 years and have an
average of 73.2 children enrolled. Finally, kindergartens are facilities for children aged 3-6
years with an average of 56.3 children enrolled.
In Denmark childcare is publicly subsidized for all families. Families pay a fee corre-
sponding to a maximum of 30% of the actual cost of a place in a childcare facility, which
can be further reduced or waived for low-income families. During the period of interest in
the present thesis (1989-2004), the number of weeks allowed on parental leave with full
benefit was extended from 26 to 52 weeks. The extended parental leave applies to par-
ents of children born after 1 January 2002. The leave is voluntary and the duration can be
adjusted and, to some extent, be shared between the parents. Although hard to maintain,
most Danish municipalities guarantee a place in a public childcare facility before the child
reaches the age of 6 months.
- Background
Disease in childhood and the impact of childcare
12
2.2. Respiratory infection
Acute respiratory infection (ARI) is a collective term covering infections of the respiratory
tract, ranging from the nasal cavity to the lungs. ARI is a state of inflammation caused by
micro-organisms leading to symptoms such as sore throat, earache, fever, chest pain and
difficulty of breathing (71;72). Depending on the age of the child and the site of infection
approximately 1%-8% of ill children are admitted to hospital in Denmark (48). In study I,
distinction is made between hospitalization for upper respiratory infection (URI) and lower
respiratory infection (LRI), whereas no distinction is made in studies III and IV. Since the
etiological pathogen is not registered for most hospitalized children in Denmark, distinc-
tion in study I was made according to infection site rather than etiological pathogen. In
table 1 below, ICD-8 and ICD-10-codes denoting hospitalization for URI and LRI are
shown. In Denmark, hospitalizations were classified according to ICD-8 codes in the pe-
riod from 1989 to 1993 whereas ICD-10-codes were used from 1994 to 2004 (73).
Table 1. ICD-8 and ICD-10-codes denoting URI and LRI
Infection ICD-8 codes ICD-10 codes
URI 032, 075, 381-383, 460-465, 500-501, 503
A36, B27, H65-H72, J00-J06, J32, J35-J36
LRI 033, 466, 470-490, 510, 513
A37, J10-J22, J45.9, J85-J86
- Background
Disease in childhood and the impact of childcare
13
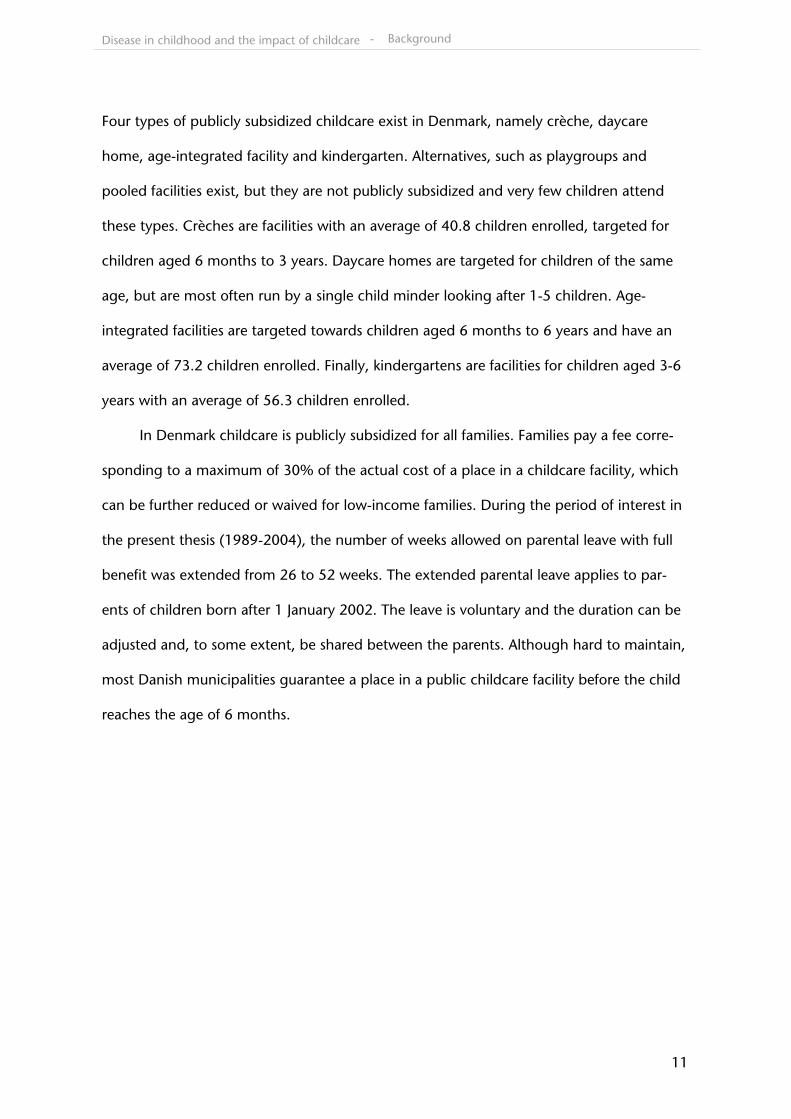
Main subtypes of URI hospitalization in children in Denmark are laryngitis, tonsillitis and
otitis media. Hospitalizations due to URI in 0-5-year-old children in Denmark in the period
1989-2004 are shown according to subtype in figure 2.
Figure 2. Hospitalizations for URI in 0-5-year-old children according to subtype, Denmark
1989-2004.
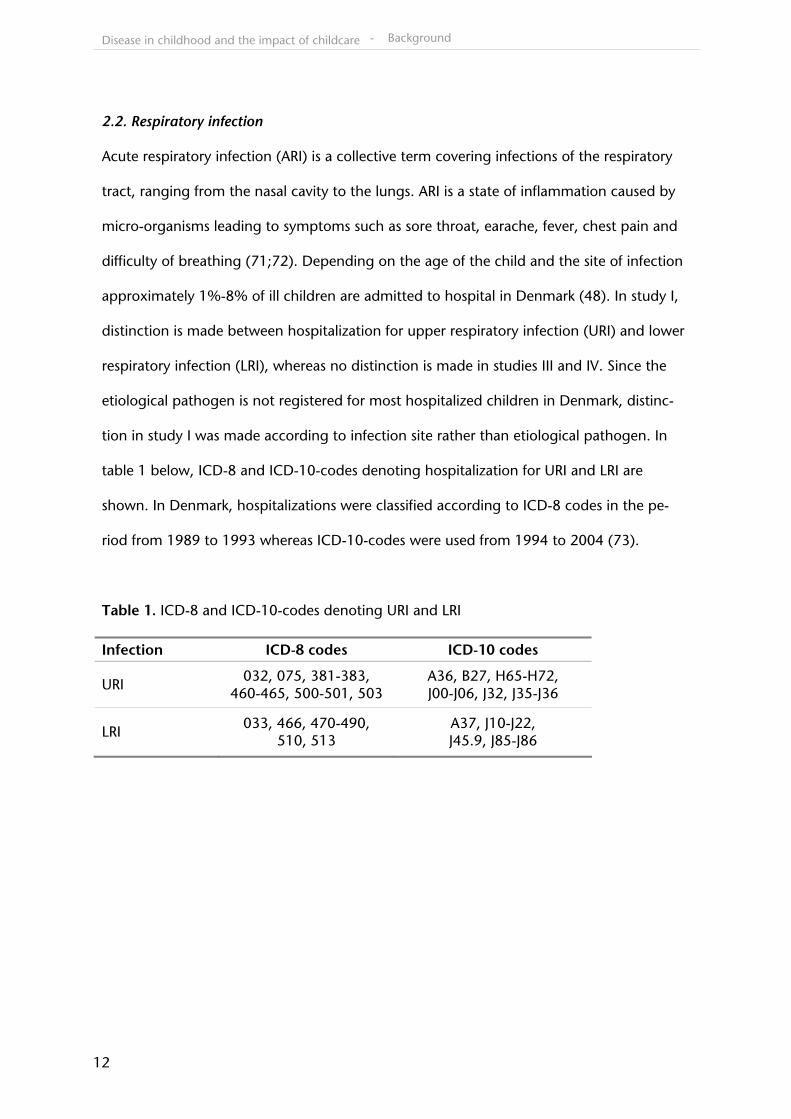
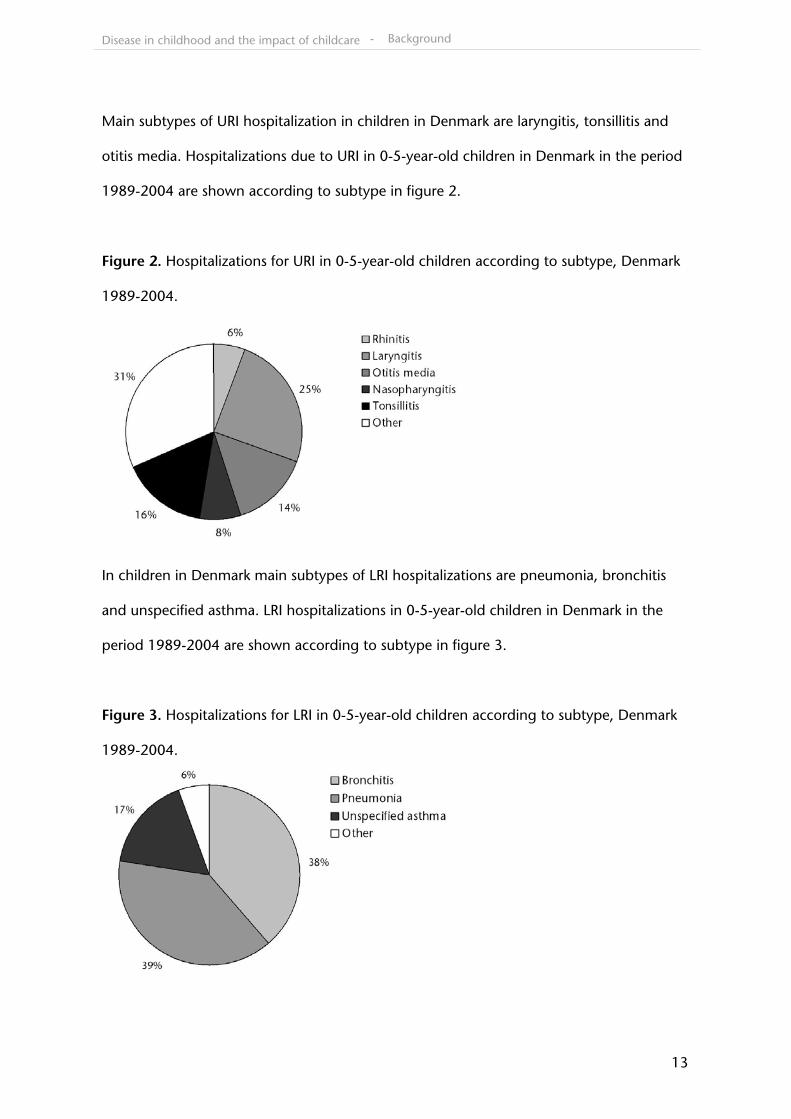
In children in Denmark main subtypes of LRI hospitalizations are pneumonia, bronchitis
and unspecified asthma. LRI hospitalizations in 0-5-year-old children in Denmark in the
period 1989-2004 are shown according to subtype in figure 3.
Figure 3. Hospitalizations for LRI in 0-5-year-old children according to subtype, Denmark
1989-2004.
- Background
Disease in childhood and the impact of childcare
14
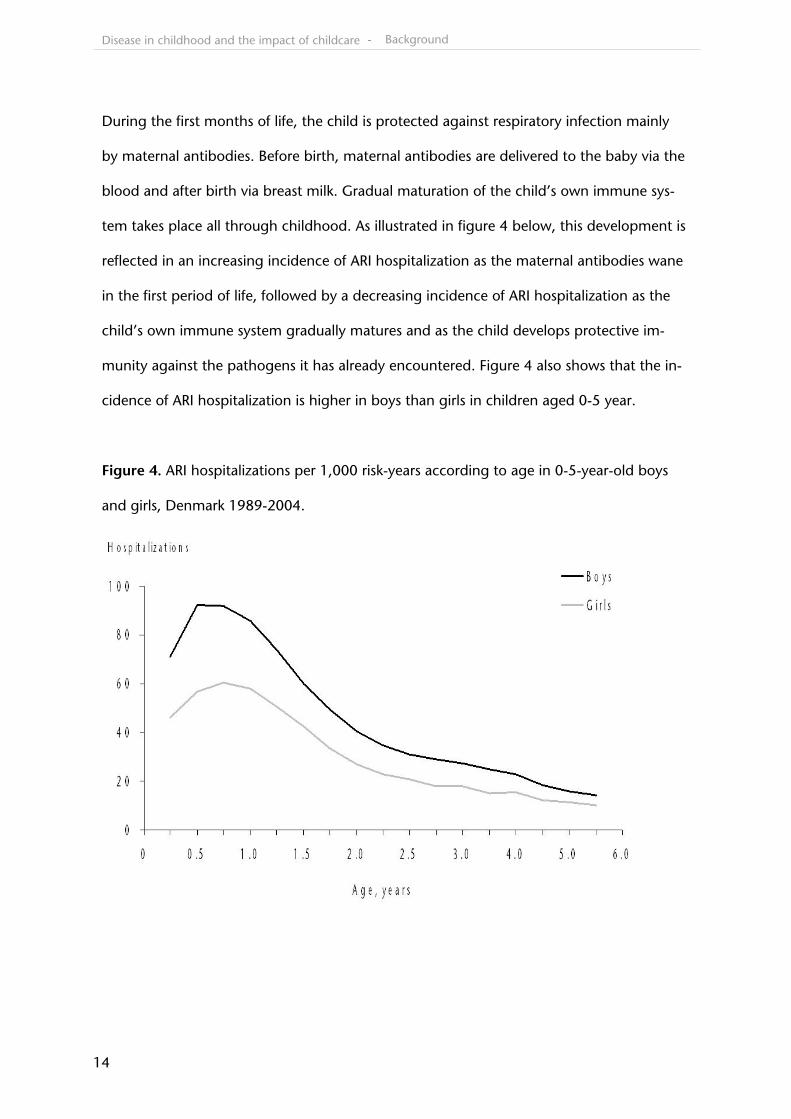
During the first months of life, the child is protected against respiratory infection mainly
by maternal antibodies. Before birth, maternal antibodies are delivered to the baby via the
blood and after birth via breast milk. Gradual maturation of the child’s own immune sys-
tem takes place all through childhood. As illustrated in figure 4 below, this development is
reflected in an increasing incidence of ARI hospitalization as the maternal antibodies wane
in the first period of life, followed by a decreasing incidence of ARI hospitalization as the
child’s own immune system gradually matures and as the child develops protective im-
munity against the pathogens it has already encountered. Figure 4 also shows that the in-
cidence of ARI hospitalization is higher in boys than girls in children aged 0-5 year.
Figure 4. ARI hospitalizations per 1,000 risk-years according to age in 0-5-year-old boys
and girls, Denmark 1989-2004.
- Background
Disease in childhood and the impact of childcare
15
2.3. Childhood acute lymphoblastic leukemia
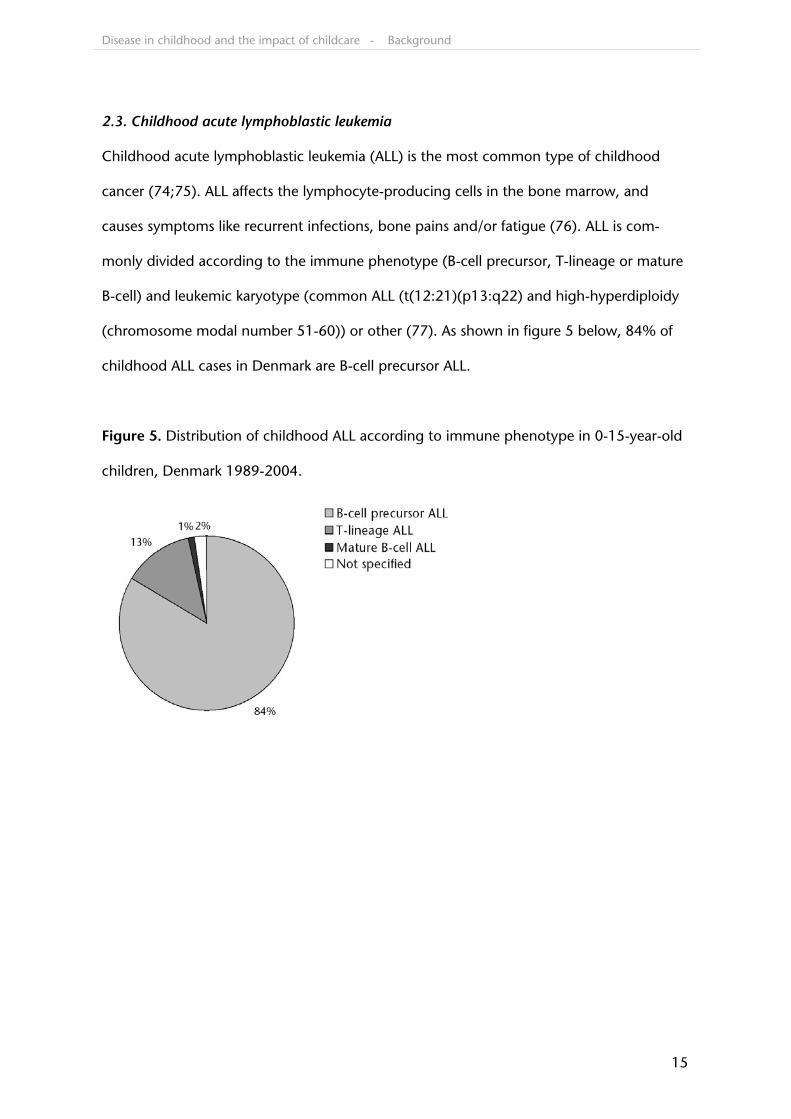
Childhood acute lymphoblastic leukemia (ALL) is the most common type of childhood
cancer (74;75). ALL affects the lymphocyte-producing cells in the bone marrow, and
causes symptoms like recurrent infections, bone pains and/or fatigue (76). ALL is com-
monly divided according to the immune phenotype (B-cell precursor, T-lineage or mature
B-cell) and leukemic karyotype (common ALL (t(12:21)(p13:q22) and high-hyperdiploidy
(chromosome modal number 51-60)) or other (77). As shown in figure 5 below, 84% of
childhood ALL cases in Denmark are B-cell precursor ALL.
Figure 5. Distribution of childhood ALL according to immune phenotype in 0-15-year-old
children, Denmark 1989-2004.
- Background
Disease in childhood and the impact of childcare
16
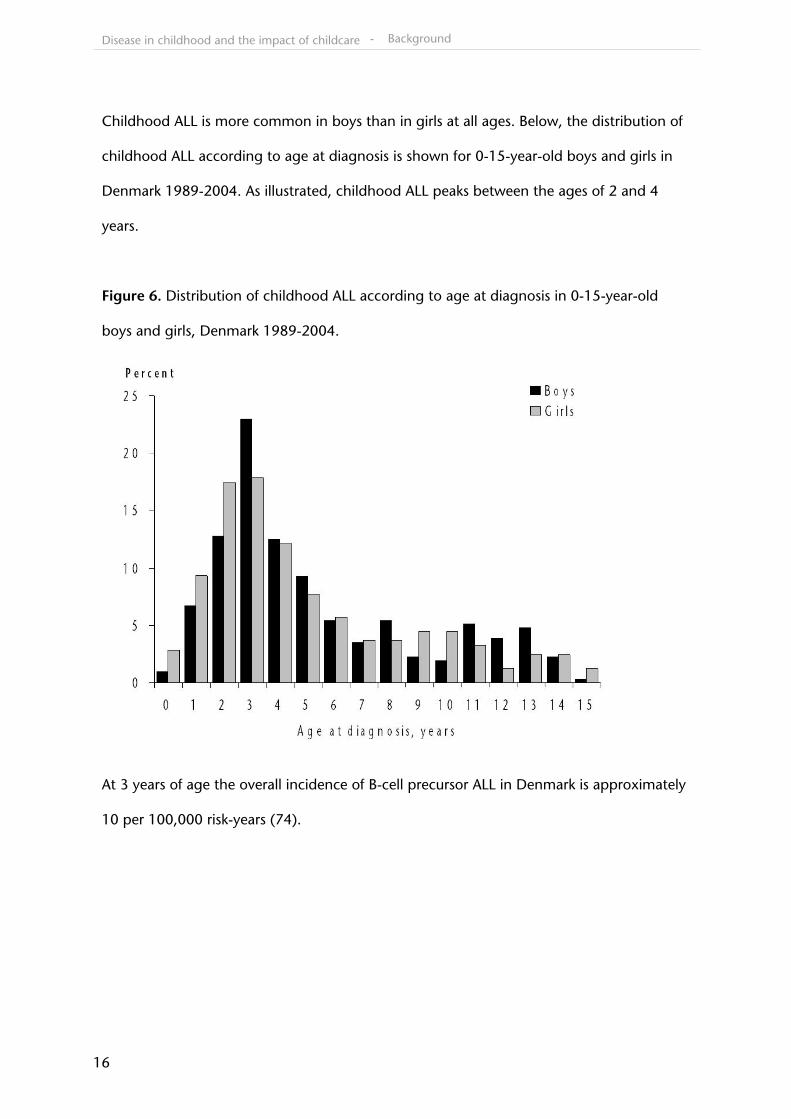
Childhood ALL is more common in boys than in girls at all ages. Below, the distribution of
childhood ALL according to age at diagnosis is shown for 0-15-year-old boys and girls in
Denmark 1989-2004. As illustrated, childhood ALL peaks between the ages of 2 and 4
years.
Figure 6. Distribution of childhood ALL according to age at diagnosis in 0-15-year-old
boys and girls, Denmark 1989-2004.
At 3 years of age the overall incidence of B-cell precursor ALL in Denmark is approximately
10 per 100,000 risk-years (74).
- Background
Disease in childhood and the impact of childcare
17
3. Aims
Below, aims are given for each of the included studies
Study I: To characterize temporal trends in the incidence of hospitalizations for infec-
tious diseases in 0-5-year-old children in Denmark in the period from 1980 to 2001
Study II: To describe the creation of, the information available in, and the potential of
the Childcare Database
Study III: To study whether the excess risk of ARI hospitalization in children attending
childcare compared with homecare varies with age, time since enrollment and other
child and family characteristics
Study IV: To characterize clustering in childcare facilities by estimating how the risk of
ARI hospitalization in children attending a childcare facility with a recently hospitalized
child (within 1 month) is modified by age, sex, and other child and family characteris-
tics
Study V: To test the hypothesis that childcare attendance early in life entails a reduced
risk of childhood ALL. Furthermore, to study whether the reduced risk is modified by
child and family characteristics
- Aims
Disease in childhood and the impact of childcare
18
4. Material
Studies included in the present thesis were based on Danish register data covering the pe-
riod 1989-2004. Children were identified by a unique person identification number, mak-
ing register linkage possible. The registers used are collected routinely for vital statistics,
health care planning and payment and distribution of childcare facility places.
4.1. Child and family data
Characteristics of children and their families were obtained from the Danish Civil Registra-
tion System (DCRS) (78;79). The DCRS encompasses all persons who have lived in Den-
mark since 1 April 1968. All individuals alive and living in Denmark on 1 April 1968 as well
as all new residents and newborn children in Denmark have since been assigned a unique
DCRS identification number. From the DCRS we extracted data regarding date of birth,
death and migrations and familial relations for all children in Denmark in the period from
1 January 1989 to 17 November 2004. Data from the DCRS was used in all the included
studies.
4.2. Infection hospitalization data
The Danish National Patient Registry (DNPR) (80-82) encompasses all contacts to hospitals
in Denmark since 1 January 1977, including in-patient and all-day contacts. For every new
contact to a hospital or transfer within a hospital, a code denoting the admission diagno-
sis is registered along with the DCRS identification number. Diagnoses in the DNPR are
coded according to the International Classification of Diseases (73). Besides the DCRS ide-
ntification number and ICD-diagnosis code(s), we obtained date(s) of admission to and
discharge from hospital from 1 January 1989 to 17 November 2004. Data from the DNPR
was used in studies I, III and IV.
- Material
Disease in childhood and the impact of childcare
19
4.3. Childcare attendance data
In Denmark all municipalities register person-identifiable data on provision of childcare.
Data is collected routinely to organize payment and distribution of places in childcare fa-
cilities. For any child, dates of enrollment and withdrawal from childcare facilities as well
as the type of childcare facility and a unique facility code were recorded. Based on mu-
nicipal data, three data management companies (KMD, GK-Consult and IST-Software)
provided person-identifiable data on children attending childcare. Data was provided for
266 of the 271 Danish municipalities. Registration of childcare attendance started at dif-
ferent times in different municipalities. The first municipalities registered childcare atten-
dance from 1 January 1989, whereas the last municipality started registering from 1 Janu-
ary 2004. Half the municipalities had started registering childcare attendance by 1 No-
vember 1991. We collected data up to 17 November 2004. Childcare attendance data
was used in studies II, III, IV and V.
4.4. Childcare facility data
Denmark’s national statistical office, Statistics Denmark (SD), routinely collects data on so-
cial and health-related resources for administrative purposes. Reporting to SD is manda-
tory and nationwide. From the SD register ‘Den sociale ressourceopgørelse’ (83), which is
an annual registration of social and health-related municipal resources available for chil-
dren, seniors and disabled persons, we obtained data regarding number of employed
teachers and number of enrolled children in each childcare facility for the year 1997. In
contrast to the other sources, data from the SD was obtained at a facility rather than a
person level. Childcare facility data was linked to the person level data via the unique
childcare facility code. Childcare facility data was used in study II.
- Material
Disease in childhood and the impact of childcare
20
4.5. The Childcare Database (study II)
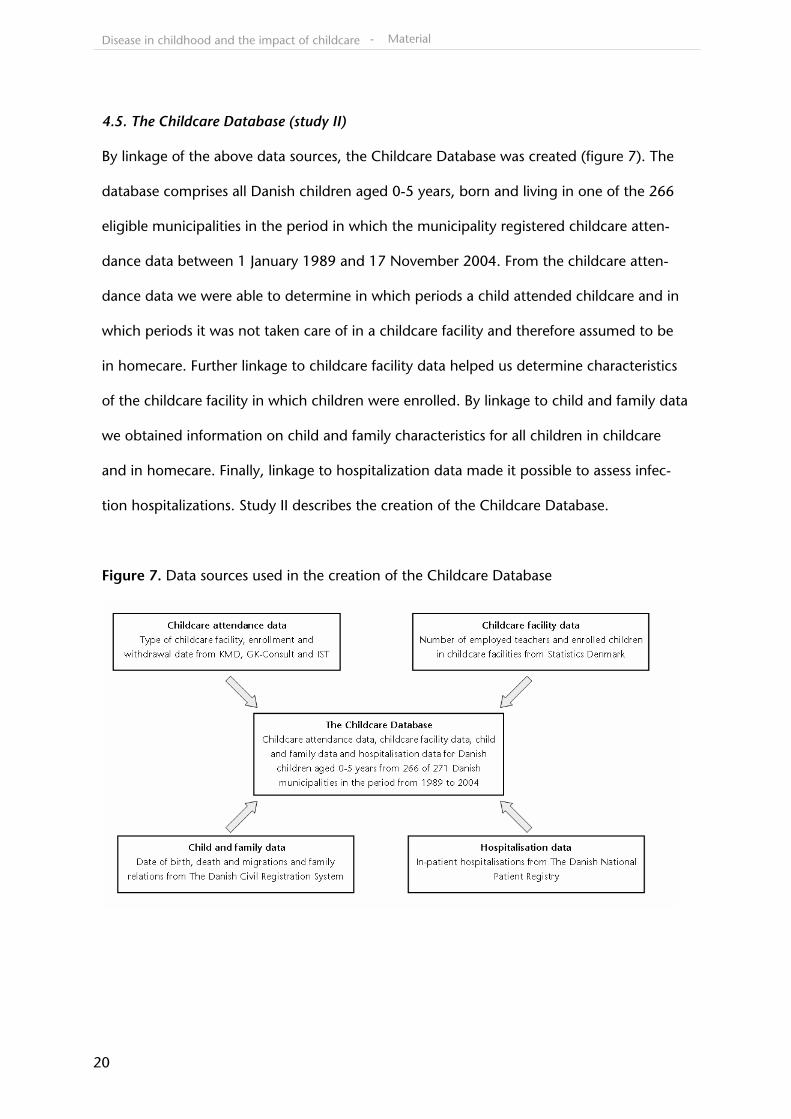
By linkage of the above data sources, the Childcare Database was created (figure 7). The
database comprises all Danish children aged 0-5 years, born and living in one of the 266
eligible municipalities in the period in which the municipality registered childcare atten-
dance data between 1 January 1989 and 17 November 2004. From the childcare atten-
dance data we were able to determine in which periods a child attended childcare and in
which periods it was not taken care of in a childcare facility and therefore assumed to be
in homecare. Further linkage to childcare facility data helped us determine characteristics
of the childcare facility in which children were enrolled. By linkage to child and family data
we obtained information on child and family characteristics for all children in childcare
and in homecare. Finally, linkage to hospitalization data made it possible to assess infec-
tion hospitalizations. Study II describes the creation of the Childcare Database.
Figure 7. Data sources used in the creation of the Childcare Database
- Material
Disease in childhood and the impact of childcare
21
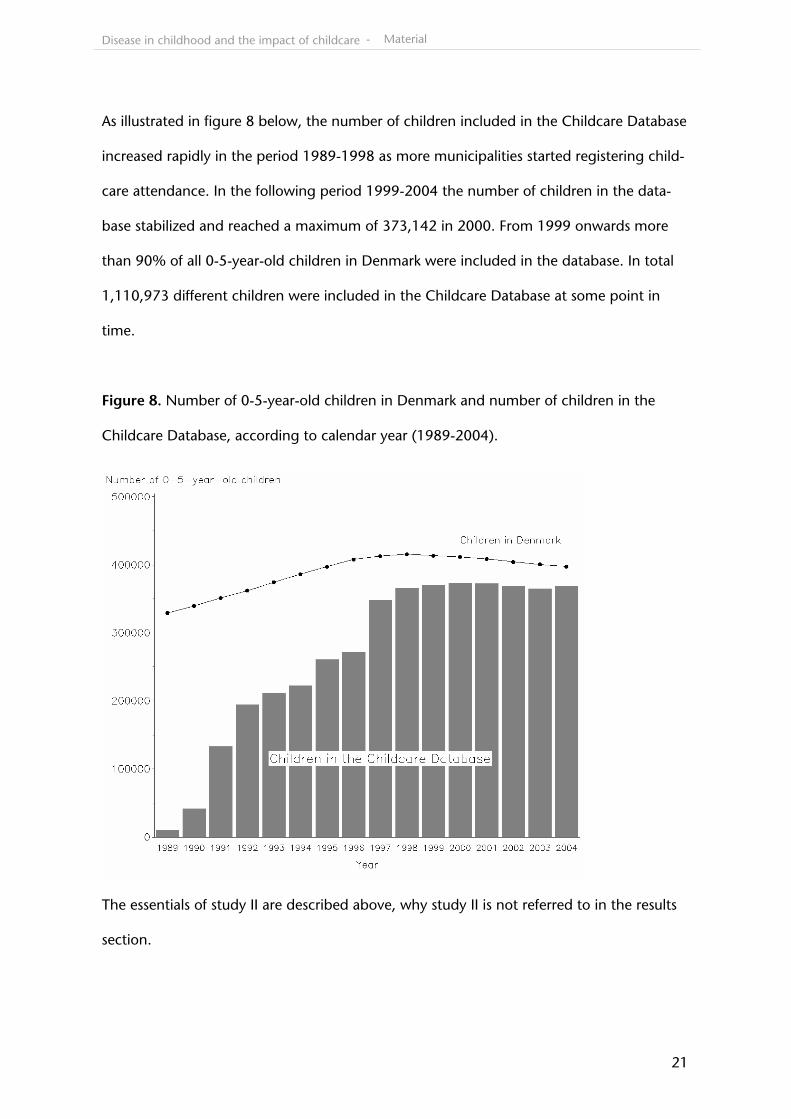
As illustrated in figure 8 below, the number of children included in the Childcare Database
increased rapidly in the period 1989-1998 as more municipalities started registering child-
care attendance. In the following period 1999-2004 the number of children in the data-
base stabilized and reached a maximum of 373,142 in 2000. From 1999 onwards more
than 90% of all 0-5-year-old children in Denmark were included in the database. In total
1,110,973 different children were included in the Childcare Database at some point in
time.
Figure 8. Number of 0-5-year-old children in Denmark and number of children in the
Childcare Database, according to calendar year (1989-2004).
The essentials of study II are described above, why study II is not referred to in the results
section.
- Material
Disease in childhood and the impact of childcare
22
4.6. Childhood leukemia data
We identified all incident cases of ALL diagnosed in children aged 0-15 years in Denmark
with a date of diagnosis between 1 January 1989 and 17 November 2004 in the Nordic
Society of Paediatric Haematology and Oncology (NOPHO) database. NOPHO have regis-
tered all pediatric ALL cases in the Nordic countries since July 1981. For each case of ALL
we obtained information on date of diagnosis, subtype of ALL and presence of Down syn-
drome at time of diagnosis. Childhood leukemia data was used in study V.
4.7. Birth characteristics data
From the Danish Medical Birth Registry (84) we obtained information on birth weight and
gestational age. The registry contains neonatal data for all children born to mothers resi-
dent in Denmark, since January 1 1973. Data on birth weight was used in studies I and V,
and information on gestational age was used in study I.
- Material
Disease in childhood and the impact of childcare
23
5. Methods
5.1. Cohort studies (studies I, III and IV)
Studies I, III and IV are prospective cohort studies based on calculation of incidence rates
(IRs) and incidence rate ratios (IRRs). IRs and IRRs with accompanying 95% confidence in-
tervals (CI) were estimated by multiple log-linear Poisson regression of the number of
hospitalizations with the logarithm of person-years at risk as offset (85). In studies III and
IV, we used a quasi Poisson regression model based on a Poisson quasi-likelihood where
the variance is allowed to be the mean multiplied by an over dispersion factor. The inci-
dence rate ratios estimates are the same as in the traditional Poisson regression model but
the confidence intervals are slightly widened (85). Estimation in studies I, III and IV was
performed by PROC GENMOD in SAS with Poisson error distribution and log link. In stud-
ies III and IV a dispersion factor estimated from Pearson statistics was included (86).
In study I, person-years at risk were calculated from one week after birth or immigra-
tion, whichever came last. The first week after birth was not included as hospitalizations in
this period were considered to be due to perinatal complications. Children were consid-
ered at risk until the first of the following events: emigration, death, sixth birthday or end
of follow-up. Studies III and IV were restricted to person-years at risk and hospitalizations
occurring in municipalities with complete registration of childcare attendance. Children
enrolled in childcare facilities as well as in homecare were included in study III, whereas
only person-years at risk and hospitalizations among children attending childcare were in-
cluded in study IV. In study I, only first-time hospitalizations and risk-years until first-time
hospitalization, emigration, death, sixth birthday or end of follow-up were included. In
studies III and IV, each admission to hospital of the same child during the follow-up period
was counted as a new hospitalization. Children were not considered at risk during the first
fourteen days following a hospitalization since hospitalizations in this period could be re-
- Methods
Disease in childhood and the impact of childcare
24
lated to the preceding hospitalization. Thus, person-years and hospitalizations in this pe-
riod were not included in the analyses.
Relevant variables were created as time-dependent variables in studies I, III and IV,
implying that the same child could contribute with person-years at risk and hospitaliza-
tions in more than one category of a variable. Examples of such time-dependent variables
are period (study I), time since enrollment (study III) and time since latest ARI hospitaliza-
tion in the childcare facility (study IV). Variables were tested and included as confounders
by forward inclusion if they changed the estimates of main interest by 5% or more. Inter-
action was evaluated using models with a two-way interaction term between relevant co-
variates.
5.2. Case-control study (study V)
Study V is a matched case-control study nested in cohort, in which we used the risk set
sampling technique (87). This implies that controls were selected among children at risk
of ALL in the Danish population at the time of diagnosis of the corresponding case. We
matched ten controls per case on sex and date of birth. Each control was assigned a date
of pseudo-diagnosis, corresponding to the date of diagnosis of the matching case.
Whether attendance to childcare was associated with risk of childhood ALL was
evaluated by rate ratios (RRs) and accompanying 95% CIs, estimated using conditional lo-
gistic regression models. Main exposure was attendance to childcare during the first two
years of life. Variables were tested and included as confounders by forward inclusion if
they changed the estimate of ever attendance to childcare by 5% or more. Homogeneity
and interactions were evaluated by Wald’s tests. Analyses in study V were performed in
SAS using the TPHREG procedure including a strata-statement, handling the matched de-
sign (86).
- Methods
Disease in childhood and the impact of childcare
25
6. Results
6.1. Study I
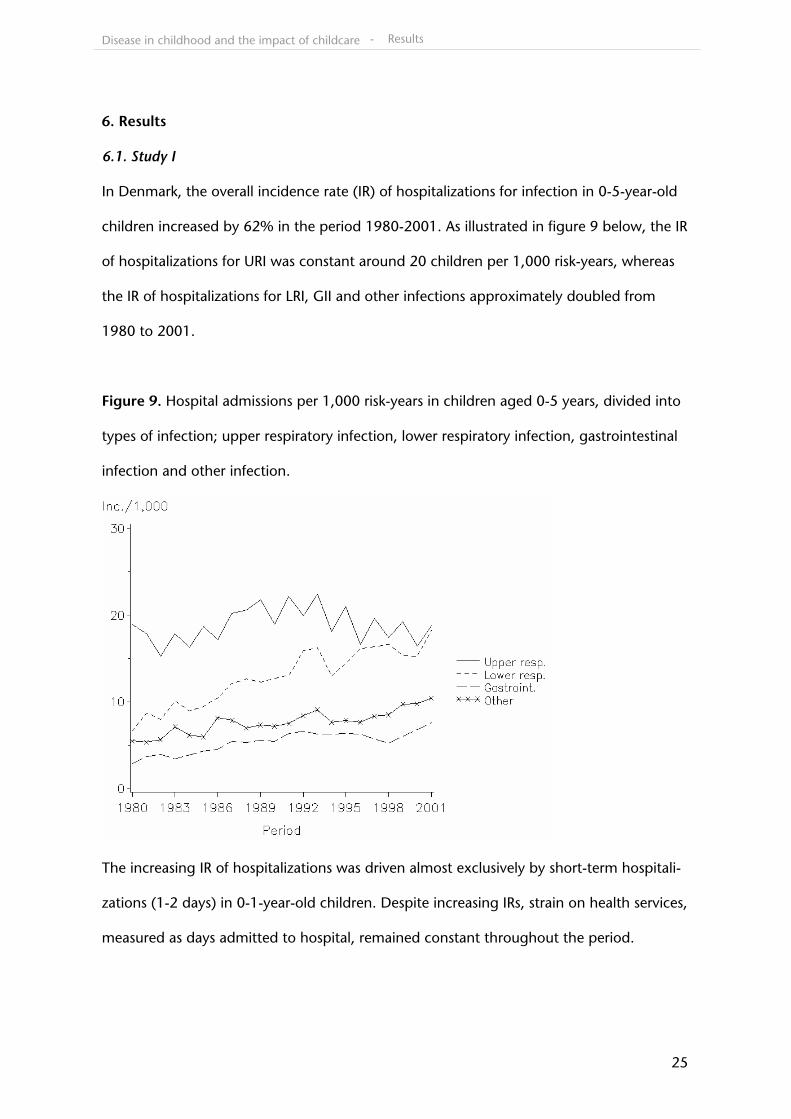
In Denmark, the overall incidence rate (IR) of hospitalizations for infection in 0-5-year-old
children increased by 62% in the period 1980-2001. As illustrated in figure 9 below, the IR
of hospitalizations for URI was constant around 20 children per 1,000 risk-years, whereas
the IR of hospitalizations for LRI, GII and other infections approximately doubled from
1980 to 2001.
Figure 9. Hospital admissions per 1,000 risk-years in children aged 0-5 years, divided into
types of infection; upper respiratory infection, lower respiratory infection, gastrointestinal
infection and other infection.
The increasing IR of hospitalizations was driven almost exclusively by short-term hospitali-
zations (1-2 days) in 0-1-year-old children. Despite increasing IRs, strain on health services,
measured as days admitted to hospital, remained constant throughout the period.
- Results
Disease in childhood and the impact of childcare
26
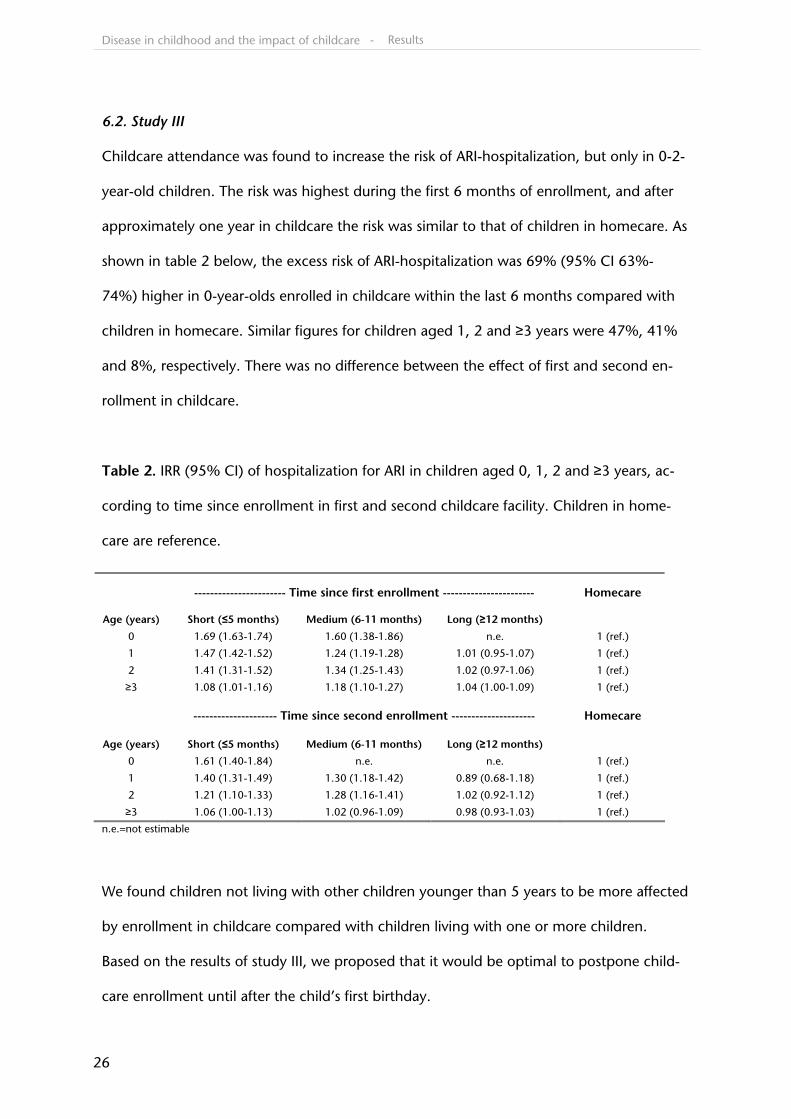
6.2. Study III
Childcare attendance was found to increase the risk of ARI-hospitalization, but only in 0-2-
year-old children. The risk was highest during the first 6 months of enrollment, and after
approximately one year in childcare the risk was similar to that of children in homecare. As
shown in table 2 below, the excess risk of ARI-hospitalization was 69% (95% CI 63%-
74%) higher in 0-year-olds enrolled in childcare within the last 6 months compared with
children in homecare. Similar figures for children aged 1, 2 and ≥3 years were 47%, 41%
and 8%, respectively. There was no difference between the effect of first and second en-
rollment in childcare.
Table 2. IRR (95% CI) of hospitalization for ARI in children aged 0, 1, 2 and ≥3 years, ac-
cording to time since enrollment in first and second childcare facility. Children in home-
care are reference.
n.e.=not estimable
We found children not living with other children younger than 5 years to be more affected
by enrollment in childcare compared with children living with one or more children.
Based on the results of study III, we proposed that it would be optimal to postpone child-
care enrollment until after the child’s first birthday.
----------------------- Time since first enrollment ----------------------- Homecare
Age (years) Short (≤5 months) Medium (6-11 months) Long (≥12 months)
0 1.69 (1.63-1.74) 1.60 (1.38-1.86) n.e. 1 (ref.)
1 1.47 (1.42-1.52) 1.24 (1.19-1.28) 1.01 (0.95-1.07) 1 (ref.)
2 1.41 (1.31-1.52) 1.34 (1.25-1.43) 1.02 (0.97-1.06) 1 (ref.)
≥3 1.08 (1.01-1.16) 1.18 (1.10-1.27) 1.04 (1.00-1.09) 1 (ref.)
--------------------- Time since second enrollment --------------------- Homecare
Age (years) Short (≤5 months) Medium (6-11 months) Long (≥12 months)
0 1.61 (1.40-1.84) n.e. n.e. 1 (ref.)
1 1.40 (1.31-1.49) 1.30 (1.18-1.42) 0.89 (0.68-1.18) 1 (ref.)
2 1.21 (1.10-1.33) 1.28 (1.16-1.41) 1.02 (0.92-1.12) 1 (ref.)
≥3 1.06 (1.00-1.13) 1.02 (0.96-1.09) 0.98 (0.93-1.03) 1 (ref.)
- Results
Disease in childhood and the impact of childcare
27
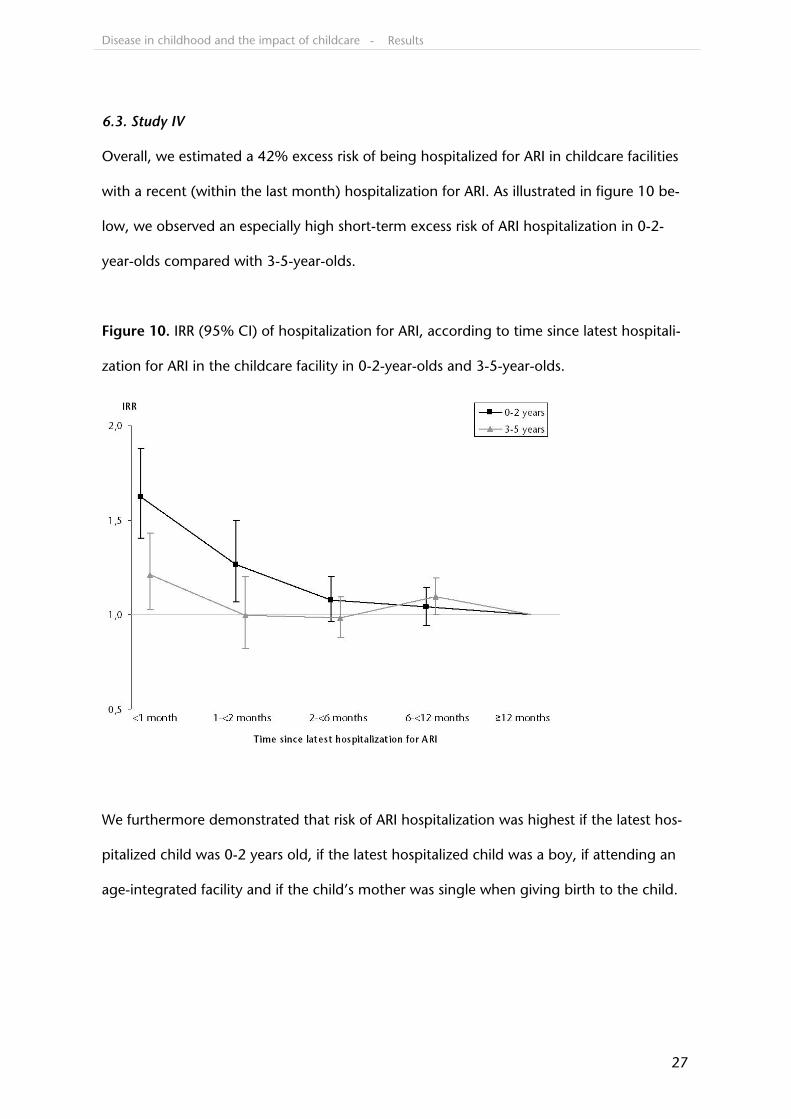
6.3. Study IV
Overall, we estimated a 42% excess risk of being hospitalized for ARI in childcare facilities
with a recent (within the last month) hospitalization for ARI. As illustrated in figure 10 be-
low, we observed an especially high short-term excess risk of ARI hospitalization in 0-2-
year-olds compared with 3-5-year-olds.
Figure 10. IRR (95% CI) of hospitalization for ARI, according to time since latest hospitali-
zation for ARI in the childcare facility in 0-2-year-olds and 3-5-year-olds.
We furthermore demonstrated that risk of ARI hospitalization was highest if the latest hos-
pitalized child was 0-2 years old, if the latest hospitalized child was a boy, if attending an
age-integrated facility and if the child’s mother was single when giving birth to the child.
- Results
Disease in childhood and the impact of childcare
28
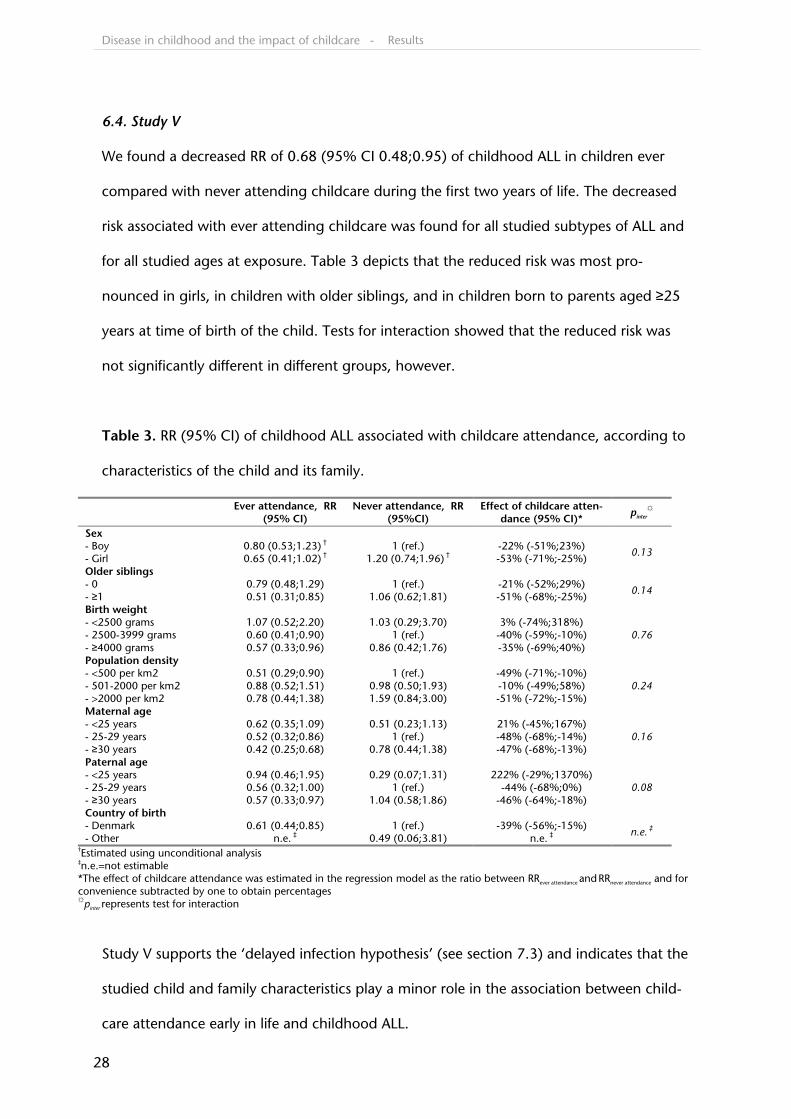
6.4. Study V
We found a decreased RR of 0.68 (95% CI 0.48;0.95) of childhood ALL in children ever
compared with never attending childcare during the first two years of life. The decreased
risk associated with ever attending childcare was found for all studied subtypes of ALL and
for all studied ages at exposure. Table 3 depicts that the reduced risk was most pro-
nounced in girls, in children with older siblings, and in children born to parents aged ≥25
years at time of birth of the child. Tests for interaction showed that the reduced risk was
not significantly different in different groups, however.
Table 3. RR (95% CI) of childhood ALL associated with childcare attendance, according to
characteristics of the child and its family.
Ever attendance, RR
(95% CI) Never attendance, RR
(95%CI) Effect of childcare atten-
dance (95% CI)* pinter
☼
Sex - Boy 0.80 (0.53;1.23) † 1 (ref.) -22% (-51%;23%) - Girl 0.65 (0.41;1.02) † 1.20 (0.74;1.96) † -53% (-71%;-25%)
0.13
Older siblings - 0 0.79 (0.48;1.29) 1 (ref.) -21% (-52%;29%) - ≥1 0.51 (0.31;0.85) 1.06 (0.62;1.81) -51% (-68%;-25%)
0.14
Birth weight - <2500 grams 1.07 (0.52;2.20) 1.03 (0.29;3.70) 3% (-74%;318%) - 2500-3999 grams 0.60 (0.41;0.90) 1 (ref.) -40% (-59%;-10%) - ≥4000 grams 0.57 (0.33;0.96) 0.86 (0.42;1.76) -35% (-69%;40%)
0.76
Population density - <500 per km2 0.51 (0.29;0.90) 1 (ref.) -49% (-71%;-10%) - 501-2000 per km2 0.88 (0.52;1.51) 0.98 (0.50;1.93) -10% (-49%;58%) - >2000 per km2 0.78 (0.44;1.38) 1.59 (0.84;3.00) -51% (-72%;-15%)
0.24
Maternal age - <25 years 0.62 (0.35;1.09) 0.51 (0.23;1.13) 21% (-45%;167%) - 25-29 years 0.52 (0.32;0.86) 1 (ref.) -48% (-68%;-14%) - ≥30 years 0.42 (0.25;0.68) 0.78 (0.44;1.38) -47% (-68%;-13%)
0.16
Paternal age - <25 years 0.94 (0.46;1.95) 0.29 (0.07;1.31) 222% (-29%;1370%) - 25-29 years 0.56 (0.32;1.00) 1 (ref.) -44% (-68%;0%) - ≥30 years 0.57 (0.33;0.97) 1.04 (0.58;1.86) -46% (-64%;-18%)
0.08
Country of birth - Denmark 0.61 (0.44;0.85) 1 (ref.) -39% (-56%;-15%) - Other n.e. ‡ 0.49 (0.06;3.81) n.e. ‡
n.e. ‡ †Estimated using unconditional analysis ‡n.e.=not estimable *The effect of childcare attendance was estimated in the regression model as the ratio between RRever attendance and RRnever attendance and for convenience subtracted by one to obtain percentages ☼pinter represents test for interaction
Study V supports the ‘delayed infection hypothesis’ (see section 7.3) and indicates that the
studied child and family characteristics play a minor role in the association between child-
care attendance early in life and childhood ALL.
- Results
Disease in childhood and the impact of childcare
29
7. Discussion
7.1. The temporal trend in infection hospitalizations
Studies have reported an increase in the rate of pediatric hospitalizations in European
countries over the last decades (88-95). The studies do not agree on whether the ob-
served increase is due to an increase in childhood morbidity (95) or due to changes in
hospitalization practices and utilization (89;90;93). An increase in morbidity could be due
to the proportion of children attending childcare away from their home having increased
considerably in the study period. However, in study I we found the increase in pediatric
infection hospitalizations to be specific to 0-1-year-old children hospitalized for 1-2 days.
Such an age and duration-dependent pattern is more likely to be due to the major
changes in hospitalization practices and utilization that have occurred in Denmark during
the study period (89;96) than due to an increase in childhood morbidity.
In study I we only studied first-time infection hospitalizations, equivalent to 65% of
pediatric infection hospitalizations, whereas we studied all infection hospitalizations in
studies III and IV. This had only a minor effect, however. The overall incidence rate of ARI
hospitalizations in 0-5-year-olds in study I was 37.6 per 1,000 risk-years and the corre-
sponding ARI incidence rate was 34.9 per 1,000 risk-years in study III. This indicates that
the trends in study I apply not only to first-time infection hospitalizations, but to all infec-
tion hospitalizations.
- Discussion
Disease in childhood and the impact of childcare
30
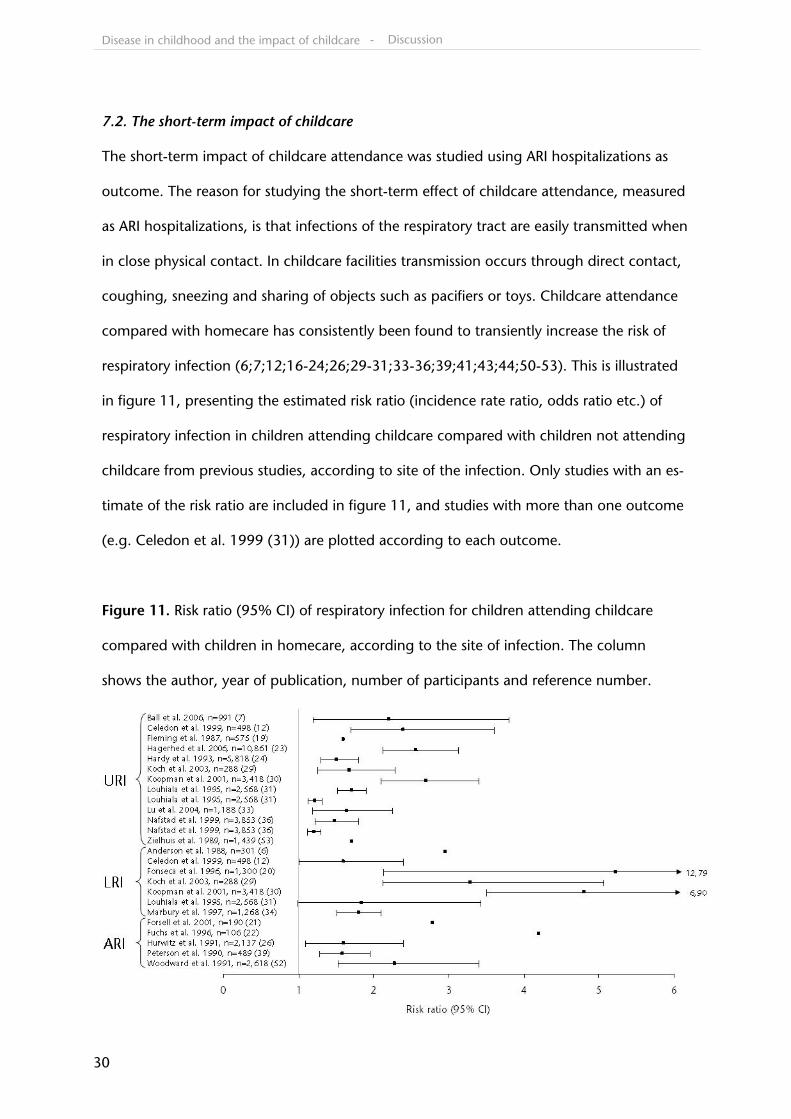
7.2. The short-term impact of childcare
The short-term impact of childcare attendance was studied using ARI hospitalizations as
outcome. The reason for studying the short-term effect of childcare attendance, measured
as ARI hospitalizations, is that infections of the respiratory tract are easily transmitted when
in close physical contact. In childcare facilities transmission occurs through direct contact,
coughing, sneezing and sharing of objects such as pacifiers or toys. Childcare attendance
compared with homecare has consistently been found to transiently increase the risk of
respiratory infection (6;7;12;16-24;26;29-31;33-36;39;41;43;44;50-53). This is illustrated
in figure 11, presenting the estimated risk ratio (incidence rate ratio, odds ratio etc.) of
respiratory infection in children attending childcare compared with children not attending
childcare from previous studies, according to site of the infection. Only studies with an es-
timate of the risk ratio are included in figure 11, and studies with more than one outcome
(e.g. Celedon et al. 1999 (31)) are plotted according to each outcome.
Figure 11. Risk ratio (95% CI) of respiratory infection for children attending childcare
compared with children in homecare, according to the site of infection. The column
shows the author, year of publication, number of participants and reference number.
- Discussion
Disease in childhood and the impact of childcare
31
Only few previous studies have aimed and had a sufficient sample size to study the effect
of childcare attendance in different groups of children, for instance according to the age
of the child or according to the number of siblings. Therefore, knowledge about the influ-
ence of child and family characteristics on the association between childcare attendance
and respiratory infections is scarce.
As illustrated in figure 4, a high incidence of ARI hospitalization is closely related to
young age. Not only is the risk of ARI hospitalization highest in young age, in study III we
showed that young age was a period where childcare attendance imposed an excess risk
of ARI hospitalization. In children <1 year of age, the first 6 months of enrollment in child-
care was associated with an increased risk of ARI hospitalization of 69%. This excess risk
has substantial public health impact when considering that the overall incidence of 69 ARI
hospitalizations per 1,000 risk-years in <1-year-olds is already high. In study IV, we found
that clustering of ARI hospitalizations was a minor problem in a public health sense; only
1% of ARI hospitalizations occurred in childcare facilities in which another child had been
hospitalized within the last month. Clusters involved 0-2-year-olds relatively more often
than older children. The observed clusters can be interpreted in different ways. A cluster of
ARI can be interpreted as indication of transmission of ARI within the childcare facilities.
The rapidly decreasing risk of hospitalization for ARI associated with increasing time since
latest ARI hospitalization supports such an interpretation. However, it is important to bear
in mind that transmission may very well have occurred outside of the childcare facility.
Thus, only in some instances, is the latest hospitalized child in the childcare facility likely to
be the one transmitting the ARI to the subsequently hospitalized child. Another interpreta-
tion is that clusters of ARI reflect increased awareness of ARI among parents of children in
facilities in which a child was recently hospitalized for ARI. It is not unthinkable that defen-
sive hospitalizations are practiced more often if doctors are consulted by worried parents.
Nevertheless, the fact that characteristics of the first hospitalized child affect the risk of the
- Discussion
Disease in childhood and the impact of childcare
32
other children in the facility supports that also transmission within the childcare facility
plays an important role in the occurrence of the observed clusters.
Although boys are generally at a higher risk of ARI hospitalization than girls, a similar
excess risk of ARI hospitalization when attending childcare was found in boys and girls in
studies III and IV. This is in contrast with a previous finding (34), in which childcare atten-
dance was found to have a more negative impact on girls than boys. Transmission of mea-
sles and polio from the opposite sex has been shown to increase the severity of the infec-
tion (97;98). However, in our study of ARIs severe enough to result in hospitalization we
observed no special increased short-term excess if the latest hospitalized child was of the
opposite sex. We did, however, find an especially increased risk of ARI hospitalization the
first month following an ARI hospitalization if the latest hospitalized child in the facility
was a boy. This is likely to reflect that boys show more active play than girls (99).
We studied several other variables associated with exposure to infection, namely
time since enrollment in childcare, type of childcare, siblings, population density, type of
parenthood and season. Generally, the results of the analyses of interaction between these
variables and childcare attendance suggest that the risk of ARI hospitalization when at-
tending childcare is dependent on previous exposure to infection. The children most af-
fected by childcare attendance were those who were recently enrolled in childcare, those
not living together with other children and children of mothers who were single at birth
of the child. It is generally believed that large childcare facilities confer a greater risk of in-
fection than daycare homes. However, we found no clear indication that one type of
childcare facility generally imposed a higher risk of ARI hospitalization than another. We
did not find clear patterns between the risk of ARI hospitalization when attending child-
care and population density and season, respectively. Thus, childcare seems to be un-
equivocally associated with increased risk of ARI hospitalization, irrespective of the type of
childcare, the underlying population density, and the season. Studies III and IV helped
- Discussion
Disease in childhood and the impact of childcare
33
identify groups of children that are more vulnerable when attending childcare than other
groups. Initiatives towards lowering the short-term detrimental effect of childcare should
therefore be targeted towards the youngest children and children who prior to childcare
enrollment have been sparsely exposed to infections.
7.3. The long-term impact of childcare
The long-term effect of childcare attendance was evaluated using ALL as outcome. The
idea that childcare attendance may influence the risk of childhood ALL is based on the hy-
pothesis that two hits are needed in order to induce childhood ALL (100;101). The first hit
is thought to be due to mutations occurring prenatally, whereas the second hit may be
induced by delayed or diminished exposure to childhood infections. This so-called ‘de-
layed infection hypothesis’ by Greaves (100) was put forward specifically for childhood B-
cell precursor ALL. Since no specific infection has been associated with a reduced risk of
childhood ALL, attendance to childcare has previously been used as a proxy measure of a
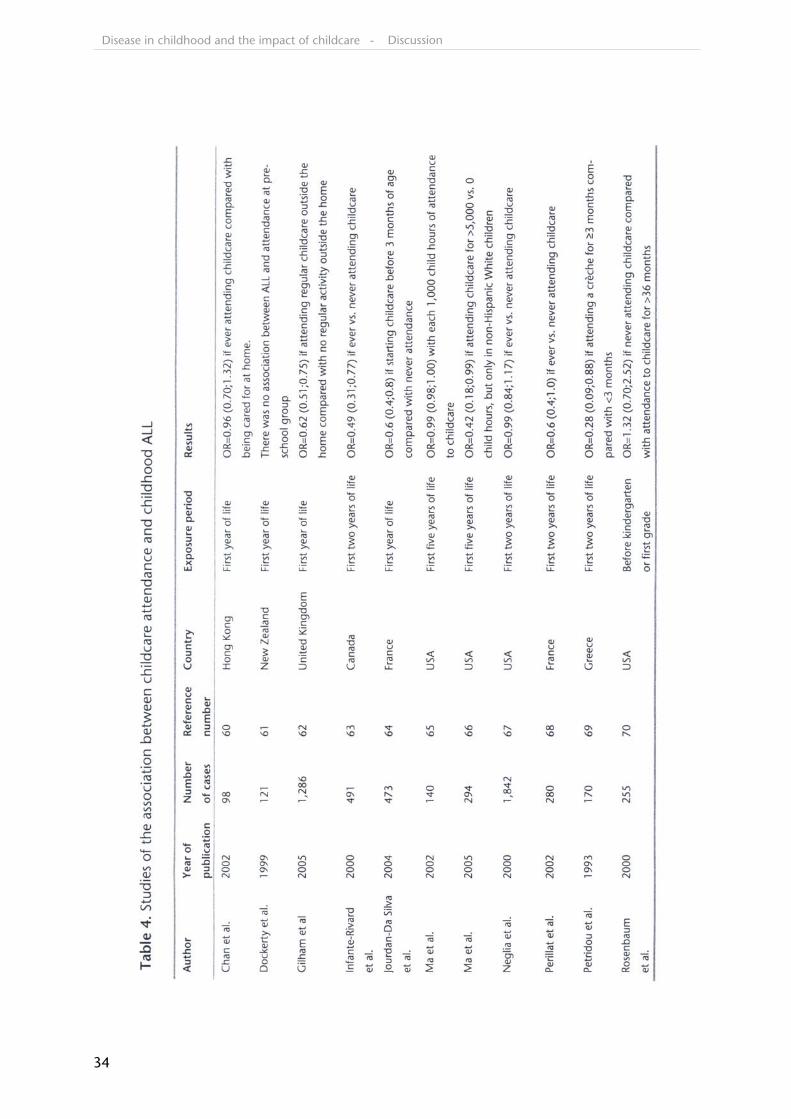
high infection load (60-70). Like in most (62-66;68;69), but not all (60;61;67;70) previous
studies, we found a significantly decreased risk of childhood ALL if attending childcare
early in life in study V. Previous studies of the association between childcare attendance
and childhood ALL are presented in table 4. Also in accordance with previous findings
(62;66;68), we demonstrated that the reduced risk was not specific to B-cell precursor
ALL, but applied to all studied subtypes of childhood ALL. We found that the reduced risk
was not specific to exposure at a certain age in early childhood. This has only been stud-
ied indirectly in one other study (69), but table 4 supports this finding because previous
studies with different exposure periods have found a reduced risk.
- Discussion
Disease in childhood and the impact of childcare
34
- Discussion
Disease in childhood and the impact of childcare
35
Interactions between the effect of childcare and child characteristics on the risk of child-
hood ALL have only been studied in one previous study (66). This study found that the
reduced risk of childhood ALL was specific to non-Hispanic White children. We found a
more pronounced reduced risk of childhood ALL in girls than in boys, which may reflect
the biology of ALL, since boys and girls differ both in their distribution of subsets of ALL
(77) and in the course of their disease (102). The reduced risk was not significantly differ-
ent for boys and girls, however. Also, the reduced risk when attending childcare was more
pronounced for children with older siblings and for children of parents aged 25 or more at
time of child birth than for other children, however not statistically significant. The under-
lying mechanism may be the same in the two groups. It remains to be explored, whether
high parental age reflects biological factors related to the type of ALL such as accumula-
tion of chromosomal aberrations and mutations (103;104), or behavioral characteristics,
such as frequency of social contacts.
7.4. Confounding, bias and interaction
Consensus exists that confounding is a distortion in the estimated effect of exposure, that
results from differences in risk between the exposed and the unexposed, and that is not
due to exposure (105). There is, however, not consensus about how to identify confound-
ing factors and when to adjust for them. In all studies in the present thesis, we chose to
identify confounders using the change-in-estimates method suggested by Rothman and
Greenland (105). Covariates changing the estimated effect of exposure by 5% or more
were included as confounders and adjusted for. In studies I and V, no confounders were
identified using this approach. Some readers of epidemiological literature tend not to be-
lieve in studies without confounder adjustment. However, inaccurate adjustment for con-
founders can create spurious associations in the data (106).
- Discussion
Disease in childhood and the impact of childcare
36
As opposed to the majority of previous epidemiological research within the area of disease
in childhood and the impact of childcare, the studies included in the present thesis were
based on data obtained from registers. Therefore information on some possible confound-
ing factors that are not routinely registered in Denmark, was not available. An example of
such a possible confounding factor is breastfeeding. Studies have shown that children
who are exclusively breastfed are at lower risk of hospitalization for respiratory infection
(107) and are less often enrolled in childcare (108) compared with children who are par-
tially breastfed or not breastfed. Therefore some of the excess risk of ARI hospitalization as-
sociated with childcare attendance compared with homecare demonstrated in study III
may be due to an uneven distribution of breastfeeding among children in childcare and in
homecare. Based on figures from the above studies, we estimated that the excess risk of
ARI hospitalization associated with childcare attendance demonstrated in study III was
overestimated by 5%-10% due to confounding from breastfeeding. In study V, the direct
opposite may be the case; that the reduced risk of childhood ALL when attending child-
care may be underestimated because of an uneven distribution of breastfeeding.
Another possible source of distortion is confounding by indication. Parents of frail
children may choose not to enroll or to withdraw their child from childcare. Thereby,
these children may have contributed to an artificially high risk of ARI hospitalization in
children in homecare and thereby underestimated the excess risk in study III. Therefore we
performed additional analyses to evaluate whether frail children being moved from child-
care back to homecare could have biased our results, but we found no such indication.
Likewise in study V, children with childhood ALL may have had a pre-diagnostic phase
with recurrent infections, bone pains and/or fatigue that caused the parents to refrain
from enrolling their child in childcare. However, since a lower risk if ever attending child-
care was seen in children diagnosed at age 5 years or later compared with those diag-
nosed before 5 years of age, we find this explanation very unlikely.
- Discussion
Disease in childhood and the impact of childcare
37
There are major advantages of using a nationwide register-based sample. First, the sample
size ensures precise estimation and allows for interaction analyses with reasonable statisti-
cal power. The sample size of studies I and III is the largest to date in the area. Second, the
risk of selection bias was minimized since children from all families were included, irre-
spective of socioeconomic background and place of residence. Children from five munici-
palities that could not deliver childcare data electronically, were not included in the stud-
ies. These municipalities include small, medium and large municipalities from all geo-
graphical parts of Denmark. Therefore we have no reason to believe that this should have
affected our results. Third, information on exposure and covariates was drawn from inde-
pendent registers and registered prior to the outcome. This minimized the risk of informa-
tion bias, particularly differential misclassification. Non-differential misclassification in the
data cannot be ruled out since children attending unregistered childcare facilities may
have been misclassified as in homecare, leading to bias towards the null hypothesis. We
believe the problem with private and unregistered childcare facilities is small since most
Danish municipalities guarantee a place in a public childcare facility before 6 months of
age.
The outcome of studies III and IV was ARI hospitalizations rather than self-reported
or childcare teacher-reported ARI morbidity like in most previous studies. We found results
comparable with those of previous studies regarding well known risk factors for ARI such
as young age, male sex and childcare attendance compared with homecare. This suggests
that the new results presented in studies III and IV are applicable not only to ARI hospitali-
zations, but to some degree to non-hospital-demanding ARI morbidity as well.
- Discussion
Disease in childhood and the impact of childcare
38
Interaction, also known as effect modification or synergism/antagonism, has been the sub-
ject of much debate, primarily because the term is commonly used to describe both bio-
logical and statistical phenomena. According to Ahlbom and Alfredson (109), biological
interaction refers to situations in which two risk factors are involved in the same sufficient
cause of disease, or pathway towards disease. For instance, human papiloma virus seems
to be a necessary, but not sufficient cause, in the development of cervical cancer. Biologi-
cal interaction is measured as risk differences on an additive scale (110). Statistical interac-
tion, on the other hand, refers to situations where the relation between the exposure and
outcome variables is not additive, and inclusion of an interaction term in the statistical
model is necessary for the model to fit the data. Statistical interaction is a relative measure
e.g. rate ratio, odds ratio etc. on a multiplicative scale. All models used in the present the-
sis are generalized linear models with either a log (Poisson regression) or logit (logistic re-
gression) link function. Since interaction is scale-dependent, the term interaction in the
present thesis refers to statistical interaction. It would have been possible to estimate a
measure of biological interaction in studies III and IV if additive linear rate models had
been applied. In case control studies, like study V, a measure of biological interaction is
not estimable, however (111).
- Discussion
Disease in childhood and the impact of childcare
39
7.5. Analytical challenges
The outcome in studies I, III and IV was infectious disease which is challenging to model
statistically. Unique to the field of infectious disease epidemiology are the concepts of
transmission and immunity, which impose dependency between individuals since one in-
dividual may be a determinant for disease in other individuals, and some individuals will
not be at risk of contracting the disease (112). One assumption of standard statistical
models, such as Poisson regression and logistic regression models, is that events occur in-
dependently of each other (85). As exemplified in study IV, hospitalizations for ARI among
children in childcare facilities tend to accumulate in time and space, why the assumption
of independency is challenged. In order to account for the possible dependency between
events in studies I, III and IV, we attempted to fit multi-level Poisson regression models in-
cluding a random effect of the childcare facilities. Due to the large number of childcare fa-
cilities in the cohort (n=15,703), such models were not feasible, however. Instead estima-
tion in study III and IV was carried out using quasi Poisson regression models with a dis-
persion factor (113) estimated from Pearson statistics to take into account the possible
over dispersion induced by dependency of events within the same person, families or
childcare facilities.
Another analytical challenge has been that some of the variables of interest were ex-
actly linear dependent, ruling out the possibility of simultaneous estimation when using
standard methods (114). For instance, estimation of the effect of time since enrollment in
childcare (t) was not possible while taking into account the age of the child (a) and the
enrollment age (e), since t=a-e. This estimability problem was handled by postulating a
common age effect in all children, irrespective of whether the child attended childcare or
not. This method was suggested by Heuch et al. in a study of temporal effects of child-
birth on cancer risk (115). A common age effect in all children was assumed in early stage
analyses, but not in any of the final manuscripts.
- Discussion
Disease in childhood and the impact of childcare
40
8. Conclusions and perspectives
8.1. Conclusions
The research presented in the present thesis is summarized in the following study-specific
conclusions:
Study I: The incidence of hospitalizations due to infection among 0-5-year-old chil-
dren increased markedly in the period 1980-2001 in Denmark. The increase was al-
most exclusively driven by short-term hospitalizations in 0-1-year-old children
Study II: Currently, the Childcare Database offers a unique potential for epidemiologi-
cal research. Future updates and linkages with other data sources will further expand
this potential
Study III: Childcare attendance is associated with an excess risk of ARI hospitalization,
but only in 0-2-year-olds, during the first period of enrollment and in children not liv-
ing with other children
Study IV: ARI hospitalizations cluster among children in childcare facilities. Clusters in-
volve 0-2-year-olds and boys as first hospitalized child relatively more often than other
children
Study V: Childcare attendance during the first two years of life entails a reduced risk of
childhood ALL. Child and family characteristics seem to play a minor role in this asso-
ciation
- Conclusions and perspectives
Disease in childhood and the impact of childcare
41
Conclusively, in the present thesis we have confirmed an increased infection hospitaliza-
tion incidence over time, documented the establishment of the Childcare Database, and
confirmed that childcare attendance is associated with an increased risk of ARI hospitaliza-
tion and a decreased risk of childhood ALL. The thesis contributes with new knowledge by
identifying subgroups of children involved in the increased infection hospitalization inci-
dence over time, and by demonstrating that the association between childcare attendance
and ARI hospitalization varies with characteristics of the child and the child’s family,
whereas these characteristics seem to play a minor role in the association between child-
care attendance and childhood ALL.
8.2. Perspectives
The studies included in the present thesis were conducted in order to understand the as-
sociation between childcare and disease in childhood in more detail, rather than to put
forward recommendations for the use of childcare in Denmark. Such recommendations
must not be based on risk of disease alone, but should also be based on the impact on the
child’s social life and learning. Today only few parents are in a position to choose not to
enroll their child in childcare. Hence, childcare attendance is a part of childhood for most
children in Denmark. Continued research to ensure optimal childcare is therefore encour-
aged. The Childcare Database opens possibility for further research of the short-term im-
pact of childcare and has already been used to study invasive pneumococcal disease in
Denmark (116). Also the sparsely studied area of the long-term impact of childcare atten-
dance on immune disorders, such as insulin dependent diabetes mellitus, asthma, allergy
and Crohn’s disease deserves further scientific attention.
- Conclusions and perspectives
Disease in childhood and the impact of childcare
42
9. English summary
The present PhD thesis is based on five epidemiological studies of Danish register data re-
garding infection-related hospitalizations, childhood acute lymphoblastic leukemia (ALL)
and attendance to childcare facilities in children aged 0-5 years in the period 1989-2004.
The overall aim of the thesis was to study the impact of childcare attendance on disease in
childhood on a short and a long-term basis, respectively. Short-term impact of childcare
attendance was studied using hospitalizations for acute respiratory infections (ARI) as out-
come, whereas ALL was studied to evaluate the long-term impact of childcare.
Initially, temporal trends in the incidence of hospitalizations for childhood infections
in the period 1980-2001 in Denmark were characterized. We found an increase in the in-
cidence of hospitalizations for infections, almost exclusively driven by short-term hospitali-
zations in 0-1-year-old children. Secondly, we described the creation of, the information
available in, and the potential of the Childcare Database, containing more than 1 million
children and created for the purpose of the present thesis. Thirdly, we assessed the short-
term impact of childcare attendance on ARI. We found that childcare attendance was as-
sociated with an excess risk of ARI hospitalization, but only in 0-2-year-olds, during the
first period of enrollment and in children not living with other children. Fourthly, we stud-
ied factors related to clustering of ARI in childcare facilities. We found that ARI hospitaliza-
tions cluster among children in childcare facilities. Clusters involved 0-2-year-olds and
boys as first hospitalized child relatively more often than other children. Finally, we studied
whether attendance to childcare early in life was associated with childhood ALL. We found
childcare attendance during the first two years of life to entail a reduced risk of childhood
ALL and the studied child and family characteristics seemed to play a minor role in the as-
sociation between childcare attendance and childhood ALL.
- English summary
Disease in childhood and the impact of childcare
43
We have confirmed an increased infection hospitalization incidence over time, docu-
mented the establishment of the Childcare Database, and confirmed that childcare atten-
dance is associated with an increased risk of ARI hospitalization and a decreased risk of
childhood ALL. The thesis contributes with new knowledge by identifying subgroups of
children involved in the increased infection hospitalization incidence over time, and by
demonstrating that the association between childcare attendance and ARI hospitalization
varies with characteristics of the child and the child’s family, whereas these characteristics
seem to play a minor role in the association between childcare attendance and childhood
ALL.
- English summary
Disease in childhood and the impact of childcare
44
10. Dansk resumé
Nærværende ph.d.-afhandling er baseret på fem epidemiologiske studier af danske regi-
sterdata vedrørende infektionshospitaliseringer, akut lymfoblastisk børneleukæmi (ALL) og
pasning af 0-5-årige børn i perioden 1989-2004. Det overordnede formål med afhandlin-
gen var at studere betydningen af børnepasning for børnenes sygelighed på henholdsvis
kort og lang sigt. Udfaldet i studierne af betydningen på kort sigt var hospitalisering for
akut luftvejsinfektion (ARI), mens betydningen på lang sigt blev vurderet for ALL.
Indledningsvis karakteriserede vi udviklingen i infektionshospitaliseringer blandt børn
i perioden 1980-2001 i Danmark. Vi fandt en stigning i incidensen af infektionshospitalise-
ringer, næsten udelukkende drevet af korttidsindlæggelser blandt 0-1-årige børn. Dernæst
beskrev vi dannelsen af, og de tilgængelige informationer i, ’The Childcare Database’, som
omfatter mere end 1 million børn. Databasen blev dannet til brug i artiklerne i nærværen-
de ph.d.-afhandling. Herefter vurderede vi korttidseffekten af børnepasning på risikoen for
ARI-hospitalisering. Vi fandt at børnepasning medførte en øget risiko for ARI-
hospitalisering, men kun blandt 0-2-årige børn, i løbet af de første seks måneder efter
indmeldelse i en børnepasningsordning og blandt børn som ikke boede sammen med an-
dre børn. Herefter studerede vi faktorer relateret til clustering af ARI-hospitaliseringer i
børnepasningsordninger. Clusters involverede 0-2-årige og drenge som først hospitalise-
rede barn relativt oftere end andre børn. Endelig studerede vi, om børnepasning tidligt i
livet var associeret med risiko for ALL. Vi fandt, at børnepasning i de første to leveår ned-
satte risikoen for ALL. De studerede karakteristika ved barnet og barnets familie havde ikke
betydelig indflydelse på associationen mellem børnepasning tidligt i livet og ALL.
- Dansk resumé
Disease in childhood and the impact of childcare
45
Vi har bekræftet en stigende incidens af infektionshospitaliseringer over tid, beskrevet dan-
nelsen af ’The Childcare Database’ samt bekræftet, at børnepasning er associeret med en
øget risiko for ARI hospitalisering og en nedsat risiko for ALL. Afhandlingen bidrager med
ny viden ved at identificere undergrupper af børn, som er involveret i den stigende inci-
dens af infektionshospitaliseringer over tid, og ved at demonstrere, at associationen mel-
lem børnepasning og ARI hospitalisering afhænger af karakteristika ved barnet og barnets
familie, hvorimod disse karakteristika ikke synes at have betydelig indflydelse på associati-
onen mellem børnepasning og ALL.
- Dansk resumé
Disease in childhood and the impact of childcare
46
11. References
(1) Lichtenstein A. Nosocomial Infections in Children's Hospitals and Institutions. Our Means for combating these Infections. Acta Paediatr 1935;Suppl. 17:36.
(2) Gyllenswärd C. Anti-Catarrhal Vaccination in Homes for Children under School-Age. Acta Paediatr 1935;suppl. 1 17:78.
(3) Kamerman SB. Early childhood education and care: an overview of developments in the OECD countries. New York: Elsevier Science Ltd; 2000. Report No.: 33.
(4) Statistics Denmark. Statistical yearbook. Copenhagen 2006.
(5) Alexander CS, Zinzeleta EM, Mackenzie EJ, Vernon A, Markowitz RK. Acute gastro-intestinal illness and child care arrangements. Am J Epidemiol 1990 Jan;131(1):124-31.
(6) Anderson LJ, Parker RA, Strikas RA, Farrar JA, Gangarosa EJ, Keyserling HL et al. Day-care center attendance and hospitalization for lower respiratory tract illness. Pedi-atrics 1988 Sep;82(3):300-8.
(7) Ball TM, Holberg CJ, Aldous MB, Martinez FD, Wright AL. Influence of attendance at day care on the common cold from birth through 13 years of age. Arch Pediatr Adolesc Med 2002 Feb;156(2):121-6.
(8) Bartlett AV, Moore M, Gary GW, Starko KM, Erben JJ, Meredith BA. Diarrheal illness among infants and toddlers in day care centers. II. Comparison with day care homes and households. J Pediatr 1985 Oct;107(4):503-9.
(9) Bell DM, Gleiber DW, Mercer AA, Phifer R, Guinter RH, Cohen AJ et al. Illness asso-ciated with child day care: a study of incidence and cost. Am J Public Health 1989 Apr;79(4):479-84.
(10) Berg AT, Shapiro ED, Capobianco LA. Group day care and the risk of serious infec-tious illnesses. Am J Epidemiol 1991 Jan 15;133(2):154-63.
(11) Brady MT. Infectious disease in pediatric out-of-home child care. Am J Infect Con-trol 2005 Jun;33(5):276-85.
(12) Celedon JC, Litonjua AA, Weiss ST, Gold DR. Day care attendance in the first year of life and illnesses of the upper and lower respiratory tract in children with a famil-ial history of atopy. Pediatrics 1999 Sep;104(3 Pt 1):495-500.
(13) Collet JP, Burtin P, Gillet J, Bossard N, Ducruet T, Durr F. Risk of infectious diseases in children attending different types of day-care setting. Epicreche Research Group. Respiration 1994;61 Suppl 1:16-9.
(14) Cordell RL, MacDonald JK, Solomon SL, Jackson LA, Boase J. Illnesses and absence due to illness among children attending child care facilities in Seattle-King County, Washington. Pediatrics 1997 Nov;100(5):850-5.
(15) Dahl IL, Grufman M, Hellberg C, Krabbe M. Absenteeism because of illness at day-care centers and in three-family systems. Acta Paediatr Scand 1991 Apr;80(4):436-45.
(16) Dales RE, Cakmak S, Brand K, Judek S. Respiratory illness in children attending day-care. Pediatr Pulmonol 2004 Jul;38(1):64-9.
- References
Disease in childhood and the impact of childcare
47
(17) Denny FW, Collier AM, Henderson FW. Acute respiratory infections in day care. Rev Infect Dis 1986 Jul;8(4):527-32.
(18) Douglas RM, Woodward A, Miles H, Buetow S, Morris D. A prospective study of proneness to acute respiratory illness in the first two years of life. Int J Epidemiol 1994 Aug;23(4):818-26.
(19) Fleming DW, Cochi SL, Hightower AW, Broome CV. Childhood upper respiratory tract infections: to what degree is incidence affected by day-care attendance? Pe-diatrics 1987 Jan;79(1):55-60.
(20) Fonseca W, Kirkwood BR, Barros AJ, Misago C, Correia LL, Flores JA et al. Atten-dance at day care centers increases the risk of childhood pneumonia among the urban poor in Fortaleza, Brazil. Cad Saude Publica 1996 Apr;12(2):133-40.
(21) Forssell G, Hakansson A, Mansson NO. Risk factors for respiratory tract infections in children aged 2-5 years. Scand J Prim Health Care 2001 Jun;19(2):122-5.
(22) Fuchs SC, Maynart R, Costa LF, Cardozo A, Schierholt R. Duration of day-care at-tendance and acute respiratory infection. Cad Saude Publica 1996 Jul;12(3):291-6.
(23) Hagerhed-Engman L, Bornehag CG, Sundell J, Aberg N. Day-care attendance and increased risk for respiratory and allergic symptoms in preschool age. Allergy 2006 Apr;61(4):447-53.
(24) Hardy AM, Fowler MG. Child care arrangements and repeated ear infections in young children. Am J Public Health 1993 Sep;83(9):1321-5.
(25) Haskins R, Kotch J. Day care and illness: evidence, cost, and public policy. Pediat-rics 1986 Jun;77(6 Pt 2):951-82.
(26) Hurwitz ES, Gunn WJ, Pinsky PF, Schonberger LB. Risk of respiratory illness associ-ated with day-care attendance: a nationwide study. Pediatrics 1991 Jan;87(1):62-9.
(27) Istre GR, Conner JS, Broome CV, Hightower A, Hopkins RS. Risk factors for primary invasive Haemophilus influenzae disease: increased risk from day care attendance and school-aged household members. J Pediatr 1985 Feb;106(2):190-5.
(28) Johansen AS, Leibowitz A, Waite LJ. Child care and children's illness. Am J Public Health 1988 Sep;78(9):1175-7.
(29) Koch A, Molbak K, Homoe P, Sorensen P, Hjuler T, Olesen ME et al. Risk factors for acute respiratory tract infections in young Greenlandic children. Am J Epidemiol 2003 Aug 15;158(4):374-84.
(30) Koopman LP, Smit HA, Heijnen ML, Wijga A, van Strien RT, Kerkhof M et al. Respi-ratory infections in infants: interaction of parental allergy, child care, and siblings-- The PIAMA study. Pediatrics 2001 Oct;108(4):943-8.
(31) Louhiala PJ, Jaakkola N, Ruotsalainen R, Jaakkola JJ. Form of day care and respira-tory infections among Finnish children. Am J Public Health 1995 Aug;85(8 Pt 1):1109-12.
(32) Louhiala PJ, Jaakkola N, Ruotsalainen R, Jaakkola JJ. Day-care centers and diarrhea: a public health perspective. J Pediatr 1997 Sep;131(3):476-9.
- References
Disease in childhood and the impact of childcare
48
(33) Lu N, Samuels ME, Shi L, Baker SL, Glover SH, Sanders JM. Child day care risks of common infectious diseases revisited. Child Care Health Dev 2004 Jul;30(4):361-8.
(34) Marbury MC, Maldonado G, Waller L. Lower respiratory illness, recurrent wheez-ing, and day care attendance. Am J Respir Crit Care Med 1997 Jan;155(1):156-61.
(35) McCutcheon H, Woodward A. Acute respiratory illness in the first year of primary school related to previous attendance at child care. Aust N Z J Public Health 1996 Feb;20(1):49-53.
(36) Nafstad P, Hagen JA, Oie L, Magnus P, Jaakkola JJ. Day care centers and respiratory health. Pediatrics 1999 Apr;103(4 Pt 1):753-8.
(37) Nielsen AM, Koefoed BG, Møller R, Laursen B. [Occurrence of recent illness in Dan-ish children in 1994 and 2000]. Ugeskr Laeger 2006 Jan 23;168(4):373-8.
(38) Osterholm MT. Infectious disease in child day care: an overview. Pediatrics 1994 Dec;94(6 Pt 2):987-90.
(39) Petersson C, Hakansson A. A retrospective study of respiratory tract infections among children in different forms of day care. Scand J Prim Health Care 1990 Jul;8(2):119-22.
(40) Reves RR, Morrow AL, Bartlett AV, III, Caruso CJ, Plumb RL, Lu BT et al. Child day care increases the risk of clinic visits for acute diarrhea and diarrhea due to rotavi-rus. Am J Epidemiol 1993 Jan 1;137(1):97-107.
(41) Schwartz B, Giebink GS, Henderson FW, Reichler MR, Jereb J, Collet JP. Respiratory infections in day care. Pediatrics 1994 Dec;94(6 Pt 2):1018-20.
(42) Shi L, Huang Y, Kelly K, Zhao M, Solomon SL. Gastrointestinal symptoms and use of medical care associated with child day care and health care plan among pre-school children. Pediatr Infect Dis J 1999 Jul;18(7):596-603.
(43) Stahlberg M.R. The influence of form of day care on occurrence of acute respira-tory tract infections among young children. Thesis, University of Turku 1980.
(44) Strangert K. Respiratory illness in preschool children with different forms of day care. Pediatrics 1976 Feb;57(2):191-6.
(45) Takala AK, Jero J, Kela E, Ronnberg PR, Koskenniemi E, Eskola J. Risk factors for pri-mary invasive pneumococcal disease among children in Finland. JAMA 1995 Mar 15;273(11):859-64.
(46) Thacker SB, Addiss DG, Goodman RA, Holloway BR, Spencer HC. Infectious dis-eases and injuries in child day care. Opportunities for healthier children. JAMA 1992 Oct 7;268(13):1720-6.
(47) Thrane N, Olesen C, Md JT, Sondergaard C, Schonheyder HC, Sorensen HT. Influ-ence of day care attendance on the use of systemic antibiotics in 0- to 2-year-old children. Pediatrics 2001 May;107(5):E76.
(48) Uldall P. [Common morbidity in infants and young children - occurrence and social consequences]. Thesis, University of Copenhagen 1986.
(49) Wald ER, Dashefsky B, Byers C, Guerra N, Taylor F. Frequency and severity of infec-tions in day care. J Pediatr 1988 Apr;112(4):540-6.
- References
Disease in childhood and the impact of childcare
49
(50) Wald ER, Guerra N, Byers C. Upper respiratory tract infections in young children: duration of and frequency of complications. Pediatrics 1991 Feb;87(2):129-33.
(51) Wald ER, Guerra N, Byers C. Frequency and severity of infections in day care: three-year follow-up. J Pediatr 1991 Apr;118(4 ( Pt 1)):509-14.
(52) Woodward A, Douglas RM, Graham NM, Miles H. Acute respiratory illness in Ade-laide children--the influence of child care. Med J Aust 1991 Jun 17;154(12):805-8.
(53) Zielhuis GA, Heuvelmans-Heinen EW, Rach GH, van den BP. Environmental risk fac-tors for otitis media with effusion in preschool children. Scand J Prim Health Care 1989 Mar;7(1):33-8.
(54) Hedin K, Petersson C, Cars H, Beckman A, Hakansson A. Infection prevention at day-care centres: Feasibility and possible effects of intervention. Scand J Prim Health Care 2006 Mar;24(1):44-9.
(55) Huskins WC. Transmission and control of infections in out-of-home child care. Pe-diatr Infect Dis J 2000 Oct;19(10 Suppl):S106-S110.
(56) Osterholm MT, Reves RR, Murph JR, Pickering LK. Infectious diseases and child day care. Pediatr Infect Dis J 1992 Aug;11(8 Suppl):S31-S41.
(57) Ponka A, Poussa T, Laosmaa M. The effect of enhanced hygiene practices on ab-sences due to infectious diseases among children in day care centers in Helsinki. In-fection 2004 Feb;32(1):2-7.
(58) Roberts L, Smith W, Jorm L, Patel M, Douglas RM, McGilchrist C. Effect of infection control measures on the frequency of upper respiratory infection in child care: a randomized, controlled trial. Pediatrics 2000 Apr;105(4 Pt 1):738-42.
(59) Hesselvik L. Ill-health among school children who had previously attended day nurseries. Acta Paediatr 1953 Nov;42(6):491-8.
(60) Chan LC, Lam TH, Li CK, Lau YL, Li CK, Yuen HL et al. Is the timing of exposure to infection a major determinant of acute lymphoblastic leukaemia in Hong Kong? Paediatr Perinat Epidemiol 2002 Apr;16(2):154-65.
(61) Dockerty JD, Skegg DC, Elwood JM, Herbison GP, Becroft DM, Lewis ME. Infec-tions, vaccinations, and the risk of childhood leukaemia. Br J Cancer 1999 Jul;80(9):1483-9.
(62) Gilham C, Peto J, Simpson J, Roman E, Eden TO, Greaves MF et al. Day care in in-fancy and risk of childhood acute lymphoblastic leukaemia: findings from UK case-control study. BMJ 2005 Apr 22.
(63) Infante-Rivard C, Fortier I, Olson E. Markers of infection, breast-feeding and child-hood acute lymphoblastic leukaemia. Br J Cancer 2000 Dec;83(11):1559-64.
(64) Jourdan-Da Silva N, Perel Y, Mechinaud F, Plouvier E, Gandemer V, Lutz P et al. In-fectious diseases in the first year of life, perinatal characteristics and childhood acute leukaemia. Br J Cancer 2004 Jan 12;90(1):139-45.
(65) Ma X, Buffler PA, Selvin S, Matthay KK, Wiencke JK, Wiemels JL et al. Daycare at-tendance and risk of childhood acute lymphoblastic leukaemia. Br J Cancer 2002 May 6;86(9):1419-24.
- References
Disease in childhood and the impact of childcare
50
(66) Ma X, Buffler PA, Wiemels JL, Selvin S, Metayer C, Loh M et al. Ethnic difference in daycare attendance, early infections, and risk of childhood acute lymphoblastic leukemia. Cancer Epidemiol Biomarkers Prev 2005 Aug;14(8):1928-34.
(67) Neglia JP, Linet MS, Shu XO, Severson RK, Potter JD, Mertens AC et al. Patterns of infection and day care utilization and risk of childhood acute lymphoblastic leu-kaemia. Br J Cancer 2000 Jan;82(1):234-40.
(68) Perrillat F, Clavel J, Auclerc MF, Baruchel A, Leverger G, Nelken B et al. Day-care, early common infections and childhood acute leukaemia: a multicentre French case-control study. Br J Cancer 2002 Apr 8;86(7):1064-9.
(69) Petridou E, Kassimos D, Kalmanti M, Kosmidis H, Haidas S, Flytzani V et al. Age of exposure to infections and risk of childhood leukaemia. BMJ 1993 Sep 25;307(6907):774.
(70) Rosenbaum PF, Buck GM, Brecher ML. Early child-care and preschool experiences and the risk of childhood acute lymphoblastic leukemia. Am J Epidemiol 2000 Dec 15;152(12):1136-44.
(71) Viral Infections of Humans - Epidemiology and Control. Fourth edition. New York: Plenum Medical Book Company; 1997.
(72) Bacterial Infections of Humans - Epidemiology and Control. Third edition. New York: Kluwer academic/plenum publishers; 1998.
(73) International classification of diseases. WHO Collaborating Centers. Epidemiol Bull 1998 Sep;19(3):7-11.
(74) Hjalgrim LL, Rostgaard K, Schmiegelow K, Soderhall S, Kolmannskog S, Vetten-ranta K et al. Age- and sex-specific incidence of childhood leukemia by immuno-phenotype in the Nordic countries. J Natl Cancer Inst 2003 Oct 15;95(20):1539-44.
(75) Stiller CA, Parkin DM. Geographic and ethnic variations in the incidence of child-hood cancer. Br Med Bull 1996 Oct;52(4):682-703.
(76) Hjalgrim LL. Aspects of the natural history of childhood leukaemia. Thesis, Univer-sity of Copenhagen 2003.
(77) Forestier E, Schmiegelow K. The incidence peaks of the childhood acute leukemias reflect specific cytogenetic aberrations. J Pediatr Hematol Oncol 2006 Aug;28(8):486-95.
(78) Malig C. The Civil Registration System in Denmark. Bethesda, MD: International Institute for Vital Registration and Statistics. IIVRS Technical paper 1996;66:1-6.
(79) Pedersen CB, Gotzsche H, Moller JO, Mortensen PB. The Danish Civil Registration System. A cohort of eight million persons. Dan Med Bull 2006 Nov;53(4):441-9.
(80) Andersen TF, Madsen M, Jorgensen J, Mellemkjoer L, Olsen JH. The Danish Na-tional Hospital Register. A valuable source of data for modern health sciences. Dan Med Bull 1999 Jun;46(3):263-8.
(81) Mosbech J, Jorgensen J, Madsen M, Rostgaard K, Thornberg K, Poulsen TD. [The Danish National Patient Registry. Evaluation of data quality]. Ugeskr Laeger 1995 Jun 26;157(26):3741-5.
- References
Disease in childhood and the impact of childcare
51
(82) Nickelsen TN. [Data validity and coverage in the Danish National Patient Registry. A literature review]. Ugeskr Laeger 2001 Dec 31;164(1):33-7.
(83) Statistics Denmark. [Social conditions, health and judicial system]. Technical Re-port. Copenhagen 1999.
(84) Knudsen LB, Olsen J. The Danish Medical Birth Registry. Dan Med Bull 1998 Jun;45(3):320-3.
(85) McCullach P, Nelder J. Generalized Linear Models. London: Chapman & Hall; 1989.
(86) SAS Institute Inc. SAS/STAT software release 8.2. Cary, NC: SAS Institute Inc. Com-puter program 2001.
(87) King G, Zeng L. Estimating risk and rate levels, ratios and differences in case-control studies. Stat Med 2002 May 30;21(10):1409-27.
(88) Durojaiye LI, Hutchison T, Madeley RJ. Improved primary care does not prevent the admission of children to hospital. Public Health 1989 May;103(3):181-8.
(89) Forfar JO. Trends in paediatric medical admissions. BMJ 1989 Jun 24;298(6689):1711.
(90) Hill AM. Trends in paediatric medical admissions. BMJ 1989 Jun 3;298(6686):1479-83.
(91) MacFaul R, Werneke U. Recent trends in hospital use by children in England. Arch Dis Child 2001 Sep;85(3):203-7.
(92) Nielsen A, Lie H, Keiding L, Madsen M. [Admissions in hospital]. [The health of children in Denmark].Copenhagen: Danish Institute of Clinical Epidemiology; 1998.
(93) Pearson G, Barry P, Timmins C, Stickley J, Hocking M. Changes in the profile of paediatric intensive care associated with centralisation. Intensive Care Med 2001 Oct;27(10):1670-3.
(94) Spencer NJ, Lewis MA. Multiple admissions under 2 years of age. Arch Dis Child 1991 Aug;66(8):938-40.
(95) Wickman M, Farahmand BY, Persson PG, Pershagen G. Hospitalization for lower respiratory disease during 20 yrs among under 5 yr old children in Stockholm County: a population based survey. Eur Respir J 1998 Feb;11(2):366-70.
(96) Kastrup KW, Andersen KV. [Emergency pediatric/monitoring department. The Danish Pediatric Society]. Ugeskr Laeger 2001 Mar 19;163(12):1693.
(97) Aaby P. Influence of cross-sex transmission on measles mortality in rural Senegal. Lancet 1992 Aug 15;340(8816):388-91.
(98) Nielsen NM, Wohlfahrt J, Melbye M, Molbak K, Aaby P. Does cross-sex transmis-sion increase the severity of polio infection? A study of multiple family cases. Scand J Infect Dis 2002;34(4):273-7.
(99) Smith PK, Daglish L. Sex differences in parent and infant behavior in the home. Child Dev 1977 Dec;48(4):1250-4.
- References
Disease in childhood and the impact of childcare
52
(100) Greaves MF. Aetiology of acute leukaemia. Lancet 1997 Feb 1;349(9048):344-9.
(101) Smith MA, Chen T, Simon R. Age-specific incidence of acute lymphoblastic leuke-mia in U.S. children: in utero initiation model. J Natl Cancer Inst 1997 Oct 15;89(20):1542-4.
(102) Pui CH, Boyett JM, Relling MV, Harrison PL, Rivera GK, Behm FG et al. Sex differ-ences in prognosis for children with acute lymphoblastic leukemia. J Clin Oncol 1999 Mar;17(3):818-24.
(103) Hemminki K, Kyyronen P, Vaittinen P. Parental age as a risk factor of childhood leukemia and brain cancer in offspring. Epidemiology 1999 May;10(3):271-5.
(104) Dockerty JD, Draper G, Vincent T, Rowan SD, Bunch KJ. Case-control study of pa-rental age, parity and socioeconomic level in relation to childhood cancers. Int J Epidemiol 2001 Dec;30(6):1428-37.
(105) Rothman K.J., Greenland S. Modern Epidemiology. Second edition. Philadelphia: Lippincott-Raven; 1998.
(106) Glymour MM, Weuve J, Berkman LF, Kawachi I, Robins JM. When is baseline ad-justment useful in analyses of change? An example with education and cognitive change. Am J Epidemiol 2005 Aug 1;162(3):267-78.
(107) Quigley MA, Kelly YJ, Sacker A. Breastfeeding and hospitalization for diarrheal and respiratory infection in the United Kingdom Millennium Cohort Study. Pediatrics 2007 Apr;119(4):e837-e842.
(108) Benn CS, Wohlfahrt J, Aaby P, Westergaard T, Benfeldt E, Michaelsen KF et al. Breastfeeding and risk of atopic dermatitis, by parental history of allergy, during the first 18 months of life. Am J Epidemiol 2004 Aug 1;160(3):217-23.
(109) Ahlbom A, Alfredsson L. Interaction: A word with two meanings creates confusion. Eur J Epidemiol 2005;20(7):563-4.
(110) Rothman K.J. Measuring interactions. Epidemiology - an introduction. Oxford Uni-versity Press; 2002.
(111) Skrondal A. Interaction as departure from additivity in case-control studies: a cau-tionary note. Am J Epidemiol 2003 Aug 1;158(3):251-8.
(112) Giesecke J. Modern Infectious Disease Epidemiology. Second edition. London: Ar-nold; 2002.
(113) Tjur T. [The Poisson model with over dispersion]. Copenhagen Business School 2004.
(114) Holford TR. Analysing the temporal effects of age, period and cohort. Stat Methods Med Res 1992;1(3):317-37.
(115) Heuch I, Albrektsen G, Kvale G. Modeling effects of age at and time since delivery on subsequent risk of cancer. Epidemiology 1999 Nov;10(6):739-46.
(116) Hjuler T, Wohlfahrt J, Simonsen J, Kaltoft MS, Koch A, Kamper-Jorgensen M et al. Perinatal and crowding-related risk factors for invasive pneumococcal disease in in-fants and young children: a population-based case-control study. Clin Infect Dis 2007 Apr 15;44(8):1051-6.
- References
Study I
53
54

ORIGINAL ARTICLE
Temporal trend in paediatric infections in DenmarkM Kamper-Jørgensen, J Wohlfahrt, J Simonsen, N Thrane, C S Benn. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Mr M Kamper-Jørgensen,Department ofEpidemiology Research,Statens Serum Institut,Artillerivej 5, 2300Copenhagen S, Denmark;[email protected]
Accepted 30 January 2006Published Online First7 February 2006. . . . . . . . . . . . . . . . . . . . . . .
Arch Dis Child 2006;91:401–404. doi: 10.1136/adc.2005.085787
Aim: To study temporal trends in the incidence of hospitalisations due to infection in children in Denmark.Methods: A national register based cohort of 1 892 711 Danish children aged 0–5 years were studiedfrom 1980 to 2001. Child and family characteristics were identified in the Danish Civil RegistrationSystem; hospitalisations were identified in the Danish National Patient Registry. Annual incidence rateswere estimated using log-linear Poisson regression.Results: During the studied period, the incidence of hospitalisations from infection increased by 62% in0–5 year old children. The increase was mainly due to a sevenfold increase in the incidence of infectionsleading to short term hospitalisation in children aged 0–1 years. Since the increase in incidence wascontrasted with a decrease in duration of hospitalisation, no further strain was put on the health services inDenmark.Conclusion: During the last two decades, the incidence of short term hospitalisations due to infectionsincreased markedly among the youngest children. However, the strain on the health services remainedconstant. The observed increase in the incidence of short term hospitalisations among the youngestchildren may reflect changes in hospitalisation practices and utilisation, rather than an increase inincidence of infections.
Arecent study1 showed that 33 boys and 23 girls,respectively, were admitted to hospital with a respira-tory infection per 1000 risk years in children aged 0–5
years in Denmark. Other epidemiological studies have shownan increase in the rates of hospitalised children during thepast decades.2–9 These studies do not agree as to whether theobserved increase is due to an increase in morbidity,2 orwhether it is due to other factors, such as changedhospitalisation practices and utilisation.3 6 7 To further inves-tigate this, we studied the incidence of hospitalisations due toinfections in children aged 0–5 years in the period from 1980to 2001. This was done in a national prospective registerbased study, in which annual incidence rates were stratifiedon types of infection, age groups, and duration of hospitalisa-tion.
METHODSAs of 1 January 2001, the population in Denmark was5 349 212, of which 8% were 0–5 years old.10
Population and hospitalisation dataThe present study is based on Danish register data and wasapproved by the Danish Data Protection Agency. In theDanish Civil Registration System (DCRS)11 we identified allchildren in Denmark between 0 and 5 years of age in theperiod from 1980 to 2001. The DCRS was established on1 April 1968, and all residents and newborns in Denmarkhave since been given a unique 10-digit person identificationnumber, which is also recorded in other Danish registers.From the DCRS, information was retrieved regarding date ofbirth, sex, county of residence and possible date of immigra-tion, emigration, and death of the child. Information on birthorder, marital state, and age of the mother at the time ofdelivery, as well as ethnicity of the child, was subsequentlyobtained by identifying the parents in the DCRS. Theinformation from the DCRS was linked with informationregarding discharge diagnosis and duration of the hospitaladmission from the Danish National Patient Registry(DNPR).12 Finally, birth weight and gestational age datawas obtained from the Danish Medical Birth Registry13 and
linked with the information from DCRS and DNPR. Theoutcome of the study was defined as first inpatient admissionto hospital with an infection (main condition only).Diagnoses were classified into groups of upper respiratoryinfections, lower respiratory infections, gastrointestinalinfections, and other infections (table 1).
Statistical methodsAnnual incidence rates were estimated as the annual numberof cases divided by the annual amount of person-years atrisk. Person-years at risk were calculated by assuming thatchildren were at risk from one week after birth, immigration,or start of 1980, whichever came first, until the first of thefollowing events: first inpatient admission to hospital with aninfection, emigration, death, end of 2001, or 6th birthday.The first week after birth was not included as infections inthis period were considered to be due to perinatal complica-tions. Data from the DNPR was available from 1977, but weexcluded data before 1980 from our analyses to reduce therisk of a later hospitalisation being counted as the first.Estimation of incidence rates according to other covariateswas performed in the same manner within strata of thecovariate. When estimating incidence rates according toduration of hospital admission, the annual number of caseswas divided according to duration, whereas the annualperson-years at risk were used in all categories. Incidence rateratios were estimated by log-linear Poisson regression of thenumber of cases with the logarithm of person-years at risk asoffset. Estimation was performed by PROC GENMOD in SASwith Poisson error distribution and log link.14
RESULTSThe population under study consisted of 1 892 711 children,of which 51.2% were boys. During follow up, a total of309 737 first hospital admissions with infections wererecorded. Upper respiratory infections were most frequent(41%), followed by lower respiratory infections (29%), other
Abbreviations: DCRS, Danish Civil Registration System; DNPR, DanishNational Patient Registry
401
55
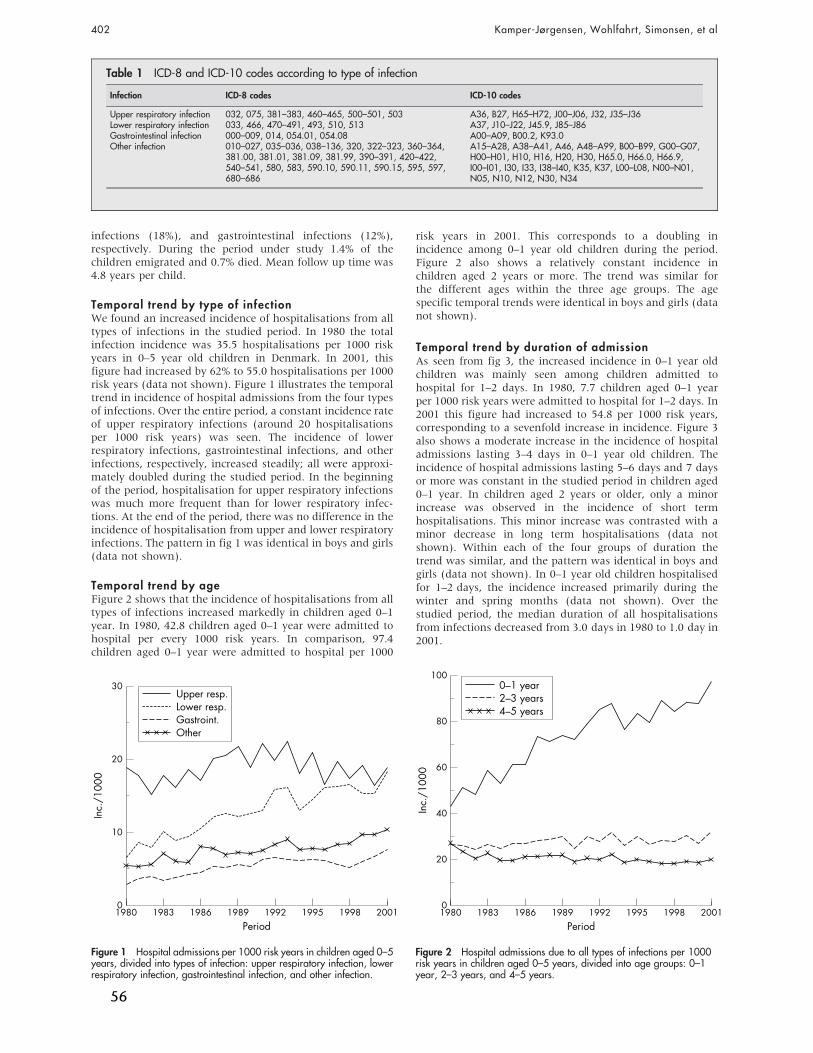
infections (18%), and gastrointestinal infections (12%),respectively. During the period under study 1.4% of thechildren emigrated and 0.7% died. Mean follow up time was4.8 years per child.
Temporal trend by type of infectionWe found an increased incidence of hospitalisations from alltypes of infections in the studied period. In 1980 the totalinfection incidence was 35.5 hospitalisations per 1000 riskyears in 0–5 year old children in Denmark. In 2001, thisfigure had increased by 62% to 55.0 hospitalisations per 1000risk years (data not shown). Figure 1 illustrates the temporaltrend in incidence of hospital admissions from the four typesof infections. Over the entire period, a constant incidence rateof upper respiratory infections (around 20 hospitalisationsper 1000 risk years) was seen. The incidence of lowerrespiratory infections, gastrointestinal infections, and otherinfections, respectively, increased steadily; all were approxi-mately doubled during the studied period. In the beginningof the period, hospitalisation for upper respiratory infectionswas much more frequent than for lower respiratory infec-tions. At the end of the period, there was no difference in theincidence of hospitalisation from upper and lower respiratoryinfections. The pattern in fig 1 was identical in boys and girls(data not shown).
Temporal trend by ageFigure 2 shows that the incidence of hospitalisations from alltypes of infections increased markedly in children aged 0–1year. In 1980, 42.8 children aged 0–1 year were admitted tohospital per every 1000 risk years. In comparison, 97.4children aged 0–1 year were admitted to hospital per 1000
risk years in 2001. This corresponds to a doubling inincidence among 0–1 year old children during the period.Figure 2 also shows a relatively constant incidence inchildren aged 2 years or more. The trend was similar forthe different ages within the three age groups. The agespecific temporal trends were identical in boys and girls (datanot shown).
Temporal trend by duration of admissionAs seen from fig 3, the increased incidence in 0–1 year oldchildren was mainly seen among children admitted tohospital for 1–2 days. In 1980, 7.7 children aged 0–1 yearper 1000 risk years were admitted to hospital for 1–2 days. In2001 this figure had increased to 54.8 per 1000 risk years,corresponding to a sevenfold increase in incidence. Figure 3also shows a moderate increase in the incidence of hospitaladmissions lasting 3–4 days in 0–1 year old children. Theincidence of hospital admissions lasting 5–6 days and 7 daysor more was constant in the studied period in children aged0–1 year. In children aged 2 years or older, only a minorincrease was observed in the incidence of short termhospitalisations. This minor increase was contrasted with aminor decrease in long term hospitalisations (data notshown). Within each of the four groups of duration thetrend was similar, and the pattern was identical in boys andgirls (data not shown). In 0–1 year old children hospitalisedfor 1–2 days, the incidence increased primarily during thewinter and spring months (data not shown). Over thestudied period, the median duration of all hospitalisationsfrom infections decreased from 3.0 days in 1980 to 1.0 day in2001.
Table 1 ICD-8 and ICD-10 codes according to type of infection
Infection ICD-8 codes ICD-10 codes
Upper respiratory infection 032, 075, 381–383, 460–465, 500–501, 503 A36, B27, H65–H72, J00–J06, J32, J35–J36Lower respiratory infection 033, 466, 470–491, 493, 510, 513 A37, J10–J22, J45.9, J85–J86Gastrointestinal infection 000–009, 014, 054.01, 054.08 A00–A09, B00.2, K93.0Other infection 010–027, 035–036, 038–136, 320, 322–323, 360–364,
381.00, 381.01, 381.09, 381.99, 390–391, 420–422,540–541, 580, 583, 590.10, 590.11, 590.15, 595, 597,680–686
A15–A28, A38–A41, A46, A48–A99, B00–B99, G00–G07,H00–H01, H10, H16, H20, H30, H65.0, H66.0, H66.9,I00–I01, I30, I33, I38–I40, K35, K37, L00–L08, N00–N01,N05, N10, N12, N30, N34
30
20
10
02001
Period
Other
Inc.
/100
0
1980 1983 1986 1989 1992 1995 1998
Gastroint.Lower resp.Upper resp.
Figure 1 Hospital admissions per 1000 risk years in children aged 0–5years, divided into types of infection: upper respiratory infection, lowerrespiratory infection, gastrointestinal infection, and other infection.
100
80
60
20
40
02001
Period
Inc.
/100
0
1980 1983 1986 1989 1992 1995 1998
4–5 years2–3 years0–1 year
Figure 2 Hospital admissions due to all types of infections per 1000risk years in children aged 0–5 years, divided into age groups: 0–1year, 2–3 years, and 4–5 years.
402 Kamper-Jørgensen, Wohlfahrt, Simonsen, et al
56
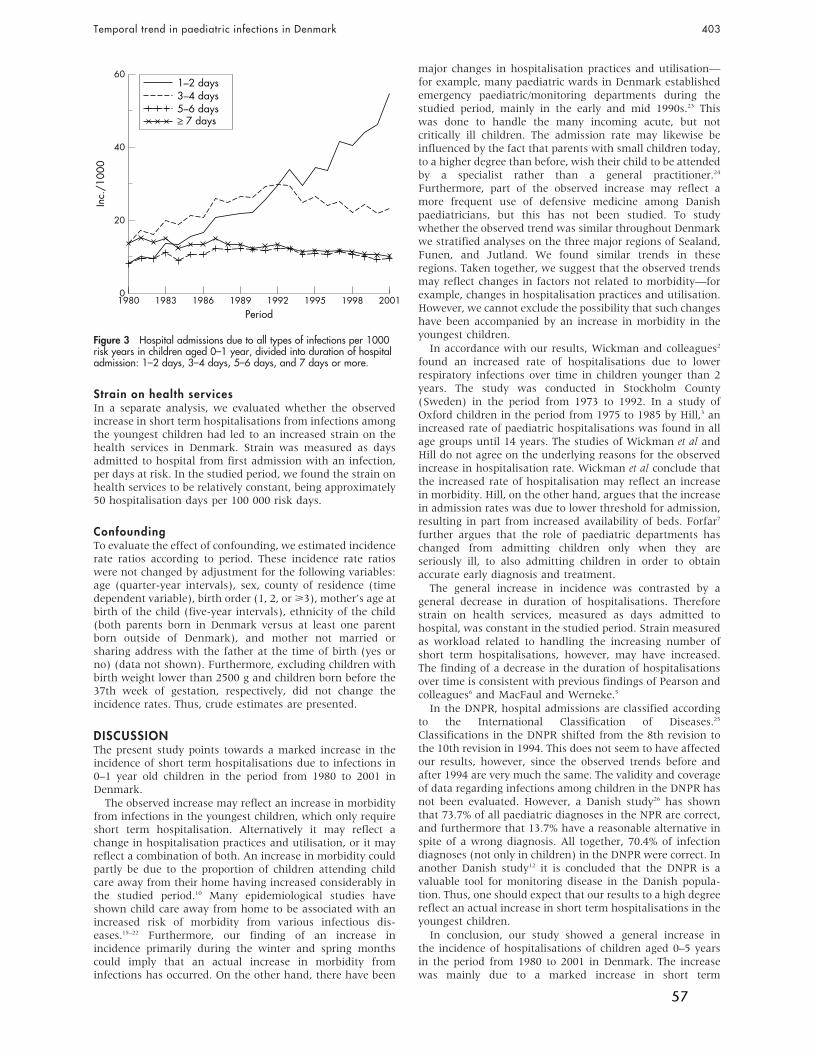
Strain on health servicesIn a separate analysis, we evaluated whether the observedincrease in short term hospitalisations from infections amongthe youngest children had led to an increased strain on thehealth services in Denmark. Strain was measured as daysadmitted to hospital from first admission with an infection,per days at risk. In the studied period, we found the strain onhealth services to be relatively constant, being approximately50 hospitalisation days per 100 000 risk days.
ConfoundingTo evaluate the effect of confounding, we estimated incidencerate ratios according to period. These incidence rate ratioswere not changed by adjustment for the following variables:age (quarter-year intervals), sex, county of residence (timedependent variable), birth order (1, 2, or >3), mother’s age atbirth of the child (five-year intervals), ethnicity of the child(both parents born in Denmark versus at least one parentborn outside of Denmark), and mother not married orsharing address with the father at the time of birth (yes orno) (data not shown). Furthermore, excluding children withbirth weight lower than 2500 g and children born before the37th week of gestation, respectively, did not change theincidence rates. Thus, crude estimates are presented.
DISCUSSIONThe present study points towards a marked increase in theincidence of short term hospitalisations due to infections in0–1 year old children in the period from 1980 to 2001 inDenmark.
The observed increase may reflect an increase in morbidityfrom infections in the youngest children, which only requireshort term hospitalisation. Alternatively it may reflect achange in hospitalisation practices and utilisation, or it mayreflect a combination of both. An increase in morbidity couldpartly be due to the proportion of children attending childcare away from their home having increased considerably inthe studied period.10 Many epidemiological studies haveshown child care away from home to be associated with anincreased risk of morbidity from various infectious dis-eases.15–22 Furthermore, our finding of an increase inincidence primarily during the winter and spring monthscould imply that an actual increase in morbidity frominfections has occurred. On the other hand, there have been
major changes in hospitalisation practices and utilisation—for example, many paediatric wards in Denmark establishedemergency paediatric/monitoring departments during thestudied period, mainly in the early and mid 1990s.23 Thiswas done to handle the many incoming acute, but notcritically ill children. The admission rate may likewise beinfluenced by the fact that parents with small children today,to a higher degree than before, wish their child to be attendedby a specialist rather than a general practitioner.24
Furthermore, part of the observed increase may reflect amore frequent use of defensive medicine among Danishpaediatricians, but this has not been studied. To studywhether the observed trend was similar throughout Denmarkwe stratified analyses on the three major regions of Sealand,Funen, and Jutland. We found similar trends in theseregions. Taken together, we suggest that the observed trendsmay reflect changes in factors not related to morbidity—forexample, changes in hospitalisation practices and utilisation.However, we cannot exclude the possibility that such changeshave been accompanied by an increase in morbidity in theyoungest children.
In accordance with our results, Wickman and colleagues2
found an increased rate of hospitalisations due to lowerrespiratory infections over time in children younger than 2years. The study was conducted in Stockholm County(Sweden) in the period from 1973 to 1992. In a study ofOxford children in the period from 1975 to 1985 by Hill,3 anincreased rate of paediatric hospitalisations was found in allage groups until 14 years. The studies of Wickman et al andHill do not agree on the underlying reasons for the observedincrease in hospitalisation rate. Wickman et al conclude thatthe increased rate of hospitalisation may reflect an increasein morbidity. Hill, on the other hand, argues that the increasein admission rates was due to lower threshold for admission,resulting in part from increased availability of beds. Forfar7
further argues that the role of paediatric departments haschanged from admitting children only when they areseriously ill, to also admitting children in order to obtainaccurate early diagnosis and treatment.
The general increase in incidence was contrasted by ageneral decrease in duration of hospitalisations. Thereforestrain on health services, measured as days admitted tohospital, was constant in the studied period. Strain measuredas workload related to handling the increasing number ofshort term hospitalisations, however, may have increased.The finding of a decrease in the duration of hospitalisationsover time is consistent with previous findings of Pearson andcolleagues6 and MacFaul and Werneke.5
In the DNPR, hospital admissions are classified accordingto the International Classification of Diseases.25
Classifications in the DNPR shifted from the 8th revision tothe 10th revision in 1994. This does not seem to have affectedour results, however, since the observed trends before andafter 1994 are very much the same. The validity and coverageof data regarding infections among children in the DNPR hasnot been evaluated. However, a Danish study26 has shownthat 73.7% of all paediatric diagnoses in the NPR are correct,and furthermore that 13.7% have a reasonable alternative inspite of a wrong diagnosis. All together, 70.4% of infectiondiagnoses (not only in children) in the DNPR were correct. Inanother Danish study12 it is concluded that the DNPR is avaluable tool for monitoring disease in the Danish popula-tion. Thus, one should expect that our results to a high degreereflect an actual increase in short term hospitalisations in theyoungest children.
In conclusion, our study showed a general increase inthe incidence of hospitalisations of children aged 0–5 yearsin the period from 1980 to 2001 in Denmark. The increasewas mainly due to a marked increase in short term
60
40
20
02001
Period
Inc.
/100
0
1980 1983 1986 1989 1992 1995 1998
5–6 days3–4 days1–2 days
≥ 7 days
Figure 3 Hospital admissions due to all types of infections per 1000risk years in children aged 0–1 year, divided into duration of hospitaladmission: 1–2 days, 3–4 days, 5–6 days, and 7 days or more.
Temporal trend in paediatric infections in Denmark 403
57

hospitalisations in 0–1 year old children. Due to a decrease induration of hospitalisations, the strain from hospitalisation ofchildren with infections on the health services in Denmarkwas not increased during the period. We suggest that theobserved increase in the incidence of short term hospitalisa-tions in the youngest children reflects changes in hospitalisa-tion practices and utilisation rather than an actual increase inthe incidence of infections. Future research within the areashould evaluate the effect of factors such as child careattendance and hospitalisation practices and utilisation onhospitalisation incidence.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
M Kamper-Jørgensen, J Wohlfahrt, J Simonsen, Department ofEpidemiology Research, Statens Serum Institut, DenmarkN Thrane, Department of Paediatrics, Herning Central Hospital,DenmarkC S Benn, Bandim Health Project, Statens Serum Institut, Denmark
Funding: The present study received support from the Danish GraduateSchool in Public Health Science, the Health Insurance Foundation, theEgmont Foundation, the National Union of Nursery and Child-careAssistance, Rosalie Petersens Fond and Gangstedfonden. All contribut-ing authors are independent of funders.
Competing interests: none declared
REFERENCES1 Jensen-Fangel S, Mohey R, Johnsen SP, et al. Gender differences in
hospitalization rates for respiratory tract infections in Danish youth.Scand J Infect Dis 2004;36:31–6.
2 Wickman M, Farahmand BY, Persson PG, et al. Hospitalization for lowerrespiratory disease during 20 yrs among under 5 yr old children in StockholmCounty: a population based survey. Eur Respir J 1998;11:366–70.
3 Hill AM. Trends in paediatric medical admissions. BMJ 1989;298:1479–83.4 Spencer NJ, Lewis MA. Multiple admissions under 2 years of age. Arch Dis
Child 1991;66:938–40.5 MacFaul R, Werneke U. Recent trends in hospital use by children in England.
Arch Dis Child 2001;85:203–7.6 Pearson G, Barry P, Timmins C, et al. Changes in the profile of paediatric
intensive care associated with centralisation. Intensive Care Med2001;27:1670–3.
7 Forfar JO. Trends in paediatric medical admissions. BMJ 1989;298:1711.8 Nielsen A, Lie H, Keiding L, et al. Admissions in hospital. In: The health of
children in Denmark. Copenhagen: Danish Institute of Clinical Epidemiology,1998:50–4.
9 Durojaiye LI, Hutchison T, Madeley RJ. Improved primary care does notprevent the admission of children to hospital. Public Health 1989;103:181–8.
10 http://www.statbank.dk, 2004.11 Malig C. The Civil Registration System in Denmark, IIVRS technical paper.
Bethesda, MD: International Institute for Vital Registration and Statistics,1996;66:1–6.
12 Andersen TF, Madsen M, Jorgensen J, et al. The Danish National HospitalRegister. A valuable source of data for modern health sciences. Dan Med Bull1999;46:263–8.
13 Knudsen LB, Olsen J. The Danish Medical Birth Registry. Dan Med Bull1998;45:320–3.
14 SAS Institute Inc. SAS/STAT software release 8.2. Cary, NC: SAS Institute Inc,2001.
15 Collet JP, Burtin P, Gillet J, et al. Risk of infectious diseases in childrenattending different types of day-care setting. Epicreche Research Group.Respiration 1994;61(suppl 1):16–19.
16 Klein JO. Infectious diseases and day care. Rev Infect Dis 1986;8:521–6.17 Louhiala PJ, Jaakkola N, Ruotsalainen R, et al. Form of day care and
respiratory infections among Finnish children. Am J Public Health1995;85:1109–12.
18 Louhiala PJ, Jaakkola N, Ruotsalainen R, et al. Day-care centers anddiarrhea: a public health perspective. J Pediatr 1997;131:476–9.
19 Nafstad P, Hagen JA, Oie L, Magnus P, et al. Day care centers andrespiratory health. Pediatrics 1999;103:753–8.
20 Stahlberg MR. The influence of form of day care on occurrence of acuterespiratory tract infections among young children. Thesis, University of Turku,1980.
21 Uldall P. [Forms of care and children’s infections. 1. Occurrence and causalfactors]. Ugeskr Laeger 1990;152:2345–8.
22 Wald ER, Guerra N, Byers C. Frequency and severity of infections in day care:three-year follow-up. J Pediatr 1991;118:509–14.
23 Kastrup KW, Andersen KV. [Emergency pediatric/monitoring department.The Danish Pediatric Society]. Ugeskr Laeger 2001;163:1693.
24 Lindenskov L, Bronderslev L, Andersen KV. [Why do parents of small childrenvisit casualty ward when their children suffer of acute illness?]. Ugeskr Laeger2001;163:1089–92.
25 International Classification of Diseases. WHO Collaborating Centers.Epidemiol Bull 1998;19:7–11.
26 Mosbech J, Jorgensen J, Madsen M, et al. [The national patient registry.Evaluation of data quality]. Ugeskr Laeger 1995;157:3741–5.
What this study adds
N Hospitalisation with infection has increased more than60% during the last two decades in 0–5 year oldchildren in Denmark
N The increase is almost exclusively seen in short termhospitalisations in 0–1 year old children, suggestingchanges in hospitalisation practices and utilisationrather than increase in childhood morbidity as theunderlying reason
What is already known on this topic
N Hospitalisation of children with infections has increasedover the past decades in several countries
N There is no consensus on the underlying reason for theincrease
404 Kamper-Jørgensen, Wohlfahrt, Simonsen, et al
58
Study II
59
60
Dow
nloa
ded
By:
[DN
L] A
t: 11
:33
19 J
une
2007
STUDY DESIGN ARTICLE
The Childcare Database: a valuable register linkage
MADS KAMPER-JØRGENSEN1, JAN WOHLFAHRT1, JACOB SIMONSEN1 &
CHRISTINE S. BENN2
1Statens Serum Institut, Department of Epidemiology Research, and 2Statens Serum Institut, Bandim Health Project
AbstractRationale: To assess the impact of childcare attendance on morbidity for an entire country the Childcare Database wascreated by linking person-identifiable data from several Danish national data sources. The present paper describes thecreation, characteristics, and potential of the Childcare Database. Design and measurement: Based on the unique DanishCivil Registration System (DCRS) identification number register data were linked regarding childcare attendance, child andfamily characteristics, childcare facility characteristics, and hospitalizations for children aged 0 to 5 years in the period from1989 to 2004. Population and sample size: The number of children in the database increased in the period from 1989 to 1998as more municipalities started registering childcare, whereafter it stabilized. The maximum number of children in thedatabase was 373,142 in 2000. From 1999 to 2004 the Childcare Database covered more than 90% of all 0- to 5-year-oldchildren in Denmark. At age 1 year 53% of children were enrolled in a childcare facility and approximately 75% wereenrolled from 3 to 5 years of age. Potential: The Childcare Database offers a unique potential for epidemiological researchwithin the area of childcare and morbidity. Future updates and linkages with other data sources will further expand thepotential of the database. Due to the high quality of the linked nationwide register data, the Childcare Database enablesconduction of epidemiological studies of high internal and external validity.
Key Words: Childcare, database, Denmark, register linkage
Rationale
The field of childcare and morbidity has been
thoroughly studied in Scandinavia [1–17], but has
so far been assessed using small sample sizes. Three
of the above studies [1,10,17] have been based on
local registry data while the remainder have collected
data by means of questionnaires or interviews.
Danish registers offer a unique possibility for
conducting epidemiological research using nation-
wide data within a variety of public-health-related
areas. In order to estimate the short- and long-term
impact of childcare attendance on morbidity with
high precision for an entire country we created the
Childcare Database. Person-identifiable data from
several Danish data sources were used. In the
present article we describe the creation of, the
information available in, and the potential of the
Childcare Database.
Material and methods
The material used in creating the Childcare
Database was obtained from national data sources
that identify individuals by their unique Danish Civil
Registration System (DCRS) identification number,
making linkage of data possible. The Childcare
Database includes information regarding childcare
attendance, childcare facility characteristics, child
and family characteristics, and hospitalizations.
Childcare attendance data
In Denmark all municipalities register person-
identifiable data on provision of childcare. Data are
collected routinely to organize the payment for and
distribution of places in childcare facilities. For any
child, dates of enrolment and withdrawal from a
Correspondence: Mads Kamper-Jørgensen, Department of Epidemiology Research, Statens Serum Institut, Artillerivej 5, 2300 Copenhagen S, Denmark.
Tel: +45 32688339. E-mail: [email protected]
(Accepted 17 October 2006)
Scandinavian Journal of Public Health, 2007; 35: 323–329
ISSN 1403-4948 print/ISSN 1651-1905 online/07/030323-7 # 2007 Taylor & Francis
DOI: 10.1080/14034940601072356
61

Dow
nloa
ded
By:
[DN
L] A
t: 11
:33
19 J
une
2007
childcare facility as well as the type of childcare
facility and a unique facility code were recorded.
Based on municipal data, three Danish data
management companies (KMD, GK-Consult, and
IST-Software) provided person-identifiable data on
children attending childcare. Data were provided for
266 municipalities, while data were not available for
5 municipalities. Three of these municipalities
(Odense, Aalborg, and Læsø) were not able to
deliver data electronically and two municipalities
(Mariager and Spøttrup) could only provide data
that were not readily compatible with the remaining
data. Municipalities for which data were not avail-
able included two large (Odense and Aalborg
withw150,000 inhabitants), two middle-sized
(Mariager and Spøttrup withw5,000 inhabitants),
and one small (Læsø withv2,500 inhabitants)
municipality, according to Danish standards.
Registration of enrolment into childcare started at
different times in different municipalities. The first
municipalities registered childcare attendance from
1 January 1989, whereas the last municipality started
registering from 1 January 2004. Half the munici-
palities had started registering childcare attendance
by 1 November 1991. We collected data up to 17
November 2004.
Childcare facility data
Denmark’s national statistical office, Statistics
Denmark (SD), routinely collects data on social
and health-related resources for administrative pur-
poses. Reporting to SD is mandatory and nation-
wide. From the SD register ‘Den sociale
ressourceopgørelse’ [18], which is an annual regis-
tration of social and health-related municipal
resources available for children, seniors, and dis-
abled persons, we obtained data regarding number
of employed teachers (recalculated as full years’
work for one person) and number of enrolled children
in each childcare facility for the year 1997. In contrast
to the other sources, data from SD were obtained at a
facility rather than a person level. Childcare facility
data were linked to the person level data via the unique
childcare facility code.
Child and family data
The DCRS [19] encompasses all persons who have
lived in Denmark since 1 April 1968. All individuals
alive and living in Denmark on 1 April 1968 as well
as all new residents and newborns in Denmark have
since been given a unique DCRS identification
number. From the DCRS data were extracted
regarding date of birth, death, and migrations and
familial relations for all Danish children in the period
from 1 January 1989 to 17 November 2004.
Hospitalization data
The Danish National Patient Registry (DNPR) [20]
encompasses all contacts with hospitals in Denmark,
including inpatient and all-day contacts. Data from
DNPR are collected routinely and reported to the
National Board of Health for administrative pur-
poses. For every new contact with a hospital or
transfer within a hospital, a code denoting the
admission diagnosis is registered along with the
unique DCRS identification number. The diagnosis
is coded according to the International Classification
of Diseases , which has been revised several times,
the latest in 1994 when the 10th revision (ICD-10)
was introduced in Denmark. Besides the unique
DCRS number and ICD-diagnosis codes (ICD-8
and ICD-10), we obtained the date of admission to
and discharge from hospital.
Creation of the Childcare Database
By linking the above data sources the Childcare
Database was created (Figure 1). The database
comprises all Danish children between 0 and 5 years
of age born and living in one of the 266 eligible
municipalities in the period in which the munici-
pality registered childcare attendance data between 1
January 1989 and 17 November 2004. From the
childcare attendance data we were able to determine
in which periods a child attended childcare and in
which periods he/she was not taken care of in a
childcare facility and thus was assumed to be in
homecare. Further linkage to the childcare facility
data helped us determine characteristics of the
childcare facility in which children were enrolled.
By linkage to child and family data we obtained
information on child and family characteristics for all
children in childcare and in homecare. Finally,
linkage to hospitalization data made it possible to
assess hospitalizations. At present information on
the following covariates is available in the Childcare
Database: type of childcare facility, number of
employed teachers in the childcare facility, number
of children enrolled in the childcare facility, age at first
and second enrolment, time since first and second
enrolment, sex, age, maternal age when giving birth to
the child, maternal parenthood status at time of birth
of the child, number of additional children younger
than 5 years living in the household, number of
inhabitants per km2 in the residence area, and season.
The initial steps towards forming the Childcare
Database were taken in 1999, whereas the first
324 M. Kamper-Jørgensen et al.
62
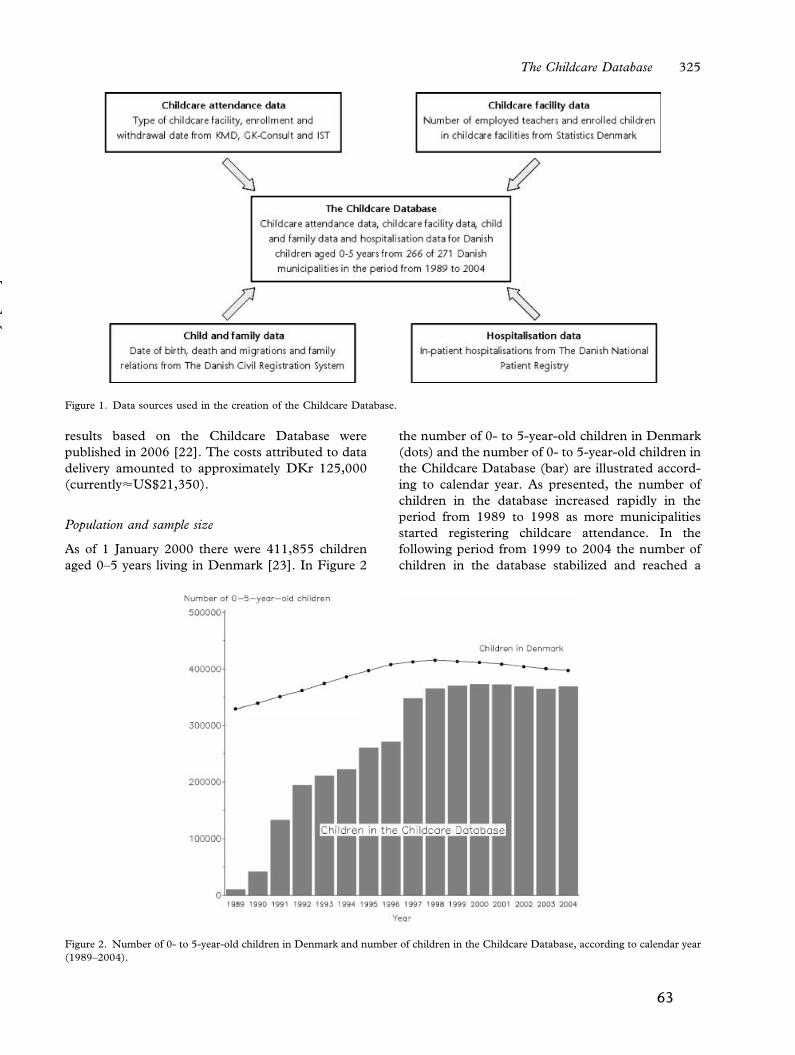
Dow
nloa
ded
By:
[DN
L] A
t: 11
:33
19 J
une
2007
results based on the Childcare Database were
published in 2006 [22]. The costs attributed to data
delivery amounted to approximately DKr 125,000
(currently<US$21,350).
Population and sample size
As of 1 January 2000 there were 411,855 children
aged 0–5 years living in Denmark [23]. In Figure 2
the number of 0- to 5-year-old children in Denmark
(dots) and the number of 0- to 5-year-old children in
the Childcare Database (bar) are illustrated accord-
ing to calendar year. As presented, the number of
children in the database increased rapidly in the
period from 1989 to 1998 as more municipalities
started registering childcare attendance. In the
following period from 1999 to 2004 the number of
children in the database stabilized and reached a
Figure 1. Data sources used in the creation of the Childcare Database.
Figure 2. Number of 0- to 5-year-old children in Denmark and number of children in the Childcare Database, according to calendar year
(1989–2004).
The Childcare Database 325
63
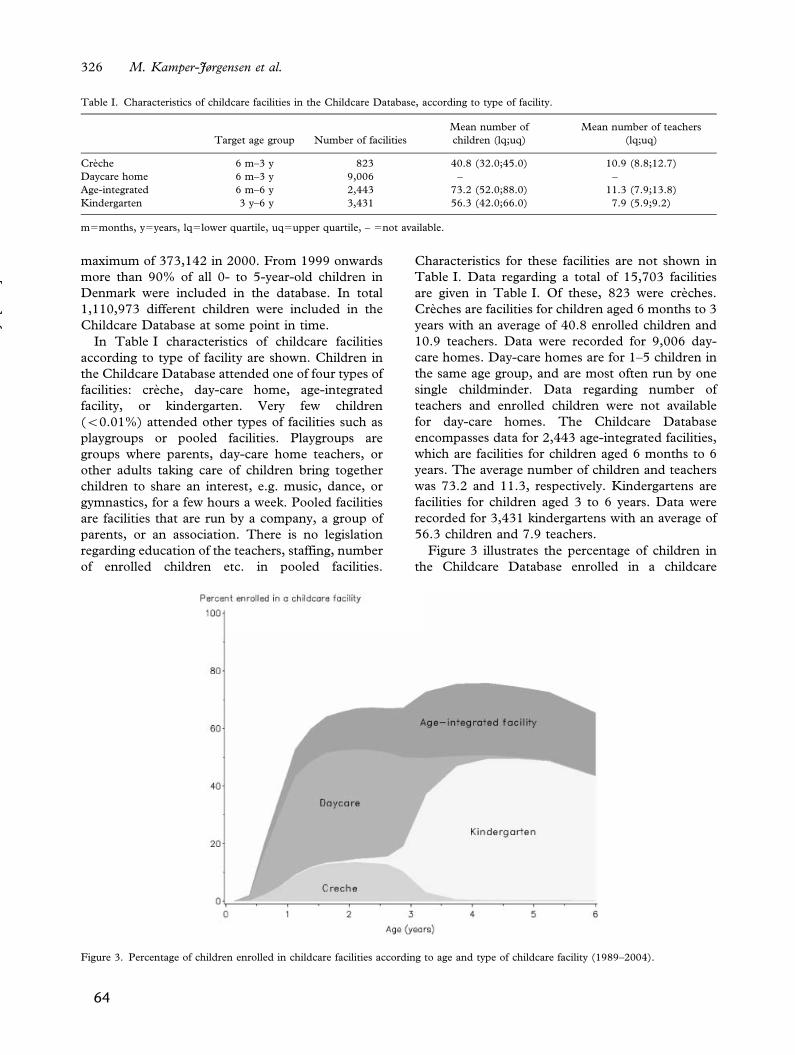
Dow
nloa
ded
By:
[DN
L] A
t: 11
:33
19 J
une
2007
maximum of 373,142 in 2000. From 1999 onwards
more than 90% of all 0- to 5-year-old children in
Denmark were included in the database. In total
1,110,973 different children were included in the
Childcare Database at some point in time.
In Table I characteristics of childcare facilities
according to type of facility are shown. Children in
the Childcare Database attended one of four types of
facilities: creche, day-care home, age-integrated
facility, or kindergarten. Very few children
(v0.01%) attended other types of facilities such as
playgroups or pooled facilities. Playgroups are
groups where parents, day-care home teachers, or
other adults taking care of children bring together
children to share an interest, e.g. music, dance, or
gymnastics, for a few hours a week. Pooled facilities
are facilities that are run by a company, a group of
parents, or an association. There is no legislation
regarding education of the teachers, staffing, number
of enrolled children etc. in pooled facilities.
Characteristics for these facilities are not shown in
Table I. Data regarding a total of 15,703 facilities
are given in Table I. Of these, 823 were creches.
Creches are facilities for children aged 6 months to 3
years with an average of 40.8 enrolled children and
10.9 teachers. Data were recorded for 9,006 day-
care homes. Day-care homes are for 1–5 children in
the same age group, and are most often run by one
single childminder. Data regarding number of
teachers and enrolled children were not available
for day-care homes. The Childcare Database
encompasses data for 2,443 age-integrated facilities,
which are facilities for children aged 6 months to 6
years. The average number of children and teachers
was 73.2 and 11.3, respectively. Kindergartens are
facilities for children aged 3 to 6 years. Data were
recorded for 3,431 kindergartens with an average of
56.3 children and 7.9 teachers.
Figure 3 illustrates the percentage of children in
the Childcare Database enrolled in a childcare
Table I. Characteristics of childcare facilities in the Childcare Database, according to type of facility.
Target age group Number of facilities
Mean number of
children (lq;uq)
Mean number of teachers
(lq;uq)
Creche 6 m–3 y 823 40.8 (32.0;45.0) 10.9 (8.8;12.7)
Daycare home 6 m–3 y 9,006 – –
Age-integrated 6 m–6 y 2,443 73.2 (52.0;88.0) 11.3 (7.9;13.8)
Kindergarten 3 y–6 y 3,431 56.3 (42.0;66.0) 7.9 (5.9;9.2)
m5months, y5years, lq5lower quartile, uq5upper quartile, – 5not available.
Figure 3. Percentage of children enrolled in childcare facilities according to age and type of childcare facility (1989–2004).
326 M. Kamper-Jørgensen et al.
64

Dow
nloa
ded
By:
[DN
L] A
t: 11
:33
19 J
une
2007
facility according to type of the facility and age of the
child. Overall 2% of children were enrolled in a
childcare facility before the age of 3 months. At age 6
months 21% and at age 1 year 53% of children were
currently enrolled in a childcare facility. From 3 to 5
years of age approximately 75% of children were
enrolled in a childcare facility. At ages 0 to 2 years
the majority of children attended day care while
fewer attended creche or age-integrated facilities. At
around 3 years of age a shift from day care and
creche was seen towards attendance at kindergarten.
Children attending other types of childcare facilities
(v0.01%) are not illustrated in Figure 3. Compared
with figures from Statistics Denmark [23] covering
the same period, the percentage of children enrolled
in a childcare facility in the Childcare Database was
slightly lower for all age groups. When excluding the
first years of the study period, the percentage of
children attending childcare was similar in the
Childcare Database and Statistics Denmark. In the
first years of the study period the percentage of
children enrolled in a childcare facility was markedly
lower in the Childcare Database compared with
Statistics Denmark. We believe this difference to be
due to incomplete municipal registration of childcare
attendance. In the period before 2004 figures from
Statistics Denmark were based on reports during the
spring months, whereas figures from 2004 onwards
are based on reports during the autumn months.
Change in timing of the reports from Statistics
Denmark has shown that fewer children are enrolled
in childcare facilities during autumn months com-
pared with spring months [23]. In the Childcare
Database the difference between the percentage
enrolled during spring and autumn months was 3
percentage points.
Discussion
The present article describes the creation of a
register-based nationwide database covering data
on childcare attendance, childcare facility character-
istics, child and family characteristics, and hospita-
lizations. The database covers the period from 1989
to 2004 with an increasing number of municipalities
registering childcare attendance in the period from
1989 to 1998 and thus covers more than 90% of all
Danish 0- to 5-year-old children in the period from
1999 to 2004.
Data were obtained from six Danish national data
sources. Since data regarding childcare attendance
are collected routinely to organize the payment and
distribution of places in childcare facilities in
Denmark, the quality of data is thought to be high
[17]. The DCRS contains very sensitive information
for all Danish citizens, and is thus affected by various
laws securing high data quality [24].
Data from five Danish municipalities were not
included in the database. According to Danish
standards two of these municipalities were big, two
were middle-sized, and one was small. This may
induce a slight under-representation of children
from big municipalities. However, this would only
affect estimation of an association between childcare
and morbidity if the association was modified by the
number of inhabitants in the municipality, which we
have no reason to suspect.
In the Childcare Database private and unregis-
tered childcare facilities are not included. This may
cause children who are taken care of in a private or
an unregistered childcare facility to be misclassified
as being in homecare. The misclassification, how-
ever, is thought to be non-differential, thus leading
only to a slight under-estimation of the effect of
attendance at childcare. Furthermore, the problem
with private and unregistered childcare facilities is
thought to be small since most Danish municipalities
guarantee a place in a public childcare facility before
for example 6 months of age. In the future, private
childcare may be included in the database since
municipalities contribute up to 75% of the expenses
of having children taken care of privately by, e.g., a
maid, grandparents, or a friend of the family.
Municipal contributions to private childcare are
registered in a system similar to that of municipal
childcare. Currently we are working on getting
access to the data.
When using the Childcare Database a population-
based design is used thereby including information
on all Danish children. This may reduce the risk of
selection biases, which may have influenced the
results of previous studies. Furthermore, by using
the Childcare Database we are able to determine
exposure status such as attendance at a certain type
of childcare at all times during follow-up. Thus
relevant variables can be constructed as being time-
dependent. This gives the advantage of precise
estimation since, for instance, shifts from childcare
to homecare or to another type of childcare during
follow-up can be taken into account. Compared with
previous studies where only one measure of, say,
childcare attendance at baseline is being used,
studies based on the Childcare Database can give
more precise estimates of effects.
The validity and coverage of data regarding
infections among children in the DNPR has not
been evaluated. However, a Danish study [25] has
shown that 73.7% of all paediatric diagnoses in the
DNPR are correct, and furthermore that 13.7% have
The Childcare Database 327
65

Dow
nloa
ded
By:
[DN
L] A
t: 11
:33
19 J
une
2007
a reasonable alternative in spite of a wrong diagnosis.
All together, 70.4% of infection diagnoses (not only
in children) in the DNPR were correct. In another
Danish study [20] it is concluded that the DNPR is a
valuable tool for monitoring disease in the Danish
population.
Previously a register-based regional database
covering childcare attendance and drug prescrip-
tions in the County of Northern Jutland, Denmark
has been established [17]. The database covers
5,035 children born in 1997 and has been used to
study prospectively the influence of day-care atten-
dance on use of systemic antibiotics [26]. In the
database covering the County of Northern Jutland as
well as in the Childcare Database, short-term
consequences of attendance at childcare facilities –
such as morbidity due to infectious diseases – can be
studied. Long-term consequences such as possible
protective effects on immune-related disorders,
however, require long periods of follow-up and a
large sample size. Initial studies of long-term
consequences are currently feasible when using the
Childcare Database but to increase the statistical
power the database will be regularly updated. We
plan to link the Childcare Database with disease
outcome measures from the Danish Childhood
Diabetes Register [27] and the Danish Cancer
Registry [28]. Using these registers it is our wish to
study the hypothesis that children heavily exposed to
infections during their first years of life are less prone
to develop immune-related disorders such as dia-
betes and leukaemia. Future plans for the Childcare
Database furthermore include linkage with the
Danish Register of Medicinal Product Statistics
[29], which will provide national information on
sales of prescription drugs. Thereby it will be
possible to study a sensitive and relevant proxy
measure of infectious disease morbidity. We further-
more aim to obtain information regarding parents’
occupational and educational level as well as their
income from Statistics Denmark. Such a linkage will
make adjustment for social and economic confoun-
ders possible and studies of differences in morbidity
in different social and economic groups feasible.
Finally we plan to link data to the Danish National
Birth Cohort [30] to study the potential confound-
ing effects of lifestyle-related factors in a sub-sample
of the Childcare Database.
The identity of the children in the Childcare
Database is given by the unique DCRS number.
This allows for linkage with other national registries
but strict rules given by the Danish Data Protection
Agency on data handling are to be followed to ensure
privacy, confidentiality, and data protection. In
Denmark strictly register-based studies with no
approach to the included subjects are not to be
notified to the Scientific Ethical Committee. No
subject-identifiable results can be reported and all
projects based on the Childcare Database are to be
notified to the Danish Data Protection Agency.
Potential
Currently the Childcare Database offers a unique
potential for epidemiological research within the
field of consequences of attendance at childcare for
an entire country. Future updates and linkage with
other data sources will further expand the possibi-
lities of the database. In conclusion the Childcare
Database allows epidemiological studies of high
internal and external validity to be conducted.
Acknowledgements
The present article received financial support from the
Health Insurance Foundation, the Egmont Found-
ation, the Danish Graduate School in Public Health
Science, Rosalie Petersens Fond, Gangstedfonden,
Aase og Ejnar Danielsens Fond and the National
Union of Nursery and Child-care Assistance.
References
[1] Bondestam M, Rasmussen F. Preschool children’s absentee-
ism from Swedish municipal day-care centres because of
illness in 1977 and 1990. Geographical variations and
characteristics of the day-care centres. Scand J Soc Med
1994;22:20–6.
[2] Dahl IL, Grufman M, Hellberg C, Krabbe M. Absenteeism
because of illness at daycare centers and in three-family
systems. Acta Paediatr Scand 1991;80:436–45.
[3] Forssell G, Hakansson A, Mansson NO. Risk factors for
respiratory tract infections in children aged 2–5 years. Scand
J Prim Health Care 2001;19:122–5.
[4] Hagerhed-Engman L, Bornehag CG, Sundell J, Aberg N.
Day-care attendance and increased risk for respiratory and
allergic symptoms in preschool age. Allergy 2006;61:447–53.
[5] Hasle H, Viskum B. [Morbidity among children attending
nursery schools]. Ugeskr Laeger 1989;151:2148–50.
[6] Hedin K, Petersson C, Cars H, Beckman A, Hakansson A.
Infection prevention at day-care centres: Feasibility and
possible effects of intervention. Scand J Prim Health Care
2006;24:44–9.
[7] Nafstad P, Hagen JA, Oie L, Magnus P, Jaakkola JJ. Day
care centers and respiratory health. Pediatrics
1999;103:753–8.
[8] Nielsen AM, Koefoed BG, Møller R, Laursen B. [Recent
morbidity in Danish children in 1994 and 2000]. Ugeskr
Laeger 2006;168:373–8.
[9] Nystad W, Skrondal A, Magnus P. Day care attendance,
recurrent respiratory tract infections and asthma. Int J
Epidemiol 1999;28:882–7.
[10] Petersson C, Hakansson A. A retrospective study of
respiratory tract infections among children in different forms
of day care. Scand J Prim Health Care 1990;8:119–22.
328 M. Kamper-Jørgensen et al.
66
Dow
nloa
ded
By:
[DN
L] A
t: 11
:33
19 J
une
2007
[11] Rindel AK, Kronborg D, Jensen ST. [Morbidity in
Copenhagen nurseries according to social, physical, envir-
onmental and hygienic factors]. Ugeskr Laeger 1992;154:
2140–6.
[12] Rindel AK, Christensen M, Kronborg D, Jensen ST.
[Influence of space for morbidity in Copenhagen nurseries].
Ugeskr Laeger 1997;159:6205–10.
[13] Sennerstam RB. Absence due to illness among toddlers in
daycare centres in relation to child group structure. Public
Health 1997;111:85–8.
[14] Soderstrom M, Martensson F, Grahn P, Blennow M. [The
outdoor environment of day care centres. Its importance to
play and development]. Ugeskr Laeger 2004;166:3089–92.
[15] Strangert K. Respiratory illness in preschool children with
different forms of day care. Pediatrics 1976;57:191–6.
[16] Uldall P. [Common morbidity in infants and young children –
occurrence and social consequences] Thesis, Copenhagen,
1986.
[17] Thrane N. Prescription of systemic antibiotics for Danish
children. Thesis, Aarhus, 2000.
[18] Statistics Denmark, [Social conditions, health and judicial
system]. Technical Report. Available at: http://www.dst.dk,
1999.
[19] Malig C. The Civil Registration System in Denmark, IIVRS
Technical Paper 66. Bethesda, MD: International Institute
for Vital Registration and Statistic; 1996. p 1–6.
[20] Andersen TF, Madsen M, Jorgensen J, Mellemkjoer L,
Olsen JH. The Danish National Hospital Register: A
valuable source of data for modern health sciences. Dan
Med Bull 1999;46:263–8.
[21] International classification of diseases, WHO Collaborating
Centers. Epidemiol Bull 1998;19:7–11.
[22] Kamper-Jorgensen M, Wohlfahrt J, Simonsen J,
Grønbæk M, Benn CS. Population–based study of the
impact of childcare attendance on hospitalizations for acute
respiratory infections. Pediatrics 2006;118:1439–46.
[23] Statistics Denmark, Statistical yearbook. Copenhagen:
Author; 2002.
[24] The Civil Registration System [2005]. Available at: http://
www.cpr.dk.
[25] Mosbech J, Jorgensen J, Madsen M, Rostgaard K,
Thornberg K, Poulsen TD. [The national patient registry.
Evaluation of data quality]. Ugeskr Laeger 1995;157:
3741–5.
[26] Thrane N, Olesen C, Md JT, Sondergaard C,
Schonheyder HC, Sorensen HT. Influence of day care
attendance on the use of systemic antibiotics in 0- to 2-year-
old children. Pediatrics 2001;107:E76.
[27] Svensson J. Incidence of Type 1 diabetes 1970–2000 and
risk factors for developing Type 1 diabetes in Danish
children 2002. Thesis, Copenhagen, 2003.
[28] Storm HH, Michelsen EV, Clemmensen IH, Pihl J. The
Danish Cancer Registry: History, content, quality and use.
Dan Med Bull 1997;44:535–9.
[29] Anon [Access to Statistics Denmark’s Lægemiddeldatabasen
(2005)]. Available at: http://www.dst.dk.
[30] Olsen J, Melbye M, Olsen SF, Sorensen TI, Aaby P,
Andersen AM, et al. The Danish National Birth Cohort: Its
background, structure and aim. Scand J Public Health
2001;29:300–7.
The Childcare Database 329
67

68
Study III
69
70
ARTICLE
Population-Based Study of the Impact of ChildcareAttendance on Hospitalizations for AcuteRespiratory InfectionsMads Kamper-Jørgensen, MSca, Jan Wohlfahrt, DMSca, Jacob Simonsen, MSca, Morten Grønbæk, DMScb, Christine Stabell Benn, PhDc
aDepartment of Epidemiology Research and cBandim Health Project, Statens Serum Institut, Copenhagen, Denmark; bNational Institute of Public Health, Copenhagen,Denmark
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVES. It is well known that children attending childcare have a higher risk ofacute respiratory infections compared with children in home care; however,knowledge is sparse regarding how the excess risk of acute respiratory infectionvaries with age, time since enrollment, and other factors.
METHODS.A national register-based study of 138 821 inpatient admissions to hospitalfor acute respiratory infection during 3 982 925 person-years of follow-up inDanish children aged 0 to 5 years. Data on child and family characteristics,childcare attendance, and hospitalizations were obtained from Danish registries.The outcome of the study was inpatient admissions to hospital for acute respiratoryinfection. Incidence rate ratios were estimated using Poisson regression.
RESULTS. In children �1 year of age, the first 6 months of enrollment in the firstchildcare facility were associated with a 69% higher incidence of hospitalizationsfor acute respiratory infection compared with children in home care. Similarfigures for children aged 1, 2, and �3 years were 47%, 41%, and 8%, respectively.The incidence decreased after the first 6 months, and after �1 year in childcare theincidence was comparable with that of children in home care. Similar patternswere seen after second enrollment. For 0- to 2-year-old children living in house-holds with no additional children �5 years, the excess incidence during the first 6months of enrollment was 100% compared with 25% and 9% for children livingwith 1 and �2 additional children, respectively.
CONCLUSIONS. The increased risk of acute respiratory infection was most pronouncedamong 0- to 2-year-old children living with no other children during the first 6months of enrollment. Our findings may suggest that it would be optimal topostpone enrollment into childcare until after 1 year of age.
www.pediatrics.org/cgi/doi/10.1542/peds.2006-0373
doi:10.1542/peds.2006-0373
KeyWordschildcare, acute respiratory infection,morbidity, epidemiology
AbbreviationsARI—acute respiratory infectionDCRS—Danish Civil Registration SystemDNPR—Danish National Patient RegistryICD—International Classification ofDiseasesURI—upper respiratory infectionLRI—lower respiratory infectionIRR—incidence rate ratioCI—confidence interval
Accepted for publication May 24, 2006
Address correspondence to Mads Kamper-Jørgensen, Department of EpidemiologyResearch, Statens Serum Institut, Artillerivej 5,2300 Copenhagen S, Denmark. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005;Online, 1098-4275). Copyright © 2006 by theAmerican Academy of Pediatrics
71

PREVIOUS STUDIES HAVE consistently found that chil-dren who are taken care of in a childcare facility
away from their home have a higher risk of acute respi-ratory infections (ARIs) than children in home care.1–22
In some studies, age4,8,11,21,22 or type of facility1,2,8,12,14–16
have been studied as modifying factors in the associationbetween childcare attendance and the risk of ARIs. How-ever, sample sizes of these studies have not allowed forsafe conclusions, and many potential modifying factorshave not yet been studied. Modifying factors are impor-tant to study to identify particularly vulnerable groupsand focus on a possible intervention.
In the present study, we took advantage of a nationalcentral registration of enrollment into childcare facilities,child and family characteristics, and hospitalizations. Us-ing this material, we were able to determine child andfamily characteristics at all times during the study pe-riod. Thus, we could obtain precise and reliable estimatesof the impact of childcare attendance on hospitalizationsfor ARI and identify child- and family-related factorsthat might modify the association.
MATERIALS
Study PopulationThe study was based on a cohort of all of the Danishchildren born in the period from January 1, 1989, toNovember 17, 2004, in a municipality with childcareregistration at time of birth. The study population wasidentified in the Danish Civil Registration System(DCRS).23 The DCRS was established April 1, 1968, whenall individuals alive and living in Denmark were assigned aunique person identification number. Since April 1, 1968,all newborns in Denmark have been assigned a uniqueperson identification number. The number is also re-corded in other Danish registers. From the DCRS, infor-mation was retrieved regarding date of birth of the child,maternal age at birth of the child, and gender of thechild, and throughout follow-up, information was ob-tained on postal address, migration, and death of thechild, as well as number of children �5 years of age inthe household.
Childcare Attendance DataThe information from the DCRS was linked with infor-mation regarding enrollment into childcare facilitiesfrom 3 data sources. These sources cover all childcareattendance in 266 of the 271 Danish municipalities. Foreach enrollment, date of enrollment and date of with-drawal was retrieved. Children from the 266 eligiblemunicipalities who did not figure in any of the 3 child-care enrollment registers were considered in home care.Registration of enrollment into childcare did not start atthe same date in all of the municipalities. Therefore, thestudy period differed between municipalities. The firstmunicipalities registered enrollment from January 1,
1989, whereas the last municipality started registeringfrom January 1, 2004. Creches and day care homes arefacilities for children aged 6 months to 3 years. Increches, an average of 11 teachers look after 41 children,whereas day care homes are attended by �5 childrenand run by 1 single child minder. Age-integrated facili-ties are attended by children aged 6 months to 6 years.On average, 11 teachers mind 73 children. Kindergar-tens are facilities for children aged 3 to 6 years where, onaverage, 8 teachers mind 56 children.
According to national guidelines,24 ill/infectious chil-dren should not attend childcare until they are well andno longer contagious. A child is well when able to par-ticipate in usual activities without special care.
Hospitalization DataFrom the Danish National Patient Registry (DNPR),25
International Classification of Diseases (ICD) 8, orICD-10 diagnoses were identified for children who hadbeen hospitalized during the relevant follow-up period.The outcome of the study was defined as an inpatientadmission to hospital for ARI as the main condition.Diagnoses used to define ARI in the period from 1989 to1993 were 032, 033, 075, 381 to 383, 460 to 466, 470 to486, 490, 500, 501, 503, 510, and 513 (ICD-8) and A36,A37, B27, H65 to H67, H70, J00 to J06, J10 to J22, J32,J35, J36, J45, J85, and J86 (ICD-10) in the period from1994 to 2004. ARIs were subgrouped into upper respi-ratory infection (URI) and lower respiratory infection(LRI) as described in a previous publication.26
Statistical MethodsImpact of childcare attendance on ARI was evaluatedby incidence rate ratio (IRR). IRRs with 95% confi-dence intervals (CI) were estimated by multiple log-linear quasi-Poisson regression of the number of caseswith the logarithm of person-years at risk as offset. Aquasi-Poisson regression model was used instead of atraditional Poisson regression model to take into accountthe overdispersion that potentially could be induced bythe clustering of events within the same person, families,or childcare facilities. The quasi-Poisson regressionmodel is based on a Poisson quasi-likelihood where thevariance is allowed to be the mean multiplied by anoverdispersion factor.27 The IRR estimates are the sameas in the traditional Poisson regression model, but theCIs are slightly widened.
Person-years at risk were calculated from 1 week afterbirth, immigration, or date of first registration in one ofthe eligible municipalities, whichever came last. The firstweek after birth was not included, because infections inthis period were considered to be because of perinatalcomplications. Children were considered at risk until thefirst of the following events: emigration, moving to anineligible municipality, death, sixth birthday, or end offollow-up (November 17, 2004). Each admission to hos-
72

pital of the same child during the follow-up period wascounted as a new case of hospitalization with covariatesaccording to the time of hospitalization. However, chil-dren were not considered at risk the first 14 days after ahospitalization, because hospitalizations in this periodcould be related to the preceding hospitalization. Thus,person-years and cases (ie, hospital admissions) fromthis period were not included in the analyses.
Time since enrollment in childcare (regardless oftype) is a time-dependent variable categorized as fol-lows: never in childcare and currently in home care, 0 to5 months in the first enrollment, 6 to 11 months in thefirst enrollment, �12 months in the first enrollment,once in childcare and currently in home care, 0 to 5months in the second enrollment, 6 to 11 months in thesecond enrollment, �12 months in the second enroll-ment, twice in childcare and currently in home care, or�3 times enrolled in childcare. The first category is re-ferred to as home care. Type of (current) childcare is atime-dependent variable categorized as home care,creche, kindergarten, age-integrated facility, or day carehome. In an additional analysis, the group of childrencategorized as “once in childcare and currently in homecare” was categorized as in childcare according to timesince first enrollment to evaluate the potential effect offrail children being moved from childcare to home care.The variables year, season, county of residence, popula-tion per kilometer squared in the residence area, age ofthe child, number of additional children �5 years livingin the household, and type of childcare were created astime-dependent variables. Variables were categorized asfollows: age (quarter-year intervals at ages 0–2 years andhalf-year intervals at ages 3–5 years), gender (boy versusgirl), maternal age when giving birth (�20, 20–24, 25–29, 30–34, or �35 years), type of parenthood at time ofbirth (single versus shared), year (1-year intervals), pop-ulation per kilometers squared in the residence area(�50, 51–500, 501–2000, 2001–4000, or �4000 km2),county (numbers 1–14), season (summer [June to Au-
gust], fall [September to November], winter [Decemberto February], or spring [March to May]), and additionalchildren �5 years living in the home (0, 1, or �2).
By means of quasi-Poisson regression, all of the vari-ables were tested and included as confounders if theychanged the estimated IRRs of time since first enroll-ment presented in Table 1 by 5% or more. Effect mod-ification was evaluated using models with a 2-way in-teraction term between relevant covariates. Estimationwas performed by PROC GENMOD in SAS (SAS Insti-tute Inc, Cary, NC) with Poisson error distribution, loglink, and a dispersion factor estimated from Pearsonstatistics.28 Population-attributable risk for the scenariothat no children attended childcare was estimated as 1 ��(pa/IRRa), with a as age groups 0, 1, 2, 3, 4, 5 years, pa
as the observed proportion of ARI cases in childcare inage group a, and IRRa as the estimated IRR of ARIhospitalization at age a in children in childcare comparedwith children in home care adjusted for age, gender,season, year, mother’s age when giving birth, number ofadditional children �5 years in the household, popula-tion per kilometer squared in the residence area, andtype of parenthood at time of birth.29,30
RESULTSDuring 3 982 925 person-years of follow-up, a total of138 821 inpatient hospitalizations for ARI occurredamong 0- to 5-year-old children. The hospitalizationswere distributed with 46 750 (34%) among children �1year old, 39 186 (28%) among 1-year-olds, 19 179(14%) among 2-year-olds, 14 398 (10%) among 3-year-olds, 11 394 (8%) among 4-year-olds, and 7914 (6%)among 5-year-olds. Overall, 37% of the infections wereLRIs, and 63% were URIs. Among the hospitalized chil-dren, 65% were admitted once, 20% were admitted 2times, and 15% were admitted �3 times. During follow-up, 0.2% of the children died. The proportion of childrenleaving the cohort was 6% at �1 year old, 7% at age 1year, and 7% at 2 years of age.
TABLE 1 IRR and 95% CIs of Hospitalization for ARI in Children Aged 0, 1, 2, and>3 Years, According toTime Since Enrollment Into First and Second Child Care Facility, Respectively
Variable Short(�5 mo)
Medium(6–11 mo)
Long(�12 mo)
Home Care(Ref)
Time since first enrollmentAge 0 y 1.69 (1.63–1.74) 1.60 (1.38–1.86) NE 1Age 1 y 1.47 (1.42–1.52) 1.24 (1.19–1.28) 1.01 (0.95–1.07) 1Age 2 y 1.41 (1.31–1.52) 1.34 (1.25–1.43) 1.02 (0.97–1.06) 1Age �3 y 1.08 (1.01–1.16) 1.18 (1.10–1.27) 1.04 (1.00–1.09) 1
Time since second enrollmentAge 0 y 1.61 (1.40–1.84) NE NE 1Age 1 y 1.40 (1.31–1.49) 1.30 (1.18–1.42) 0.89 (0.68–1.18) 1Age 2 y 1.21 (1.10–1.33) 1.28 (1.16–1.41) 1.02 (0.92–1.12) 1Age �3 y 1.06 (1.00–1.13) 1.02 (0.96–1.09) 0.98 (0.93–1.03) 1
95% CIs are shown in parentheses. Adjusted for gender, age, season, year, mother’s age when giving birth, number of additional children �5years in the household, population per kilometer squared in the residence area, and type of parenthood at time of birth. Ref indicates children inhome care as reference; NE, not estimable because of small numbers.
73
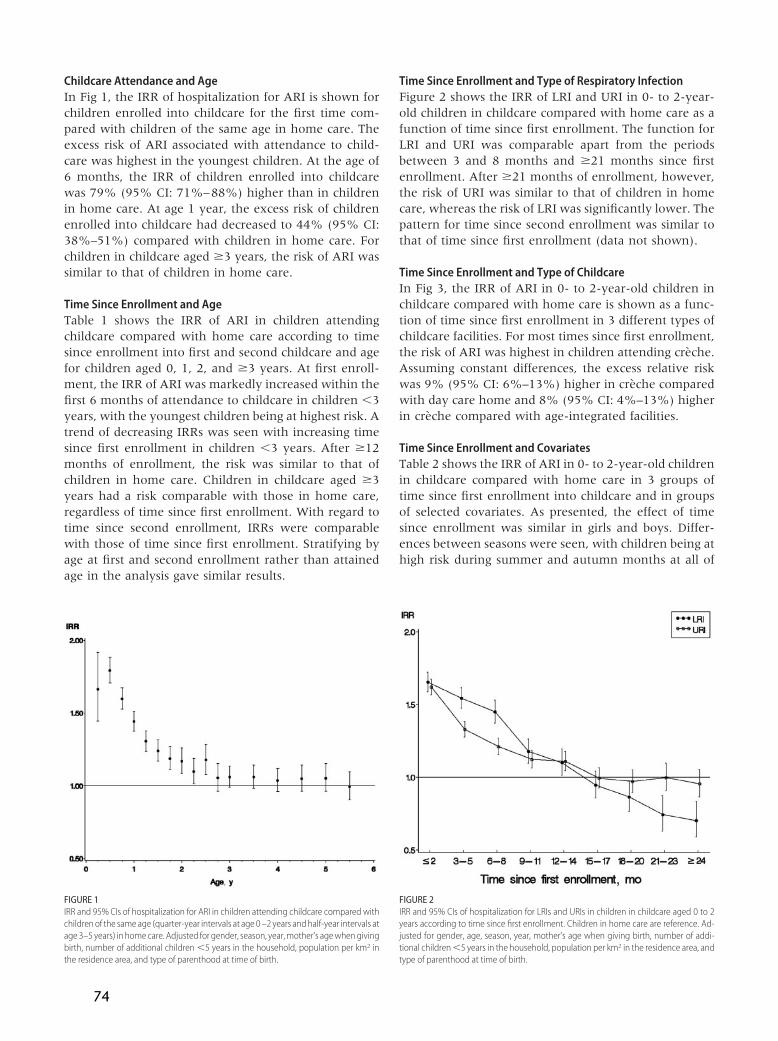
Childcare Attendance and AgeIn Fig 1, the IRR of hospitalization for ARI is shown forchildren enrolled into childcare for the first time com-pared with children of the same age in home care. Theexcess risk of ARI associated with attendance to child-care was highest in the youngest children. At the age of6 months, the IRR of children enrolled into childcarewas 79% (95% CI: 71%–88%) higher than in childrenin home care. At age 1 year, the excess risk of childrenenrolled into childcare had decreased to 44% (95% CI:38%–51%) compared with children in home care. Forchildren in childcare aged �3 years, the risk of ARI wassimilar to that of children in home care.
Time Since Enrollment and AgeTable 1 shows the IRR of ARI in children attendingchildcare compared with home care according to timesince enrollment into first and second childcare and agefor children aged 0, 1, 2, and �3 years. At first enroll-ment, the IRR of ARI was markedly increased within thefirst 6 months of attendance to childcare in children �3years, with the youngest children being at highest risk. Atrend of decreasing IRRs was seen with increasing timesince first enrollment in children �3 years. After �12months of enrollment, the risk was similar to that ofchildren in home care. Children in childcare aged �3years had a risk comparable with those in home care,regardless of time since first enrollment. With regard totime since second enrollment, IRRs were comparablewith those of time since first enrollment. Stratifying byage at first and second enrollment rather than attainedage in the analysis gave similar results.
Time Since Enrollment and Type of Respiratory InfectionFigure 2 shows the IRR of LRI and URI in 0- to 2-year-old children in childcare compared with home care as afunction of time since first enrollment. The function forLRI and URI was comparable apart from the periodsbetween 3 and 8 months and �21 months since firstenrollment. After �21 months of enrollment, however,the risk of URI was similar to that of children in homecare, whereas the risk of LRI was significantly lower. Thepattern for time since second enrollment was similar tothat of time since first enrollment (data not shown).
Time Since Enrollment and Type of ChildcareIn Fig 3, the IRR of ARI in 0- to 2-year-old children inchildcare compared with home care is shown as a func-tion of time since first enrollment in 3 different types ofchildcare facilities. For most times since first enrollment,the risk of ARI was highest in children attending creche.Assuming constant differences, the excess relative riskwas 9% (95% CI: 6%–13%) higher in creche comparedwith day care home and 8% (95% CI: 4%–13%) higherin creche compared with age-integrated facilities.
Time Since Enrollment and CovariatesTable 2 shows the IRR of ARI in 0- to 2-year-old childrenin childcare compared with home care in 3 groups oftime since first enrollment into childcare and in groupsof selected covariates. As presented, the effect of timesince enrollment was similar in girls and boys. Differ-ences between seasons were seen, with children being athigh risk during summer and autumn months at all of
FIGURE 1IRR and 95% CIs of hospitalization for ARI in children attending childcare compared withchildren of the sameage (quarter-year intervals at age 0–2 years andhalf-year intervals atage 3–5 years) in homecare. Adjusted for gender, season, year,mother’s agewhengivingbirth, number of additional children �5 years in the household, population per km2 inthe residence area, and type of parenthood at time of birth.
FIGURE 2IRR and 95% CIs of hospitalization for LRIs and URIs in children in childcare aged 0 to 2years according to time since first enrollment. Children in home care are reference. Ad-justed for gender, age, season, year, mother’s age when giving birth, number of addi-tional children�5 years in the household, population per km2 in the residence area, andtype of parenthood at time of birth.
74
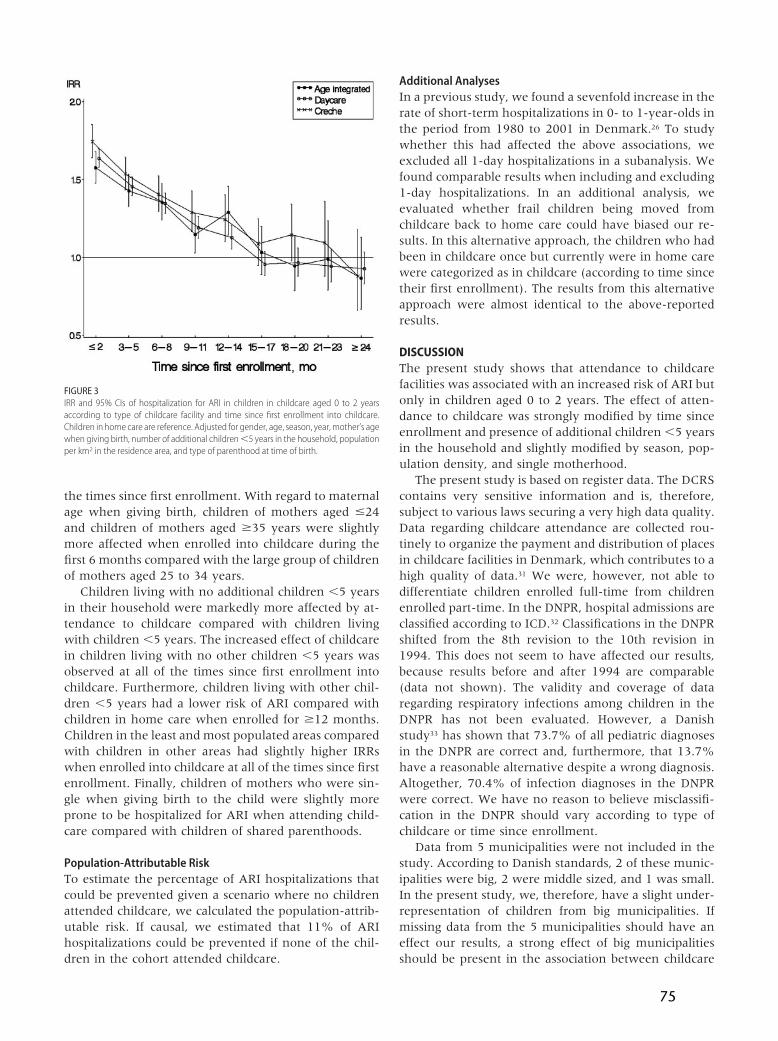
the times since first enrollment. With regard to maternalage when giving birth, children of mothers aged �24and children of mothers aged �35 years were slightlymore affected when enrolled into childcare during thefirst 6 months compared with the large group of childrenof mothers aged 25 to 34 years.
Children living with no additional children �5 yearsin their household were markedly more affected by at-tendance to childcare compared with children livingwith children �5 years. The increased effect of childcarein children living with no other children �5 years wasobserved at all of the times since first enrollment intochildcare. Furthermore, children living with other chil-dren �5 years had a lower risk of ARI compared withchildren in home care when enrolled for �12 months.Children in the least and most populated areas comparedwith children in other areas had slightly higher IRRswhen enrolled into childcare at all of the times since firstenrollment. Finally, children of mothers who were sin-gle when giving birth to the child were slightly moreprone to be hospitalized for ARI when attending child-care compared with children of shared parenthoods.
Population-Attributable RiskTo estimate the percentage of ARI hospitalizations thatcould be prevented given a scenario where no childrenattended childcare, we calculated the population-attrib-utable risk. If causal, we estimated that 11% of ARIhospitalizations could be prevented if none of the chil-dren in the cohort attended childcare.
Additional AnalysesIn a previous study, we found a sevenfold increase in therate of short-term hospitalizations in 0- to 1-year-olds inthe period from 1980 to 2001 in Denmark.26 To studywhether this had affected the above associations, weexcluded all 1-day hospitalizations in a subanalysis. Wefound comparable results when including and excluding1-day hospitalizations. In an additional analysis, weevaluated whether frail children being moved fromchildcare back to home care could have biased our re-sults. In this alternative approach, the children who hadbeen in childcare once but currently were in home carewere categorized as in childcare (according to time sincetheir first enrollment). The results from this alternativeapproach were almost identical to the above-reportedresults.
DISCUSSIONThe present study shows that attendance to childcarefacilities was associated with an increased risk of ARI butonly in children aged 0 to 2 years. The effect of atten-dance to childcare was strongly modified by time sinceenrollment and presence of additional children �5 yearsin the household and slightly modified by season, pop-ulation density, and single motherhood.
The present study is based on register data. The DCRScontains very sensitive information and is, therefore,subject to various laws securing a very high data quality.Data regarding childcare attendance are collected rou-tinely to organize the payment and distribution of placesin childcare facilities in Denmark, which contributes to ahigh quality of data.31 We were, however, not able todifferentiate children enrolled full-time from childrenenrolled part-time. In the DNPR, hospital admissions areclassified according to ICD.32 Classifications in the DNPRshifted from the 8th revision to the 10th revision in1994. This does not seem to have affected our results,because results before and after 1994 are comparable(data not shown). The validity and coverage of dataregarding respiratory infections among children in theDNPR has not been evaluated. However, a Danishstudy33 has shown that 73.7% of all pediatric diagnosesin the DNPR are correct and, furthermore, that 13.7%have a reasonable alternative despite a wrong diagnosis.Altogether, 70.4% of infection diagnoses in the DNPRwere correct. We have no reason to believe misclassifi-cation in the DNPR should vary according to type ofchildcare or time since enrollment.
Data from 5 municipalities were not included in thestudy. According to Danish standards, 2 of these munic-ipalities were big, 2 were middle sized, and 1 was small.In the present study, we, therefore, have a slight under-representation of children from big municipalities. Ifmissing data from the 5 municipalities should have aneffect our results, a strong effect of big municipalitiesshould be present in the association between childcare
FIGURE 3IRR and 95% CIs of hospitalization for ARI in children in childcare aged 0 to 2 yearsaccording to type of childcare facility and time since first enrollment into childcare.Children in home care are reference. Adjusted for gender, age, season, year,mother’s agewhen giving birth, number of additional children�5 years in the household, populationper km2 in the residence area, and type of parenthood at time of birth.
75
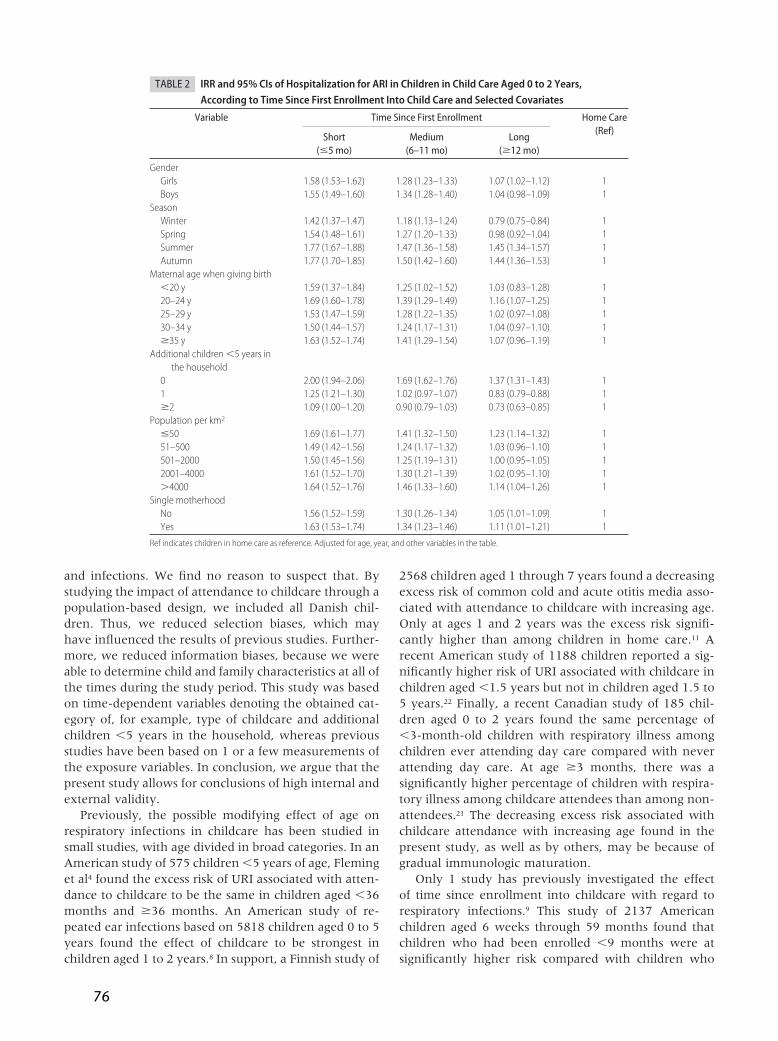
and infections. We find no reason to suspect that. Bystudying the impact of attendance to childcare through apopulation-based design, we included all Danish chil-dren. Thus, we reduced selection biases, which mayhave influenced the results of previous studies. Further-more, we reduced information biases, because we wereable to determine child and family characteristics at all ofthe times during the study period. This study was basedon time-dependent variables denoting the obtained cat-egory of, for example, type of childcare and additionalchildren �5 years in the household, whereas previousstudies have been based on 1 or a few measurements ofthe exposure variables. In conclusion, we argue that thepresent study allows for conclusions of high internal andexternal validity.
Previously, the possible modifying effect of age onrespiratory infections in childcare has been studied insmall studies, with age divided in broad categories. In anAmerican study of 575 children �5 years of age, Fleminget al4 found the excess risk of URI associated with atten-dance to childcare to be the same in children aged �36months and �36 months. An American study of re-peated ear infections based on 5818 children aged 0 to 5years found the effect of childcare to be strongest inchildren aged 1 to 2 years.8 In support, a Finnish study of
2568 children aged 1 through 7 years found a decreasingexcess risk of common cold and acute otitis media asso-ciated with attendance to childcare with increasing age.Only at ages 1 and 2 years was the excess risk signifi-cantly higher than among children in home care.11 Arecent American study of 1188 children reported a sig-nificantly higher risk of URI associated with childcare inchildren aged �1.5 years but not in children aged 1.5 to5 years.22 Finally, a recent Canadian study of 185 chil-dren aged 0 to 2 years found the same percentage of�3-month-old children with respiratory illness amongchildren ever attending day care compared with neverattending day care. At age �3 months, there was asignificantly higher percentage of children with respira-tory illness among childcare attendees than among non-attendees.21 The decreasing excess risk associated withchildcare attendance with increasing age found in thepresent study, as well as by others, may be because ofgradual immunologic maturation.
Only 1 study has previously investigated the effectof time since enrollment into childcare with regard torespiratory infections.9 This study of 2137 Americanchildren aged 6 weeks through 59 months found thatchildren who had been enrolled �9 months were atsignificantly higher risk compared with children who
TABLE 2 IRR and 95% CIs of Hospitalization for ARI in Children in Child Care Aged 0 to 2 Years,According to Time Since First Enrollment Into Child Care and Selected Covariates
Variable Time Since First Enrollment Home Care(Ref)
Short(�5 mo)
Medium(6–11 mo)
Long(�12 mo)
GenderGirls 1.58 (1.53–1.62) 1.28 (1.23–1.33) 1.07 (1.02–1.12) 1Boys 1.55 (1.49–1.60) 1.34 (1.28–1.40) 1.04 (0.98–1.09) 1
SeasonWinter 1.42 (1.37–1.47) 1.18 (1.13–1.24) 0.79 (0.75–0.84) 1Spring 1.54 (1.48–1.61) 1.27 (1.20–1.33) 0.98 (0.92–1.04) 1Summer 1.77 (1.67–1.88) 1.47 (1.36–1.58) 1.45 (1.34–1.57) 1Autumn 1.77 (1.70–1.85) 1.50 (1.42–1.60) 1.44 (1.36–1.53) 1
Maternal age when giving birth�20 y 1.59 (1.37–1.84) 1.25 (1.02–1.52) 1.03 (0.83–1.28) 120–24 y 1.69 (1.60–1.78) 1.39 (1.29–1.49) 1.16 (1.07–1.25) 125–29 y 1.53 (1.47–1.59) 1.28 (1.22–1.35) 1.02 (0.97–1.08) 130–34 y 1.50 (1.44–1.57) 1.24 (1.17–1.31) 1.04 (0.97–1.10) 1�35 y 1.63 (1.52–1.74) 1.41 (1.29–1.54) 1.07 (0.96–1.19) 1
Additional children �5 years inthe household
0 2.00 (1.94–2.06) 1.69 (1.62–1.76) 1.37 (1.31–1.43) 11 1.25 (1.21–1.30) 1.02 (0.97–1.07) 0.83 (0.79–0.88) 1�2 1.09 (1.00–1.20) 0.90 (0.79–1.03) 0.73 (0.63–0.85) 1
Population per km2
�50 1.69 (1.61–1.77) 1.41 (1.32–1.50) 1.23 (1.14–1.32) 151–500 1.49 (1.42–1.56) 1.24 (1.17–1.32) 1.03 (0.96–1.10) 1501–2000 1.50 (1.45–1.56) 1.25 (1.19–1.31) 1.00 (0.95–1.05) 12001–4000 1.61 (1.52–1.70) 1.30 (1.21–1.39) 1.02 (0.95–1.10) 1�4000 1.64 (1.52–1.76) 1.46 (1.33–1.60) 1.14 (1.04–1.26) 1
Single motherhoodNo 1.56 (1.52–1.59) 1.30 (1.26–1.34) 1.05 (1.01–1.09) 1Yes 1.63 (1.53–1.74) 1.34 (1.23–1.46) 1.11 (1.01–1.21) 1
Ref indicates children in home care as reference. Adjusted for age, year, and other variables in the table.
76

had been enrolled �9 months. This was found to asimilar degree in all 3 of the studied age groups (6 weeksto 17 months, 18–35 months, and 36–59 months). Inthe present study, however, we found a short-term in-creased risk when enrolled into childcare only in chil-dren aged 0 to 2 years.
Intriguingly, we observed that enrollment into firstchildcare facility for �12 months was associated with adecreased risk of ARI in children living with no otherchildren �5 years, and enrollment for �18 months wasassociated with a lower risk of LRI. This could reflect aselection effect rather than a biological effect if the chil-dren most prone to respiratory infections were taken outof childcare over time, leaving the healthiest children inchildcare and, thus, giving an artificially low IRR esti-mate for childcare after a long time of enrollment. How-ever, this effect persisted after conducting an additionalanalysis of children aged 0 to 2 years in which childrenwho once were in childcare were considered in child-care irrespective of whether they went back to home,eliminating the potential bias introduced by frail chil-dren being taken out of childcare. Thus, the lower IRRafter a long time of enrollment into childcare is likely toreflect a biological phenomenon. To our knowledge, thepresent study is the first to show that increasing timesince enrollment into first childcare can be associatedwith a protective effect against ARI and LRI in certaingroups.
Regarding the type of childcare facility, we foundattendance in creche to be associated with a slightlyhigher risk of ARI compared with attendance in homeday care. This has been found previously by others andis most often ascribed to crowding in the type of fa-cility.3,4,8,12 Despite the same degree of crowding as increches, we found a slightly lower risk in age-integratedfacilities. This may be caused by the fact that age-inte-grated facilities are a recent phenomenon in Denmarkand that the facilities are, therefore, designed for child-care purposes, whereas older creches are often housed inbuildings made for purposes other than childcare.
By studying time since enrollment in different strataof covariates, we attempted to identify factors that mightmodify the impact of childcare and thereby identify vul-nerable groups. The short-term increased risk of ARI wasmodified by some of the covariates, whereas it was notmodified by others.
We found autumn and summer months to be associ-ated with a higher excess risk of ARI when attendingchildcare compared with during winter months. Thismay be because of the fact that during winter monthsyoung children are generally at a high risk of ARI, andthe effect of childcare becomes less important.
Children from households with no additional chil-dren �5 years of age were found to have a markedlyincreased risk of ARI when enrolled into childcare com-pared with children living with other children �5 years.
We believe that this reflects less exposure to ARIs fromsurroundings before enrollment into childcare. Anotherexplanation may be that women becoming first-timemothers in households with no additional children �5years have not been exposed to infectious diseases to thesame degree as multiparous women and, therefore, havenot delivered the same degree of protective antibodies toher first child.
Children of mothers who were single when givingbirth were more frequently hospitalized for ARIs thanchildren from shared parenthoods (data not shown). This,however, does not explain why children of single motherswere more prone to ARIs than children from shared par-enthoods when enrolled into childcare. We have no ap-parent explanation to this finding.
A recent Danish study34 found the male/female ratioof admissions because of respiratory tract infections inchildren aged 0 to �5 years to be 1.45 (95% CI: 1.42–1.48). In our material, we found similar gender differ-ences (data not shown), but although boys were moreprone to ARI than girls, attendance to childcare had asimilar effect on boys and girls. This is in contrast with aprevious finding by Marbury et al,12 who found childcareattendance to have a more negative impact on girlscompared with boys.
As opposed to most previous studies, the outcome ofthe present study was hospitalizations for ARIs ratherthan self-reported or childcare teacher-reported ARImorbidity. As described, we found results comparablewith those of previous studies regarding well-known riskfactors for ARIs, such as young age, male gender, andday care attendance versus no day care attendance. Thissuggests that the new results presented in the presentarticle are applicable not only to ARI hospitalizations butto nonhospital-demanding ARI morbidity as well. Be-cause it is difficult to differentiate inflammatory frominfectious respiratory diseases using a register-based ma-terial like DNPR with few clinical data, we used a broaddefinition of ARI, including hospitalizations for asth-matic bronchitis and asthma without specification. Asth-matic bronchitis and asthma without specification ac-counted for 0.8% and 8.2% of the total number of ARIhospitalizations, respectively.
In 2002, maternity/paternity leave was extended to atotal of 52 weeks on benefit for parents in Denmark.Thus, it is made possible for parents to keep their child athome for a longer time, thereby delaying enrollmentinto childcare. This is well in line with our findings of themost vulnerable period during the first year of life. Sub-analyses did not indicate that extension of the materni-ty/paternity leave in 2002 affected the percentage ofDanish children attending childcare or the overall in-cidence of ARI. Because most countries do not havematernity/paternity leave as long as in Denmark, a moremodifiable factor might be for parents to enroll theirchildren in day care homes or age-integrated facilities in
77

preference to creches, although only minor differenceswere seen.
In the entire cohort of 0- to 5-year-old children, weestimated that 11% of all of the inpatient ARI hospital-izations were because of attendance to childcare ifcausal. This population attributable risk percent is con-cordant with a previous study of American 0- to 5-year-old children.9
CONCLUSIONSWe found that children between 0 and 2 years had anexcess risk of ARI when attending childcare. The excessrisk of ARI decreased with increasing age. We found therisk of ARI to be highest within the first short period ofenrollment. However, it increased again with a shift to anew childcare facility. Finally, children living with noother children �5 years had an increased risk of ARIwhen attending childcare. Our findings may suggest thatit would be optimal to postpone enrollment into child-care until after 1 year of age.
ACKNOWLEDGMENTSThe present study received support from the HealthInsurance Foundation, the Egmont Foundation, theDanish Graduate School in Public Health Science, Rosa-lie Petersens Fond, Gangstedfonden, and the NationalUnion of Nursery and Childcare Assistance.
REFERENCES1. Anderson LJ, Parker RA, Strikas RA, et al. Day-care center
attendance and hospitalization for lower respiratory tract ill-ness. Pediatrics. 1988;82:300–308
2. Bell DM, Gleiber DW, Mercer AA, et al. Illness associated withchild day care: a study of incidence and cost. Am J Public Health.1989;79:479–484
3. Celedon JC, Litonjua AA, Weiss ST, Gold DR. Day care atten-dance in the first year of life and illnesses of the upper andlower respiratory tract in children with a familial history ofatopy. Pediatrics. 1999;104:495–500
4. Fleming DW, Cochi SL, Hightower AW, Broome CV. Childhoodupper respiratory tract infections: to what degree is incidenceaffected by day-care attendance? Pediatrics. 1987;79:55–60
5. Fonseca W, Kirkwood BR, Barros AJ, et al. Attendance at daycare centers increases the risk of childhood pneumonia amongthe urban poor in Fortaleza, Brazil. Cad Saude Publica. 1996;12:133–140
6. Forssell G, Hakansson A, Mansson NO. Risk factors for respi-ratory tract infections in children aged 2–5 years. Scand J PrimHealth Care. 2001;19;122–125
7. Fuchs SC, Maynart R, Costa LF, Cardozo A, Schierholt R.Duration of day-care attendance and acute respiratory infec-tion. Cad Saude Publica. 1996;12:291–296
8. Hardy AM, Fowler MG. Child care arrangements and repeatedear infections in young children. Am J Public Health. 1993;83:1321–1325
9. Hurwitz ES, Gunn WJ, Pinsky PF, Schonberger LB. Risk ofrespiratory illness associated with day-care attendance: a na-tionwide study. Pediatrics. 1991;87:62–69
10. Koch A, Molbak K, Homoe P, et al. Risk factors for acuterespiratory tract infections in young Greenlandic children.Am J Epidemiol. 2003;158;374–384
11. Louhiala PJ, Jaakkola N, Ruotsalainen R, Jaakkola JJ. Form ofday care and respiratory infections among Finnish children.Am J Public Health. 1995;85:1109–1112
12. Marbury MC, Maldonado G, Waller L. Lower respiratory ill-ness, recurrent wheezing, and day care attendance. Am J RespirCrit Care Med. 1997;155:156–161
13. Nafstad P, Hagen JA, Oie L, Magnus P, Jaakkola JJ. Day carecenters and respiratory health. Pediatrics. 1999;103:753–758
14. Petersson C, Hakansson A. A retrospective study of respiratorytract infections among children in different forms of day care.Scand J Prim Health Care. 1990;8:119–122
15. Stahlberg M.R. The Influence of Form of Day Care on Occurrence ofAcute Respiratory Tract Infections Among Young Children [thesis].Turku, Finland: University of Turku; 1980
16. Strangert K. Respiratory illness in preschool children withdifferent forms of day care. Pediatrics. 1976;57:191–196
17. Uldall P. Common Morbidity in Infants and Young Children - Oc-currence and Social Consequences [thesis]. Copenhagen, Denmark:University of Copenhagen; 1986
18. Woodward A, Douglas RM, Graham NM, Miles H. Acute re-spiratory illness in Adelaide children–the influence of childcare. Med J Aust. 1991;154:805–808
19. Zielhuis GA, Heuvelmans-Heinen EW, Rach GH, van den BP.Environmental risk factors for otitis media with effusion inpreschool children. Scand J Prim Health Care. 1989;7:33–38
20. Koopman LP, Smit HA, Heijnen ML, et al. Respiratory infec-tions in infants: interaction of parental allergy, child care, andsiblings– The PIAMA study. Pediatrics. 2001;108;943–948
21. Dales RE, Cakmak S, Brand K, Judek S. Respiratory illness inchildren attending daycare. Pediatr Pulmonol. 2004;38;64–69
22. Lu N, Samuels ME, Shi L, Baker SL, Glover SH, Sanders JM.Child day care risks of common infectious diseases revisited.Child Care Health Dev. 2004;30;361–368
23. Malig C. The Civil Registration System in Denmark; IIVRS Techni-cal Paper. Bethesda, MD: International Institute for Vital Reg-istration and Statistics; 1996;66:1–6
24. National Board of Health. Infectious Diseases in Children: Guide-lines for Daycare Facilities, Schools and Parents. Copenhagen,Denmark: National Board of Health; 1996
25. Andersen TF, Madsen M, Jorgensen J, Mellemkjoer L, Olsen JH.The Danish National Hospital Register. A valuable source of datafor modern health sciences. Dan Med Bull. 1999;46:263–268
26. Kamper-Jorgensen M, Wohlfahrt J, Simonsen J, Thrane N,Benn CS. Temporal trend in paediatric infections in Denmark.Arch Dis Child. 2006;91;401–404
27. McCullach P, Nelder J. Generalized Linear Models. London,United Kingdom: Chapman & Hall; 1989
28. SAS Institute Inc. SAS/STAT software release 8.2 [computerprogram]. Cary, NC: SAS Institute Inc; 2001
29. Bruzzi P, Green SB, Byar DP, Brinton LA, Schairer C. Estimat-ing the population attributable risk for multiple risk factorsusing case-control data. Am J Epidemiol. 1985;122:904–914
30. Benichou J. Attributable risk. In: Armitage P, Colton T, eds.Encyclopedia of Biostatistics. 2nd ed. Chichester, England: JohnWiley & Sons; 2005:255
31. Thrane N. Prescription of systemic antibiotics for Danish chil-dren [thesis]. Aarhus, Denmark: University of Aarhus; 2000
32. World Health Organization Collaborating Centers. Interna-tional classification of diseases. Epidemiol Bull. 1998;19:7–11
33. Mosbech J, Jorgensen J, Madsen M, Rostgaard K, Thornberg K,Poulsen TD. The national patient registry. Evaluation of dataquality. Ugeskr Laeger. 1995;157:3741–3745
34. Jensen-Fangel S, Mohey R, Johnsen SP, Andersen PL, So-rensen HT, Ostergaard L. Gender differences in hospitalizationrates for respiratory tract infections in Danish youth. ScandJ Infect Dis. 2004;36;31–36
78
Study IV
79
80
Determinants of clustering of acute respiratory infection hospitalizations in
childcare facilities
Mads Kamper-Jørgensen1 MSc, Christine Stabell Benn2 PhD, Jacob Simonsen1 MSc,
Nana Thrane3 PhD, Jan Wohlfahrt1 DMSc
1Department of Epidemiology Research, Statens Serum Institut
2Bandim Health Project, Statens Serum Institut
3Department of Pediatrics, Herning Central Hospital, Denmark
Word count, text only: 2,886
Word count, abstract: 233
Correspondence
Mads Kamper-Jørgensen, Department of Epidemiology Research,
Statens Serum Institut, Artillerivej 5, 2300 Copenhagen S.
E-mail: [email protected], Telephone: +45 32688339
Project support
The present study received support from the Health Insurance Foundation, the
Egmont Foundation, the Danish Graduate School in Public Health Science, Rosalie
Petersens Fond, Gangstedfonden, Aase og Ejnar Danielsens Fond and the National
Union of Nursery and Childcare Assistance
81
Abstract
Context
Clustering of acute respiratory infection (ARI) childcare facilities can be character-
ized by the transient change in hospitalization rate of ARI in children attending a
facility with a recent hospitalization for ARI
Objective
To estimate how risk of ARI hospitalization in children attending a childcare facility
with a recently (within 1 month) hospitalized child is modified by sex, age and
other characteristics
Design, setting and participants
Population-based prospective cohort study of Danish 0-5-year-old children attend-
ing a childcare facility from 1989 to 2004. Information was collected from Danish
registers
Main outcome measures
Incidence rate ratios (IRRs) of in-patient hospitalization for ARI
82
Results
During 1,777,999 years of follow-up 42,681 hospitalizations for ARI occurred, of
which 362 (1%) occurred within 1 month after another child was hospitalized for
ARI in the facility. Children attending a facility with a recent ARI hospitalization had
an increased risk of 42% (95% CI 27%;60%) compared with other children. The
increased risk was higher in 0-2-year-old children than in 3-5-year-old children
(55% vs. 17%, p=0.02) and if the latest hospitalized child was 0-2 years rather than
3-5 years (52% vs. 19%, p=0.04) The increased risk was similar in boys and girls,
but was higher if the latest hospitalized child was a boy rather than a girl (52% vs.
13%, p=0.02).
Conclusion
Clusters of ARI hospitalizations in childcare facilities involve 0-2-year-olds and boys
as first hospitalized child relatively more often than other children
83
Introduction
Childcare facilities are considered a risk factor for acquiring acute respiratory infec-
tion (ARI)1-6. Due to the infectious nature of ARI, disease within a childcare facility
will tend to cluster in time. Although this is common knowledge, previous studies
have not tried to investigate what characterizes clustering of ARI in childcare facili-
ties. One possible approach is to analyze the transient change in hospitalization
rate of ARI in children attending a facility with a recent hospitalization for ARI. Such
an approach is complicated by the need of precise information on who is attending
which childcare facility at any time during follow-up. However, this is now possible
in Denmark on a population-based level with the establishment of the Childcare
Database7 supplemented with information on child and family characteristics and
ARI hospitalizations from national registries. In the present study we used this new
nation-wide material to prospective follow up 0-5 year-old children from 1989 to
2004 in order to investigate what characterizes the clustering of ARI in childcare fa-
cilities.
84
Material
The present study was based on the Childcare Database, which is described in de-
tail elsewhere7. A brief description of the study cohort, the exposure and the out-
come variables is given below.
Study cohort
The study cohort consisted of all Danish children born in the period from 1 January
1989 to 17 November 2004 in a municipality which registered childcare atten-
dance. Children were identified using the Danish Civil Registration System
(DCRS)8,9, in which all individuals alive and living in Denmark since 1 April 1968 are
assigned a unique person identification number. This unique identification number
is recorded in several other Danish registers, making linkage possible. From the
DCRS, information was retrieved regarding the fixed variables date of birth of the
child, sex of the child and maternal age at birth of the child. Throughout follow-
up, information was furthermore obtained on the time-dependent variables postal
address, migration and death of the child as well as number of children younger
than 5 years in the household.
Exposure
The information from the DCRS was linked with the Childcare Database, which is a
Danish population-based register of enrollment into childcare facilities. In this regis-
ter all municipal childcare attendance is covered in 266 of the 271 Danish munici-
palities. In Denmark the vast majority of preschool children attend municipal child-
care. Daycare homes are targeted for children aged 0-3 years and run by a child
minder looking after 1-5 children. Crèche refers to facilities for children up to 3
years of age and with an average of 41 children enrolled. Age-integrated facilities
are for children aged 0 to 6 years with a mean of 73 children enrolled, and kinder-
85
gartens are facilities enrolling on average 56 children aged 3 to 6 years7. For each
enrollment, date of enrollment and date of withdrawal was retrieved. Daycare
homes were excluded since it was not possible to differentiate between different
daycare homes within a municipality, because all daycare homes were registered
using the same code. Other types of childcare facilities were allocated a unique
code within each municipality and could thus be differentiated.
Children from the 266 eligible municipalities who did not figure in the
childcare attendance register were considered in homecare. Registration of enroll-
ment into childcare did not start on the same date in all municipalities. Therefore
the study period differed between municipalities. The first municipalities registered
enrollment from 1 January 1989, whereas the last municipality started registering
from 1 January 2004.
Outcome
The outcome of the study was defined as in-patient admissions to hospital for ARI
as main condition. Hospitalization diagnoses obtained from the Danish National
Patient Registry (DNPR)10 were classified according to the International Classifica-
tion of Diseases (ICD) versions 8 and 1011. In the period from 1989 to 1993 the fol-
lowing ICD-8 diagnoses were used to define ARI hospitalizations: 032, 033, 075,
381-383, 460-466, 470-486, 490, 500, 501, 503, 510, 513 whereas the following
ICD-10 diagnoses were used to define ARI hospitalizations in the period from 1994
to 2004 : A36, A37, B27, H65-H67, H70, J00-J06, J10-J22, J32, J35, J36, J45, J85,
J86.
86
Methods
Risk of hospitalization for ARI was evaluated by incidence rate ratios (IRRs) with ac-
companying 95% confidence intervals (CIs). IRRs and CIs were estimated using
multiple log-linear quasi Poisson regression of the number of ARI hospitalizations
with the logarithm of person-years at risk as offset. Quasi Poisson regression models
were used to take into account the over-dispersion that potentially could be in-
duced by dependence of events within the same person, families or childcare facili-
ties. The quasi Poisson regression model is based on a Poisson quasi-likelihood
where the variance is allowed to be the mean multiplied by an over-dispersion fac-
tor12. IRR-estimates based on the quasi Poisson regression model are the same as in
the traditional Poisson regression model but with slightly widened CIs. Estimation
was performed using PROC GENMOD in SAS with Poisson error distribution, log
link and a dispersion factor estimated from Pearson statistics13.
Person-years at risk were calculated from the date of enrollment into a
childcare facility until the first of the following events: date of withdrawal, emigra-
tion, moving to an ineligible municipality, death, sixth birthday or end of follow-
up. Each admission to hospital of the same child during the follow-up period was
counted as a new hospitalization. However, children were not considered at risk
during the fourteen days following a hospitalization since hospitalizations in this
period could be related to the preceding hospitalization. Thus, person-years and
hospitalizations in this period were excluded from the analyses. Person-years and
ARI hospitalizations occurring while the child lived in a municipality which did not
register childcare, or while the child was enrolled in a daycare home, were ex-
cluded from the analyses.
We determined time since latest hospitalized child in the childcare facility
as a time-dependent variable. This implies that with every new hospitalization in
the childcare facility, the date from which time since latest ARI hospitalization in
87
the childcare facility was counted was reset. The latest hospitalized child in the
childcare facility could not be the child itself. Time since latest ARI hospitalization in
the childcare facility was categorized as <1 month, 1-<2 months, 2-<6 months, 6–
<12 months, ≥12 months or no previous hospitalization. The sex (boy or girl) and
age (one-year age groups at age 0 through 5) of the latest hospitalized child was
determined, also as time-dependent variables. Furthermore current type of child-
care attended (crèche, kindergarten or age-integrated facility), time since first en-
rollment into childcare (3-month intervals), age (quarter-year intervals at age 0
through 2 and half-year intervals at age 3 through 5), period (one-year intervals
from 1989 to 2004), season (one-month intervals) and number of additional chil-
dren younger than 5 years living in the household (0, 1 or ≥2) were created as
time-dependent variables. Sex (boy or girl), maternal age when giving birth (5-year
intervals) and type of parenthood at time of birth (single or shared) were created as
fixed variables.
All covariates were tested and included in the quasi Poisson regression
model as confounders if they changed any of the estimated IRRs of time since latest
hospitalized child in the childcare facility, shown in Figure 1, by 5% or more. In the
analyses presented in Figure 1, the no previous hospitalization category was com-
bined with the ≥12 month-group and used as reference group. Estimates of the
relatively higher rate of ARI in facilities with a recent hospitalization for ARI were
denoted short-term excess risk. Short-term excess risk represents the estimated ra-
tio between the IRR-estimate for children attending a childcare facility in which an-
other child had been hospitalized for ARI within the latest month and the IRR-
estimate for children attending a childcare facility in which no child had been hos-
pitalized for ARI within the latest month. The ratio and its 95% confidence interval
were estimated in the regression model and for convenience the ratio was sub-
tracted by one to achieve percentages. For two- and three-way interactions p-
88
values based on likelihood ratio tests are presented. P-values for three-way interac-
tions in Table 3 were calculated in models including the underlying two-way inter-
actions.
89
Results
During 1,777,999 years of follow-up a total of 42,681 hospitalizations for ARI oc-
curred, corresponding to an overall incidence rate of 24.0 per 1,000 risk years
among 0-5-year-old Danish children in childcare. The following variables were in-
cluded in the models as confounders: age, sex, type of childcare facility, time since
enrollment and season.
Table 1 presents ARI hospitalizations according to time since latest
hospitalization for ARI in the childcare facility and covariates. One percent of hospi-
talizations (n=362) occurred in children attending a childcare facility in which an-
other child had been hospitalized for ARI within the latest month (denoted ‘recent’
in the following). The distribution of age and sex of the latest hospitalized child in
the childcare facility is shown only for the 4,769 children attending a facility in
which another child was previously hospitalized for ARI.
As presented in Figure 1, in 0-2-year-olds the IRR was 62% (95% CI
40%;88%) higher if attending a facility with a recent ARI hospitalization compared
with facilities where no children had been hospitalized for ARI within the latest 12
months. In 3-5-year-olds, the corresponding increase was 21% (95%CI 3%;43%).
In 0-2-year-olds the initial excess risk following a recent ARI was followed by a de-
creasing risk with increasing time since latest hospitalized child. In 3-5-year-olds no
effect was seen after the initial elevated risk following a recent ARI hospitalization.
In Table 2, time since latest child hospitalized for ARI was dichoto-
mized and IRRs are presented according to covariates. The short-term excess risk,
denoting the stratum-specific excess risk of ARI hospitalization associated with at-
tendance to a facility in which another child was recently hospitalized for ARI, was
similar in boys and girls (p=0.27), although boys generally were at a higher risk
than girls. If the latest hospitalized child was a boy, however, the short-term excess
risk was 52% (95% CI 32%;75%) compared with 13% (95% CI -8%;40%) if the
90
latest hospitalized child was a girl. A more pronounced short-term excess risk when
attending a facility with a recent ARI was furthermore seen if the child’s own age
was 0-2 years vs. 3-5 years (p=0.02), if age of the latest hospitalized child was 0-2
years rather than 3-5 years (p=0.04) and in age-integrated facilities compared with
crèches and kindergartens (p=0.03). Finally, attendance to a facility with a recent
ARI increased the IRR by 95% (95%CI 51%;151%) in children from single parent-
hoods compared with 34% (95% CI 19%;51%) in children from shared parent-
hoods.
In Table 3 the short-term excess risk associated with attendance to a
facility with a recent ARI hospitalization compared with attendance to a facility
without a recent ARI hospitalization is presented for all combinations of own sex,
own age, sex of latest hospitalized child and age of latest hospitalized child. There
was no indication that sex or age of the latest hospitalized child modified the ef-
fects of each other or the effect of the child’s own sex or age when adjusted for the
effects presented in Table 2.
Had children in daycare homes not been excluded and had children
in homecare been included, like in a previous study3, the overall incidence of ARI
hospitalizations would have been 34.9 rather than 24.0 per 1,000 person-years due
to the high incidence of ARI in toddlers. The overall incidence of 24.0 per 1,000
person-years corresponds to 1.2 ARI hospitalizations over a one-year period in a fic-
titious childcare facility with 50 children aged 0 to 5 years enrolled.
91
Discussion
In the present study we characterized clustering of acute respiratory infection (ARI)
in childcare facilities by the transient change in hospitalization rate of ARI in chil-
dren attending a facility with a recent hospitalization for ARI. We estimated a 42%
excess risk of being hospitalized for ARI in childcare facilities with a recent hospitali-
zation for ARI. We observed an especially high short-term excess risk, if the child
was 0-2 years old, if the latest hospitalized child was 0-2 years old, if the latest hos-
pitalized child was a boy, if attending an age-integrated facility, and if the child’s
mother was single when giving birth. Thus, children with these characteristics are
relatively more often involved in clusters of ARI in childcare facilities.
The observed clusters can be interpreted in different ways. A cluster of ARI can be
interpreted as indication of transmission of ARI within the childcare facilities. The
rapidly decreasing risk of hospitalization for ARI associated with increasing time
since latest ARI hospitalization supports such an interpretation. However, it is im-
portant to bear in mind that transmission may very well have occurred outside of
the childcare facility. Thus, only in some instances, is the latest hospitalized child in
the childcare facility likely to be the one transmitting the ARI to the subsequently
hospitalized child. One interpretation is that clusters of ARI reflect increased aware-
ness of ARI among parents of children in facilities in which a child was recently
hospitalized for ARI. Hospitalization practices in Denmark changed during the
study period14, and it is not unthinkable that defensive medicine is practiced more
often if doctors are consulted by worried parents. Nevertheless, the fact that char-
acteristics of the first hospitalized child affect the risk of the other children in the
facility supports that also transmission within the childcare facility plays an impor-
tant role in the occurrence of the observed clusters.
92
Clustering of ARI hospitalizations in childcare facilities did relatively
more often involve 0-2-year-olds than 3-5 year-olds. This was observed in two
ways. Firstly, we observed an especially high excess risk in facilities with a recent
hospitalization in 0-2-year-olds compared with older children, presumably due to
an immature immune system. Secondly, irrespective of the child’s own age, at-
tending a facility where the latest hospitalized child was 0-2 years old inferred a
higher short-term excess risk than if the latest hospitalized child was older. The lat-
ter finding suggests that 0-2-year-olds transmit ARI easier than older children. Al-
though boys were generally more prone to ARI than girls, the short-term excess risk
associated with attendance to a facility with a recent ARI was found to be similar in
boys and girls. If attending a facility where the latest hospitalized child was a boy,
however, the short-term excess risk was significantly higher than if it was a girl.
This most likely reflects that boys show more active play than girls15 which may en-
tail a higher risk of contracting as well as transmitting infection. Transmission of
measles and polio from the opposite sex has previously been shown to increase the
severity of the infection16,17. However, in our study of ARIs severe enough to result
in hospitalization we observed no special increased short-term excess if the latest
hospitalized child was of the opposite sex.
Clusters were relatively more often observed in children in age-
integrated facilities compared with in other children. Age-integrated facilities are
characterized by attendance of many children both below and above three years of
age. However, the relatively higher occurrence of clusters in age-integrated facili-
ties cannot be attributed to cross-age infection between 0-2-year-olds and older
children, since the higher excess risk associated with young age was not modified
by age of the latest hospitalized child.
Besides generally being at a higher risk of ARI, children of mothers
who where single when giving birth were relatively more often involved in clusters
93
than children from shared parenthoods. Mothers who were single when giving
birth are likely to be from a lower socioeconomic position than cohabiting par-
ents18. The fact that children born to single mothers were more affected by child-
care attendance suggests that this small group of children (12%) may be more
susceptible to infections than other children, maybe due to shorter duration of
breast feeding19, poorer housing conditions18 or domestic smoking20.
The estimated increased risk of 42% stresses the importance of fol-
lowing guidelines for exclusion of children from childcare during infectious periods.
In Denmark such guidelines are given by the National Board of Health21. A recent
US study showed that even though familiarity with such guidelines is generally low,
childcare providers and parents correctly exclude 65%-98% of children requiring
exclusion22.
The outcome, namely hospitalizations for ARI, is classified according to the Interna-
tional Classification of Diseases11 in the DNPR. Classifications shifted from ICD-8 to
ICD-10 in 1994, leaving out the ICD-9 version. We found similar results before and
after 1994 (data not shown). The validity and coverage of data regarding ARI
among children in the DNPR has not been evaluated. However, according to a
study using DNPR data23 73.7% of all pediatric diagnoses are correct, and another
13.7% have a reasonable alternative in spite of a wrong diagnosis. In the present
study, we do not distinguish between different types of infections e.g. according to
etiology or site of infection, why we do not believe misclassification of the ICD-
code to be a concern. If present, we have no reason to believe that the misclassifi-
cation varies according to time since latest ARI in the childcare facility.
94
Conclusively, a recently hospitalized child significantly increased the risk of hospi-
talization for ARI in other children attending the childcare facility. This clustering of
ARI hospitalizations in childcare facilities involve 0-2-year-olds and boys as first hos-
pitalized child relatively more often than other children.
Likewise, children in age-integrated facilities and children whose mother was single
when giving birth were also relatively more often involved in clusters when com-
paring with other children.
95
References
(1) Celedon JC, Litonjua AA, Weiss ST, Gold DR. Day care attendance in the first year of life and illnesses of the upper and lower respiratory tract in children with a familial history of atopy. Pediatrics. 1999;104:495-500.
(2) Hurwitz ES, Gunn WJ, Pinsky PF, Schonberger LB. Risk of respiratory illness associated with day-care attendance: a nationwide study. Pediatrics. 1991;87:62-69.
(3) Kamper-Jorgensen M, Wohlfahrt J, Simonsen J, Grønbæk M, Benn CS. Population-based study of the impact of childcare attendance on hospitali-zations for acute respiratory infections. Pediatrics. 2006;118:1439-1446.
(4) Louhiala PJ, Jaakkola N, Ruotsalainen R, Jaakkola JJ. Form of day care and respiratory infections among Finnish children. Am J Public Health. 1995;85:1109-1112.
(5) Nafstad P, Hagen JA, Oie L, Magnus P, Jaakkola JJ. Day care centers and res-piratory health. Pediatrics. 1999;103:753-758.
(6) Woodward A, Douglas RM, Graham NM, Miles H. Acute respiratory illness in Adelaide children--the influence of child care. Med J Aust. 1991;154:805-808.
(7) Kamper-Jorgensen M, Wohlfahrt J, Simonsen J, Benn CS. The Childcare Da-tabase: a valuable register linkage. Scand J Public Health. In press.
(8) Malig C. The Civil Registration System in Denmark. Bethesda, MD: Interna-tional Institute for Vital Registration and Statistics. IIVRS Technical paper. 1996;66:1-6.
(9) Pedersen CB, Gotzsche H, Moller JO, Mortensen PB. The Danish Civil Regis-tration System. A cohort of eight million persons. Dan Med Bull. 2006;53:441-449.
(10) Andersen TF, Madsen M, Jorgensen J, Mellemkjoer L, Olsen JH. The Danish National Hospital Register. A valuable source of data for modern health sci-ences. Dan Med Bull. 1999;46:263-268.
(11) International classification of diseases. WHO Collaborating Centers. Epide-miol Bull. 1998;19:7-11.
(12) McCullach P, Nelder J. Generalized Linear Models. London: Chapman & Hall; 1989.
(13) SAS Institute Inc. SAS/STAT software release 8.2. Cary, NC: SAS Institute Inc. [ 2001.
(14) Kamper-Jorgensen M, Wohlfahrt J, Simonsen J, Thrane N, Benn CS. Tempo-ral trend in paediatric infections in Denmark. Arch Dis Child. 2006;91:401-404.
(15) Smith PK, Daglish L. Sex differences in parent and infant behavior in the home. Child Dev. 1977;48:1250-1254.
96
(16) Aaby P. Influence of cross-sex transmission on measles mortality in rural Senegal. Lancet. 1992;340:388-391.
(17) Nielsen NM, Wohlfahrt J, Melbye M, Molbak K, Aaby P. Does cross-sex transmission increase the severity of polio infection? A study of multiple family cases. Scand J Infect Dis. 2002;34:273-277.
(18) Christensen, E. [7 years of child life - welfare, health and well-being in chil-dren born in 1995]. 04:13. 2004. The Danish National Institute of Social Research. Report 2004.
(19) Benn CS, Wohlfahrt J, Aaby P et al. Breastfeeding and risk of atopic dermati-tis, by parental history of allergy, during the first 18 months of life. Am J Epidemiol. 2004;160:217-223.
(20) Ekholm O, Kjøller M, Davidsen M et al. Danish Health and Morbidity Survey 2005 .... & trends since 1987. Copenhagen: National Institute of Public Health; 2006.
(21) National Board of Health. [Infectious diseases in children, guidelines for daycare facilities, schools and parents]. Report 1996.
(22) Copeland KA, Harris EN, Wang NY, Cheng TL. Compliance with American Academy of Pediatrics and American Public Health Association illness exclu-sion guidelines for child care centers in Maryland: who follows them and when? Pediatrics. 2006;118:e1369-e1380.
(23) Mosbech J, Jorgensen J, Madsen M, Rostgaard K, Thornberg K, Poulsen TD. [The national patient registry. Evaluation of data quality]. Ugeskr Laeger. 1995;157:3741-3745.
97
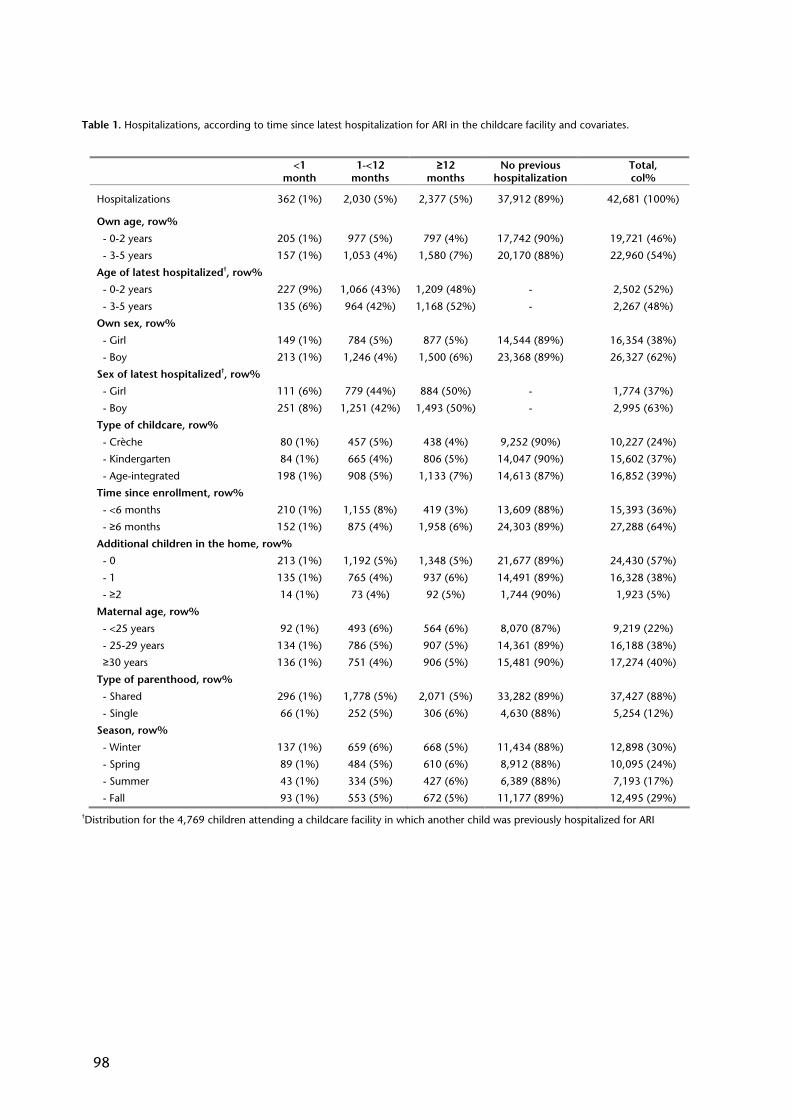
Table 1. Hospitalizations, according to time since latest hospitalization for ARI in the childcare facility and covariates.
†Distribution for the 4,769 children attending a childcare facility in which another child was previously hospitalized for ARI
<1 month
1-<12 months
≥12 months
No previous hospitalization
Total, col%
Hospitalizations 362 (1%) 2,030 (5%) 2,377 (5%) 37,912 (89%)
42,681 (100%)
Own age, row%
- 0-2 years 205 (1%) 977 (5%) 797 (4%) 17,742 (90%) 19,721 (46%)
- 3-5 years 157 (1%) 1,053 (4%) 1,580 (7%) 20,170 (88%) 22,960 (54%)
Age of latest hospitalized†, row%
- 0-2 years 227 (9%) 1,066 (43%) 1,209 (48%) - 2,502 (52%)
- 3-5 years 135 (6%) 964 (42%) 1,168 (52%) - 2,267 (48%)
Own sex, row%
- Girl 149 (1%) 784 (5%) 877 (5%) 14,544 (89%) 16,354 (38%)
- Boy 213 (1%) 1,246 (4%) 1,500 (6%) 23,368 (89%) 26,327 (62%)
Sex of latest hospitalized†, row%
- Girl 111 (6%) 779 (44%) 884 (50%) - 1,774 (37%)
- Boy 251 (8%) 1,251 (42%) 1,493 (50%) - 2,995 (63%)
Type of childcare, row%
- Crèche 80 (1%) 457 (5%) 438 (4%) 9,252 (90%) 10,227 (24%)
- Kindergarten 84 (1%) 665 (4%) 806 (5%) 14,047 (90%) 15,602 (37%)
- Age-integrated 198 (1%) 908 (5%) 1,133 (7%) 14,613 (87%) 16,852 (39%)
Time since enrollment, row%
- <6 months 210 (1%) 1,155 (8%) 419 (3%) 13,609 (88%) 15,393 (36%)
- ≥6 months 152 (1%) 875 (4%) 1,958 (6%) 24,303 (89%) 27,288 (64%)
Additional children in the home, row%
- 0 213 (1%) 1,192 (5%) 1,348 (5%) 21,677 (89%) 24,430 (57%)
- 1 135 (1%) 765 (4%) 937 (6%) 14,491 (89%) 16,328 (38%)
- ≥2 14 (1%) 73 (4%) 92 (5%) 1,744 (90%) 1,923 (5%)
Maternal age, row%
- <25 years 92 (1%) 493 (6%) 564 (6%) 8,070 (87%) 9,219 (22%)
- 25-29 years 134 (1%) 786 (5%) 907 (5%) 14,361 (89%) 16,188 (38%)
≥30 years 136 (1%) 751 (4%) 906 (5%) 15,481 (90%) 17,274 (40%)
Type of parenthood, row%
- Shared 296 (1%) 1,778 (5%) 2,071 (5%) 33,282 (89%) 37,427 (88%)
- Single 66 (1%) 252 (5%) 306 (6%) 4,630 (88%) 5,254 (12%)
Season, row%
- Winter 137 (1%) 659 (6%) 668 (5%) 11,434 (88%) 12,898 (30%)
- Spring 89 (1%) 484 (5%) 610 (6%) 8,912 (88%) 10,095 (24%)
- Summer 43 (1%) 334 (5%) 427 (6%) 6,389 (88%) 7,193 (17%)
- Fall 93 (1%) 553 (5%) 672 (5%) 11,177 (89%) 12,495 (29%)
98
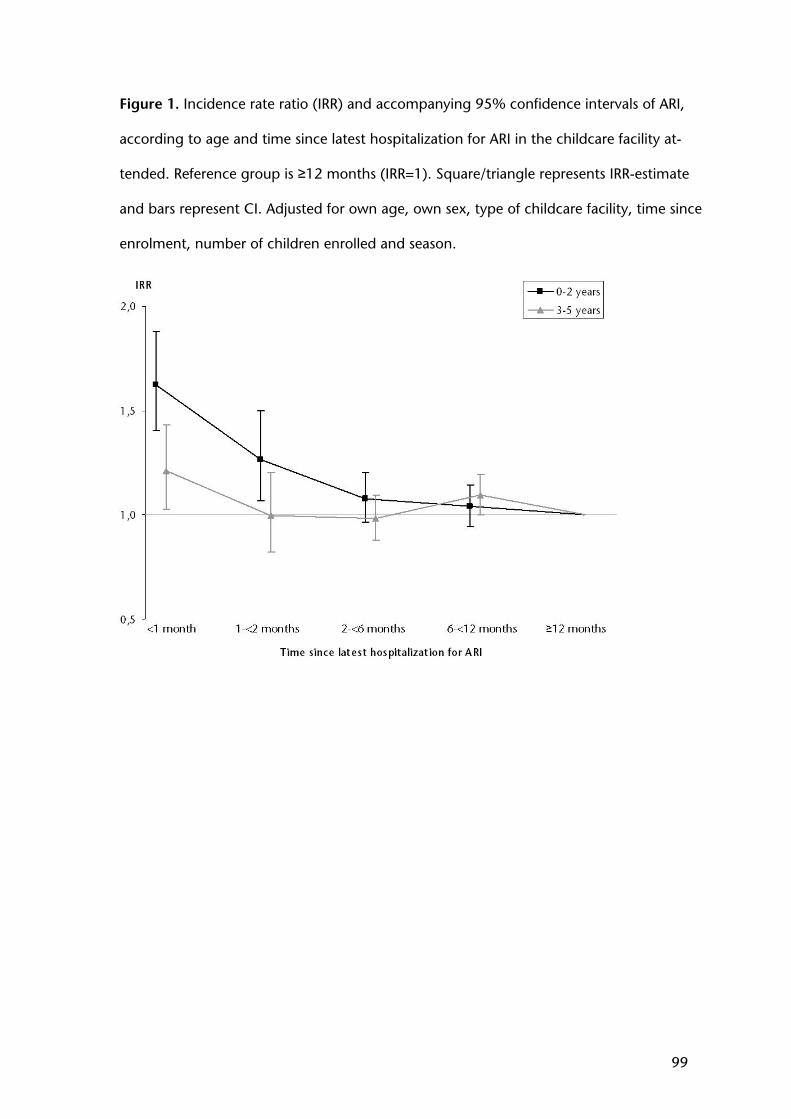
Figure 1. Incidence rate ratio (IRR) and accompanying 95% confidence intervals of ARI,
according to age and time since latest hospitalization for ARI in the childcare facility at-
tended. Reference group is ≥12 months (IRR=1). Square/triangle represents IRR-estimate
and bars represent CI. Adjusted for own age, own sex, type of childcare facility, time since
enrolment, number of children enrolled and season.
99
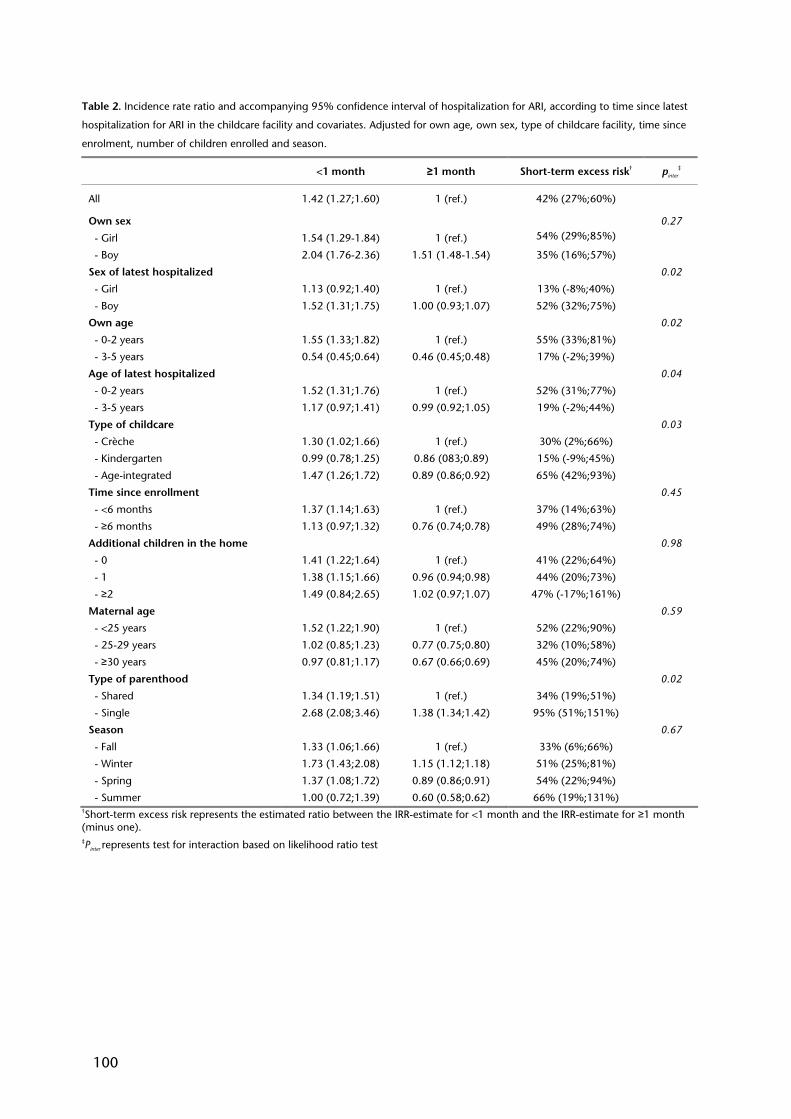
Table 2. Incidence rate ratio and accompanying 95% confidence interval of hospitalization for ARI, according to time since latest
hospitalization for ARI in the childcare facility and covariates. Adjusted for own age, own sex, type of childcare facility, time since
enrolment, number of children enrolled and season.
†Short-term excess risk represents the estimated ratio between the IRR-estimate for <1 month and the IRR-estimate for ≥1 month (minus one). ‡Pinter represents test for interaction based on likelihood ratio test
<1 month ≥1 month Short-term excess risk† pinter
‡
All 1.42 (1.27;1.60) 1 (ref.) 42% (27%;60%)
Own sex 0.27
- Girl 1.54 (1.29-1.84) 1 (ref.) 54% (29%;85%)
- Boy 2.04 (1.76-2.36) 1.51 (1.48-1.54) 35% (16%;57%)
Sex of latest hospitalized 0.02
- Girl 1.13 (0.92;1.40) 1 (ref.) 13% (-8%;40%)
- Boy 1.52 (1.31;1.75) 1.00 (0.93;1.07) 52% (32%;75%)
Own age 0.02
- 0-2 years 1.55 (1.33;1.82) 1 (ref.) 55% (33%;81%)
- 3-5 years 0.54 (0.45;0.64) 0.46 (0.45;0.48) 17% (-2%;39%)
Age of latest hospitalized 0.04
- 0-2 years 1.52 (1.31;1.76) 1 (ref.) 52% (31%;77%)
- 3-5 years 1.17 (0.97;1.41) 0.99 (0.92;1.05) 19% (-2%;44%)
Type of childcare 0.03
- Crèche 1.30 (1.02;1.66) 1 (ref.) 30% (2%;66%)
- Kindergarten 0.99 (0.78;1.25) 0.86 (083;0.89) 15% (-9%;45%)
- Age-integrated 1.47 (1.26;1.72) 0.89 (0.86;0.92) 65% (42%;93%)
Time since enrollment 0.45
- <6 months 1.37 (1.14;1.63) 1 (ref.) 37% (14%;63%)
- ≥6 months 1.13 (0.97;1.32) 0.76 (0.74;0.78) 49% (28%;74%)
Additional children in the home 0.98
- 0 1.41 (1.22;1.64) 1 (ref.) 41% (22%;64%)
- 1 1.38 (1.15;1.66) 0.96 (0.94;0.98) 44% (20%;73%)
- ≥2 1.49 (0.84;2.65) 1.02 (0.97;1.07) 47% (-17%;161%)
Maternal age 0.59
- <25 years 1.52 (1.22;1.90) 1 (ref.) 52% (22%;90%)
- 25-29 years 1.02 (0.85;1.23) 0.77 (0.75;0.80) 32% (10%;58%)
- ≥30 years 0.97 (0.81;1.17) 0.67 (0.66;0.69) 45% (20%;74%)
Type of parenthood 0.02
- Shared 1.34 (1.19;1.51) 1 (ref.) 34% (19%;51%)
- Single 2.68 (2.08;3.46) 1.38 (1.34;1.42) 95% (51%;151%)
Season 0.67
- Fall 1.33 (1.06;1.66) 1 (ref.) 33% (6%;66%)
- Winter 1.73 (1.43;2.08) 1.15 (1.12;1.18) 51% (25%;81%)
- Spring 1.37 (1.08;1.72) 0.89 (0.86;0.91) 54% (22%;94%)
- Summer 1.00 (0.72;1.39) 0.60 (0.58;0.62) 66% (19%;131%)
100
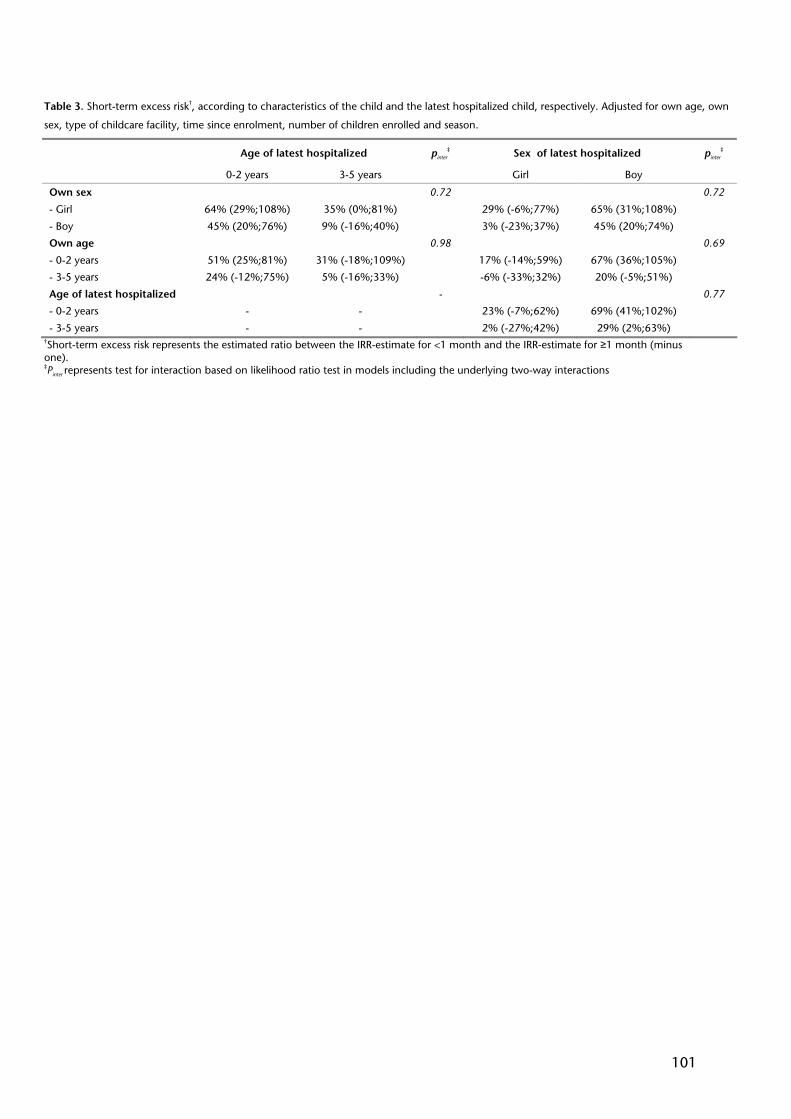
Table 3. Short-term excess risk†, according to characteristics of the child and the latest hospitalized child, respectively. Adjusted for own age, own
sex, type of childcare facility, time since enrolment, number of children enrolled and season.
†Short-term excess risk represents the estimated ratio between the IRR-estimate for <1 month and the IRR-estimate for ≥1 month (minus one). ‡Pinter represents test for interaction based on likelihood ratio test in models including the underlying two-way interactions
Age of latest hospitalized pinter
‡ Sex of latest hospitalized pinter
‡
0-2 years 3-5 years Girl Boy
Own sex 0.72 0.72
- Girl 64% (29%;108%) 35% (0%;81%) 29% (-6%;77%) 65% (31%;108%)
- Boy 45% (20%;76%) 9% (-16%;40%) 3% (-23%;37%) 45% (20%;74%)
Own age 0.98 0.69
- 0-2 years 51% (25%;81%) 31% (-18%;109%) 17% (-14%;59%) 67% (36%;105%)
- 3-5 years 24% (-12%;75%) 5% (-16%;33%) -6% (-33%;32%) 20% (-5%;51%)
Age of latest hospitalized - 0.77
- 0-2 years - - 23% (-7%;62%) 69% (41%;102%)
- 3-5 years - - 2% (-27%;42%) 29% (2%;63%)
101

102
Study V
103
104

LETTER TO THE EDITOR
Childcare in the first 2 years of life reduces the risk of childhood acute lymphoblasticleukemia
Leukemia advance online publication, 9 August 2007;doi:10.1038/sj.leu.2404884
Based on the two-hit hypothesis, exposure to infections early inlife has been hypothesized to reduce the risk of childhood acutelymphoblastic leukemia (ALL).1 The first hit should occurprenatally, whereas the second hit is related to delayed ordiminished exposure to infections in early childhood, accom-panied by an abnormal immune response.1,2 So far, no specificinfectious agents affecting the risk of childhood ALL have beenidentified. Instead, established risk factors for infections early inlife, such as attendance to childcare, have been commonly usedas a proxy measure of an early high infection load. Previousstudies on childcare attendance have presented conflictingresults, which could reflect childcare facility differences or thatthe effect of childcare on childhood ALL is modified by otherfactors. To evaluate the association between childcare atten-dance and childhood ALL, we conducted a nationwide studyusing Danish register data. The study was carried out as amatched case–control study nested in the cohort of all Danishchildren in the period 1989–2004. All incident cases of ALLdiagnosed in children aged 0–15 years in Denmark wereidentified. Ten population controls per case were individuallymatched on date of birth and sex. Data were retrieved fromthree population-based registries: The Nordic Society ofPaediatric Haematology and Oncology (NOPHO) database,3
the Danish Civil Registration System4 and the ChildcareDatabase.5
During the study period, 559 children were diagnosed withchildhood ALL in Denmark. The immune phenotype of 467cases (84%) was B-cell precursor ALL, 73 cases (13%) had T-lineage ALL, 7 cases (1%) had mature B-cell ALL and for 12cases (2%) information about immune phenotype was lacking inthe register. The leukemic karyotype classified 199 cases (36%)as common ALL (t(12;21)(q13;q22) translocation or a hyperdi-ploid karyotype), whereas the karyotype was lacking orconsisted of other aberrations for the remaining 360 cases. Awhite blood cell count of o50 was found in 430 cases (77%),whereas 118 cases (21%) had a white blood cell count of X50.White blood cell count was not available for 11 cases. Medianage at diagnosis was 4.0 years. Ten cases (2%) were diagnosedwith childhood ALL before the age of 1.0 year. In Table 1,characteristics of cases and controls are shown. Information onchildcare attendance during the first 2 years of life was completefor 176 cases (32%) and 1571 controls (28%). Overall, everattendance to childcare was associated with a rate ratio (RR) of0.68 (95% CI 0.48; 0.95). Children with incomplete registrationof childcare but with one or more registration of childcare had aRR of 0.59 (0.43; 0.81). Each additional month enrolled inchildcare was associated with an insignificantly decreasing RRof 0.98 (95% CI 0.94; 1.03). There was no statistically significantdifference between different types of childcare (P¼ 0.57).Increased risks of childhood ALL, however not significant, wereseen with increasing birth weight and increasing maternal and
paternal age. No significant main effect of birth order orpopulation density on ALL risk was observed. Significantly fewercases than controls were born outside of Denmark (4 vs 10%,Po0.01). None of the covariates listed in Table 1 changed theestimated effect of ever attendance to childcare on ALL risk by5% or more; thus, crude estimates are presented. The variablechanging the estimated effect of ever attendance to childcare themost was birth weight. When adjusted for birth weight, theestimate for ever attendance to childcare decreased to 0.65(95% CI 0.47; 0.92).
In the analyses presented in Tables 2–4, a total of 142 casesand 1545 controls were included in the ‘Ever attendance’category. Besides the 110 cases and 1114 controls withcomplete registration of childcare who ever attended childcare,the category included an additional 32 cases and 431 controlswith one or more enrollments during follow-up, but with anincomplete registration of childcare attendance. The distributionof clinical characteristics did not differ between children everattending childcare, never attending childcare and children withincomplete registration. Table 2 presents cases, matchedcontrols and RR (95% CI) of childhood ALL according toattendance to childcare and childhood ALL subtype. Everattendance to childcare was associated with a similarly reducedrisk of all childhood ALL subtypes, albeit not significantly forsubtypes with few cases. Since the risk reduction was compar-able for all subtypes, we analyzed all cases together in thesubsequent analyses. Table 3 shows cases, matched controlsand RR (95% CI) of childhood ALL according to age at exposureto childcare. Regardless of the age at exposure, ever attendanceto childcare was found to impose a decreased risk of childhoodALL. A test for homogeneity showed that the lower risk couldnot be attributed to any special ages at exposure. We alsoevaluated the role of exposure at different ages by studying theeffect of age at enrollment (data not shown). Since we stoppedfollow-up at 2 years of age, and very few children in that agegroup are withdrawn from childcare once enrolled, the effect ofage at enrollment was almost identical to the effect of timeenrolled in childcare presented in Table 1. Finally, as asensitivity analysis, we studied different time windows of everattendance to childcare by varying the definition of exposure aso6, o12, o18 and o24 months of age. The different measuresled to similar results (data not shown). Table 4 presentsinteraction analyses between attendance to childcare andcovariates. Girls attending childcare had a statistically signifi-cantly decreased risk of ALL of 53% (95% CI 25%; 71%),whereas the risk was not significantly reduced for boys.However, the test for interaction revealed that the effect ofchildcare attendance was not significantly different for girls andboys (Pinter¼ 0.13). Although children with X1 older siblingshad a more reduced risk than children with no older siblings ifever attending childcare, the risk reduction was not significantlydifferent (Pinter¼ 0.14). No interaction was observed with birthweight (Pinter¼ 0.76) or population density (Pinter¼ 0.24). Withregard to parental age, children of parents aged 25 years or morehad a more pronounced reduced risk of childhood ALL if ever
Leukemia (2007), 1–5& 2007 Nature Publishing Group All rights reserved 0887-6924/07 $30.00
www.nature.com/leu
105
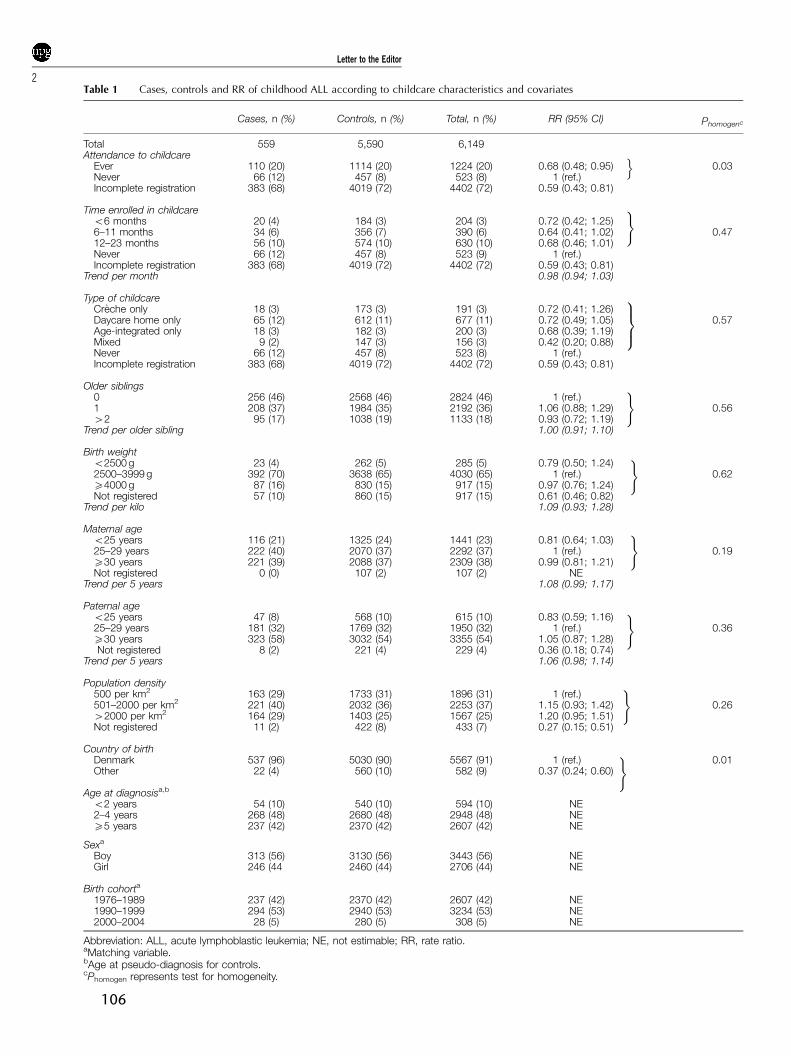
Table 1 Cases, controls and RR of childhood ALL according to childcare characteristics and covariates
Cases, n (%) Controls, n (%) Total, n (%) RR (95% CI) Phomogenc
Total 559 5,590 6,149Attendance to childcare
Ever 110 (20) 1114 (20) 1224 (20) 0.68 (0.48; 0.95) 0.03Never 66 (12) 457 (8) 523 (8) 1 (ref.)Incomplete registration 383 (68) 4019 (72) 4402 (72) 0.59 (0.43; 0.81)
Time enrolled in childcareo6 months 20 (4) 184 (3) 204 (3) 0.72 (0.42; 1.25)6–11 months 34 (6) 356 (7) 390 (6) 0.64 (0.41; 1.02) 0.4712–23 months 56 (10) 574 (10) 630 (10) 0.68 (0.46; 1.01)Never 66 (12) 457 (8) 523 (9) 1 (ref.)Incomplete registration 383 (68) 4019 (72) 4402 (72) 0.59 (0.43; 0.81)
Trend per month 0.98 (0.94; 1.03)
Type of childcareCreche only 18 (3) 173 (3) 191 (3) 0.72 (0.41; 1.26)Daycare home only 65 (12) 612 (11) 677 (11) 0.72 (0.49; 1.05) 0.57Age-integrated only 18 (3) 182 (3) 200 (3) 0.68 (0.39; 1.19)Mixed 9 (2) 147 (3) 156 (3) 0.42 (0.20; 0.88)Never 66 (12) 457 (8) 523 (8) 1 (ref.)Incomplete registration 383 (68) 4019 (72) 4402 (72) 0.59 (0.43; 0.81)
Older siblings0 256 (46) 2568 (46) 2824 (46) 1 (ref.)1 208 (37) 1984 (35) 2192 (36) 1.06 (0.88; 1.29) 0.5642 95 (17) 1038 (19) 1133 (18) 0.93 (0.72; 1.19)
Trend per older sibling 1.00 (0.91; 1.10)
Birth weighto2500 g 23 (4) 262 (5) 285 (5) 0.79 (0.50; 1.24)2500–3999 g 392 (70) 3638 (65) 4030 (65) 1 (ref.) 0.62X4000 g 87 (16) 830 (15) 917 (15) 0.97 (0.76; 1.24)Not registered 57 (10) 860 (15) 917 (15) 0.61 (0.46; 0.82)
Trend per kilo 1.09 (0.93; 1.28)
Maternal ageo25 years 116 (21) 1325 (24) 1441 (23) 0.81 (0.64; 1.03)25–29 years 222 (40) 2070 (37) 2292 (37) 1 (ref.) 0.19X30 years 221 (39) 2088 (37) 2309 (38) 0.99 (0.81; 1.21)Not registered 0 (0) 107 (2) 107 (2) NE
Trend per 5 years 1.08 (0.99; 1.17)
Paternal ageo25 years 47 (8) 568 (10) 615 (10) 0.83 (0.59; 1.16)25–29 years 181 (32) 1769 (32) 1950 (32) 1 (ref.) 0.36X30 years 323 (58) 3032 (54) 3355 (54) 1.05 (0.87; 1.28)Not registered 8 (2) 221 (4) 229 (4) 0.36 (0.18; 0.74)
Trend per 5 years 1.06 (0.98; 1.14)
Population density500 per km2 163 (29) 1733 (31) 1896 (31) 1 (ref.)501–2000 per km2 221 (40) 2032 (36) 2253 (37) 1.15 (0.93; 1.42) 0.2642000 per km2 164 (29) 1403 (25) 1567 (25) 1.20 (0.95; 1.51)Not registered 11 (2) 422 (8) 433 (7) 0.27 (0.15; 0.51)
Country of birthDenmark 537 (96) 5030 (90) 5567 (91) 1 (ref.) 0.01Other 22 (4) 560 (10) 582 (9) 0.37 (0.24; 0.60)
Age at diagnosisa,b
o2 years 54 (10) 540 (10) 594 (10) NE2–4 years 268 (48) 2680 (48) 2948 (48) NEX5 years 237 (42) 2370 (42) 2607 (42) NE
Sexa
Boy 313 (56) 3130 (56) 3443 (56) NEGirl 246 (44 2460 (44) 2706 (44) NE
Birth cohorta
1976–1989 237 (42) 2370 (42) 2607 (42) NE1990–1999 294 (53) 2940 (53) 3234 (53) NE2000–2004 28 (5) 280 (5) 308 (5) NE
Abbreviation: ALL, acute lymphoblastic leukemia; NE, not estimable; RR, rate ratio.aMatching variable.bAge at pseudo-diagnosis for controls.cPhomogen represents test for homogeneity.
o
)
9>=>;
)
)
)
)
)
)
Letter to the Editor
2
106
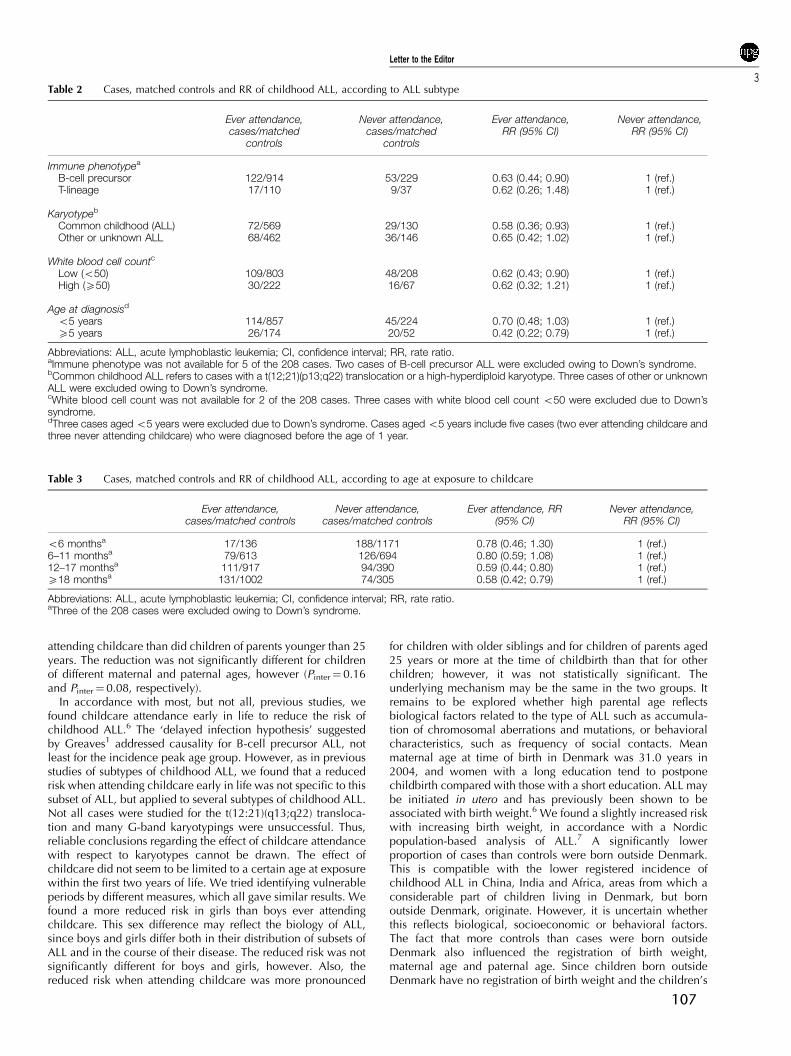
attending childcare than did children of parents younger than 25years. The reduction was not significantly different for childrenof different maternal and paternal ages, however (Pinter¼ 0.16and Pinter¼ 0.08, respectively).
In accordance with most, but not all, previous studies, wefound childcare attendance early in life to reduce the risk ofchildhood ALL.6 The ‘delayed infection hypothesis’ suggestedby Greaves1 addressed causality for B-cell precursor ALL, notleast for the incidence peak age group. However, as in previousstudies of subtypes of childhood ALL, we found that a reducedrisk when attending childcare early in life was not specific to thissubset of ALL, but applied to several subtypes of childhood ALL.Not all cases were studied for the t(12:21)(q13;q22) transloca-tion and many G-band karyotypings were unsuccessful. Thus,reliable conclusions regarding the effect of childcare attendancewith respect to karyotypes cannot be drawn. The effect ofchildcare did not seem to be limited to a certain age at exposurewithin the first two years of life. We tried identifying vulnerableperiods by different measures, which all gave similar results. Wefound a more reduced risk in girls than boys ever attendingchildcare. This sex difference may reflect the biology of ALL,since boys and girls differ both in their distribution of subsets ofALL and in the course of their disease. The reduced risk was notsignificantly different for boys and girls, however. Also, thereduced risk when attending childcare was more pronounced
for children with older siblings and for children of parents aged25 years or more at the time of childbirth than that for otherchildren; however, it was not statistically significant. Theunderlying mechanism may be the same in the two groups. Itremains to be explored whether high parental age reflectsbiological factors related to the type of ALL such as accumula-tion of chromosomal aberrations and mutations, or behavioralcharacteristics, such as frequency of social contacts. Meanmaternal age at time of birth in Denmark was 31.0 years in2004, and women with a long education tend to postponechildbirth compared with those with a short education. ALL maybe initiated in utero and has previously been shown to beassociated with birth weight.6 We found a slightly increased riskwith increasing birth weight, in accordance with a Nordicpopulation-based analysis of ALL.7 A significantly lowerproportion of cases than controls were born outside Denmark.This is compatible with the lower registered incidence ofchildhood ALL in China, India and Africa, areas from which aconsiderable part of children living in Denmark, but bornoutside Denmark, originate. However, it is uncertain whetherthis reflects biological, socioeconomic or behavioral factors.The fact that more controls than cases were born outsideDenmark also influenced the registration of birth weight,maternal age and paternal age. Since children born outsideDenmark have no registration of birth weight and the children’s
Table 2 Cases, matched controls and RR of childhood ALL, according to ALL subtype
Ever attendance,cases/matched
controls
Never attendance,cases/matched
controls
Ever attendance,RR (95% CI)
Never attendance,RR (95% CI)
Immune phenotypea
B-cell precursor 122/914 53/229 0.63 (0.44; 0.90) 1 (ref.)T-lineage 17/110 9/37 0.62 (0.26; 1.48) 1 (ref.)
Karyotypeb
Common childhood (ALL) 72/569 29/130 0.58 (0.36; 0.93) 1 (ref.)Other or unknown ALL 68/462 36/146 0.65 (0.42; 1.02) 1 (ref.)
White blood cell countc
Low (o50) 109/803 48/208 0.62 (0.43; 0.90) 1 (ref.)High (X50) 30/222 16/67 0.62 (0.32; 1.21) 1 (ref.)
Age at diagnosisd
o5 years 114/857 45/224 0.70 (0.48; 1.03) 1 (ref.)X5 years 26/174 20/52 0.42 (0.22; 0.79) 1 (ref.)
Abbreviations: ALL, acute lymphoblastic leukemia; CI, confidence interval; RR, rate ratio.aImmune phenotype was not available for 5 of the 208 cases. Two cases of B-cell precursor ALL were excluded owing to Down’s syndrome.bCommon childhood ALL refers to cases with a t(12;21)(p13;q22) translocation or a high-hyperdiploid karyotype. Three cases of other or unknownALL were excluded owing to Down’s syndrome.cWhite blood cell count was not available for 2 of the 208 cases. Three cases with white blood cell count o50 were excluded due to Down’ssyndrome.dThree cases aged o5 years were excluded due to Down’s syndrome. Cases aged o5 years include five cases (two ever attending childcare andthree never attending childcare) who were diagnosed before the age of 1 year.
Table 3 Cases, matched controls and RR of childhood ALL, according to age at exposure to childcare
Ever attendance,cases/matched controls
Never attendance,cases/matched controls
Ever attendance, RR(95% CI)
Never attendance,RR (95% CI)
o6 monthsa 17/136 188/1171 0.78 (0.46; 1.30) 1 (ref.)6–11 monthsa 79/613 126/694 0.80 (0.59; 1.08) 1 (ref.)12–17 monthsa 111/917 94/390 0.59 (0.44; 0.80) 1 (ref.)X18 monthsa 131/1002 74/305 0.58 (0.42; 0.79) 1 (ref.)
Abbreviations: ALL, acute lymphoblastic leukemia; CI, confidence interval; RR, rate ratio.aThree of the 208 cases were excluded owing to Down’s syndrome.
Letter to the Editor
3
107
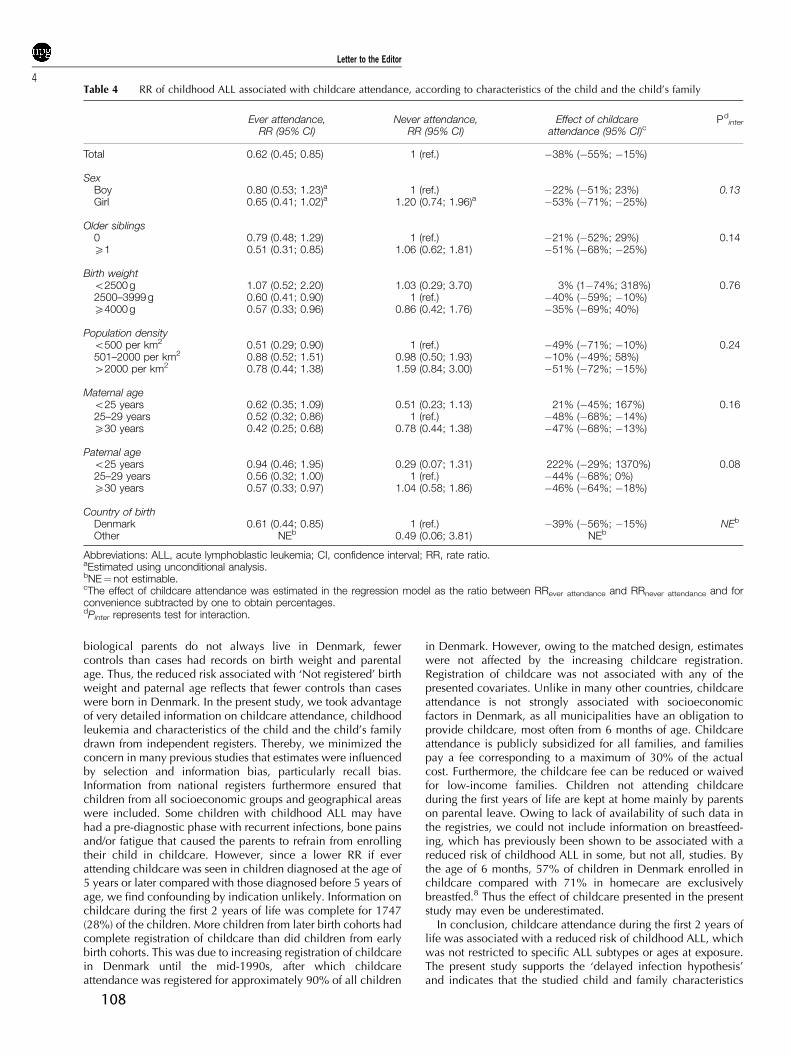
biological parents do not always live in Denmark, fewercontrols than cases had records on birth weight and parentalage. Thus, the reduced risk associated with ‘Not registered’ birthweight and paternal age reflects that fewer controls than caseswere born in Denmark. In the present study, we took advantageof very detailed information on childcare attendance, childhoodleukemia and characteristics of the child and the child’s familydrawn from independent registers. Thereby, we minimized theconcern in many previous studies that estimates were influencedby selection and information bias, particularly recall bias.Information from national registers furthermore ensured thatchildren from all socioeconomic groups and geographical areaswere included. Some children with childhood ALL may havehad a pre-diagnostic phase with recurrent infections, bone painsand/or fatigue that caused the parents to refrain from enrollingtheir child in childcare. However, since a lower RR if everattending childcare was seen in children diagnosed at the age of5 years or later compared with those diagnosed before 5 years ofage, we find confounding by indication unlikely. Information onchildcare during the first 2 years of life was complete for 1747(28%) of the children. More children from later birth cohorts hadcomplete registration of childcare than did children from earlybirth cohorts. This was due to increasing registration of childcarein Denmark until the mid-1990s, after which childcareattendance was registered for approximately 90% of all children
in Denmark. However, owing to the matched design, estimateswere not affected by the increasing childcare registration.Registration of childcare was not associated with any of thepresented covariates. Unlike in many other countries, childcareattendance is not strongly associated with socioeconomicfactors in Denmark, as all municipalities have an obligation toprovide childcare, most often from 6 months of age. Childcareattendance is publicly subsidized for all families, and familiespay a fee corresponding to a maximum of 30% of the actualcost. Furthermore, the childcare fee can be reduced or waivedfor low-income families. Children not attending childcareduring the first years of life are kept at home mainly by parentson parental leave. Owing to lack of availability of such data inthe registries, we could not include information on breastfeed-ing, which has previously been shown to be associated with areduced risk of childhood ALL in some, but not all, studies. Bythe age of 6 months, 57% of children in Denmark enrolled inchildcare compared with 71% in homecare are exclusivelybreastfed.8 Thus the effect of childcare presented in the presentstudy may even be underestimated.
In conclusion, childcare attendance during the first 2 years oflife was associated with a reduced risk of childhood ALL, whichwas not restricted to specific ALL subtypes or ages at exposure.The present study supports the ‘delayed infection hypothesis’and indicates that the studied child and family characteristics
Table 4 RR of childhood ALL associated with childcare attendance, according to characteristics of the child and the child’s family
Ever attendance,RR (95% CI)
Never attendance,RR (95% CI)
Effect of childcareattendance (95% CI)c
Pdinter
Total 0.62 (0.45; 0.85) 1 (ref.) �38% (�55%; �15%)
SexBoy 0.80 (0.53; 1.23)a 1 (ref.) �22% (�51%; 23%) 0.13Girl 0.65 (0.41; 1.02)a 1.20 (0.74; 1.96)a �53% (�71%; �25%)
Older siblings0 0.79 (0.48; 1.29) 1 (ref.) �21% (�52%; 29%) 0.14X1 0.51 (0.31; 0.85) 1.06 (0.62; 1.81) �51% (�68%; �25%)
Birth weighto2500 g 1.07 (0.52; 2.20) 1.03 (0.29; 3.70) 3% (1�74%; 318%) 0.762500–3999 g 0.60 (0.41; 0.90) 1 (ref.) �40% (�59%; �10%)X4000 g 0.57 (0.33; 0.96) 0.86 (0.42; 1.76) �35% (�69%; 40%)
Population densityo500 per km2 0.51 (0.29; 0.90) 1 (ref.) �49% (�71%; �10%) 0.24501–2000 per km2 0.88 (0.52; 1.51) 0.98 (0.50; 1.93) �10% (�49%; 58%)42000 per km2 0.78 (0.44; 1.38) 1.59 (0.84; 3.00) �51% (�72%; �15%)
Maternal ageo25 years 0.62 (0.35; 1.09) 0.51 (0.23; 1.13) 21% (�45%; 167%) 0.1625–29 years 0.52 (0.32; 0.86) 1 (ref.) �48% (�68%; �14%)X30 years 0.42 (0.25; 0.68) 0.78 (0.44; 1.38) �47% (�68%; �13%)
Paternal ageo25 years 0.94 (0.46; 1.95) 0.29 (0.07; 1.31) 222% (�29%; 1370%) 0.0825–29 years 0.56 (0.32; 1.00) 1 (ref.) �44% (�68%; 0%)X30 years 0.57 (0.33; 0.97) 1.04 (0.58; 1.86) �46% (�64%; �18%)
Country of birthDenmark 0.61 (0.44; 0.85) 1 (ref.) �39% (�56%; �15%) NEb
Other NEb 0.49 (0.06; 3.81) NEb
Abbreviations: ALL, acute lymphoblastic leukemia; CI, confidence interval; RR, rate ratio.aEstimated using unconditional analysis.bNE¼ not estimable.cThe effect of childcare attendance was estimated in the regression model as the ratio between RRever attendance and RRnever attendance and forconvenience subtracted by one to obtain percentages.dPinter represents test for interaction.
Letter to the Editor
4
108

play a minor role in the association between childcareattendance early in life and childhood ALL.
Acknowledgements
This study was supported by the Danish Foundation of ChildCancer, the Health Insurance Foundation, the Egmont Foundationand Mikael Goldschmidt Holding A/S.
M Kamper-Jørgensen1, A Woodward2, J Wohlfahrt1, CS Benn3,J Simonsen1, H Hjalgrim1 and K Schmiegelow4,5
1Department of Epidemiology Research, Statens SerumInstitut, Copenhagen, Denmark;
2School of Population Health, University of Auckland,Auckland, New Zealand;
3Bandim Health Project, Statens Serum Institut, Copenhagen,Denmark and
4Pediatric Clinic, The University Hospital Rigshospitalet andThe Medical Faculty, University of Copenhagen, Copenhagen,
DenmarkE-mail: [email protected]
5The author holds the Danish Childhood Cancer Foundationprofessorship in Pediatric Oncology.
References
1 Greaves M. Infection, immune responses and the aetiology ofchildhood leukaemia. Nat Rev Cancer 2006; 6: 193–203.
2 Knudson Jr AG. Mutation and cancer: statistical study of retino-blastoma. Proc Natl Acad Sci USA 1971; 68: 820–823.
3 Hjalgrim LL. Aspects of the natural history of childhood leukaemia.Thesis, Copenhagen 2003.
4 Pedersen CB, Gotzsche H, Moller JO, Mortensen PB. The DanishCivil Registration System. A cohort of eight million persons. DanMed Bull 2006; 53: 441–449.
5 Kamper-Jorgensen M, Wohlfahrt J, Simonsen J, Benn CS. TheChildcare database: a valuable register linkage. Scand J PublicHealth 2007; 35: 323–329.
6 McNally RJ, Eden TO. An infectious aetiology for childhood acuteleukaemia: a review of the evidence. Br J Haematol 2004; 127:243–263.
7 Hjalgrim LL, Rostgaard K, Hjalgrim H, Westergaard T, ThomassenH, Forestier E et al. Birth weight and risk for childhood leukemia inDenmark, Sweden, Norway, and Iceland. J Natl Cancer Isnt 2004;96: 1549–1556.
8 Benn CS, Wohlfahrt J, Aaby P, Westergaard T, Benfeldt E,Michaelsen KF et al. Breastfeeding and risk of atopic dermatitis,by parental history of allergy, during the first 18 months of life. Am JEpidermiol 2004; 160: 217–223.
Letter to the Editor
5
109





























