Embed Size (px)
Citation preview

Archives ofDisease in Childhood 1996; 74: 232-235
Alagille's syndrome associated with cystic renaldisease
S R Martin, L Garel, F Alvarez
AbstractAlthough renal abnormalities have beendescribed in children with Alagille'ssyndrome, cystic kidney disease has notoften been documented, and then usuallyonly at necropsy. Three children withAlagille's syndrome are described, in twoofwhom a unilateral multicystic dysplas-tic kidney was detected by prenatal ultra-sound; in the other, a solitary cortical cystwas found later in childhood. All havenormal renal function, growth, and liversynthetic function but continue to haveclinical and biochemical signs ofcholesta-sis. These cases show that unilateral cystickidney disease with or without renal dys-plasia may be associated with Alagille'ssyndrome, that the clinical course isnot necessarily unfavourable, and thatAlagille's syndrome should be included inthe differential diagnosis of cystic kidneydisorders associated with cholestatic liverdisease. Patients with Alagille's syndromeshould be evaluated by renal ultrasound.(Arch Dis Child 1996; 74: 232-235)
Keywords: Alagille's syndrome, multicystic dysplastickidney, ultrasound.
Division ofGastroenterology andNutrition, H6pitalSainte-Justine, 3175Cote Ste Catherine,Montreal, QuebecH3T 1C5, CanadaS R MartinL GarelF Alvarez
Correspondence to:Dr Martin.
Accepted 4 December 1995
Alagille's syndrome, one of the most commoncauses of intrahepatic cholestasis of infancy, isa familial disorder characterised by five majorfeatures: abnormal facies, chronic cholestasis,butterfly vertebrae, peripheral pulmonaryartery stenosis, and posterior embryotoxon ofthe eye. Renal involvement, which is includedamong a number of other less common mani-festations, has recently been reported moreoften.2-12 Renal abnormalities comprise threemain types: non-specific mild alterations inrenal function,8 10 12 those possibly related tothe hypercholesterolaemia that is associatedwith cholestasis, such as mesangiolipidosis,2-4and those resulting from abnormalities in renalmorphogenesis.2 4-12 We present three FrenchCanadian children with Alagille's syndromeassociated with cystic kidney disease, in twoof whom the diagnosis was initially made byfetal ultrasound. These observations have
importance for the significance of multicystickidneys detected prenatally and extends thedifferential diagnosis of hepatic disordersassociated with cystic kidney disease.
Case 1
A 21 month male was admitted to hospital at 4months of age for jaundice associated withacholic stools. Previously, he had been investi-gated for renal disease that presented with amulticystic right kidney detected by fetal ultra-sound at 16 and 24 weeks' gestation and con-firmed postnatally (fig 1). Evaluation in theneonatal period revealed a urinary tract infec-tion with Escherichia coli that was treated. Hewas jaundiced in the first week of life but thejaundice resolved spontaneously. Results ofinvestigations of his kidney disease are shownin table 1. At 4 months of age investigationsfor cholestasis revealed a total bilirubin of139 mmol/l (normal <23 mmol/l) and directbilirubin of 105 mmol/l (normal <19 mmoYl).The -y glutamyltranspeptidase (-yGT) was 40xnormal and there was evidence of fat solublevitamin deficiency. The diagnosis of Alagille'ssyndrome was suggested by the presence offour of the five major clinical features -
cholestasis associated with the typical facies,peripheral pulmonary stenosis, and posteriorembryotoxon. In addition, the patient's crywas high pitched, as previously described inthis syndrome.2 Liver biopsy revealed diffusecholestasis, enlargement of the portal tractswith mild fibrosis, paucity of interlobular bileducts, and a degeneration ofthe bile ducts withvacuolisation of the epithelium.At 23 months of age, his course has been
marked by normal growth (height 5th centilefor age, weight 10th centile), variable choles-tasis (currently: total bilirubin 136 mmol/l;direct bilirubin 74 mmol/1; -yGT 15X normal,and normal liver synthetic function). Hereceives supplemental fat soluble vitamins.Xanthomas were first observed at 14 months ofage; serum cholesterol peaked at 17 months ofage at 41 mmol/l (normal <4 3 mmol/l) andhas since gradually declined to 15-9 mmol/l.Pruritus became clinically significant at 10months of age and was treated with variable
Table 1 Investigations of renal disease in the three patients
Patient 1 Patient 2 Patient 3
BUN N N NCreatinine N N NDMSA scan* Non-functioning right kidney Non-functioning left kidney NDUltrasound Multicystic, dysplastic right kidney Multicystic, dysplastic left kidney Right renal cortical cystCT scan N Atrophic left kidney NDVCUG** Thick bladder wall, diverticulum Vesicoureteral reflux, grade I ND
*Dimercaptosuccinic acid, **voiding cystourethrogram. ND= not done; N=normal.
232
on 6 Decem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.74.3.232 on 1 March 1996. D
ownloaded from

Alagille 's syndrome and cystic renal disease
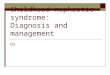
Figure 1 Patient 1 at 4 months of age. (A) Longitudinal scan of the right kidney. Macrocystic changes are obvious in a76 mm kidney. The left kidney (not shown) was normal (66 mm in length in compensatory hypertrophy). (B) Transversescan.
success with hydroxyzine, phenobarbitone,ursodeoxycholic acid, or rifampicin.
Case 2A left multicystic dysplastic kidney wasdetected by prenatal ultrasound in this patientat 19 weeks (fig 2) and confirmed at 21 and 27weeks' gestation. He was born at term with abirth weight of 3750 g. Jaundice was noted onthe third day of life; the serum bilirubin con-centration peaked on the fifth day (total bili-rubin 208 mmoll; direct 111 mmol/l ). At sixweeks of age he was admitted to hospital forinvestigation of his kidney disorder and persis-tent cholestasis. The renal findings are sum-marised in table 1. The diagnosis of Alagille'ssyndrome was established from the presenceof chronic cholestasis, peripheral pulmonarystenosis, posterior embryotoxon, butterflyvertebrae, and typical facies. Follow up wasnotable only for biochemical signs of choles-tasis (total bilirubin 23 mmol/l; direct bilirubin
19 mmol/l; -yGT 29 x normal, cholesterol6-9 mmol/l) without xanthomas, for which hehas received supplemental fat soluble vitamins,and a mild pruritus that was successfullytreated with ursodeoxycholic acid. His growthis normal (weight 10th centile for age, height50th centile).
Case 3This 14 year old patient was initially dis-covered to have a solitary cortical cyst of theright kidney on routine follow up ultrasound at1 1 years of age (table 1). He was first admittedto hospital at Hopital Sainte Justine at 21months of age for pruritus and biochemicalchanges consistent with cholestasis. He hadpresented elsewhere with cholestasis on thefourth day of life that had not subsequentlybeen extensively investigated. The presenceof cholestasis, typical facies, peripheral pul-monary stenosis, and posterior embryotoxonsuggested the diagnosis of Alagille's syndrome;
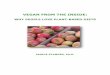
Figure 2 Antenatal ultrasound ofpatient 2 at 19 weeks'gestation. (A) Longitudinal scan. Normal right kidney (inbetween calipers); multicystic dysplasia ofleft kidney (LK). (B) Transverse scan.
233
11
on 6 Decem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.74.3.232 on 1 March 1996. D
ownloaded from

Martin, Garel, Alvarez
his mother was also observed to have thetypical facies of Alagille's syndrome, pruritus,and characteristic voice, but she refusedfurther investigation. A liver biopsy at 21months of age revealed a paucity of bile ductswithout fibrosis or histological signs ofcholestasis. The evolution of this patient's ill-ness was characterised by almost completeremission of the cholestasis (total bilirubin5 mmol/l, direct bilirubin 0 mmol/l, yGT 3 Xnormal, cholesterol 4'1 mmol/1). He receivesrifampicin for mild pruritus and fat solublevitamin supplementation, and is growing nor-
mally (weight 75th centile for age, height 50thcentile).
DiscussionRenal involvement was not a prominent featureof early reports of Alagille's syndrome.' Sincethen, a variety of non-specific findings has beendescribed, including azotaemia, urine concen-tration defects, and nephrolithiasis. Mesangio-lipidosis is common and while it most probablyrelates to the hypercholesterolaemia that isassociated with chronic cholestasis,2-4 Alagilleand coworkers did not find a correlation withthe serum lipid levels.2 In addition, a variety ofabnormalities in renal morphogenesis has beendescribed, which include small kidneys,6 10 12congenital single kidney,5 '0 microcystic tubulardilatation with interstitial fibrosis,4 9-l1 andrenal Cysts.2 4 5 7 9 11 The association of cystickidney disease with Alagille's syndrome hasbeen reported infrequently (table 2), possiblybecause of the poor definition of cysts usingolder ultrasound equipment and the difficultyin identifying early lesions by ultrasound.Medullary cystic kidney disease was found atnecropsy in two patients with a partial form ofAlagille's syndrome,5 in one dying of sepsisfollowing liver transplantation at three years ofage,4 and in another who died at two months ofage in renal failure.I1 All other documentedcases of cystic kidney disease have beendescribed at necropsy, prompting some investi-gators to question whether this finding maysuggest a poor prognosis in Alagille's syn-drome.5 6 However, none of our three patientshas shown signs of deteriorating renal function,while showing the full spectrum of possibleevolution of their cholestasis. This implies thatcystic kidney disease may not of itself indicate a
poor prognosis, but rather the type (simple cystversus nephronophthisis) and extent (unilateralversus bilateral) of renal involvement thatgoverns the patient's prognosis.
Hyams and colleagues, in observing thattheir patient did not have dysplastic changes ineither kidney, suggested that the findings inAlagille's syndrome differed from other condi-tions with cystic renal lesions associated withbiliary tract abnormalities such as Meckel'ssyndrome, Jeune's syndrome, and Zellweger'ssyndrome.9 Two of our patients presented pre-natally with a unilateral multicystic dysplastickidney, suggesting that dysplastic kidneys mayalso occur in this syndrome. Indeed, concen-
tric layering of mesenchymal cells around bileducts in early Alagille's syndrome was sug-gested to be superficially reminiscent ofchanges observed in dysplastic kidneys. 13Desmet hypothesised that a defect in epithe-lial-mesenchymal inductive interactions inearly gestation may explain the coexistence ofbiliary and renal cystic abnormalities in a
variety of inherited malformation syndromesassociated with fibrocystic cholangiopathy andabnormal remodelling of the primitive ductalplate.'4 In some, progression of the diseaseleads to ductal degeneration and involution.He suggested that because intrahepatic paucityof interlobular bile ducts is not associated withrenal lesions, the cause and mechanism of bileduct destruction is probably different fromthose disorders associated with congenitalhepatic fibrosis. Our observations, togetherwith other reports of abnormalities in renalmorphogenesis with Alagille's syndrome,suggest that a defect in epithelial-mesenchymalinduction may also be responsible for the con-
stellation of abnormalities in this disorder. Thelack of reports of ductal plate malformationdoes not necessarily exclude Alagille's syn-
drome from Desmet's hypothesis. Rather thismay merely reflect a slower, less aggressivehepatic disease process that allows more com-
plete ductal plate remodelling to occur, whilein other organs more severe disturbances arisein early development, giving the typical post-natal pattern of malformations of Alagille'ssyndrome. The cause of such failures of induc-tion is likely to be multifactorial and mayinclude differences in the expression of genesregulating inductive interactions. Such differ-ences may account for the variability of clinicalexpression of inherited disorders with biliaryand renal manifestations.
In conclusion, Alagille's syndrome belongsin the spectrum of disorders associated withcystic renal disease and thus expands the dif-ferential diagnosis of multicystic kidneydetected by prenatal ultrasound. Cysticdysplastic kidneys may be included in the
Table 2 Review ofpublished cases of cystic renal abnormalities in Alagille's syndrome
Reference Features* Renalfindings Status
2 5/5 'Polycystic kidneys' Died4 5/5 1-5 mm Corticomedullary cysts; microcystic tubular dilatation; interstitial fibrosis Died
4/5 Single 2 cm subcapsular cyst Died5 1/5 Medullary cystic disease (nephronophthisis) Died
1/5 Medullary cystic disease (nephronophthisis)7 3/5 'Cystic kidney disease' Died
3/5 'Cystic kidney disease' Died9 3/5 Severe tubulointerstitial nephropathy with microcystic tubular dilatation Died10 3/5 Bilateral focal tubular dilatation; interstitial fibrosis Alive11 3/5 Subcortical cysts; interstitial fibrosis; nephronophthisis) Died
*Number of major characteristics of Alagille's syndrome.
234
on 6 Decem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.74.3.232 on 1 March 1996. D
ownloaded from

Alagille's syndrome and cystic renal disease 235
spectrum of abnormalities of renal morpho-genesis associated with Alagille's syndrome.Cystic renal lesions are not always associatedwith a poor prognosis. We support the recom-mendation that all patients with Alagille's syn-drome be evaluated by renal ultrasound inorder to determine the prevalence of cysticrenal disease.
1 Alagille D, Odievre M, Gauthier M, Dommergues JP.Hepatic ductular hypoplasia associated with characteristicfacies, vertebral malformations, retarded physical, mentaland sexual development, and cardiac murmur. J Pediatr1975; 86: 63.
2 Alagille D, Estrada A, Hadchouel M, Gauthier M, OdievreM, Dommergues JP. Syndromic paucity of interlobularbile ducts (Alagille syndrome or arteriohepatic dyplasia):review of 80 cases. 7 Pediatr 1987; 110: 195-200.
3 Chung-Park M, Petrelli M, Hall PW, Henoch MS, DahmsBB. Renal lipidosis associated with arteriohepatic dys-plasia (Alagille's syndrome). Clin Nephrol 1982; 18:314-20.
4 Russo PA, Demetrius E, Hashida Y. Renal histopathologyin Alagille's syndrome. Pediatr Pathol 1987; 7:557-68.
5 Oestreich AE, Sokol RJ, Suchy FJ, Heubi JE. Renal
abnormalities in arteriohepatic dysplasia and nonsyn-dromic intrahepatic biliary hypoplasia. Ann Radiol 1983;26: 203-9.
6 Wolfish NM, Shanon A. Nephropathy in arteriohepatic dys-plasia (Alagille's syndrome). Child Nephrol Urol 1988; 89:169-72.
7 Greenwood RD, Rosenthal A, Crocker AC, Nadas AS.Syndrome of intrahepatic biliary dysgenesis and cardio-vascular malformations. Pediatrics 1976; 58: 243-7.
8 Riely CA, Cotlier E, Jensen PS, Klatskin G. Arteriohepaticdysplasia: a benign syndrome of intrahepatic cholestasiswith multiple organ involvement. Ann Intern Med 1979;91: 520-7.
9 Hyams JS, Berman MM, Davis BH. Tubulointerstitialnephropathy asssociated with arteriohepatic dysplasia.Gastroenterology 1983; 85: 430-4.
10 Labreque DR, Mitros FA, Nathan RJ, Romanchuk KG,Judisch GF, El-Khoury GH. Four generations of arterio-hepatic dysplasia. Hepatology 1982; 2: 467-74.
11 Tolia V, Dubois RS, Watts FB, Perrin E. Renal abnor-malities in paucity of interlobular bile ducts. J PediatrGastroenterol Nutr 1987; 6: 971-6.
12 Rosenfield NS, Kelley MJ, Jensen PS, Cotlier E, RosenfieldAT, Riley CA. Arteriohepatic dysplasia: radiologicfeatures of a new syndrome. Am 7 Radiol 1980; 135:1217-23.
13 Hashida Y, Yunis EJ. Syndromatic paucity of interlobularbile ducts. Hepatic histopathology of the early and end-stage liver. Pediatr Pathol 1988; 8: 1-17.
14 Desmet VJ. The cholangiopathies. In: Suchy F, ed. Liverdisease in children. St Louis: Mosby, 1994: 145.
on 6 Decem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.74.3.232 on 1 March 1996. D
ownloaded from