Embed Size (px)
Citation preview

F8 Archives of Disease in Childhood 1995; 72: F8-F13
Randomised clinical trial of two treatmentregimens of natural surfactant preparations inneonatal respiratory distress syndrome
Christian P Speer, Olaf Gefeller, Peter Groneck, Edgar Laufk6tter, Claudia Roll,Ludwig Hanssler, Karsten Harms, Egbert Herting, Herbert Boenisch, Jiirgen Windeler,Bengt Robertson
Department ofPaediatrics, Universityof GottingenC P SpeerK HarmsE Herting
Department ofMedical StatisticsO Gefeller
Department ofPaediatrics,StadtischesKrankenhaus, KolnP Groneck
Department ofPaediatrics, UniversityofBochumE Laufkotter
Department ofPaediatrics, Universityof EssenC RollL Hanssler
StadtischesKrankenhausBraunschweig,H Boenisch
Department ofMedical Informaticsand Biomathematics,University ofBochumJ Windeler
Karolinska Institute,Research Unit forExperimentalPerinatal Pathology,Karolinska Hospital,Stockholm, SwedenB Robertson
Correspondence to:Dr Christian P Speer,Department of Neonatology,University of Tubingen,RumelinstralBe 23, 72070Tuibingen, Germany.Accepted 17 August 1994
AbstractAims-To compare treatment regimensof two widely used natural surfactantpreparations Curosurf and Survanta inrespiratory distress syndrome (RDS).Methods-The effects of the two treat-ment regimens on gas exchange, ventila-tory requirements, and 28 day outcome ininfants with RDS were compared. Seventyfive preterm infants (birth weight 700-1500g) with RDS requiring artificial ventilationwith an FIO2 of :0 4, were randomlyselected at 1-24 hours of age. One groupreceived an initial dose of Curosurf (200mg/kg); the other group Survanta (100mg/kg). Patients who remained dependenton artificial ventilation with an FIO2 ofB0*3received up to two additional doses ofCurosurf (each of 100 mg/g) after 12 and24 hours or up to three additional doses ofSurvanta (each of 100 mg/kg) between sixand 48 hours after the initial dose.Results-There was a rapid improvementin oxygenation and ventilatory require-ments were reduced in both groups.However, infants treated with Curosurfhad a higher arterial:alveolar oxygentension ratio and required a lower peakinspiratory pressure and mean airwaypressure at several time points within 24hours of randomisation (p<0.05-0.001).The incidences of pneumothorax in theCurosurf and Survanta groups were 6%and 12-5%S respectively; the correspond-ing figures for grades 3-4 intracerebralhaemorrhage were 30/0 and 12/5%o respec-tively. Mortality was 30/0 in the Curosurfgroup and 12-5% in the Survanta group.However, these differences did not reachsignificance.Conclusion-The Curosurf treatmentregimen resulted in a more rapid improve-ment in oxygenation than Survanta andreduced ventilatory requirements up to 24hours after start of treatment. This wasassociated with a trend towards reducedincidence of serious pulmonary and non-pulmonary complications.(Arch Dis Child 1995; 72: F8-F13)
Keywords: surfactant treatment, respiratory distresssyndrome, Curosurf, Survanta.
Surfactant treatment with natural or syntheticpreparations reduces the incidence of neonatal
mortality and pneumothorax in babies withrespiratory distress syndrome (RDS).1 Naturalsurfactants seem to improve oxygenation andlung function more rapidly than syntheticsurfactants,2 but there have been no studiescomparing the effects of two natural surfac-tants.We designed a pilot trial to compare the
acute effects of the bovine preparationSurvanta (Beractant, Ross Laboratories,Columbus, Ohio, USA) and the porcine sur-factant Curosurf (Chiesi Farmaceutici, Parma,Italy). The two surfactant preparations havebeen carefully evaluated in clinical trials36 7-9;they are licensed in Europe and have severalfeatures in common but differ in some poten-tially important biophysical characteristics.10
In preparation for a trial comparing thera-peutic regimens involving these two naturalsuxfactants, the present study was performedto test case record forms, compliance with ran-domisation guidelines in the collaboratingcentres, feasibility of monitoring procedures,adherence of centres to general good clinicalprinciples, and for sample size calculations of alarge definitive trial.
MethodsCurosurf is a natural surfactant, prepared frompig lungs. It contains almost exclusively polarlipids - in particular phosphatidylcholine(about 60% of the total phospholipids) and 1%of the specific hydrophobic low molecularweight apoproteins SP-B and SP-C. Furtherdetails of the composition and the physicalproperties have been described before. I1Survanta is a bovine lung extract contain-ing phospholipids, neutral lipids, fatty acids,and surfactant associated apoproteins SP-Band SP-C. Dipalmitoylphosphatidylcholine,palmitic acid, and tripalmitin are added tostandardise the composition, and to mimicthe surfactant properties of natural lungsurfactant. 12The present pilot study was designed to
determine possible differences between thetwo surfactant treatment regimens. It wasplanned to recruit at least 35 infants for eachtreatment group. No short term endpointsrelating to oxygenation or ventilator settingswere defined. Five German neonatal intensivecare units collaborated in this trial whichstarted 1 December 1991 and ended 15 July1992. The number of patients randomised byeach unit varied because of differences in the

Comparison of two natural suifactants in RDS F9
Table 1 Number ofpatients randomised in eachcontributing unit
No ofpatientsContributingunits Curosurf Survanta Total
Bochum 2 5 7Braunschweig 1 3 4Essen 9* 9 18Gottingen 9 9 18Cologne 14* 14 28
*One patient treated with Curosurf was excluded (violation ofentry criteria).
size of the population from which theywere recruited and because of differences inadmission policies (table 1).
Criteria for entry were:(i) birth weight 700-1500 g;(ii) clinical and radiological findings typical ofRDS;(iii) age at randomisation of 1-24 hours;(iv) requirement of artificial ventilation with afraction of inspired oxygen (FiO2) of >0 4;(v) no complicating diseases; and(vi) parental consent.
Complicating diseases leading to exclusionof infants were: (i) prolonged rupture ofmembranes (>3 weeks); (ii) intracranialhaemorrhage (ICH) grade III-IV beforerandomisation; and (iii) severe birth asphyxia(Apgar score of -3 at five minutes, umbilicalarterial cord blood pH of <7<1), or major con-genital anomalies. Anaemia, hypotension,hypoglycaemia, acidosis, and pneumothoraxand neonatal infection (with group B strepto-cocci, for example) were treated by appropriatemeasures before surfactant replacement.Infants were excluded if they had persistentphysiological instability such as hypotension,hypoglycaemia, and pneumothorax.
At randomisation, all infants were mechani-cally ventilated with an FiO2 of ¢'0 4 (entrycriterion), a frequency of40-80 breaths/minute,a peak inspiratory pressure (PIP) of <30 cmH20, a positive end expiratory pressure(PEEP) of 2-5 cm H20, and an inspiration toexpiration ratio of 1:1 to 1:2.On a random basis, infants with RDS who
met eligibility criteria were allocated to treat-ment with Curosurf or Survanta by means ofsealed opaque envelopes. Stratified randomisa-tion within each centre was applied with regardto birth weight (700-999 g and 1000-1500 g).After randomisation of a patient each con-tributing centre contacted the BiometricCentre at the University of Gottingen toprovide centre number, patient's number, dateof birth and treatment group. This informedthe Biometric Centre of the inclusion of a newpatient into the study, ensuring an objectiveverification of the randomisation sequence.Because the recommended doses, volumes,dose interval and dose procedures differedbetween both surfactant preparations, blindingof surfactant administration was not feasible.
All infants randomised to Curosurf treat-ment received 200 mg of Curosurf/kgbodyweight (2>5 mi/kg), divided in twoportions instilled into each main bronchus.3Retreatment with 100 mg/kg per dose wasperformed at 12 hours and 24 hours after the
first treatment if the babies required an FiO2 of>0 3 to keep Pao2 to 350 mm Hg (36-7 kPa)on mechanical ventilation. Details of the instil-lation manoeuvre have been described before.4The maximal cumulative dose was 400 mg/kg.
Survanta was administered intratracheally ata dose of 100 mg/kg (4 0 mi/kg) divided intofour equal amounts, instilled into the fourquadrants of the lung, as recommended by themanufacturer. Retreatment with Survanta wasperformed as early as 6 hours after the initialdose, provided the baby required an FiO2 of30 3 and was still on the ventilator. Six hoursafter the first dose until 48 hours of age, thepatients could receive up to three additionaltreatments, no more than every six hours ifthey remained intubated and required an FiO2of >0 3 to maintain Pao2 of 350 mm Hg(36-7 kPa). Each of these doses was100 mg/kg which means the maximumcumulative dose of Survanta was the same asfor Curosurf - 400 mg/kg. The retreatmentdoses (if required) were administered in twodoses into each lung quadrant. Details of theinstillation procedure have been reported.9 11No suctioning of the airways was performed
during the first six hours after instillation ofCurosurf or Survanta. After surfactantadministration the baby was reconnected tothe ventilator, and FiO2 and ventilator settingswere immediately adjusted according toclinical response to maintain adequate bloodgases (Pao2 of 50-70 mm Hg); (Paco240-50 mm Hg, pH 37 3) with the lowestpossible level of FiO2 and PIP. To obtainthis goal, FiO2 was lowered first; subsequentadjustments included reduction of insufflationpressure and inspiration:expiration ratio. APEEP of 2-5 cm H20 was maintained duringthe first hours after surfactant instillation.
Arterial or transcutaneous blood gas valueswere determined at regular intervals (five, 30,60 minutes; three, six, 12, 24 hours, and two,three, four, seven, and 10 days after surfactantreplacement). The Curosurf and Survantagroups were compared with respect to the fol-lowing measurements: Fio2, Pao2, Paco2, pH,Pao2:Fio2 ratio, arterial to alveolar P02 ratio(a:APO2), PIP, mean airway pressure (MAP),inspiration:expiration ratio, PEEP, ventilatoryefficiency index,4 and arterial blood pressure.The groups were also compared with respect tothe following complications diagnosed within28 days: pulmonary interstitial emphysema(PIE); pneumothorax; patent ductus arteriosus(PDA); intracerebral haemorrhage/(ICH);pulmonary haemorrhage; septicaemia; bron-chopulmonary dysplasia (BPD); and death.Furthermore, total time of exposure to supple-mental oxygen and complete duration ofmechanical ventilation during hospital staywere recorded. Chest x ray pictures wereexamined by a local paediatric radiologist whowas not involved in the study and was blindedto the randomisation of the patients. PIE andpneumothorax were diagnosed according torecent definitions.13 Sequential echocardio-grams and Doppler measurements to assessshunting across the ductus arteriosus wereobtained every 24 hours during the first week

F10 Speer, Gefeller, Groneck, et al
Table 2 Patient details
Curosurf (n=33*) Survanta (n=40)
Gestational age, weeks (mean (SD)) 28-9 (2 3) 28-8 (2 2)Birth weight g (mean (SD)) 1095-3 (226-4) 1082-4 (252 2)Male sex (%) 11 (33 3) 22 (55 0)Prenatal steroids (%/6) 14 (42-4) 15 (37 5)Umbilical cord pH (mean (SD)) 7-31 (0-06) 7-27 (0-14)Rectal temperature on admission ('G)t 36-5 (36-37) 36-3 (35 6-37)Age at treatment, hourst 3-2 (2-7-6-1) 3 0 (2-64-41)FI2o at randomisationt 0 9 (0 55-1 0) 0 9 (0 7-1 0)
*No of patients included in the final calculations after exclusion of two patients (violation ofentry criteria). tMedian (25th-75th percentile). tFraction of inspired oxygen.
of life and whenever clinical signs ofPDA werepresent. Ultrasonographic examinations of thehead were performed daily for the first sevendays and on day 10, and ICH was classifiedaccording to Papile et al 14; in surviving infantsa further cranial ultrasound scan was per-formed at 28 days to look for ischaemiclesions. 15 Pulmonary haemorrhage was definedas the appearance of bright red blood in theendotracheal tube associated with signs ofclinical deterioration of the baby. Septicaemiawas defined as clinical signs of systemic infec-tion and positive blood culture.16 BPD wasdefined as oxygen requirement at a postcon-ceptional age of 36 completed weeks.The trial was approved by the ethics com-
mittee of the University of Gottingen and wasperformed in compliance with good clinicalpractice guidelines. This compliance took intoaccount approval by relevant regulatorybodies, written informed consent of a parentbefore randomisation, and the 'CPMPWorking Party on Efficacy of MedicinalProducts: Notes for Guidance' on 'GoodClinical Practice for Trials on MedicinalProducts in the European Community'.
1.0 A0= Curosurf
0 9 -= Survanta08
0-76' 06o_ 06 **
0-5
024 -
03
0 1 2 3 4 5 6 7 8 9 10Time (days)
1-0 B
0-8
clriy **< ,*** <*1 *p001 ovrinfatr 0c 2=-8ka
0-4
0-2
STATISTICAL ANALYSISThe statistical treatment of the trial data wasapproached by an intention-to-treat analysis ofall eligible study subjects.17 Differencesbetween the two randomised groups withrespect to gas exchange and ventilatory settingsat different time points were evaluated usingthe Wilcoxon-Mann-Whitney test. When theoverall measures ofventilatory requirement andoxygen dependence were compared, the log-rank test, with the data from all patients (notonly the survivors), was used.'8 As specified inthe study protocol, logistic regression analysiswas used to assess the effect of the surfactanttreatment regimen on the 28 day outcome vari-ables while simultaneously controlling for theconfounding influence of birth weight, sex, andallocation to different hospitals. The resultingadjusted odds ratios (OR) represent approxi-mate relative risks and are accompanied bytheir 95% confidence intervals.'9
ResultsCHARACTERISATION OF PATIENTS ANDTREATMENT REGIMENSThirty five patients were randomised to theCurosurf group and 40 to the Survanta group.For two babies who were randomised toCurosurf, treatment entry criteria had been vio-lated (birth weight was <700 g in one preterminfant and > 1500 g in the other). These infantstherefore had to be excluded from furtheranalyses (neither of them had pulmonary orextrapulmonary complications until dischargefrom the hospital, outcome results includingthese babies would have favoured the Curosurfgroup). Table 2 shows that the baseline charac-teristics of both groups were quite wellmatched, with the exception that the Curosurfgroup had a higher percentage offemale babies.Median age at first treatment was about 3 hoursin both groups, and in all patients the treatmentwas initiated before the age of 15 hours.
In the Curosurf group 16 (49%) infantsreceived a single dose, 11 (33%) received twodoses, and six (18%) received three doses. Thecorresponding numbers in the Survanta groupwere 15 (38%), nine (23%), and eight (20%).Eight (20%) babies also received four doses ofSurvanta. Overall, 51-5% of the Curosurf and62-5% of the Survanta babies needed multipledoses. The cumulative dose was 273 (SD 87)mg/kg in the Curosurf group and 218 (115)mg/kg in the Survanta group, and the numberof patients requiring more than two doses wassubstantially larger in the Survanta group(40 0% v 18-2%; p=0 07 derived from Fisher'sexact test). Due to dosing errors, one Curosurfinfant received a lower initial dose; in anotherbaby the second Curosurf dose was doubled. Intwo Survanta babies the initial dose was toolow, and in one a repeat dose of Survanta wasgiven after 48 hours of age. One infant receivedthe last Survanta dose at an FIo2 of <0 3.
GAS EXCHANGE AND VENTILATOR SETTINGSAFTER SURFACTANT REPLACEMENTInitial treatment with Curosurf (200 mg/kg) or

Comparison of two natural surfactants in RDS Fll
30 A
28 o = Curosurf* = Survanta
26
240N22 *
E 20
o18
16
14
12
100 1 2 3 4 5 6 7 8 9 10
Time (days)
16 B
14
12-
10
10c =0-8ka
E*88
4-
2
00 1 2 3 4 5 6 7 8 9 10
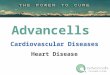
Time (days)Figure 2Peak inspiratory pressure (PIP) (A) and mean airway pressure (AMP) (B) inpatients treated with multiple doses of Curosurf or Survanta at various time points afterrandomisation. Values are given as median and 25th and 75th percentile. The points forthe two groups are offsetnfor clarity. *p<0l5, **p<0.01, ***p<0001: conversionfactor:10cm H20=098 kPa.
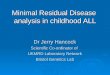
Survanta (100 mg/kg) resulted in improvedoxygenation. Median Fio2 could be loweredwithin five minutes, from 09 to0D34, inCurosurf neonates and from0g 9 to0i 5 inbabies receiving Survanta (fig 1). However,between five minutes and six hours theCurosurf treatment patients needed lessoxygen than the Survanta group(p<005-0 01); this difference was sustaineduntil 24 hours (p<0ed 5-0i001). During thefirst 24 hours after initial treatment theCurosurf babies also had a greater improve-ment in a:APO2 (p<005-OO01) (fig 1).
PIP and MIAP could gradually be reduced inboth groups; however, at various time pointsthe Curosurf treatment patients needed alower PIP and MAP than the Survanta treatedneonates (p<0i05) (fig 2). The differencesin oxygenation and ventilatory support favour-ing Curosurf treated infants did not persistbeyond 24 hours after start of treatment. At
representative time points the ventilatory effi-ciency index was not different between thegroups: median values for the Curosurf andSurvanta treatment babies before treatmentwere 0 12 v 0d13, at 3 hours 0 16 v 0 14, and at6 hours 0-18 v 0X19 (ml/mm Hg/kg-1), respec-tively. Values for inspiration:expiration ratio,PEEP, arterial blood pressure, Pao2, Paco2,and pH showed no relevant differencesbetween the groups (data not shown).
OUTCOMETable 3 shows the values for duration ofartificial ventilation and total time of exposureto supplemental oxygen in surviving patients:there were no differences between the groups.An identical number of patients in each groupalso had a supplemental oxygen requirement at36 weeks' postconceptional age.One Curosurf baby died at the age of 18
days from massive hepatic bleeding followingsurgical repair for spontaneous intestinalperforation. In the Survanta group two infantsdied from grade IV ICH, two from acutecardiocirculatory failure (one had tensionpneumothorax), and one due to respiratoryfailure probably related to lung hypoplasiaafter premature rupture of the membranes 17days before delivery. Age at death rangedbetween 1 and 2 days.Data on the treatment comparison for
pulmonary and extrapulmonary complica-tions are listed in table 4. The incidences ofmost of the complications were lower in theCurosurf group, but with the small number ofpatients these trends towards favourable out-come following Curosurf treatment did notreach significance. The adjusted ORs given intable 4 represent the results of risk calcula-tions for the effect of the treatment regimen(Curosurf v Survanta) on the 28 day outcomevariables controlled for the influence of birthweight, sex, and collaborating centre and thusdo not reflect imbalances between treatmentgroups with respect to these prognosticfactors.
Treatment administration problems wereonly observed in Survanta infants, probablyreflecting the larger volume of the surfactantdose. Reflux of administered surfactant wasobserved in three, and oxygen saturation of lessthan 85% in two babies five minutes afteradministration.
DiscussionThe results of our pilot trial show that infantstreated with Curosurfhad less oxygen and ven-tilator requirements than babies treated withSurvanta. Although the long term measures ofoutcome favoured the Curosurf infants, thedifferences were not significant. These results,however, provide a sound basis for an accuratesample size calculation for the large scale trialto follow; a reduction from 25% to 15% for theoccurrence of the primary endpoint 'death orBPD' is a reasonable assumption on the differ-ence to be detected. Thus, a total of 708infants is required in the definitive study to find

F12 Speer, Gefeller, Groneck, et al
Table 4 Comparison of 28 day outcome measurements with crude and adjusted odds ratios (OR) and 95% confidenceintervals (CI) as well as corresponding p values in Curosurf (n=33) and Survanta (n= 40) treated babies
Curosuf Survanta OR OR 95% CI of pOutcome measurements No/% No/% crude* adjusted** adjusted OR ValuetPulmonary interstitial emphysema 1 (3 0) 4 (10-0) 0-28 0 30 0-03-3-42 0 33Pneumothorax 2 (6-1) 5 (12-5) 0 45 0 49 0-08-2-88 0 43Intracerebral haemorrhage
Total 7 (21-2) 14 (35-0) 0 50 044 0-14-1-36 0-15Grades 3-4 1 (3 0) 5 (12 5) 0-22 0-18 0-02-1-78 0-14
Persistent ductus arteriosus 18 (54-6) 12 (30 0) 2 80 2-83 0-98-8-21 0-06Bronchopulmonarydysplasiat 4 (12-5) 4 (11-4) 1 11 1-03 0-21-5 21 0-97Pulmonary haemorrhage 0 (0) 1 (2-5) - - -
Septicaemia:Total No 12 (36-4) 11 (27 5) 1-51 1-33 0-37-4-81 0-66Onset 62 days 6 (18-2) 4 (10-0) 1-94 1-55 0-32-7-43 0-58Onset>2 days 6 (18-2) 7 (17-5) 1-05 1-02 0-24-4-30 0-98
Mortality 1 (3-0) 5 (12-5) 0-22 0-23 0-02-2-54 0-23
*Derived from the fourfold table of treatment times outcome.**Derived from the logistic model incorporating covariate information.tDerived from the test in the logistic model whether the adjusted OR equals 1.tOxygen dependency at 36 weeks' postconceptional age.
such a difference with 90% power using a two-sided test at a significance level of 5%.
In general, the data of the present pilot studymust be interpreted with caution. The trendtowards favourable 28 day outcome inCurosurf treated infants has to be viewed in thelight of the small number of babies enrolled inthe study and the non-blind trial design.Although we are not aware of any systematicbias in the assessment of outcome measures,we cannot rule out this possibility. However,additional data analysis stratified by collaborat-ing centre did not indicate heterogeneity in ourresults. Thus, if systematic bias were present itwould have to be the same in all centres, whichseems unlikely.There are at least three possible explana-
tions for the improved lung function in theCurosurf treated babies during the first 24hours. These are, firstly, that the trial collabo-rators had more experience with the porcinesurfactant preparation; secondly, the Curosurfis a more effective surfactant than Survanta;and thirdly, that the dose of phospholipids -namely, 200 mg/kg v 100 mg/kg was critical.The first explanation seems very unlikely.
Although the collaborating neonatologists haveparticipated in previous Curosurf trials,4 6 theirexpertise in administering Survanta is compar-able as each of the centres had been usingSurvanta in routine clinical practice for manymonths before the trial started.The two surfactant preparations used in the
present trial differ in some potentially import-ant biophysical characteristics. Curosurf andSurvanta are both derived from minced animallungs by washing and extraction with organicsolvents; this latter procedure removes watersoluble components including the surfactantassociated apoproteins SP-A and SP-D, leav-ing only hydrophobic constituents with about1% SP-B and SP-C. Curosurf is further 'puri-fied' by a liquid-gel chromatography procedureremoving neutral lipids such as triacylglycerol,cholesterol, and cholesteryl esters.'1 Survanta,in contrast, is enriched with synthetic DPPC,triacylglycerol, and palmitic acid to standardiselipid composition and reduce film compress-ibility. It is not clear how these differentmodifications of the surfactant preparationsinfluence their physiological properties underin vivo conditions. Nohara et al confirmed that
in vitro film compressibility of a bovine equiva-lent to Curosurf could indeed be lowered byenrichment with synthetic lipids 20; however,this was associated with retarded spreadingand did not seem to improve furtherphysiological variables of lung mechanics inventilated immature newborn rabbits.The present trial was designed to investigate
whether these differences in biochemicaland biophysical properties between the twopreparations would have an impact on theirclinical effects in babies with RDS. We realisethat, under optimal trial conditions, Curosurfand Survanta should have been given atidentical doses and treatment intervals in ablind manner. However, this was not possible,as different treatment regimens were alreadyestablished for each of the two surfactants. Thetrial design thus implied that Curosurf wasgiven at a larger initial dose, whereas themaximum dose during the first two days ofpostnatal life was the same for the two prepara-tions. We found that, after administration ofeither Curosurf or Survanta, there was a rapidimprovement of gas exchange, as reflected by asignificant increase in a:APO2, and FiO2 couldtherefore be reduced in both groups of babies.However, five minutes to 24 hours after surfac-tant replacement Curosurf treated infantsneeded less oxygen than patients in theSurvanta group and had a more noticeableimprovement in a:APO2. Apparently, theeffect of the Survanta treatment regimen wasdelayed.At some time points PIP and MAP were
significantly lower in the Curosurf group thanin the Survanta group. Five minutes afterinstillation of Survanta a slight increase inmedian PIP was observed; this phenomenoncould have been due to the larger volume ofthe initial Survanta dose compared with theCurosurf dose. The superior improvement inoxygenation and ventilatory pressure in theCurosurf group may reflect the higher initialdose (200 mg/kg Curosurf v 100 mg/kgSurvanta) or the different preparation. Thedifference in ventilatory requirementsbetween the groups might explain the trendtowards the lower incidence of PIE and pneu-mothorax in Curosurf babies compared withSurvanta babies. There was also a trendtowards lower incidence of ICH in the

Comparison of two natural surfactants in RDS F13
Curosurf group; severe ICH was present inonly one (3%) of the Curosurf treated infantsand in five (12.5%) patients in the Survantagroup. Our data support the concept thatbabies with RDS benefit from receiving a highinitial dose4 and also indicate that a highinitial dose reduces the need for retreatment.Each administration procedure, whichinvolves deconnection from the ventilator andinstillation of fluid into the airways, is poten-tially traumatic and usually associated with aslight drop in arterial blood pressure,21 andmay even lead to transient depression of cere-broelectrical activity.22
In summary, we feel confident in concludingthat preterm infants with RDS treated accord-ing to the Curosurf regimen had improvedoxygenation and reduced ventilatory require-ments during the first 24 hours compared withSurvanta treated neonates. There was also atrend towards lower incidence of air leaks andsevere ICH in babies receiving Curosurf.These findings need to be confirmed in a largerrandomised trial.The trial was supported in part by a research grant from ChiesiFarmaceutici SpA, Parma, Italy, but was designed, conducted,and analysed independently of the company.The trial is dedicated to our friend and trial collaborator Dr
Edgar Laufkotter, who died in April 1994.We are grateful for the support given by the attending inten-
sive care nurses and neonatologists in all contributing units andacknowledge the assistance of Mrs Astrid Becker-Keymling inall organisational aspects of the trial.
1 Jobe AH. Pulmonary surfactant therapy. N Engl J Med1993; 328: 861-8.
2 Horbar JD, Wright LL, Soll RF, Wright EC, Fanaroff AA,Korones SB, et al. A multicentre randomized trial com-paring two surfactants for the treatment of neonatal res-piratory distress syndrome. J Pediatr 1993; 123: 757-66.
3 Collaborative European Multicenter Study Group.Surfactant replacement therapy for severe neonatal res-piratory distress syndrome: an international randomizedclinical trial. Pediatrics 1988; 82: 683-91.
4 Speer CP, Robertson B, Curstedt T, Halliday HL,Compagnone D, Gefeller 0, et al. Randomized Europeanmulticenter trial of surfactant replacement therapy forsevere neonatal respiratory distress syndrome: single ver-sus multiple doses of Curosurf. Pediatrics 1992; 89:13-20.
5 Egberts J, de Winter JP, Sedin G, de Kleine NJK, BrobergerU, van Bel 0, et al. Comparison of prophylaxis and rescuetreatment with Curosurf in babies less than 30 weeks ges-tation. A randomized trial. Pediatrics 1993; 92: 768-74.
6 Halliday HL, Tarnow-Mordi WO, Corcoran JD, PattersonCC. A multicentre randomised trial comparing high andlow dose surfactant regimens for the treatment of respira-tory distress syndrome (the Curosurf 4 trial). Arch DisChild 1993; 69: 276-80.
7 Horbar JD, Soll RF, Sutherland JM, Kofagal U, PhilipAGS, Kessler DL, et al. A multicenter randomized,placebo-controlled trial of surfactant therapy for respira-tory distress syndrome. NEnglJMed 1989; 320: 959-65.
8 Soll RF, Hoekstra RE, Fangman JJ, Corbet AJ, Adams JM,James LS, et al. Multicenter trial of single-dose modifiedbovine surfactant extract (Survanta) for prevention ofrespiratory distress syndrome. Pediatrics 1990; 85:1092-102.
9 Hoekstra RE, Jackson JC, Myres TF, Frantz JD, Stem ME,Powers WF, et al. Improved neonatal survival followingmultiple doses of bovine surfactant in very prematureneonates at risk for respiratory distress syndrome.Pediatrics 1991; 88: 10-18.
10 Fujiwara T, Robertson B. Pharmacology of exogenoussurfactant. In: Robertson B, van Golde LMG, BattenburgJJ, eds. Pulmonary surfactant: from molecular biology to clinicalpractice. Amsterdam: Elsevier Science, 1992: 561-92.
11 Robertson B, Curstedt T, Johansson J, J6mvall H,Kobayashi T. Structural and functional characterizationof porcine surfactant isolated by liquid-gel chromato-graphy. In: von Wichert P, Muller B, eds. Basic research onlung surfactant. Progress in Respiration Research. Vol 25.Basel: Karger, 1990: 237-46.
12 Liechty EA, Donovan E, Purohit D, Gilhooly J, FeldmannB, Noguchi A, et al. Reduction of neonatal mortality aftermultiple doses of bovine surfactant in low birth weightneonates with respiratory distress syndrome. Pediatrics1991; 88: 19-28.
13 Speer CP, ReuB3 D, Harms K, Herting E, Gefeller 0.Neutrophil elastase and acute pulmonary damage ininfants with severe respiratory distress syndrome.Pediatrics 1993; 91: 794-9.
14 Papile LA, Burstein J, Burstein R, Koffler H. Incidence andevolution of subependymal and intraventricular hemor-rhage: a study of infants birth weight less than 1500 g.jPediatr 1978; 92: 529-34.
15 Fawer CL, Diebold P, Calame A. Periventricular leucoma-lacia and neurodevelopmental outcome in preterminfants. Arch Dis Child 1987; 62: 30-6.
16 Speer CP, Rethwilm M, Gahr M. Elastase-oal-proteinaseinhibitor: an early indicator of septicemia and bacterialmeningitis in children. J Pediatr 1987; 111: 667-71.
17 Newell DJ. Intention-to-treat analysis: implications forquantitative and qualitative research. IntJEpidemiol 1992;21:837-41.
18 Kalbfleisch JD, Prentice RL. The statistical analysis offailuretime data. New York: John Wiley and Sons, 1980.
19 Hosmer DW, Lemeshow S. Applied logistic regression. NewYork: John Wiley and Sons, 1989.
20 Nohara K, Berggren P, Curstedt T, Grossman G, NilssonR, Robertson B. Correlations between physical andphysiological properties of various preparations of lungsurfactant. EurJRespirDis 1986; 69: 321-35.
21 Skov K. Hellstr6m-Westas L, Jacobsen T, Greisen G,Svenningsen NW. Acute changes in cerebral oxygenationand cerebral blood volume in preterm infantsduring surfactant treatment. Neuropediatrics 1992; 23:126-30.
22 Hellstr6m-Westas L, Bell AH, Skov L, Greisen G,Svenningsen NW. Cerebroelectrical depression followingsurfactant treatment in preterm neonates. Pediatrics 1992;89: 643-7.