Embed Size (px)
Citation preview


By
Khaled Saad ZaghloulKhaled Saad Zaghloul


Interstitial lung diseases (ILDs) in childhood are a diverse group of conditions that primarily involve the alveoli and perialveolar tissues, leading to derangement of gas exchange, restrictive lung physiology, and diffuse infiltrates on radiographs.
Because ILDs can involve the distal airspaces as well as the interstitium, the term diffuse infiltrative lung disease has been suggested. This nomenclature may be more accurate than ILD, but children's interstitial lung disease (chILD) has become the preferred term.
Chronic interstitial lung disease (ILD) Chronic interstitial lung disease (ILD) in children is defined as the presence in children is defined as the presence of respiratory symptoms, diffuse of respiratory symptoms, diffuse infiltrates on chest radiographs, infiltrates on chest radiographs, abnormal pulmonary function tests abnormal pulmonary function tests with evidence of restrictive with evidence of restrictive ventilatory defect and/or impaired gas ventilatory defect and/or impaired gas exchange, and persistence of these exchange, and persistence of these findings for >3 months with findings for >3 months with considerable mortality and morbidity.considerable mortality and morbidity.
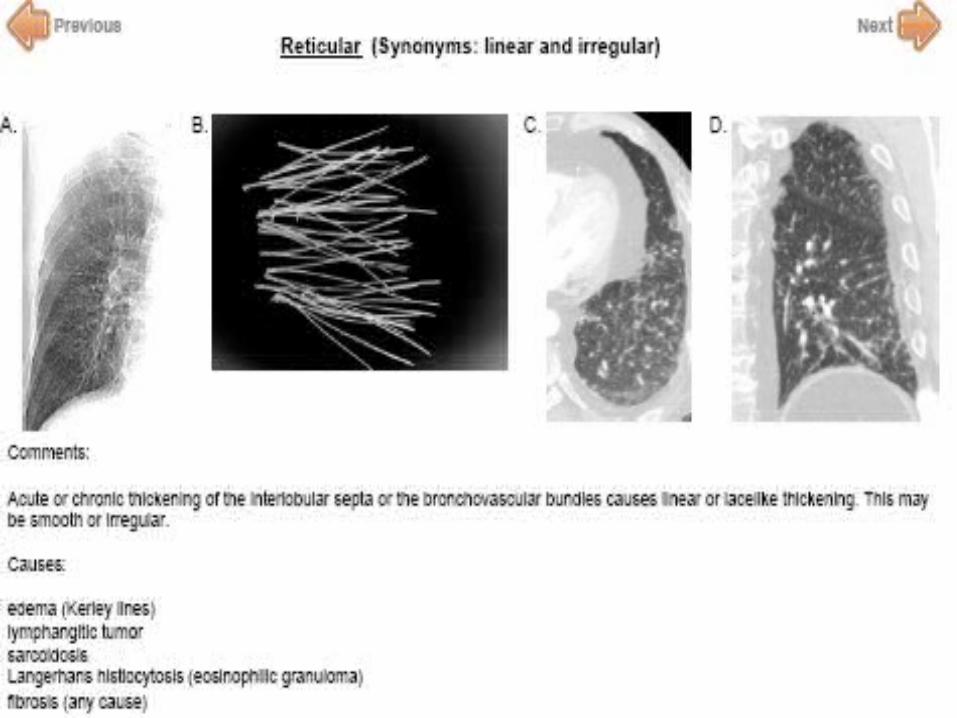
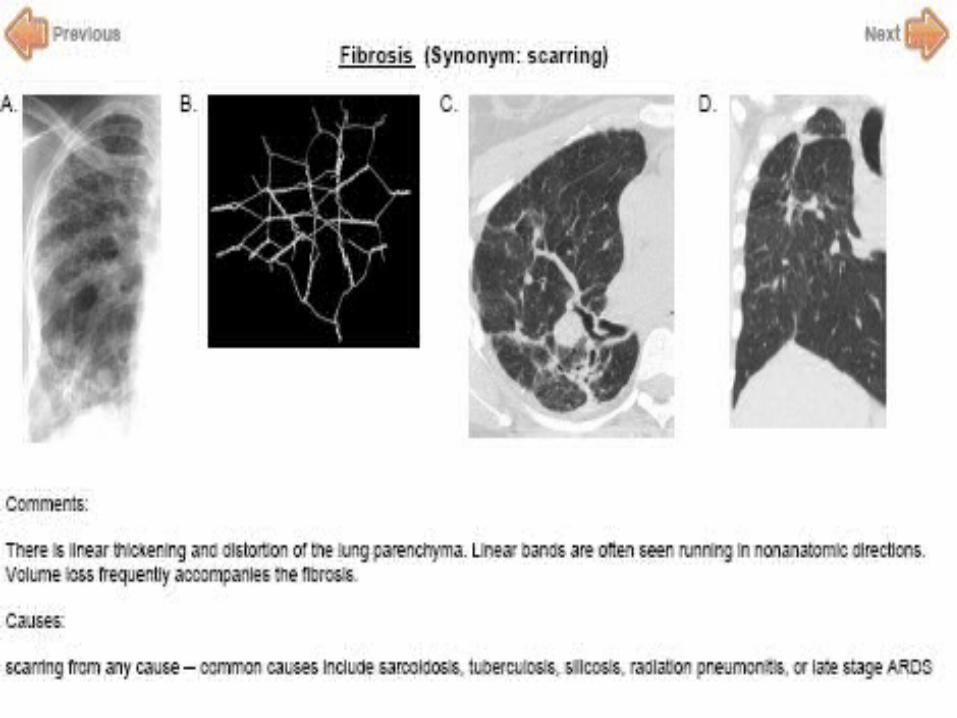
The interstitium of the lung is not normally visible radiographic- ally; it becomes visible only when disease (e.g., edema, fibrosis, tumor) increases its volume and attenuation.
The interstitium of the lung is not normally visible radiographic- ally; it becomes visible only when disease (e.g., edema, fibrosis, tumor) increases its volume and attenuation.
The interstitial space is defined as continuum of loose connective tissue throughout the lung composed of three subdivisions: The interstitial space is defined as continuum of loose connective tissue throughout the lung composed of three subdivisions:
(i) the bronchovascular, surrounding the bronchi, arteries, and veins from the lung root to the level of the respiratory bronchiole.
(i) the bronchovascular, surrounding the bronchi, arteries, and veins from the lung root to the level of the respiratory bronchiole.(ii) the parenchymal (acinar), situated between the alveolar and capillary basement membranes.(ii) the parenchymal (acinar), situated between the alveolar and capillary basement membranes.
(iii) the subpleural, situated beneath the pleura, as well as in the interlobular septae.(iii) the subpleural, situated beneath the pleura, as well as in the interlobular septae.
The Lung Interstitium

Pathophysiology
The pathophysiology The pathophysiology is more complex is more complex than adult disease than adult disease because the injury because the injury occurs during the occurs during the process of lung process of lung growth and growth and differentiation.differentiation.
In ILD, the initial injury causes damage In ILD, the initial injury causes damage to the alveolar epithelium and capillary to the alveolar epithelium and capillary endothelium.endothelium.
Abnormal healing of injured tissue may Abnormal healing of injured tissue may be more prominent than inflammation be more prominent than inflammation in the initial steps of the development in the initial steps of the development of chronic ILD.of chronic ILD.

The development of a chronic inflammatory response was thought to perpetuate the recruitment of inflammatory and immunoregulatory cells into the interstitium, alveolar walls and perialveolar tissues, progressively leading to a thickened alveolar wall with extensive fibrosis and loss of the alveolar gas exchange function..

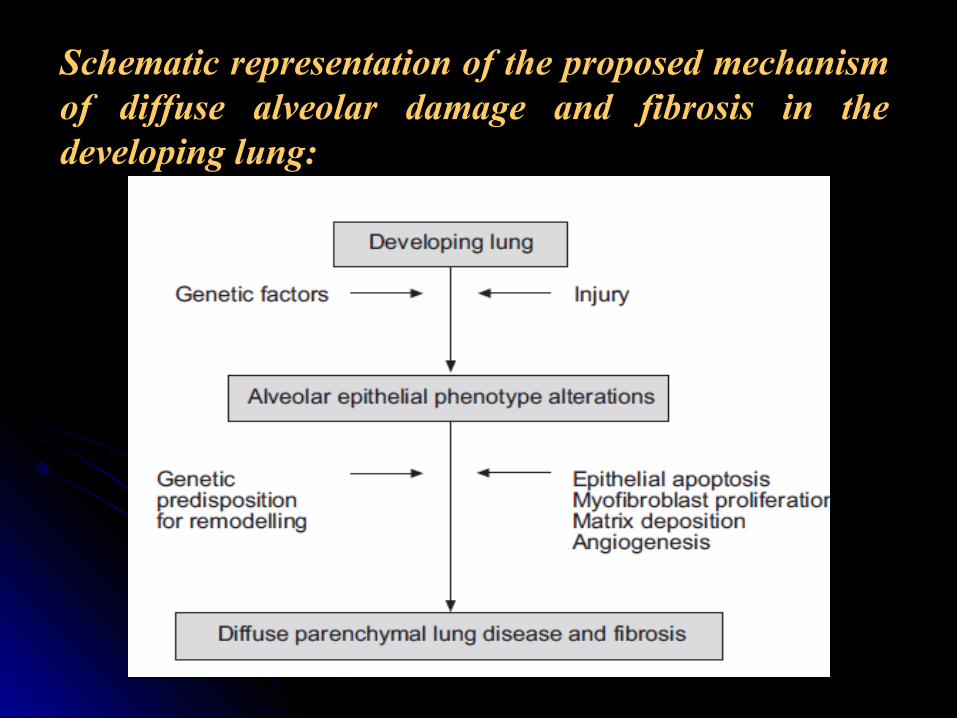
Schematic representation of the proposed mechanism of diffuse alveolar damage and fibrosis in the developing lung:
CLASSIFICATION OF ILD
The classification of ILd in children is The classification of ILd in children is not characterized but it is helpful to not characterized but it is helpful to separate diseases into those of known separate diseases into those of known and unknown etiology.and unknown etiology.

INTERSTIAL LUNG DISEASES OF KNOWN ETIOLOGYAspiration syndromesChronic infection Bronchopulmonary dysplasiaHypersensitivity pneumonitis ( drugs,
environment or occupation associated )Surfactant B or C deficiency
Drugs include: Antibiotics (penicillin, Antibiotics (penicillin, nitofurantin, cephalosporines, isoniazid, nitofurantin, cephalosporines, isoniazid, sulfonamides), anticancer therapies, drugs sulfonamides), anticancer therapies, drugs of abuse, radiation.of abuse, radiation.
Environment or occupation exposure include: inorganic and organic dust, gases (fumes, vapors ), hydrocarbons, resins and nitrogen oxides.
INTERSTIAL LUNG DISEASES OF UNKNOWN ETIOLOGY Usual Interstial pneumonitisUsual Interstial pneumonitis (UIP)(UIP) Desquamative pneumonitis ( DIP )Desquamative pneumonitis ( DIP ) Lymphocytic Interstial pneumonitis (LIP ) and Lymphocytic Interstial pneumonitis (LIP ) and
related disordersrelated disorders Nonspecific Interstial pneumonitisNonspecific Interstial pneumonitis Pulmonary hemosiderosisPulmonary hemosiderosis Goodpasture diseaseGoodpasture disease Pulmonary infiltrates with eosinophiliaPulmonary infiltrates with eosinophilia Pulmonary Interstial glycogenosis (PIG )Pulmonary Interstial glycogenosis (PIG )
INTERSTIAL LUNG DISEASES OF UNKNOWN ETIOLOGY Neuroendocrine cell hyperplasia in infancy Neuroendocrine cell hyperplasia in infancy (NEHI)(NEHI) Bronchiolitis obliteransBronchiolitis obliterans Bronchiolitis obliterans with organizing Bronchiolitis obliterans with organizing pneumonia (BOOP )pneumonia (BOOP ) Alveolar proteinosisAlveolar proteinosis Pulmonary vascular disordersPulmonary vascular disorders Pulmonary lymphatic disordresPulmonary lymphatic disordres Pulmonary microlithiasisPulmonary microlithiasis

OTHER DISORDERS WITH PULMONARY INVOLVMENT
Connective tissue disorders ( Rheumatoid Connective tissue disorders ( Rheumatoid arthritis, SLE, Dermatomyositis )arthritis, SLE, Dermatomyositis )
MalignanciesMalignancies Langerhans cell histocytosisLangerhans cell histocytosis SarcoidosisSarcoidosis Wegener granulomatosisWegener granulomatosis Neurocutaneous syndromes: Neurocutaneous syndromes:
(neurofibromatosis, tuberous sclerosis)(neurofibromatosis, tuberous sclerosis)
OTHER DISORDERS WITH PULMONARY INVOLVMENT
Storage diseases Gaucher disease, Niemann-Storage diseases Gaucher disease, Niemann-Pick disease )Pick disease )
Hemansky-Pudlak syndromeHemansky-Pudlak syndrome
Clinico-pathologic classification of interstitial and diffuse lung disease in
childhood

I. Disorders more prevalent in infancy
Diffuse developmental disorders Acinar/alveolar dysgenesis; alveolar capillary dysplasia with misalignment of pulmonary veins (ACD-MPV)
Lung growth abnormalities Pulmonary hypoplasia, chronic neonatal lung disease (BPD)
Specific conditions of unknown or poorly understood etiology
Neuroendocrine cell hyperplasia of infancy (NEHI), pulmonary interstitial glycogenosis (P.I.G.)
Surfactant dysfunction disorders SFTPB, SFTPC, ABCA3, NKX2.1/TTF1, other genetic mutations

II. Disorders not specific to infancy
Disorders of the normal host ("immune intact")
Infectious/post-infectious processes, aspiration, related to environmental agents (hypersensitivity pneumonitis), eosinophilic pneumonia
Disorders of the immunocompromised host
Opportunistic infections, related to therapeutic intervention, related to transplantation or rejection syndromes
Disorders related to systemic disease processes
Immune-mediated disorders (eg, connective tissue disorders such as SLE, polymyositis/dermatomyositis, and systemic sclerosis), storage disease, sarcoidosis, Langerhans cell histiocytosis, malignant infiltrates
Disorders masquerading as ILD Arterial, venous, lymphatic disorders
Unclassified Captures cases of ILD that cannot be classified for any reason. Common reasons include end-stage disease, nondiagnostic biopsies, or inadequate biopsy material.

EpidemiologyILD is rare in children. Cases tend to cluster
in infancy, and 10-16% appear to be familial. A national survey of cases of chronic ILD in immunocompetent children aged 0-16 years in the United Kingdom and Ireland over a three year period (1995-1998) yielded an estimated prevalence of 3.6 per million.
Clinical ManifestationsHistory: Diagnosing children's interstitial History: Diagnosing children's interstitial
lung disease (chILD) requires a high index lung disease (chILD) requires a high index of suspicion on the part of the physician. of suspicion on the part of the physician. The delay between the onset of symptoms The delay between the onset of symptoms and ultimate diagnosis is often months to and ultimate diagnosis is often months to years. Respiratory symptoms can be subtle years. Respiratory symptoms can be subtle in infants and children, and clinicians often in infants and children, and clinicians often treat ILD as asthma. A delay in referral can treat ILD as asthma. A delay in referral can lead to clinically significant remodeling of lead to clinically significant remodeling of the lung before diagnosis.the lung before diagnosis.
Clinical ManifestationsThe clinical history varies by age. The onset The clinical history varies by age. The onset
of disease is often insidious, with caregivers of disease is often insidious, with caregivers or patients unsure when the illness actually or patients unsure when the illness actually began. Occasionally, patients present with began. Occasionally, patients present with relatively few symptoms but with abnormal relatively few symptoms but with abnormal findings on chest radiographs or pulmonary findings on chest radiographs or pulmonary function tests (PFTs). Some patients, function tests (PFTs). Some patients, especially newborns with surfactant-especially newborns with surfactant-dysfunction mutations (SDMs), may present dysfunction mutations (SDMs), may present with respiratory failure.with respiratory failure.
Tachypnea and/or dyspneaTachypnea and/or dyspneaTachypnea is present in most patients Tachypnea is present in most patients (75%), particularly in infants.(75%), particularly in infants.Younger infants manifest retractions, Younger infants manifest retractions, difficulty in feeding, and diaphoresis difficulty in feeding, and diaphoresis with feeding. Cyanosis may be evident with feeding. Cyanosis may be evident during feeding or at rest.during feeding or at rest.Exercise intolerance is often noted in Exercise intolerance is often noted in older childrenolder children

A A coughcough that is described as dry and that is described as dry and nonproductive is commonly present nonproductive is commonly present (75%) and can be the only symptom of (75%) and can be the only symptom of ILD, even in the newborn.ILD, even in the newborn.
Failure to thrive Failure to thrive and weight loss are and weight loss are common symptoms that may result common symptoms that may result from anorexia, difficulty in feeding, from anorexia, difficulty in feeding, and increased energy expenditure from and increased energy expenditure from increased work of breathing.increased work of breathing.

HemoptysisHemoptysis may indicate the presence may indicate the presence of a vasculitic process or a pulmonary of a vasculitic process or a pulmonary hemorrhage syndrome.hemorrhage syndrome.
Older children may report Older children may report chest painchest pain..FeverFever may be present, suggesting may be present, suggesting
infectious or inflammatory causes.infectious or inflammatory causes.WheezingWheezing occurs in 40% of patients, occurs in 40% of patients,
according to the history, and is present according to the history, and is present upon examination in as many as 20%.upon examination in as many as 20%.
A careful family history is critical A careful family history is critical because some forms of ChILD may because some forms of ChILD may have a genetic basis, which may be have a genetic basis, which may be associated with neonatal deaths, associated with neonatal deaths, unexplained childhood respiratory unexplained childhood respiratory disease, or ILD in adults disease, or ILD in adults
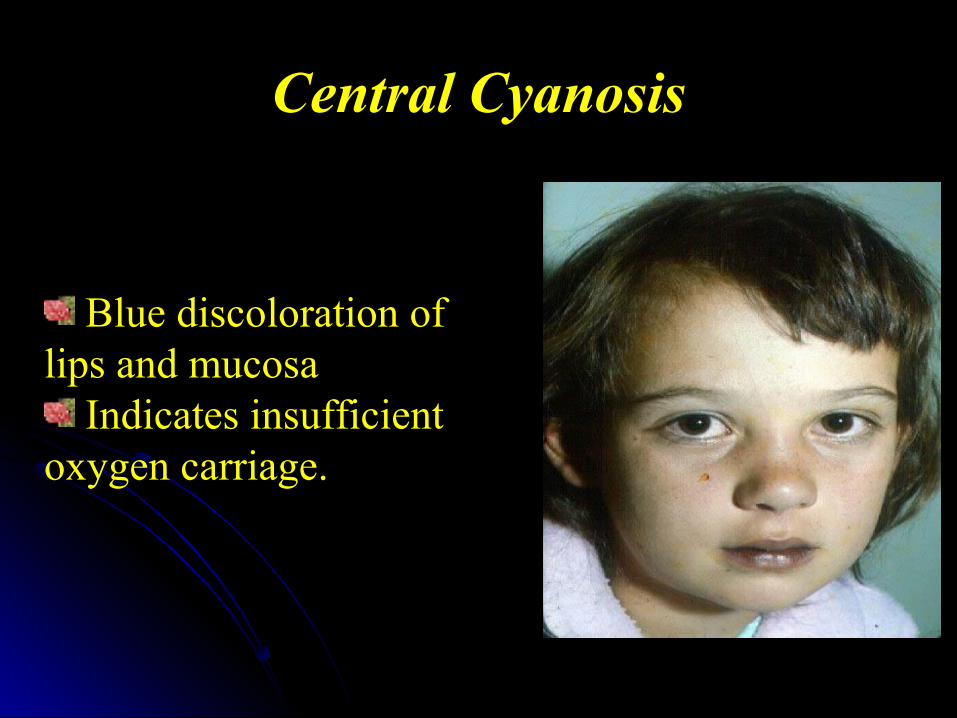
Central Cyanosis
Blue discoloration oflips and mucosa
Indicates insufficientoxygen carriage.
General physical findingsGeneral physical findings
Growth retardation, signs of weight loss, Growth retardation, signs of weight loss, and/or failure to thrive may be evident.and/or failure to thrive may be evident.
Hypoxemia on room air is common (87% of Hypoxemia on room air is common (87% of patients with saturation below 90% in one patients with saturation below 90% in one series).series).
Desaturation may occur during sleep, Desaturation may occur during sleep, during feeding (infants), or with exercise.during feeding (infants), or with exercise.
Auscultation may reveal normal findings or Auscultation may reveal normal findings or dry crackles.dry crackles.

Signs of hyperinflation, such as increased Signs of hyperinflation, such as increased chest diameter or palpable liver and spleen chest diameter or palpable liver and spleen may be evident.may be evident.
Signs consistent with pulmonary Signs consistent with pulmonary hypertension may be present. hypertension may be present.
Cyanosis and clubbing are late Cyanosis and clubbing are late manifestations of ILD.manifestations of ILD.
Stigmata of collagen vascular diseases, Stigmata of collagen vascular diseases, vasculitides, and other systemic disorders vasculitides, and other systemic disorders should be carefully sought.should be carefully sought.

Clubbing of fingers
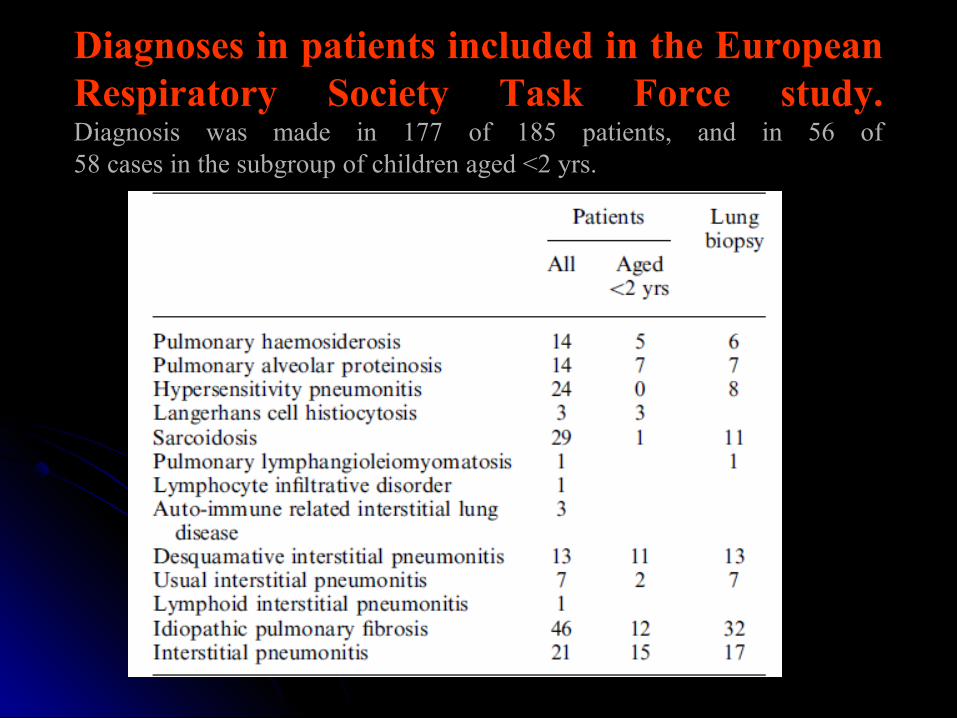
Diagnoses in patients included in the European Respiratory Society Task Force study.Diagnosis was made in 177 of 185 patients, and in 56 of58 cases in the subgroup of children aged <2 yrs.
DIAGNOSIS OF ILD

Systematic Approach to Systematic Approach to DiagnosisDiagnosis
Infant PFTs BAL
HRCT

Evaluation of ILDs in children HRCT, hig-resolution thin out computed tomography ACE, angiotensin-converting enzyme; ANCA ant neutrophil cytoplasmic antibody pHT (idiopathic) pulmonary haemosiderosis V/Q ventilation/perfusion, EPA erect posterior anterior DLCO diffusion capacity of lung for curbon monoxid
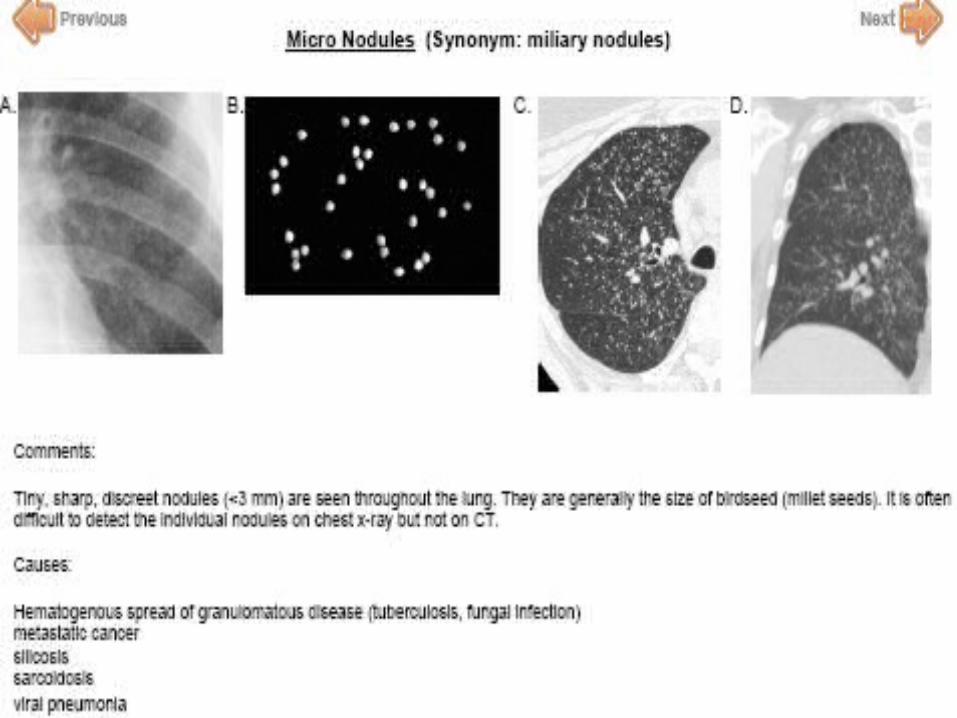
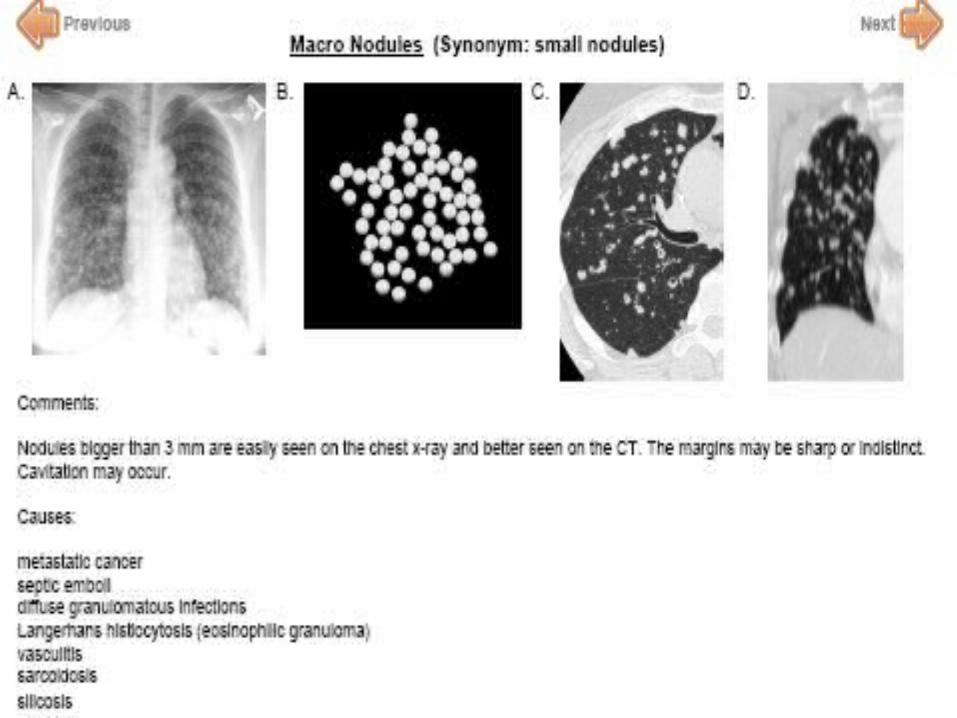
Radiography
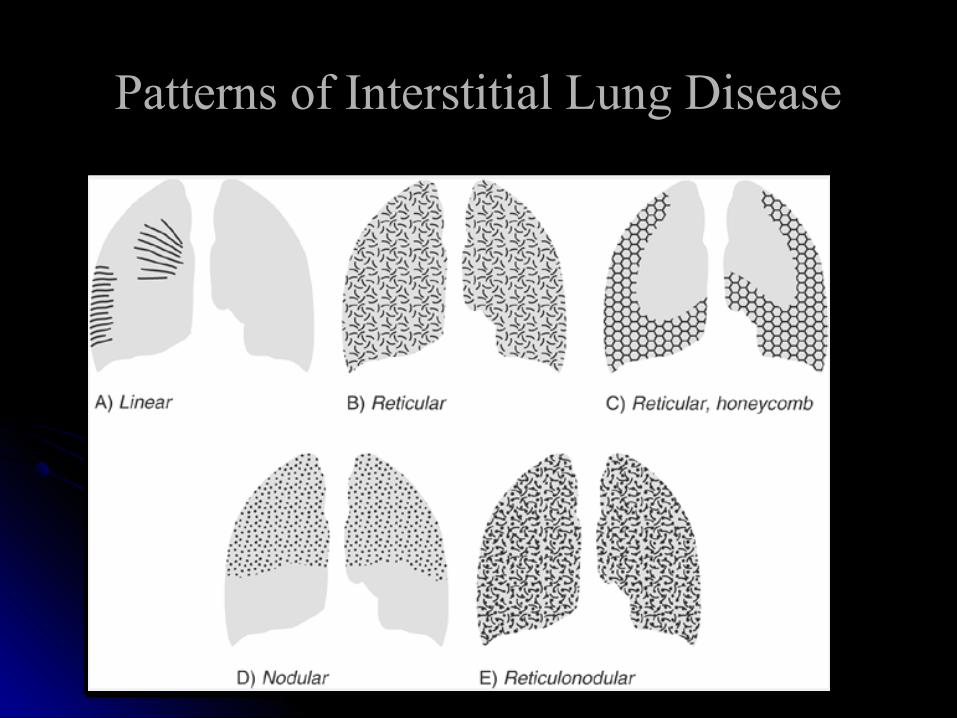
Patterns of Interstitial Lung DiseasePatterns of Interstitial Lung Disease


High-resolution CT ( HRCT )
Better defines the extent and distribution of disease.
Provides specific information for selection of a biopsy site.
Serial HRCT may be benefit in monitoring disease progression and severity.

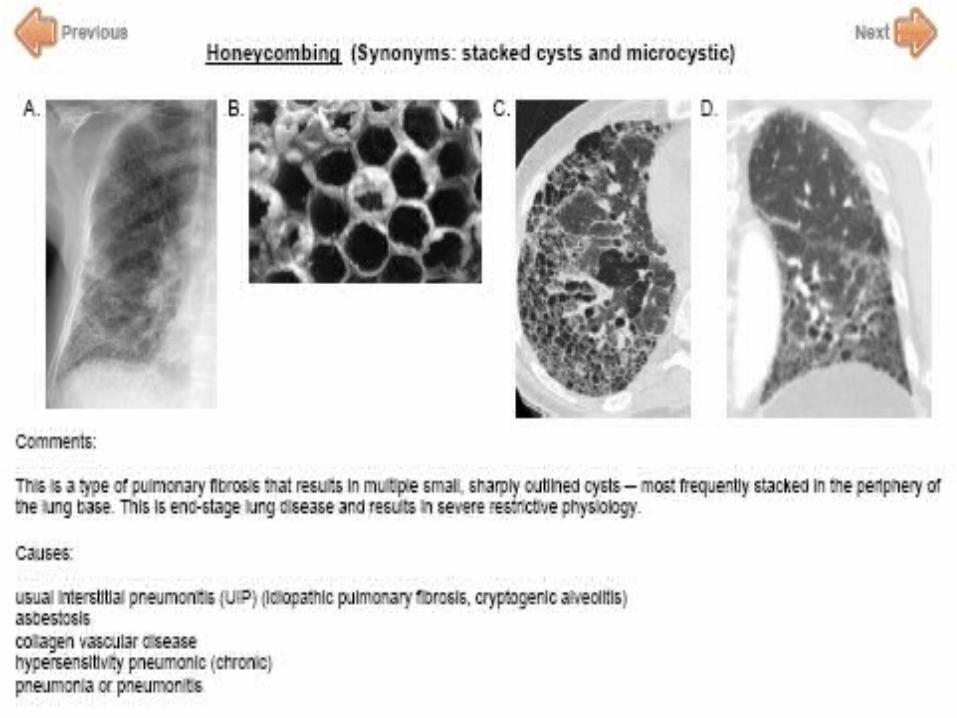
Severe honeycombing and permanent loss of functioning lung tissue
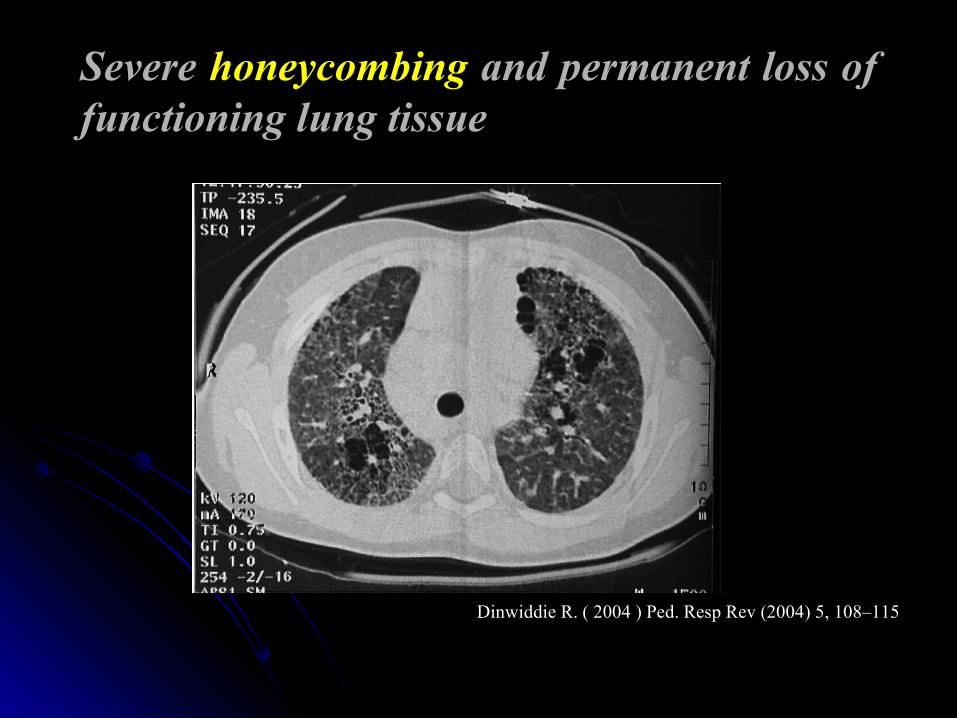
Severe honeycombing and permanent loss of functioning lung tissue
Dinwiddie R. ( 2004 ) Ped. Resp Rev (2004) 5, 108–115Dinwiddie R. ( 2004 ) Ped. Resp Rev (2004) 5, 108–115
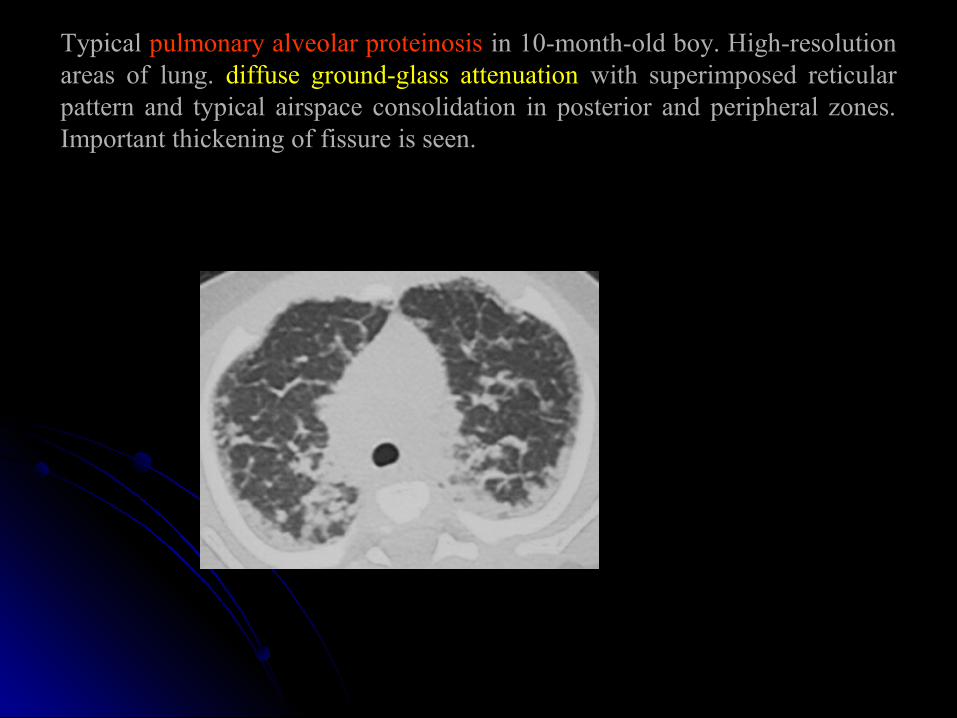
Typical pulmonary alveolar proteinosis in 10-month-old boy. High-resolution areas of lung. diffuse ground-glass attenuation with superimposed reticular pattern and typical airspace consolidation in posterior and peripheral zones. Important thickening of fissure is seen.
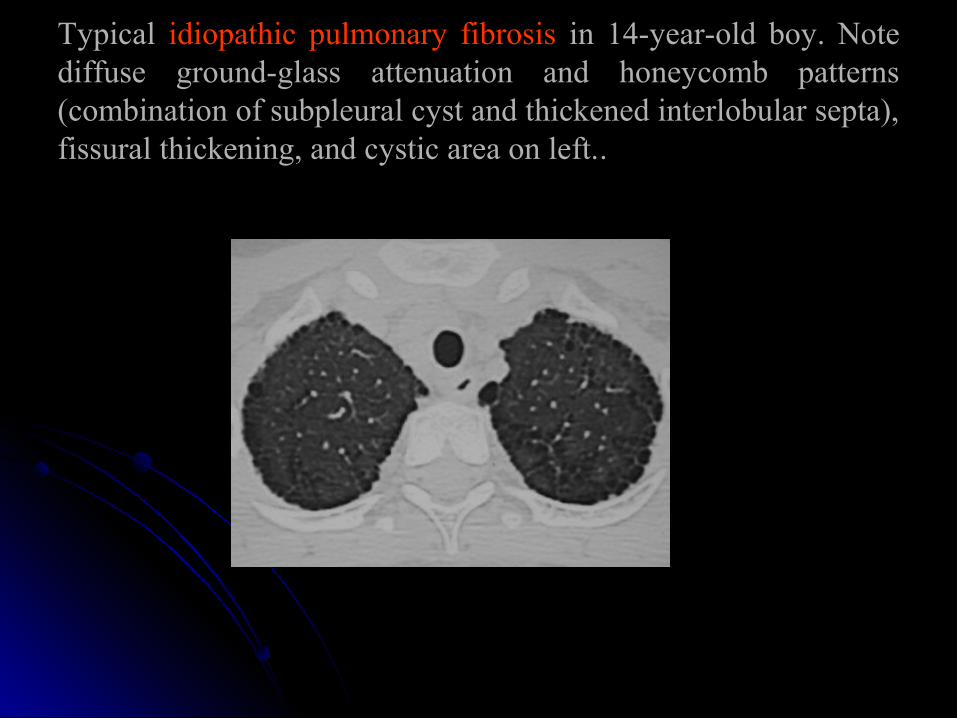
Typical idiopathic pulmonary fibrosis in 14-year-old boy. Note diffuse ground-glass attenuation and honeycomb patterns (combination of subpleural cyst and thickened interlobular septa), fissural thickening, and cystic area on left.. .
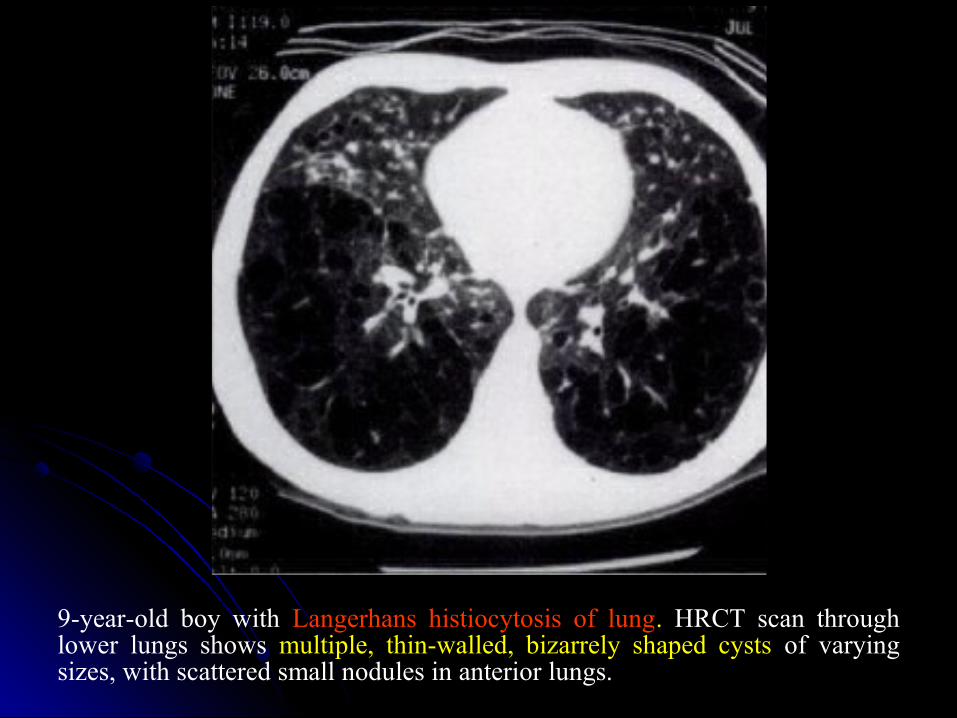
9-year-old boy with Langerhans histiocytosis of lung. HRCT scan through lower lungs shows multiple, thin-walled, bizarrely shaped cysts of varying sizes, with scattered small nodules in anterior lungs.

10-month-old female infant with biopsy-proven nonspecific interstitial pneumonitis. Thin-section CT scan of upper zones shows predominant honeycomb pattern.
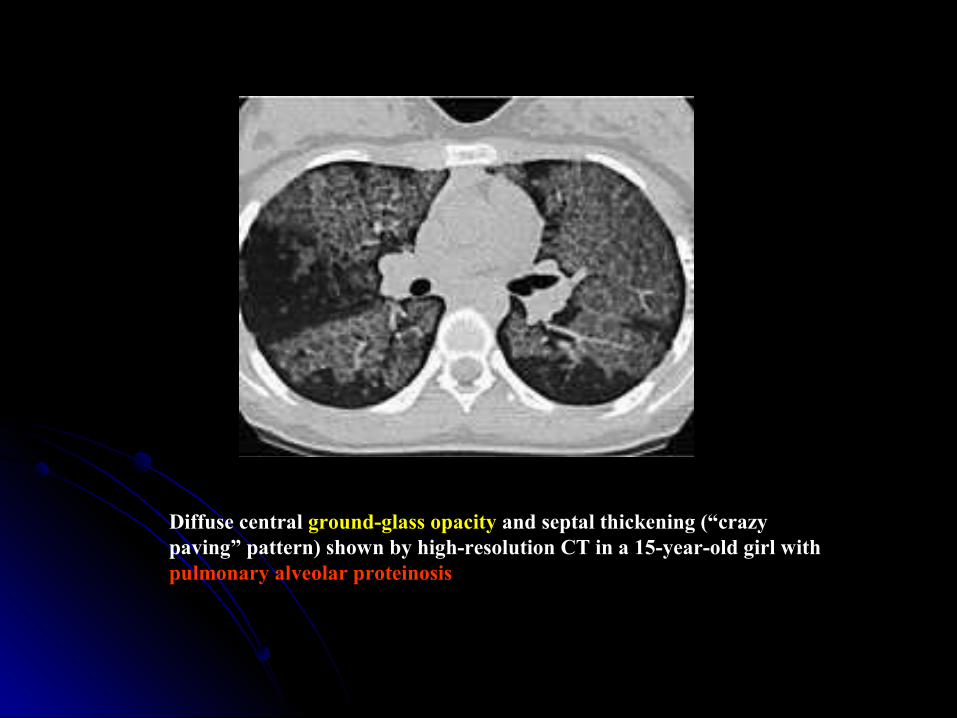
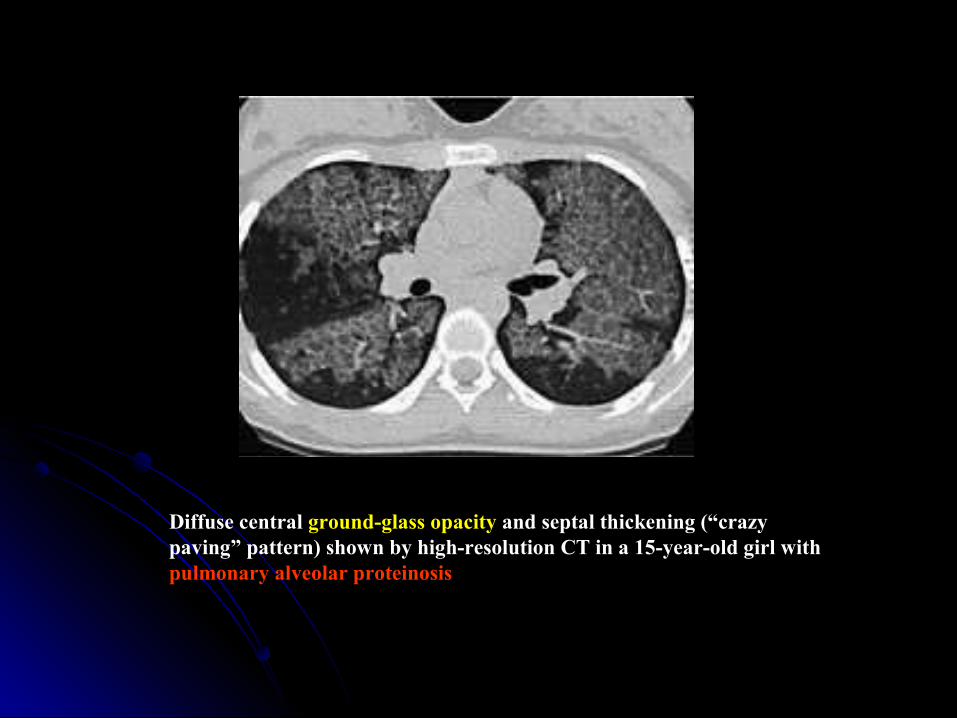
Diffuse central ground-glass opacity and septal thickening (“crazy paving” pattern) shown by high-resolution CT in a 15-year-old girl with pulmonary alveolar proteinosis
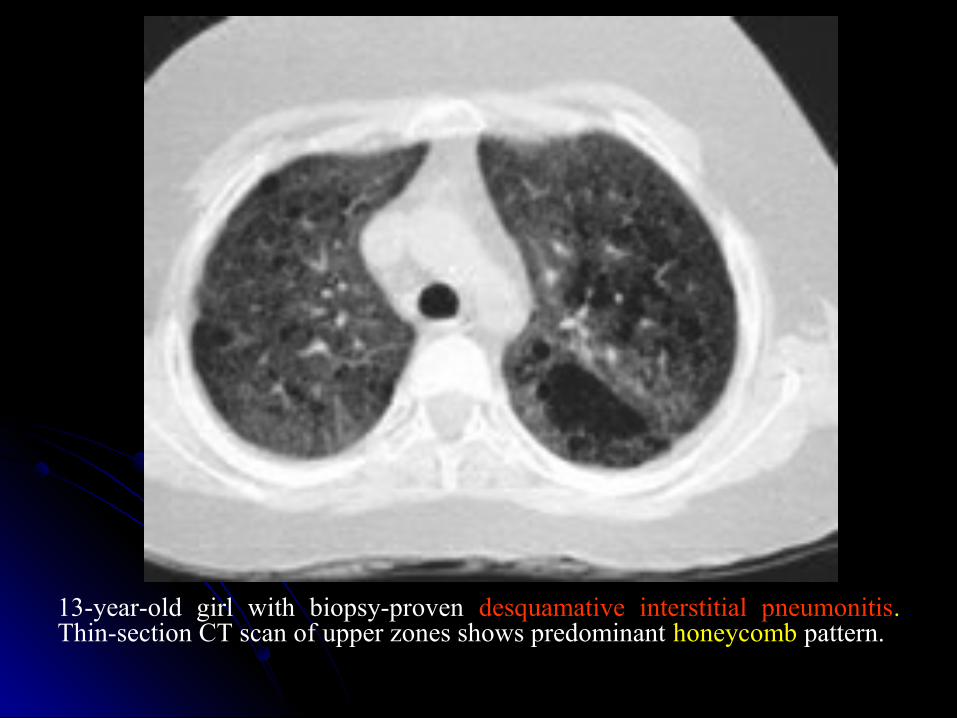
13-year-old girl with biopsy-proven desquamative interstitial pneumonitis. Thin-section CT scan of upper zones shows predominant honeycomb pattern.
Diffuse central ground-glass opacity and septal thickening (“crazy paving” pattern) shown by high-resolution CT in a 15-year-old girl with pulmonary alveolar proteinosis

Pulmonary function tests
Important in defining the degree of restrictive lung disease.
Follow up : the response to treatmentIn ILD, pulmonary function abnormalities
demonstrate a restrictive ventilatory deficit with decreased lung volume.
Bronchoalveolar lavage BAL
Provide helpful information regarding secondary infection, bleeding, or aspiration but will not usually determine the exact diagnosis.
BAL is diagnostic for pulmonary alveolar proteinosis.
Transthoracic Lung Biopsy
It is usually the final step and is necessary
For a conclusive diagnosis.
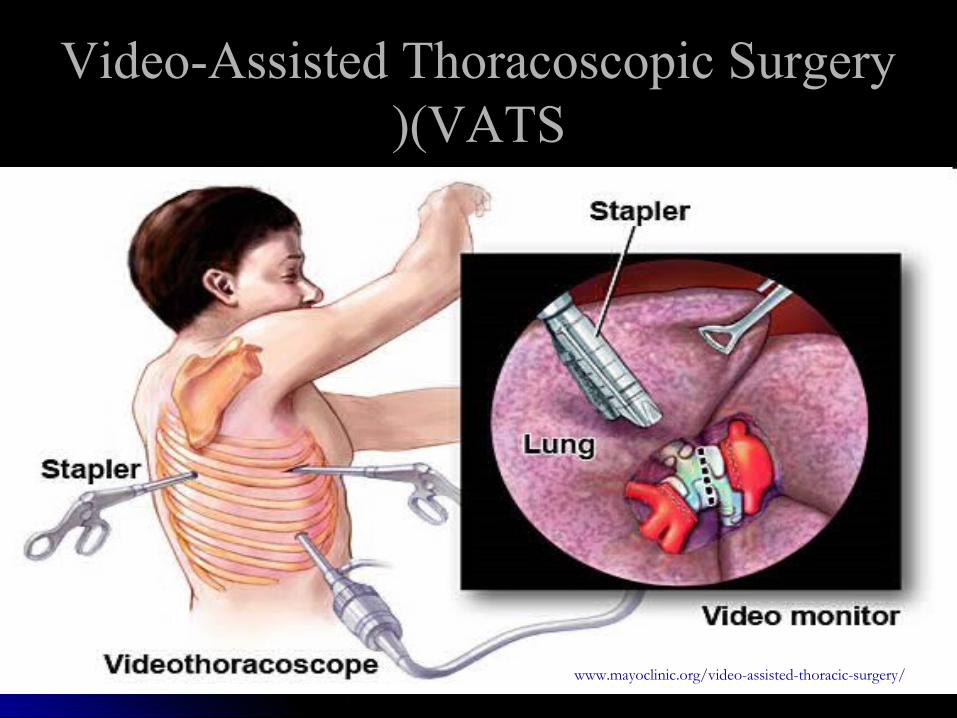
Video-Assisted Thoracoscopic Surgery Video-Assisted Thoracoscopic Surgery (VATS(VATS((
www.mayoclinic.org/video-assisted-thoracic-surgery/
Conventional thoracotomy or video-assisted thoracoscopy is used to obtain tissue from children with suspected ILD.
Evaluation for possible systemic disease may also be necessary.
MortalityThe overall mortality of ILD is dependent on
specific diagnosis : high - 20% in infants and children.
Prognosis is variable and poor in children with :
- pulmonary hypertension
- failure to thrive
- sever fibrosis

Mortality
Children AdultsDIP 39% 5%UIP 4% 50-80%
King. AJRCCM 2005;172:268

TREATMENT OF ILD

Treatment
Supportive care is essential and includes :Supportive care is essential and includes :supplemental oxygen for hypoxia and
nutrition for growth failure.. Antimicrobial treatment may be necessary
for recurrent infections.. Some patients may be responsive to Some patients may be responsive to
bronchodilators.bronchodilators.

Corticosteroids
Anti-inflammatory treatment with corticosteroids remains the initial treatment of choice.
Controlled trials are lacking.The usual dose of prednisone 1-2 mg /kg/24
for 6 -8 wk with tapering directed by clinical response
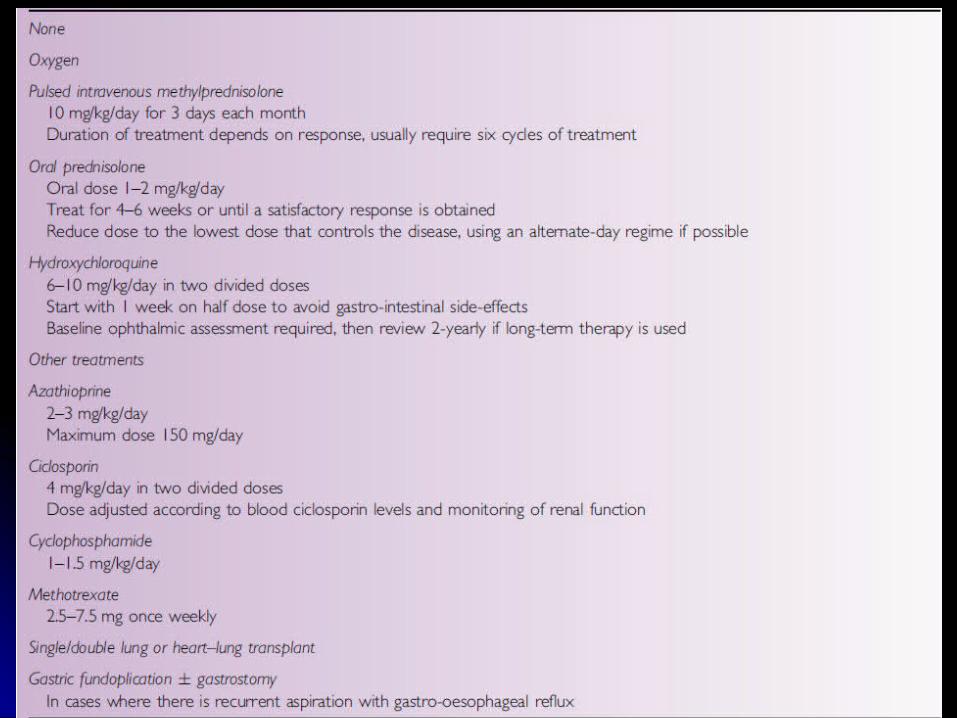
Alternative, but not adequately evaluated therapy includes:
HydroxychloroquineAzathioprineCyclophosamideCyclosporineMethotrexateI V immunoglobulinPulsed high-dose steroids
Lung transplantation for progressive or end-stage ILD is successful in some infants and children.
Appropriate treatment for underlying systemic disease is indicated.
Hydroxychloroquine treatment is successful in some children with classic ILD , particulary those with histopathologic changes of DIP.
Key MessagesKey MessagesDiagnosis of ILD requires a high index of suspicion, as the clinical presentation is subtle, variable, nonspecific and is likely to be confused with other pneumonias.
Progressive nature of the illness, clinical findings, serial chest xrays, HRCT and BAL will be helpful in the diagnosis of ILD, in the absence of lung biopsy.






























