Embed Size (px)
DESCRIPTION
Dermatologi
Citation preview

Backgroundhttp://emedicine.medscape.com/article/1049216-overview#showall
Allergic contact dermatitis (ACD) is a delayed type of induced sensitivity (allergy) resulting from cutaneous contact with a specific allergen to which the patient has developed a specific sensitivity. This allergic reaction causes inflammation of the skin manifested by varying degrees of erythema, edema, and vesiculation.
The term contact dermatitis sometimes is used incorrectly as a synonym for allergic contact dermatitis. Contact dermatitis is inflammation of the skin induced by chemicals that directly damage the skin (see Irritant Contact Dermatitis) and by specific sensitivity in the case of allergic contact dermatitis.
Jadassohn first described allergic contact dermatitis in 1895. He developed the patch test to identify the chemicals to which the patient was allergic. Sulzberger popularized patch testing in the United States in the 1930s. The Finn chamber method for patch testing was designed in the 1970s; these chambers consist of small metal cups, typically attached to strips of tape, filled with allergens dispersed in either petrolatum or water. The thin-layer rapid use epicutaneous (TRUE) test for patch testing became available in the United States in the 1990s.
The importance of specific substances as causes of allergic contact dermatitis varies with the prevalence of that substance in the environment. Mercury compounds once were significant causes of allergic contact dermatitis but rarely are used as topical medications and, currently, are uncommon as a cause of allergic contact dermatitis. Ethylenediamine, which was present in the original Mycolog cream, declined as a primary cause of allergic contact dermatitis once Mycolog cream was reformulated to no longer contain this allergen.
A detailed history, both before and after patch testing, is crucial in evaluating individuals with allergic contact dermatitis. Before patch testing, the history identifies potential causes of allergic contact dermatitis and the materials to which individuals are exposed that should be included in patch testing. After patch testing, the history determines the clinical significance of the findings. (See Clinical.)
Topical corticosteroids are the mainstay of treatment, while a variety of symptomatic treatments can provide short-term relief of pruritus. However, the definitive treatment of allergic contact dermatitis is the identification and removal of any potential causal agents; otherwise, the patient is at increased risk for chronic or recurrent dermatitis. (See Treatment.)
Go to Irritant Contact Dermatitis, Pediatric Contact Dermatitis, and Protein Contact Dermatitis for complete information on these topics.

PathophysiologyApproximately 3000 chemicals are well documented as specific causes of allergic contact dermatitis. Most of the chemicals able to provoke allergic contact dermatitis are small molecules (< 500 d). These molecules must bind to carrier proteins on Langerhans cells, which are situated within the suprabasilar layer of the epidermis.
Langerhans cells are the antigen-presenting cells within the skin. Langerhans cells interact with CD4+ T cells (helper T cells). Skin irritation by both nonallergenic and allergenic compounds induces Langerhans cell migration and maturation. In contrast, only allergenic compounds induce CD1a+ CD83+ Langerhans cell migration with partial maturation at subtoxic concentrations.[1]
Cytokines also play an important role in allergic contact dermatitis because they regulate accessory-adhesion molecules, such as intercellular adhesion molecule 1. Interleukin 8 may be a cytokine indicating allergic contact dermatitis, not irritant contact dermatitis.
Langerhans cells can migrate from the epidermis to the regional draining lymph nodes. Sensitization to a chemical requires intact lymphatic pathways.
The initial sensitization typically takes 10-14 days from initial exposure to a strong contact allergen such as poison ivy. Some individuals develop specific sensitivity to allergens following years of chronic low-grade exposure; for example, sensitivity to chromate in cement can eventually develop in individuals with chronic irritant contact dermatitis resulting from the alkaline nature of cement. Once an individual is sensitized to a chemical, allergic contact dermatitis develops within hours to several days of exposure.
CD4+ CCR10+ memory T cells persist in the dermis after clinical resolution of allergic contact dermatitis.
Filaggrin barrier defects that predispose individuals to atopic dermatitis might also predispose them to allergic contact dermatitis by allowing greater penetration of chemical haptens.[2]
Etiology Approximately 25 chemicals appear to be responsible for as many as one half of all cases of allergic contact dermatitis. These include nickel, preservatives, dyes, and fragrances.
Poison ivy
Poison ivy (Toxicodendron radicans) is the classic example of acute allergic contact dermatitis in North America. Allergic contact dermatitis from poison ivy is characterized by linear streaks of acute dermatitis that develop where plant parts have been in direct contact with the skin.

Nickel
Nickel is the leading cause of allergic contact dermatitis in the world. The incidence of nickel allergic contact dermatitis in North America is increasing; in contrast, new regulations in Europe have resulted in a decreasing prevalence of nickel allergy in young and middle-aged women.[3, 4]
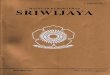
Allergic contact dermatitis to nickel typically is manifested by dermatitis at the sites where earrings or necklaces (see the image below) containing nickel are worn or where metal objects (including the keypads of some cell phones[5] ) containing nickel are in contact with the skin.
Nickel may be considered a possible occupational allergen. Workers in whom nickel may be an occupational allergen primarily include hairdressers, retail clerks, caterers, domestic cleaners, and metalworkers. Individuals allergic to nickel occasionally may develop vesicles on the sides of the fingers (dyshidrotic hand eczema or pompholyx) from nickel in the diet.
Allergic contact dermatitis to nickel in a necklace.
Rubber gloves
Allergy to 1 or more chemicals in rubber gloves is suggested in any individual with chronic hand dermatitis who wears them, unless patch testing demonstrates otherwise. Allergic contact dermatitis to chemicals in rubber gloves typically occurs maximally on the dorsal aspects of the hand. Usually, a cutoff of dermatitis occurs on the forearms where skin is no longer in contact with the gloves. Individuals allergic to chemicals in rubber gloves may develop dermatitis from other exposures to the chemicals (eg, under elastic waistbands).
Hair dye and temporary tattoos
p-Phenylenediamine (PPD) is a frequent component of and sensitizer in permanent hair dye products and temporary henna tattoos[6] ; exposure in to it in hair dye products may cause acute dermatitis with severe facial edema. Severe local reactions from PPD may occur in black henna tattoos in adults and children. Epidemiologic data indicate that the median prevalence of positive patch test reactions to PPD among dermatitis patients is 4.3% (increasing) in Asia, 4% (plateau) in Europe, and 6.2% (decreasing) in North America.[7]

Textiles
Individuals allergic to dyes and permanent press and wash-and-wear chemicals added to textiles typically develop dermatitis on the trunk, which occurs maximally on the lateral sides of the trunk but spares the vault of the axillae. Primary lesions may be small follicular papules or may be extensive plaques.
Individuals in whom this allergic contact dermatitis is suspected should be tested with a series of textile chemicals, particularly if routine patch testing reveals no allergy to formaldehyde. New clothing is most likely to provoke allergic contact dermatitis, since most allergens decrease in concentration in clothing following repeated washings.
Preservatives
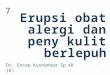
Preservative chemicals added to cosmetics, moisturizers, and topical medications are major causes of allergic contact dermatitis (see the image below). The risk of allergic contact dermatitis appears to be highest to quaternium-15, followed by allergic contact dermatitis to isothiazolinones (Kathon CG). Although parabens are among the most widely used preservatives, they are not a frequent cause of allergic contact dermatitis.
Severe allergic contact dermatitis resulting from preservatives in sunscreen. Patch testing was negative to the active ingredients in the sunscreen.
Schnuch et al estimated that preservatives found in leave-on topical products varied over 2 orders of magnitude in relative sensitization risk.[8]
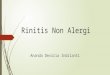
Formaldehyde is a major cause of allergic contact dermatitis (see the image below). Certain preservative chemicals widely used in shampoos, lotions, other moisturizers, and cosmetics are termed formaldehyde releasers (ie, quaternium-15 [Dowicil 200], imidazolidinyl urea [Germall 115], and isothiazolinones[8] ).

Onycholysis developing from allergic contact dermatitis to formaldehyde used to harden nails.
Fragrances
Individuals may develop allergy to fragrances. Fragrances are found not only in perfumes, colognes, aftershaves, deodorants, and soaps, but also in numerous other products, often as a mask to camouflage an unpleasant odor. Unscented products may contain fragrance chemicals used as a component of the product and not labeled as fragrance.
Individuals allergic to fragrances should use fragrance-free products. Unfortunately, the exact chemicals responsible for a fragrance in a product are not labeled. Four thousand different fragrance molecules are available to formulate perfumes. The fragrance industry is not required to release the names of ingredients used to compose a fragrance in the United States, even when individuals develop allergic contact dermatitis to fragrances found in topical medications.
Deodorants may be the most common cause of allergic contact dermatitis to fragrances because they are applied to occlude skin that is often abraded by shaving in women.
Massage and physical therapists and geriatric nurses are at higher risk of occupational allergic contact dermatitis to fragrances.
Corticosteroids
In the last decade, it has become clear that some individuals with chronic dermatitis develop allergy to topical corticosteroids. Most affected individuals can be treated with some topical corticosteroids, but an individual can be allergic to all topical and systemic corticosteroids. Budesonide and tixocortol pivalate are useful patch test corticosteroids for identifying individuals allergic to topical corticosteroids.

Neomycin
The risk of allergy to neomycin is related directly to the extent of its use in a population. The risk of allergy to neomycin is much higher when it is used to treat chronic stasis dermatitis and venous ulcers than when it is used as a topical antibiotic on cuts and abrasions in children. Assume that individuals allergic to neomycin are allergic to chemically related aminoglycoside antibiotics (eg, gentamicin, tobramycin).[9] Avoid these drugs both topically and systemically in individuals allergic to neomycin.
Benzocaine
Avoid topical use of benzocaine. Benzocaine is included in most standard patch test trays. Individuals allergic to benzocaine may safely use or be injected with lidocaine (Xylocaine), which does not cross-react with benzocaine.
Many individuals complain of adverse reactions to sunscreens, but many of these individuals are not allergic to the sunscreen materials. They may be allergic to preservatives in these products or may have nonspecific cutaneous irritation from these products.
Photoallergy
Occasionally, individuals develop photoallergic contact dermatitis. Allergic contact dermatitis may be accentuated by ultraviolet (UV) light, or patients may develop an allergic reaction only when a chemical is present on the skin and when the skin is exposed sufficiently to ultraviolet light A (UV-A; 320-400 nm).

Epidemiology
United States statistics
The National Health and Nutrition Examination Survey (NHANES) estimated the prevalence of contact dermatitis to be 13.6 cases per 1000 population, using physical examinations by dermatologists of a selected sample of patients. NHANES underreported the prevalence compared with the physical examination findings.
The National Ambulatory Medical Care Survey conducted in 1995 estimated 8.4 million outpatient visits to American physicians for contact dermatitis. This was the second most frequent dermatologic diagnosis. Of office visits to dermatologists, 9% are for dermatitis. At a student health center dermatology clinic, 3.1% of patients presented for allergic contact dermatitis, and 2.3% presented for irritant contact dermatitis.
The TRUE test Web site can provide accurate basic information on common allergens. The Contact Allergen Management Program is provided as a service to the American Contact Dermatitis Society (ACDS) members and is particularly valuable for allergens found in topical skin care products. The Contact Allergen Replacement Database (CARD) contains more than 8100 known ingredients cataloged in more than 5500 commercial skincare products and is available as a Smartphone application.
International statistics
A Swedish study found that prevalence of allergic contact dermatitis of the hands was 2.7 cases per 1000 population. A Dutch study found that prevalence of allergic contact dermatitis of the hands was 12 cases per 1000 population.
Race, sex, and age-related demographics
No racial predilection exists for allergic contact dermatitis. Allergic contact dermatitis is more common in women than in men. This predominantly is a result of allergy to nickel, which is much more common in women than in men in most countries.
Allergic contact dermatitis may occur in neonates. In elderly individuals, the development of allergic contact dermatitis may be delayed somewhat, but the dermatitis may be more persistent once developed. Contact allergy to topical medicaments is more common in persons older than 70 years.[10]

Prognosis Individuals with allergic contact dermatitis may have persistent or relapsing dermatitis, particularly if the material(s) to which they are allergic is not identified or if they continue to practice skin care that is no longer appropriate (ie, they continue to use harsh chemicals to wash their skin, they do not apply creams with ceramides or bland emollients to protect their skin).
The longer an individual has severe dermatitis, the longer it is believed it will take the dermatitis to resolve once the cause is identified.
Some individuals have persistent dermatitis following allergic contact dermatitis, which appears to be true especially in individuals allergic to chrome.
A particular problem is neurodermatitis (lichen simplex chronicus), in which individuals repeatedly rub or scratch an area initially affected by allergic contact dermatitis.
Mortality
Death from allergic contact dermatitis is rare in the United States. Allergic contact dermatitis to the weed wild feverfew caused deaths in India when the seeds contaminated wheat shipments to India. This plant then became widespread and a primary cause of severe airborne allergic contact dermatitis.
Patient Education Patients have the best prognosis when they are able to remember the materials to which they are allergic and how to avoid further exposures. Provide patients with as much information as possible concerning the chemical to which they are allergic, including all known names of the chemical. Web sites, Smartphone applications, standard textbooks, and the TRUE test kit contain basic information about the chemicals.
Susceptible individuals need to read the list of ingredients before applying cosmetic products to their skin, since preservative chemicals are used widely in consumer, medical, and workplace products. The same chemical may have different names when used for consumer or industrial purposes.
Provide pamphlets with color pictures of poison ivy to individuals allergic to the plant. The American Academy of Dermatology also has pamphlets on allergic contact dermatitis and hand eczema.
For patient education information, see the Skin, Hair, and Nails Center, as well as Contact Dermatitis.

HistoryA detailed history, both before and after patch testing, is crucial in evaluating individuals with allergic contact dermatitis. Potential causes of allergic contact dermatitis and the materials to which individuals are exposed should be included in patch testing. Evaluation of allergic contact dermatitis requires a much more detailed history than most other dermatologic disorders.
History is equally important after patch testing. Only history and questioning can determine whether the materials to which a patient is allergic are partly or wholly responsible for the current dermatitis. A positive patch reaction may indicate only a sensitivity and not the cause of current dermatitis.
Preexisting skin diseases
Individuals with stasis dermatitis are at high risk for developing allergic contact dermatitis to materials and agents applied to the areas of stasis dermatitis and leg ulcers. Neomycin is an important cause of allergic contact dermatitis in these individuals because it is used frequently despite the lack of documentation of its efficacy in the treatment of stasis ulcers.
Individuals with otitis externa frequently are allergic to topical neomycin and topical corticosteroids.
Individuals with pruritus ani and pruritus vulvae may become sensitized to benzocaine and other medications applied to chronic pruritic processes.
Women with lichen sclerosus et atrophicus frequently develop allergic contact dermatitis, complicating the severe chronic vulvar dermatosis. Patch testing these patients may provide important information that can help in the management of recalcitrant and difficult-to-manage dermatosis.
Atopic dermatitis
Patients with a history of atopic dermatitis are at increased risk for developing nonspecific hand dermatitis and irritant contact dermatitis. However, they do not appear to be at an increased risk for allergic contact dermatitis, despite the wide range of topical medications and moisturizers used by individuals with chronic atopic dermatitis. They are at lower risk of allergic contact dermatitis to poison ivy. Some European studies indicate that patients with atopic dermatitis may have increased incidence of allergic contact dermatitis to nickel.
Onset of symptoms
Individuals with allergic contact dermatitis typically develop dermatitis, within a few days of exposure, in areas that were exposed directly to the allergen. Certain allergens (eg, neomycin)

penetrate intact skin poorly, and the onset of dermatitis may be delayed up to a week following exposure.
A minimum of 10 days is required for individuals to develop specific sensitivity to a new contactant. For example, an individual who never has been sensitized to poison ivy may develop only a mild dermatitis 2 weeks following the initial exposure but typically develops severe dermatitis within 1-2 days of the second and subsequent exposures.
Remember that removing the poison ivy allergen from the skin is difficult, and unless an individual washes exposed skin within 30 minutes of exposure, allergic contact dermatitis will develop. The hallmark of the diagnosis of poison ivy is linear dermatitic lesions. The possibility of an external cause of dermatitis always must be considered if the dermatitis is linear or sharply defined.
The immediate onset of dermatitis following initial exposure to material suggests either a cross-sensitization reaction, prior forgotten exposure to the substance, or nonspecific irritant contact dermatitis provoked by the agent in question.
Eyelid dermatitis
Individuals may develop dermatitis on eyelids and other exposed skin following exposure to airborne allergens or allergens transferred to that site by the fingers. Contact dermatitis may also result from allergy to eyelid makeup.
Contact urticaria
Immediate reactions, ie, visible lesions developing less than 30 minutes after exposure, indicate contact urticaria (not allergic contact dermatitis). This is particularly true if the lesions are urticarial in appearance and if the skin reaction is associated with other symptoms, such as distant urticaria, wheezing, ophthalmedema, rhinorrhea, or anaphylaxis.
Latex
Rubber latex currently is the most important source of allergic contact urticaria (see Latex Allergy). The term hypoallergenic may refer to gloves that do not contain sensitizing chemicals added to rubber latex but may not indicate whether the gloves are rubber latex free.
Some individuals may have delayed specific contact sensitivity to rubber latex, but contact urticaria to rubber latex is much more common than allergic contact dermatitis to latex. Individuals with hand dermatitis, hospital workers, children with spina bifida, and atopic individuals are at increased risk of developing contact urticaria to rubber latex. Individuals may have allergic contact dermatitis to chemicals added to rubber gloves and have contact urticaria to latex. Individuals wearing rubber gloves should be evaluated carefully for both possibilities.

Rare reports exist of immediate anaphylactic reactions to topical antibiotics (eg, bacitracin).
Occupational dermatitis
Contact dermatitis is 1 of the 10 leading occupational illnesses. It may prevent individuals from working. The hands are the sites exposed most intensely to contact allergens and irritants, both at work and at home. Allergic contact dermatitis in response to workplace materials may improve initially on weekends and during holidays, but individuals with chronic dermatitis may not demonstrate the classic history of weekend and holiday improvement.
Irritant contact dermatitis is more likely if multiple workers are affected in the workplace. Most allergens rarely sensitize a high percentage of the population.
Hobbies
Hobbies may be the source of allergic contact dermatitis. Examples include woodworking with exotic tropical woods or processing film using color-developing chemicals that may provoke cutaneous lesions of lichen planus from direct skin exposure.
Medications
Medications (both self-prescribed and physician-prescribed) are important causes of allergic contact dermatitis. The workplace nurse may dispense ineffective and sensitizing topical preparations, such as thimerosal (Merthiolate), which may change a simple abrasion into a severe case of allergic contact dermatitis. Individuals may develop allergy to preservatives in medications and/or to the active ingredients in topical medications, especially neomycin and topical corticosteroids.[11, 12]
Patients with dermatitis that did not clear with topical corticosteroid treatment should be considered for patch testing with a corticosteroid series and the commercial preparations of corticosteroids and their vehicles.
Physical ExaminationAcute allergic contact dermatitis is characterized by pruritic papules and vesicles on an erythematous base. Lichenified pruritic plaques may indicate chronic allergic contact dermatitis. Occasionally, allergic contact dermatitis may affect the entire integument (ie, erythroderma, exfoliative dermatitis). The initial site of dermatitis often provides the best clue regarding the potential cause of allergic contact dermatitis. Note the following.
Hands
Hands are an important site of allergic contact dermatitis, particularly in the workplace. Common causes of allergic dermatitis on the hands include the chemicals in rubber gloves.

Topical medication sites
Allergic contact dermatitis is frequent in the perianal area as a result of the use of sensitizing medications and remedies (eg, topical benzocaine). Topical medications are also important causes of allergic contact dermatitis in cases of otitis externa. Allergy to chemicals in ophthalmologic preparations may provoke dermatitis around the eyes.
Airborne allergic contact dermatitis
Chemicals in the air may produce airborne allergic contact dermatitis. This dermatitis usually occurs maximally on the eyelids, but it may affect other areas exposed to chemicals in the air, particularly the head and the neck.
Hair dyes
Hair dye—in particular, the component p-phenylenediamine (PPD)—may trigger allergic contact dermatitis. Individuals allergic to hair dyes typically develop the most severe dermatitis on the ears and adjoining face rather than on the scalp.
Stasis dermatitis and stasis ulcers
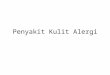
Individuals with stasis dermatitis and stasis ulcers are at high risk for developing allergic contact dermatitis to topical medications applied to inflamed or ulcerated skin (see the image below). The chronicity of this condition and the frequent occlusion of applied medications contribute to the high risk of allergic contact dermatitis to medicament (eg, neomycin) in these patients.
Individuals may develop widespread dermatitis from topical medications applied to leg ulcers or from cross-reacting systemic medications administered intravenously. For example, a patient allergic to neomycin may develop systemic contact dermatitis if treated with intravenous gentamicin.
Chronic stasis dermatitis with allergic contact dermatitis to quaternium-15, a preservative in moisturizer. Allergic contact dermatitis produces areas of erythema in areas of atrophie blanche and varicose veins.

Erythema multiforme
Erythema multiforme (EM) is a severe cutaneous reaction with targetoid lesions that occurs primarily after exposure to certain medications or is triggered by infection, most commonly by herpes simplex virus. Rare cases of EM have been reported after allergic contact dermatitis resulting from exposure to poison ivy,[13] tropical woods, nickel, and hair dye (see the image below).
Erythema multiformelike reaction that developed acutely following hair dying.
Intraoral metal contact allergy may result in mucositis that mimics lichen planus, which has an association with intraoral squamous cell carcinoma. Intraoral squamous cell carcinoma adjacent to a dental restoration containing a metal to which the patient was allergic has been reported.[14]
Allergic contact dermatitis may be a direct trigger for skin ulceration in patients with venous insufficiency. Early diagnosis and treatment of allergic contact dermatitis may prevent the development of venous ulcers.
Complications
Darkly pigmented individuals may develop areas of hyperpigmentation or hypopigmentation from allergic contact dermatitis. Occasionally, they may develop depigmentation at sites of allergic contact dermatitis to certain chemicals.
Occasionally, allergic contact dermatitis is complicated by secondary bacterial infection, which may be treated by the appropriate systemic antibiotic.

Diagnostic ConsiderationsContact dermatitis from allergy must be differentiated from contact dermatitis due to irritation, as well as other forms of dermatitis. In addition, the specific substance to which the patient is sensitive needs to be identified.
Differentials Asteatotic Eczema Contact Dermatitis, Irritant Drug-Induced Bullous Disorders Drug-Induced Photosensitivity Nummular Dermatitis Onycholysis Perioral Dermatitis Phytophotodermatitis Prurigo Nodularis Seborrheic Dermatitis Tinea Corporis Transient Acantholytic Dermatosis Urticaria, Contact Syndrome
Translate To Indo
Background
Dermatitis kontak alergi (ACD) adalah jenis keterlambatan yang disebabkan sensitivitas (alergi) yang dihasilkan dari kontak kulit dengan alergen tertentu yang mana pasien telah mengembangkan sensitivitas tertentu. Reaksi alergi menyebabkan peradangan pada kulit dimanifestasikan oleh berbagai tingkat eritema, edema vesiculation, dan.Para dermatitis kontak istilah kadang-kadang digunakan secara tidak benar sebagai sinonim untuk dermatitis kontak alergi. Dermatitis kontak adalah peradangan pada kulit yang disebabkan oleh bahan kimia yang secara langsung merusak kulit (lihat Dermatitis iritan Kontak) dan oleh sensitivitas khusus dalam kasus dermatitis kontak alergi.Jadassohn pertama kali dijelaskan dermatitis kontak alergi pada 1895. Ia mengembangkan tes patch untuk mengidentifikasi bahan kimia untuk pasien yang alergi. Sulzberger dipopulerkan patch pengujian di Amerika Serikat pada 1930-an. Ruang Finn metode untuk patch pengujian dirancang pada tahun 1970; ruang ini terdiri dari cangkir logam kecil, biasanya melekat pada strip dari pita, penuh dengan alergen tersebar baik dalam petrolatum atau air. Para lapis tipis menggunakan epicutaneous cepat (TRUE) uji untuk pengujian patch yang menjadi tersedia di Amerika Serikat pada 1990-an.

Pentingnya zat tertentu sebagai penyebab dermatitis kontak alergi bervariasi dengan prevalensi bahwa zat di lingkungan. Senyawa merkuri dulu penyebab signifikan dermatitis kontak alergi tapi jarang digunakan sebagai obat topikal dan, saat ini, jarang terjadi sebagai penyebab dermatitis kontak alergi. Etilendiamina, yang hadir pada krim Mycolog asli, menurun sebagai penyebab utama dari dermatitis kontak alergi sekali krim Mycolog direformulasi untuk tidak lagi mengandung alergen ini.Sejarah rinci, baik sebelum dan sesudah patch pengujian, sangat penting dalam mengevaluasi individu dengan dermatitis kontak alergi. Sebelum patch pengujian, sejarah mengidentifikasi potensi penyebab dermatitis kontak alergi dan bahan-bahan untuk mana individu yang terkena yang harus disertakan dalam pengujian patch. Setelah patch pengujian, sejarah menentukan signifikansi klinis dari temuan. (Lihat klinis.)Kortikosteroid topikal merupakan andalan pengobatan, sementara berbagai perawatan simtomatik dapat memberikan bantuan jangka pendek dari pruritus. Namun, pengobatan definitif dermatitis kontak alergi adalah identifikasi dan penghapusan setiap agen penyebab potensial, jika tidak, pasien berada pada peningkatan risiko untuk dermatitis kronis atau berulang. (Lihat Pengobatan.)Pergi ke Dermatitis iritan kontak, Dermatitis Kontak Pediatric, dan Protein Dermatitis kontak untuk informasi lengkap mengenai topik ini.
PatofisiologiSekitar 3000 bahan kimia yang didokumentasikan dengan baik sebagai penyebab spesifik dari dermatitis kontak alergi. Sebagian besar bahan kimia mampu memancing dermatitis kontak alergi adalah molekul kecil (<500 d). Molekul-molekul ini harus mengikat protein pembawa pada sel Langerhans, yang terletak dalam lapisan suprabasilar dari epidermis.Langerhans sel adalah penyajian antigen-sel dalam kulit. Langerhans sel berinteraksi dengan sel T CD4 + (sel T pembantu). Iritasi kulit oleh kedua migrasi senyawa nonallergenic dan alergi sel Langerhans dan menginduksi pematangan. Sebaliknya, hanya senyawa antialergi menginduksi CD1a + CD83 + migrasi sel Langerhans dengan pematangan parsial pada konsentrasi subtoxic [1].Sitokin juga memainkan peran penting dalam dermatitis kontak alergi karena mereka mengatur aksesori-adhesi molekul, seperti molekul adhesi antar sel 1. Interleukin 8 mungkin sitokin menunjukkan dermatitis kontak alergi, bukan dermatitis kontak iritan.Sel Langerhans dapat bermigrasi dari epidermis ke kelenjar getah bening regional pengeringan. Sensitisasi terhadap suatu bahan kimia yang memerlukan jalur limfatik utuh.Sensitisasi awal biasanya memakan waktu 10-14 hari dari awalnya berhubungan dengan alergen kontak kuat seperti poison ivy. Beberapa individu mengembangkan kepekaan khusus terhadap alergen setelah tahun kronis tingkat rendah paparan, misalnya, kepekaan terhadap kromat dalam semen akhirnya dapat berkembang pada individu dengan dermatitis kontak iritan kronis akibat sifat alkali dari semen. Setelah seorang individu peka terhadap bahan kimia, dermatitis kontak alergi berkembang dalam beberapa jam sampai beberapa hari paparan.CD4 + CCR10 + memori T sel bertahan dalam dermis setelah resolusi klinis dermatitis kontak alergi.Cacat penghalang Filaggrin yang mempengaruhi individu untuk dermatitis atopik mungkin juga mempengaruhi mereka untuk dermatitis kontak alergi dengan memungkinkan penetrasi yang lebih besar haptens kimia. [2]

EtiologiSekitar 25 bahan kimia tampaknya bertanggung jawab untuk sebanyak satu setengah dari semua kasus dermatitis kontak alergi. Ini termasuk nikel, bahan pengawet, pewarna, dan wewangian.
Poison ivyPoison ivy (radicans Toxicodendron) adalah contoh klasik dari dermatitis kontak alergi akut di Amerika Utara. Dermatitis kontak alergi dari poison ivy ditandai dengan garis-garis linier dermatitis akut yang berkembang di mana bagian tanaman telah melakukan kontak langsung dengan kulit.
NikelNikel adalah penyebab utama dari dermatitis kontak alergi di dunia. Kejadian dermatitis kontak alergi nikel di Amerika Utara meningkat;. Sebaliknya, peraturan baru di Eropa telah mengakibatkan penurunan prevalensi alergi nikel pada wanita muda dan setengah baya [3, 4]Dermatitis kontak alergi terhadap nikel biasanya dimanifestasikan oleh dermatitis di tempat di mana anting atau kalung (lihat gambar di bawah) yang mengandung nikel yang dipakai atau di mana benda logam (termasuk keypad beberapa ponsel [5]) yang mengandung nikel berada dalam kontak dengan kulit.Nikel dapat dianggap sebagai alergen kerja mungkin. Pekerja di antaranya nikel dapat menjadi alergen kerja terutama meliputi penata rambut, panitera ritel, katering, pembersih rumah tangga, dan pengrajin logam. Individu alergi terhadap nikel mungkin kadang-kadang mengembangkan vesikel di sisi jari-jari (tangan eksim dyshidrotic atau pompholyx) dari nikel dalam makanan.
Sarung Tangan KaretAlergi terhadap 1 atau lebih bahan kimia dalam sarung tangan karet yang disarankan dalam setiap individu dengan dermatitis tangan kronis yang mengenakannya, kecuali patch pengujian menunjukkan sebaliknya. Dermatitis kontak alergi terhadap bahan kimia dalam sarung tangan karet biasanya terjadi secara maksimal pada aspek dorsal tangan. Biasanya, cutoff dermatitis terjadi pada lengan bawah di mana kulit tidak lagi kontak dengan sarung tangan. Individu alergi terhadap bahan kimia dalam sarung tangan karet dapat mengembangkan dermatitis dari eksposur lain untuk bahan kimia (misalnya, di bawah ikat pinggang elastis).
Pewarna Rambut dan tato sementarap-phenylenediamine (PPD) adalah komponen sering dan sensitizer dalam produk pewarna rambut permanen dan tato henna sementara [6]; paparan untuk itu dalam produk pewarna rambut dapat menyebabkan dermatitis akut dengan edema wajah yang parah. Reaksi lokal yang parah dari PPD dapat terjadi pada tato henna hitam pada orang dewasa dan anak-anak. Data epidemiologi menunjukkan bahwa prevalensi rata-rata reaksi uji tempel positif terhadap PPD antara pasien dermatitis adalah 4,3% (meningkat) di Asia, 4% (dataran tinggi) di Eropa, dan 6,2% (penurunan) di Amerika Utara. [7]

TekstilIndividu alergi terhadap pewarna dan tekan permanen dan cuci-dan-pakai bahan kimia ditambahkan ke tekstil biasanya mengembangkan dermatitis pada batang, yang terjadi secara maksimal di sisi lateral bagasi tetapi suku cadang kubah dari axillae tersebut. Lesi primer mungkin papula folikuler kecil atau mungkin plak yang luas.Individu dalam siapa ini dermatitis kontak alergi dicurigai harus diuji dengan serangkaian bahan kimia tekstil, terutama jika rutin patch pengujian menunjukkan tidak ada alergi terhadap formaldehida. Pakaian baru yang paling mungkin untuk memprovokasi dermatitis kontak alergi, karena alergen yang paling penurunan konsentrasi dalam pakaian setelah dicuci berulang-ulang.pengawetPengawet bahan kimia ditambahkan ke kosmetik, pelembab, dan obat topikal adalah penyebab utama dermatitis kontak alergi (lihat gambar di bawah). Risiko dermatitis kontak alergi tampaknya tertinggi untuk Quaterinium-15, diikuti oleh dermatitis kontak alergi terhadap isothiazolinones (Kathon CG). Walaupun paraben adalah salah satu pengawet paling banyak digunakan, mereka tidak sering menjadi penyebab dermatitis kontak alergi.
PengawetPengawet bahan kimia ditambahkan ke kosmetik, pelembab, dan obat topikal adalah penyebab utama dermatitis kontak alergi (lihat gambar di bawah). Risiko dermatitis kontak alergi tampaknya tertinggi untuk Quaterinium-15, diikuti oleh dermatitis kontak alergi terhadap isothiazolinones (Kathon CG). Walaupun paraben adalah salah satu pengawet paling banyak digunakan, mereka tidak sering menjadi penyebab dermatitis kontak alergi. Parah dermatitis kontak alergi akibat pengawet dalam tabir surya. Patch pengujian adalah negatif terhadap bahan aktif dalam tabir surya. Schnuch dkk memperkirakan bahwa bahan pengawet yang ditemukan dalam meninggalkan-on produk topikal bervariasi lebih dari 2 lipat risiko sensitisasi relatif. [8]Formaldehida merupakan penyebab utama dari dermatitis kontak alergi (lihat gambar di bawah). Bahan kimia pengawet tertentu banyak digunakan dalam shampo, lotion, pelembab lain, dan kosmetik ini disebut releasers formaldehida (yaitu, Quaterinium-15 [Dowicil 200], imidazolidinyl urea [Germall 115], dan isothiazolinones [8]).
WewangianIndividu dapat mengembangkan alergi terhadap wewangian. Wewangian ditemukan tidak hanya di parfum, cologne, aftershaves, deodoran, dan sabun, tetapi juga dalam produk lain banyak, sering sebagai topeng untuk menyamarkan bau yang tidak menyenangkan. Produk diberi wewangian mungkin mengandung bahan kimia aroma digunakan sebagai komponen produk dan tidak dicap sebagai wewangian.Individu alergi terhadap wewangian harus menggunakan aroma bebas produk. Sayangnya, bahan kimia yang tepat yang bertanggung jawab untuk aroma dalam suatu produk tidak berlabel. Empat ribu molekul aroma yang berbeda tersedia untuk merumuskan parfum. Industri aroma tidak diperlukan untuk melepaskan nama-nama bahan yang digunakan untuk menulis wangi di Amerika Serikat, bahkan ketika individu mengembangkan dermatitis kontak alergi terhadap wewangian ditemukan dalam obat topikal.

Deodoran dapat menjadi penyebab paling umum dermatitis kontak alergi terhadap wewangian karena mereka diterapkan untuk menutup jalan kulit yang sering terkelupas dengan mencukur pada perempuan.Pijat dan fisik terapis dan perawat geriatri memiliki resiko lebih tinggi dari dermatitis kontak akibat kerja alergi terhadap wewangian.
kortikosteroidDalam dekade terakhir, telah menjadi jelas bahwa beberapa individu dengan dermatitis kronis mengembangkan alergi terhadap kortikosteroid topikal. Kebanyakan individu yang terkena bisa diobati dengan beberapa kortikosteroid topikal, tetapi seseorang dapat menjadi alergi untuk semua kortikosteroid topikal dan sistemik. Budesonide dan tixocortol pivalate adalah tes yang berguna kortikosteroid patch untuk mengidentifikasi individu alergi terhadap kortikosteroid topikal.
NeomisinRisiko alergi terhadap neomisin berhubungan langsung dengan tingkat penggunaannya dalam populasi. Risiko alergi terhadap neomisin jauh lebih tinggi bila digunakan untuk mengobati dermatitis kronis stasis dan ulkus vena daripada bila digunakan sebagai antibiotik topikal pada luka dan lecet pada anak. Asumsikan bahwa individu alergi terhadap neomisin alergi terhadap antibiotik aminoglikosida kimia terkait (misalnya, gentamisin, tobramycin) [9]. Hindari obat-obatan baik topikal dan sistemik pada orang alergi terhadap neomisin.
BenzokainHindari penggunaan topikal benzokain. Benzokain termasuk dalam nampan patch yang paling standar uji. Individu alergi terhadap benzokain aman dapat menggunakan atau disuntikkan dengan lidokain (Xylocaine), yang tidak bereaksi silang dengan benzokain.Banyak orang mengeluhkan reaksi negatif terhadap tabir surya, tapi banyak dari orang-orang tidak alergi terhadap bahan tabir surya. Mereka mungkin alergi terhadap pengawet dalam produk ini atau mungkin memiliki iritasi kulit nonspesifik dari produk ini.
PhotoallergySesekali, individu mengembangkan dermatitis kontak fotoalergi. Dermatitis kontak alergi dapat ditekankan oleh ultraviolet (UV), atau pasien dapat mengembangkan reaksi alergi hanya bila suatu bahan kimia yang ada pada kulit dan bila kulit terkena cukup sinar ultraviolet A (UV-A; 320-400 nm) .

EpidemiologiAmerika Serikat statistikKesehatan Nasional dan Gizi Survey (NHANES) memperkirakan prevalensi dermatitis kontak menjadi 13,6 kasus per 1000 penduduk, dengan menggunakan pemeriksaan fisik oleh ahli kulit dari sampel yang dipilih pasien. NHANES dilaporkan prevalensi dibandingkan dengan temuan pemeriksaan fisik.Para Ambulatory Medical Care Survey Nasional dilakukan pada tahun 1995 diperkirakan 8,4 juta kunjungan rawat jalan ke dokter Amerika untuk dermatitis kontak. Ini adalah diagnosa dermatologi kedua yang paling sering. Kunjungan kantor untuk dermatologists, 9% adalah untuk dermatitis. Pada sebuah klinik kesehatan mahasiswa pusat dermatologi, 3,1% pasien disajikan untuk dermatitis kontak alergi, dan 2,3% disajikan untuk dermatitis kontak iritan.Situs tes BENAR Web dapat memberikan informasi dasar yang akurat pada alergen yang umum. Para Allergen Kontak Pengelolaan Program disediakan sebagai layanan pada Dermatitis Kontak American Society (ACD) orang dan sangat berharga untuk alergen ditemukan dalam produk perawatan kulit topikal. Para Allergen Kontak Penggantian Database (CARD) berisi lebih dari 8100 bahan dikenal katalog di lebih dari 5500 produk perawatan kulit komersial dan tersedia sebagai aplikasi Smartphone.Internasional statistikSebuah studi di Swedia menemukan bahwa prevalensi dermatitis kontak alergi dari tangan adalah 2,7 kasus per 1000 penduduk. Sebuah penelitian di Belanda menemukan bahwa prevalensi dermatitis kontak alergi dari tangan adalah 12 kasus per 1000 penduduk.Ras, jenis kelamin, dan usia yang berhubungan dengan demografiTidak ada predileksi ras ada untuk dermatitis kontak alergi. Dermatitis kontak alergi lebih sering terjadi pada wanita dibandingkan pada pria. Ini terutama merupakan hasil dari alergi terhadap nikel, yang jauh lebih umum pada perempuan dibandingkan pada pria di banyak negara.Dermatitis kontak alergi dapat terjadi pada neonatus. Pada orang tua, perkembangan dermatitis kontak alergi mungkin tertunda sedikit, tetapi dermatitis dapat menjadi lebih kuat sekali dikembangkan. Hubungi alergi terhadap obat-obatan topikal lebih sering terjadi pada orang tua dari 70 tahun [10].
PrognosaIndividu dengan dermatitis kontak alergi mungkin memiliki dermatitis persisten atau kambuh, terutama jika bahan (s) yang mereka alergi tidak diidentifikasi atau jika mereka terus berlatih perawatan kulit yang tidak lagi sesuai (yaitu, mereka terus menggunakan bahan kimia untuk mencuci kulit mereka, mereka tidak berlaku krim dengan ceramides atau emolien hambar untuk melindungi kulit mereka).Semakin lama seorang individu telah dermatitis yang parah, semakin lama diyakini akan memakan dermatitis untuk menyelesaikan sekali penyebabnya diidentifikasi.Beberapa individu memiliki dermatitis persisten setelah dermatitis kontak alergi, yang tampaknya benar terutama pada individu yang alergi terhadap krom.Sebuah masalah tertentu adalah neurodermatitis (lichen chronicus simpleks), di mana setiap individu berulang kali menggosok atau menggaruk area awalnya dipengaruhi oleh dermatitis kontak alergi.Kematian

Kematian dari dermatitis kontak alergi jarang terjadi di Amerika Serikat. Dermatitis kontak alergi terhadap feverfew liar gulma menyebabkan kematian di India ketika benih terkontaminasi pengiriman gandum ke India. Tanaman ini kemudian menjadi luas dan penyebab utama dari dermatitis kontak alergi berat udara.
Pasien PendidikanPasien memiliki prognosis yang terbaik bila mereka mampu mengingat bahan yang mereka alergi dan bagaimana untuk menghindari paparan lebih lanjut. Menyediakan pasien dengan informasi sebanyak mungkin tentang kimia yang mereka alergi, termasuk semua nama yang dikenal bahan kimia. Situs web, aplikasi Smartphone, buku teks standar, dan test kit BENAR berisi informasi dasar tentang bahan kimia.Individu yang rentan perlu membaca daftar bahan sebelum menerapkan produk kosmetik untuk kulit mereka, karena bahan kimia pengawet digunakan secara luas di konsumen, medis, dan produk di tempat kerja. Bahan kimia yang sama mungkin memiliki nama yang berbeda bila digunakan untuk keperluan konsumen atau industri.Menyediakan pamflet bergambar warna poison ivy kepada individu alergi terhadap tanaman. American Academy of Dermatology juga memiliki pamflet pada dermatitis kontak alergi dan eksim tangan.Untuk informasi pendidikan pasien, lihat Kulit, Rambut, dan Kuku Pusat, serta Dermatitis Kontak.
SejarahSejarah rinci, baik sebelum dan sesudah patch pengujian, sangat penting dalam mengevaluasi individu dengan dermatitis kontak alergi. Potensi penyebab dermatitis kontak alergi dan bahan-bahan untuk mana individu yang terkena harus dimasukkan dalam pengujian patch. Evaluasi dermatitis kontak alergi membutuhkan sejarah jauh lebih rinci daripada kebanyakan gangguan dermatologi lainnya.Sejarah adalah sama pentingnya setelah patch pengujian. Hanya sejarah dan mempertanyakan dapat menentukan apakah bahan-bahan yang pasien alergi sebagian atau seluruhnya bertanggung jawab atas dermatitis saat ini. Reaksi patch yang positif dapat menunjukkan hanya kepekaan dan bukan penyebab dermatitis saat ini.Sudah ada penyakit kulitIndividu dengan dermatitis stasis memiliki resiko tinggi untuk mengembangkan dermatitis kontak alergi terhadap bahan dan agen diterapkan pada bidang dermatitis stasis dan borok kaki. Neomisin merupakan penyebab penting dari dermatitis kontak alergi pada individu-individu karena sering digunakan meskipun kurangnya dokumentasi kemanjurannya dalam pengobatan ulkus stasis.Individu dengan otitis eksterna seringkali alergi terhadap neomisin topikal dan kortikosteroid topikal.Individu dengan pruritus ani dan vulvae pruritus mungkin menjadi peka terhadap benzokain dan obat lain diterapkan pada proses pruritic kronis.Wanita dengan lichen et sclerosus atrophicus sering mengembangkan dermatitis kontak alergi, menyulitkan kronis parah vulva dermatosis. Patch pengujian pasien ini dapat memberikan informasi penting yang dapat membantu dalam pengelolaan dermatosis bandel dan sulit-untuk-mengelola.

Dermatitis atopikPasien dengan riwayat dermatitis atopik adalah pada peningkatan risiko untuk mengembangkan dermatitis tangan spesifik dan dermatitis kontak iritan. Namun, mereka tampaknya tidak berada pada peningkatan risiko untuk dermatitis kontak alergi, meskipun berbagai obat topikal dan pelembab yang digunakan oleh individu dengan dermatitis atopik kronis. Mereka yang berisiko lebih rendah dari dermatitis kontak alergi terhadap racun ivy. Beberapa penelitian di Eropa menunjukkan bahwa pasien dengan dermatitis atopik mungkin telah meningkatkan kejadian dermatitis kontak alergi terhadap nikel.
Timbulnya gejalaIndividu dengan dermatitis kontak alergi biasanya mengembangkan dermatitis, dalam beberapa hari paparan, di daerah yang terkena langsung ke alergi. Alergen tertentu (misalnya, neomisin) menembus kulit utuh buruk, dan terjadinya dermatitis mungkin tertunda hingga paparan berikut minggu.Minimal 10 hari diperlukan bagi individu untuk mengembangkan kepekaan khusus untuk contactant baru. Sebagai contoh, seorang individu yang pernah telah peka terhadap poison ivy dapat mengembangkan dermatitis ringan hanya 2 minggu setelah paparan awal tetapi biasanya berkembang dermatitis parah dalam waktu 1-2 hari dari eksposur kedua dan selanjutnya.Ingat bahwa menghapus alergi poison ivy dari kulit sulit, dan kecuali seorang individu mencuci kulit yang terpapar dalam waktu 30 menit pemaparan, dermatitis kontak alergi akan berkembang. Ciri dari diagnosis poison ivy adalah lesi dermatitic linier. Kemungkinan penyebab dermatitis eksternal harus selalu dipertimbangkan jika dermatitis adalah linear atau tajam didefinisikan.Onset segera dermatitis setelah paparan awal terhadap bahan menunjukkan baik reaksi sensitisasi silang, paparan sebelum lupa substansi, atau dermatitis kontak iritan nonspesifik diprovokasi oleh agen yang bersangkutan.
Kelopak mata dermatitisIndividu dapat mengembangkan dermatitis pada kelopak mata dan kulit berikut paparan terkena alergen udara atau alergen ditransfer ke situs tersebut dengan jari. Dermatitis kontak juga bisa terjadi akibat alergi terhadap riasan kelopak mata.
Hubungi urtikariaReaksi langsung, yaitu, lesi terlihat berkembang kurang dari 30 menit setelah terkena, mengindikasikan urtikaria kontak (tidak dermatitis kontak alergi). Hal ini terutama berlaku jika lesi urtikaria dalam penampilan dan jika reaksi kulit dikaitkan dengan gejala lain, seperti urtikaria jauh, mengi, ophthalmedema, Rhinorrhea, atau anafilaksis.

GetahKaret lateks saat ini adalah sumber yang paling penting dari urtikaria kontak alergi (lihat Lateks Alergi). Para hypoallergenic panjang mungkin merujuk ke sarung tangan yang tidak mengandung bahan kimia peka ditambahkan ke lateks karet tetapi mungkin tidak menunjukkan apakah sarung tangan lateks karet gratis.Beberapa individu mungkin telah tertunda sensitivitas kontak tertentu terhadap karet lateks, tapi kontak urtikaria terhadap karet lateks jauh lebih umum dari dermatitis kontak alergi terhadap lateks. Individu dengan dermatitis tangan, pekerja rumah sakit, anak-anak dengan spina bifida, dan individu atopik berada pada peningkatan risiko kontak urticaria untuk karet lateks. Individu mungkin memiliki dermatitis kontak alergi terhadap bahan kimia ditambahkan ke sarung tangan karet dan memiliki kontak urtikaria terhadap lateks. Individu mengenakan sarung tangan karet harus dievaluasi dengan hati-hati untuk kedua kemungkinan.Laporan Langka ada reaksi anafilaksis langsung terhadap antibiotik topikal (misalnya, bacitracin).
Kerja dermatitisDermatitis kontak adalah 1 dari 10 penyakit kerja terkemuka. Ini dapat mencegah individu dari bekerja. Tangan adalah situs terkena paling intensif untuk menghubungi alergen dan iritan, baik di kantor maupun di rumah. Dermatitis kontak alergi dalam menanggapi materi tempat kerja dapat meningkatkan awalnya pada akhir pekan dan selama liburan, tetapi individu dengan dermatitis kronis mungkin tidak menunjukkan sejarah klasik akhir pekan dan liburan perbaikan.Dermatitis kontak iritan lebih mungkin jika beberapa pekerja yang terkena di tempat kerja. Sebagian besar alergen jarang peka persentase yang tinggi dari populasi.
HobiHobi bisa menjadi sumber dermatitis kontak alergi. Contohnya termasuk kayu dengan kayu tropis yang eksotis atau film pengolahan menggunakan warna-mengembangkan bahan kimia yang dapat menimbulkan lesi kulit dari lichen planus dari paparan langsung dengan kulit.
ObatObat-obatan (baik diri diresepkan dan dokter-resep) adalah penyebab penting dari dermatitis kontak alergi. Perawat tempat kerja dapat mengeluarkan preparat topikal tidak efektif dan kepekaan, seperti thimerosal (Merthiolate), yang dapat mengubah abrasi sederhana menjadi kasus yang parah dermatitis kontak alergi. Individu dapat mengembangkan alergi terhadap pengawet dalam obat dan / atau bahan aktif dalam obat topikal, terutama neomisin dan kortikosteroid topikal [11, 12].Pasien dengan dermatitis yang tidak jelas dengan pengobatan kortikosteroid topikal harus dipertimbangkan untuk pengujian patch dengan serangkaian kortikosteroid dan persiapan komersial kortikosteroid dan kendaraan mereka.

Pemeriksaan fisikDermatitis kontak alergi akut ditandai oleh papula pruritus dan vesikel pada dasar eritematosa. Plak gatal lichenified dapat menunjukkan dermatitis kontak alergi kronis. Kadang-kadang, dermatitis kontak alergi dapat mempengaruhi seluruh integumen (yaitu, eritroderma, dermatitis eksfoliatif). Tempat awal dermatitis sering memberikan petunjuk terbaik tentang penyebab potensi dermatitis kontak alergi. Perhatikan berikut.
TanganTangan adalah situs penting dermatitis kontak alergi, terutama di tempat kerja. Penyebab umum dari dermatitis alergi pada tangan meliputi bahan kimia dalam sarung tangan karet.
Obat topikal situsDermatitis kontak alergi sering terjadi di daerah perianal sebagai akibat dari penggunaan obat dan obat sensitisasi (misalnya, topikal benzokain). Obat topikal juga penyebab penting dari dermatitis kontak alergi pada kasus otitis eksterna. Alergi terhadap bahan kimia dalam persiapan ophthalmologic dapat menimbulkan dermatitis sekitar mata.
Airborne dermatitis kontak alergiBahan kimia di udara dapat menghasilkan dermatitis kontak alergi udara. Dermatitis ini biasanya terjadi secara maksimal pada kelopak mata, tetapi dapat mempengaruhi daerah lain terkena bahan kimia di udara, terutama kepala dan leher.
Rambut pewarnaRambut dye-khususnya, komponen p-phenylenediamine (PPD)-dapat memicu dermatitis kontak alergi. Individu alergi terhadap pewarna rambut biasanya mengembangkan dermatitis paling parah di telinga dan wajah sebelah bukan di kulit kepala.
Stasis dermatitis dan ulkus stasisIndividu dengan dermatitis stasis dan borok stasis berada pada risiko tinggi untuk mengembangkan dermatitis kontak alergi terhadap obat topikal dioleskan pada kulit meradang atau ulserasi (lihat gambar di bawah). Kronisitas dari kondisi ini dan oklusi sering obat diterapkan berkontribusi pada risiko tinggi dermatitis kontak alergi terhadap obat (misalnya, neomisin) pada pasien ini.Individu dapat mengembangkan dermatitis luas dari obat topikal diterapkan pada borok kaki atau dari lintas bereaksi obat sistemik diberikan secara intravena. Misalnya, seorang pasien alergi terhadap neomisin dapat mengembangkan dermatitis kontak sistemik jika diobati dengan gentamisin intravena.
Eritema multiformeEritema multiforme (EM) adalah reaksi kulit yang parah dengan lesi targetoid yang terjadi terutama setelah terpapar obat tertentu atau dipicu oleh infeksi, simplex virus paling sering dengan herpes. Kasus langka EM telah dilaporkan setelah dermatitis kontak alergi akibat paparan racun ivy, [13] hutan tropis, nikel, dan pewarna rambut (lihat gambar di bawah).

Reaksi eritema multiformelike yang mengembangkan rambut akut berikut sekarat.Logam alergi kontak intraoral dapat mengakibatkan mucositis yang meniru lichen planus, yang memiliki asosiasi dengan karsinoma sel skuamosa intraoral. Karsinoma sel skuamosa intraoral berdekatan dengan restorasi gigi yang mengandung logam untuk pasien yang alergi telah dilaporkan [14].Dermatitis kontak alergi mungkin merupakan pemicu langsung untuk ulserasi kulit pada pasien dengan insufisiensi vena. Diagnosis dini dan pengobatan dermatitis kontak alergi dapat mencegah perkembangan ulkus vena.
KomplikasiDarkly individu berpigmen dapat mengembangkan bidang hiperpigmentasi atau hipopigmentasi dari dermatitis kontak alergi. Sekali waktu, mereka mengembangkan depigmentasi di situs dari dermatitis kontak alergi terhadap bahan kimia tertentu.Kadang-kadang, dermatitis kontak alergi adalah rumit oleh infeksi bakteri sekunder, yang dapat diobati dengan antibiotik sistemik yang sesuai.Diagnostik PertimbanganDermatitis kontak dari alergi harus dibedakan dari dermatitis kontak akibat iritasi, serta bentuk lain dari dermatitis. Selain itu, substansi tertentu yang mana pasien sensitif terhadap kebutuhan diidentifikasi.
Diferensial• Asteatotic Eksim• Kontak Dermatitis, Iritan• Obat-induced bulosa Gangguan• Obat-induced Fotosensitifitas• Dermatitis nummular• Onycholysis• Dermatitis perioral• Phytophotodermatitis• prurigo nodularis• Dermatitis seboroik• Tinea Corporis• Transient Acantholytic Dermatosis• Urtikaria, Sindrom Kontak