-
7/29/2019 alergi kacang
1/12
JournalImmunoDiagnosticsScientific news,opinions and reports
Journal No. 4. 2013
3 CAPture
4 Clinical Utility o Peanut Components
CAPture and Peanut sensitization phenotypesCAPture highlights
three recent articles; the rst shows that wheata/b/g-gliadins are
importantmarkers in wheat-dependent exercise induced anaphylaxis
(WDEIA), and the second demonstratesthat also in the Mediterranean
area storage proteins are the major severity markers in peanut
allergy.The last article reviewed describes how sensitization in
grass allergy spreads on the component levelduring childhood.
With the advent o recombinant peanut components the diagnosis o
peanut allergy has beenimproved by allowing the discrimination o
patients o dierent sensitization patterns. That thesesensitization
phenotypes correlate with dierent clinical maniestations o the
allergy gains more andmore support rom studies published, which is
reviewed in this issue.
-
7/29/2019 alergi kacang
2/12
ImmunoDiagnostics Journal No. 4. 013
CONTENTS
3 CAPture A selection o recentallergy papers
4 Clinical Utility o Peanut Components Background
Sensitization Phenotypes o Peanut Allergy
Combining tests or increased perormance
Confrm or exclude peanut allergy
Literature list
ImmunoDiagonstics Journal is the Journal o
Thermo Fisher Scientifc
This issue is published by Thermo Fischer Scientic -Phadia
ABP.O. 6460, SE-75137 Uppsala, Sweden
EditorMalin Berthold
Contributor(s)
Jan Hed, Anita Kober
Peanut Allergy Focus
For almost 40 years,Thermo Fisher Scientic
ImmunoDiagnostics,previously known asPhadia, have
maintainedglobal leadership in allergytesting and become oneo the
worlds leadingautoimmune disease testproviders. Through
clinical
excellence, laboratory eciency and our dedication,we strive to
deliver the highest quality and clinicalvalue in our diagnostic
tests, as well as providing
clinical expertise and scientic inormation.This ourth issue o
Immunodiagnostics Journalincludes a CAPture section with summaries
o somerecent interesting publications in the eld o allergy,ollowed
by an article summarizing the clinical utility opeanut
components.
With the introduction o allergen components thediagnosis o
peanut allergy has been dramaticallyimproved. Peanut sensitization
patterns revealdierent phenotypes o peanut allergy that are
associated with dierent clinical maniestations. Notonly can
component resolved diagnosis help toidentiy those patients who run
a high risk o severereactions, but they may also contribute to
minimizingthe need or oral ood challenges as suggested inseveral
publications. The review gives reerences torecent papers supporting
the concept o MolecularAllergology in peanut allergy and gives an
overviewo the peanut components that orm the basis or thedierent
sensitization phenotypes. The benet ocombining peanut extract tests
and components oran optimal combination o sensitivity and specicity
isdescribed based on published results.
I hope that the ImmunoDiagnostics Journal providesyou with an
easy way to catch up with or learn moreon topics o interest to
you.
-
7/29/2019 alergi kacang
3/12
3
ImmunoDiagnostics Journal No. 4. 013
CAPture A selection o recent allergy papers
SYNOPSISCombined testing o sIgE to a/b/g-gliadin
andw5-gliadinincreased the sensitivity to 100% in a population
o
WDEIA patients
Serum IgE tow5-gliadin has earlier been shown to have an 80%
sensitivity todetect wheat-dependent exercise-induced anaphylaxis
(WDEIA). The aim o thepresent study was to analyze the IgE
sensitization proles o adult WDEIA patients(n=17) using well
characterized puried wheat allergen components on theImmunoCAP
platorm. The diagnosis o WDEIA was based on clinical history
andchallenge tests o most patients.
The sensitivity o serum IgE to either w5-gliadin or
a/b/g-gliadin was both 82%(14/17) when a cut o at 0.35 kUA/l was
applied. Three patients negative tow5-gliadin were all positive to
a/b/g-gliadin, indicating that by combined testingor specic IgE to
w5-gliadin and a/b/g-gliadin would increase the test sensitivityto
100% in this population. Analyzing sIgE to HMW (high molecular
weight glutenin)in addition to w5-gliadin did not increase the
sensitivity o testing, and serum IgEto HMW on itsel was shown to
have a sensitivity o 59%. Only one patient haddetectable serum IgE
to wheat LTP and AAI dimer in this study.
The authors conclude that by using combined testing o IgE to
w5-gliadin anda/b/g-gliadin, the gap in the in vitro diagnostics o
WDEIA might be closed.
Citation: Hofmann SC et al. IgE detection toa/b/g-gliadin and
its clinicalrelevance in wheat-dependent.
Allergy 2012; 67:1457.
Citation: Pedrosa M et al. Peanut seed storage proteins are
responsible forclinical reactivity in Spanish peanut-allergic
children.Pediatr Allergy Immunol. 2012;23:654-9.
Adultpatients(agerange17-60y)withtypicalhistoryoWDEIA
wererecruited.
Infvepatientsco-actorssuchasaspirin,alcoholand/orinection
wereinvolvedinelicitingsymptoms.
IgEtowheatextractandtow5-gliadinwerequantifedwithcommerciallyavailableImmunoCAPtestsusingacutoat
0.35kUA/l.(PhadiaLaboratorySystem,ThermoFisherScientifc,
Uppsala,Sweden).
SerumIgEtoa/b/g-gliadin,high-molecular-weightglutenin(HMW-glutenin),alpha-amylaseinhibitordimer(AAI)andwheatLTP
wereanalyzedusingexperimentalImmunoCAP.
Theresultswerebasicallyconfrmedinamicroarraytechnology
platorm.
SYNOPSISThe majority o peanut allergic children in the
Mediterranean area are sensitized to storage proteins
and not LTP
Previous studies have shown geographical variations in the
sensitization prolesand clinical phenotypes in peanut ood allergy.
The most established conclusionhas been that sensitization to
storage proteins dominates worldwide except in theMediterranean
area where sensitization to lipid transer protein (LTP) related
topeach allergy is common.
The aim o the present study was to see i this could be conrmed
by comparing
sera rom unselected peanut allergic Spanish children and peanut
tolerantchildren with suspected ood allergy using the ImmunoCAP
ISAC microarray.Sensitization to storage proteins was more common
than sensitization to LTP(76% vs. 47%) in Spanish peanut allergic
children. IgE to storage proteinswas signicantly (p
-
7/29/2019 alergi kacang
4/12
4
ImmunoDiagnostics Journal No. 4. 013
Clinical Utility o Peanut Components
phenotypic characterization o peanut
allergic patients
Background
Peanut allergy is one o the most common ood allergiesin
childhood in many parts o the world, oten appearingalready during
the rst two years o lie. The prevalence hasbeen estimated to be 1-
2% but this gure varies widelybetween studies rom dierent countries
and also dependson how the diagnosis is made e.g. reported disease
vs.
challenge veried disease(1, 2).
Peanut allergic inants oten have a concomitant allergy to
otheroods e.g. egg and milk. Unlike milk and egg allergy,
peanutallergy used to be considered a lielong disease. However,
itis now reported that approximately 20% o peanut allergicchildren
develop tolerance within the rst ve years o lie, andthat in those
with low peanut-specic IgE levels as many as50-60% may outgrow
their peanut allergy(3, 4).
The requency o peanut allergy appears to have increasedduring
recent years and as allergy to peanut and tree nutsoten lead to
severe systemic reactions and anaphylacticshock, they have received
much attention(5-9). In the ewcases where peanut allergy leads to
atal reactions, mainlyadolescents and young adults with concomitant
asthma are
aected(10, 11).
Peanut allergen components have since several yearsbeen used in
clinical studies, showing the relationbetween dierent sensitization
phenotypes and clinicalmaniestations o peanut allergy. Some o the
previousconclusions drawn on prevalence, incidence and
tolerancedevelopment in peanut allergy based on peanut extracttests
may have to be re-evaluated with these new tools.
-
7/29/2019 alergi kacang
5/12
5
ImmunoDiagnostics Journal No. 4. 013
Sensitization Phenotypes o Peanut AllergyRecombinant DNA
technology allows the ecientproduction o pure peanut allergen
components that todayare used or component resolved diagnosis (CRD)
inpatients with a suspicion o peanut allergy. CRD helps toidentiy
the most serious sensitization phenotypes where
the allergic patients runs the risk o anaphylactic reactions,and
to distinguish these rom those who will react only withmild, i any,
symptoms. Patients previously diagnosed aspeanut allergic may
thereby be relived rom daily anxiety aswell as unnecessary dietary
restrictions.
Peanut allergy related to storage proteins
Peanut allergy associated with sensitization to the
storageproteins Ara h 1, Ara h 2 and/or Ara h 3 is the most
seriousorm o peanut allergy, and has now been described all overthe
world Europe, USA, Asia and Australia(13-17) andrecently also in
the Mediterranean area, where previouslypeanut allergic children
and adults were shown to mainly beo other sensitization
phenotypes(18).
The sensitization to storage proteins oten appears early inlie,
even beore the age o one year, and can be shownin patients with
clinical allergy also to other legumes suchas soy(19, 20) and
lentils(21) but also to tree nuts(22) andvarious seeds such as
sesame seeds(22-24). Children whosuer rom severe atopic dermatitis
and who are sensitizedto egg and milk during their rst year o lie
appear to beat higher risk o sensitization to peanut and soy
storageproteins(15, 25-27).
Peanut allergic patients who develop tolerance over time
may be those sensitized to storage proteins, as the diseaseonset
precedes that o sensitization to aeroallergens.Ho et al. showed
that low levels (< 3 kUA/l) o IgE topeanut extract in the rst 2
years or decreasing levels bythe age o 3 predict likely remission o
peanut allergy(28).A similar decrease in sensitization requency
during therst three years o lie has been shown also in soy
extract
sensitized inants(29). This indicates that sensitizationto
storage proteins, although associated with severesymptoms, still
may be outgrown in early lie. Recurrenceo peanut allergy has been
shown at older age in somestudies however i this phenomenon is due
to the samestorage protein dependent phenotype or is due to an
onseto a new, pollen related phenotype, has not been shown(3).
Storage proteins are very stable to heat, low pH andprotease
activity in the gastrointestinal tract, explaining whythis peanut
sensitization phenotype is highly associated withallergic
anaphylaxis and even death.
It is well known that many more individuals are peanutsensitized
than who actually have allergic symptoms topeanut. In the MAAS
birth cohort, or example, it wasshown that 11.8% o 8 years old
children were sensitizedto peanut extract while only 22.4% o the
sensitized
children reacted in peanut challenge tests(12). Thus,
eightypercent o those showing positive peanut extract testswere not
peanut allergic in this non-selected childhoodpopulation. In the
same study peanut storage proteincomponents could discriminate
between serious and lessserious sensitization phenotypes o peanut
allergy.
Component Protein type Comments
Arah1 Storageprotein
7Svicilin-likeglobulin
Peanutspecifcmarker
Arah2 Storageprotein
2Salbumin,conglutinin
Peanutspecifcmarker
Arah3 Storageprotein
11Sglobulin
Peanutspecifcmarker
Arah5 Proflin Markerograsspollencross-reactivity,
lowclinicalrelevance
Arah6 Storageprotein
2Salbumin,conglutinin
Peanutspecifcmarker
HighlysimilartoArah2
Arah8 PR-10protein Markerotreepollencross-reactivity
Arah9 nsLTP Markeropeachcross-reactivity
Peanut allergen components
-
7/29/2019 alergi kacang
6/12
ImmunoDiagnostics Journal No. 4. 013
LTP-related peanut allergy
The LTP (lipid transer protein) phenotype o peanut
allergy,characterized by sensitization to Ara h 9, has mainly
beendescribed in the Mediterranean area and is suggestedto be
caused by cross-reactivity in patients sensitized topeach LTP(17,
30). In contrast to storage protein-relatedpeanut allergy, this orm
o peanut allergy seems to startsomewhat later in lie, apparently
when sensitizations aretriggered by inhalant allergens(17).
Patients with LTP-relatedpeanut allergy are seldom reported to be
under 10 yearso age and are usually older(30, 31).
LTPs are very stable in the gastrointestinal tracts (low
pH,proteases) and thereore LTP sensitization is also a riskactor or
serious systemic reactions in peanut allergic
(lip swelling, stomach cramping and tiredness), possibly dueto
sensitization to other storage proteins such as Ara h 6 (38).
As always, in assessing the risk o severe reactions to
anyallergen it is important to be aware o the act that
allergicsymptoms are not only based on the allergen specic
IgEconcentrations but also on the dose o the allergen per se,as
well as other contributing actors such exercise, NSAIDdrugs and
inections.
Grass pollen related allergy
Grass sensitization is the most common cause o prolinand
cross-reactive carbohydrate determinant (CCDs)sensitization in ood
allergic patients, and both prolinand CCD antibodies are highly
cross-reactive with peanutprolin (Ara h 5) and CCDs(39). It is
however broadlyaccepted that the clinical relevance o these
sensitizationsis generally low, which is true also in peanut
allergy (40-46).
As or other pollen allergens, sensitization to prolin is
mainly detectable ater inancy (> 2 years o age). Whenusing
recombinant components in the diagnostic testing,sensitization to
CCDs is not detected, and thus theseclinically irrelevant
antibodies do not obscure the testresults.
Tree pollen-related peanut allergy
Extract based peanut specic IgE tests are oten positive
inpatients living in areas rich in birch due to
cross-reactivitybetween Bet v 1 in birch and its homolog Ara h 8
inpeanut. In other geographic areas, PR-10 proteins romother tree
pollen such as alder, beech or oak may giverise to the same type o
cross-reactivity(36, 37). PR-10sensitization thereore coincides
with the development oinhalation allergies and is mostly seen in
children older than
2 years o age.Food allergic reactions caused by PR-10
sensitization areusually restricted to the oral cavity which can be
ascribedto their unstable nature; already in the mouth the allergen
isdegraded and heated oods are oten tolerated.
Thus, the PR-10 dependent sensitization phenotype inpeanut
allergy is considered a mild orm, with low riskor severe reactions.
This was nicely and convincinglydemonstrated in a clinical study
rom Sweden whereAsarnoj et al. showed that 90% o children
sensitized only
to Ara h 8 (the level o sensitization to storages proteinsAra h
1, Ara h 2 and Ara h 3 was below 0.35 kUA/l) didnot react in peanut
challenge while 9.7% reacted with OASat the rst two, but not
subsequent challenge doses. Onlyone single individual reported
other symptoms
patients, although in this phenotype it is also common thatonly
local reactions are elicited.
Although peach allergy is suspected to be the predominantcause o
LTP sensitization in the Mediterranean area, up to
25% o the peanut allergic patients are in act suggested tohave
primary sensitization to something else than peach(31).Gao et al.
recently showed that in Chinese peach allergicpatients the primary
driver o LTP-sensitization diereddepending on the geographical
location and exposureto dierent possible triggers(32), and already
previouslymugwort and plane tree pollen were suggested to drive
LTPsensitization(32-35). In conclusion, there are
uncertaintiesregarding the primary source o LTP sensitization.
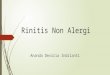
Labile protein low amount
Stable protein high amount
Ara h 5 Ara h 8 Ara h 9 Ara h 1
Ara h 2
Ara h 3
PR-10 LTPProfilinStorageProteins
Likelihood of
asymptomatic
sensitization
Two peanut sensitization phenotypes can give rise to serious
systemic reactions; those caused by sensitization to storage
proteins and to lipid transer
proteins (LTP), respectively. These are both stable proteins and
abundant in peanuts. The proflin and PR-10 phenotypes may be
asymptomatic or eliciting
mainly local reactions, as these proteins are readily degraded,
heat sensitive and o low abundance in peanuts.
-
7/29/2019 alergi kacang
7/12
ImmunoDiagnostics Journal No. 4. 013
Combining tests or increased perormance
Improved clinical sensitivity
Increased sensitivity o the ImmunoCAP technology nowenables
reliable quantication o allergen-specic IgE downto 0.1 kUA/l, as
compared to previously 0.35 kUA/l. As aconsequence, the clinical
sensitivity has also improved, as
shown in recently published studies. In a selected populationand
using the lower limit o detection (0.1 kUA/l), a
100%sensitivity(47) was obtained when diagnosing peanut allergyas
compared to 90-96% sensitivity in similar populationswhen the
higher cut o level was applied(48, 49).
Peanut allergic patients o all phenotypes - storage protein,LTP,
PR-10 and prolin - are positive in peanut extracttests when using
the 0.1 kUA/l cut-o
(12, 31, 50), and thus anegative test excludes peanut allergy
with a high degree ocertainty, i.e. the NPV is high.
Ideally, in vitrodiagnostic tests should provide results
thatenable complete separation o patients in those who havea
disease and those who do not, leaving no cases ounclear diagnosis -
in other words the positive and negativepredictive values should
both be 100%. This is howevernever the case or any allergy test as
many dierent actorsinfuence the clinical symptoms and there is no
singlemeasurable marker that alone can discriminate betweenclinical
disease and no disease.
O importance or the clinical situation is that predictivevalues
depend not only on the sensitivity and specicityo the test, but
also to a high degree on the prevalence odiseased patients in the
tested population. As soon as thesensitivity and specicity are less
than 100% the positiveand negative predictive values decrease
rapidly as theprevalence decreases. This means that specic IgE
testingnever should be used as a screening test in a
generalpopulation but only be used as an aid or the clinician
whenthere is a suspicion o allergy.
Increasing clinical specifcity
A high specicity is needed to obtain a high positivepredictive
value o a diagnostic test, especially i theprevalence o the disease
is low. Increasing the specicitywhile maintaining the sensitivity
improves the test, and in
the case o peanut allergy this is now achieved by usingCRD in
combination with extract based testing. A negativetest (below 0.1
kUA/l) or the storage protein Ara h 2excludes storage protein
related peanut allergy with a veryhigh probability (although it
cannot be ully excluded), andadditional testing o IgE antibodies to
other storage proteins- Ara h 1, Ara h 3 and Ara h 6 - increases
thecertainty(15, 18, 51-53).
AnegativeIgEtest(
-
7/29/2019 alergi kacang
8/12
ImmunoDiagnostics Journal No. 4. 013
Confrm or exclude peanut allergyThe use o peanut extract based
tests
The cut-o o 15kUA/l or extract based peanut IgE testshas been
widely used in studies and clinical routine tominimize the number o
challenges perormed(49, 54, 55).However, this decision point is
based on data rom aselected population at an allergy specialist
level and haslow sensitivity since roughly 50% o patients
sensitizedbelow this level are clinical reactive(12, 47, 56). This
indicatesthat test designs solely based on peanut extract can
onlyreplace a certain number o ood challenges in the
clinicalroutine.
Storage proteins as discriminators
Through many studies it is now well established
thatsensitization to the storage protein Ara h 2 has the
highest
potential o the three storage proteins or discriminatingbetween
symptomatic and non-symptomatic peanutallergy(12, 47, 53, 57-61).
Decision points o both 100%sensitivity and specicity have been
determined in dierentstudies by quantiying IgE to Ara h 2 down to
0.1kUA/l
(53,
57, 58, 62). However it must be noted that such decisionpoints
also or components are dependent on the kind opatients tested and o
the prevalence o the disease in thetested population.
Addition o Ara h 1, Ara h 3 and Ara h 6 specic IgE testswill
increase specicity and sensitivity to some degree, asnot all
patients who develop symptoms show sensitizationto Ara h 2(15, 18,
52, 53). In accordance with this,Ebisawa et al. showed that a
combination o all threecomponents increased the specicity but
decreased thesensitivity, underlining the dominating role o Ara h 2
orclinical symptoms(15).
SerumIgEtoArah2isthebestdiscriminatorosymptomaticandnon-symptomaticsensitizationinthe
storageproteinphenotype
ThetestcombinationIgEtopeanutextract(highsensitivity)andtoArah2(highspecifcity)would
decreasetheneedooodchallengetestwith50-100%
IgEtestingtoadditionalstorageproteins(Arah1,Arah3,Arah6)mightleadtoimprovedrisk
assessment
Furthermore, it has been shown that both epitope diversitywithin
an allergen component as well as diversity including
concomitant sensitization to several dierent componentsis
associated with a more severe orm o storage proteinrelated peanut
allergy(63). This indicates that measuringsensitization to all
storage proteins could have additionalclinical value or risk
assessment(47, 55, 59).
In order to achieve an accurate and sae diagnosis o
peanutallergy, it is vital to quantiy also very low levels o
peanutcomponent specic IgE, as suggested by a study on apopulation
o peanut allergic inants where roughly 20 % othose with clinical
peanut allergy were shown to have Ara h 2levels below 0.35
kUA/l
(52).
It is essential to veriy a suspected diagnosis o storageprotein
related peanut allergy. Equally important, asSicherer et al
recently pointed out, is to be able to excludea hidden storage
protein dependent allergy in pollensensitized patients who have
mild peanut-associatedreactions(64).
-
7/29/2019 alergi kacang
9/12
ImmunoDiagnostics Journal No. 4. 013
Reduced need or ood challenges
In ood allergy, double blind placebo controlled oodchallenge
(DBPCFC) is considered the gold standard or anaccurate diagnosis;
in practice however open challengesare mostly perormed. DBPCFC are
cumbersome,expensive and potentially dangerous, and thereore
thereis a strong need to reduce the number o challenges
stillreaching a sae and accurate diagnosis. CRD has beenshown in
several publications to be an aid in ullling thisneed in peanut
allergy.
In the study o Codreanu, a cut o o 0.23 kUA/l or IgE toAra h 2
was calculated that distinguished between clinicalpeanut allergy
and non-symptomatic sensitization with asensitivity and specicity o
93% and 96% respectively,and they concluded that by combining the
high sensitivityo the peanut extract based test with the high
specicity o
the Ara h 2-IgE test, oral challenges could be replaced(52).A
similar testing strategy, reducing the need o oodchallenge was
proposed by Lieberman et al. who showeda specicity o 91% using the
cut o value 0.35 kUA/l
(47).A third study that propose an analogous strategy is byDang
et al. where the need o ood challenge is shown to
Clinical Utility of peanut CRD
Helpstoexcludeclinicalpeanutallergy
Helpstoconfrmclinicalpeanutallergy
Identifespatientsathighriskorsystemicreaction(phenotyping)
Reducesneedoroodchallengetestinthediagnosticprocess
decrease by two thirds i inants rst are tested with IgEpeanut
extract and then Ara h 2, and only those withAra h 2 - specic IgE
levels between 0.1 and 1.0 kUA/lare selected or challenge test(14).
Hong et al. could denean optimal cut o point with a 99.1%
sensitivity and98.3% specicity with only 1.2% misclassication(28),
andin a patient population studied by Eller at al. the need oood
challenge tests decreased with 55% when using a cuto or Ara h 2 at
>1.63 kUA/l.
Taken together, these studies suggest that the optimalstrategy
is to combine extract based peanut IgE tests withquantication o Ara
h 2-specic IgE antibodies down to0.1 kUA/l. Application o this
diagnostic workup woulddecrease the need o ood challenge test with
50-100%depending on the tested population.
The best guess based on what has been reported up totoday is
that a decision point with high predictive value(above 95%) or
diagnosing storage protein related peanutallergy would be somewhere
between 0.25-1.5 kUA/ldepending on the selected population.
-
7/29/2019 alergi kacang
10/12
10
ImmunoDiagnostics Journal No. 4. 013
LITERATURE LIST1. Custovic A, Nicolaou N.
Peanutallergy:overestimatedinepidemiologyorunderdiagnosedinprimarycare?J
Allergy Clin Immunol. 2011;127:631-2.
2. Sicherer SH.Epidemiologyooodallergy.J Allergy Clin Immunol.
2011;127:594-602.
3. Fleischer DM, Conover-Walker MK, Christie L, Burks AW, Wood
RA.Thenaturalprogressionopeanutallergy:Resolutionandthepossibilityorecurrence.[seecomment].J
Allergy Clin Immunol. 2003;112(1):183-9.
4. Skolnick HS, Conover-Walker MK, Koerner CB, Sampson HA, Burks
W, Wood RA.Thenaturalhistoryopeanutallergy.J Allergy Clin Immunol.
2001;107(2):367-74.
5. Grundy J, Matthews S, Bateman B, Dean T, Arshad
SH.Risingprevalenceoallergytopeanutinchildren:Datarom2sequentialcohorts.J
Allergy Clin Immunol. 2002;110(5):784-9.
6. Lin RY, Anderson AS, Shah SN, Nurruzzaman
F.Increasinganaphylaxishospitalizationsinthefrst2decadesolie:NewYorkState,1990-2006.
Ann Allergy Asthma Immunol. 2008;101:387-93.
7. Rinaldi M, Harnack L, Oberg C, Schreiner P, St Sauver J,
Travis
L.PeanutallergydiagnosesamongchildrenresidinginOlmstedCounty,
Minnesota.J Allergy Clin Immunol. 2012;130:945-50.
8. Sicherer SH, Munoz-Furlong A, Godbold JH, Sampson
HA.USprevalenceosel-reportedpeanut,treenutandsesameseedallergy:11yearollowup.J
Allergy Clin Immunol. 2010;125:1322-6.
9. Sampson HA.Foodanaphylaxis.Br Med Bull. 2000;56:925-35.
10. Bock SA, Munoz-Furlong A, Sampson
HA.Fatalitiesduetoanaphylacticreactionstooods.J Allergy Clin
Immunol. 2001;107(1):191-3.
11. Foucard T, Malmheden Yman
I.AstudyonsevereoodreactionsinSwedenissoyproteinanunderestimatedcauseooodanaphylaxis?
Allergy. 1999;54(3):261-5.
12. Nicolaou N, Poorashar M, Murray C, Simpson A, Winell H,
Kerry G, et al.
Allergyortoleranceinchildrensensitizedtopeanut:prevalenceanddierentiationusingcomponent-resolveddiagnostics.J
Allergy Clin Immunol. 2010 Jan;125(1):191-7 e1-13.
13. Chiang WC, Pons L, Kidon MI, Liew WK, Goh A, Wesley Burks
A.SerologicalandclinicalcharacteristicsochildrenwithpeanutsensitizationinanAsiancommunity.Pediatr
Allergy Immunol. 2010 Mar;21(2 Pt 2):e429-38.
14. Dang TD, Tang M, Choo S, Licciardi PV, Koplin JJ, Martin PE,
et al.IncreasingtheaccuracyopeanutallergydiagnosisbyusingArah2.J
Allergy Clin Immunol. 2012 Apr;129(4):1056-63.
15. Ebisawa M, Movrare R, Sato S, Maruyama N, Borres MP, Komata
T.MeasurementoArah1-,2-,and3-specifcIgEantibodiesisuseulindiagnosisopeanutallergyinJapanesechildren.Pediatric
Allergy and Immunology. 2012;23(6):573-81.
16. L in YT, Wu CT, Cheng JH, Huang JL, Yeh
KW.PatternsosensitizationtopeanutallergencomponentsinTaiwanesePreschoolchildren.J
Microbiol Immunol Infect. 2012 Apr;45(2):90-5.
17. Vereda A, van Hage M, Ahlstedt S, Ibanez MD, Cuesta-Herranz
J, van Odijk J, et
al.Peanutallergy:Clinicalandimmunologicdierencesamongpatientsrom3dierentgeographicregions.J
Allergy Clin Immunol. 2010 Nov 17.
18. Pedrosa M, Boyano-Martinez T, Garcia-Ara MC, Caballero T,
Quirce
S.PeanutseedstorageproteinsareresponsibleorclinicalreactivityinSpanishpeanut-allergicchildren.Pediatr
Allergy Immunol. 2012 Nov;23(7):654-9.
19. Adachi A, Horikawa T, Shimizu H, Sarayama Y, Ogawa T,
Sjolander S, et
al.Soybeanbeta-conglycininasthemainallergeninapatientwithood-dependentexercise-inducedanaphylaxisbytou:oodprocessingalterspepsinresistance.Clin
Exp Allergy. 2009 Jan;39(1):167-73.
20. Holzhauser T, Wackermann O, Ballmer-Weber BK,
Bindslev-Jensen C, Scibilia J,Perono-Garoo L, et
al.Soybean(Glycinemax)allergyinEurope:Glym5(beta-conglycinin)andGlym6(glycinin)arepotentialdiagnosticmarkersorsevereallergicreactions
tosoy.J Allergy Clin Immunol. 2009 Feb;123(2):452-8.
21. Lopez-Torrejon G, Salcedo G, Martin-Esteban M, Diaz-Perales
A, Pascual CY,Sanchez-Monge
R.Lenc1,amajorallergenandvicilinromlentilseeds:ProteinisolationandcDNAcloning.J
Allergy Clin Immunol. 2003;112(6):1208-15.
22. Pastorello EA, Pompei C, Pravettoni V, Brenna O, Farioli L,
Trambaioli C, et
al.Lipidtranserproteinsand2Salbuminsasallergens.
Allergy. 2001;56(Suppl 67):45-7.
23. Leduc V, Moneret-Vautrin DA, Tzen JT, Morisset M, Guerin L,
Kanny
G.Identifcationooleosinsasmajorallergensinsesameseedallergicpatients.
Allergy. 2006 Mar;61(3):349-56.
24. Magni C, Ballabio C, Restani P, Fuggetta D, Alessandri C,
Mari A, et al.
MolecularinsightintoIgE-mediatedreactionstosesame(Sesamum
indicumL.)seedproteins.
Ann Allergy Asthma Immunol. 2010 Dec;105(6):458-64.
25. Du Toit G, Roberts G, Sayre PH, Plaut M, Bahnson HT,
Mitchell H, et
al.Identiyinginantsathighriskopeanutallergy:TheLearningEarlyAboutPeanutAllergy(LEAP)screeningstudy.J
Allergy Clin Immunol. 2013;131(1):135-43.e12.
26. Sicherer SH, Wood RA, Stablein D, Burks AW, Liu AH, Jones
SM, et
al.Immunologiceaturesoinantswithmilkoreggallergyenrolledinanobservationalstudy(ConsortiumoFoodAllergyResearch)ooodallergy.J
Allergy Clin Immunol. 2010 May;125(5):1077-83 e8.
27. Sicherer SH, Wood RA, Stablein D, Lindblad R, Burks AW, Liu
AH, et
al.Maternalconsumptionopeanutduringpregnancyisassociatedwithpeanutsensitizationinatopicinants.J
Allergy Clin Immunol. [doi: DOI:
10.1016/j.jaci.2010.08.036].2010;126(6):1191-7.
28. Ho MH, Wong WH, Heine RG, Hosking CS, Hill DJ, Allen KJ.
Earlyclinicalpredictorsoremissionopeanutallergyinchildren.J
Allergy Clin Immunol. 2008 Mar;121(3):731-6.
29. Ahn KM, Han YS, Nam SY, Park HY, Shin MY, Lee
SI.Prevalenceosoyproteinhypersensitivityincowsmilkprotein-sensitivechildreninKorea.J
Korean Med Sci. 2003;18:473-7.
30. Javaloyes G, Goikoetxea MJ, Garcia-Nunez I, Aranda A, Sanz
ML, Blanca M, et
al.Prup3actsasastrongsensitzerorpeanutallergyinSpain.J Allergy Clin
Immunol. 2012;130:1432-4.
31. Krause S, Reese G, Randow S, Zennaro D, Quaratino D, Palazzo
P, et
al.Lipidtranserprotein(Arah9)asanewpeanutallergenrelevantoraMediterraneanallergicpopulation.J
Allergy Clin Immunol. 2009 Aug 7.
32. Gao ZS, Yang ZW, Wu SD, Wang HY, Liu ML, Mao WL, et
al.PeachallergyinChina:Adominantroleormugwortpollenlipidtranserproteinasaprimarysensitizer.J
Allergy Clin Immunol. 2013 Jan;131(1):224-6 e3.
33. Lauer I, Miguel-Moncin MS, Abel T, Foetisch K, Hartz C,
Fortunato D, et
al.Identifcationoaplanepollenlipidtranserprotein(Plaa3)anditsimmunologicalrelationtothepeachlipid-transerprotein,Prup3.Clin
Exp Allergy. 2007 Feb;37(2):261-9.
34. Lombardero M, Garcia-Selles FJ, Polo F, Jimeno L, Chamorro
MJ,Garcia-Casado G, et
al.PrevalenceosensitizationtoArtemisiaallergensArtv1,Artv3and
Artv60kDa.Cross-reactivityamongArtv3andotherrelevantlipid-transerproteinallergens.Clin
Exp Allergy. 2004 Sep;34(9):1415-21.
35. Pascal M, Munoz-Cano R, Reina Z, Palacin A, Vilella R,
Picado C, et
al.Lipidtranserproteinsyndrome:clinicalpattern,coactoreectandprofleomolecularsensitizationtoplant-oodsandpollens.Clin
Exp Allergy. 2012 Oct;42(10):1529-39.
36. Egger C, Focke M, Bircher AJ, Scherer K, Mothes-Luksch N,
Horak F, et al.Theallergenprofleobeechandoakpollen.Clin Exp
Allergy. 2008 Aug 25.
37. Maeda Y, Ono E, Fukutomi Y, Taniguchi M, Akiyama
K.CorrelationsbetweenalderspecifcIgEandalder-relatedtreepollenspecifcIgEbyRASTmethod.
Allergol Int. 2008 Mar;57(1):79-81.
38. Asarnoj A, Nilsson C, Lidholm J, Glaumann S, stblom E,
Hedlin G, et
al.PeanutcomponentArah8sensitizationandtolerancetopeanut.J Allergy
Clin Immunol. 2012;130(2):468-72.
39. Cabanos C, Tandang-Silvas MR, Odijk V, Brostedt P, Tanaka A,
Utsumi S, et
al.Expression,purifcation,cross-reactivityandhomologymodelingopeanutproflin.Protein
Expr Purif. 2010 Sep;73(1):36-45.
40. Diez-Gomez ML, Quirce S, Cuevas M, Sanchez-Fernandez C, Baz
G,Moradiellos FJ, et
al.Fruit-pollen-latexcross-reactivity:implicationoproflin(Betv2).
Allergy. 1999;54(9):951-61.
41. Ebo DG, Hagendorens MM, Bridts CH, De Clerck LS, Stevens
WJ.Sensitizationtocross-reactivecarbohydratedeterminantsandtheubiquitousproteinproflin:mimickersoallergy.
Clin Exp Allergy. 2004;34(1):137-44.42. Guilloux L, Morisset M,
Codreanu F, Parisot L, Moneret-Vautrin DA.
PeanutAllergyDiagnosisintheContextoGrassPollenSensitizationor125Patients:RolesoPeanutandCross-ReactiveCarbohydrateDeterminantsSpecifcIgE.Int
Arch Allergy Immunol. 2009 Jan 6;149(2):91-7.
-
7/29/2019 alergi kacang
11/12
11
ImmunoDiagnostics Journal No. 4. 013
43. Moverare R, Ahlstedt S, Bengtsson U, Borres MP, van Hage M,
Poorashar M, et
al.EvaluationoIgEAntibodiestoRecombinantPeanutAllergensinPatientswithReportedReactionstoPeanut.Int
Arch Allergy Immunol. 2011 Jun 29;156(3):282-90.
44. Radauer C, Willerroider M, Fuchs H, Homann-Sommergruber K,
Thalhamer J,Ferreira F, et
al.Cross-reactiveandspecies-specifcimmunoglobulinEepitopesoplantproflins:anexperimentalandstructure-basedanalysis.Clin
Exp Allergy. 2006 Jul;36(7):920-9.
45. Twardosz-Kropmuller A, Singh MB, Niederberger V, Horak F,
Krat D, Spitzauer S,et al.
AssociationoallergicpatientsphenotypeswithIgEreactivitytorecombinantpollenmarkerallergens.
Allergy. 2009 Oct 12.
46. van der Veen MJ, van Ree R, Aalberse RC, Akkerdaas J,
Koppelman SJ,Jansen HM, et
al.Poorbiologicactivityocross-reactiveIgEdirectedtocarbohydratedeterminantsoglycoproteins.J
Allergy Clin Immunol. 1997;100(3):327-34.
47. Lieberman JA, Glaumann S, Batelson S, Borres MP, Sampson HA,
Nilsson
C.TheutilityopeanutcomponentsinthediagnosisoIgE-mediatedpeanutallergyamongdistinctpopulations.J
Allergy Clin Immunol In Practice. 2013;1:75-82.
48. Maloney JM, Rudengren M, Ahlstedt S, Bock SA, Sampson
HA.TheuseoserumspecifcIgEmeasurementsorthediagnosisopeanut,treenut,andseedallergy.
J Allergy Clin Immunol. 2008 May 23.49. Sampson HA, Ho DG.
Relationshipbetweenood-specifcIgEconcentrationsandtheriskopositiveoodchallengesinchildrenandadolescents.J
Allergy Clin Immunol. 1997;100(4):444-51.
50. Romano A, Fernandez-Rivas M, Caringi M, Amato S, Mistrello
G, Asero
R.Allergytopeanutlipidtranserprotein(LTP):requencyandcross-reactivitybetweenpeanutandpeachLTP.Eur
Ann Allergy Clin Immunol. 2009 Aug;41(4):106-11.
51. Codreanu F, Collignon O, Roitel O, Thouvenot B, Sauvage C,
Vilain AC, et
al.ANovelImmunoassayUsingRecombinantAllergensSimplifesPeanutAllergyDiagnosis.Int
Arch Allergy Immunol. 2011 Sep 21;154(3):216-26.
52. Asarnoj A, Glaumann S, Elstrom L, Lilja G, Lidholm J,
Nilsson C, et
al.AnaphylaxistoPeanutinaPatientPredominantlySensitizedtoArah6.Int
Arch Allergy Immunol. 2012 Jun 1;159(2):209-12.
53. Eller E, Bindslev-Jensen C.
Clinicalvalueocomponent-resolveddiagnosticsinpeanut-allergicpatients.Allergy.
2012 Dec 14.
54. Roberts G, Lack
G.DiagnosingpeanutallergywithskinprickandspecifcIgEtesting.J
Allergy Clin Immunol. 2005 Jun;115(6):1291-6.
55. van Nieuwaal NHG, Lasar W, Meijer Y, Kentie PA, Flinterman
AE, Pasmans SGAM,et
al.Utilityopeanut-specifcIgElevelsinpredictingtheoutcomeodouble-blind,placebo-controlledoodchallenges.J
Allergy Clin Immunol. [doi: DOI:
10.1016/j.jaci.2010.01.057].2010;125(6):1391-2.
56. Beyer K, Ellman-Grunther L, Jarvinen KM, Wood RA, Hourihane
J, Sampson
HA.Measurementopeptide-specifcIgEasanadditionaltoolinidentiyingpatientswithclinicalreactivitytopeanuts.J
Allergy Clin Immunol. 2003;112(1):202-7.
57. Nicolaou N, Murray C, Belgrave D, Poorashar M, Simpson A,
Custovic
A.QuantifcationospecifcIgEtowholepeanutextractandpeanutcomponentsinpredictionopeanutallergy.J
Allergy Clin Immunol. 2011 Jan 25.
58. Asarnoj A, Moverare R, Ostblom E, Poorashar M, Lilja G,
Hedlin G, et
al.IgEtopeanutallergencomponents:relationtopeanutsymptomsandpollensensitizationin8-year-olds.
Allergy. 2010 Sep;65(9):1189-95.
59. Flinterman AE, van Hoen E, den Hartog Jager CF, Koppelman S,
Pasmans SG,Hoekstra MO, et
al.ChildrenwithpeanutallergyrecognizepredominantlyArah2andArah6,whichremainsstableovertime.Clin
Exp Allergy. 2007 Aug;37(8):1221-8.
60. Hong X, Caruso D, Kumar R, Liu R, Liu X, Wang G, et
al.IgE,butnotIgG4,antibodiestoArah2distinguishpeanutallergyromasymptomaticpeanutsensitization.
Allergy. 2012 Oct 25.
61. Glaumann S, Nopp A, Johansson SG, Rudengren M, Borres MP,
Nilsson
C.Basophilallergenthresholdsensitivity,CD-sens,IgE-sensitizationandDBPCFCinpeanut-sensitizedchildren.
Allergy. 2012 Feb;67(2):242-7.
62. Klemans RJ, Otte D, Knol M, Knol EF, Meijer Y,
Gmelig-Meyling FH, et
al.ThediagnosticvalueospecifcIgEtoArah2topredictpeanutallergyinchildreniscomparabletoavalidatedandupdateddiagnosticpredictionmodel.J
Allergy Clin Immunol. 2013;131:157-63.
63. Shrefer WG, Beyer K, Chu TH, Burks AW, Sampson
HA.Microarrayimmunoassay:associationoclinicalhistory,in
vitroIgEunction,andheterogeneityoallergenicpeanutepitopes.[seecomment].J
Allergy Clin Immunol. 2004;113(4):776-82.
64. Sicherer SH, Wood RA.Advancesindiagnosingpeanutallergy.J
Allergy Clin Immunol In Practice. 2013;1:1-13.
-
7/29/2019 alergi kacang
12/12
Printedonrecycledpaper.
Head ofce Sweden+46 18 16 50 00Austria+43 1 270 20 20
Belgium +32 2 749 55 15Brazil+55 11 3345 5050China+86 21 6865
4588Czech Republic +420 220 518 743Denmark+45 70 23 33 06Finland
+358 9 3291 0110France +33 1 61 37 34 30
thermoscientifc.com/phadia
2013 Thermo Fisher Scientic Inc. All rights reserved. All
trademarks are the property o Thermo Fisher Scientic Inc. and its
subsidiaries.Manuacturer; Phadia AB, Uppsala Sweden.
Germany+49 761 47 8050Hong Kong +852 2885 4613
India +91 11 4610 7555/56Italy +39 02 64 163 411Japan +81 3 5365
8332Korea+82 2 2027 5400Norway+47 21 67 32 80Portugal +351 21 423
5350South Arica +27 11 792 6790
Spain +34 935 765 800Sweden +46 18 16 60 60Switzerland +41 43
343 4050Taiwan +886 2 2516 0925The Netherlands +31 30 602 37
00United Kingdom/Ireland +44 1 908 769 110USA+1 800 346 4364Other
countries +46 18 16 50 00