Embed Size (px)
Citation preview

Dental Workforce Capacity and California’s Expanding Pediatric Medicaid PopulationCarrie Tsai, DMD, MPH*
Elizabeth Mertz, PhD, MA
Cynthia Wides, MA
DPH 175 Seminar, March 26th, 2013

Background
California’s public insurance programs have served
> 6 million children in 2010 Medicaid (4.5 million); State Children’s Health Insurance Program (S-CHIP) (1.7 million)
Called “Healthy Families” in California
Income Poor Low Middle High
Type of Insuran
ce
Medicaid
(ESPDT)
CHIP
Private Insurance through State Exchanges and
Possible Coverage Through Employers

Income ( as percentage of FPL )
250%
200%
133%
100%
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Age of Child
Medicaid (Denti-Cal)
Medicaid
S-CHIP
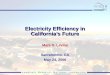
Former HFP & Medicaid Income Eligibility Levels

Healthy Families Transition Currently in the process of being eliminated shifting of almost
900,000 low-income children from S-CHIP to Medicaid
Income ( as percentage of FPL )
250%
200%
133%
100%
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Age of Child
Medicaid (Denti-Cal)
Medicaid
S-CHIP

Healthy Families Transition Currently in the process of being eliminated shifting of almost
900,000 low-income children from S-CHIP to Medicaid
Income (as percentage of FPL)
250%
200%
133%
100%
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Age of Child
All Covered by Medicaid

Patient Protection and Affordable Care Act (ACA)
Access to affordable, stable health insurance Key provision: universal coverage of pediatric dental care
Requires inclusion of dental benefits as integral to the required pediatric benefit package*
Maintains Medicaid eligibility and enrollment standards Expands minimum coverage for children of all age groups to
138% federal poverty level (FPL) Maintains S-CHIP program until 2019, ensured funding through
2015
* Unclear at this point if purchasing of dental plan will be required in the state exchanges

Study Goal
Assess the dentist workforce capacity to serve the newly
expanded Medicaid population
ACA mandated enrollment
Healthy Families Transition
The largest contributing factor

Methods
The following data was obtained for years 2006, 2008, 2011 Census data on total eligible Medicaid and S-CHIP populations
based on income eligibility brackets Numbers/locations of California Medicaid dental providers Numbers/locations of California Pediatric dental providers Pediatric dental enrollment and utilization within Medicaid and S-
CHIP (Healthy Families)
These data were analyzed using descriptive statistics to examine trends
Using a ratio of 1:1000 provider to population ratio (with a sensitivity analysis from 1:800 to 1:1200), shortages in each county were computed and these trends were analyzed according to county type

Methods
DEFINITIONS
Throughout the study, counties are differentiated by… Rural (N=35) vs urban (N=23):
“Rural Counties” defined as > 75% MSSAs designated rural or frontier “Urban Counties” defined as > 75% MSSAs designated urban by CA
Office of State Health Planning and Development (OSHPD)
Relative wealth of county As designated by Median Household Income of county Differentiated by top and bottom half, and by quartiles

Findings Outline
PopulationProvidersCapacity

California's Low-income Pediatric Population

Low-Income Pediatric Population
2006 2007 2008 2009 2010 2011 2012700000
750000
800000
850000
900000
950000
Enrolled
2005-2006
2006-2007
2007-2008
2008-2009
2009-2010
2010-2011
2000000
2100000
2200000
2300000
2400000
2500000
2600000
2700000
2800000
2900000
3000000
Children Eligible/Enrolled in Medicaid
Enrolled
Eligible
Alongside population increases, there are increases in enrollment in Medicaid and Healthy Families from 2006-2011
1 2 3 4 5 62,300,000
2,350,000
2,400,000
2,450,000
2,500,000
S-CHIP (Healthy Families) Eligible

2005-
2006
2006-
2007
2007-
2008
2008-
2009
2009-
2010
2010-
2011
-
2,000,000
4,000,000
6,000,000
8,000,000
10,000,000
12,000,000
Number of Medicaid Dental Procedures, age 0-20
Diagnostic
Preventive
Restorative
2005-2006
2006-2007
2007-2008
2008-2009
2009-2010
2010-2011
15
20
25
30
35
40
45
50
Medicaid Utilization Rate, age 0-20
Diagnostic
Preventive
Restorative
Pre
cen
t
AND, of those enrolled in Medicaid, numbers of procedures and rates of using dental services are increasing
• Note that in 2009, most adult Medicaid dental benefits were cut
Low-income Pediatric Population

Expanding Pediatric Medicaid Population from 2011 to end of 2013
Considering only those currently ENROLLED …
Now considering those that will be ELIGIBLE…
2.6 Million 3.5 Million Children
2.8 Million 5.2 Million Children

Medicaid Providers

Where are Medicaid-accepting dentists located? * Inclusive of pediatric dentists
1070494%
6886%
Medicaid Dentists by County Type
Urban Rural
309537%
418749%
7969%
3865%
Medicaid Dentists by Wealth of County
Highest Second Third Lowest
QUARTILES BY MEDIAN HOUSEHOLD INCOME
94% Medicaid dentists in urban counties, 6% in rural counties 86% in the wealthiest half of counties 49% in the wealthiest quartile of counties

Loss of Medicaid Providers
PERCENT CHANGE AND (N) IN MEDICAID DENTISTS FROM 2006-2011
Urban Counties Rural Counties
-5% (-533) -19% (-156)
Wealthiest Quartile of Counties
Poorest Quartile of Counties
-8% (-269) -15% (-69)
From 2006 to 2011, there was a decline in total dentists accepting Medicaid from 12,101 to 11,392
There was a disproportionate loss of Medicaid dentists when counties were differentiated by rural/urban status and by wealth (median household income) from 2006 to 2011

526%
83394%
Pediatric Dentists by County Type
Rural Urban
California Pediatric Dentists
35640%
48355%
303%
152%
Pediatric Dentists by Wealth of County
Highest Second Third Lowest
888 Total, 41% accept Medicaid
Urban: 833 pediatric dentists (36% accept Medicaid) Rural: 52 pediatric dentists (46% accept Medicaid) 95% in the wealthiest half of counties, 40% in the wealthiest quartile
QUARTILES BY MEDIAN HOUSEHOLD INCOME

So… we have a hugely expanding pediatric Medicaid population AND a shrinking Medicaid Network.
What, then, is the capacity of Medicaid dentists to serve the current and newly expanded pediatric Medicaid population?

Medicaid Dentist Shortages (Assumes no crossover from former HFP-only providers to Medicaid)
Dentists Available to Maintain 1:1000 provider to population ratio (range of 1:800 to 1:1200)
Current Eligible Population Newly Eligible Population
Urban -3 dentists (-628 to 413) -2129 (-3284 to -1359)
Rural -106 (-192 to -48) -337 (-481 to -214)
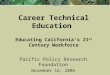
Currently, shortages that exist now are disproportionately seen in the rural counties
The shortages become more severe in all counties after ACA policy change and the HFP transition AND the shortage is worse in rural counties Would need a 20% increase in dentists in urban counties Would need a 50% increase in dentists in rural counties

Some Notable Counties
When calculating dentists available for the current Medicaid-eligible population using the 1:1000 provider to patient ratio, there were only a few counties with an actual surplus of dentists
These counties are all considered urban counties 3 out of 5 are in the wealthiest quartile
• Orange County• Los Angeles County• San Bernardino County • Santa Clara County• Ventura County

Some Notable Counties
When calculating dentists available for the newly Medicaid-eligible population using the 1:1000 provider to patient ratio, the following counties will have the largest shortages:
* Two of these counties have managed care Medicaid
• Sacramento*• Los Angeles*• San Diego• Riverside

-350
-300
-250
-200
-150
-100
-50
0
50
100
150
200
With Currently Eligible Med-icaid Population
With Newly Eligible Medicaid Population
Counties Ranked from more urban to more rural MSSA make-up
De
nti
sts
Av
aila
ble
(ne
ga
tiv
e #
= s
ho
rta
ge
, p
os
itiv
e #
= s
urp
lus
)
Dentists Available for the Current and Newly Eligible Pediatric Medicaid Population
RURAL COUNTIESURBAN COUNTIES
Outlier Los Angeles: -572 (range from -328 to -937)

Conclusions
The pediatric Medicaid population and enrollment into Medicaid increasing in size Possibly due to general population increase, policy changes
In addition, those children that are enrolled are utilizing dental services at increasing rates
Two very important policy changes happening NOW ACA mandated enrollment of low-income children in dental
programs Transition of ~880,000 children from Healthy Families (S-CHIP)
to Medicaid….

Conclusions
A misdistribution of dentists already exists (even more exaggerated with specialists) 94% of all Medicaid dentists and 94% pediatric dentists in urban
areas 90% of all Medicaid dentists and 95% pediatric dentists in the
wealthiest half of counties The Medicaid network has been shrinking… rural and poor
areas are experiencing a disproportionately higher loss of Medicaid dentists Dentists are either physically leaving or choosing to not accept
Medicaid anymore; new dentists are choosing not to accept Medicaid
There will be large shortages of Medicaid providers with the expanded population in all counties that continue to disproportionately affect rural and poor counties in California

Recommendations In order to keep up with the expanding pediatric Medicaid population…
more providers need to accept Medicaid OR existing Medicaid providers must accept and treat more Medicaid patients
1. Recruit more and maintain dental providers into the Medicaid program1. Streamline and expedite the enrollment process
2. Increase the reimbursement rates
3. Simplify the administration process for submitting claims
2. Improve data collection and monitoring capabilities1. Improve State data capacity
2. Make Medicaid (Denti-Cal) provider and claims info more easily accessible, timely and in more usable formats
3. Collect ESPDT dental data from federally funded clinics
4. Support programs like CHIS
3. Funding for the State Dental Director position