Embed Size (px)
Citation preview

DEFINITIONS
• acidemia/alkalemia– an abnormal pH
• acidosis/alkalosis– a process that if uncompensated would
lead to an abnormal pH

HENDESON-HASSELBACH
H+ = 24 pCO2
HCO3
H+ = 24 lungskidney
H+ = 24 4024

HENDERSON-HASSELBACH
H+ of 40nmol = pH of 7.4
for each 0.1 increase in pH multiply normal H+ x 0.8
for each 0.1 decrease in pH multiply normal H+ x 1.25

EXPECTED COMPENSATION
• metabolic acidosis - 1 HCO3/ 1 pCO2
• metabolic alkalosis - variable
• resp. acidosis– acute 1 HCO3 / 10 pCO2
– chronic 3-4 HCO3 / 10 pCO2
• resp. alkalosis– acute 2-3 HCO3 / 10 pCO2
– chronic 5 HCO3 / 10 pCO2

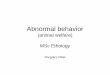
ACID-BASE COMPENSATION
ALKALOSES
pH 7.4
ACIDOSES
METABOLIC CHANGES RESPIRATORY CHANGES
DECREASE pCO2
INCREASE p CO2
INCREASE HCO3
DECREASE HCO3

THE ANION GAP
[Na] - (Cl + HCO3)
NaCl
HCO3
albumin
Anion gap

ANION GAP METABOLIC ACIDOSIS
• ketoacidosis• lactic acidosis• uremic acidosis• intoxications
– ASA– methanol– ethylene glycol– paraldehyde

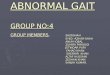
ASSESSMENT OF ACID-BASE DISTURBANCES
Arterial pH
< 7.35 Acidemia > 7.45 Alkalemia
Hx & Px
Check pH
Check pCO2
and HCO3
ExpectedcompensationACUTECHRONIC
CheckAnion GapNa-(Cl+HCO3)
PossibleDiagnoses
Low HCO3Metabolic Acidosis
High pCO2
Respiratory Acidosis
High HCO3Metabolic Alkalosis
Low pCO2
Respiratory Alkalosis
1 HCO3: 1 pCO2
1 HCO3: 1 pCO2
10 Pco2 :1 HCO3 10 Pco2 :3 HCO3
1 HCO3: 0.5 pCO2
1 HCO3: 0.5 pCO2
10 Pco2 :2 HCO3 10 Pco2 :5 HCO3
=12-16 >16
HCO3 LossR.T.A.Diarrhea
KetoacidosisLactic AcidosisRenal FailureIntoxications
ASAMethanolEthylene Glycol
COPDDrugs-CNS/RespDepressants
May be increased dueto increased negative
charge of proteins
Normotensive Hypertensive
Urine Cl
< 10Vomiting
Post-hypercapneia
> 10Diuretics
Conn’sCushing’s
Renal Artery Stenosis
DrugsHigh Altitude
ASAPregnancy
Sepsis

ANION GAP - METABOLIC ACIDOSIS
• H+ gaining acidoses– the H+ is buffered by HCO3
- so this is consumption of bicarbonate and a fall in plasma HCO3
• This process converts strong acids to weak acids– H2So4 + NaHCO3
NaHSO4 + H2CO3

ANION GAP METABOLIC ACIDOSES
• The consumption of bicarbonate by combining with a cation is electrically neutral and thus the Cl concentration stays normal as the bicarbonate falls and thus the anion gap [Na-(Cl+HCO3)] increases

NON-ANION GAP METABOLIC ACIDOSIS
• renal tubular acidosis
• diarrhea
• hyperailementation

ASSESSMENT OF ACID-BASE DISTURBANCES
Arterial pH
< 7.35 Acidemia > 7.45 Alkalemia
Hx & Px
Check pH
Check pCO2
and HCO3
ExpectedcompensationACUTECHRONIC
CheckAnion GapNa-(Cl+HCO3)
PossibleDiagnoses
Low HCO3Metabolic Acidosis
High pCO2
Respiratory Acidosis
High HCO3Metabolic Alkalosis
Low pCO2
Respiratory Alkalosis
1 HCO3: 1 pCO2
1 HCO3: 1 pCO2
10 Pco2 :1 HCO3 10 Pco2 :3 HCO3
1 HCO3: 0.5 pCO2
1 HCO3: 0.5 pCO2
10 Pco2 :2 HCO3 10 Pco2 :5 HCO3
=12-16 >16
HCO3 LossR.T.A.Diarrhea
KetoacidosisLactic AcidosisRenal FailureIntoxication's
ASAMethanolEthylene Glycol
COPDDrugs-CNS/RespDepressants
May be increased dueto increased negative
charge of proteins
Normotensive Hypertensive
Urine Cl
< 10Vomiting
Post-hypercapneia
> 10Diuretics
Conn’sCushing’s
Renal Artery Stenosis
DrugsHigh Altitude
ASAPregnancy
Sepsis

NON-ANION GAP MATABOLIC ACIDOSES
• These are HCO3 losing type metabolic acidoses
• The loss of HCO3 by the lower GI tract or the kidneys results in the need for increased Cl reabsorption to maintain electroneutrality
• Thus as HCO3 falls, Cl increases and the anion gap [Na-(Cl+HCO3)] stays normal

RENAL TUBULAR ACIDOSIS
• Renal loss of HCO3
– PCT a decrease in the tubular maximum for HCO3 reabsorption
– DCT a failure to be able to secrete H+

BICARBONATE RECLAMATION (PCT)
NaHCO3
URINE
H2CO3
pCO2 + H2O
CO2 + H2O
CA
H2CO3
HCO3H+
CA = Carbonic Anhydrase
CA
Na
HCO3

BICARBONATE REGENERATION(DCT)
NaHPO4
URINE
CO2 + H2O
CA
H2CO3
HCO3H+
CA = Carbonic Anhydrase
Na
HCO3
NaHSO4
H2PO4H2SO4
NH3NH4
+

METABOLIC ALKALOSIS
• vomiting
• post-hypercapneic
• diuretics
• Bartter’s syndrome

ASSESSMENT OF ACID-BASE DISTURBANCES
Arterial pH
< 7.35 Acidemia > 7.45 Alkalemia
Hx & Px
Check pH
Check pCO2
and HCO3
ExpectedcompensationACUTECHRONIC
CheckAnion GapNa-(Cl+HCO3)
PossibleDiagnoses
Low HCO3Metabolic Acidosis
High pCO2
Respiratory Acidosis
High HCO3Metabolic Alkalosis
Low pCO2
Respiratory Alkalosis
1 HCO3: 1 pCO2
1 HCO3: 1 pCO2
10 Pco2 :1 HCO3 10 Pco2 :3 HCO3
1 HCO3: 0.5 pCO2
1 HCO3: 0.5 pCO2
10 Pco2 :2 HCO3 10 Pco2 :5 HCO3
=12-16 >16
HCO3 LossR.T.A.Diarrhea
KetoacidosisLactic AcidosisRenal FailureIntoxications
ASAMethanolEthylene Glycol
COPDDrugs-CNS/RespDepressants
May be increased dueto increased negative
charge of proteins
Normotensive Hypertensive
Urine Cl
< 10Vomiting
Post-hypercapneia
> 10Diuretics
Conn’sCushing’s
Renal Artery Stenosis
DrugsHigh Altitude
ASAPregnancy
Sepsis

VOMITING
• Lose NaCl
• Lose HCl
• Lose volume
• this loss of acid generates the metabolic alkalosis
• ECF volume contraction also leads to secondary hyperaldosteronism

VOMITING
• Renal reaction volume contraction leads to avid Na reabsorption– NaCl first with elimination of Cl from urine– Na-H exchange but alkalosis means not
much H available– Na-K exchange but loss of K limits this
– thus NaHCO3 absorption which perpetuates the alkalosis

METABOLIC ALKALOSIS-POST HYPERCAPNEIA
• The primary problem is respiratory acidosis with the increased pCO2 leading to increased HCO3 to compensate
• If the pCO2 is suddenly normalized (e.g. by a respirator) the HCO3 is now in excess and there is a metabolic alkalosis. This metabolic alkalosis is called post-hypercapneic metabolic alkalosis

METABOLIC ALKALOSIS-POST HYPERCAPNEIA
• The kidney takes time to get rid of the excess HCO3 and if the patient is volume contracted the kidney may not be able to get rid of the HCO3 because it is avid for Na reabsorption.

RESPIRATORY ACIDOSIS
• Alveolar hypoventilation– Acute
• airway obstruction, drugs, CNS disease
• 1 mEq/l increase HCO3/10 mmHg pCO2
– Chronic (>72 hr.)• COPD, CNS disease
• 3-4 mEq/l increase HCO3/10 mmHg pCO2

ASSESSMENT OF ACID-BASE DISTURBANCES
Arterial pH
< 7.35 Acidemia > 7.45 Alkalemia
Hx & Px
Check pH
Check pCO2
and HCO3
ExpectedcompensationACUTECHRONIC
CheckAnion GapNa-(Cl+HCO3)
PossibleDiagnoses
Low HCO3Metabolic Acidosis
High pCO2
Respiratory Acidosis
High HCO3Metabolic Alkalosis
Low pCO2
Respiratory Alkalosis
1 HCO3: 1 pCO2
1 HCO3: 1 pCO2
10 Pco2 :1 HCO3 10 Pco2 :3 HCO3
1 HCO3: 0.5 pCO2
1 HCO3: 0.5 pCO2
10 Pco2 :2 HCO3 10 Pco2 :5 HCO3
=12-16 >16
HCO3 LossR.T.A.Diarrhea
KetoacidosisLactic AcidosisRenal FailureIntoxications
ASAMethanolEthylene Glycol
COPDDrugs-CNS/RespDepressants
May be increased dueto increased negative
charge of proteins
Normotensive Hypertensive
Urine Cl
< 10Vomiting
Post-hypercapneia
> 10Diuretics
Conn’sCushing’s
Renal Artery Stenosis
DrugsHigh Altitude
ASAPregnancy
Sepsis

RESPIRATORY ALKALOSIS
• Alveolar Hyperventilation– Acute
• drugs, sepsis, CNS disease
• 2 mEq/l decrease HCO3/10 mmHg pCO2
– Chronic• altitude, pregnancy, liver disease, CNS disease
• 5 mEq/l decrease HCO3/10 mmHg pCO2

ASSESSMENT OF ACID-BASE DISTURBANCES
Arterial pH
< 7.35 Acidemia > 7.45 Alkalemia
Hx & Px
Check pH
Check pCO2
and HCO3
ExpectedcompensationACUTECHRONIC
CheckAnion GapNa-(Cl+HCO3)
PossibleDiagnoses
Low HCO3Metabolic Acidosis
High pCO2
Respiratory Acidosis
High HCO3Metabolic Alkalosis
Low pCO2
Respiratory Alkalosis
1 HCO3: 1 pCO2
1 HCO3: 1 pCO2
10 Pco2 :1 HCO3 10 Pco2 :3 HCO3
1 HCO3: 0.5 pCO2
1 HCO3: 0.5 pCO2
10 Pco2 :2 HCO3 10 Pco2 :5 HCO3
=12-16 >16
HCO3 LossR.T.A.Diarrhea
KetoacidosisLactic AcidosisRenal FailureIntoxications
ASAMethanolEthylene Glycol
COPDDrugs-CNS/RespDepressants
May be increased dueto increased negative
charge of proteins
Normotensive Hypertensive
Urine Cl
< 10Vomiting
Post-hypercapneia
> 10Diuretics
Conn’sCushing’s
Renal Artery Stenosis
DrugsHigh Altitude
ASAPregnancy
Sepsis

ACID-BASE
Disorder Serum pH Serum pCO2 SerumHCO3
MetabolicAcidosis
MetabolicAlkalosis
RespiratoryAcidosis
RespiratoryAlkalosis