Embed Size (px)
Citation preview

~ .w ,. ~
~ ~ O~illloma ~tat~ Univ~r~icy Int~rli~rruy 1oill1 ~~~ ~: m.~~o J~ij :-= 0 Joumallit e: Joumal of !~e Ameri~an A~aaem~ of lota!io~: Mal~,~!r = _ Ort~o~aeai~ ~ur~eons.
~ol~m~: 1~ l~s~~: I Mo~t~N ~ar: L~~o
=-::!:= D~no~· ~oi ..- :i:;; r Q~v~. vo R
•
A~l~l M~~~ost:
: ~ Artitle iille: ~om~licatio~~ ~~er treatme~t or lie~ or te~~o~ i~jijrie~. ~~~~~eO 0~: -- 0 Article Au!~or: lill~ ~1,
~ ~orrower: ~A~I~:cor ~ ~atron: ~ .. z r Ill ~um~er: ·1~J1~1~ 00
~ 0
Ariel: 1L~~~L,Jti~~ rax:
~~~~~in~ MOre~s: ~tW: Mor~a~ li~ra~ li~ffi~

Soma I. Lilly, MD
Terry M. Messer, MD
Volume '14, Number 7, July 2006
Complications After Treatment of Flexor Tendon Injuries
Abstract The goals of flexor tendon repair are to promote intrinsic tendon healing and minimize extrinsic scarring in order to optimize tendon gliding and range of motion. Despite advances in the materials and methods used in surgical repair and postoperative rehabilitation, complications following flexor tendon injuries continue to occur, even in patients treated by experienced surgeons and therapists. The most common complication is adhesion formation, which limits active range of motion. Other complications include joint contracture, tendon rupture, triggering, and pulley failure with tendon bowstringing. Less common problems include quadriga, swan-neck deformity, and lumbrical plus deformity. Meticulous surgical technique and early postoperative tendon mobilization in a well-supervised therapy program can minimize the frequency and severity of these complications. Prompt recognition. of problems and treatment with hand therapy, splinting, and/or surgery may help minimize recove1y time and improve function. In the future, the use of novel biologic modulators of healing may nearly eliminate complications associated with flexor tendon injuries.
T endon lacerations within the digital sheath are difficult tore
pair. 1 As a result of poor outcomes following primary tendon repair within the digital sheath (zone II), the area within the sheath containing the flexor digitorum profundus (FOP) and flexor digitorum superficialis (FDS) tendons has been referred to as "no man's land."2 In the 1960s, the development of stronger suture materials and improved suture techniques led to a renewed interest in primary repair within the digital sheath.3 Primary repair is now the standard of care. Despite these advances, outcomes have been rated fair or poor in 7% to 20% of patients
after flexor tendon repair.4•5 A thorough knowledge of the basic science of flexor tendon healing is essential for improving outcomes and for understanding, recognizing, and managing the various complications.
Basic Science of Flexor Tendon Healing
Anatomy Tendons are made up of spiraling
bundles of mature tenocytes and predominantly type I collagen. In the distal palm and digits, the tendons are enclosed in a synovial sheath. The synovial sheath enhances gliding of the tendons and is thickened
387

Complications After Treatment of Flexor Tendon Injuries
----------------------------------
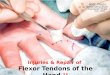
Lateral view of the flexor tendon synovial sheath, including the palmar aponeurosis (PA), five annular (A) pulleys, and three cruciform (C) pulleys. The critical pulleys are A2 and A4, located over the proximal and middle phalanges, respectively. (Reproduced with permission from Doyle JR: Anatomy of the finger flexor tendon sheath and pulley system. J Hand Surg {Am}1988;13:473·484.)
in specific areas between the joints; these thickened are<:1S are called pulleys. The pulleys enhance efficiency of motion within the digit by preventing tendon bowstringing and maximizing tendon excursion. Most critical to this system are the A2 and A4 pulleys, which are located over the proxi1T1~1l and middle phalanges, respectively6 (Figure 1). The FDP and FDS tendons are contained within the digital flexor sheath.
Flexor Tendon Healing Tendon healing consists of three
phases: inflammatory, proliferative, and remodeling. 7 The infLunmatory phase occurs during the first week after injury and involves migration of fibroblasts and macrophages to the injured area, with ensuing phagocytosis of the clot and necrotic tissue. In the proliferative phase, which lasts fron'l weeks 1 through 3, fibroblasts proliferate, and there is immature collagen deposition and neovascularization. Finally, the remodeling phase occurs in weeks 3 through 8. Collagen fibers become organized in a linear rn.anner parallel to the tendoi1. Adhesion formation between tendon and sheath is most clinically evident during this last phase.
Two n~echanisms for healing have been described in the literature: extrinsic and intrinsic. The extrinsic mechanisn'l is predominately medi-
ated by <111 influx of synovial fibroblasts and inflammatory cells from the tendon sheath. Healing also occurs via the intrinsic mechanism, in which fibroblasts <mel inflammatory cells from the tendon and epitenon invade the injured site. The extrinsic mechanism is thought to predominate early in tendon healing and in cases of digit immobilization; the intrinsic mechanism becomes increasingly active after 21 days.8 The greater proliferative and inflammatory response of the synovial sheath, along with the greater cytokine reactivity and capacity for matrix degradation of synovial fibroblasts, favor the extrinsic pathway.8 Extrinsic healing produces increased collagen content at the injury site, but in a disorganized fashion. Tendon healing is likely a combination of both mechanisms, but the predominance of extrinsic healing leads to scar formation and adhesions between the tendon and the surrounding sheath.
Requirements for Tendon Healing
Requirements for tendon healing include motion and tension at the repair site, adequate tendon nutrition and vascular perfusion, minimal gap formation at the repair site, and a strong repairY· 12 Early-motion protocols in <mimal flexor tendons resulted in a progressively greater ul-
timate tensile load over time than was the case in tendons managed with immobilization protocolsY Early-motion protocols also helped avoid the loss of strength that occurs in early phases of tendon healing. 10
Addition<llly, both motion and tension arc needed to stimulate tenocyte development and increase collagen amount and organization.''
Tendon nutrition is provided through vascular perfusion and synovial fluid diffusion. Flexor tendon vascular supply originates from vessels in the proximal synovial fold, segmental branches of digital arteries through the vincular system, and the osseous insertion of the FDS and FDP tendons. 13 Diffusion of nutrients through synovial fluid occurs via imbibition, in which fluid is forced through interstices on the surface of the tendon. 14 This process is facilitated by the pumping mechanism created by flexion and extension of the digit.
Gap formation as a result of cyclic loading before tendon failure is seen routinely after flexor tendon repair. 15 The average gap is 3.2 mm. 16
Gaps have previously been associated with adhesion formation and poor gliding. 17 Gelberman et al, 12 however, demonstrated that gap length has no relationship to adhesion formation, but it does have a negative ef. feet on the acquisition of tendon tensile properties during healing. In their canine study, repair gaps >3 mm did not gain stiffness or strength from 10 to 42 days, but gaps <3 nun had a 320% increase in stiffness and a 90% increase in strength over the same period. 12
Techniques for maximizing tendon repair strength comprise a large portion of flexor tendon research. A strong repair is one that can withstand early motion with minimal gap formation, thereby allowing successful tendon healing. Wellaccepted, established principles of tendon repair include using core sutures of 3-0 or 4-0 nonabsorbable polyfilament material, an increased
388 Journal of the American Academy of Orthopaedic Surgeons

nun1ber of sutures crossing the repair, and equal strength across all strands. In addition, certain locking suture techniques [ie, tr<msverse limb of repair passed superficial to the longitudinal component) have been shown to increase repair strength. 18·20 A peripheral locking epitendinous suture also should be added to enh<mce rep<tir strength. 21
Complications
Adhesion Formation Adhesion formation is the most
com.mon complication following flexor tendon repair. Prevention of adhesion formation is facilitated by optimizing intrinsic healing. Early research reflected the belief that tendon healing depended on extrinsic cellular ingrowth, which required immobilization. However, the ability of tendons to heal by intrinsic mechanisms alone has since been well documented. 22 Methods of adhesion prevention can be divided into mechanical and biologic factors designed to promote intrinsic healing.
Mechanical Factors
Mechanical factors for preventing adhesions include early postoperative motion protocols, preservation of sheath and pulley components, partial FDS resection, and a traumatic handling of the tendon and sheath. Motion, which leads to a predominance of intrinsic over extrinsic healing, is critical to preventing adhesions. Three primary motion protocols are described in the literature: passive, active, and synergistic. In 1977, Lister et al'--3 published the first results of tendon repair using a controlled passive motion protocol. The Kleinert splint was used to allow active digital extension coupled with passive digital flexion. Good to excellent results were reported in 80% of tendon lacerations in zone 11. 23
The splint has since been modified by adding a mid palmar bar or pulley, resulting in improved distal tendon gliding and differential tendon ex-
Volume 14, Number 7, July 2006
cursion.:'A The <lcldition of synergistic wrist motion (wrist flexion-finger extension combined with wrist extension-finger flexion) also has been shown to improve overall tendon gliding and excursion. 25
Early active motion protocols subsequently have been developed to address concerns about variability in tendon gliding with passive protocols. Bainbridge et aF" reported on a consecutive series comp~tring controlled active motion with active extension-passive flexion protocols. Patients treated with controlled active motion acquired greater final motion. 26 Other series using early active motion have reported good to excellent results ranging from 57% to 92%, with rupture rates from 5% to 46% _27·2" These findings are comparable to rates reported with passive motion regimens. Improved suture matexials and techniques see1n capable of withstanding the higher forces associated with active motion protocols.30-32 However, recent research in repaired canine tendon by Boyer et aP3 demonstrated no advantage with high-force rehabilitation in the accrual of eithex stiffness or stxength compared with low-fmce rehabilitation.
The synergistic motion regimen allows high tendon excursion with low force on the repair site.34 This protocol consists of passive digit flexion combined with active wrist extension, followed by active wrist flexion com.bined with passive digit extension. Zhao et aP5 compared synergistic motion with passive motion regimens in the management of canine flexor tendon repairs. They noted fewer adhesions with the synergistic motion group but reported elevated gap fonnation in the motion group (30%) versus the passive group (6%).35 Currently, agreement is universal that repaired flexor tendons should be subjected to early mobilization; however, no single rehabilitation protocol is accepted by all.
Preservation of sheath components is controversial. When the vas-
Soma I. Lilly, MD, and Terry M. Messer, MD
cular source of nutrition is compromised because of trauma, the tendon sheath can maintain nutrition through imbibition until the vascular system is reestablished.30 Preservation of flexor tendon sheath integrity may reduce adhesions through its positive effect on intrinsic healing_37 However, sheath repair also may lead to impaired tendon gliding and increased rcsistance. 17 Another study compared sheath repair with excision and found no difference in final motion when early mobilization was done.38
Recently, resection of all or part of the FDS tendon has been suggested as a method of decreasing gliding resistance of the FDP within the sheath.39 Loss of the FDS tendon is not associated with significant functional compromise. However, this technique was initially dismissed because a considerable portion of the FDP blood supply is provided by capillaries emanating from the FDS tendon. In a cadaveric study, FDS resection was found to be a viable option for improving the gliding of a bulky · FDP repair. The authors did not demonstrate any advantage of complete resection versus partial resection.39
The use of meticulous surgical technique as a method for decreasing adhesion formation is well documented. Adhesion formation is known to be proportional to the amount of tissue crushing and to the number of surface injuries incurred by the tendon and sheath during repair.~ Accordingly, stiffness is more common in digits after crush injuries as well as in those with concomitant neurovascular and bone injuries. 40
Biologic Factors
Development of novel biologic factors to provide so-called scarless healing is an active area of research.22·41 Advances in this arena could lead to less reliance on postoperative motion for adhesion prevention. Methods currently under investigation include mechanical barriers to adhesion formation, as well as
389

Complications After Treatment of Flexor Tendon Injuries
chemical and molecular modulation of scar fmmation. Many mechanical barrier methods have been studied, including silicone, alumina sheaths, polyethylene/ and polytetrafluoroethylene, but none is in widespread clinical use. 22 ADCON-T/N (Gliatech, Cleveland, OH), a gelatin and carbohydrate polymer, has shown some potential.41 In a recent doubleblind randomized study in which ADCON-T/N was applied to the tendon after repair, the authors found no significant effect on final motion; however, time to achieve final n1.otion was shorter with the use of ADCON-T/N:n
Ibuprofen and corticosteroids have been investigated as possible modulatms of adhesion formation. 42•43 Ibupwfen has been shown to im.prove tendon excursion in animal n10dels.-12
Ketchum43 demonstrated that although corticosteroids decrease the strength and density of adhesions, they are associated with smaller, weaker tendons, diminished wound healing/ and decreased resistance to infection. These problems have limited their use in flexor tendon repair.
Nevv Research
Modulation of scar formation on a molecular level is a new area of research in tendon healing. This research has been directed toward understanding the role of cytokines in tendon metabolism and repair.22·4-I,-IS Two cytokines, transforming growth factor-~ (TGF-~) <1nd basic fibroblast growth factor (bFGF), have shown the most potential in adhesion prevention. 44
•45 TGF-~ has
been implicated in numerous biologic activities related to wound healing, such as fibroblast and macrophage recruitment, angiogenesis, stimulation of collagen production, downregulation of proteinase activity, and increased metalloproteinase inhibitor activity:14
Chang et al'l5 demonstrated that flexor tendons exposed to transection and repair exhibit increased TGF-~ in both tenocytes and inflam-
390
matory cells from the tendon sheath. These findings are significant because TGF-~ is thought to be involved in the pathogenesis of excessive scar formation. Therefore, perioperative modulation of this cytokine may lead to decreased adhesion formation. Three isoforms have been identified; the TGF-01 isoform is thought to be primarily responsible for the proinflammatory and scarring activities.22 The TGF-03 isoform demonstrates anti-scarring properties and acts as an inhibitor of scarring in injury models. 22
Similar to TGF-~, bFGF has been implicated in early tendon healing.4s Basic FGF is a potent stimulator of angiogenesis and is able to induce rnigration and proliferation of endothelial cells in tissue culture. In 1998, Chang et al45 found that bFGF was upregulated in tenocytes, tendon sheath fibroblasts, and inflammatory cells from flexor tendons exposed to a tendon wound environment. With further research, modification of bFGF expression may also be useful in postoperative adhesion reduction.
Research into chen1ical modulation of cytokines has yielded 5-fluoromacil (5-FU) as a possible candidate:16·47 5-FU is an antimetabolite that decreases scarring by an unknown n1echanisrn. Khan et al46
tested this drug in a rabbit model by treating the injured synovial sheath of partially lacerated tendons with a 5-min application of 5-FU before closure. A significant (P < 0.001) decrease in the proliferative and inflammatory response of synovial fibroblasts was demonstrated. There was also a significant (P < 0.001) decrease in the expression of TGF-~ in the treated tissue. Others have reported the ability of 5-FU to reduce postoperative adhesions in a chicken model.47 These findings are still experimental, however, and have not yet been implemented in clinical practice.
When adhesion prevention is unsuccessful, early recognition is critical to ensure a good clinical outcome and prevent further progression
of stiffness. Adhesion and tendon rupture present clinically with simihlr physical findings. Both conditions may demonstrate loss of active flexion, but patients with adhesions have preservation of some residual active motion. Imaging studies, such as magnetic resonance imaging or ultrasound, may be indicated to determine the source of motion loss. Magnetic resonance imaging has been shown to be 100% accurate in distinguishing adhesions from rupture. 48
When adhesions are identified, therapy should be directed toward programs that maximize differential motion between the FDS and FDP tendons.25•26 Splinting also may be a useful adjunct. When therapy and splinting fail to produce effective results, tenolysis may be indicated.
Tenolysis
Flexor tenolysis is indicated when active range of motion (ROM) measurements do not improve within several weeks to months, despite strict patient compliance with splinting and ROM exercises. 49 Tenolysis should not be considered until the soft tissues have reached a state of equilibrium, with supple skin and subcutaneous tissues. To achieve a good result, the digit must have minimal joint contractures and nearnormal passive ROMP Most surgeons recommend waiting for 3 to 6 months after tendon repair or grafting before performing tenolysis. 49•50
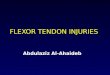
When performing flexor tenolysis, a local anesthetic combined with intravenous sedation is recommended to allow the patient to perform active flexion in the operating room. 5° This intraoperative testing is critical to achieve a successful outcome. A midlateral or Bruner zigzag incision is used to expose the length of the tendon. The neurovascular bundles are encountered at the ends of the digital creases, and the surgeon must take care to prevent iatrogenic injury to these structures. The scarred tendon and its sheath are visualized (Figure 2, A),51 the aclhe-
Journal of the American Academy of Orthopaedic Surgeons

SomaL Lilly, MD, and Terry M, Messer, MD
------~------~·--------"·'· ___ ' __ _ Eigure 2 , , , , " , , , , ,, , , , " , " , , , " , , ,
' ' ' ' ' ' ' ' ,, ,, ' ,, ,, ' "' ' ' ' ' " "' " "" " 'p ' ' ' 'iii ~ v '" ' v v' ' ' '
A
c
sions released, and the tendon borders identified. A useful technique is to pass a small eleva tor through windows made in less critical parts of the sheath (Figure 2., C). As rnuch of the pulley system as possible must be preserved (Figure '2, Bh when this is not feasible, pulley reconstruction or a staged tendon implant should be considered. If pulley reconstruction requires protected mobilization, however, the end result may be compromised. Additionally, any concomitant procedure, such as tendon lengthening or shortenil'lg, skin grafting, osteotomy, or capslllotomy, may have an adverse effeq on the outcome of flexor tenolysis. I? At the end of the procedure, the patient should be placed in a splint that permits immediate active R<JM. Patients for whom active RQM improves in the first few wet::ks after --~
Volume 14, Number 7, July 2006
B
Flexor tenolysis is performed by identifying the scarred tendon and sheath (A), followed by release of adhesions and careful preservation of the pulley system (B). C, Release may be facilitated by passing a small elevator or dental probe through windows in less critical portions of the sheath (eg, proximal to A2, or between A2 and A4 pulleys). (Reprinted from Strickland JW: Flexor tenolysis, in Strickland JW [ed]: Master Techniques in Orthopaedic Surgery: The Hand. Philadelphia, PA: Lippincott-Raven, 1998, pp 525-538. Illustrations copyright © Gary Schnitz and the Indiana Hand Center.)
surgery tend to maintain these gains. Significant pain and little early improvement in motion may be an indication for inserting an indwelling polyethylene catheter containing local anesthetic. so
One complication of flexor tenolysis is tendon or pulley rupture, which should be managed with a staged tendon reconstruction. Other complications include postoperative edema and pain as well as inadvertent neurovascular injury that may lead to loss of viability in a digit with marginal preoperative circulation. Flexor tenolysis is a technically demanding procedure, and the postoperative rehabilitation is equally arduous. Not all patients are candidates for tenolysis. The surgeon must evaluate how the loss of active motion will affect the patient's needs and desires as well as the abil-
ity to perform activities of daily living and to return to his or her occupation. The surgeon also must consider the sensory and circulatory status of the finger, the condition of the other digits, and the age and general health of the patient. Patients who are noncompliant with therapy after their initial repair typically are poor candidates for tenolysis.
Joint Contracture Even with adherence to early
motion regimens, the reported rate of proximal interphalangeal (PIP) and distalinterphalangeal (DIP) joint contracture is 17%.36 Contractures may be caused by unrecognized disruption or scarring of the volar plate, tendon bowstringing secondary to pulley incompetence, concomitant fracture or neurovascular injUty, prolonged healing in a flexed position, collaterallig-
391

Complications After Treatment of Flexor Tendon Injuries
A 8 c
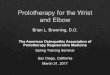
Splints used to manage proximal interphalangeal (PIP) flexion contractures. A, Dorsal forearm-based thermoplast splint with a felt block placed dorsally at the level of the PIP joint. B, Joint Jack Finger Splint (Sammons Preston Rolyan, Bolingbrook, IL). C, Safety Pin Splint (Sammons Preston Rolyan).
ament contracture, skin contracture, or flexor tendon atll1esions. They also may be secondaty to inadequate postoperative motion regimens and dynamic flexion splinting. The latter may be prevented through correct positioning of the wrist, hand, and digits in the postoperative splint and early motion.lVlost postoperative protocols involve splinting the m.etacarpophalangcal (MCP) joint in flexion (approximately 60°) with the interphalangeal (IP) joints fully extended.
Nonsurgical management o£ joint contractures consists of early identification and modification of splinting to allow greater PIP and DIP joint extension. A felt or foam block placed inside a dorsal splint at the level of the proximal phalanx, in addition to increasing MCP joint flexion to relax the intrinsic mechanism, will help resolve PIP joint contracture (Figure :3, A). This method can be used \Vith buddy taping and active-assisted extension exercises. Static nighttime extension splinting and passive extension exercises with Velcro bands applied to the splint to impart an extension force on the digit also may be useful. As the tendon continues to heal and strengthen, finger splints (eg, Joint Jack, Safety Pin) can be used (Figure ,i, Band C).
Vilhen nonsurgical management of contractures is unsuccessful, surgery should be considered. No absolute guidelines exist regarding the
392
degree of contracture that requires surgical release; rather, the decision for surgery is based on the patient's functional limitations and goals. Preoperatively, the surgeon should attempt to determine whether the contracture is caused by extrinsic factors (eg, skin contracture, proximal flexor tendon adhesions) or an intrinsic joint contracture. When extrinsic factors are responsible, PIP joint extension will improve with MCP joint flexion. PIP joint release should be performed only after all flexor tendon adhesions and skin contmctures have been .addressed.
For PIP joint release, exposure is performed through a Bruner or midlateral incision. The radial and ulnm neurovascular bundles are identified and protected. The Cl portion of the flexor sheath is excised between the A'2 and AB pulleys, and the FDP and FDS tendons are exposed"2 (Figure 4, A). Flexor tenolysis is performed initially; the checkrein ligaments are identified by passing a small hemostat or elevator volar to the transverse retinacular vessels as they enter the flexor sheath just proximal to the collateral ligament origin. The checkrein ligaments are volar to the transverse rctinacular vessels and can be divided sharply at this level. The transverse retinacular vessels should be preserved whenever possible because they supply the tendon vincular system.
When full passive PIP joint extension cannot be obtained, release of the collateral ligaments is performed at their insertion on the head of the proximal phalanx, beginning with the accessory collateral ligaments (Figure 4, B). Release of the collateral ligaments should be performed sequentially, progressing from palmar to dorsal, until full extension is achieved. When full extension cannot be achieved, release of the volar plate may be necessary.
Tendon Rupture Rupture of a tendon repair is not
an uncomn1on problem. In one study, a rupture rate of 4% was reported in 7'28 digital flexor tendon repairs 1440 paticnts).5•1 The authors were unable to identify the inciting factor in these failures. Another series reported a 5. 7% rate of rupture in digital flexor tendon repairs. 19
Factors that predispose tendon repairs to rupture include inadequate suture material, poor surgical technique, overly aggressive therapy, or early termination of postoperative splinting. Patient noncompliance, such as removing the splint, lifting heavy objects, or attempting strong grasp, is a frequent cause of rnpture.53
Tendon repairs are weakest between postoperative days 6 and 18.35 Although rupture is most common during this period, it may be
Journal of the American Academy of Orthopaedic Surgeons

seen as late as 6 to 7 weeks after surgery.·16 Timely surgical exploration is indicated once tendon rupture is identified. When repair attenuation is seen without obvious rupture and < 1 em of scar is present, the scar can be resected and the primary repair revised. When the scar is > 1 em, a tendon grafting procedure should be considered because excessive distal advancement of the tendon can lead to contractures and quadriga.36 With complete tendon rupture, the time from the original repair influences the course of action. If the rupture occurs in the early postoperative period, the tendon may be primarily repaired. When the rupture occurs 4 to 6 weeks after the original repair, tendon grafting or a staged reconstruction is recommended. Staged grafting is preferred when there is significant scarring within the sheath. Pediatric urethral or vascular dilators can be used to expand a constricted but otherwise intact sheath, thereby eliminating the need for a two-stage reconstruction.
Triggering Triggering can occur after tendon
repair and is usually the result of the repair site's catching on a pulley or sheath. Causes of triggering include a bulbous tendon repair or a tightly repaired area of the tendon sheath. The surgeon should intraoperatively assess tendon gliding to identify areas that may cause triggering or restrict gliding. In the acute setting, a partial tendon sheath excision or release may be used. In contrast, sheath repair may reduce triggering of a bulky repair by acting as a funnel. Postoperatively, ultrasound or massage may be helpful. Once the tendon is healed, a corticosteroid injection may be indicated. Reduction tenoplasty may be considered when nonsurgical measures fail; however, this technique carries a risk of tendon rupture.54
Recent studies have addressed the feasibility of partial sheath resection to decrease triggering and gliding 1·e-
Volume 14, Number 7, July 2006
Soma I. Lilly, MD, and Terry M. Messer, MD
EigureiJ. .
Checkrein ligament of the palmar plate
Sheath excised
A
8
DIP joint
Accessory collateral ligament released
PIP joint
A, Joint contracture release via excision of the C1 portion of the flexor tendon sheath between the A2 and A3 pulleys exposes the flexor digitorum superficia!is (FDS) and flexor digitorum profundus (FOP) tendons. B, The checkrein ligaments are released with subsequent release of the collateral ligaments from palmar to dorsaL*= transverse retinacular vessels, DIP= distal interphalangeal, PIP= proximal interphalangeal (Reproduced from Idler RS: Capsulectomies of the metacarpophalangeal and proximal interphalangeal joints, in Strickland JW [ed]: Master Techniques in Orthopaedic Surgery: The Hand. Philadelphia, PA: LippincottRaven, 1998, pp 361-379. Illustrations copyright © Gary Schnitz and the Indiana Hand Center.)
sistance. This problem is of particular concern when it involves the A'l or A4 pulleys. Tang et al5s found a decrease in gliding resistance with partial pulley release. However, a cadaveric study by Mitsionis et a156
dem.onstrated that, although excision of up to '25% of both the A'l and A4 pulleys had no significant effect on the efficiency of motion, it did not achieve the goal of decreasing sheath resistance.
Partial Tendon Injury Partial tendon lacerations can be
challenging; if not managed properly, they carry the risk of triggering, entrapment, or secondary ruptureY Repair has been recommended for lacerations involving >60% of the tendon substance. 58 In other studies, the authors reported that trimming digital flexor tendon lacerations involving >50% of the tendon substance was not associated with trig-
393

Complicalions After Treatment of Flexor Tendon Injuries
A digit in which pulley reconstruction necessitated a two-stage revision. The A2 and A4 pulleys were repaired using excised flexor tendons sutured to the retained tendon sheath edge combined with a silicone rod tendon. (Courtesy of GeorgeS. Edwards, Jr, MD, Raleigh, NC.)
gering or rupture.59 In a study by Erhard et al60 that compared trimming with repair of partial lacerations, the lowest gliding resistance was produced with trimming, without a concomitant decrease in tendon strength.
Pulley Failure and Bowstringing
The A2 and A4 pulleys are responsible for preserving digital motion and finger strength {grip and pinch power). Loss of the integrity of these pulleys results in howstringing, with loss of the A4 pulley causing the greatest change in the efficiency of tendon excursion, work, and force. 01 Avoidance of bowstringing is the best management strategy and may be facilitated by performing tendon repair through cruciate pulley windows, using external pulley rings for compromised pulleys, and reconstructing pulleys in a one- or two-stage procedure when native tissue is unsalvagcable36 (Figure 5).
Many techniques for pulley reconstruction have been described, such as·Bunnell, Kleinert, Lister, and Karev. Nishida et al62 found that Lister's technique of using the exten-
394
-
....... ~--------
B ¥
A, In normal finger mechanics, interphalangeal (IP) flexion occurs with concomitant lumbrical relaxation. B, In lumbrical plus deformity, extension of the IP joints paradoxically is through the lateral bands once the limit of lumbrical relaxation is reached. (Reproduced with permission from Parkes A: The "lumbrical plus" finger. J Bone Joint Surg Br 1971 ;53:236-239.)
sor retinaculum for pulley reconstruction had the least resistance to tendon gliding.
Quad riga Quadriga is the inability of unin
jured fingers of the same hand to obtain full flexion. It manifests as a weak grasp on physical examination. This complication is caused by functional shortening of the FDP tendon. Shortening of one FDP tendon affects the function of the FDP tendons of adjacent fingers, causing overadvancement of the PDP tendon, proximal tendon tethering or adhesions, and insertion of a short tendon graft. Anatomically, quadriga occurs because the common FDP muscle belly to the midclle, ring, and small fingers permits only as much proximal excursion in each digit as that of the shortest tendon. Proper tendon tensioning during repair prevents this problem. When quadriga occurs, tenolysis of the proximal adhesions or transection of the shortened tendon will release the uninjured profundi.7
Swan-neck Deformity Swan-neck deformity consists of
hyperextension at the PIP joint with
flexion at the DIP joint. In flexor tendon repair, common causes include isolated FDS rupture and volar plate injury. This complication is infrequent, howeveri loss of the FDS is usually associated with minimal functional deficit. Careful attention to and correction of volar plate injuries at the time of tendon repair prevents this problem. Surgical management of the hyperextension deformity may be facilitated through tenodesis with one slip of the FDS tendon.
Lumbrical Plus Deformity Lumbrical plus deformity is the
paradoxical extension at the IP joints of the injured digit with attempted forceful flexion. Normally, PIP and DIP joint flexion occurs in conjunction with simultaneous relaxation of the lumbrical muscle (Figure 6, A). Paradoxical extension arises when the PDP distal to the lumbrical muscle is functionally too long or is not present. Flexor tendon force is thereby transmitted to the lumbrical and subsequently to the extensor mechanism via the lateral bands before full digital flexion is reached (Figure 6, B). Other causes of lumbrical plus deformity include <1Vulsion of the
Journal of the American Academy of Orthopaedic Surgeons

Soma I. Lilly, MD, and Terry M. Messer, MD
--------------------------------------------------------------------------------------------FDP tendon or amputation through the proximal phalanx.03 Management involves lumbrical muscle release or placement of a tendon graft of appropriate length.
Summary
Despite advances in flexor tendon surgery over the past 50 years, complications continue to occur. The most common are adhesion formation and joint contracture. Achieving optimal outcomes occurs through meticulous surgical repair using 3-0 or 4-0 polyfilament core suture with a minimum of four strands reinforced with an epitendinous suture, a well-fitting splint, early controlled mobilization, and vigilant patient monitoring for compliance with the rehabilitation program. Biochemical and molecular advances in the research into scarless healing likely will lead to future advances.
References
Evidence-based Medicine: Level I/II prospective studies include references 16, 26, 27, 29, 30, 40, and 41. The rernarnrng references are casecontrolled reports or experimental observations.
Citation numbers printed m bold type indicate references published within the past 5 years.
l. Verdan CE: Half a century of flexortendon surgery: Current status and changing philosophies. 1 Bone Joint Surg Am 1972;54:472-491.
2. Bunnell S: Repair of tendons in the fingers and description of two new instruments. Surg Gynecol Obstet 1918;26:103-110.
3. Kleinert HE, Kutz JE, Ashbell TS, Martinez E: Primary repair of lacerated flexor tendons in "no man's land." 1 Bone Joint Surg Am 1967;49:577.
4. Strickland JW: Development of flexor tendon surgery: Twenty-five years of progress. J Hand Surg [Am] 2000;25: 214-235.
5. Saldana MJ, Chow JA, Gerbino P, Westerbeck P, Schacherer TG: Further experience in rehabilitation of
Volume 14, Number 7, July 2006
zone II flexor tendon repair with dynamic traction splinting. Plast Reconstr Surg 1991;87:543-546.
6. Doyle JR: Anatomy of the finger flexor tendon sheath <mel pulley system. I Hand Surg (Am/ 1988; 13:473-484.
7. Strickland JW: Flexor tendons-;Jcute injuries, in Green DP, Hotchkiss RN, Pederson VvC (eels): Green's Operative Hand Surgery, eel 4. New York, NY: Churchill Livingstone, 1999, vol 2, pp 1851-1897.
8. Kakar S, Khan U, McGrouther DA: Differential cellular response within the rabbit tendon unit following tendon injury. 1 Hond Surg [Bz}1998;23: 627-632.
9. Gelberman RH, Woo SL, Lothringer K, Akeson WI-I, Amici D: Effects of early intermittent passive mobilization on healing canine flexor tendons. /Hond Surg {Am} 1982;7:170-175.
10. Aoki M, Kubota I-I, Pruitt DL, Manske PR: Biomechanical and histologic characteristics of canine flexor tendon repair using early postoperative mobilization. f Hanel Surg [Am] 1997;22:107-114.
11. Kubota I-I, Manske PR, Aoki M, Pruitt DL, Larson BL: Effect of motion and tension on injured flexor tendons in chickens.[Hand Smg {Am] 1996;21: 456-463.
12. Gel berman RH, Boyer MI, Brodt MD, Winters SC, Silva MJ: The effect of gap formation at the repair site on the strength and excursion of intrasynovial flexor tendons: An experimental study on the early stages of tendonhealing in dogs. J Bone faint Surg Am 1999;81:975-982.
13. Ochiai N, Matsui T, Miyaji N, Merklin RJ, Hunter JM: Vascular anatomy of flexor tendons: I. Vincular system and blood supply of the profundus tendon in the digital sheath. 1 1-I and Su rg [Am/ 1979;4:321-330.
14. Weber ER, Hardin G, Haynes DW: Synovial fluid nutrition of flexor tendons. Presented at the 25th Annual Meeting of the Orthopaedic Research Society, San Francisco, CA, February 20-22, 1979.
15. Pruitt DL, Manske PR, Fink B: Cyclic stress analysis of flexor tendon repair. J Hanel Surg [Amj 1991;16:701-707.
16. Silfverskii:ilcl KL, May EJ, Ti:irnvall AH: Gap formation during controlled motion after flexor tendon repair in zone II: A prospective clinical study. J Hanel Surg [Am} 1992; 17:539-546.
17. Boyer MI, Strickland JW, Engles D, Sachar K, Leversec!ge FJ: Flexor tendon repair and rehabilitation: State of the art in 2002. Instr Course Lect
2003;52:137-161. 18. Hatanaka H, Zhang], Maske PR: An
in vivo study of locking and grasping techniques using a passive mobilization protocol in experimental animals./ Hanel Surg [Am/ 2000;25:260-269.
19. Tanaka T, Amadio PC, Zhao C, Zobitz ME, Yang C, An KN: Gliding characteristics and gap formation for locking <ll1d grasping tendon repairs: A biomechanical study in a hum~m cadaver model. f Hanel Surg [Am/ 2004;29: 6-15.
20. Barrie KA, Tomak SL, Cholewicki J, Merrell GA, Wolfe SW: Effect of suture locking and suture caliber on fatigue strength of flexor tendon repairs. /Hand Surg [Am/ 2001;26:340-346.
21. Lin GT, An KN, Amadio PC, Cooney WP III: Biomechanical studies of running suture for flexor tendon repair in clogs. J l-Ionel Surg [Amj1988;13:553-558.
22. Beredjiklian PI<: Biologic aspects of flexor tendon laceration and repair. J Bone Joint Surg Am 2003;85:539-550.
23. Lister GD, Kleinert HE, Kutz JE, Atasoy E: Primary flexor tendon repair followed by immediate controlled mobilization. f Hand Surg [Amj 1977;2:441-451.
24. Chow JA, Thomes LJ, Dovelle S, Milnor WH, Seyfer AE, Smith AC: A combined regimen of controlled motion following flexor tendon repair in "no man's land." Plast Reconstr Surg 1987;79:447-453.
25. Horii E, Lin GT, Cooney WP, Linscheicl RL, An KN: Comparative flexor tendon excursion after passive mobilization: An in vitro study. 1 Hanel Smg [Am/1992; 17:559-566.
26. Bainbridge LC, Robertson C, Gillies D, Elliot D: A comparison of postoperative mobilization of flexor tendon repairs with "passive flexionactive extension" and "controlled active motion" techniques. 1 Hand Surg [Br] 1994;19:517-521.
27. Peck FH, Biicher CA, Watson JS, Roe A: A comparative study of two methods of controlled mobilization of flexor tendon repairs in zone 2. J Hand Smg [Brj 1998;23:41-45.
28. Riaz M, Hill C, Khan K, Small JO: Long term outcome of early active mobilization following flexor tendon repair in zone 2. 1 Hand Surg {Br] 1999;24:157-160.
29. Kitsis CK, Wade PJ, Krikler SJ, Parsons NK, Nicholls LK: Controlled active motion following primary flexor tendon repair: A prospective study over
395

Complications After Treatment of Flexor Tendon Injuries
9 years. 1 Hond Surg [Br/ !998;13: 344-349.
30. Wada A, Kubota H, Miyanishi K, Hatanaka H, Miura H, lw<lmoto Y: Comparison of postoperative early active mobilization and immobilization in vivo utilising a four-strand flexor tendon repair. J Hond Surg [Brj 1001; 16:30 l-306.
31. Tang JB, Wang B, Chen F, Pan CZ, Xic RG: Biomechanical evaluation of flexor tendon repair techniques. Clin Orthop Relot Res 1001;386:151-159.
32. Labana N, Messer T, Lautenschlager E, Nagda S, Nagle D: A biomcchanic<Jl analysis of the modified Tsugc suture technique for repair of flexor tendon lacerations. I 1-land Surg /Brj 1001; 26:297-300.
33. Boyer Ml, Gelbcrman RH, Burns ME, Dinopoulos 1-l, Hofem R, Silva MJ: Intrasynovial flexor tendon rep<lir: An experimental study comparing low and high levels of in vivo force during rehabilit;1tion in canines. I Bone Joint Surg Am 2001;83:891-899.
34. Lieber RL, Silva MJ, Amici D, Gel herman RH: Wrist and digital joint motion produce unique flexor tendon force and excursion in the canine forelimb. 1 Biomech 1999;32: 175-181.
35. Zhao C, Amadio PC, Momose T, Couvreur P, Zobitz ME, An KN: Effect of synergistic wrist motion on adhesion formntion after repair of partial flexor digitorum profundus tendon lacerations in <1 canine model in vivo. I Bone Joint SliTg Am 2002;84:78-84.
36. Taras }S, Gray RM, Culp RW: Complications of flexor tendon injuries. Hand Clin !994;10:93-109.
37. Peterson W\V, Manske PR, Dunlap J, Horwitz DS, Kahn B: Effect of various methods of restoring flexor sheath integrity on the formation of adhesions after tendon injury. I Hand Smg [Am/ 1990;15:48-56.
38. Gelberman RH, Woo SL, Amici D, Horibe S, Lee D: Influences of flexor sheath continuity and early motion on tendon healing in dogs. I Hand Smg /Am/ 1990;15:69-77.
39. Zhao C, Amadio PC, Zobitz ME, An KN: Resection of the flexor digitorum superficialis reduces gliding resistance after zone II flexor digitorum
.profundus repair m vitro. J Hund Surg /Am/ 2002;2 7:316-32!.
40. Chow SP, Pun WK, So YC, et al: A prospective study of 245 open digital frac-
396
tuiTS of the hand. I l-Ionel Surg [Hrj I 991; 16:137-140.
41. Golash A, Kay A, \1./;Jrner JG, Peck F, W;Hson JS, Lees VC: Efficacy of ADCON-T /N after primary flexor tendon repair in zone Il: A controlled clinical trial. 1 Hu]J(/ Surg [Brj 1003; 28:113-115.
42. Kulick MI, Smith S, Hacllcr K: Oral ibuprofen: Evaluation of its dfect on pcritendinous adhesions and the breaking strength of a tenorrh<lphy. I Hunt! Surg /Am/ 1986;11:110-120.
43. Ketchum LD: Effects of triamcinolone on tendon he<lling and function: A laboratory study. Plast l~econst r Surg 1971;47:471-482.
44. Chang J, Most D, Stclnicki E, et al: Gene expression of transforming growth factor beta-! in rabbit zone II flexor tendon wound healing: Evidence for dual mechanisms of repair. !'last Reconslr Stng 1997; 100:937-944.
45. Chang J, Most 0, Thunder R, Mehrara B, Longaker JVlT, Lineawe<JVer WC: Molecular studies in flexor tendon wound healing: The role of basic fibroblast growth factor gene expression. J Hand Smg [rlmj 1998;23:1052-1058.
46. Khan U, Kakar S, Akali A, Bentley G, McGrouther DA: Modulation of the formation of adhesions during the healing of injured tendons. J Bone Joint Surg Br 2000;82:1054-1058.
47. Moran SL, Ryan CK, Orl.mdo GS, Pratt CE, Miehalko KB: Effects of 5-iluorouracil on flexor tendon repair. I /-land Surg /Am} 2000;25:242-25 !.
48. Matloub HS, Dzwierzynski WW, Erickson S, Sanger jR, Yousif N), Muoncke V: Magnetic resonance im<1ging scanning in the di:1gnosis of zone II flexor tendon rupture. 1 Hand Surg [Am] 1996;21:451-455.
49. Strickland JvV: Flexor tenolysis. !-land Clin 1985;1:121-132.
50. Feldscher SB, Schneider LH: Flexor tenolysis. Hand Surg 2002;7:61-74.
51. Strickland JW: Flexor tenolysis, in Strickland JW (ed): Master Techniques in Orthopaedic Surgery: The !-land. Philadelphia, PA: LippincottRaven, 1998, pp 525-538.
52. Idler RS: Capsulectomies of the metacarpophalange<ll and proximal interphaLmgeal joints, in Strickland JW (ed): Master Techniques in Orthopaedic Surgery: The Hand. Philadel-
phia, PA: Lippincott-Raven, 1998, pp 361-379.
S3. Harris SB, Harris D, Foster AL Elliot D: The aetiology of acute rupture of flexor tendon repairs in zones I and 2 of the fingers during early mobilization. f Hand Surg /Brj 1999;24:275-280.
54. Seraclge H, Kleinert HE: Reduction ilexor tenoplasty: Treatment of stenosing flexor tenosynovitis distal to the first pulley. 1 /-!and Smg [Am} 1981 ;6:543-544.
55. Tang JB, Wang YI-l, Gu YT, Chen F: Effect of pulley integrity on excursions and work of flexion in healing flexor tendons. 1 Hand Svrg [Am] 2001;26: 347-353.
56. Mitsionis G, Bastidas JA, Grewal R, Pfaefflc HJ, Fischer K), Tomaino MM: Feasibility of partial A2 and A4 pulley excision: Effect on finger flexor tendon biomechanics. I Hand Surg /Am/ 1999;24:310-314.
57. Schlenker )D, Lister GD, Kleinert HE: Three complications of untreated partial laceration of the flexor tendonentmpnlent, rupture, and triggering. J Hand Surg /Am/ 1981;6:392-398.
58. Bishop AT, Cooney WP Ill, Woocl MB: Treatment of partial flexor tendon lacerations: The effect of tenorrhaphy and early protected mobilization. T Trauma 1986;26:301-312.
59. al-Qatt<ll1 MM: Conservative management of zone II partial flexor tendon lacerations greater than half the width of the tendon. f Hand Surg jAm/ 2000;25:1118-1121.
60. Erhard L, Zobitz ME, Zhao C, Amadio PC, An KN: Treatment of partial lacerations in flexor tendons by trimming: A biomechanical in vitro study. J Bone 1oinL Surg Am 2002;84: 1006-1012.
61. Rispler D, Greenwald D, Shumway S, Allan C, Mass D: Efficiency of the flexor tendon pulley system in human cadaver hands. I Hand Surg [Am] 1996;21 :444-450.
62. Nishida J, Amadio PC, Bettinger PC, An KN: Flexor tendon-pulley interaction after pc1lley reconstruction: A biomechanical study in a human model in vitro. f I-fond Surg /Am] 1998;23:665-672.
63. Parkes A: The "lumbrical plus" finger. T Bone Joint Surg Br 1971;53:236-239.
Journal of the American Academy of Orthopaedic Surgeons















![Flexor Tendon Injuries[1]](https://img.pdfslide.us/doc/110x75/546eeaf2b4af9f8c068b465a/flexor-tendon-injuries1-558457890f347.jpg)