Anatomy
FLEXOR TENDON INJURYPRESENTER: DR. SOUVIK /DR.NAVEENMODERATOR:DR
VIVEK SINGH
ANATOMYExtrinsic flexorsSuperficial groupPT, FCR, FCU,
PLIntermediate groupFDS Deep groupFPL FDP
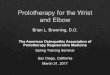
AnatomyCondensations of the fibrous retinacular sheath form the
flexor pulleys
Cruciform pully:allow digital flexion to occur without
significant deformation of annular pulley system
Annular pulley : stiffer and thicker A1A2A3A4A5
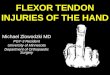
ZONE 1Contains only one tendon-FDPTendon laceration occurs close
to its insertionTendon to bone repair is required
Green DP, JBJS 2002Kleinert and verdan classified into 5
anatomic zones
ZONE II-NO MANS LANDFrom metacarpal head to middle phalanxFDS n
FDP within one sheathAdhesion formation risk is amplified at
campers chiasm ZONE IIIB/W transverse carpal ligament and proximal
margin of tendon sheath formationLumbricals origin here prevents
profundus tendons from over acting
ZONE IVLies deep to deep transverse ligamentTendon injuries are
rareLies proximal to transverse carpal ligament in the forearm ZONE
V
DIAGNOSISHistoryClinical examinationSpecial tests
DiagnosisH/o trauma by sharp objects
completely transected :no active flexion and loss of tenodesis
effect
Loss of inherent flexor tone and extended posture at PIP and
DIP
Functional tests of FDS and FDP
light touch and static two-point discrimination
Capillary refill of the volar digital pulp and the nail bed
Flexor tendon repairTypes : Primary: first 12-24 hours of
injury
Delayed primary repair : 24 hours to 10 days
Secondary repair: 10 to 14 days,
Late secondary repair: after 4 weeks
Ref campbell 12 th ed
Primary repairEmergency repair needed if altered digital
perfusion present
Clean wound caused by sharp object.
Secondary repairIndicated if a/w extensive crushing with bony
comminution severe neurovascular injurysevere joint injury and skin
loss requiring a coverage procedure
Primary repair gives better functional outcomes than secondary
repairs
Ref: Tang JB :Injury. 2006 Nov
Surgical IncisionsIncisions should not compromise viability of
skin flaps shd not create contractures or cosmetically unsightly
scars
Zigzag (Brunner) or midaxial incisions and midlateral
incisions
Suture Materials
Core Non-absorbable 4/0 suture 4-0 or 3-0 prolene or mersilene
suture may be used5-0 or 6-0 monofilament running epitenon
suture.
Ref: J Bone Joint Surg Am.1998. Singer G,
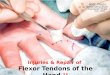
Zone I InjuriesDirect repair (primary tenorraphy): laceration
>1 cm from FDP insertion
Entire A4 annular pulley preserved
proximal tendon Retrieved by feeding tube and passed underneath
A4 pulley
Tendon advancement(3 to 6 weeks with tendon degeneration and
scar within the tendon sheath.
3. Large section of tendon has been damaged in zone 2 injury
4.Delayed presentation of FDP avulsion injuries associated with
significant tendon retraction.
Boyes' Preoperative Classification
Grade 1 Good: Minimal scar with mobile joints and no trophic
changes
Grade 2 Cicatrix: because of injury , failed primary repair or
infection
Grade 3 Joint damage: with restricted range of motion
Grade 4 Nerve damage: resulting in trophic changes
Grade 5 Multiple damage: Involvement of multiple fingers with
combination of above problems
From Boyes JH: J Bone Joint Surg Am 32:489-499, 1950.
Surgical principles One graft in each finger.Never sacrifice
intact flexor digitorum superficialis (FDS).Graft of small
caliber.Perform the junctions outside of the tendon sheath.Ensure
adequate graft tension.
Graft choicesPalmaris longus[1] tendon present in approximately
85% of all individuals of sufficient length and size . Plantaris
[2] when graft length is important. present in about 93% of
population EDL[3]EI [3]EDM[3]FDS of unaffected finger[4]
Ref: 1. MARTIN I. BOYER.JBJS 20022.MorrisonWA J Hand Surg
[Br]19923. HarveyFJ,J Hand Surg [Am]19834.SnowJW: Plast Reconstr
Surg1968
Proximal anchoringTendon weave in any area outside the flexor
sheath Stronger than the end-to-end suture techniques Allow to
modulate graft tension
Ref:PulvertaftRG:JBJS Am1980;42:1363-1371. RankBK: 2nd
ed.Edinburgh,E & S Livingstone,1988.
Distal anchoringProfundus stump not available:
Profundus stump available:
Technical Points 1cm FDP stump ,1 to 2cm FDS tendon near
insertion Obtaining flexor graft Graft threaded under pulleys with
suture passer(pediatric feeding tube/red rubber catheter Distal
juncture created
Proximal juncture into the FDP tendon just distal to the
lumbrical origin. (3 interweaves)
SourmelisSG:J Hand Surg Br1987;
.
In patients with DIP joint hyperextension, tenodesis or
arthrodesis can be offered.
Postoperative Care Static dorsal blocking splint (4 to 6 weeks)
with the wrist neutral, MP joints at 45 degrees, and IP joints
neutral. Treat flexion contractures with passive stretching and
splinting (6 to 8 weeks).
TWO-STAGE FLEXOR TENDON RECONSTRUCTION: STAGE I
Passive tendon implants at first surgery, placement of tendon
graft at second surgery
Indications Crushing injuries a/w # or skin damage Damaged
pulley system Excessive scarring of the tendon bed Failure of
previous operations Contracted joints
Technical Points 1-cm FDP stump kept & proximal FDP tendon
transected at the level of the lumbrical origin.
Through distal forearm incision identify the involved FDS
tendon, draw it into the wound, and transect it near the
musculotendinous junctionAppropriate size of the silicone
implant.Assess pulley system
Pass implant from proximal palm to distal forearm between the
FDP and FDS Distal juncture suture appliedROM checked
If implant assumes bowstring posture, pulley reconstruction done
by Bunnell encircling method/ Kleinert technique
.
Postoperative Care :Splint with wrist in 35 degrees of flexion,
MP joints at 60 to 70 degrees of flexion, and IP joints extended.
Start passive motion on first postoperative visitContracture
releases may benefit from dynamic splinting (6 to 8 weeks).
TWO-STAGE FLEXOR TENDON RECONSTRUCTION: STAGE II
Indication: Patient who underwent stage I of flexor
reconstruction process
Interval between stages I and II :2-3 months.Hand must be soft,
and joints well mobilized.
Surgical principles: Implant distal and proximal ends located
Tendon graft obtained Graft sutured to proximal end of implant, and
pull it distally through sheath.
Fix distal juncture and proximal juncture.(in palm or distal
forearm)
.Proper tension of graft maintaining necessary
Postoperative Care
Apply a short arm dorsal blocking splint Protected passive range
of motion early Dynamic splinting for contractures.
THANK YOU.