Embed Size (px)
Citation preview

Tendinopathy, Tendon Healing & Tendon Regeneration
Alayna E. Loiselle, PhDAssociate Professor
IND 464 Musculoskeletal Basic Science CourseOctober 21, 2019

Outline
• Review of homeostasis• Effects of Aging• Disruptions in homeostasis• Pathogenesis of tendinopathy/ tendinitis• Mechanisms of regeneration and healing

!"#$%#&'()*%)+,-.-&,*"&#%.&,&/#('%*0&1%1/+,.(%#
23456(#&2788,9:&&234:;2788,9:&<=>?@"-.&A=2B@&C87D
!"#$%&$"'!"#$%(')*+',-./
0"1%" !"#$%(')*+',-./
23%4&$5%4'!"#$%(')*+',-./ +6"4&74'5$'"1(8'!%7*9%:(',-./
;7%&5115';"<8'#4=#<1%&>5?'?"$"

Tendon Cell Proliferation During Growth
Grinstein eLIFE 2019

Tendon Cell Proliferation During Growth
Grinstein eLIFE 2019

!"##$%&'%(%)*+!"#$%&'()*+)(,%-,./0()%,1%%/(2344523678*")$%9(&,+*-:;%'.#(2<=>%/9*/(&/9(+"-#$%().*:-.%-(?'*+(:&,.%/,-()*'/(@23<A523BAC--%--+%/,(*?(,.--"%(,"'/*D%'('&,%
,("-"*-".(&./&0.10&-%#-"(2
!%#-&0*(&-3%*-4

Tendon HomeostasisYoung Aged
• Matrix composition and organization is not dramatically different• Decreased proteoglycan content• Changes in cell morphology
Functional Consequences of Aging?

Tendon is not mechanically sensitive to aging
Ackerman et al., 2017. JOR
TT Fa
scicl
eFD
LFC
U

!"#$%#&'&()*#)! !"#%+,-" ./*"0+"#+"&1#$&2%3456"./"#+,&789&
-/6#%:"6;&$"+6"10"$&0"#0*-*:*-,&-%&1)*#)&<:0=&>%#"?
! @%3":"6A&1)*#)&*0&100%+*1-"$&3*-BC&*#+6"10"$&-"#$*#%D1-B,A&*ED1*6"$&B"12*#)
! FD%#&+B122"#)"&<*#G/6,A&+%E%6>*$*-*"0?&1)"$&-"#%+,-"0&B1:"&*ED1*6"$&1>*2*-,&-%&6"0D%#$&6"0/2-*#)&*#&1)"46"21-"$&-"#$%#&D1-B%2%),

!"#$%#&'()*+!"#$%#$&'(&)*$&)$+,'+
! -%"+(./! 01%2$34%)$,&45&%2)"6")5! 7'#)&2'88'+&"+&)*$&92*"//$#! :$+,'+")"#;&%2.)$&"+(/%88%)"'+&%+,&"+<.35;&%2.)$&"+(/%88%)"'+&%+,&"+<.35
=2"6$)>2'8

!"#$%#&'()*+!"#$%#$&'(&)*$&)$+,'+
! -%"+(./! 01%2$34%)$,&45&%2)"6")5
! 7$+,"+'#"#8&2*3'+"2&9")*&,$:$+$3%)"6$&2$//./%3&2*%+:$#;&+'&"+(/%<<%)"'+
! ='3$&2'<<'+&)*%+&)$+,"+")"#! >'+)"+."+:&('3&/'+:$3&)*%+&?&<'+)*#
@2"6$)A2'<
8&2*3'+"2&9")*&,$:$+$3%)"6$&2$//./%3&

!"#$%&'()*+&,')-'.+"*#")/%012'3'4+%&#"567/8%,/#"%07,'98)0%0)8':7--; !:1#&&+,'.+"*)" <%0+&&%8'.+"*)" =&+>)8'.+"*)"
()7,+?%"#"+?1#:@+"A%0A%BB#04)8,+<#5
()7,+A%0A%BB#0
()7,+A%0
CD+8'EF'%"#$%&,':1%8%:0+8#G+*H
$),0':)$$)"IA%0
()7,+
9H; 6),&)J,@2 KLM'+0'%&NM'L'61)7&*+8'O&B)J'6785 HPPQRSIETEUEPV9V; .1)$)/)7&), +0'%&NM'LCAN'VFHS'98+D#+J;
(+:1%"#:%&':1+$#:%&'
?)$/&+0+'08%",+:0#)"WXY 8+/%#8
<%80#%&'08%",+:0#)"Z#)/,2'/7":1
.+"*#")/%012
4+%&#"5
67/8%,/#"%07,'98)0%0)8':7--; !:1#&&+,'.+"*)" <%0+&&%8'.+"*)" =&+>)8'.+"*)"
Z#)/,2'/7":1?)$/&+0+'08%",+:0#)"
W'8+/%#8<%80#%&'08%",+:0#)"
Z#)/,2'/7":1
(+:1%"#:%& =%0#57+'&)%*#"5
=7&&'01#:@"+,,M'/%80#%&'J#*01.+"*)"'0)'B)"+'1+%&#"5
[#%B+0#:'0+"*#")/%012

!"#$%&'()*
!"#$%&'#(')#!*#+(,,-.(/0##1&2%-)3#4'#$&,,#54-,-6/7#8-,9:&#;<=7#>?;@7#>AAB<>?

!"#$%&&%'()"*(+*%*,)'-"'*&-.(%')/*)#*'-".("),%'01
!"#$%$&'()'$*+,'-./01 2345+

!"#$%&'()*+,-(,#'.#"#/*!".0('(#
1,2'$,3 !".0('"4
! !"#$%&%'%&()'*+%"$),()&"#-.#/! 01"2.+$)*+")3.$&)$"#$%&%'"! 4*&5.1.6%7*1)75*#6"$)%#7+"*$")8%&5)-%$"*$")-9+*&%.#
! :(;")<)*#-)&(;")<<)-%*,"&%7$)*+")"=9*11()$9$7";&%,1")&.)>1"2.+)&"#-%#.;*&5(
! <#7+"*$"-)+*&").>)+9;&9+"! :?@A)>9+&5"+)%3;*%+$)&"#-.#)5"*1%#6)*>&"+)+9;&9+").+)%#B9+(

Collagenase Induced Tendinopathy
LD= low doseHD= high dose collagenase
Induces degenerative changes via collagen degradation
Orfei C et al. (2016) PLOS ONE 11(8): e0161590.

Mechanically Induced Tendinopathy• Fatigue loaded under anaesthesia• Uphill treadmill running• Downhill treadmill running
Neviaser A. 2012. J Shoulder Elbow Surg. N Andarawis-Puri et al., 2014. JOR
UnloadedLow levelloading
Moderateloading
High levelloading
Fatigue Loading Induces Apoptosis
Induces matrix and cellular changes

!"#$%&#$'()(%! !"#$%&&%'()"*)#*'+,*-+,%'+! .%/-,-0*("#$%&&%')12*3(-,%-,-4*("#,5'()"4*("6/12! 7)-'*5)&&)"$2*("*+%"38*91(-'
:5(;,'<5)&

!"#"$%&'()*+*,%-."*,%/"$*%0*&1%)"('2*3"(%.1(%#'3'.!"#"$%&'()*+*,%-."*,%/"$*%0*&1%)"('2*3"(%.1(%#'3'.4%(35%$
6"(/%(
78"+38*.&+2"
9%("
:(0"23"/
6"(/%(
9%("

!"#"$%&'()*"+,')-'$"#*%#)./$01230+"4,56/#+),'71#*4)("
! !"#$%&'()*+,"-#.#%(&/$0&1+*23*$%&0#4."5/%#"$4! 63%/%#"$&#$&7".8! 9*$0"$:4)*5#1#5&7".8 ;<: =>?" @-$"+,/.&A/#%B&C"#$%&./D#%(B&/.%*+*0&5"../A*$&4%+35%3+*
! 7".8EF: /.%*+*0&%*$0"$&4%+35%3+*B&#,)/#+*0&%*$0"$&'*/.#$A
?3$&*%&/.GB&@!HG&IJKLB&!"'$4%"$&*%&/.GB&!<MG&IJKN
/.%*+*0&%*$0"$&4%+35%3+*B&#,)/#+*0&%*$0"$&'*/.#$A

Summary of Tendinopathy
Future Directions• Continue to identify co-morbidities that predispose or accelerate tendinopathy
• Most clinical data are from late stage pathology
• Beginning to use genetic animals models to better understand tendinopathy
Remodeling BalancePhysiological exercise increases: proliferation
collagen productiontenocytic gene expression (w/o chondro/ osteo/adipo)
Overuse/ Fatigue: Matrix DamageTenocyte apoptosis
Effects of pathology and/ or co-morbidities: promote degeneration +/- inflammationSmokingobesityhigh cholesterol

!"#$%#&'"()*#+! ,-../...&0"#$%#&1"2(*1&21%3"$41"5&2"1&6"(1
! 78"1&9:.&;*))*%#&*#&(55%3*(0"$&<"()0<&3(1"&3%505
! '"()*#+&*5&3%=2)*3(0"$&>6&53(1&?%1=(0*%#
@%1=()&0"#$%# A3(1&!*554"
!"#$%&'#()*+,#-"&&./. ())(,#0"1"!2.34.5& ())6,#7"815&9% ())+
!"#$%#
B$<"5*%#
C"$53(2"D3%=

!"#$%&%'%()*(+*,-"./)%"/0*12(3-2'%-&
Maximum Load at Failure
14 21 28 35 42 49 63 0
2
4
6
8
10
Days Post-Surgery
[N]
Control
40-5(2*6-)7()
!"#$%&&%'%(')&*+',--.*'/01 2'3&#)$$"4 %(')&*+',--.*'/'566& 278$*'
94&"):%: &"):%:
!".%00-&*6-)7()

Similarities between wound and tendon healing
AJ Jomas et al. 2014. Advanced Drug Delivery ReviewThiruvoth et al. 2015. Plastic and Aesthetic Research

Similarities between wound and tendon healing
Nichols, Best, Loiselle. 2019

Well-regulated inflammation is beneficial-activates healing cascade
-recruitment/activation of cellsExcessive/ Chronic inflammation is pathological
-degenerative matrix changes-fibrotic healing
Inflammation
Benefits of Anti-inflammatory therapy is controversialTiming may be key!
Generally effective at preventing excess scar formationEarly inhibition decreases mechanicsDelayed healing maintains mechanics
Cell-type specific considerations
Virchenko et al., 2004. Am J Sports Med, Geary et al. 2015. PlosOne

Proliferative/ Granulation Phase• Lasts a few weeks• Begins ~day 7 in mouse model• Proliferation of ‘fibroblasts’• Bridging on injury site• Production of ECM components (Col1/ Col3)• Rapid deposition of disorganized ECM
Day 3 Day 14
Thomopoulos et al., 2009. JOR, Thomopoulos et al., 2010. JBJS, Katzel et al. 2010. JOR, Awad Lab, Loiselle Lab
Col3a1 ISH
Tendon
Tendon
ScarTissue

Remodeling Phase• Lasts many months• Begins ~day 21 in mouse model• Reorientation of ECM• Mmp-mediated remodeling
Day 21 Day 28 Day 35

!"#$%&'())*+,-$)./0+%-123/1-
4/#%-$1-5+6-/53/+1.7-8+9():
4;2$.%-5+0).5./0+'(/#6.3/+<+16%-/06,
=.13%0$/.7-5+>?6%$#-))()$%+@$6%.?+A>B@C
>?#-11.D-+>B@+E%35(#6.3/ 4/1(''.#.-/6+>B@+F-;35-)./0
B3)G8+B3)H
>B@+E%35(#./0+B-))1 @@E+E%35(#./0+B-))1
I-/53/+4/J(%K
@$6%.?+@-6$))32%36-./$1-1
'())*+,-$)./0+%-123/1-
4;2$.%-5+0).5./0+'(/#6.3/+<+16%-/06,
4/#%-$1-5+6-/53/+1.7-8+9():
=.13%0$/.7-5+>?6%$#-))()$%+@$6%.?+A>B@C
>?#-11.D-+>B@+E%35(#6.3/ 4/1(''.#.-/6+>B@+F-;35-)./0
B3)G8+B3)H
>B@+E%35(#./0+B-))1
@-6$))32%36-./$1-1
@@E+E%35(#./0+B-))1
!"#$%&'&$( )"*$+",&(-
"(##-11'()+F-2$.%L+M+=-).#$6-+9$)$/#-+3'+5-231.6.3/+$/5+%-;35-)./0

Double-edged sword of tendon healing
Matrix deposition Mechanical properties

Fibrosis
• Thickening and/or scarring of connective tissue• Typically in response to injury• In response to injury fibrosis= scar tissue• Excess matrix deposition• Disorganized matrix• Exuberant healing response
Inflammation Matrix Deposition

!"#$%&'()'*+,&'+-./%,.'01,2+&3'$-.'43#,'!!'*+$1,&,2'(-'4,-.(-'5,$6+-7
!"#$%&'$()*'$+!%(,-$./0$12&3$45"6$4&'7$3*&8$2"8'5"3$
9):;$%&'$()*'$+9%(,-$</0$12&3$45"6$4&'7$=>(?
@A#B$"3C$?&3*
DEFG!H<I$?)2*
!%($
9%(
/
()*'$)8)')&')"8
J**BKL F ./ .@ >. >M
(&NK$O"K'APQ5:*5N
9&5R*K'KPQ5:*5N
.>
S2B*56&8T O3"KU8*V$>/.FV
Body Weight
LFD HFD 0
10
20
30
40
50
Bo
dy
Wei
gh
t (g
)
Diet
LFDHFD
*Fasting Blood Glucose
LFD HFD0
50
100
150
200
250
Diet
mg
/dL
*Glucose Tolerance Test
0 15 30 60 120 0
200
400
600
Blo
od
Glu
cose
[mg
/dL
]
LFDHFD
* **
Time Post-Glucose Bolus
Body Weight
LFD HFD 0
10
20
30
40
50
Bo
dy
Wei
gh
t (g
)
Diet
LFDHFD
*
LFD HFD0
20
40
60
Diet
Bod
y Fa
t [%
]
Percent Body Fat
****

T2DM Impairs Tendon Healing
Ackerman+ PlosOne. 2017.
MTP Flexion Angle
10 14 21 280
10
20
30
40
50
MTP
Fle
xion
Ang
le [D
egre
es]
Days Post- Repair
LFDHFD
**
Gliding Resistance
10 14 21 280
20
40
60
80
Days Post- Repair
Glid
ing
Res
ista
nce
[A.U
.]
*
Max Load at Failure
10 14 21 280
1
2
3
4
Days Post- Repair
Max
Loa
d at
Fai
lure
[N]
LFD HFD **
Col3a1
3 7 10 14 21 280
2
4
6
Days Post-Repair
Rel
ativ
e m
RN
A E
xpre
ssio
n
* *
*HFDLFD
Col1a1
3 7 10 14 21 280
1
2
3
4
Days Post-Repair
Rel
ativ
e m
RN
A E
xpre
ssio
n
*
**
*

!"#$%&'()(*+,%-*.%/)01',%2*3)-44-05(*!"#$%&'()*&+ ,-./
01234
012345555.678 012345555.678
!"#$%#!"#$%#
*
*
*
*
6+9):;'#< 7=">?#)@5-4AB@
F4/80
7 14 21 280
1
2
3
4
5
6
7
Days Post-Repair
Rel
ativ
e E
xpre
ssio
n
Non-T2DMT2DM
*
*
*
&#'(")*"$+,)'(%-.)/"+'%#0"#01(%2%#/"$+,)'(%-.)/"+-("*"#'"&#'(")*"$3+-(%2%#/"$+-(%45#62),,)0%(7+89+,)'*&#'(")*"$3+")(27+)#0545#62),,)0%(7:+8;+,)'*

Aging decreases fibrotic tendon healing (too much)
Ackerman et al., JOR. 2017.

Aging decreases fibrotic tendon healing (too much)
Ackerman et al., JOR. 2017.
No change in proliferative capacityDecreased matrix production on a per cell basisIs the cellular environment the same?

!"#$#%&'(&)*++,&-."#%$&/*%0'%&1*2+#%$3&4%5"#%,#6&7&895"#%,#6
/:*&6*++.+2"&6';<'%*%5,&'(&5*%0'%&:*2+#%$&2"*&%'5&=*++&6:2"265*"#>*0543
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 85-A · NU M B ER 3 · MARCH 2003BIOLOG I C AS P E C T S OF FLEXOR TENDON LA CER A T I ON A N D REPAIR
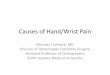
response observed clinically is a combination of extrinsic andintrinsic mechanisms (Fig. 4)1.
The differences between the extrinsic and intrinsic mech-anisms extend beyond the site of origin of the healing cells. Theextrinsic mechanism appears to be active earlier in the healingsequence, whereas the intrinsic mechanism is often delayed10,11.Some studies have demonstrated that the synovial sheath reactswith a greater proliferative and inflammatory response com-pared with the endotenon and tendon proper12. Other studieshave shown the synovial fibroblasts to be more reactive to cy-tokines and to have a greater capacity for degradation of theextracellular matrix11. In addition, it is thought that predomi-nance of the extrinsic mechanism of healing leads to increasedcollagen content at the injury site as well as to a reduction inthe level of collagen organization and material properties of thereparative tendon tissue13,14. For these reasons, it is believed thatthe predominance of the extrinsic mechanism of healing leadsto scar formation and adhesions between the tendon and sur-rounding peritendinous structures.
Modulating the healing process to enhance the intrinsicpathway (and augment end-to-end tendon healing) whilesuppressing the extrinsic pathway (and diminishing adhesionsof the tendon to surrounding tissues) could lead to improve-
ments in the treatment of these injuries. While investigationsinto the biology of tendon healing have shed some light on themechanisms by which tendon tissue heals, there has been rela-tively little progress toward the biologic enhancement of thehealing process after injury and repair. As a result, modulationof the process by which tendons heal remains an appealing,but not currently practicable, concept.
Biologic Solutions to Adhesion Formation: Historical PerspectiveIt is well recognized that motion prevents scar formation1,7,15-17.There is not a specific amount of motion that is needed, onlya relative amount�that is, enough to overcome the problemsof scarring and adhesion formation. If one could decrease theamount of scarring associated with a given amount of mo-tion, less motion would be required. This approach wouldeliminate the need for aggressive postoperative motion pro-tocols that place the tendon repair site at risk for dehiscence.If the ideal scar inhibitor could be found, the patient couldbe treated with postoperative immobilization in a cast orsplint until the tendon healed, allowing the repair to heal in amechanically protected environment without concern aboutadhesions.
Historically, prevention of adhesion formation has beenattempted on two fronts. The first method has been to place aphysical and mechanical barrier between the healing tendonand the surrounding tissues. The rationale for this approachis that limiting contact between the tendon and its sheathdiminishes the amount of adhesions around the repaired ten-don�that is, the tendon is allowed to heal to itself but not tothe sheath and surrounding tissues. The various barrier ma-terials that have been tried include silicone18, polyethylenemembranes19, alumina sheaths20, polytetrafluoroethylene21, andchondroitin sulfate-coated polyhydroxyethyl methacrylate mem-branes22, among many others. In spite of the many differentmaterials studied for this purpose, none are in routine clinicaluse at this time.
In a similar approach, many authors have attempted touse chemical modulation to diminish the amount of scar for-mation after repair. The chemical agents that have been usedin these efforts include local23,24 and parenteral25,26 corticoste-roids, dimethyl sulfoxide27, beta-aminoproprionitrile28, hyalu-ronic acid29,30, and 5-fluorouracil31,32, among many others. Thecommon principle of these methodologies is reduction of in-flammation. In the case of the corticosteroids and hyaluronicacid, the goal is to diminish inflammation by inhibiting lym-phocyte migration, proliferation, and chemotaxis as well asmacrophage motility. Similarly, 5-fluorouracil, an antimetab-olite, suppresses scar formation by inhibiting contraction ofcollagen lattice and proliferation of inflammatory cells31,32.
Researchers using barrier and chemical techniques havereported some degree of adhesion reduction in laboratory andclinical studies of tendon repair18,20,21,23,25,29,31,32. In spite of thesefindings, these methods are not widely used in clinical prac-tice. This suggests that none of them have been demonstratedto be effective in most clinical settings.
Fig. 4
Schematic representation of extrinsic (A) and intrinsic (B) pathways of tendon healing. (Adapted from: Gelberman RH, Vande Berg JS, Lund-borg GN, Akeson WH. Flexor tendon healing and restoration of the glid-ing surface. An ultrastructural study in dogs. J Bone Joint Surg Am. 1983;65:78-79.)
on October 7, 2006 www.ejbjs.orgDownloaded from
543
TH E JO U R NA L OF BONE & JOINT SURGER Y · J BJ S .ORG
VO LU M E 85-A · NU M B ER 3 · MARCH 2003BI O LO G I C AS P E C T S OF FLEXOR TENDON LA CER A T I ON A N D REPAIR
response observed clinically is a combination of extrinsic andintrinsic mechanisms (Fig. 4)1.
The differences between the extrinsic and intrinsic mech-anisms extend beyond the site of origin of the healing cells. Theextrinsic mechanism appears to be active earlier in the healingsequence, whereas the intrinsic mechanism is often delayed10,11.Some studies have demonstrated that the synovial sheath reactswith a greater proliferative and inflammatory response com-pared with the endotenon and tendon proper12. Other studieshave shown the synovial fibroblasts to be more reactive to cy-tokines and to have a greater capacity for degradation of theextracellular matrix11. In addition, it is thought that predomi-nance of the extrinsic mechanism of healing leads to increasedcollagen content at the injury site as well as to a reduction inthe level of collagen organization and material properties of thereparative tendon tissue13,14. For these reasons, it is believed thatthe predominance of the extrinsic mechanism of healing leadsto scar formation and adhesions between the tendon and sur-rounding peritendinous structures.
Modulating the healing process to enhance the intrinsicpathway (and augment end-to-end tendon healing) whilesuppressing the extrinsic pathway (and diminishing adhesionsof the tendon to surrounding tissues) could lead to improve-
ments in the treatment of these injuries. While investigationsinto the biology of tendon healing have shed some light on themechanisms by which tendon tissue heals, there has been rela-tively little progress toward the biologic enhancement of thehealing process after injury and repair. As a result, modulationof the process by which tendons heal remains an appealing,but not currently practicable, concept.
Biologic Solutions to Adhesion Formation: Historical PerspectiveIt is well recognized that motion prevents scar formation1,7,15-17.There is not a specific amount of motion that is needed, onlya relative amount�that is, enough to overcome the problemsof scarring and adhesion formation. If one could decrease theamount of scarring associated with a given amount of mo-tion, less motion would be required. This approach wouldeliminate the need for aggressive postoperative motion pro-tocols that place the tendon repair site at risk for dehiscence.If the ideal scar inhibitor could be found, the patient couldbe treated with postoperative immobilization in a cast orsplint until the tendon healed, allowing the repair to heal in amechanically protected environment without concern aboutadhesions.
Historically, prevention of adhesion formation has beenattempted on two fronts. The first method has been to place aphysical and mechanical barrier between the healing tendonand the surrounding tissues. The rationale for this approachis that limiting contact between the tendon and its sheathdiminishes the amount of adhesions around the repaired ten-don�that is, the tendon is allowed to heal to itself but not tothe sheath and surrounding tissues. The various barrier ma-terials that have been tried include silicone18, polyethylenemembranes19, alumina sheaths20, polytetrafluoroethylene21, andchondroitin sulfate-coated polyhydroxyethyl methacrylate mem-branes22, among many others. In spite of the many differentmaterials studied for this purpose, none are in routine clinicaluse at this time.
In a similar approach, many authors have attempted touse chemical modulation to diminish the amount of scar for-mation after repair. The chemical agents that have been usedin these efforts include local23,24 and parenteral25,26 corticoste-roids, dimethyl sulfoxide27, beta-aminoproprionitrile28, hyalu-ronic acid29,30, and 5-fluorouracil31,32, among many others. Thecommon principle of these methodologies is reduction of in-flammation. In the case of the corticosteroids and hyaluronicacid, the goal is to diminish inflammation by inhibiting lym-phocyte migration, proliferation, and chemotaxis as well asmacrophage motility. Similarly, 5-fluorouracil, an antimetab-olite, suppresses scar formation by inhibiting contraction ofcollagen lattice and proliferation of inflammatory cells31,32.
Researchers using barrier and chemical techniques havereported some degree of adhesion reduction in laboratory andclinical studies of tendon repair18,20,21,23,25,29,31,32. In spite of thesefindings, these methods are not widely used in clinical prac-tice. This suggests that none of them have been demonstratedto be effective in most clinical settings.
Fig. 4
Schematic representation of extrinsic (A) and intrinsic (B) pathways of tendon healing. (Adapted from: Gelberman RH, Vande Berg JS, Lund-borg GN, Akeson WH. Flexor tendon healing and restoration of the glid-ing surface. An ultrastructural study in dogs. J Bone Joint Surg Am. 1983;65:78-79.)
on October 7, 2006 www.ejbjs.orgDownloaded from
!"#"$%&'(&)*+,--.
895"#%,#6&1*2+#%$ 4%5"#%,#6&1*2+#%$
?'%*&;2""'=@&6#"6.+25#%$&6*++,
A%0*(#%*0&B#+#*.CBD'(#E"'E+2,5, F!CGBHICG:*25:&FJ"$KI&C?2,*;*%5&;*;E"2%*
F+2;#%#%ICL
M*,#0*%5&/*%'6D5*,
G69C+#%*2$*
B26"'<:2$*,@&4%(+2;;25'"D&6*++,

!"##$#%&'(%)*)'+,'-"%#*./0'1.2&*.)*3'!"##)4".+352")0'637 &"8%*.)'9")2'8%&:"&';*2<'/"."2*3'2++#)
!"#$%%&$'&(%)*&+,-.)&/012$3

!"#$%%&$'&(%)*&+,-.)&/01$2'1310&4$5"6'7
89:$2' $'&(%)*&+,-;)&<%"7=2$)
>"17$%%$&$'&(%)*&+,,?)&@=4
/(A(B$ $'&(%)*&+,-C)&@DE)
E"2'61BF'1"2&"3&/0GH0$%%7&'"&I$(%12J&17&0"2'6"K$671(%&(2L&0"2'$G'&L$5$2L$2'
8(9&; 8(9&.
8(9&-M 8(9&+-
/0G
!"#$%%&$'&(%)*&+,-.)&/01$2'1310&4$5"6'7

!"#$%& $&'()*+',-./*'0)123%$
!"# !$%
&'()*+,-)+'(.'/.!"01*2#+3 &1003.)'.4120+(56.7151(1*2)+'(.2(8.!"2*.9'*:2)+'(.+3.;("012*
9-(")+'(.+3.0+<10=.)'.,1."'()1#).81>1(81()

!"#$%&$'()*+,-."/0
1234/5 6-77)$6(5*0/89*-$*($:0/;</5<$'(.97"*/(5$8#$!"#$%&
1234/5 !='>
?5+/5@90-; !"#$A$'()*+,-."/0
!"#$B%$'()*+,-."/0
!"
#$!% !$
CD3
&'()*+
, -EF .#
/)+0'121
A- ScxLin – Tmx Washout
3'1245467*1'88'49:;<34.,#=

!"#$%&!"#$%&'()*+,-./.
!"#$%&'((%)'*+,%-./012'3%4'*(567%8'6316%!+0'67+,
012'()"*&34056+,-./0
! !"##$"%$&'( ')**#$+#$,)-)%+'+.*$/"$*./)$0).*+-1
()"'
()"0

!"##$#%&'(%)*)'+,'-"%#*./0'1.2&*.)*3'!"##)
!"#$%&'()'"$*+',-..*'/$%012(
4%5*.*.
!+.2&*6$2*+.'+,'6%)"5".2'5"56&%."'7#%5*.*.89'3"##)'2+':"%#*./'%.;'%;:")*+.',+&5%2*+.

!"##$%&$'(&!)* )+,,-&.$/+&(0-10')1&-2$10$,&+*23+--04'&23450,+-&(630'7&.+$,0'7
89
899
:$;&<"
&=4-1>?
+2$03
!"
!""
#$%&'(#)**+,
>@"%
>A >%BC*
?+2$03
# DEF <"
G$3/+-1
!)*>83+H?1<I&?4-$>J0KI&&!"##$%>LM=234C41+3X
-./0121&3'/.44.156#7-18*)9

Cellular Basis of Healing: Extrinsic Cells
Fluorescence
Bone Marrow AblationBone Marrow Harvest
Bone Marrow Transplant
GFP Bone Marrow Chimeric Mouse
Tendon Injury and Repair
C57BL/6 GFP

!"##$#%&'(%)*)'+,'-"%#*./0'123&*.)*4'!"##)
5%6'78
!"#$%#
!"#$%#
&'()*!+,,-"
!+.3&+#
!"#$%#
(+."'9%&&+:'5"&*;"<'!"##)'9*/&%3"'=>"4*,*4%##6'3+'3?"'@">%*&'=*3"
.%+,"//"*"0*(/12*34531*6/%,7#"2*8(9+:(;(2*<1*"0*(/1*=%-)#(/*%>*?"//*6@A,+%/%BA1*344C
A.B*.C$&"< 5%6'D
! =>"4*,*4'=$EB>+>$#%3*+.)'&"F%*.'$.G.+:.
! H$.43*+.'.+3'I4#"%&
! DEFEGHI*,->>+'+"#0*>%)*($@",+%#*>%)G(0+%#

Future Work
• Delineate intrinsic vs. extrinsic contributions of cell types– Macrophages– S100a4
• Define functions of intrinsic & extrinsic populations• Understand how homeostatic populations change in response
to injury

!"#"$"%&'()"*+"&,($#-*./0%12$(3
!"#"$%&'(&)* +,-".-)(/0-1223/-4**)(5-67-!&68"$&9)(-:*;&*""#&*;
4"'&,*56""7 8&'9%"*56""7
:$;($
<9%"=
:$;($
<9%"=
>$<9%"=
>$<9%"=

!"#"$"%&'()"*+"&,($#-*./0%12$(3
!"#"$%&'(&)* +,-".-)(/0-1223/-456
789#:;*&<-)*$-)$=(.-."*$;*-&8>()*."$-&*-.;-.?"-9)<'-.;-$"."#8&*"-&@-"89#:;*&<-."*$;*A-<;=($-?")(-A<)#B("AA(: &*-)*-)$=(.-"*C&#;*8"*.
D$=(.E-F""'
789#:;*&<E-F""'
789#:;*&<G-F""'A

!"#"$"%&'()"*+"&,($#-*."/$&'&,
!"#$%%&$'&(%)*&+,-.&/012$3

!"#$%&'()*+),')%-./)0123/)4,5,-678,9'
!"#"$"%&'()"*+"&,($#-*."/$&'&,0%&1($#*2,(34,($"&#"*1",,5*&6'"%*"$'7"5(5 ($89%:
2,(;:,69%'%- ;6<9=)%><-'

Where do we go from here? (2017)üCritical mass of labs studying cell lineage/fate/functionüBig data and single-cell RNAseq• Development of tendon specific tools• Identification of new ‘tendon-specific’ markers

! !"#$%#&'"((&)"*"+%,"#"-*.! /"(-#"0*"&12#3*-%#4&%1&4256%62(0*-%#4! 7""$&*%&$"1-#"&3"((&%+-,-#8&(-#"0,"&0#$&10*"! 9#$"+4*0#$-#,&%1&3"((:3"((8&3"((:;0*+-<&-#*"+03*-%#&!6="#%*.6"
>="+"&$%&?"&,%&#%?@!"#$%#&'"((&)"*"+%,"#"-*.
A;;2#"&'"((4B"4-$"#*&!"#%3.*"4
C-5+%*-3&)"0(-#,
9#$"+4*0#$-#,&'"((:'"((&A#*"+03*-%#4/"1-#-#,&'"((&D-#"0,"&0#$&!"+;-#0(&C0*"
A#E2+.
FGHH0I(-#"0,"JK FGHH0I03*-L"J
FGHH0I(-#"0,"JK FGHH0I03*-L":K&MFNOJ
N.%1-5+%5(04*4
FGHH0I(-#"0,"JK FGHH0I03*-L"JK&MFNO:
7%#:;.%1-5+%5(04*4

Tenocyte transition to myofibroblasts?
Ø ”Specialized”/ Activated FibroblastsØ Involved in matrix deposition Ø Restoration of tissue integrity

!"#$%#&'#()*+ ,-.*%/-/
0%&!*"123"#2/
!"#%4+2"&5"2"*%6"#"-2+7$-88"*"#2-19&*"/:%#/"&2%&-#()*+
,-.*%/-/
;4)2"&'#8913312-%# <=4"//&<>?&@":%/-2-%#
?14*%:516"&A"*/-/2"#4">5*%#-4&9%B79"C"9&-#8913312-%#
?+%8-.*%.91/2&A"*/-/2"#4"<=4"//&<>?&A*%$)42-%#

Am J Respir Cell Mol Biol, 2019https://www.atsjournals.org/doi/abs/10.1165/rcmb.2018-0313OC
Fibroblast heterogeneity at baseline with differential contributions to myofibroblast fate

!"#$%&'#$()*+
!"#$%&'()*+,$-+./$*&)%$,0+1").&1+%2#3+&)4#

!"#$%&$'()*+,-./0.# !"#$12$'()*+,-./0.#
! ,34$'(
)*5
! ,34$6)
7&8
50 !m
50 !m50 !m
50 !m
9+,34$$$6)7&8 !4':
9+,34$$$ '()*5 !4': 9+,34$$$ '()*5 !4':
9+,34$$$6)7&8 !4':
4
;
<
!
'=05(*#7>?$"5@$A-5?*>(5"B$)=>A*)$(C0.$*>D0

!"#$%&'()&*#)+,-.$)#.-(,&'+",/$0#(1##'$2344-5$-'6$!7289
!"#$%%$&'($% $#)*+,)-./0)12345236515,)782119
! :#-).;$-..$6#)<-.$=,0)&0.-+(+$-)#$2344-5>?@7289>
! :&$%&7.&%-.,A-(,&'$+##'$,'$BC,#+%#'($&)$-%(,*-(#6$"#/-(,%$+(#..-(#$%#..+
2344-5 @7289 <#)D#
EF,0)&0.-+(?$(#'&%;(#G 8;&=,0)&0.-+(+
HI8$J#/&+,(,&'
HI8$I&'()-%(,&'
J#=,','D$("#$<;&=,0)&0.-+($/)#7%C)+&)+$6C),'D$(#'6&'$"#-.,'D

0
20
40
60
80
Fluo
resc
ent a
rea
[%]
**
S100a4Lin+; α-SMA+
S100a4-GFPpromoter+; α-SMA+
S100a4+ cells are not myofibroblasts in the healing tendonBut, S100a4-lineage cells become α-SMA+ myofibroblasts
Ackerman et al., eLife. 2019

!"#$ %&'()*+),'-./&+.-'!01.234/
567'8!"#93:;<!=9(97>
!"?@A%#3/93:)*+), =3"@
B%4@?/'&@CD.C'"@??/'&E%&'@#-A@//'!"# )*+),'D%1/'-./&+/FAG@A1
!"#$%
5@-%3A
&
H%AI@/&
(1C%03"'J.C&A34F&3.C'.2'!"#B3C %CD'!"# K#-A@//3.C'&.'=1.234A.4?%/&'6%&@