Embed Size (px)
Citation preview

REVIEW OF HAND REHABILITATION PROTOCOLS AFTER FLEXOR TENDON INJURY REPAIR
BY:Dr. Mohammed A.Alhussein
Baghdad universityAlkindy college of medicine

Terms should be explained• standard protocols employ a dorsal shell with the wrist, MCPs, and IPs flexed. • Active extension (to prevent PIP contracture) and passive flexion are
encouraged after the first postoperative day, when bleeding should not be provoked.
• After 2 to 3 weeks, “place and hold no power” can be initiated along with protected passive motion to maintain joint mobility and avoid contractures especially the PIP joint.
• Differential gliding of the uninjured tendons can also start at that time with wrist tenodesis and “suitcase” power fist.
• isolated active tendon differential gliding of the injured tendon begins by at least 4 to 6 weeks and active, assisted, complete fist and passive range of motion.
• Protective splinting may continue with progressive resistance exercises for up to 8 weeks total
• With gradually increased active resistance-strengthening exercises up to 12 weeks
• PAUL ZIDEL Grabb and Smith's Plastic Surgery, Sixth Edition

In this lecture I will try to give short review on the common rehabilitation protocols.
Rehabilitation involve mainly 3 objects:1. Immobilization method and positions2. Type and timing of mobilization3. Time of splint removal and return to full
unprotected functioning.

• In order to facilitate dealing with this hard subject I will divide type of physiotherapy according to zone of injury then I will summarize these common protocols.
• By the end of this lecture we should be familiar with the common terms used above.

Repair of Zone 1 Lacerations or Avulsions:
• Definition: Laceration of the FDP tendon distal to the insertion of the FDS tendon or avulsion from its insertion at the base of the proximal aspect of the distal phalanx .
• If the tendon is lacerated, and the distal tendon stump is less than 1 cm long, FDP tendon advancement and primary repair to bone is usually indicated.
• If more than 1 cm of FDP stump is available for suture, primary tenorrhaphy is usually done because shortening of the FDP tendon by greater than 1 cm may result in a “quadrigia” effect.

Zone 1 Rehabilitation
Immobilization:• Apply dorsal splint with wrist and MP joints
flexed and PIP and DIP joints at 0 to 10 degrees flexion.

Zone 1 Rehabilitation
• Mobilization:The rehabilitation protocol generally follows the
same progression as for zone 2 injuries.• Return to Activities:The patient may return to full activity at 4 to 6
months after surgery.

Zone II injury
• definition : any injury at the proximal portion of the flexor tendon sheath A1 pulley and extends to the FDS insertion.

Zone II injury Rehabilitation
• Immobilization: the wrist flexed (20 to 30 degrees) and MP joints flexed (50 to 70 degrees), and PIP and DIP joints at zero or slight flexion.

Zone II injury Rehabilitation
• Rehabilitation divided into 3 groups according to protocol used in 1st 3-4 wks :
1. Immobilization:2. Early Controlled Motion– Duran & Houser– Kleinert & Chow
3. Active Mobilization– Silfversksold & May– Strickland

• Return to Activities• The patient may return to unrestricted
activity at 4 to 6 months after surgery

Tendon injury in Zones 3, 4, and 5
• Zone III is between the distal palmer crease distally and the distal margin of the carpal tunnel proximally.
• Zone IV is within the carpal tunnel.• Zone V is proximal to the carpal tunnel in the
distal forearm.

• Both immobilization and mobilization protocol are similar to zone 2 except modification which should be done when there is association with Arterial and nerve injuries in these areas are which are common.

Total Immobilization
• Indication:1. Children2. Non-compliant adults3. Patients unable to understand the protocol4. Any contraindication for early mobilization:.Nerve injury repair.Replantation and vascular repair. Fractures with unstable repair.

Immobilization position
• Cast or splint hold the wrist in neutral or slight flexion.
• MCP significantly flexed.• IPJ only slightly flexed or extended.• Splint removed after 3-4 weeks to start active
and passive movement.

Contraindication for mobilization
.Nerve injury
.Replantation and vascular repair
. fractures

Early Controlled Motion
All Early Controlled Motion should minimize edema and allow IPJ extension to prevent joint contracture.
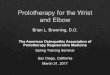
Kleinert & Chow protocol:• a controlled active extension–passive flexion
motion protocol.• The wrist is palmary flexed with a dorsal
protective splint with 30–40° wrist flexion, 50–70° MCP joint flexion, and the IP joints are allowed full extension.

Original Kleinert

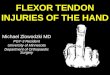
Modified Kleinert regime (Chow)

• Original Kleinert regime had been changed to Modified Kleinert regime (Chow) due to rubber band traction was found to lead to flexion contractures of the finger.
• Modified Kleinert regime (Chow) differ by:1. a palmer bar at the level of the MCP joint as a pulley for
the rubber bands to create greater flexion of both the PIP and DIP joints.
2. the elastic band is detached at night and the fingers are strapped into extension within the splint to minimize the risk of flexion contractures of the fingers.

• All fingers should be included in the rubber band traction to ensure added FDP protection and to promote better tendon excursion also decrease risk of PIP contracture through more efficient action of EDC.
• mobilization program is begun 1 to 3 days postoperatively.
• The finger to be actively extended within the limitations of the splint. The patient is instructed to perform this exercise 10 times every waking hour.

• At 3 weeks, the splint is altered to further extend the metacarpophalangeal joints with the wrist neutral.
• At 4 weeks, the dorsal splint can be removed, leaving the line/rubber band attached to a wristlet. Wrist exercises are encouraged.
• at 5th week, the rubber band is discontinued; the patient actively flexes without resistance.

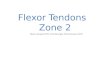
Duran–Houser method
• This is a controlled passive finger flexion protocol without traction of rubber bands.
• dorsal splint is applied with the wrist in 20° flexion, the MCP joint in 50° flexion, and the IP joints are allowed full extension .
Within the first 4-5 weeks, the patients perform:• 10 passive DIP joint extensions with PIP and MCP
joint flexions.• 10 passive PIP joint extensions with MCP and DIP
joint flexions hourly within the splint.

In other word it include:• Full isolated passive flexion of DIP joint.• Full isolated passive flexion of PIP joint.• Full passive flexion of MP, PIP, and DIP joints.


Advantages:• decreased the frequency of PIP joint contracture
seen with Kleinert’s rubber band traction.• Better differential gliding.• Improved protection between exercise time.Disadvantages:• Greater tension on repair site.• Patient may not be able to resist temptation to flex
against volar strap.




Early controlled Active Mobilization
All early active mobilization technique require strong tendon repair at least 4 strand core stitches with strong epitendinous repair.



Early controlled Active Mobilization• Strickland indiana protocol(Controlled “place-and-hold”):• After removal of the surgical bandage, a traditional dorsal blocking
splint that positions the wrist in 20 degrees of palmer flexion, MP joints in 50 degrees of flexion, and IP joints in extension is applied.
• A another tenodesis splint with a wrist hinge is fabricated to allow for full wrist flexion, wrist extension of 30 degrees, and maintenance of MP joint flexion of at least 60 degrees.
• After composite passive digital flexion, the wrist is extended, and passive flexion is maintained. The patient actively maintains digital flexion and holds that position for about 5 seconds. Patients are instructed to use the lightest muscle power necessary to maintain digital flexion.

• This exercise should be repeated fo 25 time per awake hour for 4 weeks.
• After 5 weeks light active flexion with wrist extension commenced.


Early controlled Active Mobilization
• Silfversksold & May:• All fingers are placed in dynamic traction with palmer
bar and the patient use their uninjured hand to ensure complete flexion.
• by post operative day 1 to 3 supervised unassisted active flexion is commenced patient are kept in the hospital for 3 to 4 days .
• PIP joint is actively flexed through about 30° and the DIP joint through 5–10°. In subsequent weeks, the range of active motion is gradually increased.

• there after un assisted active flexion is done only weekly with medical supervision
• active flexion is continued at home in conjunction with passive flexion.
• Active extension is encouraged and interphalangeal joints are held in full extension by volar strap at night.
• After 4 weeks all splints are removed and active flexion and extension are allowed.

Differential gliding exercises

Extrinsic stretching for maximum FDS and FDP glide.

Isolated PIP joint blocking for isolation of FDS contraction.

FDP and FDS blocking exercises.

Resistive exercise

summery




THANK YOU