Embed Size (px)
Citation preview

Brit. 7. Ophthal. ('975) 59, 476
Dark-without-pressure fundus lesions
KRISHAN C. NAGPAL, MORTON F. GOLDBERG, GEORGE ASDOURIAN,MICHAEL GOLDBAUM, AND FELIPE HUAMONTEFrom the Sickle Cell Eye Clinic, University of Illinois Eye and Ear Infirmary, Chicago, Illinois
Geographical grey or white areas in the peripheralretina (Schepens, 1952; Rutnin and Schepens, I967;Karlin and Curtin, I973; Nagpal, Huamonte,Constantaras, Asdourian, Goldberg, and Busse,in press) have been called white-with-pressure orwhite-without-pressure depending on the necessityof scleral indentation for them to be visible. Condonand Serjeant (0972a, I972b) reported mottled brownareas in the retinas of patients with haemoglo-binopathies SS and SC. The purpose of this paperis to report homogeneous, geographical, flat,brown areas in the fundi of black patients and todiscuss the nature and clinical significance of theselesions.
Case reportsCase I, a i6-year-old black youth with haemoglobinSS, was first seen at the Sickle Cell Eye Clinic inFebruary 1973. At initial examination he had a visualacuity of 20120 in both eyes. Slit-lamp examinationshowed a positive conjunctival sickling sign. Fundusexamination showed arteriolar occlusions of the peri-pheral retina at the 6.30 o'clock position in the righteye and at 2.30 o'clock in the left eye. In June 1973fluorescein angiography revealed these vessels to bepatent. In April 1974 the left fundus showed a smalldark brown area at 7.30 o'clock in the midperiphery.It was about I disc diameter in size (Fig. ia) and hadsharply demarcated margins. This lesion appeared flatand was a uniform brown in colour. Fluorescein angio-graphy showed neither blockage of retinal or choroidalfluorescence nor any hyperfluorescence. In August 1974this area was smaller and had faded; in February 1975it had disappeared (Fig. ib). A vitreous examination atthis time with a Goldmann three-mirror contact lensshowed a complete posterior vitreous detachment butwithout shrinkage that is, collapse-of the formedvitreous and no other vitreous abnormalities. Therewere no vitreo-retinal adhesions in the region of thedark brown area.
This study was supported in part by contract NIH 72 2956 B andgrant IP I8 HL I5I68-03 from the National Heart and LungInstitute, Bethesda, Maryland
Address for reprints: Morton F. Goldberg, MD, University ofIllinois Eye and Ear Infirmary, 1855 West Taylor Street, Chicago,Illinois 6o6I2
Case 2, a 25-year-old black man with haemoglobinSS, was first seen in September 1974, and eye examina-tion revealed a visual acuity of 20120 in both eyes and apositive conjunctival sickling sign. Fundus examinationand fluorescein angiography of the right eye showed anoccluded arteriole in the horizontal raphe just temporal tothe macular area. Two black sunbursts were seen at 8and I o'clock at the equator. There was a I i disc diameterbrown area at 2 to 4 o'clock (Fig. 2a) in the midperi-phery. The anterior margin was straight; the verticallyoriented posterior margin had a dentate border. Fluo-rescein angiography of this brown area was normal.In November 1974 this area was smaller (Fig. 2b), andthe anterior margin had also become irregular. At12.30 o'clock another brown area j disc diameter insize and oval in shape was found. Vitreous examinationwith Goldmann three-mirror contact lens showedcomplete, shallow, posterior vitreous detachment with-out collapse, including the brown areas. The vitreousbase remained attached.
Case 3, a 56-year-old black man with haemoglobinSC, was seen in March 1974. Eye examination showed noanterior segment abnormality. The visual acuity was20120 in both eyes. Fundus examination of the right eyeshowed peripheral retinal neovascularization (sea fans)at 8, 9, and 4 o'clock and black sunbursts at 1.30 and 3o'clock in the equatorial region. A dark brown area 3disc diameters above and nasal to the disc was about21 disc diameters wide (Fig. 3), with irregular margins
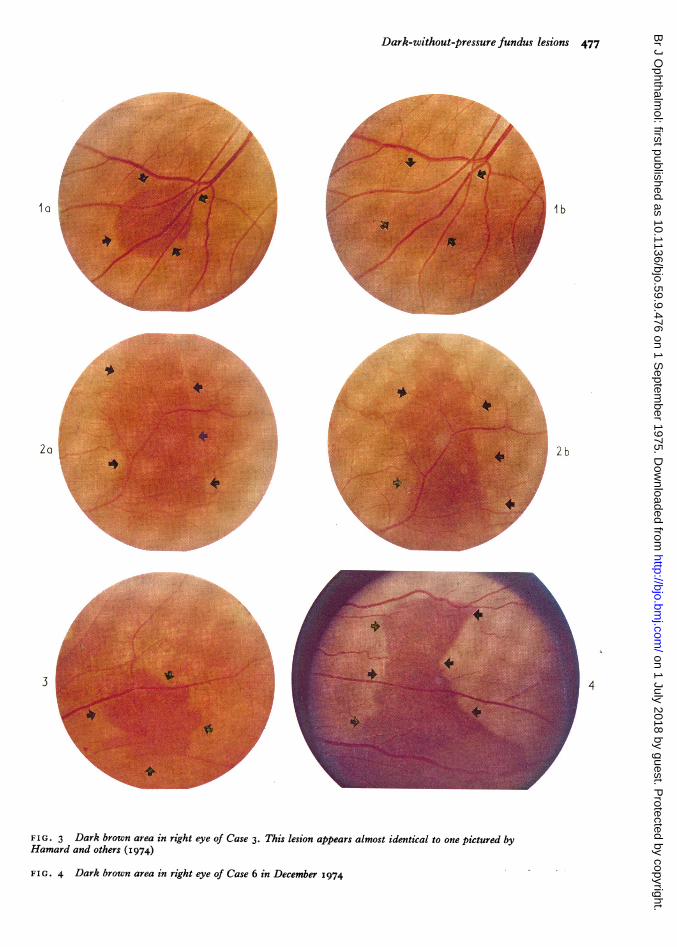
FIG. ia Dark brown area (arrows) of uniform colour inApril 1974 in left eye of Case i. Note crossing of retinalvessels and absence of mottling
FIG. ib Same area in February 1975. Dark brown areais completely gone. Arrows indicate margins of previousdark-without-pressure
FIG. 2a Dark brown area in right eye of Case 2 inSeptember 1974. Anterior margin is straight (arrows) andposterior margin dentate (arrows). Note crossing of retinalvessels and absence of mottling
FIG. 2b Same area in November I974. Note irregularanterior margins (arrows) as compared with straightmargin (arrows) in A. Posterior margin has also changed
on 1 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.9.476 on 1 Septem
ber 1975. Dow
nloaded from
Dark-without-pressure fundus lesions 477
l I bi
2 2~~~~~~~~~~~~~~~~~~~~~~b
34
FIG. 3 Dark brown area in right eye of Case 3. This lesion appears almost identical to one pictured byHamard and others (I974)
FIG. 4 Dark brown area in right eye of Case 6 in December 1974
on 1 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.9.476 on 1 Septem
ber 1975. Dow
nloaded from

478 British Journal of Ophthalmology
and a flat appearance. Fluorescein angiography showednormal circulation and fluorescence. Examination ofthe left eye showed an area of retinal neovascularizationat 3 o'clock and a large black sunburst extending from5 to 6 o'clock. Areas of retinal neovascularization were
successfully treated by argon laser photocoagulation.Follow-up examination of the dark brown area 8 monthslater showed that it was smaller and had faded to lightbrown. Vitreous examination at this time with theGoldmann three-mirror contact lens showed completeposterior vitreous detachment without collapse. Overand around the dark brown area, the vitreous body was
also attached.
Case 4, a 14-year-old black girl with haemoglobinSC, was seen in December 1974. Ocular examinationshowed a visual acuity of 20120 in both eyes. Fundusexamination of the right eye showed a black sunburst atI0 o'clock in the equatorial region, a few scattered smalliridescent spots in the fundus periphery, and a arkbrown area at 2 o'clock in the midperiphery. It was
flat, horizontally orientated, about 2 disc diameters longand I disc diameter wide, and had irregular but sharplyoutlined margins. Iridescent spots just outside theposterior edge were similar to the haemosiderin-ladenmacrophages in a resolving salmon patch. The surfaceof this brown area was smooth with no granularity.Fluorescein angiography of this brown area showednormal perfusion. The area of the old salmon patch atits posterior edge showed possible occlusion of a smallprecapillary arteriole with faint blockage of choroidalfluorescence. One month later the dark brown area was
smaller and had faded. The vitreous showed flat posteriorvitreous detachment involving the entire fundus inaddition to the region of the brown area.
Case 5, a 26-year-old black woman with SShaemoglobin, was seen in April 1974. The visual acuitywas 20120 in both eyes. Slit-lamp examination of theconjunctiva showed a positive conjunctival sickling sign.Fundus examination of the right eye showed occlusionof retinal arterioles in the equatorial region in severalareas. The left eye showed similar changes in the retinalperiphery and a small oval, dark brown area (i discdiameter) at 9.30 o'clock in the midperiphery. Fluores-cein angiography of this area was normal. In December1974 the right fundus had developed a small soft exudateabove the foveal area. In both eyes the peripheral retinalarterioles showed the spontaneous remodelling patterndescribed by Galinos, Asdourian, Woolf, Stevens, Lee,Goldberg, Chow, and Busse (I975). In February I975the dark brown area in the left eye had faded. Fluoresceinangiography showed that this area appeared normal. Thevitreous examination in February 1975 with the Gold-mann three-mirror contact lens was normal. There was
no vitreous detachment, collapse, or shrinkage.
Case 6, a 12-year-old black girl with haemoglobinSS and a history of cerebrovascular accident, was seen
in November I974. Her visual acuity was 20120 in botheyes. Fundus examination showed several areas of peri-pheral arteriolar occlusion in both eyes. The right eye
showed a flat dark brown area (Fig. 4), about 2 discdiameters nasal to the disc, extending from 2.30 to
5.30 o'clock. Its width varied from I to 3 disc diameters
and it had irregular but sharply demarcated margins.The rest of the retina had a normal appearance. Fluores-cein angiography showed normal circulation. The lefteye also showed peripheral arteriolar occlusions and adark brown area extending from 7 to io o'clock 2 discdiameters nasal to the disc. It was flat and 3 to 5 discdiameters wide. The distinct margins were surroundedby normal retina. Fluorescein angiography showednormal retinal circulation and normal choroidal fluo-rescence. The vitreous examination was normal in botheyes, showing no vitreous detachment or vitreouscollapse.
Case 7, a 46-year-old hypertensive black woman,was examined in January 1975. Her systemic bloodpressure reading was 2201120 mm Hg. Haemoglobinelectrophoresis showed haemoglobin AA. Fundusexamination revealed mild generalized narrowing ofretinal arterioles and a few linear flame-shaped hae-morrhages. In the right eye 2 disc diameters below thedisc there were two dark brown areas which were flat,irregular, and clearly demarcated. The surroundingretina was normal. Fluorescein angiography showednormal retinal circulation. Except for attachment to thedisc and vitreous base, the vitreous was shallowlydetached without collapse. No vitreo-retinal adhesionswere seen over this brown area or surrounding theretina.
Discussion
The lesions described by Condon and Serjeant(0972a, I972b) occurred in patients with homozy-gous sickle cell disease and haemoglobin SC.These areas were characterized as having a mottledbrown surface surrounded by a halo of pale retina.They were often associated with copper-coloured,iridescent, glistening spots. Fluorescein angiog-raphy showed normal circulation in these areas,but adjacent areas showed arteriolar occlusivedisease. They suggested that the mottled brownareas represented the sequelae of deep subretinalhaemorrhages. Okun (I969) showed a chorio-retinal scar surrounded by a brown area developingfrom a salmon patch in a patient with sickle celldisease. The lesions reported by Condon andSerjeant (1972a, 1972b) and Okun (I969) probablyrepresent sequelae of salmon patch haemorrhagesthat dissected deeply into the retina and into thesubretinal space-that is, they probably representedearly stages of black sunbursts.We have seen seven patients with brown lesions
(four with haemoglobin SS, two with haemoglobinSC, and one with hypertension and haemoglobinAA) of the fundus that had uniform colour withoutany mottling. These areas appeared to be unre-lated to the residue of salmon patches such asschisis cavities, iridescent spots, or sunburstlesions. These flat lesions varied in size from i toseveral disc diameters. Some had regular, round,or straight margins; whereas others had irregular,
on 1 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.9.476 on 1 Septem
ber 1975. Dow
nloaded from

Dark-without-pressure fiundus lesions 479
serrated, or dentate margins. Location and orien-tation of these lesions also varied. The lesions wesaw were located near the posterior pole or in themidperiphery. They were orientated either radiallyor circumferentially. Most of the lesions weretransient, and when followed-up for weeks tomonths, changed shape and sometimes disappearedcompletely. Fluorescein angiography in our patientsdid not reveal any vascular abnormalities in theseareas, although Case 4 showed occlusion of a smallprecapillary arteriole posterior to the brown area.Our cases resembled one pictured by Hamard,Coquelet, Jaeger, Malmejac, and Mondon (1974)which they identified as a salmon patch. We do notfeel that the lesion shown by these authors repre-sented a salmon patch, because salmon patches arebright red (later yellow), much smaller, and usuallycover retinal vessels. This lesion appeared severaldisc diameters in size and had a brown homogeneouscolour with normal overlying retinal vessels. Un-fortunately, no fluorescein angiogram of thislesion was presented. These dark-without-pressureareas cannot be related to preretinal, intraretinal,subretinal, or choroidal haemorrhages becausenormal choroid is visible in these dark areas byophthalmoscopy and fluorescein angiography.The dark brown areas may represent an island of
normal fundus surrounded by extensive white-without-pressure changes. However, some of theselesions are very small, representing only about zto 5 per cent of the total retinal surface; white-without-pressure lesions involving 95 to 98 percent of the retina appear to be only a remotepossibility. These dark brown areas, how-ever, are comparable in some respects to areasof white-without-pressure. Like white-without-pressure, they are flat, vary in shape, and can occurin numerous locations throughout the eye. Thewhite-without-pressure lesion has been noted tobe migratory in nature and can disappear withpassage of time (Nagpal and others, in press).Similarly, dark-without-pressure lesions are migra-tory and can also fade in time. Both can be seen in
the fundus without any scleral indentation. Welabelled these brown lesions as dark-without-pressure, because, like white-without-pressure,they do not need scleral indentation to be seenand are analogous to white-without-pressure lesionsin the aspects noted above.There are several differentiating features. The
white-without-pressure lesions are white or grey;they occur mostly in the equatorial region or peri-pheral to the equator and, according to our previousobservations (Nagpal and others, in press), representchanging vitreo-retinal adhesions. In contrast,dark-without-pressure lesions are brown and occurmost commonly near the posterior pole or in themidperiphery. The status of the vitreous appearsto be unrelated to the presence of the dark areas. Inthree of our patients the vitreous was normal, and infour patients there was shallow detachment of thevitreous without liquefaction, shrinkage, or collapse.These dark brown lesions may represent subtle
changes or an altered reflex in the pigment epithe-lium in the internal limiting membrane of theretina, or in other anatomical regions of the fundus.The factors leading to these changes are not known.Future histopathological examination may helpidentify the nature of these lesions.
SummarySeven black patients had dark brown homogeneousgeographical areas of the fundus. Six cases wereassociated with sickle cell haemoglobinopathiesand one was associated with systemic hypertension.These flat lesions were uniform in colour andoccurred in the posterior pole or in the midperi-phery. They appeared to be transient and oftendisappeared leaving no residue. The cause isunknown. By analogy with white-without-pressurefundus lesions, we have called these areas dark-without-pressure.
We thank Lee Jampol, MD, for referring Case 7,Jane Lantz for editing the manuscript, and BarbaraDombkowski for secretarial assistance.
ReferencesCONDON, P. I., and SERGEANT, G. R. (1972a) Amer. J3. Ophthal., 73, 533
, and (1972b) Ibid., 74, 921GALINOS, S. O., ASDOURIAN, G. K., WOOLF, M. B., STEVENS, T. s., LEE, C.-B., GOLDBERG, M. F., CHOW, J. C. F., and
BUSSE, B. (I975) Ibid., 79, 853HAMARD, H., COQUELET, M. L., JAEGER, G., MALMEJAC, N., and MONDON, N. (1974) Arch. Ophtal. (Paris), 34, 5KARLIN, B., and CURTIN, B. J. (1973) In 'Retina Congress', ed. R. C. Pruett and C. D. J. Reagan, p. 629. Appleton-
Century-Crofts, New YorkNAGPAL, K. C., HUAMONTE, F., CONSTANTARAS, A., ASDOURIAN, G. K., GOLDBERG, M. F., and BUSSE, B. Arch. Ophthal.
(Chicago) (in press)OKUN, E. (I969) Docum. ophthal. (Den Haag), 26, 574RUTNIN, u., and SCHEPENS, C. L. (I967) Amer. J. Ophthal., 64, IO63SCHEPENS, C. L. (1952) Arch. Ophthal. (Chicago), 47, 593
on 1 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.9.476 on 1 Septem
ber 1975. Dow
nloaded from





























