Embed Size (px)
DESCRIPTION
Peripheral fundus & its disorders
Citation preview

Peripheral fundus & its disordersPresented by Dr Rohit Rao

References
•Peripheral Ocular Fundus 3rd edition by William L. Jones
•Ophthalmology 3rd edition.by Yanoff, Duker
•Clinical ophthalmology 7th Edition - Jack Kanski
•Wolff's Anatomy of the Eye and Orbit 8th by Bron, Tripathi.
•Retina by Stephen.J .Ryan

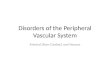
Retina
Optic DiscArea
Centralis Perifove
al
Parafoveal
Fovea
Foveola
Peripheral Retina
Ora Serrata

Periphera RetinaNear Periphery: 1.5mm Around
Area Centralis
Mid Periphery: 3mm Wide Zone Around Near Periphery
Far Periphery: Extendes From Optic Dics,
9-10mm Temoprally & 16mm Nasally

TN

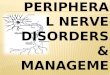
Pars plana
•Ciliary body starts 1 mm from the limbus and extends posteriorly for about 6 mm.
•First 2 mm pars plicata and 4 mm pars plana.
•Width is about 4.0-4.5 mm.

Vitreous base
•Vitreous base is a 3–4 mm wide zone straddling the ora serrata.
•Vitreous is strongly attached at base, so that following PVD, posterior hyaloids face remains intact.
•Pre-existing retinal holes within the vitreous base do not lead to RD.
•Severe blunt trauma may cause tearing of non-pigmented epithelium of pars plana & of retina.


Ora Serrata
•Retina becomes opalescent and often is marked by small rows of cystoid cavities.
•Extensive cystoid changes do not represent pathology.
•Neural retina stops abruptly at ora serrata and is continued by nonpigmented ciliary epithelium
•Pars plana is more deeply pigmented, so choroidal pattern not seen.


TN
0.7-0.8 mm
2.1 mm
6.0 mm 7.0 mm
7.0 mm
7.0 mm
TN

•Dentate processes are teeth-like extensions of retina onto the pars plana.
•Oral bays are the scalloped edges of the pars plana epithelium in between the dentate processes.
•Enclosed oral bay is a small island of pars plana surrounded by retina as a result of meeting of two adjacent dentate processes.▫Not be mistaken for a retinal hole
•Granular tissue characterized by multiple white opacities within the vitreous base ▫Can be mistaken for small peripheral
opercula.

Granular tissue
Enclosed oral bay

Meridional fold•Small radial fold of thickened retinal tissue
in line with a dentate process, • It bigns at ora serrata and runs posteriorly &
perpendicularly to it in a meridional fashion•Superonasal quadrant . •Small retinal hole at its apex•Found in approximately 20% of all eyes•Meridional complex is composed of an
enlarged dentate and ciliary process associated with a meridional fold

•Vitreous traction on meridional folds and complexes may result in the formation of retinal breaks.
•Meridional folds are not a common cause of RD, may be because these are found at vitreous base.
•Because of anterior location , cryopexy is preferred for an associated retinal break.


Pars plana cyst• Pars plana cysts are clear cystoid spaces
between the pigmented and nonpigmented epithelia.
• Scleral depression• Fluid contains hyaluronic acid.• Mostly acquired; few are congenital.• idiopathic or secondary to ocular disease.
▫Retinal detachment, may be the result of traction by the shrinking vitreous base.
▫Posterior uveitis.▫Multiple myeloma


Congenital Hypertrophy of the Retinal Pigment Epithelium•Common benign lesion. •Congenital and not a degenerative
condition.•Flat round or oval lesion, well defined,
dark grey or black in colour and up to three disc diameters in size.
•Outer retina change and does not affect the vitreo-retinal interface; so does not predispose to RD.
•Can lose pigment over time

•When occur in groups, known as bear track, Familial Adenomatous Polyposis.



Pavingstone(Cobblestone degeneration or Chorioretinal Atrophy)•25% of the population•Well defined yellow white patches
between the equator and the ora serrata.•Absence of the outer layers of the retina,
in particular the choroid, which permits an uninterrupted view of the sclera.
•Congenital and not be considered a degeneration.
•No predisposition to break formation



Microcystoid degeneration
•Tiny vesicles with indistinct boundaries. •Always starts adjacent to ora serrata and
extends circumferentially and posteriorly with a smooth undulating posterior border.
•Present in all adult eyes,•Increasing in severity with age•Although it may give rise to retinoschisis.•Do not give rise to RD


Honeycomb (reticular) degeneration•Age-related change •Fine network of
perivascular pigmentation which may extend posterior to equator.
•Caused by RPE degeneration
•More prominent in nasal quadrant

Snowflake Vitreoretinal Degeneration•Snowflake vitreoretinal degeneration
appears as tiny yellow-white spots in the far peripheral retina
•Superior temporal quadrant•Lattice degeneration •Vitreous shows fibrillar degeneration &
liquefaction.


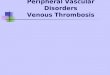
Lattice degeneration
•An Area with Absence of ILM• Overlying Area of Liquefied Vitreous•Condensation & Adherence of Vit Gel•Inner Retinal Layer Atrophy•More common superiorly•Arranged parallel to the ora serrata.•Incidence- 8% to 10%•RRD :: Lattice account for 20%•Symmetric and bilateral,•Horse shoe Tears &Atrophic holes



Complications
(A) Atypical radial lattice without breaks;
(B) U-tears(C) Linear
tear along posterior margin.
(D) multiple small holes within islands of lattice

Management of Lattice Degeneration•Lattice without Retinal Breaks - No Rx•Lattice with Atrophic Holes - No Rx•Lattice + Holes+ Sub clinical RD – Treat•Lattice+ Traction Tear - Treat : If Fellow
eye has RD,Strong Family History of RD,Aphakic Eyes
•Asymptomatic Traction Tear - No Rx•Acute Symptomatic Tears - Treat in
Phakics & Aphakics

Vitreoretinal Tufts
•Small Peripheral Retinal Elevation•Focal Vitreous Traction•Operculated or flap tears when strong
vitreous traction is applied•Rarely cause retinal detachments.•Treatment is rarely indicated•Cryopexy or photocoagulation.


Snailtrack degeneration
•Snailtrack degeneration is characterized by sharply demarcated bands of tightly packed ‘snowflakes’ which give the peripheral retina a white frost-like appearance.
•Longer than in lattice degeneration •Overlying vitreous liquefaction.


Degenerative retinoschisis
• 5% of the population over the age of 20 years and is particularly prevalent in hypermetropes.
•Bilateral •Coalescence of cystic lesions•Results in separation or splitting of the NSR
into an inner (vitreous) layer and an outer (choroidal).

•Typical retinoschisis split is in outer plexiform layer,
•Reticular retinoschisis, less common, splitting occurs at level of NFL.
•Early retinoschisis seen in inferotemporal with a smooth immobile elevation of retina.
•Progress circumferentially•Snowflakes , sheathing or ‘silver-wiring’ of
blood vessels.•Microaneurysms and small telangiectases , •Complications are very rare, •Breaks, RD in the presence of PVD, Vitreous
haemorrhage



White with pressure
•Translucent grey appearance of the retina, induced by indention.
•It does not move when indenter is moved. •Normal eyes and may have abnormally
strong vitreous attachment.•It is also observed along the posterior
border of islands of lattice degeneration, snailtrack degeneration and the outer layer of acquired retinoschisis.


White without pressure• Has the same appearance but is present without scleral
indentation.• May be mistaken for a flat retinal hole.• Giant tears occasionally develop along the posterior
border of ‘white without pressure’. • For this reason, if ‘white without pressure’ is found in the
fellow eye of a patient with a spontaneous giant retinal tear, prophylactic therapy should be performed.
• It is advisable to treat all fellow eyes of non-traumatic giant retinal tears prophylactically by 360° cryotherapy or indirect argon laser photocoagulation, irrespective of the presence of ‘white without pressure’, if they have not developed a PVD.


TREATMENT• Upon the discovery of a retinal break, the initial
decision is whether the benefits of treatment (to prevent retinal detachment) outweigh the risks and cost of treatment
• The factors under consideration in each case include ▫ Presence or absence of symptoms; ▫ Age and systemic health of the patient;▫ Refractive error of the eye;▫ Location, age, type, and size of the break;▫ Status of the fellow eye;▫ Whether the patient is aphakic, pseudophakic, or will soon
undergo cataract surgery

•Retinopexy•Cryopexy and laser photocoagulation. •Cryotherapy
▫Delivered transconjunctivally.▫It destroys the choriocapillaris, RPE, and outer
retina to provide a chorioretinal adhesion ▫It is not immediate; 1 week for partial adhesion
and up to 3 weeks for the complete.•Laser photocoagulation
▫Argon green, argon blue-green, krypton red, or diode laser.
▫Slit lamp and the indirect ophthalmoscope.
▫Instant, but maximal adhesion occurs 7–10 days later.

•Cryopexy has the advantage of not requiring clear media
•In general, retinal cryopexy and indirect ophthalmoscopic laser photocoagulation are preferred for anterior retinal breaks
•Similarly, posterior breaks managed with the slit lamp or an indirect laser delivery system.
•Retinal tear with persistent traction and recurrent vitreous Hemorrhage requires scleral buckling or vitrectomy

Cryopexy • Indirect ophthalmoscopic visualization, • Cryoprobe is placed on the conjunctiva that
overlies the break until the retina adjacent to the tear becomes gray-white.
• Approximately 2 mm of retinal whitening around the entire break
• Multiple applications are placed until the break is surrounded completely with confluent treatment.
• Do not to treat the choroid and RPE directly beneath the break, can lead to macular pucker and proliferative vitreoretinopathy.

Photocoagulation •Goldmann three-mirror lens or
panfundoscope lens with the slit-lamp delivery system.
•Tear should be surrounded completely by three to four rows of laser burns.
•Settings are 200–500 mm spot size and 0.1–0.2 seconds
•Indirect laser delivery system can also be used
•Advantage is simultaneous scleral depression allows treatment of anterior tears and even dialysis.

Thank you