Embed Size (px)
Citation preview

D R . E R I C A L . W E I N B E R G
D E C E M B E R 2 0 1 7

COPYRIGHT © 2017 BY SEA COURSES INC.
All rights reserved. No part of this document may be reproduced, copied, stored, or
transmitted in any form or by any means – graphic, electronic, or mechanical, including
photocopying, recording, or information storage and retrieval systems without prior
written permission of Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials,
acts or omissions.

CONFLICT OF INTEREST DISCLOSURE
Presenter/Faculty: Dr. Erica L. Weinberg
Relationships with Commercial Interests:
Grants/research support: none
Speaker bureau/honoraria: Sea Courses
Consulting fees: none
Other: none

POTENTIAL FOR CONFLICT OF INTEREST
I have been a member of the National Faculty at the Michael G. Degroote
National Pain Centre since 2012
I am one of the many authors on the Canadian Pain society’s revised
consensus statement on the pharmacological management of chronic
neuropathic pain

I have been a Medical Inspector
(MI) / Independent Opinion (IO)
Provider at the College of
Physicians and Surgeons of
Ontario (CPSO, ‘College’) –
frequently regarding opioid
prescribing practices

MITIGATING POTENTIAL BIAS
Information presented or recommendations made are
evidence/guideline/consensus-based
I have completed the CPFC Mainpro+/Cert+ Declaration of Conflict of
Interest form evidencing compliance with Mainpro+/Cert+ requirements,
a requisite for this program to be given accredited status
I will be discussing “off-label” uses of medications

HOW DOES THE COLLEGE GET THE CASES
Complaints/concerns from colleagues, patients, families, pharmacists,
coroners …
Narcotic Monitoring System (NMS) / Prescription Monitoring Program (PMP)
- Ontario NMS (May 2012)
▪ Limited list of drugs; most doctors do not have own access
▪ eHealth Ontario pilot project (digital health drug repository) = Guelph, ON
▪ Expected all doctors to have access by the end of 2017

WHAT DO I LOOK FOR WHEN ASSESSING THE
MANAGEMENT OF PAIN?
1. Organized approach to diagnosing the pain
2. Patient Engagement
3. Multimodal approach to the treatment
4. Rational prescribing
5. Therapies are being monitored
6. Meets the standard of practice of the profession
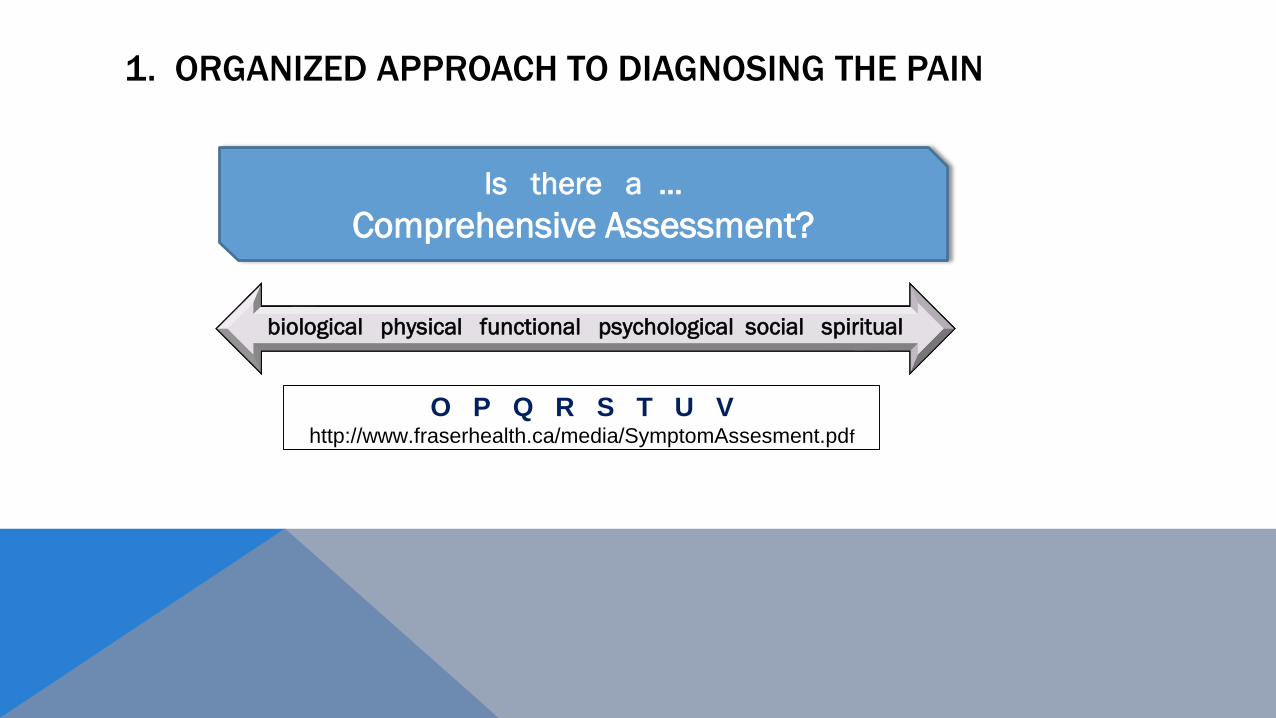
1. ORGANIZED APPROACH TO DIAGNOSING THE PAIN
biological physical functional psychological social spiritual
O P Q R S T U Vhttp://www.fraserhealth.ca/media/SymptomAssesment.pdf
Is there a …
Comprehensive Assessment?
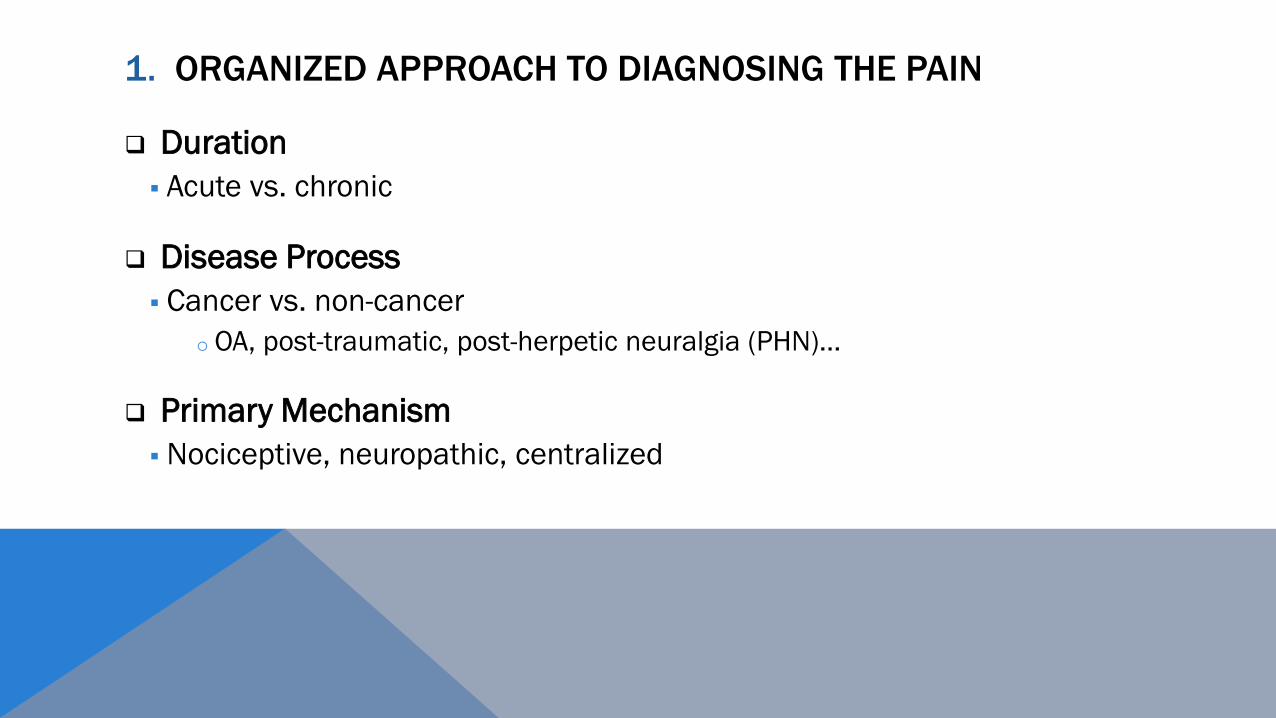
1. ORGANIZED APPROACH TO DIAGNOSING THE PAIN
Duration
▪ Acute vs. chronic
Disease Process
▪ Cancer vs. non-cancer
o OA, post-traumatic, post-herpetic neuralgia (PHN)…
Primary Mechanism
▪ Nociceptive, neuropathic, centralized

MECHANISTIC CHARACTERIZATI0N OF PAIN
NOCICEPTIVE NEUROPATHIC CENTRALIZED
Inflammation or
mechanical damage in
tissues
May respond to:
✓ NSAIDs
✓ Opioids
✓ Non-pharmacological,
CAM and procedures
Classic examples:
Acute injury pain, OA, RA
Damage or dysfunction within the nervous
system
May respond to:
✓ Peripheral agents
✓ Central agents
✓ Non-pharmacological, CAM and procedures
Classic examples:
DPNP, PHN
Primarily due to a
central disturbance in
pain processing
May respond to:
✓ Central agents
✓ Non-pharmacological,
CAM and procedures
Classic examples:
FM, IBS, TMJD
OA = osteoarthritis; RA = rheumatoid arthritis; DPNP = diabetic peripheral neuropathic pain; PHN = post-herpetic neuralgia; FM = fibromyalgia
IBS = irritable bowel syndrome; TMJD – temporal mandibular joint disease

MECHANISTIC CHARACTERIZATI0N OF PAIN
NOCICEPTIVE NEUROPATHIC CENTRALIZED
Inflammation or
mechanical damage in
tissues
May respond to:
✓ NSAIDs
✓ Opioids
✓ Non-pharmacological,
CAM and procedures
Classic examples:
Acute injury pain, OA, RA
Damage or dysfunction within the nervous
system
May respond to:
✓ Peripheral agents
✓ Central agents
✓ Non-pharmacological, CAM and procedures
Classic examples:
DPNP, PHN
Primarily due to a
central disturbance in
pain processing
May respond to:
✓ Central agents
✓ Non-pharmacological,
CAM and procedures
Classic examples:
FM, IBS, TMJD
OA = osteoarthritis; RA = rheumatoid arthritis; DPNP = diabetic peripheral neuropathic pain; PHN = post-herpetic neuralgia; FM = fibromyalgia
IBS = irritable bowel syndrome; TMJD – temporal mandibular joint disease

How do you measure pain?

MEASURING PAIN
Pain interference
o Function (recreation & work) and disability
o Sleep
Pain intensity
Mood
Other co-morbid psycho/social/spiritual issues
Risks
Goals and Expectations

2. IS THE PATIENT ENGAGED IN THE PLAN?

GOALS AND EXPECTATIONS OF TREATMENT
Improved Quality of Life
Improvement in function and reduction in disability
Patient SMARTIE goals
Reduction of pain
Tolerable pain score
Minimizing risks
Is the patient reliable enough?o Attending all appointmentso Participating in all recommended therapieso Participating fully in the minimizing risk plan
3. MULTIMODAL TREATMENT OF PAIN

3. THE 3 M’ OF PAIN MANAGEMENTS
Mind Movement Medicine

TENS-Acupuncture
Deep Massage
Trigger Points …
Relaxation
Exercise
Cognitive Therapies
Chewing Gum
Religious Beliefs …
TENS-conventional
Massage …
2
1
3
Hot
Cold
Massage
Dorsal Horn
Brain Stem
Cortex
Mechanism-based Treatment:
Non-Pharmacological
Therapies

TCA
SNRI
NRI
Opioid …
TCA
SNRI
NRI
Opioid …
Gabapentinoid
Antiepileptic/convulsant
NMDA Antagonist
Opioid
TCA
Cannabinoid …
2
1
3
NSAID
COXIB
Steroid
Capsaicin
Cortex
Brain Stem
Dorsal Horn
Mechanism-based Treatment:
Pharmacological
Therapies

4. IS THERE EVIDENCE OF RATIONAL PRESCRIBING?
Nociceptive Neuropathic Centralized
NSAIDs + - -
Opioids + + -
TCA + + +
SNRI + + +
Gabapentinoids - + +
Cannabinoids - + ?
Surgery / Injections + + -
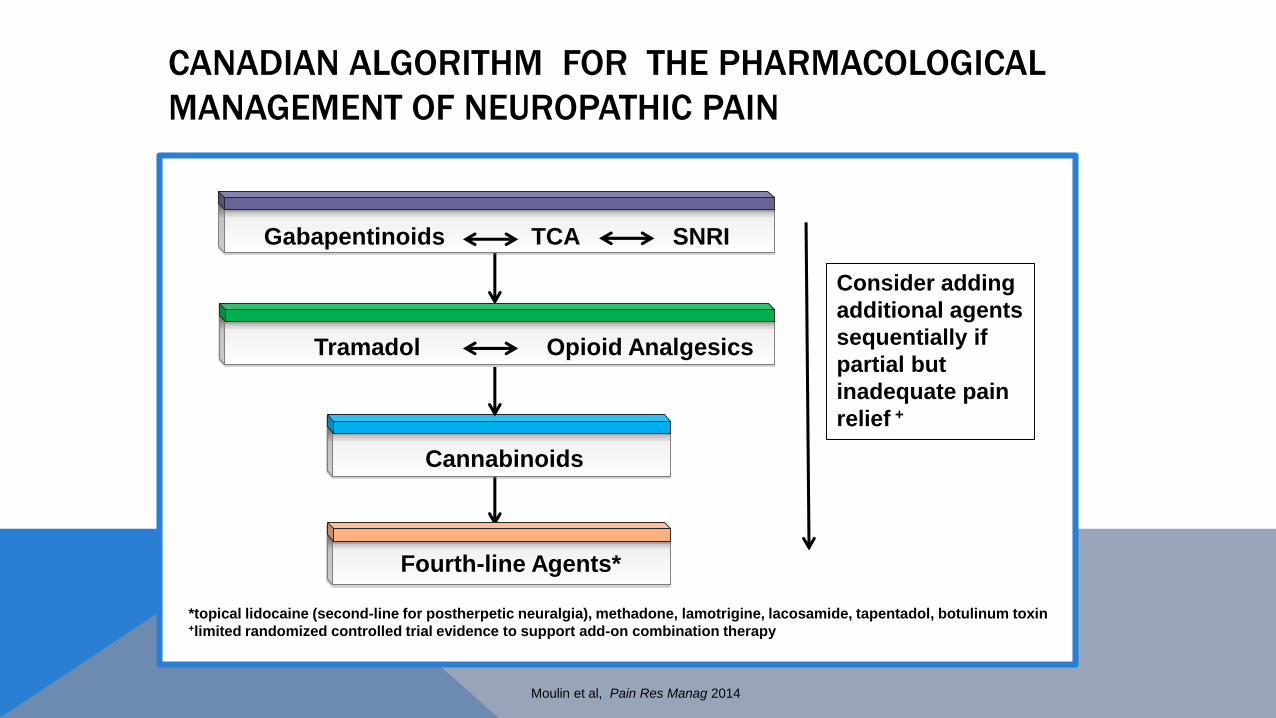
*topical lidocaine (second-line for postherpetic neuralgia), methadone, lamotrigine, lacosamide, tapentadol, botulinum toxin +limited randomized controlled trial evidence to support add-on combination therapy
CANADIAN ALGORITHM FOR THE PHARMACOLOGICAL
MANAGEMENT OF NEUROPATHIC PAIN
Consider adding
additional agents
sequentially if
partial but
inadequate pain
relief +
Gabapentinoids TCA SNRI
Tramadol Opioid Analgesics
Cannabinoids
Fourth-line Agents*
Moulin et al, Pain Res Manag 2014

5. IS THERE EVIDENCE THAT THERAPY IS BEING MONITORED?
Managing Risk – ALL therapies
“Doctors have to be risk managers in any medical
condition. In treating pain, there is no risk-free
treatment option – including doing nothing.”
S. Fishman ICPCD New York, 2007

5. IS THERE EVIDENCE THAT THERAPY IS BEING MONITORED?
Monitoring Pain
Pain interference
▪ Function, disability, sleep, relations …
Pain intensity
Periodic focused physical exams
Managing Mental Health Disorders
Depression, anxiety, PTSD, SUD/OUD …
Whole Person Approach
Other co-morbid bio/psycho/social/spiritual issues
Involvement of other Health Care Professionals

5. IS THERE EVIDENCE THAT THERAPY IS BEING MONITORED?
Managing Risk - Opioids:
Opioid misuse screening tools/CAGE-AID, NMS/PMP, UDS, circle of care, structured opioid therapy/limiting supply, opioid treatment agreements …
Consultations, collaboration and periodic reassessment
Monitoring adverse effects, medical complications, risks, ADRBs …
Accurate Medication Record
Stopping/tapering therapy if goals are not met or risks outweigh benefits
ADRB=aberrant drug-related behaviour; UDS=urine drug screen
6. STANDARD OF PRACTICE OF THE PROFESSION
What is standard of care?
6. STANDARD OF PRACTICE OF THE PROFESSION
What do most doctors do?
What does the evidence-based, peer reviewed literature say to do in
the given circumstances?
What would you teach trainees to do in the given circumstances?
What would an ethical doctor do in those circumstances?
What does your College say to do?
2018
2012
2006

6. DOES PRESCRIBING MEET THE STANDARD OF CARE?
Good practices in prescribing Non-pharmacological/non-opioid therapies optimized
Previous/concurrent SUD/OUD and active mental health conditions verified and documented
Accepted indication for opioids in specific pain condition
Informed consent
Factors impairing cognition/psychomotor ability addressed
All Rx and ‘renewals’ are documented
Appropriate action taken when
UDS results are inconsistent or unexpected, ADRBs are identified, Opioid Treatment Agreement
is violated …
Goals are not achieved and/or risks outweigh benefits
6. STANDARD OF PRACTICE OF THE PROFESSION

C D C G U I D E L I N E F O R P R E S C R I B I N G
O P I O I D S F O R C H R O N I C P A I N ( 2 0 1 6 )
✓ Age ≥18 years
✓ Chronic non-cancer pain (CNCP)
✓ 10 Recommendations (PCP, pain specialists, NPs, Regulatory Agencies, Policy Makers)
✓ 3 Good Practice + 10 Expert Guidance Statements
✓ Optimize non-opioid/non-pharmacological Rx
✓ Active SUD, active MH disorder, Hx SUD = non-opioid
✓ Start ORAL; IR or CR ≤ 50 MED; keep <90 MED or refer
✓Initiation, titration and monitoring of response
✓Discontinuation if ….
✓ Patients currently on ≥ 90 MED
✓ Challenges with problematic pain, AEs, tapering
✓ Good Practice: informed consent, monitoring, contraindications/exchange of information
✓ Expert Guidance: amounts prescribed, IR/CR, co- prescribing, sleep apnea, hypogonadism, urine drug screening, treatment agreements, tamper-resistant formulations, patch exchange, naloxone
T H E 2 0 1 7 C A N A D I A N G U I D E L I N E F O R
O P I O I D S F O R C H R O N I C N O N - C A N C E R P A I N
✓ Age ≥18 years
✓ Chronic pain outside of active cancer treatment,
palliative care and end-of-life care
✓ 12 recommendations (PCP/Internists)
✓ Non-pharmacological, non-opioid Rx preferred
✓ What to do before starting opioids and periodically
during opioid therapy: goals, R/B
✓ Start with IR opioids ≤ 50 MME; avoid ≥ 90 MME /justify
✓ Re-evaluation
✓ Acute pain
✓ Re-evaluation for risk of harm, PMP, UDT, BNZ
✓ Evidence-based Rx for OUD

Available at: https://thewellhealth.ca/wp-content/uploads/2017/03/CEP_CNCP_Main_V1.pdf

UPON COMPLETION, PARTICIPANTS
WILL BE ABLE TO:
List useful tools from the Canadian
Guideline for Safe and Effective Use of
Opioids for Chronic Non-Cancer Pain
Identify tips and risk management strategies that can be
used to avoid regulatory attention from the CPSO when
treating patients with chronic pain
Manage chronic pain more effectively and safely in their
practice

AFTER THIS SESSION, PARTICIPANTS WILL BE ABLE TO:
Identify tips and risk management strategies that can be used to avoid
regulatory attention from their College when treating patients with pain
Manage pain more effectively and safely in their practice



“The stories you are about to hear are true; only the
names (and other identifying details) have been
changed to protect the innocent”

CASE 1: ACUTE PAIN
26 y.o. Patient since age 3
What would you do?
Wiped out on dirt bike 3 weeks prior
• Splint and crutches from ER
• Knee still sore
• “On acetaO and Morphine from a friend”
acetaO = acetaminophen 325 mg/oxycodone 5 mg

CASE 1: ACUTE PAIN
26 y.o. Patient since age 3
Rx acetaO M:30
Wiped out on dirt bike 3 weeks prior
• Splint and crutches from ER
• Knee still sore
• “On acetaO and Morphine from a friend”
acetaO = acetaminophen 325 mg/oxycodone 5 mg


CDC, BC, Yukon

NEW MEASURES TO INFORM CANADIANS OF THE RISKS OF PRESCRIPTION OPIOIDS
June 16, 2017 - Ottawa, ON - Health Canada
Canada is facing an opioid crisis. Overdoses related to opioids are claiming the lives of thousands of Canadians of all ages, and from all walks of life. Some who have become dependent on prescription drugs were not even aware that the drugs they had taken contained opioids. Patients receiving prescription opioids need a clear understanding of the risks associated with these drugs, so they can make informed decisions about how to use them as safely as possible or whether to use them at all.
As part of the Government of Canada’s work to reduce problematic opioid use and its related harms, Health Canada is proposing regulations that would make a
warning sticker and patient information handout mandatory with all prescription opioids at the time of sale. This means that no matter where patients and families across Canada fill their prescriptions, the same handout and sticker would be provided to them.
The sticker would be applied by the pharmacist to the prescription opioid container to warn patients about the potential risks associated with opioid use, including dependence, addiction and overdose. The handout would contain broader information on the safe use of opioids, and on the risks associated with these drugs.
Mandatory risk management plans for opioids are also part of the Government of Canada’s commitment to addressing the opioid crisis. Through the proposed regulations, the Minister of Health would be able to require that pharmaceutical companies develop and implement risk management plans for all opioids to identify, mitigate and monitor risks associated with opioid use.
Companies would be required to keep their risk management plans evergreen by monitoring how their products are being used and develop activities should harms associated with use of these products emerge.
To finalize these regulations, Health Canada is asking Canadians to provide their comments via the Canada Gazette website. These consultations will be open for a period of 75 days, ending August 31, 2017.
https://www.canada.ca/en/health-canada/news/2017/06/new_measures_to_informcanadiansoftherisksofprescriptionopioidsou.html

CASE 1: ACUTE PAIN
And the following month … Rx acetaO M:30 x2 no visit
And 1 month later … Missed appointment with orthopedics; knee less sore Rx acetaO M:30
And the following year …
Asking for acetaO; since took for knee using 10-20/day
26 y.o. Patient since age 3
acetaO = acetaminophen 325 mg/oxycodone 5 mg
CASE 1: ACUTE PAIN
1 year prior to “wiping out”
26 y.o. Patient since age 3 Addiction and Mental Health
Clinic note:
Substance use Hx:
▪ Heavy user of MJ and EtOH for
past 4-5 years
▪ Often aggressive/fights on
weekends
▪ Trafficking
▪ Tried mushrooms and aceta/oxy
a few times
▪ Denies iv drugs
▪ Family Hx=EtOH, MJ
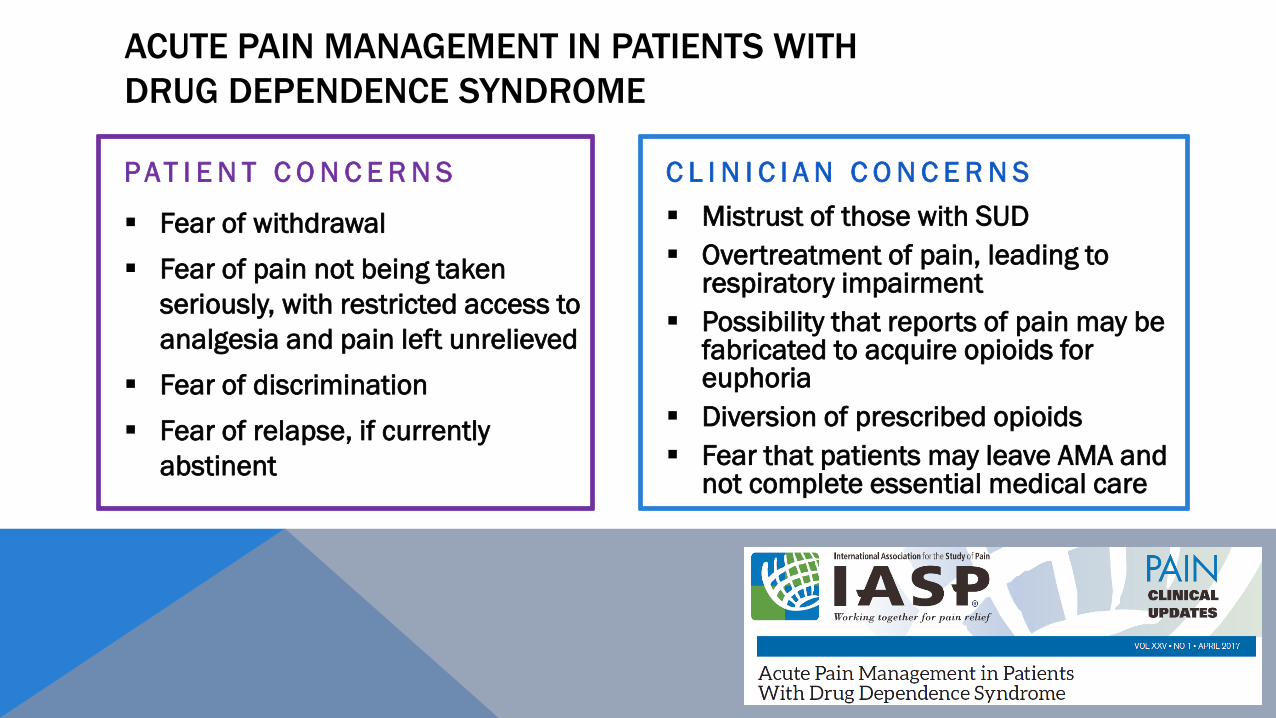
ACUTE PAIN MANAGEMENT IN PATIENTS WITH
DRUG DEPENDENCE SYNDROME
P AT I E N T C O N C E R N S
▪ Fear of withdrawal
▪ Fear of pain not being taken
seriously, with restricted access to
analgesia and pain left unrelieved
▪ Fear of discrimination
▪ Fear of relapse, if currently
abstinent
C L I N I C I A N C O N C E R N S
▪ Mistrust of those with SUD
▪ Overtreatment of pain, leading to respiratory impairment
▪ Possibility that reports of pain may be fabricated to acquire opioids for euphoria
▪ Diversion of prescribed opioids
▪ Fear that patients may leave AMA and not complete essential medical care

ACUTE PAIN MANAGEMENT IN PATIENTS WITH
DRUG DEPENDENCE SYNDROME
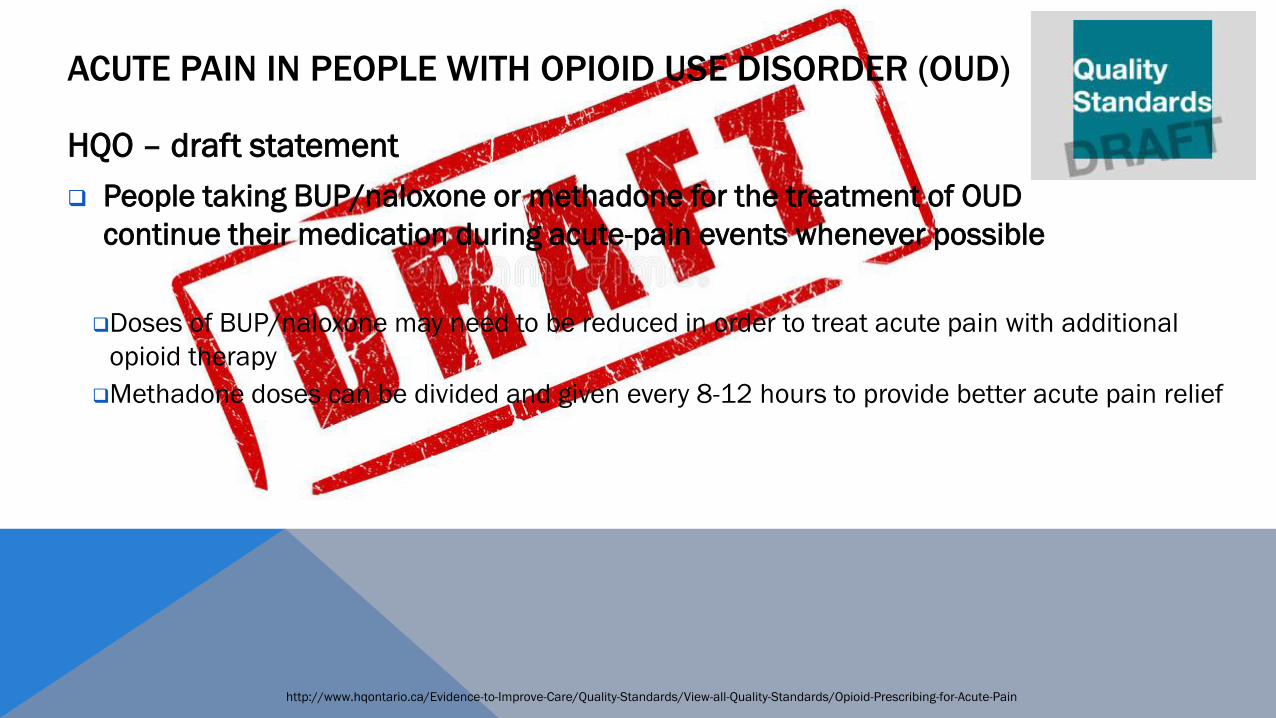
http://www.hqontario.ca/Evidence-to-Improve-Care/Quality-Standards/View-all-Quality-Standards/Opioid-Prescribing-for-Acute-Pain
HQO – draft statement
People taking BUP/naloxone or methadone for the treatment of OUD
continue their medication during acute-pain events whenever possible
Doses of BUP/naloxone may need to be reduced in order to treat acute pain with additional
opioid therapy
Methadone doses can be divided and given every 8-12 hours to provide better acute pain relief
ACUTE PAIN IN PEOPLE WITH OPIOID USE DISORDER (OUD)

PAIN AFTER SURGERY… IS THERE ANY GUIDANCE?

JAMA Surg. Published online September 27, 2017 doi:10.1001/jamasurg.2017.313
Procedure Median Rx length
Appendectomy 4 days
Cholecystectomy 4 days
Inguinal hernia repair 5 days
Hysterectomy 4 days
Mastectomy 5 days
Anterior cruciate ligament repair 5 days
Rotator cuff repair 5 days
Discectomy 7 days

CASE 2. OSTEOARTHRITIS
Performed MSK exams from time to time
Recommended non-pharmacological therapies
Initially prescribed acetaminophen for pain
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis
OP = osteoporosis; DDD = degenerative disc disease; OA = osteoarthritis; Available at: http://nationalpaincentre.mcmaster.ca/opioid
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

Hip & Knee Hand

CASE 2. OSTEOARTHRITIS
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis
Then …
Rx: acetaCc3 i-ii po qid prn
D:120 q month M:720
Rx: meloxicam 7.5 mg
i-ii od prn M:180
Refer: epidural steroid inj
OP = osteoporosis; DDD = degenerative disc disease; OA = osteoarthritis; cfpc.ca/oatool
Available at: http://nationalpaincentre.mcmaster.ca/opioid ;acetaO=acetaminophen/oxycodone (325/5 mg); acetaCc3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)

CASE 2. OSTEOARTHRITIS
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis
Then …
Rx: acetaCc3 i-ii po qid prn
D:120 q month M:720
Rx: meloxicam 7.5 mg
i-ii od prn M:180
Refer: epidural steroid inj
OP = osteoporosis; DDD = degenerative disc disease
Available at: http://nationalpaincentre.mcmaster.ca/opioid ;acetaO=acetaminophen/oxycodone (325/5 mg); acetaCc3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)

CASE 2. OSTEOARTHRITIS
Discharged from hospital
UTI, ARF on a background of CRF …
Creatinine >250 on admission; 132 on discharge (eGFR ~35)
Post discharge visits
Rx: acetaCc3 ‘as directed’ M:180 then…..
Rx: acetaO i po tid D:100 q30 days M:500
Tel-progress from/to pharmacy
Rx: Meloxicam 7.5 mg i-ii po od prn M:180
acetaO=acetaminophen/oxycodone (325/5 mg); acetaCc3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis

CASE 2. OSTEOARTHRITIS
acetaO=acetaminophen/oxycodone (325/5 mg); acetaCc3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis
Visit
• 4 bad days; nausea
• ?pneumonia
P: incr acetaO i-ii qid prn
Admitted to hospital
• Epigastric pain; GI bleed
• Hb=65
• 6 gastric ulcers
• 1 duodenal ulcer

CASE 2. OSTEOARTHRITIS
acetaO=acetaminophen/oxycodone (325/5 mg); acetaCc3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)
What are some of the
issues in the care?
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis

CASE 2. OSTEOARTHRITIS
Prescribing of NSAIDs
o eGFR 35-39; adequate monitoring
Opioid rotation
Opioids of choice in the elderly and persons with significant renal impairment
Collaboration (Good Practice Statement #3)
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis
Available at: http://nationalpaincentre.mcmaster.ca/opioid

CASE 2. OSTEOARTHRITIS
Choosing Wisely Canada Canadian Society of Nephrology
The use of NSAIDS, including cyclo-oxygenase type 2 (COX-2) inhibitors, for the pharmacological
treatment of musculoskeletal pain can elevate blood pressure, make antihypertensive drugs less
effective, cause fluid retention and worsen kidney function in these individuals. Other medication
prescribed by a healthcare professional may be safer than and as effective as NSAIDs.
http://www.choosingwiselycanada.org/wp-content/uploads/2014/09/Nephrology.pdf
Don’t prescribe nonsteroidal anti-inflammatory drugs
(NSAIDS) in individuals with hypertension or heart failure or
CKD of all causes, including diabetes.
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis

CASE 2. OSTEOARTHRITIS
Opioids - Safety Issues
Renal Failure
Avoid codeine & morphine1 for patients with renal dysfunction (Table 3)
Elderly
Nothing in 2017 guideline
Among strong opioids, oxycodone and hydromorphone may be preferred over
oral morphine1
o Less constipation & sedation
12010 Canadian opioid guideline; Available at: http://nationalpaincentre.mcmaster.ca/opioid
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis

CASE 2. OSTEOARTHRITIS
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis
Morphine Equivalent Dose (MED)/day
acetaCc3 ii po bid prn ~ _____ MED/day
acetaO i po tid prn ~ _____ MED/day
How many acetaCc3/day is 50 MED/day?
How many acetaO/day is 50 MED/day?
What about 90 MED/day?
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

CASE 2. OSTEOARTHRITIS
http://www.cmaj.ca/content/189/18/E659; 2Available at: http://nationalpaincentre.mcmaster.ca/opioid
87y.o. Hx of OP and OA knees & shoulders, plus DDD with spinal stenosis
2Table 5: Opioid conversion table

UPDATED OPIOID MANAGER / OPIOID SWITCHING FORM

GOOD PRACTICE STATEMENTS
Acquire informed consent prior to initiating opioid use for CNCP. A discussion about potential benefits, adverse effects, and complications will facilitate shared-care decision making regarding whether to proceed with opioid therapy.
Clinicians should monitor CNCP patients using opioid therapy for their response to treatments, and adjust treatment accordingly.
Clinicians with CNCP patients prescribed opioids should address any potential contraindications and exchange relevant information with the patient’s general practitioner (if they are not the general practitioner) and/or pharmacist.
1
2
3
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html
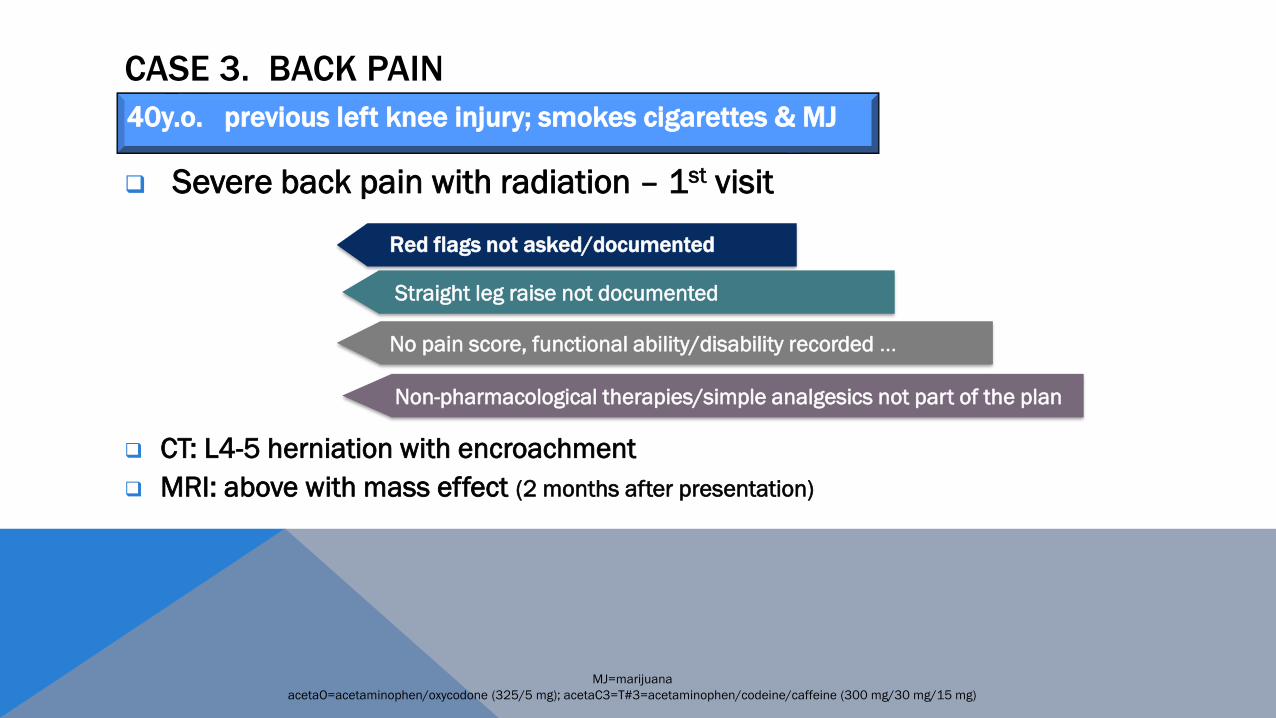
CASE 3. BACK PAIN
Severe back pain with radiation – 1st visit
CT: L4-5 herniation with encroachment
MRI: above with mass effect (2 months after presentation)
MJ=marijuana
acetaO=acetaminophen/oxycodone (325/5 mg); acetaC3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)
Red flags not asked/documented
Straight leg raise not documented
No pain score, functional ability/disability recorded …
Non-pharmacological therapies/simple analgesics not part of the plan
40y.o. previous left knee injury; smokes cigarettes & MJ

CASE 3. BACK PAIN
RED FLAGS are described by the mnemonic NIFTI:
Neurological progression, Infection, Fracture, Tumor, Inflammation
http://www.topalbertadoctors.org/download/1885/LBPguideline.pdf?_20160225091721

CORE BACK TOOL: PHYSICAL EXAM
Available from Centre for Effective Practice at www.effectivepractice.org

EXPLAIN THE PAIN SCALE IN FUNCTIONAL TERMS:
N A D I R
Requires immediate medical attention
Incapacitated because you can’t function; You miss work,
cancel social activities or stay in bed
You have Difficulty taking care of your responsibilities, rarely
enjoy yourself and your concentration is impaired
Pain is present and may even require regular medication, but
you are Able to continue performing your daily activities
No pain at all
10
8-9
6-7
1-5
0
Whitten CE, et al. Perm J. 2005;9(2):41–48

CASE 3. BRIEF PAIN INVENTORY - FUNCTION
63
Available at: http://nationalpaincentre.mcmaster.ca/opioid

Available at: http://mytopcare.org/prescribers/

CDC Guideline infographic

CASE 3. BACK PAIN
1st follow-up appointment
o No P/E, pain scale, function, questions re bowel/bladder/function …
o Clinician decides to initiate opioids
MJ=marijuana; P/E=physical examination; Available at: http://nationalpaincentre.mcmaster.ca/opioid; acetaO=acetaminophen/oxycodone (325/5 mg); acetaC3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)
40y.o. previous left knee injury; smokes cigarettes & MJ
Would you start a patient on an anti-hypertensive without measuring
the blood pressure?
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html; Available at https://www.cma.ca/Assets/assets-library/document/en/advocacy/2139_cma_opioid_poster_en.pdf

R# Possible Scenario
Trial of
opioids? Strength
2 No current or past SUD AND no other active psychiatric disorder YES Weak
3 Active SUD NO Strong
4 Active psychiatric disorder NO Weak
5 History of SUD NO Weak
PROBLEMATIC CNCP DESPITE OPTIMIZED NON-OPIOID THERAPY
HOW DO YOU KNOW IF A PATIENT HAS/HAD A SUD
Patients with CNCP and probable SUD should be screened with the CAGE
screening tool or similar validated questionnaire of alcohol use, and
validates substance abuse/misuse tools such as COMM
Although not evidence-based, UDS and review of prescription drug
monitoring data is suggested initially and periodically
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

CAGE – AID
https://www.divisionsbc.ca/CMSMedia/Divisions/DivisionCatalog-nanaimo/Documents/Resources/CAGE%20Questionnaire.pdf

Available at: http://nationalpaincentre.mcmaster.ca/documents/comm_sample_watermarked.pdf
HOW DO YOU KNOW IF A PATIENT HAS/HAD A SUD
Patients with CNCP and probable SUD should be screened with the CAGE
screening tool or similar validated questionnaire of alcohol use, and
validates substance abuse/misuse tools such as COMM
Although not evidence-based, UDS and review of prescription drug
monitoring data is suggested initially and periodically
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html
RISK MITIGATION
Expert Guidance Statement 6: Urine Drug Screening
A baseline UDS may be useful for patients currently receiving or being
considered for a trial of opioids.
When ordering a UDS, clinicians should ask patients about all
medications/drugs recently taken, and be aware of local resources to assist
them in assessing for potential false positive and false negative results
Clinicians may repeat UDS on an annual basis and more frequently if the
patient is at elevated risk or in the presence of any ADRBs.
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

RISK MITIGATION
Expert Guidance Statement 7: Treatment Agreements
A written treatment agreement may be useful in structuring a process of
informed consent around opioid use, clarifying expectations for both patient
and physician, and providing clarity regarding the nature of an opioid trial
with endpoints, goals, and strategies in event of a failed trial.
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

SOME GUIDING PRINCIPLES FOR INITIATION OF OPIOIDS
Prescriptions should be provided by the primary treating physician only,
for no more than 28 days at a time. Intervals may be shorter when
initiating therapy, in cases of suspected diversion or during dose
escalation
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

CASE 3. OPIOID INITIATION CHECKLIST
1st follow-up appointmento No P/E, pain scale, questions re bowel/bladder/function …
o Referral to neurosurgeon
o ORT done
o UDS requested
o No Treatment agreement found
acetaCc3 i po tid prn
M:270 D:90 q30 d
MJ=marijuana; P/E=physical examination; Available at: http://nationalpaincentre.mcmaster.ca/opioid; acetaO=acetaminophen/oxycodone (325/5 mg); acetaCc3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)
40y.o. previous left knee injury; smokes cigarettes & MJ

CASE 3. URINE DRUG SCREENING
Two (2) UDS were found in the chart, both with same date
o 1st positive for:
✓ BNZ, opiates, oxycodone, GBP and cotinine
o 2nd positive for:
✓ THC, cotinine
MJ=marijuana; BNZ=benzodiazepine; GBP=gabapentin
acetaO=acetaminophen/oxycodone (325/5 mg); acetaC3=T#3=acetaminophen/codeine/caffeine (300 mg/30 mg/15 mg)
40y.o. previous left knee injury; smokes cigarettes & MJ
• Always compare the UDS result to the actual patient chart/drugs prescribed -
Are the prescribed drugs/metabolites present?
- Are any prescribed drugs absent?
- Are there any unexpected drugs present?
- Read any comments listed by the laboratory
• If you encounter an inconsistent/unexpected UDS, your first action should be:
To take a careful history of medication/drug use in the past week and discuss
openly with the patient – without being accusatory
• Each type of inconsistent UDS result has a differential diagnosis and actions
for the clinician to take – documentation is key
Don’t rely on
your memory

DO YOU RECOMMEND THE USE OF GABAPENTANOIDS FOR
YOUR PATIENTS WITH ACUTE OR CHRONIC SCIATICA?

TRIAL OF PREGABALIN FOR ACUTE AND CHRONIC SCIATICAMathieson S et al, NEJM 2017 1111-1120
METHODS
We conducted a randomized, double-blind, placebo-controlled trial of pregabalin in patients with sciatica. Patients were randomly assigned to receive either pregabalin at a dose of 150 mg per day that was adjusted to a maximum dose of 600 mg per day or matching placebo for up to 8 weeks. The primary outcome was the leg-pain intensity score on a 10-point scale (with 0 indicating no pain and 10 the worst possible pain) at week 8; the leg-pain intensity score was also evaluated at week 52, a secondary time point for the primary outcome. Secondary outcomes included the extent of disability, back-pain intensity, and quality-of-life measures at prespecified time points over the course of 1 year.
RESULTS
A total of 209 patients underwent randomization, of whom 108 received pregabalin and 101 received placebo; after randomization, 2 patients in the pregabalin group were determined to be ineligible and were excluded from the analyses. At week 8, the mean unadjusted leg-pain intensity score was 3.7 in the pregabalin group and 3.1 in the placebo group (adjusted mean difference, 0.5; 95% confidence interval [CI], −0.2 to 1.2; P=0.19). At week 52, the mean unadjusted leg-pain intensity score was 3.4 in the pregabalin group and 3.0 in the placebo group (adjusted mean difference, 0.3; 95% CI, −0.5 to 1.0; P=0.46). No significant between-group differences were observed with respect to any secondary outcome at either week 8 or week 52. A total of 227 adverse events were reported in the pregabalin group and 124 in the placebo group. Dizziness was more common in the pregabalin group than in the placebo group.
CONCLUSIONS
Treatment with pregabalin did not significantly reduce the intensity of leg pain associated with sciatica and did not significantly improve other outcomes, as compared with placebo, over the course of 8 weeks. The incidence of adverse events was significantly higher in the pregabalin group than in the placebo group.

DO YOU RECOMMEND THE USE OF GABAPENTANOIDS FOR
YOUR PATIENTS WITH CHRONIC BACK PAIN?

• Gabapentin was associated with a small reduction in pain compared with placebo (very-low-quality evidence)
• Pregabalin was less effective than comparator treatments (e.g., amitriptyline, celecoxib) in relieving
pain (very-low-quality evidence)
• Gabapentin was associated with increased risks for dizziness (number needed to harm, 7), fatigue
(NNH, 8), mental difficulties (6), and visual disturbances (6)
• Pregabalin was associated with elevated risk for dizziness (NNH, 11)
Researchers examined eight randomized trials in which gabapentin or pregabalin was compared with active or inactive treatments in adults with low back pain lasting at least 3 months. Doses ranged from 300–3600 mg/day for gabapentin and 100–600 mg/day for pregabalin.
Among the findings:
The researchers conclude, "Given the lack of efficacy, risks, and costs
associated, the use of gabapentinoids for low back pain merits caution."

GUIDANCE ON LOW BACK PAIN
TOP [Toward Optimized Practice - Alberta] (2015)
▪ http://www.topalbertadoctors.org/download/1885/LBPguideline.pdf?_20160225091721
CORE Back Tool (2016)▪ http://effectivepractice.org/resources/low-back-pain-core-back-tool/
Healthy Back Exercises▪ http://www.health.gov.sk.ca/for-patients
Choosing Wisely Canada – Patient brochure▪ http://www.choosingwiselycanada.org/wp-content/uploads/2015/05/Treating-lower-back-
pain-EN.pdf

GUIDANCE ON LOW BACK PAIN
Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians▪ http://www.dssimon.com/MM/ACP-low-back-pain-guideline/files/ACP_LBP_Guideline.pdf
Systemic Pharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline▪ http://annals.org/aim/article/2603229/systemic-pharmacologic-therapies-low-back-pain-
systematic-review-american-college
3 minute Back Exam▪ https://www.youtube.com/watch?v=YcivUFHpKo4

NON-OPIOID OPTIONS
2017 Canadian Guideline
▪ CADTH: Alternatives to opioids
▪ https://cadth.ca/evidence-bundles/opioid-evidence-bundle/browse-category#alternatives
▪ Table 2: Non-opioid therapies for CNCP
Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline
▪ http://annals.org/aim/article/2603230/nonpharmacologic-therapies-low-back-pain-systematic-review-american-college-physicians
CDC Nonopioid Treatments for Chronic Pain
▪ https://www.cdc.gov/drugoverdose/pdf/alternative_treatments-a.pdf

FREE ON-LINE BEHAVIOURAL OPTIONS
MoodGYM
▪ https://moodgym.anu.edu.au/welcome
Mindfulness programs
▪ Many free on-line programs
o e.g. https://www.futurelearn.com/partners/monash-university
PAIN BC▪ https://www.painbc.ca/
▪ http://www.selfmanagementbc.ca/chronicpainprogram

CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)
2010
o On CR OC 40 mg ii tid + aceta/oxy prn
o Recently switched to truck run from walking route
o Wakes SOB at night; stops breathing = witnessed by girlfriend
▪ Sleep study = severe primarily central sleep apnea – likely opiate
o Mood worsening = decrease CR OC 40 mg tid + add TDS F 25 q3d
o No change in mood; start antidepressant + incr TDS F 50 q3d

CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)
Ca
Can this postal worker
drive safely on long-term
daily opioid therapy?

SOME GUIDING PRINCIPLES FOR A TRIAL OF OPIOIDS
During dosage titration, advise patients to avoid driving a motor vehicle until a stable dosage is established and it is certain the opioid does not cause sedation. This is especially true when taking opioids with alcohol, benzodiazepines or other sedating drugs.
Other potential AEs of opioids that warrant consideration include falls, fractures, sleep-disordered breathing (including sleep apnea), depression and a worsening of pain itself (OIH).
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

SLEEP APNEA
Expert Guidance Statement 4: Sleep Apnea
Patients with opioid-induce sleep apnea should be advised of
the associated health risks, and particularly the risk of
operating a motor vehicle. Clinicians may have a statutory duty
to report to governmental licensing authorities.
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)
2011
o 3 notes from sleep clinic = did not show up for titration/reassessment
▪ Expressed concerns re driving/MOH
CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)
2012
o Increase in pain meds give him more energy
2013
o Severe depression = short term disability
CR oxycodone 40 mg qid
aceta/oxy ii bid prn
clonazepam 0.5 mg bid
different antidepressant
testosterone replacement

CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)

CO-PRESCRIBING WITH OPIOIDS
Expert Guidance Statement 3: Co-prescribing with Opioids
Available studies yield conflicting results regarding the consequences of the
concomitant use of opioids and sedatives such as benzodiazepines (BNZ)
The expert perspective is that opioids and BNZ should
very rarely be prescribe together
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

CO-PRESCRIBING WITH OPIOIDS
What would the provinces say
Expert Guidance Statement 3: Co-prescribing with Opioids

ASHTON MANUAL
BENZODIAZEPINES: HOW THEY WORK AND HOW TO WITHDRAW
• PROTOCOL FOR THE TREATMENT OF BENZODIAZEPINE WITHDRAWAL• Medical research information from a benzodiazepine withdrawal clinic
Professor C Heather Ashton DM, FRCPRevised August 2002
• Ashton Manual Index Page• Contents Page• Introduction• Chapter I: The benzodiazepines: what they do in the body• Chapter II: How to withdraw from benzodiazepines after long-term use• Chapter II: Slow withdrawal schedules• Chapter III: Benzodiazepine withdrawal symptoms, acute & protracted
http://www.benzo.org.uk/manual/
TAPERING BENZODIAZEPINES
HYPOGONADISM
Expert Guidance Statement 5: Hypogonadism
As there is a high prevalence of secondary hypogonadism in this
population, clinicians treating men using chronic opioid therapy should
consider an evaluation for hypogonadism.
Clinicians should advise patients who are diagnosed with opioid-induced
hypogonadism regarding the potential short-term AEs, including: reduced
sexual function, amenorrhea, fatigue, mood changes and the long-term risk of
osteoporosis
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

HYPOGONADISM
Patients should be offered opioid tapering as the
initial strategy to correct hypogonadism
If opioid tapering is unsuccessful or declined,
clinicians may offer testosterone
supplementation therapy
Expert Guidance Statement 5: Hypogonadism
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

AND IF YOU ARE PRESCRIBING TESTOSTERONE REPLACEMENT …
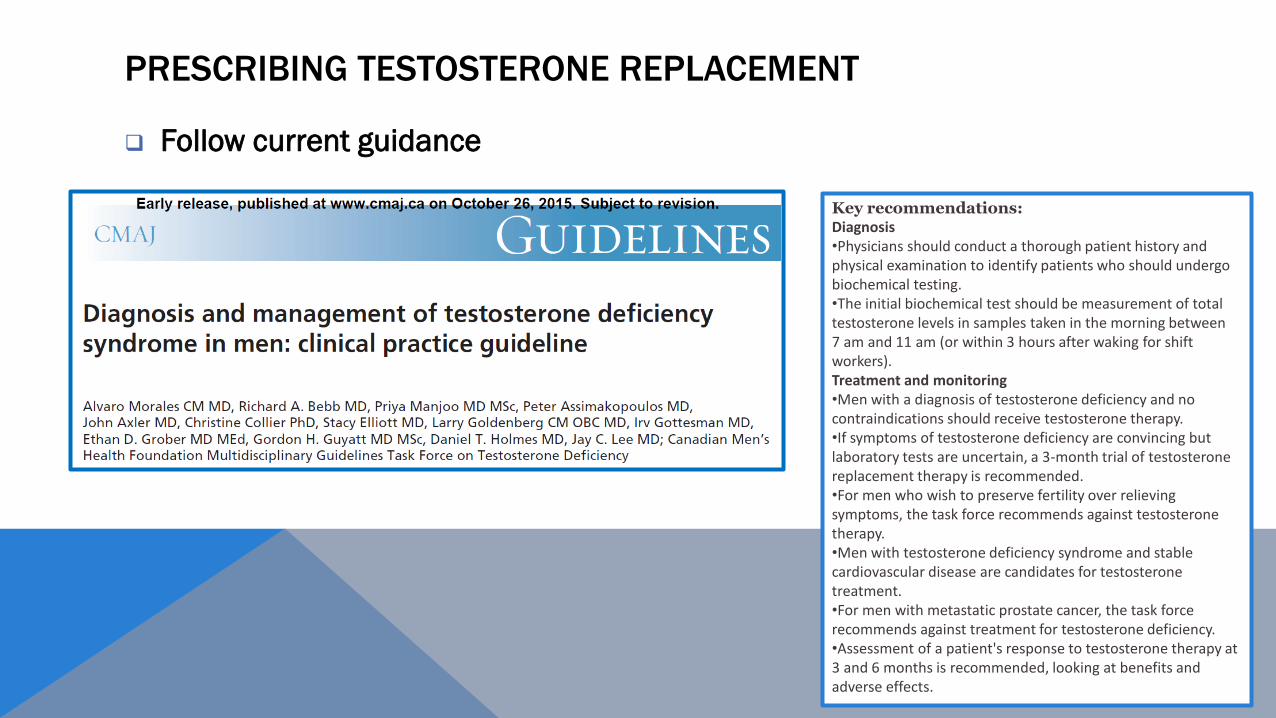
PRESCRIBING TESTOSTERONE REPLACEMENT
Follow current guidance
Key recommendations:Diagnosis•Physicians should conduct a thorough patient history and physical examination to identify patients who should undergo biochemical testing.•The initial biochemical test should be measurement of total testosterone levels in samples taken in the morning between 7 am and 11 am (or within 3 hours after waking for shift workers).Treatment and monitoring•Men with a diagnosis of testosterone deficiency and no contraindications should receive testosterone therapy.•If symptoms of testosterone deficiency are convincing but laboratory tests are uncertain, a 3-month trial of testosterone replacement therapy is recommended.•For men who wish to preserve fertility over relieving symptoms, the task force recommends against testosterone therapy.•Men with testosterone deficiency syndrome and stable cardiovascular disease are candidates for testosterone treatment.•For men with metastatic prostate cancer, the task force recommends against treatment for testosterone deficiency.•Assessment of a patient's response to testosterone therapy at 3 and 6 months is recommended, looking at benefits and adverse effects.

CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)
2013
o Severe depression = short term disability
CR oxycodone 40 mg qid
aceta/oxy ii bid prn
clonazepam 0.5 mg bid
different antidepressant
testosterone replacement

CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)
Consult note from Psychiatrist #1:
o Started smoking again; 5 cups coffee/day
o Actually using CR OC 40 mg 18 tab/day (MED > 1000)
✓ Dx Axis I: likely substance-induced Sx secondary to large dose of narcotics

CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)
6 months later ……
Independent Opinion from Psychiatrist #2 (on LTD)
o On CR OC 40 mg 12-16 tab/day
✓ “Depressed mood, lack of energy/motivation, cognitive disturbances with
memory/focus and attention issues; uses lots of caffeine possibly to counteract
sedative effects of opioid use and ends up with Sx of anxiety/palpitations”

WHAT ABOUT …
Depression

CASE 4: POSTAL WORKER
45 y.o. Postal worker CNCP = CLBP + knee pain (L>R)
Few months later ….
o c/o of gasping for breath; wants to be reassessed/go on CPAP
Sleep clinic
o Dx with OSA >4 years prior = never went on treatment

Available at https://www.cma.ca/Assets/assets-library/document/en/advocacy/2139_cma_opioid_poster_en.pdf

Reduction in opioid dose
may reduce AEs, including
cognitive impairment and
likelihood of nonfatal or
fatal unintentional
overdose.
If not done gradually, dose
reduction may cause
increased pain, decreased
function or highly aversive
symptoms of opioid
withdrawal.
Available at https://www.cma.ca/Assets/assets-library/document/en/advocacy/2139_cma_opioid_poster_en.pdf

NEW OPIOID SWITCHING FORM

Available at https://www.cma.ca/Assets/assets-library/document/en/advocacy/2139_cma_opioid_poster_en.pdf

“
“We continue to believe the prescribing of opioids is an important part of clinical practice, with
some patients achieving improvement in pain and function. But it also presents risks.
With the introduction of this guideline, physicians may re-evaluate how they prescribe opioids.
If relevant, particular attention needs to be paid to the guidelines’ recommendation about
tapering. If a dose is not reduced gradually, it may cause increased pain, decreased function or
opioid withdrawal which can be dangerous. Sudden cessation is never acceptable.”
College of Physicians and Surgeons of Ontario. Response to new Guideline; available at: cpso.cn.ca

TAPERING PLAN … BE MOTIVATIONAL

FRAMING THE CONVERSATION
Empathic tone
Concern
Shared responsibility
Optimism
“We know more about safety problems related to
opioids and we are concerned about your health and
safety. We recognize that we/the system prescribed
you these medications so now we want to help you be
safer while still managing your pain. The good news –
many patients feel better once they are on lower
doses”

FRAMING THE CONVERSATION
Other Recommendations
Offer choice/flexibility when possible
▪ Which med would you like to decrease first?
▪ Which dose of the day could you most easily lower?
Success in each step down breed success
Offer patients option to ‘pause’ prn

FRAMING THE CONVERSATION



Fast -
Slow-
Methadone or buprenorphine-naloxone


TO HELP WITH SYMPTOMS DURING TAPERING …
Clonidine has been used the longest to decrease some of the autonomic symptoms of opioid
withdrawal.
The main side effects are orthostatic hypotension and sedation. Prescribe 0.1-0.2 mg po q6h prn
maximum 6 tabs per day. The dose may have to be lowered if the patient reports orthostatic
symptoms or has a BP less than 90/60 mmHg, 1 hour after a dose. Continue clonidine until off of
opioids for 3-5 days then taper over next 3-5 days.
One of the early symptoms of opioid withdrawal is pain –the patient’s usual pain plus additional
arthralgias and myalgias - which may persist longer than other withdrawal symptoms, but will
eventually settle.
Acetaminophen, NSAIDs may be helpful. If attempting to re-evaluate a patient’s pain off of opioids,
the opioids need to be discontinued for at least 3-4 weeks to get through withdrawal pain and allow
opioid receptors to “reset.” It can take longer for an individual’s natural opioids to begin production.
Acupuncture or TENS have been shown in some studies to decrease symptoms of opioid withdrawal.
Short-term use of an antiepileptic such as carbamazepine or gabapentin or pregabalin, or the
cannabinoid nabilone for the first 1-2 weeks may help with sleep and anxiety.

TAPERING OPIOIDS – OTHER GUIDANCE
Alberta https://fmf.cfpc.ca/wp-content/uploads/2016/10/S132052_Motivational-Interviewing-to-
Support-Opioid-Tapering.pdf
WCH/ISMP
https://www.ismp-canada.org/download/OpioidStewardship/Opioid-Prescribing-Skills.pdf
CDC Pocket Guide: Tapering Opioids for Chronic Pain
https://www.cdc.gov/drugoverdose/pdf/clinical_pocket_guide_tapering-a.pdf
Navigating Opioids for CNCP Infographic
http://www.cpd.utoronto.ca/opioidprescribing/navigating-opioids/

TAPERING OPIOIDS – OTHER GUIDANCE
P Squire and R Jovey; Managing Opioid Withdrawal for Physicians
http://med-fom-tcmp.sites.olt.ubc.ca/files/2014/06/For-Physicians-TCMP-2014-Managing-
Opioid-Withdrawal.pdf
P Squire and R Jovey; Manging Opioid Withdrawal for Patients
http://med-fom-tcmp.sites.olt.ubc.ca/files/2014/06/For-Patients-TCMP-2014-Managing-
Opioid-Withdrawal.pdf

OTHER GUIDANCE
Opioids and Driving
http://www.driveable.com/
http://www.mard.ualberta.ca/SIMARDMD.aspx
http://thischangedmypractice.com/drive-on-opioid-medication/
Questionnaires for Sleep Disorders
http://www.topalbertadoctors.org/download/1923/Sleep%20Disorders%20Questionnaire.pdf
http://stopbang.ca/translation/pdf/caeng.pdf


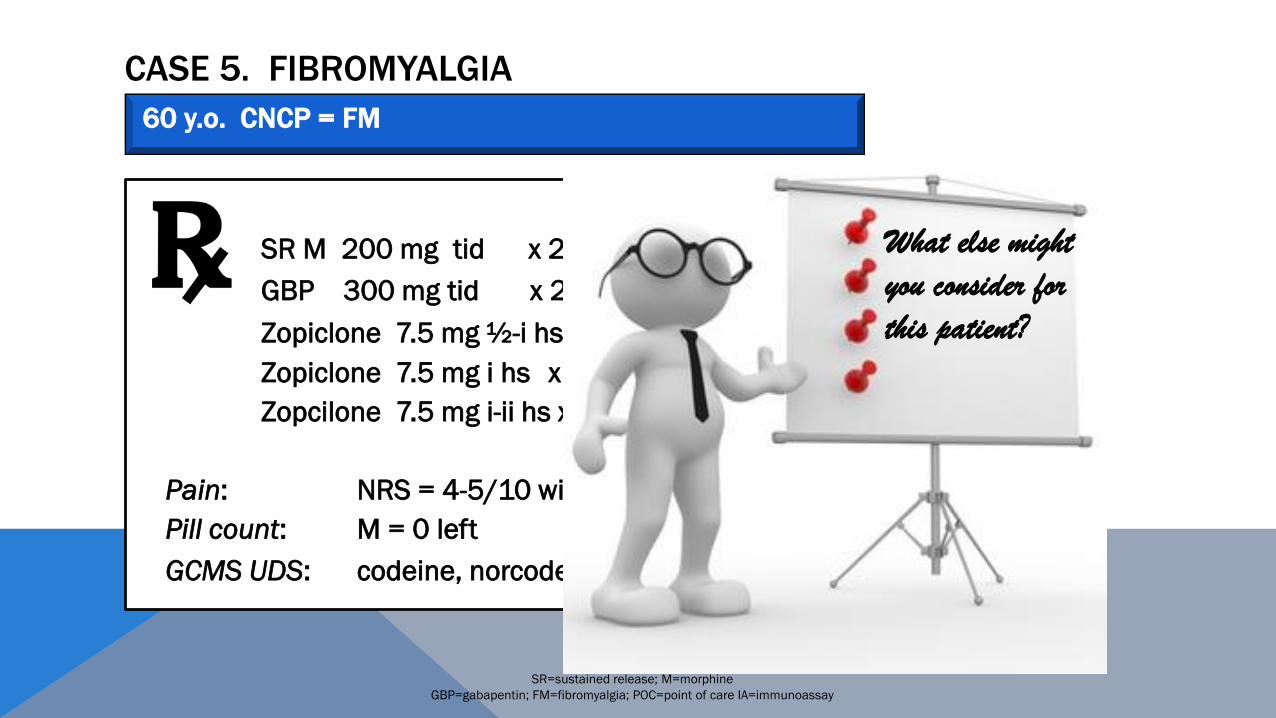
CASE 5. FIBROMYALGIA
SR M 200 mg tid x 2 months
GBP 300 mg tid x 2 months
Zopiclone 7.5 mg ½-i hs M:50 Feb
Zopiclone 7.5 mg i hs x100 days Jun
Zopcilone 7.5 mg i-ii hs x100 days Aug, Oct, Nov
Pain: NRS = 4-5/10 with walking, otherwise 2/10
Pill count: M = 0 left
POC UDS: M
60 y.o. CNCP = FM
SR=sustained release; M=morphine
GBP=gabapentin; FM=fibromyalgia; POC=point of care IA=immunoassay
Feb, Jun, Nov

CASE 5. FIBROMYALGIA
Available at: https://rheum.ca/images/documents/2012CanadianFMGuidelines_17August2012.pdf
60 y.o. CNCP = FM
Important Safety Information on Zopiclone
Dear Healthcare Professional, November 19, 2014
Subject: New dosage recommendations for IMOVANE® (zopiclone) to
minimize the risk of next-day impairment
The recommended starting dose has been reduced to 3.75 mg (one-half of the
7.5 mg tablet). IMOVANE should be taken once per night at bedtime. The lowest
effective dose for each patient should be used.
The prescribed dose should not exceed 5 mg in elderly patients, in patients with
hepatic or renal impairment or those currently treated with potent CYP3A4
inhibitors. Dose adjustment may be required with concomitant use with other CNS-
depressant drugs.
Patients should be instructed to wait for at least 12 hours after dosing before driving
or engaging in other activities requiring full mental alertness, especially for elderly
patients and for patients who take the 7.5 mg dose.

CASE 5. FIBROMYALGIA
SR M 200 mg tid x 2 months
GBP 300 mg tid x 2 months
Zopiclone 7.5 mg ½-i hs M:50 Feb
Zopiclone 7.5 mg i hs x100 days Jun
Zopcilone 7.5 mg i-ii hs x100 days Aug, Oct, Nov
Pain: NRS = 4-5/10 with walking, otherwise 2/10
Pill count: M = 0 left
GCMS UDS: codeine, norcodeine, M
60 y.o. CNCP = FM
SR=sustained release; M=morphine
GBP=gabapentin; FM=fibromyalgia; POC=point of care IA=immunoassay
Feb, Jun, Nov

OTC=over-the-counter
Could the patient be only taking OTC acetaCc1 ?
If so, what might happen if Rx is for SR M 100 mg v/day ?

CASE 5. FIBROMYALGIA
SR M 200 mg tid x 2 months
GBP 300 mg tid x 2 months
Zopiclone 7.5 mg ½-i hs M: 50 Feb
Zopiclone 7.5 mg i hs x100 days Jun
Zopcilone 7.5 mg i-ii hs x100 days Aug, Oct, Nov
SR=sustained release; M=morphine
GBP=gabapentin; FM=fibromyalgia; POC=point of care IA=immunoassay
Feb, Jun, NovThe patient moves practices and you have now taken over care
60 y.o. CNCP = FM
The patient moves practices, you have now taken over care and you work in BC

CASE 5. FIBROMYALGIA
SR=sustained release; M=morphine
GBP=gabapentin; FM=fibromyalgia; POC=point of care IA=immunoassay
Is this FM ?
Is this opioid-induced hyperalgesia (OIH) ?
Is this tolerance ?
60 y.o. CNCP = FM

OPIOID-INDUCED HYPERALGESIA (OIH) VS. TOLERANCE
Two occurrences with high dose /chronic opioid therapy:
OIH: Patients paradoxically demonstrate an increased sensitivity
to painful stimuli (i.e. hyperalgesia, allodynia or both)
Tolerance: Prolonged exposure to opioids results in a shift of the
dose-response curve to the right; in other words a larger dose
of opioids is needed over time to produce the same level of
analgesia

Condition Clinical features Onset
Response to
opioid Rx
OIH ▪ Pain may occur at a different
location and can be widespread
▪ Usually poorly defined in terms of
region and quality
Abrupt or
gradual
Pain worsens
Tolerance ▪ Characterized by persistent pain
and is localized
Gradual Pain improves
OPIOID-INDUCED HYPERALGESIA (OIH) VS. TOLERANCE

• 3 wk, daily rehab program
• Established opioid use
• Individual tapering plan
• COWS daily to monitor withdrawal
• Mean opioid dose 99 MED (range 5-600)
• 38% on multiple or combination opioids
• Used pt’s usual opioid
• Faster dose reduction at the beginning
• No adjuvants other than clonidine
✓11/55 used clonidine
• Peak withdrawal when taper was 60-80% complete
• Duration of taper:
<100 MED = mean 10 days
>200 MED = mean 28 days
• No difference based on duration of opioid use
OPIOID TAPERING IN FM – “REAL LIFE” EXPERIENCE
Cunningham et al, Opioid Tapering in FM patients: Experience from an Interdisciplinary Pain Rehab Program. Pain Med 2016 17 (9) 1676-1685
55 consecutive pts with FM admitted to Mayo Clinic Rehab Centre

OPIOID TAPERING IN FM – “REAL LIFE” EXPERIENCE
At admission, pts on opioids had higher pain scores, more depression,
lower functional status
At discharge both groups improved significantly on pain severity,
depression, catastrophizing, health perception, interference with life and
perceived life control
By discharge, no significant differences between groups
Cunningham et al, Opioid Tapering in FM patients: Experience from an Interdisciplinary Pain Rehab Program. Pain Med 2016 17 (9) 1676-1685
55 consecutive pts with FM admitted to Mayo Clinic Rehab Centre

GUIDANCE
OIHo http://ceaccp.oxfordjournals.org/content/14/3/125
o http://www.integration.samhsa.gov/pbhci-learning-community/opioid-
induced_hyperalgesia_article.pdf
Understanding Pain: Brainman stops his opioidso youtube.com/watch?v=MI1myFQPdCE
Fibromyalgia
o https://rheum.ca/images/documents/2012CanadianFMGuidelines_17August2012.pdf
o www.mdpi.com/2227-9059/5/2/20/pdf

GUIDANCE
Neuropathic Paino https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4273712/
o https://www.nice.org.uk/guidance/cg173/evidence/neuropathic-pain-pharmacological-
management-full-guideline-191621341
o http://www.watag.org.au/watag/docs/Advisor_Note_Neuropathic_Pain_Guidelines.pdf
o http://care.diabetesjournals.org/content/diacare/40/1/136.full.pdf
Managing Opioid Withdrawal –Information for Patients o http://www.bcwomens.ca/Professional-Resources-
site/Documents/Opioid%20Taper%20and%20Withdrawal.pdf
CASE 5. FIBROMYALGIA
SR M 200 mg tid x 2 months
GBP 300 mg tid x 2 months
Zopiclone 7.5 mg ½-i hs M:50 Feb
Zopiclone 7.5 mg i hs x100 days Jun
Zopcilone 7.5 mg i-ii hs x100 days Aug, Oct, Nov
Pain: NRS = 4-5/10 with walking, otherwise 2/10
Pill count: M = 0 left
GCMS UDS: codeine, norcodeine, M
SR=sustained release; M=morphine
GBP=gabapentin; FM=fibromyalgia; POC=point of care IA=immunoassay
Feb, Jun, Nov
What else might
you consider for
this patient?
60 y.o. CNCP = FM

CASE 5. FIBROMYALGIA
60 y.o. CNCP = FM
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html
CNCP Condition Quality of Evidence Therapies with some evidence of
effectiveness
Fibromyalgia (FM) Moderate Regular physical exercise probably
reduces pain in patients with FM

IS THERE EVIDENCE OF RATIONAL PRESCRIBING?
Centralized Pain
NSAIDs -
Opioids -
TCA +
SNRI +
Gabapentinoids +
Cannabinoids ?
Surgery / Injections -

TRICYCLIC ANTIDEPRESSANTS = TCA
Off-label for painPain relief independent of antidepressant effectBenefits evident in 1-2 weeks at adequate dosing
▪Start low dose (10mg)
• Titrate to effect or to maximum tolerated dose
• To decrease morning drowsiness, take at least 10-12 hrs before wake time, not at bedtime
Caution:
▪ Narrow-angle glaucoma, BPH, severe liver disease, suicide risk, severe cardiac conduction
(QTc > 440 msec /AV block)
▪ Baseline ECG recommended

VENLAFAXINE
Acts as SNRI only at higher doses (150-225 mg/day)
Off-label for pain
▪ Metabolism: hepatic (CYP 2D6)
▪ Elimination: renal
• Cautions: increased BP, recent unstable cardiac disease, bone fracture risk …
• Contraindications: MAOIs
Effexor XR® Product Monograph, November 2013 http://www.pfizer.ca/en/our_products/products/monograph/314
Pristiq® Product Monograph, July 2013 http://www.pfizer.ca/en/our_products/products/monograph/226

DESVENLAFAXINE
Active metabolite of venlafaxine MDD=50 mg/day
Off-label for pain
▪13-week RCT fixed-dose study of desvenlafaxine
• 50, 100, 200 or 400 mg/day in adults with painful DPN
• Week 13: mean change from baseline in NRS
o50 mg 0.58 (NS) 100 mg 0.59 (NS) 200 mg 1.10 (p=0.001) 400 mg 0.91 (p=0.027)
• Improvement in function at all doses
• Dose-dependent increase in the incidence of AEs and withdrawals due to AEs
Effexor XR® Product Monograph, November 2013 http://www.pfizer.ca/en/our_products/products/monograph/314
Pristiq® Product Monograph, July 2013 http://www.pfizer.ca/en/our_products/products/monograph/226
DULOXETINE
Pain approvals in Canada*:
▪NeP associated with DPN
▪Pain associated with fibromyalgia
▪Chronic low back pain
▪Pain associated with osteoarthritis of the knee
• Metabolism: hepatic (CYP 1A2, 2D6)
• Elimination: renal
• Titration: 30 mg daily (breakfast/lunch) 60-120 mg daily
▪ Cautions: increased BP & HR, bone fracture risk …
▪ Contraindications: severe liver/kidney disease; MAOIs, linezolid, potent CYP1A2 inhibitors
*Cymbalta® Product Monograph, June 2013, http://www.lilly.ca/cymbaltapm/en

GABAPENTIN
α2/δ ligand in voltage-gated Ca-channelsOff-label for pain in Canada
▪Common adverse effects (AEs)
• Somnolence, dizziness, fatigue, ataxia
▪Slower titration than pregabalin; q3-7d titration
• Start 100-300mg qhs q12h 300mg q8h maximum 2.4-3.2g/d
▪Adjust dosing in renal insufficiency
Neurontin® Product Monograph, December 2013 http://www.pfizer.ca/en/our_products/products/monograph/128

PREGABALIN
Higher affinity for α2/δ than gabapentin
Officially indicated for NeP of PHN & DPN plus pain in FM
Conditionally indicated for central NeP
▪Linear absorption kinetics – q12h dosing
▪Weekly titration starting at 25-75mg qhs q12h 300mg q12h
▪Effects may be seen within 1-2 weeks of adequate dosing
▪Adverse effects similar to gabapentin
• Dizziness, drowsiness, watch for peripheral edema
▪Adjust dosing in renal insufficiency
Finnerup et al. Pain, 2005
Lyrica® Product Monograph, January 2013, http://www.pfizer.ca/en/our_products/products/monograph/141
CANNABINOIDS
▪Compounds that act at cannabinoid receptors
• Endocannabinoids – endogenous ligands
• Phytocannabinoids – plant origin (cannabis/MJ)
▪ At least 80 different cannabinoids in cannabis
▪ Different strains have different relative concentrations
▪ THC - primary psychoactive cannabinoid in cannabis (UDS)
▪ CBD - not psychoactive
• Synthetic cannabinoids

PRESCRIPTION CANNABINOIDS
Nabilone Nabiximol Medical Marijuana (ACMPR)
Source Synthetic
cannabinoid(THC analog)
Δ9-THC:CBD Cannabis sativaTHC + other cannabinoids + other
compounds
Indications ▪ Severe nausea and
vomiting associated
with cancer
chemotherapy
▪*Adjunctive treatment for the
symptomatic relief of neuropathic pain
in multiple sclerosis in adults
▪ Adjunctive analgesic treatment in adult
patients with advanced cancer who
experience moderate to severe pain
during the highest tolerated dose of
strong opioid therapy for persistent
background pain
▪ Authorized HCPs decide which patients are
eligible
▪ The amount of dried marijuana that can be
possessed at any one time is the lesser of 30 x
daily amount stipulated by HCP or 150 g
▪ Through licensed producers (LPs) patients can
access fresh or dried MJ, or cannabis oil
▪ Some Colleges specifically prohibit clinicians
from applying to become LPs
Availability Oral capsule
- 0.25 mg,
0.5 mg, 1 mg
Buccal Spray
(27 mg/mL Δ9-THC : 25 mg/mL CBD)
- 5.5 mL vials; metering pump delivers
100 µL per spray
• Individuals can register with Health Canada to
produce marijuana for their own medical
purposes, or to designate someone else to
produce it for them
• Only LPs are authorized to sell or provide
medical marijuana.
*Approved under the Notice of Compliance with Conditions (NOC/c) Policy for its indicated uses. Patients should be advised of the conditional nature of the authorization; Product Monographs – Nabilone, Mar. 2009; Δ9-THC and CBD buccal spray, Dec. 2008
.
THC - tetrahydrocannabinol
CBD - cannabidiol

Conclusions: Limited evidence suggests that cannabis may
alleviate neuropathic pain in some patients, but insufficient
evidence exists for other types of chronic pain. Among
general populations, limited evidence suggests that
cannabis is associated with an increased risk for adverse
mental health effects.
GUIDANCE ON CANNABINOID PRESCRIBING
Your College’s guidelines/policies
CMPA (revised August 2016)▪ https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2014/medical-
marijuana-new-regulations-new-college-guidance-for-canadian-doctors
CFPC (preliminary guidance, September 2014)▪ http://www.cfpc.ca/uploadedFiles/Resources/_PDFs/Authorizing%20Dried%20Cannabis
%20for%20Chronic%20Pain%20or%20Anxiety.pdf
PRESCRIBING CANNABINOIDS
Many Colleges state that:
▪ More information is required on the medical risks and therapeutic benefits of marijuana
▪ Suggest that clinicians should only sign the medical document when they have the necessary clinical knowledge to engage in a meaningful consent discussion with patients
Some Colleges suggest:
▪ Trial Nabilone first
▪ Treat MJ/monitor MJ as you would an opioid
Risks:
▪ Mood, cognitive impairment, COPD, CVS, hepatic, hyperemesis, pregnancy/adolescents, cannabis use disorder …
▪ One joint =0.5 g 95% of patients use <3 g/day
▪ The scientific evidence for cannabis oils is lacking

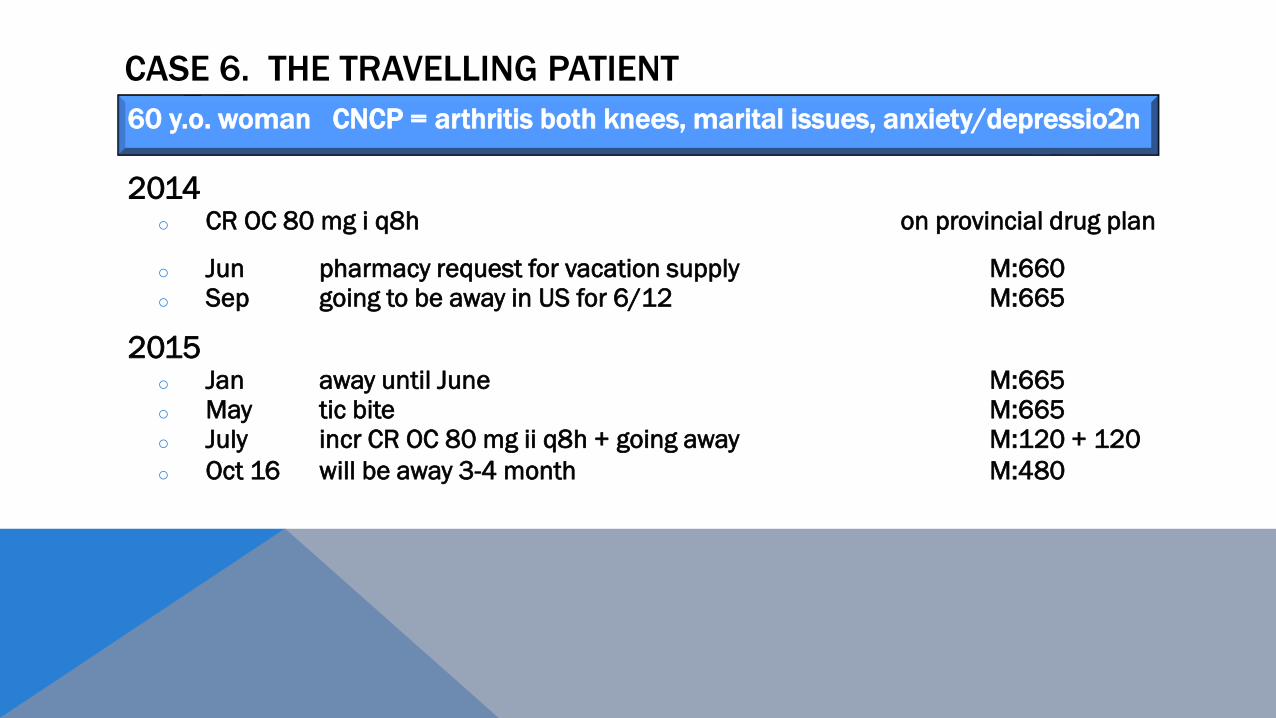
CASE 6. THE TRAVELLING PATIENT
2014o CR OC 80 mg i q8h on provincial drug plan
o Jun pharmacy request for vacation supply M:660o Sep going to be away in US for 6/12 M:665
2015o Jan away until June M:665o May tic bite M:665o July incr CR OC 80 mg ii q8h + going away M:120 + 120
o Oct 16 will be away 3-4 month M:480
60 y.o. woman CNCP = arthritis both knees, marital issues, anxiety/depression
CASE 6. THE TRAVELLING PATIENT
2014o CR OC 80 mg i q8h on provincial drug plan
o Jun pharmacy request for vacation supply M:660o Sep going to be away in US for 6/12 M:665
2015o Jan away until June M:665o May tic bite M:665o July incr CR OC 80 mg ii q8h + going away M:120 + 120
o Oct 16 will be away 3-4 month M:480
60 y.o. woman CNCP = arthritis both knees, marital issues, anxiety/depressio2n

▪ Prescriptions should be provided by the primary treating physician only for no more than 28 days at a time
▪ Intervals may be shorter when initiating therapy, in cases of suspected diversion or during dose escalation
SOME GUIDING PRINCIPLES FOR INITIATION OF OPIOIDS
Experts feel that it is reasonable to limit the amount of opioids prescribed at one time, but
also recognize that such policies may inconvenience patients who are travelling for
extended periods of time. Flexibility in such situations may be desirable
Expert Guidance Statement 1: Restriction in amounts of opioids prescribed
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

MY ADVICE FOR THE “TRAVELLING” PATIENT ON OPIOIDS
When going
How getting there
Where staying
To see plane/bus/train tickets
If on a provincial drug plan = ensure patient clears with appropriate authorities
Call contacts with patient sitting in front of you in the office

CASE 7. A YOUNG BOY
NMS record for hydrocodone liquid 200 cc:o Feb, Apr, Jun
Corresponding paper chart/EMR records for above dates:o Feb = URI; nothing about cougho Apr = diarrheao Jun = no visit
9 y.o. male = autism spectrum disorder, global development delay

CASE 7. A YOUNG BOY
Codeine is already not recommended for
children under age of 12, for any use.
Codeine should no longer be use
(contraindicated) in patients under 18 years of age to treat pain after
surgery to remove tonsils or adenoids, as
these patients are more susceptible to the risk of
serious breathing problems.
Hydrocodone is no longer recommended for children under six
years of age. This recommendation is
based on rare cases of serious breathing
problems including deaths in children in
this age group, usually involving higher-than recommended doses.
9 y.o. male = autism spectrum disorder, global development delay
Health Canada – July 2016
New safety measures for prescription codeine and hydrocodone to further restrict use in children and adolescents

CASE 7. A YOUNG BOY AND HIS FATHER
40 y.o male = Hx ACL repair; pain both shoulders and right knee
9 y.o. male = autism spectrum disorder, global development delay

CASE 7. A YOUNG BOY AND HIS FATHER
9 y.o. male = autism spectrum disorder, global development delay
40 y.o male = Hx ACL repair; pain both shoulders and right knee
CR OC 80 mg M:200 Jun 2, 16, 26 Jul 9, 23 Aug 7, 21 Sep 4, 18 Oct 2, 15, 30 Nov 13, 27 Dec 10
CR OC 80 mg M:400 Dec 30
Aceta/oxy M:180 same dates as CR OC
SR M 60 mg M:60 Jun 2, 16, 26 Jul 9, 23 Aug 7, 21 Sep 4
SR M 10 mg M:60 Oct 2, 15, 30
Hydrocodone 300 cc Jun 2 Jul 9, 23 Aug 7, 21 Sept 4 Oct 2, 15 Nov 13, 27 Dec 30
9 y.o. male = autism spectrum disorder, global development delay

CASE 7. A YOUNG BOY AND HIS FATHER
9 y.o. male = autism spectrum disorder, global development delay
40 y.o male = Hx ACL repair; pain both shoulders and right knee
CR OC 80 mg M:200 Jun 2, 16, 26 Jul 9, 23 Aug 7, 21 Sep 4, 18 Oct 2, 15, 30 Nov 13, 27 Dec 10
CR OC 80 mg M:400 Dec 30
Aceta/oxy M:180 same dates as CR OC
SR M 60 mg M:60 Jun 2, 16, 26 Jul 9, 23 Aug 7, 21 Sep 4
SR M 10 mg M:60 Oct 2, 15, 30
Hydrocodone 300 cc Jun 2 Jul 9, 23 Aug 7, 21 Sept 4 Oct 2, 15 Nov 13, 27 Dec 30
9 y.o. male = autism spectrum disorder, global development delay
Office visits:
Jan = all meds renewed early; froze,
then tried to melt them
Apr = 1-month supply; was at
grandmother’s and meds given to
drug store to destroy
Oct = All meds released early

CMAJ June 2017; https://www.ncbi.nlm.nih.gov/pubmed/28346310
Benzodiazepines, stimulants, testosterone, MJ …
Loperamide abuse:
o Recreational use of loperamide for its euphoric properties or to lessen symptoms of opioid withdrawal involves large oral dosages (>70 mg/day)
Gabapentanoid abuse:
o Gabapentin and pregabalin are abused for its euphoric/disassociation properties, particularly in the substance misuse population, especially as large quantities in a single dose
OTHER PRESCRIPTION DRUGS OF ABUSE TO THINK ABOUT


CASE 8: NEW PATIENT
Moved from BC 6 wks prior
o DM (insulin-dependent)
o Crohns (prednisone 15 mg); off biologic therapy x2 months
o Ca transverse colon – 2 surgeries
o Lost 20 lbs in last 6 wks; night sweats 2/52
o On B12 inj, antidepressant
C/o increasing severe upper abdominal pain
Using IR oxycodone 10 mg iv q4h
30 y.o. female = new patient; referred by ER

CASE 8: NEW PATIENT
1st visit
o Blood sugar measured …
o B12 injection done
o No abdominal exam done
30 y.o. female = new patient; referred by ER
Oxycodone IR 10 mg iv q4h
M:240

CASE 8: NEW PATIENT
2nd visit = 1 week later
o “lost previous script”
30 y.o. female = new patient; referred by ER
Oxycodone IR 10 mg iv q4h
M:240

CASE 8: NEW PATIENT
3rd visit = 10 days later
30 y.o. female = new patient; referred by ER
Oxycodone IR 10 mg iv q4h
M:720 D:240 q10d
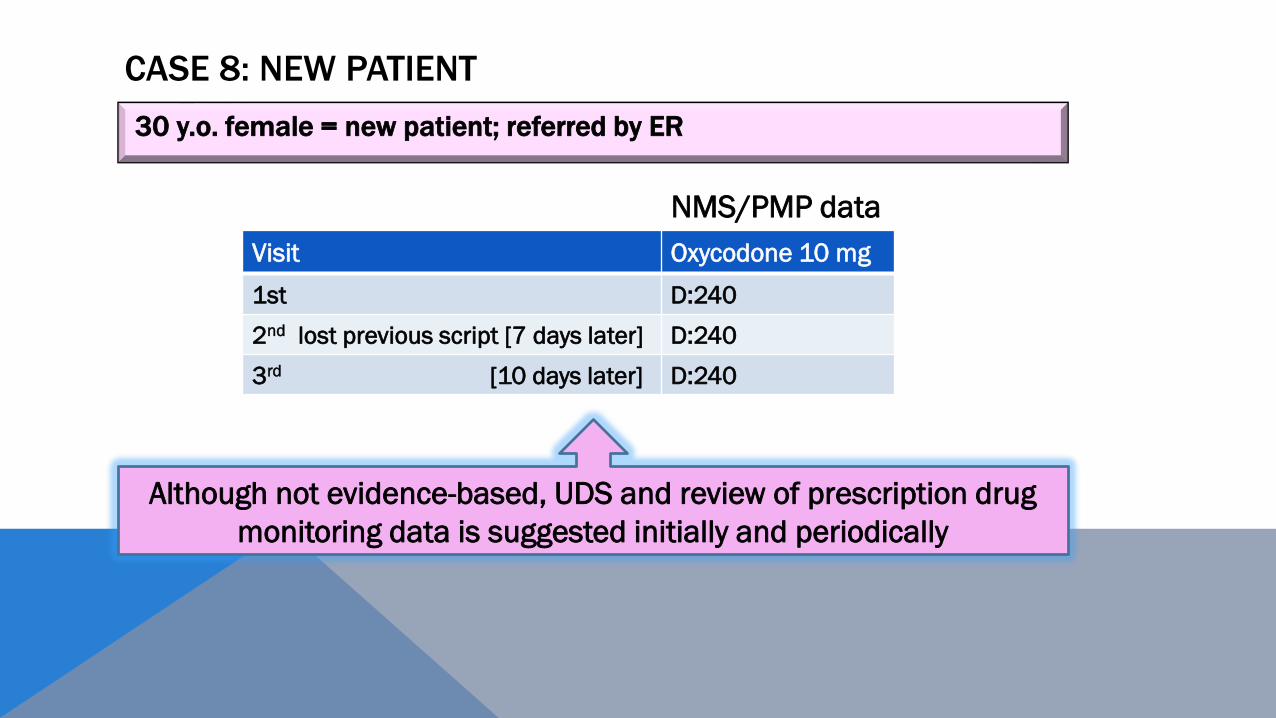
CASE 8: NEW PATIENT
NMS/PMP data
30 y.o. female = new patient; referred by ER
Although not evidence-based, UDS and review of prescription drug
monitoring data is suggested initially and periodically
Visit Oxycodone 10 mg
1st D:240
2nd lost previous script [7 days later] D:240
3rd [10 days later] D:240


CASE 8: NEW PATIENT
Doctors and pharmacies still doling out opioids to addicted patients, study finds man receives 26
prescriptions for opioids and other addictive drugs from 10 doctors in 4 months
By Angela Sterritt, CBC New Posted: Feb 22, 2017 7:32 PM PT Last Updated: Feb 22, 2017
A new case study is reminding doctors of the dangers of opioid shopping — where addicted patients
jump from doctor to doctor in search of drugs.
The College of Physicians and Surgeons of B.C., which published the study, says a database called
PharmaNet that tracks a patient's prescription drug use could mitigate the problem.
The study describes a 39 y.o. man who goes shopping for opioids and other addictive
drugs and receives more than 26 prescriptions from 10 different physicians in four months.
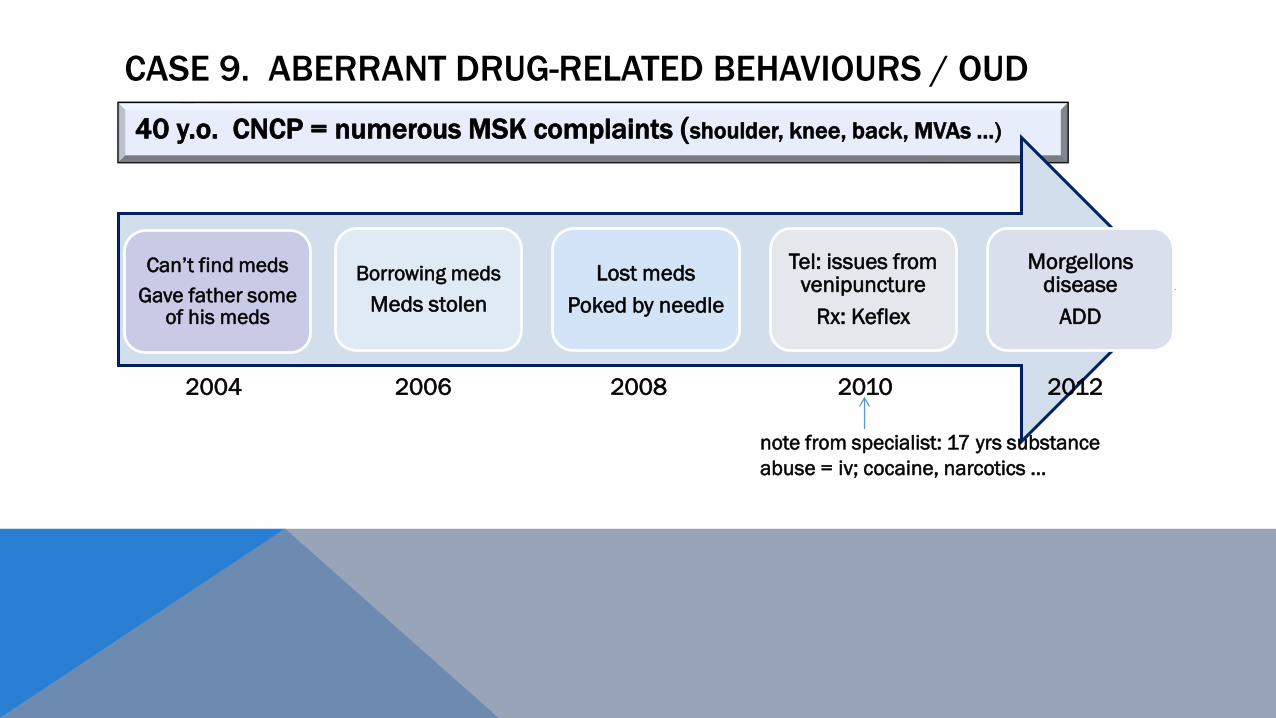
40 y.o. CNCP = numerous MSK complaints (shoulder, knee, back, MVAs …)
Can’t find meds
Gave father some of his meds
Borrowing meds
Meds stolen
Lost meds
Poked by needle
Tel: issues from venipuncture
Rx: Keflex
Morgellons disease
ADD
CASE 9. ABERRANT DRUG-RELATED BEHAVIOURS / OUD
2004 2006 2008 2010 2012
note from specialist: 17 yrs substance
abuse = iv; cocaine, narcotics …

CASE 9. ABERRANT DRUG-RELATED BEHAVIOURS / OUD
40 y.o. CNCP = numerous MSK complaints (shoulder, knee, back, MVAs …)
2013
Dog bite
2014
Tel:
Cut self & infected
ER for same :
Hx of cocaine abuse; recent relapse … injecting self with
self-clean needles
Tel x 3 for:
Stolen pills, misplaced pills,
2 month vacation

Indicator Examples
*Altering the route of delivery •Injecting, biting or crushing oral formulations
*Accessing opioids from other sources •Taking the drug from friends or relatives
•Purchasing the drug from the “street”
•Double-doctoring
Unsanctioned use •Multiple unauthorized dose escalations
•Binge rather than scheduled use
Drug seeking •Recurrent prescription losses
•Aggressive complaining about the need for higher doses
•Harassing staff for faxed scripts or fit-in appointments
•Nothing else “works”
Repeated withdrawal symptoms •Marked dysphoria, myalgias, GI symptoms, craving
Accompanying conditions •Currently addicted to alcohol, cocaine, cannabis or other drugs
•Underlying mood or anxiety disorders not responsive to treatment
Social features •Deteriorating or poor social function
•Concern expressed by family members
Views on the opioid medication •Sometimes acknowledges being addicted
•Strong resistance to tapering or switching opioids
•May admit to mood-leveling effect
•May acknowledge distressing withdrawal symptoms
CASE 9. ABERRANT DRUG-RELATED BEHAVIOURS
Available at: http://nationalpaincentre.mcmaster.ca/opioid * = behaviours more indicative of addiction /OUD

For patients with CNCP who are addicted to opioids, three treatment
options should be considered: methadone or buprenorphine treatment,
structured opioid therapy, or abstinence-based treatment.

CASE 10. OLDER PERSON
92 y.o. Multiple medical problems

CASE 10. OLDER PERSON
Geriatric Ambulatory Care Clinic
oRecommended to primary physician to reduce benzodiazepines (BNZ)
Pain Clinic
oSR opioid not helpful; refer for physiotherapy
oSuggest reducing opioids and stopping NSAID
oConcerns re 3 BNZ, especially with recurrent falls
92 y.o. Multiple medical problems

CASE 10. OLDER PERSON
92 y.o. Multiple medical problems
SR oxycodone
TDS F
AcetaO prn
Temazepam
Lorazepam
Alprazolam
NSAID

CASE 10. OLDER PERSON
Multiple falls
Left femur fracture - ORIF
Hand written note from family member
▪ “when left hospital they reduced her pain meds ; only on prn acetaO”
92 y.o. Multiple medical problems
SR oxycodone 40 bid
AcetaO prn
Lorazepam
PGB
ORIF=open reduction internal fixation; PGB=pregabalin
AcetaO=acetaminophen/oxycodone (325 mg/5 mg/); O=oxycodone

CASE 10. OLDER PERSON
Presents to local ER with 3-day Hx of increased confusion
and disorientation; dramatically improves with naloxone
1Ontario Drug Policy Research Network (2015); 2http://www.toronto.ca/legdocs/mmis/2015/hl/bgrd/backgroundfile-83429.pdf
Each year in Ontario, people aged 65 and older account
for over 40% of opioid-related hospital admissions1,2
“Decreased LOC, most likely from
narcotics and benzodiazepine toxicity”
92 y.o. Multiple medical problems




CASE 11.
41 y.o. man with chronic back and leg pain
3 previous surgeries for CLBP
4th surgery = single level fusion

CASE 11.
Arrested on suspicion of driving under the influence
Stated that his condition was the result of a reaction to mixing several
prescription drugs
41 y.o. man with chronic back and leg pain
CASE 11.
41 y.o. man with chronic back and leg pain

CASE 11.
41 y.o. man with chronic back and leg pain
Agreed to enter ‘treatment program’ to deal with prescription drugs
“Recently, I had been trying on my own
to treat my back pain and a sleep
disorder … but I realize now it was a
mistake to do this without medical
assistance”

CASE 11.
41 y.o. man with chronic back and leg pain
Agreed to enter ‘treatment program’ to deal with prescription drugs
Globe and Mail August 15, 2017
“I am continuing to work with my
doctors, and they feel I’ve made
significant progress”

CASE 11.
41 y.o. man with chronic back and leg pain
Globe and Mail August 15, 2017
Hydrocodone
Hydromorphone
Alprazolam
Zolpidem
THC
Toxicology Report
OVERCOMING BARRIERS TO CHANGE
acceptance and beliefs outreach visits
NHS: How to change practice

1. There is no substitute for an excellent
history and physical exam
2. Become familiar with signs of aberrant
drug use and opioid abuse disorder
3. Ask about patients’ sleep patterns and
mental health
4. Try alternative therapies
5. Prior to prescribing an opioid, use a risk
assessment tool like the ORT
6. Use a narcotic contract as a guiding too
for you and your patient
7. Limit the number of people you start on
narcotics and provide small amounts
8. Take the time to review addiction as a very
real risk to patients to whom you prescribe
narcotics
9. Develop an excellent relationship with
local pharmacists
10. Regularly call patients on narcotics for pill
counts and random UDS
11. If you are going to prescribe narcotics, you
should consider obtaining the knowledge
and skill to discontinue them
12. Find out from your local health unit if
naloxone kits are available in your area
13. Addiction crosses all social spectrums and
is a serious health concern
13 WAYS TO COMBAT THE OPIOID CRISIS* – BY DR. SARAH GILES
*Medical Post; February 21, 2017

https://www.cmpa-acpm.ca/static-assets/pdf/about/annual-meeting/com_16_opioids_chronic_non-cancer_pain-e.pdf