-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
1/66
Thyroid Disorders
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
2/66
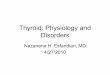
Anatomy
Over Trachea
Two Lobes
connected
together by anisthmus
15 to 20 g
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
3/66
Thyroid gland
Thyroid gland derives from the floor ofembryonic pharynx
Begins to develop around 4 weeks of gestation
Moves downthe neck while forming its
characteristic bilobular structure Thyroid development is
largely completed
between 10-20 weeks of gestation
Thyroid gland size increase gradually by
1g/year until age of 15 years were itachieves
adult size (15-25 g)
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
4/66
Sites ofnormal & ectopicthyroid tissue
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
5/66
Thyroid gland
Thyroid gland is composed overa millioncluster of follicles
Follicles are spherical & consists of
epithelial cells surrounding acentralmass (colloid)
Thyroglobulin is storage room
Two main hormones:
Tetraiodothyronine (Thyroxin)
Triiodothyronine
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
6/66
FUNCTIONAL
UNIT IS
THEFOLLICLE
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
7/66
Thyroid gland
Thyroid gland normally secretes mainly T4 70 % of T3 derived
from T4 in peripheral
tissues
T4 is converted to T3 by 5-deiodinase enzyme
Both T4 and T3 are in bound form (TBG, prealbuminand
albumin)
Only 0.025% of T4 and 0.35% of T3 are free
Free hormone concentration bestcorrelates
with thyroid status
T4 production is 5-6 Qg/kg/day in infancy withgradual
decrementto 1.5 Qg/kg/day inadult
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
8/66
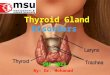
Thyroid Regulation
Somatostatin,Glucocorticoid
Dopamine
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
9/66
Thyroid hormone synthesis
1) Iodide pump Rate limiting step inthyroid hormone synthesis
which
needs energy
Follicles have intheir basement membrane an iodidetrapping
mechanism which pumps dietary I - into the cell
Normal thyroid: serum iodine is 30-40:1 Iodide uptake
enhancers:
TSH
Iodine deficiency
TSH receptors antibody
Iodide uptake inhibitors
Iodide ion
Drugs
Digoxin
Thiocynate
per chlorate
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
10/66
Thyroid hormone synthesis
2) Iodide oxidationto iodine and Organification
Inside the cells, iodide is oxidized by
peroxidase system to more reactive iodine
Iodine immediately reacts with tyrosineresidue onathyroid
glycoproteincalled
thyroglobulinto form : T1= mono-iodotyrosyl thyroglobulin
T2= di-iodotyrosyl thyroglobulin
Both processes are catalyzed by thyroid
peroxidase enzyme
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
11/66
Thyroid hormone synthesis
3) Coupling
T1& T2 couple togetherto form T3&T4
MIT +DIT = T3 (Tri-iodothyronine) DIT + DIT = T4 (Thyroxin)
All attached to thyroglobulinand stored inthecolloid
Thyroglobulin molecule
This process is stimulated by TSH
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
12/66
Production of Thyroid Hormones
NIS (Na+/I- Sympoter)
TPO
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
13/66
Effects ofthyroid hormones
Fetal brain & skeletal maturation Increase in basal
metabolic rate
Inotropic & chronotropic effects on heart
Increases sensitivity to catecholamines Stimulates gut
motility
Increase bone turnover
Increase in serum glucose, decrease in
serum cholesterol
Conversion ofcarotene to vitaminA
Play role inthermal regulation
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
14/66
Increase BMR ( Basal Metabolic Rate )
cellular metabolicactivity by :
size, total membrane surface & number of
mitochondria
ATP formation
active transport of ions ( Na+, K+ )
Promote growth & development ofthe brain during
fetal life and forthe first few years of postnatal life
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
15/66
Carbohydrate metabolism
enhanced glycolysis, gluconeogenesis,
GI absorption & insulin secretion
Fat metabolism
enhanced fat metabolism
Accelerates the oxidation of free fatty acids by the cells
plasmacholesterol, phospholipids & triglycerides
Body weight
the appetite, food intake, GI motility but the body weight
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
16/66
Cardiovascular system
vasodilatation
blood flow
cardiac output
heart rate
Respiratory
the rate and depth respiration
CNS
extreme nervous & psychoneurotic tendency
Muscle
make the muscles react with vigor ----->
muscle tremor ( 10-15 times/sec )
Sleep: extreme fatigue but is difficult to sleep
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
17/66
Causes , Clinical Features &
Consequences of Hypothyroidism
Congenital Hypothyroidism
Acquired Hypothyroidism
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
18/66
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
19/66
Etiology
Congenital
Acquired
Primary
Secondary
Tertiary
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
20/66
Congenital Hypothyroidism
Occurs inabout 1/4000 live birth Thyroxin is important for CNS
developmentand
postnatal growth
The most frequentcause is congenital absence
ofthe thyroid gland (athyrosis) Presentations may include
cyanosis, prolonged
hyperbilirubinemia, poor feeding, hoarse cry,
umbilical hernia, respiratory distress,
macroglossia, large fontanelle, and delayedskeletal
maturation
Rarely, neonatal hypothyroidism is transient
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
21/66
Congenital Hypothyroidism
Etiology
1) Thyroid dysgenesisIdiopathic:
Commonestcause in 95% ofcases Athyreosis (40%)
Hypoplasia (40%)
Ectopia (base oftongue, midline) (20%)
2) Thyroid dyshormonogenesis (A.R) (10%)
3) Hypothalamic-pituitary hypothyroidism Anencephaly,
holoprosencephaly, S.O.D
idiopathic
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
22/66
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
23/66
Congenital Hypothyroidism
4) Transient hypothyroidism Maternal TRAB
Maternal ingestion of goitrogen
5) Drugs
6) Iodine excess
7) Iodine deficiency
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
24/66
Anti-thyroid Drugs and fetus
Thionamides
PTU & MZT
Iodide
Lithium
Amiodarone
Radioiodine
After 10-12 wk gestationcan damage
fetal thyroid gland
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
25/66
Presentations ofcongenital hypothyroidism
Macroglosia Prolonged hyperbilirubinemia
Poor feeding
Hoarse cry
Decreased activity Constipation
Umbilical hernia
Dry yellow skin large fontanelle
Delayed skeletal maturation
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
26/66
Neonatal screening forcongenital hypothyroidism
Routine in mostcountries worldwide
Filter paper blood spot measuring TSH
Why ??
Clinical manifestations at birth, usually are subtle or
evenabsent (passive transplacental maternal thyroxin)
At birth, surge of TSH (stress of delivery) up to 30 -40
u/ml
Early detection will prevent mental retardation or
decreasing IQ ofaffected neonates
Thyroxin is important for CNS development from birth till
3 years of life
Screening program will miss 2ry/ tertiary cases
The program is hampered by a high rate of false
positive results
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
27/66
Acquired Hypothyroidism
More commonthan hyperthyroidism 99% is primary (< 1% due to
TSH deficiency)
Hashimotos
mostcommonthyroid problem (4% ofpopulation)
mostcommoncause in iodine-replete areas
chronic lymphocyticthyroiditis
Associated with TPO antibodies (90%), lesscommonly Tg
antibodies
Iatrogenic Hypothyroidism from radioactiveiodine therapy
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
28/66
Acquired Hypothyroidism
Subacute thyroiditis
Painful, often radiates to the ear
c/o malaise, pharyngitis, fatigue, fever, neck pain/swelling
Vir al etiology (URI/ pharyngitis)
self-limited. Cantx inflammation w/ ASA, NSAIDs or steroids
Suppurative/ Acute Infectious thyroiditis
Infections ofthe thyroid are rare
normally protected from infection by its thick capsule
Bacterial >> fungal, mycobacterial or parasitic
Pts are acutely ill w/ a painful thyroid gland
assoc w/ fever/chills, anteriorneck pain/swelling, dysphagia
and dysphonia
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
29/66
Acquired Hypothyroidism
Symptoms General Slowing Down
Lethargy/somnolence
Depression
Modest Weight Gain
Cold Intolerance
Hoarseness
Dry skin
Constipation ( peristalticactivity)
GeneralAches/Pains Arthralgias or myalgias
(worsened by cold temps)
Brittle Hair
Menstrual irregularities Excessive bleeding
Failure of ovulation
Libido
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
30/66
Acquired Hypothyroidism
Examination Dry, pale, course skin with yellowish tinge
Periorbital edema
Puffy f ace and extremities
Sinus Bradycardia
Diastolic HTN Body temperature
Delayed relaxation of reflexes
Megacolon ( peristalticactivity)
Pericardial/ pleural effusions
Congestive heart failure Non-pitting edema
Hoarse voice
Myopathy
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
31/66
Goiter
A swollenthyroidgland
Assessment;
how big, how quickly
has it developed, isit smooth ornodular,
is it painful, any
associated lymph
nodes, any sudden
changes, is it bigenough to cause
local symptoms (e.g.
breathing problems)
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
32/66
Myxedema
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
33/66
Hypothyroidism --- loss of scalp hair
A ColorAtlas of Endocrinology p70
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
34/66
Hypothyroidism with short stature
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
35/66
DiagnosisCongenital hypothyroidism
Thyroid hormone level TSH
Thyroid scan
Acquired Hypothyroidism
TSH fT4
Thyroid antibodies
Thyroid ultrasound
TSH: low in secondary hypothyroidismhigh in primary
hypothyroidism
TRH test: to differentiate between secondary& Tertiary
hypothyroidism
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
36/66
Euthyroid sick syndrome
Abnormalities inthyroid functiontestsobserved with
systemicnonthyroidal illness
Cytokine mediated
Reduced TRH release, TSH response, T4
production/release, T4 to T3 conversionandTBG production
Increased somatostatin secretion
Inhibitory effects of dopamine and
glucocorticoid on TRH action
Very low T4 values have a poor prognosis
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
37/66
Treatment
L-thyroxin replacement should be startedas soonas possible
Iftreatment is delayed > 2 months of life,
> 75% risk of hypothyroidism Onthe other hand, delayed
treatment of
hyperthyroidism will lead to advancedskeletal maturation,
craniosynostosisand intellectual deficits
L-Thyroxin is the main drug fortreatmentof hypothyroidism,
whatever is the cause
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
38/66
Treatment
8-10
6-8
5-6
4-5
2-3
25-50
50-75
75-100
100-150
150-200
0-6
6-12
1-5
6-12
>12
L-Thyroxin dose
Qg/ kg/day
L-Thyroxin dose
Total dose (Qg/day)
Age
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
39/66
Causes , Clinical Features &Consequences of
Hyperthyroidism
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
40/66
Hyperthyroidism (Thyrotoxicosis)
Definition Excessive secretion of T3 & T4
Affects metabolic processes inall body
organs Hyperthyroidism is 4-10 times more
prevalent in women
Mostcommon endocrine disease secondonly to diabetes as the most
occurring
endocrine disease
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
41/66
Thyrotoxicosis
Causes
Transient
1.Neonatal thyrotoxicosis
2.Infectious : Acute & subacute thyroiditis3.Drug induced:
Amiodarone, interferon &interleukin
4.Iatrogenic
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
42/66
Thyrotoxicosis
Causes
Persistent
1.Graves disease
2.Toxic multinodular goiter
3.Toxic solitary adenoma
4.Central (pituitary origin)
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
43/66
Neonatal Thyrotoxicosis
Only occur with 5% ofthyrotoxic mothers
Severity consistent in future pregnancies
20% mortality if untreated
Evolves rapidly, evident by day 7 of life, unlessTRAB blocking
antibody is present
Associate with cranial synostosis and learningdifficulties,
ifnottreated
Fetal thyrotoxicosis in rats leads to abnormalCNS
myelination
Parents should be aware of potential learningproblems (early
school years should bemonitored)
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
44/66
Neonatal hyperthyroidism bornto mother
with Graves disease
A ColorAtlas of Endocrinology p51
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
45/66
Graves disease
Pathogenesis T-cell dependentautoimmune disease
60% have HLAassociation with A1, B8,DR3,DR4,DR5
Autoimmune disorderthat results inproduction ofantibodies
directed againstthyroid antigens:
TS
H receptors Thyroglobulin
Thyroid peroxidase
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
46/66
Subacute Thyroiditis
Clinical course lasts weeks to months Acute phase (2-6/52) with
clinical and
biochemical hyperthyroidism
Recovery phase (weeks-months) transient
hypothyroidism then euthyroidism
Clinically, history of sore throat, fever, tender
goiter, cervical lymphadenopathy
High ES
R, negative antibodies and absentradioactive I131 uptake
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
47/66
Hyperthyroidism
May result in significant morbidity,
mortality & even death
Symptoms Jittery, shaky, nervous
Difficulty concentrating
Emotional lability Insomnia
Rapid HR, palpitations, Feeling Hot
Weight Loss
Diarrhea Fatigue
Menses : lighter flow, shorterduration
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
48/66
Hyperthyroidism
Exam Eye findings (20%)
Goiter
Thyroid brui t orthrill
Tachycardia: Sinus Tachycardia,
Atrial Fibrillation Flow murmur
Systolic hypertension
Hyperreflexia
Tremors
Proximal muscle weakness Clubbing
Onycholysis (
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
49/66
Thyrotoxicosis
Heart: Increased heart rate, contractility andcardiac output
Skeletal muscles: Proximal myopathy, easyfatigability and muscle
atrophy
Gonads: Irregular menstrual cycles,impotence
Liver: Low cholesterol LDL & apolipoprotein
Bone: Increased bone turnover, osteoporosis& increased risk
of fracture
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
50/66
Grave's ophthalmopathy
The pathogenesis of infiltrativeophthalmopathy is poorly
understood
It may occur before the onset ofhyperthyroidism oras late as 15
to 20 years
The clinical course of ophthalmopathy is
independent ofthe clinical course ofhyperthyroidism
Infiltrative ophthalmopathy may result fromimmunoglobulins
directed to specificantigensinthe extraocular muscles & orbital
fibroblasts
The antibodies are distinct from those initiatingGraves'-type
hyperthyroidism
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
51/66
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
52/66
Hyperthyroid Eye Disease
Hyper thyroidism (any cause)
Lid lag, lid retractionand stare
Due to increased adrenergictonestimulating the levator
palpebralmuscles.
True Gr aves Ophthalmopathy Proptosis
Diplopia
Inflammatory changes
Conjunctival injection
Periorbital edema Chemosis
Due to thyroid autoAbs thatcross-react w/ Ags in fibroblasts,
adipo-cytes, + myocytes behind the eyes.
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
53/66
Exophthalmos
G hth l th
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
54/66
Graves ophthalmopathy
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
55/66
Hyperthyroid Eye Disease
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
56/66
Graves Dermopathy
Thyroid Dermopathy
Thickening and redness of
the dermis
Due to lymphocytic
infiltration
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
57/66
Thyroid Acropachy
Thyroid acropachy. This is most marked in the index fingers and
thumbs
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
58/66
Tremor ofthe hand
A ColorAtlas of Endocrinology p49
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
59/66
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
60/66
Diagnosis
TSH level usually < 0.05 Qu / ml 95 % ofcases, high FT4 &
FT3
In 5% high FT3 with normal T4 (T3
Thyrotoxicosis) Thyroid receptor (TRAB) are usually
elevated at diagnosis
Antibodies againstthyroglobulin,peroxidase or both are present
inthe
majority of patients
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
61/66
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
62/66
Thyrotoxicosis- Treatment
Three modalities for more than last 50 years
Radioactive iodine,antithyroid drugs&surgery
None is optimal
None interrupts the autoimmune process Each has a drawbacks
There is no treatment for underlying cause
No other research options so far
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
63/66
Neonatal Thyrotoxicosis
Treatment
1) Lugols iodine
1 drop tid for 1-2 / 7
Dramaticcoarse therapy
Blocks T4 release, synthesis and I uptake(Wolf Chaikoff
effect)
2) Propranolol
3) Carbimazole
will take several days to have an effect on T4synthesis
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
64/66
Hyperthyroidism (Treatment)
1) -blockers (symptom control) Propr anolol (Inderal )
Atenolol (Tenormin)
Metoprolol (Lopressor)
2) 131-RAIA (70% thyroidologists prefer) Dosing
Graves: 10-15 mCi
Toxic MNG/Adenoma: 20-30 mCi
Absolute contraindications
Pregnancy and lactation (excreted in breast milk)!
Pregnancy should be deferred forat least 6 months
followingtherapy with radio-active 131
It is advisable to avoid 131-Rdio-active iodine therapy in
patientswith active moderate severe Graves ophthalmopathy.
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
65/66
Hyperthyroidism (Treatment)
3) Antithyroid Drugs (30% thyroidologists prefer)
Propylthiouracil (PTU)
100 mg bid-tid to start
Methimazole
10X more potentthe PTU
10 mg bid-tid to start Complications ofATDs
Agranulocytosis (1/200-500)
usually presents w/ acute pharyngitis/ tonsilitis or
pneumonia.
Rash
Hepaticnecrosis, Cholestaticjaundice Arthralgia
-
8/3/2019 Copy of 17+%26+18-Thyroid+Disorders
66/66
Hyperthyroidism (Treatment)
4) Surgery (sub-total thyroidectomy)
Indications
Patient preference
Large or symptomatic goiters
Whenthere is question of malignancy Need to be euthyroid priorto
surgery
To the risk ofarrhythmias during induction ofanesthesia
To the risk ofthyroid storm post operatively
ATDs + -blockers
Risks Permanent hypoparathyroidism
Recurrent laryngeal nerve problems
Permanent hypothyroidism