Embed Size (px)
Citation preview
ARTICLE
Content Validation of the International Ciassification ofFunctioning, Disability and Health Core Sets for Head andNeck Cancer: A Multicentre StudyUta Tschiesner, MD, Elisabeth Linseisen, MPH, Sven Becker, MD, Gerson Mast, MD, Simon N . Rogens, BDS, FSDRCS (Eng), FRCS (Max), MD, Rohan R. Walvekar, MD, PhD, Alexander Berghaus, MD, PhD, andAlarcos Cieza, MD, PhD
ABSTRACT
Objective: The International Classification of Functioning, Disability and Health (ICF) Core Sets for head and neck cancer (HNC)
structure the assessment of functioning and guide rehabilitation . They are an application of the ICF that was adopted by the World
Health Organization . They exist in a first version as a Comprehensive Core Set (CCS) with 112 categories for multidisciplinary
assessment and clinical studies and as a Brief Core Set (BCS) with 19 categories for data collection in clinical routine . The BCS is a
selection of the most important categories from the CCS . The objective of this study was to test whether the CCS and BCS are
relevant in patients with HNC treated in different departments and countries across the world .
Design : A multicentre, Cross-sectional study was conducted with 276 patients at 14 international study-centres . Data collection
included departments of otolaryngology, maxillofacial surgery, hemato-oncology, psychiatry, speech therapy, and physiotherapy .
Methods: Questionnaires an the CCS, the University of Washington Quality of Life questionnaire (UW-QOL version 4), and
European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC-QLQ) modules c30 and hn35
were completed by patients and health professionals . Frequency analyses and Spearman correlations were applied .
Results : For the CCS,105 of 112 categories (94%) were confirmed . New categories were not identified. For the BCS,14 of 19 categories
(74%) were confirmed, whereas several additional categories of the CCS haue qualified for upgrading and inclusion in the BCS . Correla-
tions between the UW-QOL and EORTC-QLQ (modules c30 and hn35) to the ICF-based data collection were satisfactory (mostly p < .01) .
Conclusion: The CCS proved to be exhaustive and covers a broader range of aspects than any of the testöd questionnaires . Final
selection of categories out of the CCS into the BCS requires further studies .
SOMMAIRE
Objectif: Les modules de base de la Classification internationale du fonctionnement, du handicap et de la sante (CIF) dans le
contexte du cancer de la töte et du cou (CTC) permettent de structurer I'evaluation du fonctionnement et de guider la readaptation . II
s'agit, en fait, d'applications de la CIF, adoptee par l'Organisation mondiale de la sante. Celle-ci existe en version integrale, le module
Comprehensive Core Set (CCS), qui compte 112 categories pour lös evaluations pluridisciplinaires et lös etudes cliniques, et en
version abregee, le module Brief Core Set (BCS), qui compte 19 categories pour la collecte de donnees en pratique clinique courante .
Le BCS consiste en une selection des categories lös plus importantes, tirees du CCS . L'etude avait pour objectif de verifier si lös
Uta Tschiesner, Sven Becker, and Alexander Berghaus : Department ofOtorhinolaryngology, Head and Neck Surgery, Ludwig-Maximilians-University Munich, Munich, Germany; Elisabeth Linseisen and Alarcos
Cieza : ICF Research Branch of the WHO Collaborating Center for theFamily of International Classifications at the German Institute ofMedical Documentation and Information, Institute for Health andRehabilitation Sciences, Ludwig-Maximilians- University Munich,Munich Germany; Gerson Mast : Department for Oral andMaxillofacial Surgery, Ludwig-Maximilians- University Munich,Munich, Germäny; Simon N. Rogens : Regional Maxillofacial Unit,Merseyside Head and Neck Cancer Centre, University Hospital Aintree,Aintree, United Kingdom ; Rohan R. Walvekar : Department ofOtolaryngology Head and Neck Surgery, LSU Health Sciences Center,New Orleans, LA .
DECKEI674
The study was dope in cooperation with the World Health Organization .
Alldress reprint requests to: Uta Tschiesner, MD, Department ofOtorhinolaryngology, Head and Neck Surgery, Ludwig-Maximilians-University, Marchioninistrasse 15, D-81377 Munich, Germany; e -mail:uta [email protected] .de .
DOI 10.231017070 .2010.090331
0 2010 The Canadian Society of Otolaryngology-Head & Neck Surgery
Journal of Otolaryngology-Head & Neck Surgery, Vol 39, No 6 (December), 2010 : pp 674-687

modules CCS et BCS etaient pertinents pour las patients atteints d'un CTC et traites dans differents services et dans differents pays
partout dans le monde.
Type d'etude: Une etude transversale et multicentrique a ete menee chez 276 patients, dans 14 centres internationaux de
recherche . La collecte de donnees a ete realisee dans des services d'otorhinolaryngologie, de Chirurgie maxillofaciale, d'hemato-
oncologie, de psychiatrie, d'orthophonie et de physiotherapie .
Mathedes: Des questionnaires sur le CCS, le questionnaire de I'University of Washington Quality of Life (UW-QOL version 4) et
des modules de I'European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC-QLQ)
modules c30 et hn35 dans le contexte du CTC ont ete remplis par des patients et par des professionnels de la sante . Nous avons
procede ensuite ä des analyses de frequence et ä des correlations de Spearman .
Resultats: En ce qui concerne le CCS, 105 categories sur 112 (94%) ont ete confirmees et il n'y a pas eu d'ajout de nouvelles
categories . En ce qui concerne le BCS,14 categories sur 19 (74%) ont ete confirmees, mais plusieurs autres categories du CCS ont ete
revues ä la hausse et jugees suffisamment pertinentes pour etre integrees dans le BCS . Les correlations entre l'UW-QOL et I'EORTC-QLQ
(modules c30 et hn35) par rapport ä la collecte de donnees realisee ä l'aide de la CIF etaient satisfaisantes (p < .01 pour la plupart) .
Conclusion: Le CCS s'est revele exhaustif et couvre un eventail d'aspects plus 'arge que las questionnaires compares . Toutefois,
la selection definitive des categories tirees du CCS et leur Integration dans le BCS exigent d'autres etudes .
Key words : head and neck cancer, outcome assessment, quality of life, International Ciassification of Functioning, Disability andHealth (ICF)
T he effects of head and neck cancer (HNC) and itstreatment an patient functioning haue become
increasingly important euer recent years . 1-5 Structuredoutcome research is especially relevant if different treat-ment protocols are used that haue equivalent, anticipatedoncologic outcomes and are recommended based an thepresumed functional and quality of life outcomes forselected patients . Even though mang different outcomemeasures (including patient questionnaires) are availableto assess patient functioning, an agreed-on framework forsystematic and comprehensive assessment is still missing .Different outcome measures may fit different purposes,and offen more than one measure is needed . This leavesthe clinician with a wide, sometimes confusing array ofoptions 6 and the risk of missing relevant aspects in theassessment process because the aspects are not covered bythe applied outcome measure(s) . 7 Structured outcomeresearch also needs to cover the different health profes-sional perspectives included in a multidisciplinary team . 8 ' 9Several authors haue called for a new systematic approachto outcome assessment, '°-12
As a new approach, there is an international andmultidisciplinary attempt to reach consensus an whataspects of patient functioning should be assessed inHNC. 13 The World Health Organization (WHO) providesa useful framework for classifying the components ofhealth and consequences of a disease : the InternationalClassification of Functioning, Disability and Health (ICF) .The ICF aims at providing a unified language for thedescription of health conditions in rehabilitation and acommon framework for all health professions . 14 Tofacilitate the implementation of the ICF into clinical
Tschiesner et al, Validation ICF Core Sets for Head and Neck Cancer
675
practice, ICF Core Sets are implemented as a disease-specific selection of categories out of the ICF. lt isimportant to note that ICF Core Sets are not a ready-to-use outcome measure but create a sound basis for theselection of outcome measures. ICF Core Sets haue beencreated for 16 different health conditions . 15-22
The ferst version of ICF Core Sets for HNC includes aComprehensive ICF Core Set for HNC (CCS) with 112different ICF categories and a Brief ICF Core Set (BCS)with just 19 categories .23 The CCS covers the typicalspectrum of problems in functioning and is needed formultiprofessional comprehensive assessment in cancerfollow-up and rehabilitation . The BCS is a selection fromthe CCS that aims to include the most importantcategories across health professions and countries . l tdefines categories as minimal standards to assess andreport an functioning and health in any patient with HNC .
Both the CCS and the BCS were developed in a formaldecision-making and consensus process, integrating evi-dence gathered from preparatory studies . 23 Preparatorystudies included a systematic review of the internationalliterature, 24 patient interviews,25 a worldwide survey wichexperts from different health professions, 26 and a multi-centre study an the clinical applicability of the ICF . 27
To validate the content of ICF Core Sets, the contentcovered in the categories of the CCS was compared tothe content covered in the items of two questionnairesthat apply to HNC: the University of WashingtonQuality of Life questionnaire (UW-QOL) 28 and theEuropean Organization for the Research and Treatmentof Cancer Quality of Life Questionnaire (EORTC-QLQ)modules c30 and hn35 .29 Thev were Chosen because they

676
Journal of Otolaryngology-Head & Neck Surgery, Volume 39, Number 6, 2010
refer to a wide variety of items,' are frequently applied inthe current literature, and are available in differentlanguages, which was necessary for the patients in thismulticentre study .
The CCS and UW-QOL and EORTC questionnaireswere applied to patients in different countries and indifferent departments involved in the treatment of HNC .The aims of this study were (1) to validate the categories ofthe First version of the CCS and BCS and (2) to test fornew, relevant aspects that might haue been missed in theferst version.
Methods
A Cross-sectional study was conducted at different studycentres across the world . The study protocol and consentforms were approved by the Ethics Committee of theUniversity of Munich, Germany, and by the EthicsCommittee or Institutional Review Board at each of thestudy centres. The inclusion criteria for patients were (1)cancer in one of the following locations : oral region,salivary glands, oropharynx, hypopharynx, or larynx ; (2)patients alter cancer treatment; (3) age >_ 18 years ; and (4)signed informed consent .
Data Collection Procedures
Patient recruitment was dope with consecutive sampling .Data collection included patient interviews that were heldby health professionals trained in the ICF at each of thestudy centres . Detailed and precise guidelines for perform-ing the structured interviews were provided by thecoordinating centre in Munich .
Two different questionnaires were used in the study,one for health-professionals and one for patients .Completion of the health professional questionnaire wasbased an a structured patient interview, professionalObservation of the patient, and medical records . After theinterview, patients were asked whether any other relevanthealth topics shq 14 haue B cjscussed during theinterview, and additional topics were documented .Whereas the interviews and the patient questionnaireswere in the patients' native language, the health profes-sional questionnaire was in English and the saure at allstudy centres .
Health Professional Questionnaire
Health professionals completed an English questionnaireincluding all categories of the CCS . The CCS as such is not
an outcome measure and, therefore, does not contain aqualifier scale . The level of impairment or restriction wasassessed according to the ICF qualifier scale 14 as adoptedby the WHO: 0 = no impairmentlrestriction ; 1 = mildimpairmentlrestriction ; 2 = moderate impairmentlrestric-tion; 3 = severe impairment/ restriction ; 4 = completeimpairment/restriction .
For the environmental factors component, each categorycan be either a facilitator or a barrier to the patient . Acomparable 0 to 4 scale was applied, but to denote that acategory is a facilitator, a positive sign was added (eg, +2),and to denote the category as a barrier, a negative sign wasadded (eg, -2) . The Option "not specified" was applied ifthe available Information was not sufficient to quantify theseverity of the problem, and the Option "not applicable" wasapplied if the category was not applicable to the patient . Forimpairments not caused by HNC but by comorbidity,Option C (comorbidity) was Chosen.
At the end of each section, there were two openquestions: (1) What other aspects were relevant to thepatient and haue not been covered with the above items?and (2) What were the most important aspects for thispatient of all the above-mentioned aspects?
Patient Questionnaires
All patients were asked to complete the UW-QOL version 4and the EORTC-QLQ (modules c30 and hn35),28,30-32
Data Preparation
In the health professional questionnaire, the responseoptions "not applicable" and "problem is caused bycomorbidity but not by HNC" were set to 0 and theresponse Option "not specified" was set to "misseng data ."For environmental factors, the prefixes "+" and "-" weredeleted as we only needed to know the extent of relevanceof a category and not to differentiate between barriers andfacilitators .
Analysis
Descriptive statistics were used to characterize the socio-demographic, tumour, and treatment-related characteris-tics of the study population .
Correlation of the UW-QOL and the EORTC-QLQ
To study the validity of the CCS, the items of the UW-QOL and EORTC-QLQ (ie, the questions) were translated
into the language of the ICF according to predefinedlinking rules . 33 ' 34 The correlation of answers to the UW-QOL and EORTC-QLQ (module hn35) items to answersto corresponding ICF categories of the CCS was calculatedbased an Spearman correlation coefficients .
Content Validation of the CCS
To validate the categories of the CCS, the following criteriawere applied : each ICF category that was problematic orrelevant and was caused by HNC (scores 1-4) in at least10% of all patients was considered relevant to Cancerfollow-up and rehabilitation . The category was thereforeconfirmed for inclusion in the CCS . To complement theInformation an frequencies, the median intensity ofimpairment was calculated for each ICF category .
New aspects that were not yet included in the CCS werecaptured in plain English and translated into ICFcategories according to linking rules . 33 ' 34 Frequencies werecalculated for all new aspects .
Content Validation of the BCS
The BCS is a selection of categories from the CCS . 23 The BCSaggregates categories an the second level of the ICFclassification because the second level is suggested for surveysand more general outcome evaluation, whereas the lowerlevels (third and fourth) of the classification are suggested fordetailed specialist evaluation . 14 The lower levels are appliedfor some aspects of the CCS, for example, to differentiatedifferent aspects of food ingestion and swallowing (categoriesb5100-b51052). Accordingly, problems identified at a lowerlevel category of the CCS can be reported at the corre-sponding higher level category of the BCS . For example, allproblems related to category b51050, oral swallowing, fromthe CCS refer to category b510, ingestion function, from theBCS but not the other way around . For assessment of themaximal frequency and intensity of a problem in the BCS(eg, b510, ingestion function) where several lower levelcategories had been collected in the CCS-based question-naire, the lower level category with the most impairment wasChosen for further analyses .
For validation of the BCS, two different analyses weremade:
l . All categories of the CCS that were identified in > 33%of all patients and had a median intensity rating of >25 to 49% (ie, median score 2, "moderate impairment/restriction") qualified for inclusion in the BCS at theircorresponding second-level ICF category .
Tschiesner et al, Validation ICF Core Sets for Head and Neck Cancer 677
z. Based an the open questions in the Interviews, themost important problems were captured for bodyfunctions (b) ; body structures(s), activities, andparticipation (d) ; and environmental factors (e),separately .
Date collection was based an Access for Windows. Allanalyses were made with Excel and SPSS version 15 .0 forWindows (SPSS Inc, Chicago, IL) .
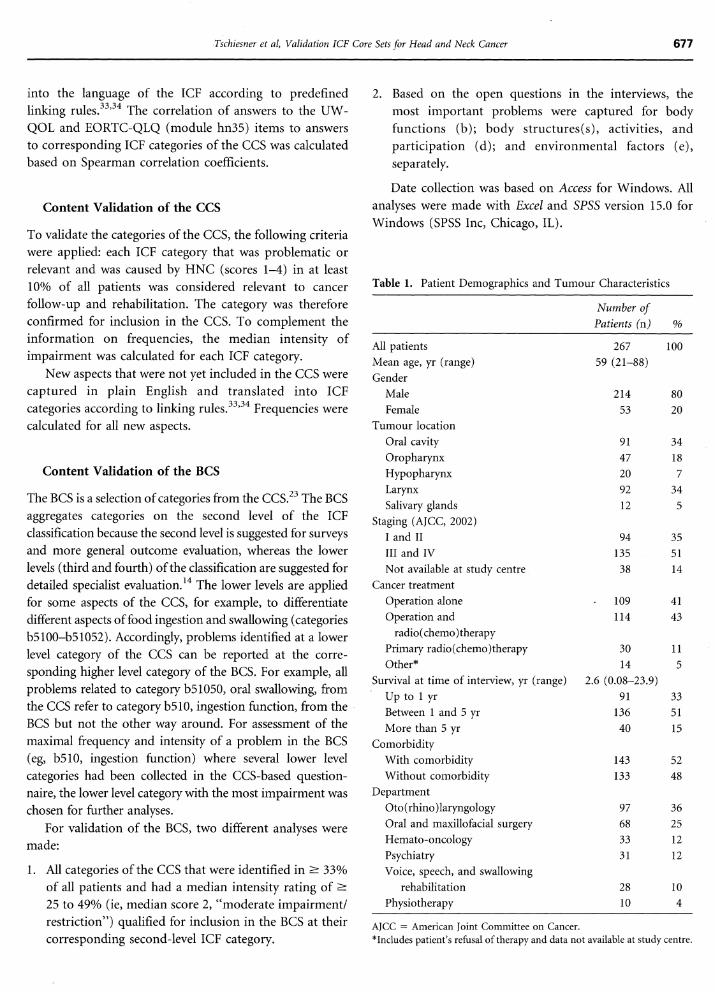
Table 1 . Patient Demographics and Tumour Characteristics
AJCC = American Joint Committee an Cancer .*Includes patient's refusal of therapy and data not available at study centre .
Number ofPatients (n)
All patients
267 100Mean age, yr (range)
59 (21-88)Gender
Male
214 80Female
53 20Tumour location
Oral cavity
91 34Oropharynx
47 18Hypopharynx
20 7Larynx
92 34Salivary glands
12 5
35Staging (AJCC, 2002)
I and II 94III and IV 135 51Not available at study centre 38 14
Cancer treatmentOperation alone
- 109 41Operation and 114 43radio (chemo) therapy
Primary radio(chemo)therapy 30 11Other* 14 5
Survival at time of interview, yr (range)
2 .6 (0 .08-23 .9)Up to 1 yr 91 33Between 1 and 5 yr 136 51More than 5 yr 40 15
ComorbidityWith comorbidity 143 52Without comorbidity 133 48
DepartmentOto(rhino)laryngology 97 36Oral and maxillofacial surgery 68 25Hemato-oncology 33 12Psychiatry 31 12Voice, speech, and swallowing
rehabilitation 28 10Physiotherapy 10 4
678
Journal of Otolaryngology-Head & Neck Surgery, Volume 39, Number 6, 2010
ResultsBetween February 2008 and January 2009, a convenienceSample of 267 patients was interviewed at 14 study centres in11 countries: 33 patients were interviewed in Seoul, Korea,31 patients in Seville, Spain, and 15 patients in Rehovot,Israel. Another 14 patients were included each in Sao Paolo,Brazil, and Patras, Greece . Thirteen patients were includedat Bialystok, Poland, and 10 patients were interviewed eachin New Orleans, Louisiana, and Munipal, India . Sevenpatients were included in Canberra, Australia, and fourpatients at Aintree, United Kingdom . A total of 116 patientswere interviewed at four different study centres in Germany :47 at Munich University, 34 in Klinikum Nuernberg, 20 atHomburg University, and 15 at Heidelberg University .
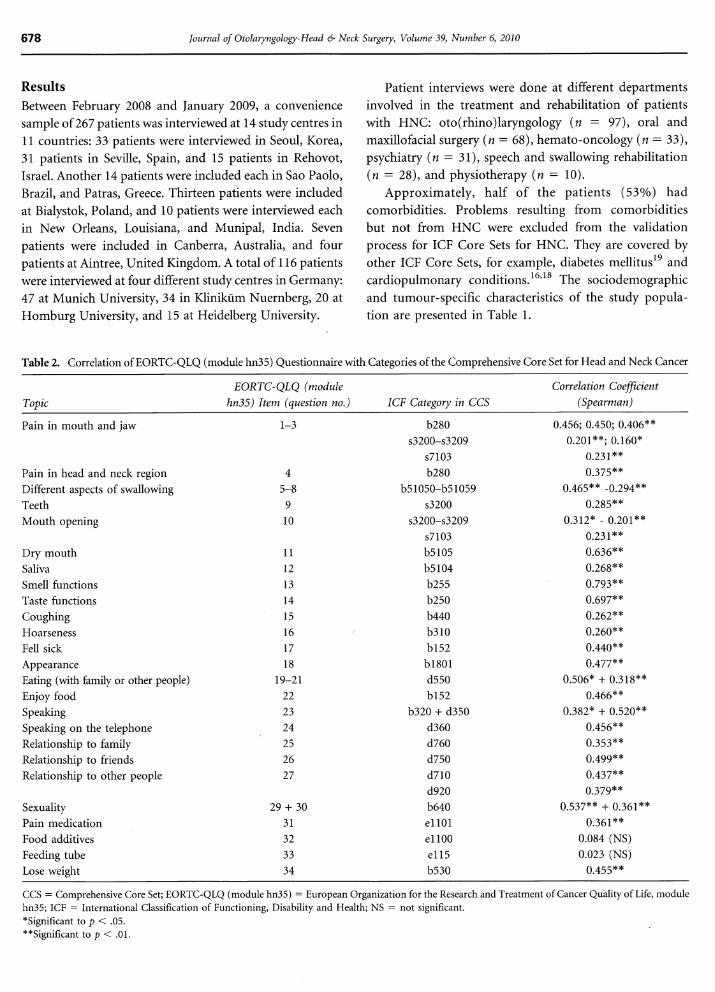
Table 2 . Correlation of EORTC-QLQ (module hn35) Questionnaire with Categories of the Comprehensive Core Set for Head and Neck Cancer
Patient Interviews were dope at different departmentsinvolved in the treatment and rehabilitation of patientswith HNC: oto(rhino)laryngology (n = 97), oral andmaxillofacial surgery (n = 68), hemato-oncology (n = 33),psychiatry (n = 31), Speech and swallowing rehabilitation(n = 28), and physiotherapy (n = 10) .
Approximately, half of the patients (53%) hadcomorbidities . Problems resulting from comorbiditiesbut not from HNC were excluded from the validationprocess for ICF Core Sets for HNC . They are covered byother ICF Core Sets, for example, diabetes mellitus 19 andcardiopulmonary conditions . 16,18 The sociodemographicand tumour-specific characteristics of the study popula-tion are presented in Table 1 .
CCS = Comprehensive Core Set ; EORTC-QLQ (module hn35) = European Organization for the Research and Treatment of Cancer Quality of Life, modulehn35 ; ICF = International Classification of Functioning, Disability and Health ; NS = not significant .*significant to p < .05.**significant to p < .01 .
TopicEORTC-QLQ (module
hn35) Item (question no. ICF Category in CCSCorrelation Coefcient
(Spearman)
Pain in mouth and jaw 1-3 b280 0.456 ; 0 .450 ; 0 .406**s3200-s3209 0.201** ; 0 .160*
s7103 0.231**Pain in head and neck region 4 b280 0.375**Different aspects of swallowing 5-8 b51050-b51059 0.465** -0.294**Teetb 9 s3200 0.285**Mouth opening 10 s3200-s3209 0312* - 0.201**
s7103 0.231**Dry mouth 11 b5105 0.636**Saliva 12 b5104 0.268**Smell functions 13 b255 0.793**Taste functions 14 b250 0.697**Coughing 15 b440 0.262**Hoarseness 16 b310 0.260**Fell sick 17 b152 0.440**Appearance 18 b1801 0.477**Eating (wich family or other people) 19-21 d550 0.506* + 0.318**Enjoy food 22 b152 0.466**Speaking 23 b320 + d350 0.382* + 0.52 0**Speaking an the telephone 24 d360 0.456**Relationship to family 25 d760 0.353**Relationship to friends 26 d750 0.499**Relationship to other people 27 d710 0.437**
d920 0.379**Sexuality 29+30 b640 0.537** + 0.361**Pain medication 31 e1101 0.361**Food additives 32 e1100 0.084 (NS)Feeding tube 33 e115 0.023 (NS)Lose weight 34 b530 0.455**
Correlation with the EORTC-QLQ and the UW-QOL
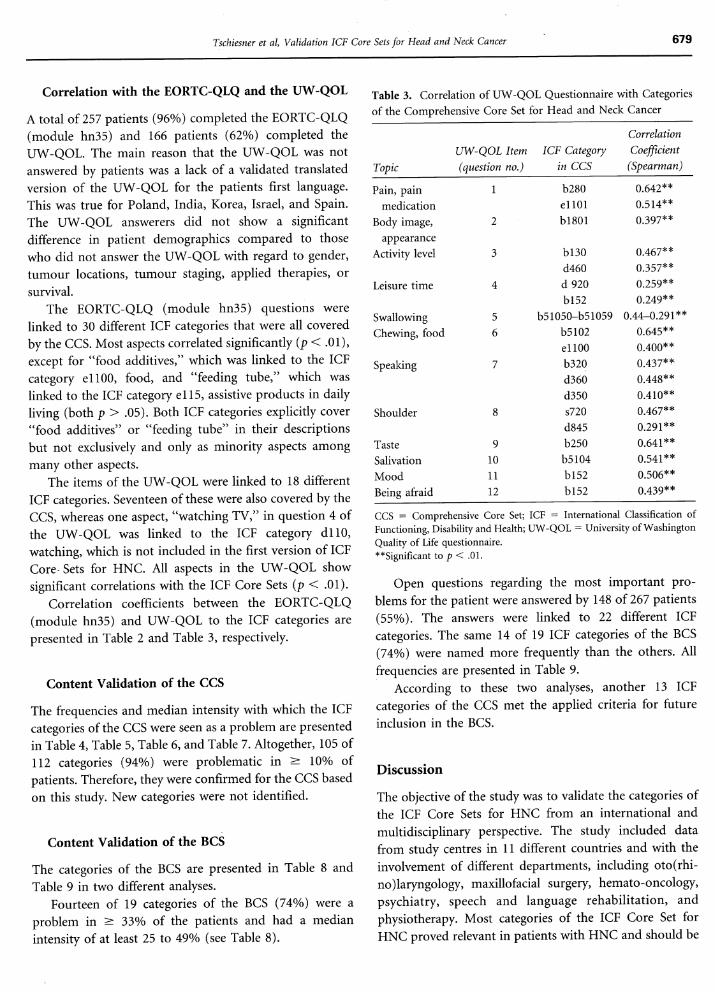
A total of 257 patients (96%) completed the EORTC-QLQ(module hn35) and 166 patients (62%) completed theUW-QOL. The main reason that the UW-QOL was notanswered by patients was a lack of a validated translatedversion of the UW-QOL for the patients First language .This was true for Poland, India, Korea, Israel, and Spain .The UW-QOL answerer did not show a significantdifference in patient demographics compared to thosewho did not answer the UW-QOL with regard to gender,tumour locations, tumour staging, applied therapies, orsurvival .
The EORTC-QLQ (module hn35) questions werelinked to 30 different ICF categories that were all coveredby the CCS . Most aspects correlated significantly (p < .01),except for "food additives," which was linked to the ICFcategory e1100, food, and "feeding tube," which waslinked to the ICF category e115, assistive products in dailyliving (both p > .05) . Both ICF categories explicitly cover"food additives" or "feeding tube" in their descriptionsbut not exclusively and only as minority aspects amongmang other aspects .
The items of the UW-QOL were linked to 18 differentICF categories . Seventeen of these were also covered by theCCS, whereas one aspect, "watching TV," in question 4 ofthe UW-QOL was linked to the ICF category dl 10,watching, which is not included in the ferst version of ICFCore Sets for HNC . All aspects in the UW-QOL showsignificant correlations with the ICF Core Sets (p < .01) .
Correlation coefficients between the EORTC-QLQ(module hn35) and UW-QOL to the ICF categories arepresented in Table 2 and Table 3, respectively .
Content Validation of the CCS
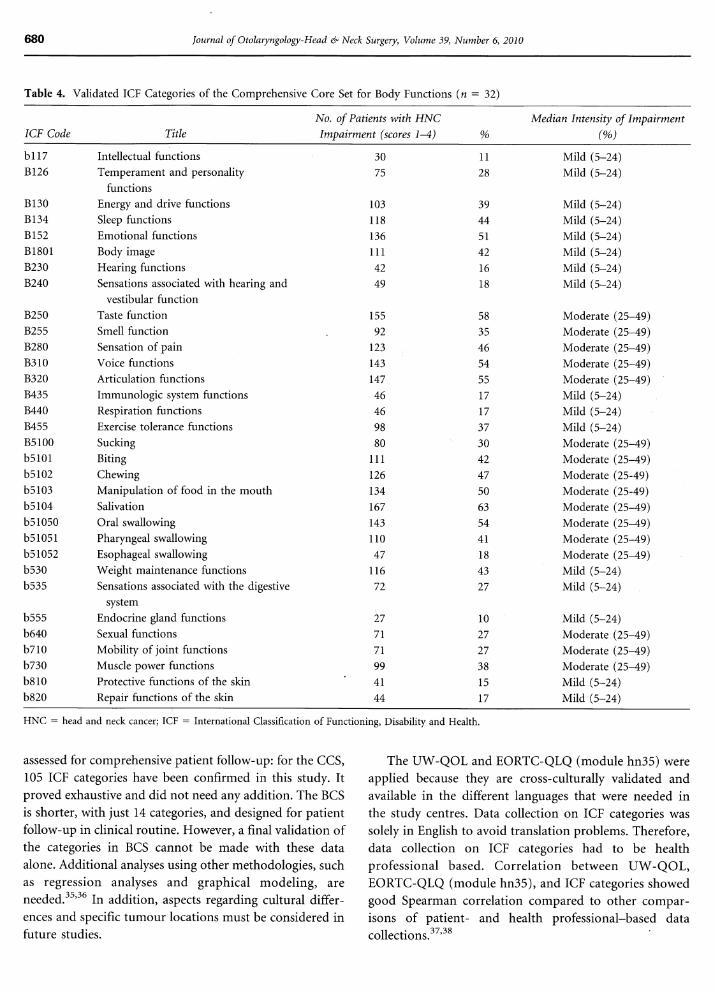
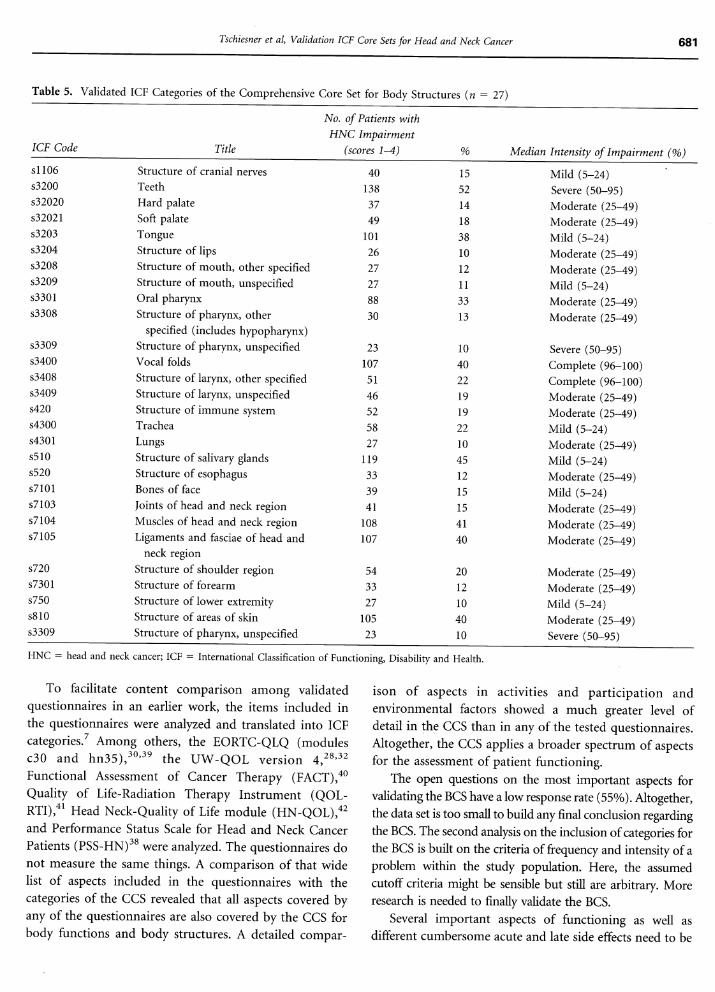
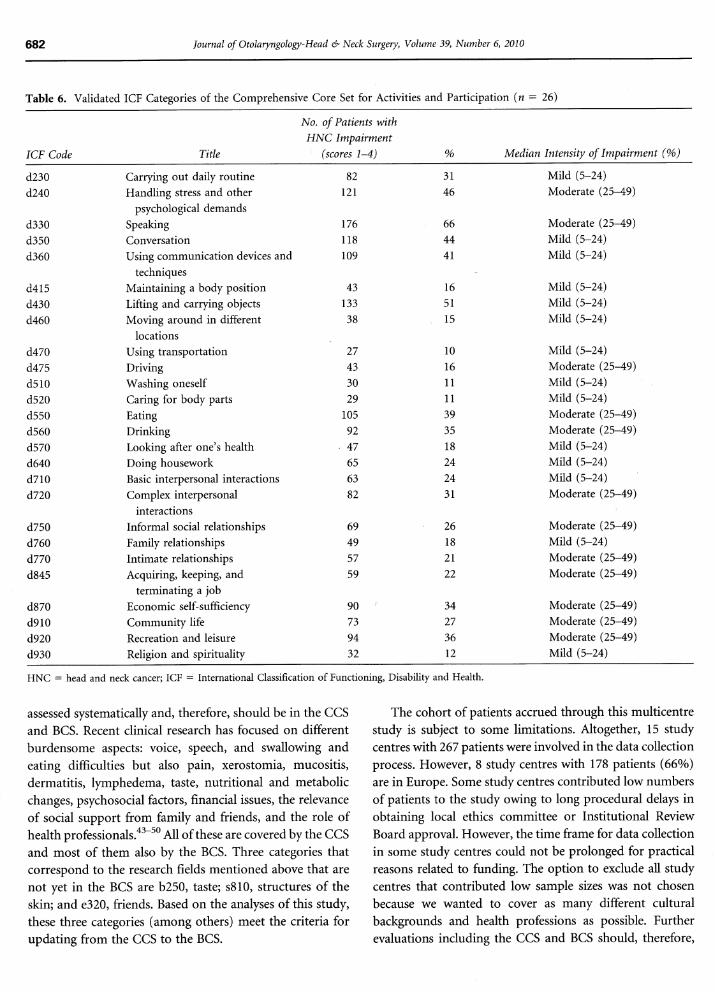
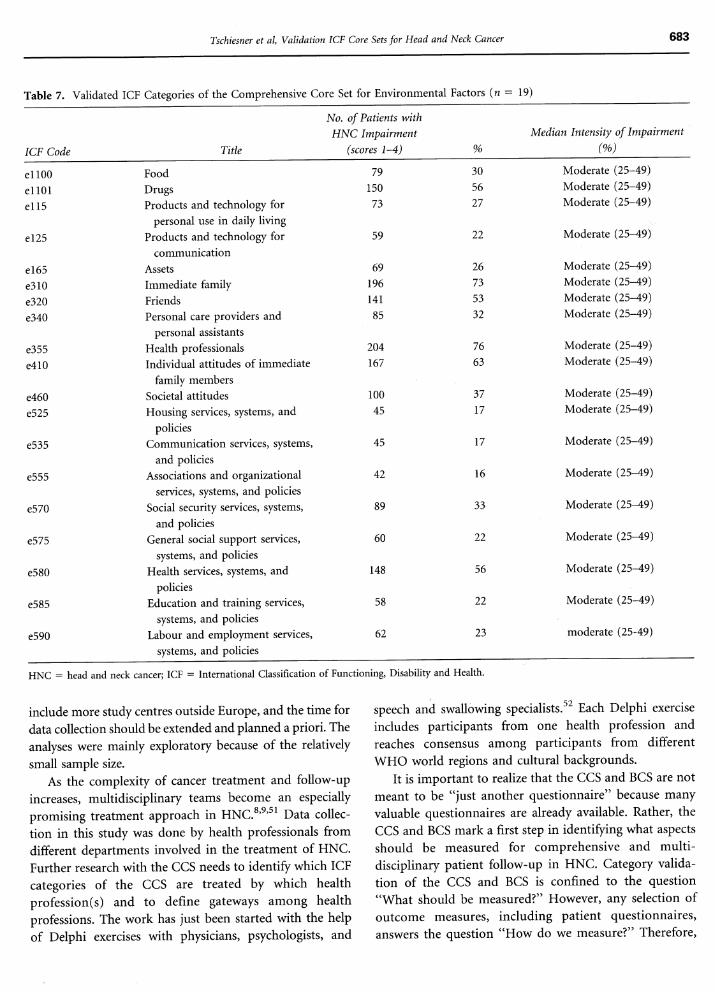
The frequencies and median intensity with which the ICFcategories of the CCS were seen as a problem are presentedin Table 4, Table 5, Table 6, and Table 7 . Altogether,105 of112 categories (94%) were problematic in ? 10% ofpatients. Therefore, they were confirmed for the CCS basedan this study. New categories were not identified .
Content Validation of the BCS
The categories of the BCS are presented in Table 8 andTable 9 in two different analyses.
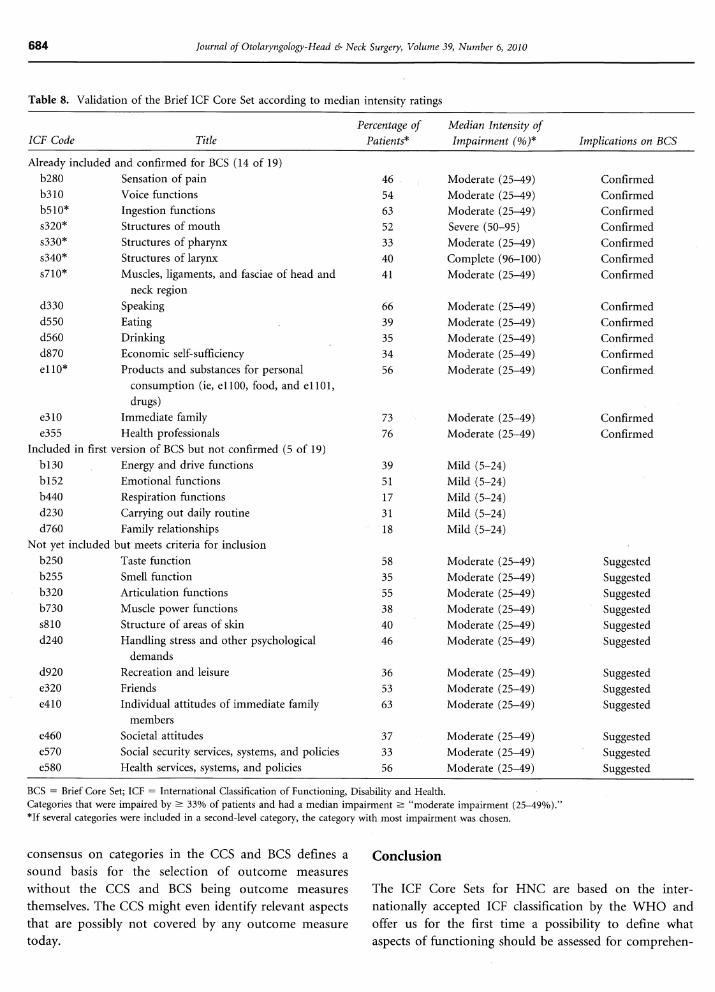
Fourteen of 19 categories of the BCS (74%) were aproblem in ? 33% of the patients and had a medianintensity of at least 25 to 49% (see Table 8) .
Tschiesner et al, Validation ICF Core Sets for Head and Neck Cancer 679
Table 3. Correlation of UW-QOL Questionnaire with Categoriesof the Comprehensive Core Set for Head and Neck Cancer
CCS = Comprehensive Core Set; ICF = International Classification ofFunctioning, Disability and Health; UW-QOL = University of WashingtonQuality of Life questionnaire .**Significant to p < .01 .
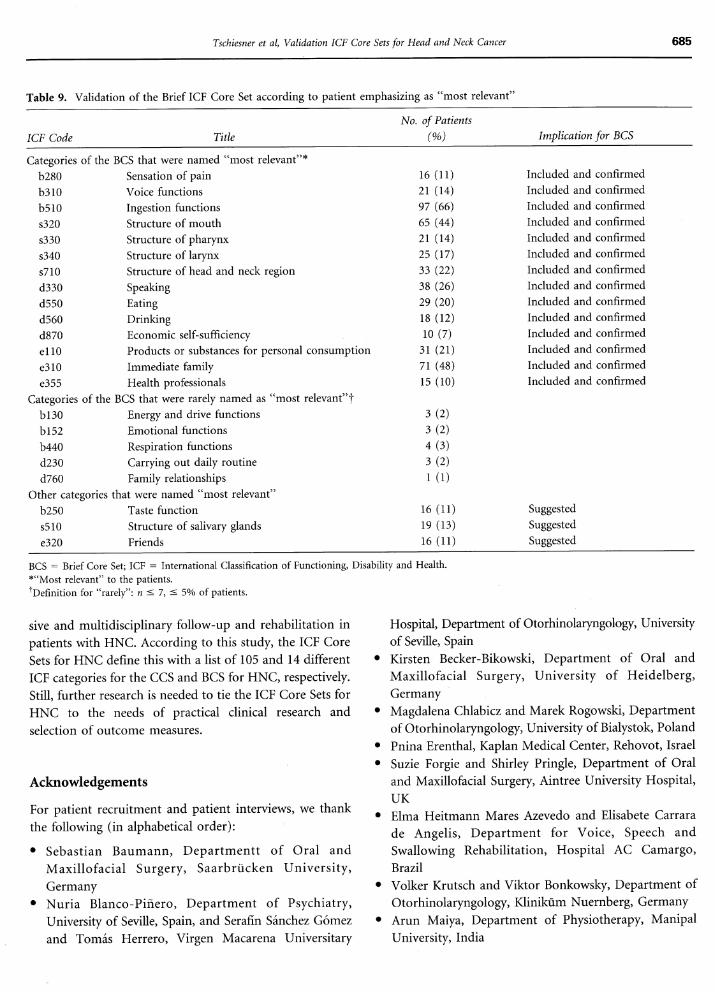
Open questions regarding the most important pro-blems for the patient were answered by 148 of 267 patients(55%) . The answers were linked to 22 different ICFcategories. The saure 14 of 19 ICF categories of the BCS(74%) were named more frequently than the others . Allfrequencies are presented in Table 9 .
According to these two analyses, another 13 ICFcategories of the CCS met the applied criteria for futureinclusion ' in the BCS .
Discussion
The objective of the study was to validate the categories ofthe ICF Core Sets for HNC from an international andmultidisciplinary perspective. The study included datafrom study centres in 11 different countries and with theinvolvement of different departments, including oto(rhi-no)laryngology, maxillofacial surgery, hemato-oncology,psychiatry, speech and language rehabilitation, andphysiotherapy. Most categories of the ICF Core Set forHNC proved relevant in patients wich HNC and should be
TopicUW-QOL Item(question no .)
ICF Categoryin CCS
CorrelationCoefcient(Spearman)
Pain, pain 1 b280 0.642**medication e1101 0.514**
Body Image, 2 b1801 0.397**appearance
Activity level 3 b130 0.467**d460 0.357**
Leisure time 4 d 920 0.259**b152 0.249**
Swallowing 5 b51050-b51059 0.44-0.291**Chewing, food 6 b5102 0.645**
e1100 0.400**Speaking 7 b320 0.437*
d360 0.448**d350 0.410**
Shoulder 8 s720 0.467**d845 0.291**
Taste 9 b250 0.641**Salivation 10 b5104 0.541**Mood 11 b152 0.506**Being afraid 12 b152 0.439**
680
Journal of Otolaryngology-Head & Neck Surgery, Volume 39, Number 6, 2010
Table 4. Validated ICF Categories of the Comprehensive Core Set for Body Functions (n = 32)
HNC = head and neck cancer; ICF = International Classification of Functioning, Disability and Health.
assessed for comprehensive patient follow-up: for the CCS,105 ICF categories haue been confirmed in this study. l tproved exhaustive and did not need any addition . The BCSis shorter, with just 14 categories, and designed for patientfollow-up in clinical routine. However, a final validation ofthe categories in BCS cannot be made with these dataalone. Additional analyses using other methodologies, suchas regression analyses and graphical modeling, areneeded . 35,36 In addition, aspects regarding cultural differ-ences and specific tumour locations raust be considered inFuture studies .
The UW-QOL and EORTC-QLQ (module hn35) wereapplied because they are Cross-culturally validated andavailable in the different languages that were needed inthe study centres . Data collection an ICF categories wassolely in English to avoid translation problems . Therefore,data collection an ICF categories had to be healthprofessional based . Correlation between UW-QOL,EORTC-QLQ (module hn35), and ICF categories showedgood Spearman correlation compared to other compar-isons of patient- and health professional-based datacollections . 3'' 3s
ICF Code TitleNo. of Patients with HNCImpairment (scores 1-4) %
Median Intensity of Impairment(%)
bi 17 Intellectual functions 30 11 Mild (5-24)B126 Temperament and personality
functions75 28 Mild (5-24)
B130 Energy and drive functions 103 39 Mild (5-24)B134 Sleep functions 118 44 Mild (5-24)B152 Emotional functions 136 51 Mild (5-24)B1801 Body Image 111 42 Mild (5-24)B230 Hearing functions 42 16 Mild (5-24)B240 Sensations associated with Kearing and
vestibular function49 18 Mild (5-24)
B250 Taste function 155 58 Moderate (25-49)B255 Smell function 92 35 Moderate (25-49)B280 Sensation of pain 123 46 Moderate (25-49)B310 Voice functions 143 54 Moderate (25-49)B320 Articulation functions 147 55 Moderate (25-49)B435 Immunologic system functions 46 17 Mild (5-24)B440 Respiration functions 46 17 Mild (5-24)B455 Exercise tolerance functions 98 37 Mild (5-24)B5100 Sucking 80 30 Moderate (25-49)b5101 Biting 111 42 Moderate (25-49)b5102 Chewing 126 47 Moderate (25-49)b5103 Manipulation of food in the mouth 134 50 Moderate (25-49)b5104 Salivation 167 63 Moderate (25-49)b51050 Oral swallowing 143 54 Moderate (25-49)b51051 Pharyngeal swallowing 110 41 Moderate (25-49)b51052 Esophageal swallowing 47 18 Moderate (25-49)b530 Weight maintenance functions 116 43 Mild (5-24)b535 Sensations associated wich the digestive
system72 27 Mild (5-24)
b555 Endocrine gland functions 27 10 Mild (5-24)b640 Sexual functions 71 27 Moderate (25-49)b710 Mobility of Joint functions 71 27 Moderate (25-49)b730 Muscle power functions 99 38 Moderate (25-49)b810 Protective functions of the skin 41 15 Mild (5-24)b820 Repair functions of the skin 44 17 Mild (5-24)
Tschiesner et ad, Validation ICF Core Sets for Head and Neck Cancer
Table 5. Validated ICF Categories of the Comprehensive Core Set for Body Structures (n = 27)
HNC = head and neck Cancer; ICF = International Classification of Functioning, Disability and Health.
To facilitate content comparison among validatedquestionnaires in an earlier work, the items included inthe questionnaires were analyzed and translated into ICFcategories . ? Among others, the EORTC-QLQ (modulesc30 and hn35), 30 ' 39 the UW-QOL version 4,28 '32
Functional Assessment of Cancer Therapy (FACT), 40
Quality of Life-Radiation Therapy Instrument (QOL-RTI), 41 Head Neck-Quality of Life module (HN-QOL), 42
and Performance Status Scale for Head and Neck CancerPatients (PSS-HN) 38 were analyzed . The questionnaires donot measure the saure things . A comparison of that widelist of aspects included in the questionnaires with thecategories of the CCS revealed that all aspects covered byany of the questionnaires are also covered by the CCS forbody functions and body structures . A detailed compar-
681
ison of aspects in activities and participation andenvironmental factors showed a muck greater level ofdetail in the CCS than in any of the tested questionnaires .Altogether, the CCS applies a broader spectrum of aspectsfor the assessment of patient functioning.
The open questions an the most important aspects forvalidating the BCS haue a low response rate (55%) . Altogether,the data set is too small to build any final conclusion regardingthe BCS . The second analysis an the inclusion of categories forthe BCS is built an the criteria of frequency and intensity of aproblem within the study population . Here, the assumedGutoff criteria might be sensible but still are arbitrary . Moreresearch is needed to finally validate the BCS .
Several important aspects of functioning as well asdifferent cumbersome acute and late side effects need to be
ICF Code Title
No. of Patients withHNC Impairment
(scores 1-4) Median Intensity of Impairment (%)s1106 Structure of cranial nerves 40 15 Mild (5-24)s3200 Teeth 138 52 Severe (50-95)s32020 Hard palate 37 14 Moderate (25-49)s32021 Soft palate 49 18 Moderate (25-49)s3203 Tongue 101 38 Mild (5-24)s3204 Structure of lips 26 10 Moderate (25-49)s3208 Structure of mouth, other specified 27 12 Moderate (25-49)s3209 Structure of mouth, unspecified 27 11 Mild (5-24)s3301 Oral pharynx 88 33 Moderate (25-49)s3308 Structure of pharynx, other
specified (includes hypopharynx)30 13 Moderate (25-49)
s3309 Structure of pharynx, unspecified 23 10 Severe (50-95)s3400 Vocal folds 107 40 Complete (96-100)s3408 Structure of larynx, other specified 51 22 Complete (96-100)s3409 Structure of larynx, unspecified 46 19 Moderate (25-49)s420 Structure of immune System 52 19 Moderate (25-49)s4300 Trachea 58 22 Mild (5-24)s4301 Lungs 27 10 Moderate (25-49)s510 Structure of salivary glands 119 45 Mild (5-24)s520 Structure of esophagus 33 12 Moderate (25-49)s7101 Bones of face 39 15 Mild (5-24)s7103 Joints of head and neck region 41 15 Moderate (25-49)s7104 Muscles of head and neck region 108 41 Moderate (25-49)s7105 Ligaments and fasciae of head and
neck region107 40 Moderate (25-49)
s720 Structure of shoulder region 54 20 Moderate (25-49)s7301 Structure of forearm 33 12 Moderate (25-49)s750 Structure of lower extremity 27 10 Mild (5-24)s810 Structure of areas of skin 105 40 Moderate (25-49)s3309 Structure of pharynx, unspecified 23 10 Severe (50-95)
682
assessed systematically and, therefore, should be in the CCSand BCS. Recent clinical research has focused an differentburdensome aspects : voice, speech, and swallowing andeating difficulties but also pain, xerostomia, mucositis,dermatitis, lymphedema, taste, nutritional and metabolicchanges, psychosocial factors, financial issues, the relevanceof social support from family and friends, and the role ofhealth professionals.43-5o All of these are covered by the CCSand most of them also by the BCS . Three categories thatcorrespond to the research fields mentioned above that arenot yet in the BCS are b250, taste ; s810, structures of theskin; and e320, friends . Based an the analyses of this study,these three categories (among others) meet the criteria forupdating from the CCS to the BCS .
Journal of Otolaryngology-Head & Neck Surgery, Volume 39, Number 6, 2010
Table 6. Validated ICF Categories of the Comprehensive Core Set for Activities and Participation (n = 26)
HNC = head and neck cancer; ICF = International Classification of Functioning, Disability and Health.
The cohort of patients accrued through this multicentrestudy is subject to some limitations. Altogether, 15 studycentres with 267 patients were involved in the data collectionprocess. However, 8 study centres with 178 patients (66%)are in Europe . Some study centres contributed low numbersof patients to the study owing to long procedural delays inobtaining local ethics committee or Institutional ReviewBoard approval . However, the time frame for data collectionin some study centres Gould not be prolonged for practicalreasons related to funding . The Option to exclude all studycentres that contributed low sample sizes was not Chosenbecause we wanted to cover as many different culturalbackgrounds and health professions as possible . Furtherevaluations including the CCS and BCS should, therefore,
ICF Code Title
No. of Patients withHNC Impairment
(scores 1-4) % Median Intensity of Impairment (%)
d230 Carrying out daily routine 82 31 Mild (5-24)
d240 Handling stress and otherpsychological demands
121 46 Moderate (25-49)
d330 Speaking 176 66 Moderate (25-49)
d350 Conversation 118 44 Mild (5-24)
d360 Using communication devices andtechniques
109 41 Mild (5-24)
d415 Maintaining a body position 43 16 Mild (5-24)d430 Lifting and carrying objects 133 51 Mild (5-24)
d460 Moving around in differentlocations
38 15 Mild (5-24)
d470 Using transportation 27 10 Mild (5-24)d475 Driving 43 16 Moderate (25-49)d510 washing oneself 30 11 Mild (5-24)d520 Caring for body parts 29 11 Mild (5-24)d550 Eating 105 39 Moderate (25-49)d560 Drinking 92 35 Moderate (25-49)d570 Looking alter one's health 47 18 Mild (5-24)d640 Doing housework 65 24 Mild (5-24)d710 Basic interpersonal interactions 63 24 Mild (5-24)d720 Complex interpersonal
interactions82 31 Moderate (25-49)
d750 Informal social relationships 69 26 Moderate (25-49)d760 Family relationships 49 18 Mild (5-24)d770 Intimate relationships 57 21 Moderate (25-49)d845 Acquiring, keeping, and
terminating a job59 22 Moderate (25-49)
d870 Economic seif-sufficiency 90 34 Moderate (25-49)d910 Community life 73 27 Moderate (25-49)d920 Recreation and leisure 94 36 Moderate (25-49)d930 Religion and spirituality 32 12 Mild (5-24)
Tschiesner et al, Validation ICF Core Sets for Head and Neck Cancer
Table 7. Validated ICF Categories of the Comprehensive Core Set for Environmental Factors (n = 19)
HNC - head and neck cancer; ICF - International Classification of Functioning, Disability and Health .
include more study centres outside Europe, and the time fordata collection should be extended and planned a priori. Theanalyses were mainly exploratory because of the relativelysmall sample size .
As the complexity of cancer treatment and follow-upincreases, multidisciplinary teams become an especiallypromising treatment approach in HNC . 8 '9' 5 ' Data collec-tion in this study was dope by health professionals fromdifferent departments involved in the treatment of HNC .Further research with the CCS needs to identify which ICFcategories of the CCS are treated by which healthprofession(s) and to define gateways among healthprofessions. The work has just been started with the helpof Delphi exercises with physicians, psychologists, and
683
speech and swallowing specialists . 52 Each Delphi exerciseincludes participants from one health profession andreaches consensus among participants from differentWHO world regions and cultural backgrounds .
lt is important to realize that the CCS and BCS are notmeant to be "just another questionnaire" because mangvaluable questionnaires are already available . Rather, theCCS and BCS mark a first step in identifying what aspectsshould be measured for comprehensive and multi-disciplinary patient follow-up in HNC. Category valida-tion of the CCS and BCS is confined to the question"What should be measured?" However, any selection ofoutcome measures, including patient questionnaires,answers the question "How do we measure?" Therefore,
ICF Code Title
No, of Patients withHNC Impairment
(scores 1-4) %Median Intensity of Impairment
(%)
e1100 Food 79 30 Moderate (25-49)
e1101 Drugs 150 56 Moderate (25-49)
e115 Products and technology forpersonal use in daily living
73 27 Moderate (25-49)
e125 Products and technology forcommunication
59 22 Moderate (25-49)
e165 Assets 69 26 Moderate (25-49)
e310 Immediate family 196 73 Moderate (25-49)
e320 Friends 141 53 Moderate (25-49)
e340 Personal care providers andpersonal assistants
85 32 Moderate (25-49)
e355 Health professionals 204 76 Moderate (25-49)
e410 Individual attitudes of immediatefamily members
167 63 Moderate (25-49)
e460 Societal attitudes 100 37 Moderate (25-49)
e525 Housing services, systems, andpolicies
45 17 Moderate (25-49)
e535 Communication services, systems,and policies
45 17 Moderate (25-49)
e555 Associations and organizationalservices, systems, and policies
42 16 Moderate (25-49)
e570 Social security services, systems,and policies
89 33 Moderate (25-49)
e575 General social support services,systems, and policies
60 22 Moderate (25-49)
e580 Health services, systems, andpolicies
148 56 Moderate (25-49)
e585 Education and training services,systems, and policies
58 22 Moderate (25-49)
e590 Labour and employment services,systems, and policies
62 23 moderate (25-49)
684
Journal of Otolaryngology-Head & Neck Surgery, Volume 39, Number 6, 2010
Table B. Validation of the Brief ICF Core Set according to median intensity ratings
consensus an categories in the CCS and BCS defines asound basis for the selection of outcome measureswithout the CCS and BCS being outcome measuresthemselves. The CCS might even identify relevant aspectsthat are possibly not covered by any outcome measuretoday .
Conclusion
The ICF Core Sets for HNC are based an the inter-nationally accepted ICF classification by the WHO andoffer us for the firnt time a possibility to define whataspects of functioning should be assessed for comprehen-
BCS = Brief Core Set ; ICF = International Classification of Functioning, Disability and Health .Categories that were impaired by ? 33% of patients and had a median impairment ? "moderate impairment (25-49%) ."*If several categories were included in a second-level category, the category with most impairment was Chosen .
ICF Code TitlePercentage ofPatients*
Median Intensity ofImpairment (%)* Implications an BCS
Already included andb280
confirmed for BCS (14 of 19)Sensation of pain 46 Moderate (25-49) Confirmed
b310 Voice functions 54 Moderate (25-49) Confirmedb510* Ingestion functions 63 Moderate (25-49) Confirmeds320* Structures of mouth 52 Severe (50-95) Confirmeds330* Structures of pharynx 33 Moderate (25-49) Confirmeds340* Structures of larynx 40 Complete (96-100) Confirmeds710* Muscles, ligaments, and fasciae of head and 41 Moderate (25-49) Confirmed
d330neck region
Speaking 66 Moderate (25-49) Confirmedd550 Eating 39 Moderate (25-49) Confirmedd560 Drinking 35 Moderate (25-49) Confirmedd870 Economic seif-sufficiency 34 Moderate (25-49) Confirmede110* Products and substances for personal 56 Moderate (25-49) Confirmed
e310
consumption (ie, e1100, food, and e1101,drugs)
Immediate family 73 Moderate (25-49) Confirmede355 Health professionals 76 Moderate (25-49) Confirmed
Included in firnt versionb130
of BCS but not confirmed (5 of 19)Energy and drive functions 39 Mild (5-24)
b152 Emotional functions 51 Mild (5-24)b440 Respiration functions 17 Mild (5-24)d230 Carrying out daily routine 31 Mild (5-24)d760 Family relationships 18 Mild (5-24)
Not yet included butb250
meets criteria for inclusionTaste function 58 Moderate (25-49) Suggested
b255 Smell function 35 Moderate (25-49) Suggestedb320 Articulation functions 55 Moderate (25-49) Suggestedb730 Muscle power functions 38 Moderate (25-49) Suggesteds810 Structure of areas of skin 40 Moderate (25-49) Suggestedd240 Handling stress and other psychological 46 Moderate (25-49) Suggested
d920Jemands
Recreation and leisure 36 Moderate (25-49) Suggestede320 Friends 53 Moderate (25-49) Suggestede410 Individual attitudes of immediate family 63 Moderate (25-49) Suggested
e460members
Societal attitudes 37 Moderate (25-49) Suggestede570 Social security services, systems, and policies 33 Moderate (25-49) Suggestede580 Health services, systems, and policies 56 Moderate (25-49) Suggested
Tschiesner et al, Validation ICF Core Sets for Head and Neck Cancer
Table 9. Validation of the Brief ICF Core Set according to patient emphasizing as "most relevant"
BCS = Brief Core Set ; ICF = International Classification of Functioning, Disability and Health .*"Most relevant" to the patients .tDefinition for "rarely" : n
7, < 5% of patients.
sive and multidisciplinary follow-up and rehabilitation inpatients with HNC. According to this study, the ICF CoreSets for HNC define this with a list of 105 and 14 differentICF categories for the CCS and BCS for HNC, respectively.Still, further research is needed to tie the ICF Core Sets forHNC to the needs of practical clinical research andselection of outcome measures .
Acknowledgements
For patient recruitment and patient Interviews, we thankthe following (in alphabetical Order) :
• Sebastian Baumann, Departmentt of Oral andMaxillofacial Surgery, Saarbrücken University,Germany
• Nuria Blanco-Pinero, Department of Psychiatry,University of Seville, Spain, and Serahn Sänchez G6mezand Tomäs Herrero, Virgen Macarena Universitary
685
Hospital, Department of Otorhinolaryngology, Universityof Seville, Spain
•
Kirsten Becker-Bikowski, Department of Oral andMaxillofacial Surgery, University of Heidelberg,Germany
•
Magdalena Chlabicz and Marek Rogowski, Departmentof Otorhinolaryngology, University of Bialystok, Poland
•
Pnina Erenthal, Kaplan Medical Center, Rehovot, Israel•
Suzie Forgie and Shirley Pringle, Department of Oraland Maxillofacial Surgery, Aintree University Hospital,UK
• Elma Heftmann Mares Azevedo and Elisabete Carrarade Angelfis, Department for Voice, Speech andSwallowing Rehabilitation, Hospital AC Camargo,Brazil
•
Volker Krutsch and Viktor Bonkowsky, Department ofOtorhinolaryngology, Klinikum Nuernberg, Germany
•
Arun Maiya, Department of Physiotherapy, ManipalUniversity, India
ICF Code TitleNo. of Patients
(%) Implication for BCS
Categories of the BCSb280
that were named "most relevant"Sensation of pain 16 (11) Included and confirmed
b310 Voice functions 21(14) Included and confirmed
b510 Ingestion functions 97 (66) Included and confirmed
s320 Structure of mouth 65 (44) Included and confirmed
s330 Structure of pharynx 21(14) Included and confirmed
s340 Structure of larynx 25 (17) Included and confirmed
s710 Structure of head and neck region 33 (22) Included and confirmed
d330 Speaking 38 (26) Included and confirmed
d550 Eating 29 (20) Included and confirmed
d560 Drinking 18 (12) Included and confirmed
d870 Economic seif sufficiency 10 (7) Included and confirmed
e110 Products or substances for personal consumption 31(21) Included and confirmed
e310 Immediate family 71(48) Included and confirmed
e355 Health professionals 15 (10) Included and confirmed
Categories of the BCSb130
that were rarely named as "most relevant"tEnergy and drive functions 3 (2)
b152 Emotional functions 3 (2)b440 Respiration functions 4 (3)d230 Carrying out daily routine 3 (2)d760 Family relationships 1 (1)
Other categories thatb250
were named "most relevant"Taste function 16 (11) Suggested
s510 Structure of salivary glands 19 (13) Suggested
e320 Friends 16 (11) Suggested
686
•
Megan Nutt, ACT Health, Capital Region CancerService, Head and Neck Oncology, Australia
•
Ilias Papathanasiou, Department of Speech andLanguage Therapy, Technological EducationalInstitute of Patras, Greece
• Yehon Hee Park and Keunchil Park, Department ofHematology-Oncology, Sämsung Medical Center,Korea
• Lena Schuster, Department of Otorhinolaryngology andOral and Maxillofacial Surgery, Munich University,Germany
• Rohan R. Walvekar, Department of OtolaryngologyHead and Neck Surgery, LSU Health Sciences Center,LA
Financial disclosure of authors : A workplace tocoordinate the different study centres was funded byDeutsche Krebshilfe e .V .
Financial disclosure of reviewers : None reported.
References
1 . Verdonck-de Leeuw I, de Bree R, Keizer A, et al . Computerizedprospective screening for high levels of emotional distress in headand neck cancer patients and referral rate to psychosocial care .Oral Oncol 2009 Apr B . [Epub ahead of print]
2 . El-Deiry M, Futran N, McDowell J, et al. Influences and predictorsoflong-term quality of life in head and neck cancer survivors. ArchOtolaryngol Head Neck Surg 2009;135 :380-4 .
3 . Kanatas A, Mehanna H, Lowe D, et al. A second national survey ofhealth-related quality of life questionnaires in head and neckoncology. Ann R Coll Surg Eng! 2009;91 :420-5 .Cognetti D, Weber R, Lai S. Head and neck cancer : an evolvingtreatment paradigm . Cancer 2008 ;l13 :1911-32 .
5 . Martino R, Ringash J . Evaluation of quality of life and Organfunction in head and neck squamous cell carcinoma . HematolOncol Clin North Am 2008 ;22 :1239-56 .
6 . Langenhoff B, Krabbe P, Wobbes T, et al . Quality of life asan outcome measure in surgical oncology . Br J Surg 2001 ;88 :643-52.
7 . Tschiesner U, Rogers SN, Harreus U, et al . Content comparison ofquality of life questionnaires used in head and neck cancer basedan the International Classification of Functioning, Disability andHealth (ICF): a systematic review. Eur Arch Otorhinolaryngol2008;265 :627-37 .
B . Westin T, Stalfors J. Tumour boards/multidisciplinary head andneck cancer meetings: are they of value to patients, treating staff ora political additional drain an healthcare resources? Curr OpinOtolaryngol Head Neck Surg 2008 ;16 :103-7 .
9 . Fleissig A, Jenkins V, Catt S, et al . Multidisciplinary teams incancer care : are they effective in the UK? Lancet Oncol 2006 ;7:935-43 .
10 . Ledeboer Q, Velden L, Boer M, et al. Physical and psychosocialcorrelates of head and neck cancer: an update of the literature andchallenges for the future (1996-2003) . Clin Otolaryngol 2005;30:303-19.
Journal of Otolaryngology-Head & Neck Surgery, Volume 39, Number 6, 2010
11 . Mlynarek A, Rieger J, Harns J, et al . Methods of functionaloutcomes assessment following treatment of oral and orophar-yngeal cancer: review of the literature. J Otolaryngol Head NeckSurg 2008 ;37 :2-10 .
12 . Trotti A, Bentzen S. The need for adverse effects reportingstandards in oncology clinical trials. J Clin Oncol 2004;22 :19-22 .
13 . Tschiesner U, Cieza A, Rogers S, et al . Developing Core Sets forpatients with head and neck cancer based an the InternationalClassification of Functioning, Disability and Health (ICF) . EurArch Otorhinolaryngol 2007;264 :1215-22 .
14 . World Health Organization . ICF - International Classification ofFunctioning, Disability and Health. Geneva: World HealthOrganization ; 2001 .
15 . Cieza A, Ewert T, Üstün B, et al . Develpment ofICF Core Sets forpatients with chronic conditions . J Rehabil Med Suppl 2004 ;44 :9-11 .
16 . Boldt C, Grill E, Wildner M, et al. ICF Core Set for patients withcardiopulmonary conditions in the acute hospital . Disabil Rehabil2005;27:375-80.
17 . Cieza A, Stucki G, Weigl M, et al . ICF Core Set for low back pain .J Rehabil Med Suppl 2004;44:69-74.
18 . Cieza A, Stucki A, Geyh S, et al. ICF Core Set for chronic ischemicheart disease. J Rehab Med Suppl 2004 ;44 :94-9 .
19 . Ruof J, Cieza A, Wolff B, et al. ICF Core Set for diabetes mellitus .J Rehabil Med Suppl 2001 ;44 :100-6 .
20 . Stucki A, Stoll T, Cieza A, et al . ICF Core Sets for obstructivepulmonary disease. J Rehabil Med Suppl 2004 ;44 :114-20 .
21 . Geyh S, Cieza A, Schnuten J, et al . ICF Core Sets for stroke.J Rehabil Med Suppl 2004;44 Suppl:135-41 .
22 . Brach M, Cieza A, Stucki G, et al . ICF Core Sets for breast cancer .J Rehabil Med Suppl 2004;44 Suppl:121-7 .
23 . Tschiesner U, Rogers SN, Dietz A, et al. Development of ICF CoreSets for head and neck cancer. Head Neck 2010 ;32 :210-20 .
24 . Tschiesner U, Rogers SN, Harreus U, et al. Comparison ofoutcome measures in head and neck cancer-a literature review2000-2006 . Head Neck 2009;31 :251-9.
25 . Tschiesner U, Linseisen E, Coenen M, et al . Evaluating sequelaealter head and neck cancer from the patient perspective wichthe help of the International Classification of Functioning,Disability and Health. Eur Arch Otorhinolaryngol 2009;266 :425-36 .
26. Tschiesner U, Becker S, Cieza A. Health professional perspective andisability in head and neck cancer. Arch Otolaryngol Head NeckSurg 2010;36 :576-83 .
27. Tschiesner U, Linseisen E, Baumann S, et al. Assessment offunctioning in patients wich head and neck cancer according to theInternational Classification of Functioning, Disability and Health(ICF)-a multi-centre study . Laryngoscope 2009;119:915-23.
28. Rogers SN, Gwanne S, Lowe D, et al . The addition of mood andanxiety domains to the University of Washington Quality of Lifescale. Head Neck 2002 ;24 :521-9 .
29. Bjordal K, de Graeff A, Fayers P, et al . A 12 country Field study ofthe EORTC QLQ-C30 (version 3 .0) and the head and neck cancerspecific module (EORTC QLQ-H&N35) in head and neckpatients. EORTC Quality of Life Group . Eur J Cancer 2000;36:1796-807 .
30. Aaronson N, Beckmann JE. The quality of life in cancer patients .EORTC Study Group an Quality of Life . J Psychosoc Oncol 1986;4:43-53 .
31 . Bjordal K, Kaasa S, Mastekaasa A. Quality of life in patients treatedfor head and neck cancer: a follow-up study 7 to 11 years alterradiotherapy. Int J Radiat Oncol Biol Phys 1994;28:847-56 .
32 . Weymuller EA Jr, Alsarraf R, Yueh B, et al . Analysis of theperformance characteristics of the University of WashingtonQuality of Life instrument and its modification (UW-QOL-R) .Arch Otolaryngol Head Neck Surg 2001 ;127 :489-93 .
33 . Cieza A, Brockow T, Ewert T, et al. Linking health-status measurements to the International Classification ofFunctioning, Disability and Health. J Rehabil Med 2002 ;34:205-10 .
34 . Cieza A, Geyh S, Chatterji S, et al. ICF linking rules : an updatebased an lessons learned . J Rehabil Med 2005;37:212-8.
35 . Cieza A, Hilfiker R, Boonen A, et al . Items from patient-orientedInstruments can be integrated into interval scales to operationalizecategories of the International Classification of Functioning,Disability and Health . J Clin Epidemiol 2009 ;62 :912-21 .
36. Strobl R, Stucki G, Grill E, et al . Graphical models illustratedcomplex associations between variables describing human func-tioning . Clin Epidemiol 2009 ;62:922-33 .
37. Campbell B, Marbella A, Layde P . Quality of life and recurrenceconcern in survivors of head and neck cancer . Laryngoscope 2000 ;110:895-906.
38. List M, D'Antonio L, Cella D, et al . The Performance Status Scalefor Head and Neck Cancer Patients and the Functional Assessmentof Cancer Therapy-Head and Neck Scale . A study of utility andvalidity. Cancer 1996;77:2294-301 .
39. Bjordal K, Hammerlid E, Ahlner-Elmgvist M, et al. Qualityof life in head and neck cancer patients : validation of theEuropean Organization for Research and Treatment of CancerQuality of Life Questionnaire-H&N35 . J Clin Oncol 1999;17 :1008-19.
40. Cella DF, Tulsky DS, Gray G, et al . The Functional Assessment ofCancer Therapy scale : development and validation of the generalmeasure . J Clin Oncol 1993;11 :570-9 .
Tschiesner et al, Validation ICF Core Sets for Head and Neck Cancer
687
41 . Trotti A, Johnson DJ, Gwede C, et al . Development of a head andneck companion module for the Quality of Life-Radiation TherapyInstrument (QOL-RTI) . Int J Radiat Oncol Biol Phys 1998 ;42 :257-61 .
42. Terrell JE, Nanavati KA, Esclamado RM, et al . Head and neckcancer-specific quality of life : instrument validation. ArchOtolaryngol Head Neck Surg 1997 ;123 :1125-32.
43. Dwivedi R, Kazi R, Agrawal N, et al. Evaluation of Speechoutcomes following treatment of oral and oropharyngeal cancers .Cancer Treat Rev 2009 ;35 :417-24 .
44 . Lazarus C . Effects of chemoradiotherapy an voice and swallowing .Curr Opin Otolaryngol Head Neck Surg 2009 ;17 :172-8 .
45 . Martino R, Ringach J . Evaluation of quality of life and Organfunction in head and neck squamous cell carcinoma . HematolOncol Clin North Am 2008 ;22 :1239-56, x.
46 . Mehanna H, De Boer M, Morton R. The association of psycho-social factors and survival in head and neck cancer . ClinOtolaryngol 2008;33 :83-9 .
47 . Murphy B, Gilbert J, Cmelak A, et al . Symptom control issues andsupportive care of patients with head and neck cancers . Clin AdvHematol Oncol 2007 ;5 :807-22.
48 . Starmer H, Tippett D, Webster K. Effects of laryngeal cancer anvoice and swallowing. Otolaryngol Clin North Am 2008;41 :793-818 .
49 . Karnell L, Christensen A, Rosenthai E, et al . Influence of socialSupport an health-related quality of life outcomes in head and neckcancer. Head Neck 2007;29:l43-6 .
50. Kagan S. The influence of nursing in head and neck cancermanagement. Curr Opin Oncol 2009;21 :248-53 .
51 . Department of Health. A policy framework for commissioningcancer Services, a report by the Expert Advisory Group an Cancer .London: Department of Health 1995 .
52. Becker S, Kirchberger I, Cieza A, et al . Content validation of theComprehensive ICF Core Set for Head and Neck Cancer (HNC) :the perspective of psychologists . Psychooncology 2009 Aug 4 .[Epub ahead of print]