Embed Size (px)
Citation preview

ONLINE ONLY
Comparison between cone-beam computedtomography and intraoral digital radiography forassessment of tooth root lesions
Vandana Kumar,a Lauren Gossett,b Ashley Blattner,b Laura R. Iwasaki,c Karen Williams,d and Jeffrey C. Nickele
Kansas City, Mo and Baltimore, Md
FromaAssisSchoobPostUnivecPrivadProfeof MieAssoOrthoThe aucts oReprinand R64108Subm0889-Copyrdoi:10
Introduction: Cone-beam computed tomography (CBCT) might be more accurate in identifying radicularsurface lesions compared with digital periapical radiography. In this study, we compared these techniques indetecting simulated root resorption lesions. Methods: A porcine mandible was used to support 10 humanmaxillary central incisors. CBCT and digital periapical radiographic images were generated before and afterthe introduction of standardized and sequentially larger root defects on either the mesial or the lingual rootsurfaces. The images were randomly labeled and evaluated by 3 examiners. Each image was classified accord-ing to defect size (0, none; 1, mild; 2, moderate; 3, severe). Results: Interrater reliability was acceptable(0.856#P#0.981). The location of the root defect (mesial vs lingual) had no significant effect on the evaluationof defect size. Both periapical radiographs and CBCTwere slightly better at detecting lingual defects thanmesialdefects (75% vs 65% and 65% vs 60%, respectively), but these effects were not statistically significant (P5 0.49andP5 0.74, respectively). Themean percentages of correctly diagnosed defect sizes were 65% for CBCT and75% for periapical radiographs. Examiners using CBCT images tended to overestimate defect sizes (k5 0.481)and correctly categorized teeth with no, mild-moderate, and severe defects 80%, 45%, and 90% of the time,respectively. Examiners using periapical radiographs tended to underestimate defect sizes (k 5 0.636) andcategorized teeth with no, mild-moderate, and severe defects 100%, 50%, and 100% of the time,respectively.Conclusions: There was no difference in accuracy of identifying defects between periapical radio-graphs and CBCT images. (Am J Orthod Dentofacial Orthop 2011;139:e533-e541)
External root resorption during orthodontic toothmovement is thought to be caused by ischemicnecrosis of the periodontal ligament, with initial
damage to the root cementum layer.1 Various biologicand mechanical risk factors have been associated withan increased risk of root resorption during orthodontictreatment. For mechanical factors, extensive toothmovement, root intrusion and torque, orthodontic force
the School of Dentistry, University of Missouri at Kansas City.tant professor, Department of Oral Pathology, Medicine and Radiology,l of Dentistry, University of Missouri at Kansas City.graduate student, Department of Orthodontics, School of Dentistry,rsity of Missouri at Kansas City.te practice, Baltimore, Maryland.ssor and director, Clinical Research Center, School of Dentistry, Universityssouri at Kansas City.ciate professor and director, Postgraduate Orthodontics and Dentofacialpedics, School of Dentistry, University of Missouri at Kansas City.uthors report no commercial, proprietary, or financial interest in the prod-r companies described in this article.t requests to: Vandana Kumar, Department of Oral Pathology, Medicineadiology, UMKC School of Dentistry, 650 E 25th St, Kansas City, MO; e-mail, [email protected], March 2010; revised and accepted, November 2010.5406/$36.00ight � 2011 by the American Association of Orthodontists..1016/j.ajodo.2010.11.018
magnitude, and duration have been implicated. Withrespect to biologic factors, genetic predisposition to hy-perinflammation, systemic disease, sex, and medicationsare associated with root resorption.2-4
The orthodontic literature contains reports of clinicaland laboratory investigations of root resorption.2,5-10 Theincidence of reported root resorption during orthodontictreatment varies widely among investigators. Toothstructure, alveolar bone structure at various locations,and types ofmovementmight explain these variations.11,12
Root resorption of the deciduous dentition is a nor-mal, essential, and physiologic process. Permanent teethcan also undergo significant external root resorption;however, this is not considered normal, essential, orphysiologic. In 1 study, root resorption of permanentteeth was found to begin in the early leveling stages oforthodontic treatment. About 4.1% of patients studiedhad an average resorption of 1.5 mm or more of the 4maxillary incisors, and about 15.5% had 1 or more max-illary incisors with resorption of 2.0 mm or more from 3to 9 months after initiation of fixed appliance therapy.13
In a separate study, it was found that mean apical rootresorption in permanent teeth was strongly correlated
e533

e534 Kumar et al
with total apical displacement of the root (R 5 0.822)and treatment duration (R5 0.852).14 The maxillary an-terior teeth were found to be the most resorbed, with25% undergoing greater than 2 mm of root resorption.The posterior teeth were relatively unaffected.15
During orthodontic therapy, early detection and cor-rect characterization of the location and the amount ofresorption of the root surface are necessary to preventfurther destruction of the tooth root. External resorptionis often first detected radiographically via analog ordigital 2-dimensional (2D) images.16,17 Studies haveshown that resorption defects are harder to detect onbuccal than proximal root surfaces. Resorption defectsof 0.6-mm diameter and 0.3-mm depth were hard todetect.18,19 Analog and digital 2D imaging modalitiesyielded false negative results in about 51.9% of casesand false positive results in about 15.3%.20 However, in2 separate studies, digital radiographic methods werefound to be superior in detecting simulated external rootresorption lesions compared with analog radiographs.21,22
The diagnostic accuracy of root lesions based ona single image can be improved from 73% to 87%when images are available from different angles.23 How-ever, intraoral radiographs do not indicate the true di-mensions of lesions.24 The amount of informationgained from 2D periapical radiographs is incomplete,since the 3-dimensional (3D) anatomy is compressedinto a 2D image. The compression causes “noise” thatmight result in underestimation of the size of the resorp-tion lesion.25 Hence, 3D imaging techniques have thepotential to offer accurate quantification of root resorp-tion defects and, perhaps, earlier detection of lesions.26
Conventional computed tomography (CT) has beenshown to have high sensitivity and specificity in the de-tection of external root resorption defects in vitro. Highcost and radiation exposure make this modality gener-ally unsuitable for routine imaging of the dentition.27
Cone-beam CT (CBCT) is an imaging modality that offersthe advantages of 3D voxels and high diagnostic yieldwith short scanning times and significantly lower radia-tion dosages than conventional CT.28 In 2 ex-vivo stud-ies evaluating CBCT for measurement of resorptiondefects, the influence of voxel size was assessed. CBCTwas found to be an accurate method for the imagingof simulated external root resorption. A 0.3 mm3 voxelappeared to produce the best results.29,30 In an in-vivoinvestigation of detection and management of root re-sorption lesions with intraoral radiography and CBCT,CBCT was found to be effective and reliable in detectingresorption lesions.31 Since this modality might be usefulfor enhancing diagnosis of early root resorption, there isa need to compare the diagnostic accuracy of CBCT withdigital periapical radiographs for assessing root defects.
June 2011 � Vol 139 � Issue 6 American
Therefore, this study was designed to evaluate the accu-racy of CBCT imaging vs intraoral periapical digital radi-ography for the identification of simulated rootresorption lesions. We compared observers’ abilities todetect simulated external root resorption defects usingthe 2 diagnostic imaging modalities: digital periapical2D radiographs produced by a radiation beam directedhorizontally to the proximal tooth surface from a directdigital system vs reconstructed images from 3D data setsgenerated from a CBCT system. The main objective wasto determine whether the ability to detect defects withthese 2 modalities was influenced by location andamount of resorption.
MATERIAL AND METHODS
A total of 40 specimens were created for imaging via2 modalities by securing maxillary incisors in a bonyhousing in a standardized fashion. A porcine mandiblewas obtained from a local abattoir and handled accord-ing to institutional policy. The ramus of the mandiblewas sectioned distally to the last molar, and the anteriorportion was used to create a simulated root socket tohouse a sample tooth root for imaging. Ten maxillary in-cisors extracted for various periodontal conditions wereobtained. Approval to use extracted teeth for the studywas given by the institutional review board of the Uni-versity of Missouri at Kansas City. Selection criteria forthe sample teeth were atraumatic removal, no restora-tions, no previous root resorption, no previous endodontictherapy, and no periapical pathosis.
Initially, each intact incisor root (category 0, no de-fect) was secured in the simulated socket to create a spec-imen, imaged by 2 methods, and then removed from thesocket. Subsequently, each root was then subjected to 3sequentially increasing sizes of defects (categories 1,mild defect; 2, moderate defect; and 3, severe defect).After each standardized defect was developed, it wasquantified, and the root was secured again in the sameposition and orientation in the simulated socket. Thespecimen was imaged via the 2 methods, and then thespecimen was disassembled. Details of these methodsare described in the following paragraphs.
The simulated root socket was created by usinga pineapple-shaped bur (H79E040, Komet, Rock Hill,SC; diameter, 6.8 mm; depth, 13.8 mm) on a slow-speed hand piece to create a hole 10 mm in depth witha uniform circumference of 2 mm of cortical bone. Threeorientation marks were made with a high-speed handpiece and a number 57 dental bur sunk to the depthof the cutting surface next to the simulated socket onthe posterior, anterior, and medial surfaces of themandible. Each tooth was placed in the simulated socket
Journal of Orthodontics and Dentofacial Orthopedics

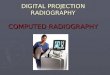
Fig 1. Maxillary central incisor oriented according to anexternal coordinate system with putty and held in placeby mounting plaster.
Kumar et al e535
and centered by using cotton pellets. Then an externalcoordinate system was fabricated from impression putty(Reprosil Vinyl Polysiloxane Impression Material, 1075mL tube; Dentsply Caulk, Milford, Del) molded aroundthe tooth and into the orientation marks. Once set, theputty was removed and cut lengthwise just lateral tothe posterior and anterior orientation marks and downthe midline of the negative tooth impression (Fig 1).Thus, when a tooth was replaced in the socket for sub-sequent CBCT and radiographic imaging, the externalcoordinate system was used to ensure that it was re-placed in the exact same orientation and that a positiveseat was formed between the tooth, the external coordi-nate system, and the orientation marks. To assemblea specimen, cotton pellets were removed, and mountingplaster (Pemaco Lab Stone, St. Louis, Mo; ratio, 30 cm3
of water to 100 g of powder) was mixed to a runnyconsistency and vibrated into the simulated socket.The tooth was placed in the bony housing by using theexternal coordinate system (Fig 1) and was imaged.
Periapical radiographs of the specimens were obtainedby using a charge-coupled device connected to an x-raymachine (RVG model FV-47, Trophy Radiology, Marietta,Ga) that provided 70 kVp and 8 mA. Exposure time was0.02 impulses, and the x-ray beam was directed at a rightangle to the proximal tooth surface. CBCT images of thespecimens were obtained with a CBCT machine (Classici-CAT model, Imaging Sciences International, Hatfield,Pa) at 120 kVp, 26 mA, and 0.25-mm voxel size.
After initial imaging (Fig 2), each tooth was removedfrom the socket and, as previously outlined, 3 standard-ized and sequentially larger defects were created oneither the mesial or the lingual root surface, 5 mmcoronal to the apex. Odd-numbered teeth (1, 3, 5, 7,and 9) received defects on the mesial surface, andeven-numbered teeth (2, 4, 6, 8, and 10) received defectson the lingual surface. Lines were drawn with a perma-nent marker on both sides of each tooth from incisaledge to apex to divide in half the 5 odd-numbered teethbuccolingually and the 5 even-numbered teeth mesio-distally. A digital gauge was used to measure 5 mm cor-onal to the apex along the previously drawn line, wherean ink mark was made on the appropriate surface. At themark, a high-speed hand piece with a number ½ rounddental bur was used to create the initial (mild) defect.The shaft of the bur was perpendicular to the long axisof the tooth, and the bur penetrated the root surfaceto the depth of the cutting surface. Similarly, moderateand severe defects were made by using number 2 and4 round burs, respectively. All defects were made bythe same investigator (L.G.) using magnified vision,and the defect depths were verified by another investiga-tor (A.B.) also using magnified vision.
American Journal of Orthodontics and Dentofacial Orthoped
After each defect was created, an impression wasmade of it with polyvinyl siloxane light-body impressionmaterial (Aquasil, Dentsply Caulk), and then the defectwas filled with base plate wax to prevent the mountingplaster from flowing into the defect. The diameter ofeach impression was quantified by using a measuringmicroscope (Luxo Magnifier, Coe-Bilt Laboratories,Chicago, Ill; 118 V, 22 W, 60 cycles) for calculation ofthe volume of the defect. The 10 CBCT and 10 periapicalradiographic images of root defects in the 4 categories(0, no defect [Fig 2]; 1, mild defect [Fig 3]; 2, moderatedefect [Fig 4]; and 3, severe defect [Fig 5]) were ran-domly labeled and viewed by 3 blinded examiners, ofwhom 1 was a board-certified oral radiologist and 2were board-certified orthodontists. The examiners wereallowed to adjust the gray scale and the magnificationof the images and to access all CBCT plane images to ar-rive at a categorization of the size of root defect (0-3)represented in each image. The examiners were requiredto complete the assessments of all 80 images in a 40-minute time frame, thus producing a realistic clinical as-sessment. A repeat session of the image categorizationwas performed approximately 1 month later to test forintra-assessor and interassessor reliability (Spearmanrho statistic). For statistical comparison of the diagnosticaccuracy of the defects, the examiners’ ratings for defectsizes were collapsed separately to produce 1 compositescore for the periapical and the CBCT images. If either2 or 3 examiners agreed on the size of the defect, thatcategorical ranking was used as the composite score.This ranking was then compared with the known goldstandard and determined to be either accurate (1) orinaccurate (0). If the 3 examiners all categorized thedefects differently for an image, it was determined to
ics June 2011 � Vol 139 � Issue 6

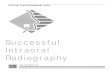
Fig 2. Sample tooth with no defect imaged via CBCT and intraoral radiograph: A, coronal; B, sagittal;C, axial views; and D, periapical radiograph.
e536 Kumar et al
be inaccurate. The McNemar change test was used tocompare the accuracy of identifying defects with CBCTimages and periapical radiographs. The direction of mis-classification was also explored between the 2 modalitiesdescriptively. Additionally, the effect of location of thedefect (mesial vs lingual) was compared to determinewhether accuracy was related to location for CBCT andperiapical radiographs separately by using chi-squareanalysis.
RESULTS
The 3 examiners showed good between-session con-sistency in image categorization (0.856 #P #0.981,Table I). Absolute agreement among examiners in thecategories of root-defect size between both imagingmodalities was 47.5%. The location of the root defect(mesial vs lingual) had no significant effect on evalua-tion of defect size. Both periapical radiographs andCBCT images were slightly better at detecting lingual de-fects than mesial defects (75% vs 65% and 65% vs 60%,
June 2011 � Vol 139 � Issue 6 American
respectively), but these effects were not statisticallysignificant (P 5 0.49 and P 5 0.74, respectively).
When the results for accuracy of categorization of theroot-defect sizes (collapsed across examiners) were as-sessed relative to measured defect volume, correct cate-gorizations were 62.5% for CBCT images and 70% forperiapical radiographs. This difference of 7.5% favoringperiapical radiographs was not statistically significant(P5 0.629). A closer examination of accuracy as a func-tion of lesion size showed a differential effect, with peri-apical radiographs more accurate for no lesions,moderate, and severe lesions, and CBCT more accuratefor mild lesions. The rates of correct categorization byindividual examiners using CBCT images varied widelyfrom 48% to 78% (Table II). Similar variability was evi-dent for periapical images, which ranged from 52% to73% for the examiners. When the degree of root defectwas incorrectly quantified based on the CBCT images,the size of the defect tended to be overestimated. In con-trast, when the degree of root defect was incorrectly
Journal of Orthodontics and Dentofacial Orthopedics

Fig 3. Sample tooth with mild defect imaged via CBCT and intraoral radiograph:A, coronal;B, sagittal;C, axial views; and D, periapical radiograph.
Kumar et al e537
quantified based on the periapical radiographs, the sizeof the defect tended to be underestimated.
DISCUSSION
Orthodontically induced inflammatory root resorp-tion (OIIRR) has been documented as an iatrogenic out-come of orthodontic tooth movement. Early detection ofresorptive lesions in vivo is challenging, particularly be-cause no clinical manifestations are usually evident.Hence, radiographs have been the main tools used toidentify and monitor OIIRR.
Although intraoral radiography is the standardmethod used clinically to detect external root resorp-tion, its inadequacy for early detection is recog-nized.32,33 The size and location of root defectsmight affect identification in 2D radiographs. Onestudy with conventional intraoral radiography showed
American Journal of Orthodontics and Dentofacial Orthoped
that resorption was harder to detect when it was onthe buccolingual aspect compared with the proximalsurfaces of the root,16 and small cavities (diameter,0.6 mm; depth, 0.3 mm) were never detected.18 Wecompared the detection of defects on the lingual andmesial root surfaces, but the location showed no statis-tically significant effects.
The significance of using more than 1 radiographfrom different angles for diagnosis has been estab-lished.18,33 In this study, detection of root defects byusing 2D radiography was based on only 1 standardx-ray projection per specimen, made perpendicular tothe tooth surface. However, experienced examinerswere on average 10% more accurate in detecting rootdefects using the resulting 2D radiographic imagesthan using the CBCT images, although this differencewas not significant. This should be considered a worst-case scenario, which penalizes the periapical method of
ics June 2011 � Vol 139 � Issue 6

Fig 4. Sample tooth with moderate defect imaged via CBCT and intraoral radiograph: A, coronal;B, sagittal; C, axial views; and D, periapical radiograph.
e538 Kumar et al
assessment. However, a single periapical image is morerealistic because it is unlikely that orthodontists in clin-ical practice routinely image regions of the dentitionfrom various angles. The accuracy of detection with peri-apical radiographs might have been increased if 2 or 3periapical projections were taken at different horizontalangulations, as suggested in the literature.34
Examiners using CBCT images correctly categorized80% of teeth with no defects and 90% of teeth with se-vere defects, but mild to moderate defects were correctlyidentified only 40% of the time. By comparison, thesame examiners were more accurate in detecting noand severe defects (100% each) using periapical radio-graphs, and 40% of the images in the mild to moderatecategory were correctly categorized.
Although the literature suggests that CBCT is a reli-able tool in detecting root resorption defects, it is rarethat studies compare CBCT efficacy with intraoral digital2D modalities.29-31,35,36 This study showed thatexaminers performed slightly inferiorly in the detectionof root defects when using CBCT images comparedwith conventional periapical radiographs. Cutoff values
June 2011 � Vol 139 � Issue 6 American
of 0.5 and 1 mm, as used in this study, could becomethe target of partial-volume averaging. Partial-volumeaveraging is an inherent artifact of CBCT imaging thatcould adversely affect its accuracy. This is because,when a single voxel contains a mixture of several tissuedensity values of the structure and the adjacent or sur-rounding structures, these density values are averagedfor that voxel. Thus, erroneous pixel or voxel signalvalues result. However, others have shown CBCT to bea reliable tool for the investigation of simulated externalroot resorption lesions of 0.6, 1.2, and 1.8 mm in diam-eter and 0.3, 0.6, and 0.9 mm in depth, in different loca-tions on the vestibular root surface, and at 3 voxelresolutions (0.2, 0.3, and 0.4 mm).29 The results ob-tained indicated that CBCT is a safe method to investi-gate external root resorption lesions, with excellentspecificity and sensitivity. The 0.3-mm voxel resolutionis the best configuration because it associates gooddiagnostic performance with less patient exposure tox-rays.29
The increased radiation dosage and expense, and thelimited availability of CBCT in most clinical settings,
Journal of Orthodontics and Dentofacial Orthopedics

Fig 5. Sample tooth with severe defect imaged via CBCT and intraoral radiograph: A, coronal;B, sagittal; C, axial views; and D, periapical radiograph.
Table I. Spearman rho (P) values of intrarater reliabil-ity in detection of sizes of root defects
CBCT images Periapical radiographsExaminer 1 0.981 0.953Examiner 2 0.896 0.882Examiner 3 0.917 0.856
Kumar et al e539
accentuate the outcome of this study: to consider thatperiapical radiographs are better at detecting root de-fects. However, when a full-mouth series or periapicalradiographs are not available and a CBCT scan of the pa-tient is already available, these CBCT data could be usedto detect root resorption via 2D or 3D evaluation withoutadditional radiation exposure.
In this study, the smallest available voxel size of 0.25mm was used to scan the teeth. CBCT machines witha minute voxel size of 80 mm or less, combined witha 13-bit gray-scale capability, are now available in themarket. The superiority of such a small voxel size andgray-scale capability in the detection of root surface le-sions need to be explored. Newer software tools havebeen introduced for CBCT to make volumetric measure-ments. Such tools could be beneficial for assessments ofsmall root defects and should be studied in the future.The methods used in this study produced defects withregular edges that might have enhanced, or detractedfrom, the ability to identify lesions. Until better in-vitro methods are developed to simulate ragged, ill-defined edges of OIIRR, our results should be interpreted
American Journal of Orthodontics and Dentofacial Orthoped
with the understanding that external resorption cavitiesdrilled with a round bur are not real replicas of OIIRR.Therefore, future studies should consider methods tocreate standardized irregular lesions. It is also acknowl-edged that this bench-top study had ideal imaginggeometries, with no associated motion. These conditionsare seldom achieved in the clinic. More robust in-vivostudies are required to determine whether CBCT imagingcould be superior to digital 2D systems in the earlydetection of root resorption defects.
CONCLUSIONS
There was no difference in accuracy of identifyingdefects between periapical radiographs and CBCT
ics June 2011 � Vol 139 � Issue 6

Table II. Simulated root resorption defects: category, size, volume, and accuracy of identification by examiners andoverall with CBCT and periapical radiographic (PR) images
Defectcategory (n)
Size(x 5 diameter, mm)
Volume(V, mm3)
Accuracy of identification (%)
Examiner 1 Examiner 2 Examiner 3
All CBCT (n) All PR (n)CBCT PR CBCT PR CBCT PRNone (10) 0.0 0.0 80 100 100 100 80 90 80 (8) 100 (10)Mild (10) 0.0\x #0.5 0.0\V #0.2 20 30 40 30 80 20 60 (6) 20 (2)Moderate (10) 0.5\x #1.0 0.2\V #1.0 100 60 20 30 70 70 20 (2) 60 (6)Severe (10) .1.0 .1.0 90 100 100 50 80 100 90 (9) 100 (10)All (40) – – 48 73 65 52 78 70 62 (25) 70 (28)
e540 Kumar et al
images. The lack of superiority of either imaging modal-ity suggests that periapical or CBCT imaging can be usedto identify root defects. However, because of the in-creased radiation exposure from CBCT, using CBCT foridentifying defects should be considered with the caveatthat CBCT data are already available for analysis.
REFERENCES
1. Pizzo G, Licata ME, Guiglia R, Giuliana G. Root resorption and or-thodontic treatment. Review of the literature. Minerva Stomatol2007;56:31-44.
2. Abuabara A. Biomechanical aspects of external root resorption in or-thodontic therapy. Med Oral Patol Oral Cir Bucal 2007;12:E610-3.
3. Apajalahti S, Peltola JS. Apical root resorption after orthodontictreatment—a retrospective study. Eur J Orthod 2007;29:408-12.
4. Lopatiene K, Dumbravaite A. Risk factors of root resorption afterorthodontic treatment. Stomatologija 2008;10:89-95.
5. Chan E, Darendeliler MA. Physical properties of root cementum:part 7. Extent of root resorption under areas of compression andtension. Am J Orthod Dentofacial Orthop 2006;129:504-10.
6. Cheng LL, Turk T, Elekdag-Turk S, Jones AS, Petocz P,Darendeliler MA. Physical properties of root cementum: part 13.Repair of root resorption 4 and 8 weeks after the application ofcontinuous light and heavy forces for 4 weeks: a microcomputed--tomography study. Am J Orthod Dentofacial Orthop 2009;136:320.e1-10; discussion 320-1.
7. Abass SK, Hartsfield JK Jr, Al-Qawasmi RA, Everett ET, Foroud TM,Roberts WE. Inheritance of susceptibility to root resorption associ-ated with orthodontic force in mice. Am J Orthod Dentofacial Or-thop 2008;134:742-50.
8. Al-Qawasmi RA, Hartsfield JK Jr, Everett ET, Flury L, Liu L,Foroud TM, et al. Genetic predisposition to external apical root re-sorption. Am J Orthod Dentofacial Orthop 2003;123:242-52.
9. �Artun J, Smale I, Behbehani F, Doppel D, Van’t Hof M,Kuijpers-Jagtman AM. Apical root resorption six and 12 monthsafter initiation of fixed orthodontic appliance therapy. Angle Or-thod 2005;75:919-26.
10. Hartsfield JK Jr, Everett ET, Al-Qawasmi RA. Genetic factors in ex-ternal apical root resorption and orthodontic treatment. Crit RevOral Biol Med 2004;15:115-22.
11. Brezniak N, Wasserstein A. Root resorption after orthodontic treat-ment: part 2. Literature review. Am J Orthod Dentofacial Orthop1993;103:138-46.
12. Brezniak N, Wasserstein A. Root resorption after orthodontic treat-ment: part 1. Literature review. Am J Orthod Dentofacial Orthop1993;103:62-6.
June 2011 � Vol 139 � Issue 6 American
13. Smale I, �Artun J, Behbehani F, Doppel D, van’t Hof M,Kuijpers-Jagtman AM. Apical root resorption 6 months after initi-ation of fixed orthodontic appliance therapy. Am J Orthod Dento-facial Orthop 2005;128:57-67.
14. Segal GR, Schiffman PH, Tuncay OC. Meta analysis of thetreatment-related factors of external apical root resorption.Orthod Craniofac Res 2004;7:71-8.
15. Sameshima GT, Sinclair PM. Predicting and preventing rootresorption: part II. Treatment factors. Am J Orthod DentofacialOrthop 2001;119:511-5.
16. Goldberg F, De Silvio A, Dreyer C. Radiographic assessment of sim-ulated external root resorption cavities in maxillary incisors. EndodDent Traumatol 1998;14:133-6.
17. Leach HA, Ireland AJ, Whaites EJ. Radiographic diagnosis ofroot resorption in relation to orthodontics. Br Dent J 2001;190:16-22.
18. Andreasen FM, Sewerin I, Mandel U, Andreasen JO. Radiographicassessment of simulated root resorption cavities. Endod DentTraumatol 1987;3:21-7.
19. Chapnick L. External root resorption: an experimental radiographicevaluation. Oral Surg Oral Med Oral Pathol 1989;67:578-82.
20. Nance RS, Tyndall D, Levin LG, Trope M. Diagnosis of external rootresorption using TACT (tuned-aperture computed tomography).Endod Dent Traumatol 2000;16:24-8.
21. Borg E, Kallqvist A, Grondahl K, Grondahl HG. Film and digitalradiography for detection of simulated root resorption cavities.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:110-4.
22. Westphalen VP, Gomes de Moraes I, Westphalen FH, Martins WD,Souza PH. Conventional and digital radiographic methods in thedetection of simulated external root resorptions: a comparativestudy. Dentomaxillofac Radiol 2004;33:233-5.
23. White SC, Atchison KA, Hewlett ER, Flack VF. Efficacy of FDAguidelines for prescribing radiographs to detect dental and intra-osseous conditions. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1995;80:108-14.
24. Kim E, Kim KD, Roh BD, Cho YS, Lee SJ. Computed tomography asa diagnostic aid for extracanal invasive resorption. J Endod 2003;29:463-5.
25. Patel S, Dawood A. The use of cone beam computed tomographyin the management of external cervical resorption lesions. IntEndod J 2007;40:730-7.
26. Danforth RA, Dus I, Mah J. 3-D volume imaging for dentistry:a new dimension. J Calif Dent Assoc 2003;31:817-23.
27. Ekestubbe A, Thilander A, Grondahl K, Grondahl HG. Absorbeddoses from computed tomography for dental implant surgery:comparison with conventional tomography. DentomaxillofacRadiol 1993;22:13-7.
Journal of Orthodontics and Dentofacial Orthopedics

Kumar et al e541
28. Sukovic P. Cone beam computed tomography in craniofacialimaging. Orthod Craniofac Res 2003;6(Suppl 1):31-6; discussion179-82.
29. Liedke GS, da Silveira HE, da Silveira HL, Dutra V, de Figueiredo JA.Influence of voxel size in the diagnostic ability of cone beam to-mography to evaluate simulated external root resorption. J Endod2009;35:233-5.
30. HahnW, Fricke-Zech S, Fricke J, Gruber RM, Dullin C, Zapf A, et al.Detection and size differentiation of simulated tooth root defectsusing flat-panel volume computerized tomography (fpVCT). OralSurg Oral Med Oral Pathol Oral Radiol Endod 2009;107:272-8.
31. Patel S, Dawood A, Wilson R, Horner K, Mannocci F. The detectionand management of root resorption lesions using intraoral radiog-raphy and cone beam computed tomography—an in vivo investi-gation. Int Endod J 2009;42:831-8.
American Journal of Orthodontics and Dentofacial Orthoped
32. Bender IB, Seltzer S. Roentgenographic and direct observation ofexperimental lesions in bone: I. 1961. J Endod 2003;29:702-706; discussion 701.
33. Brynolf I. Roentgenologic periapical diagnosis. II. One, two ormore roentgenograms? Sven Tandlak Tidskr 1970;63:345-50.
34. Bernier-Rodriguez JA, Sidow SJ, Joyce AP, McNally K,McPherson JC 3rd. Radiographic interpretation of experimental le-sions in radicular tooth structure of human maxillary anteriorteeth. J Endod 2008;34:1466-9.
35. Patel S, Kanagasingam S, Pitt Ford T. External cervical resorption:a review. J Endod 2009;35:616-25.
36. Maini A, Durning P, Drage N. Resorption: within or without? Thebenefit of cone-beam computed tomography when diagnosinga case of an internal/external resorption defect. Br Dent J 2008;204:135-7.
ics June 2011 � Vol 139 � Issue 6