Upload
abdalla-malkawi
View
2.281
Download
0
Embed Size (px)
Citation preview
COMMON VERTEBRAL JOINT PROBLEMSGregory P. GrieveFCS!' Dip T!'
Honorary Fellow of the Chartered Society of Physiotherapy Post-Registration Tutor, Department of Rheumatology and Rehabilitation, Norfolk and Norwich Hospital Former Supervisor and Clinical Tutor, Spinal Treatment Unit, Royal National Orthopaedic Hospital, London
Fo,.ewo,.d by
PHILIP H. NEWMAN
CBE DSO MC FRCS the Royal National
Latcly Consultant Orthopaedic Surgeon to the Middlesex Hospital, and Consultant Surgeon London Past President of the British Orthopaedic Association and formerly Chairman of the British Council of Management of the Journal of Bone and Joint Surgery10
Orthopaedic Hospital and Institute of Orthopaedics,
c::J c::Jc::Jc::J c::Jc::Jc::JL7CHURCHILL LIVINGSTONEEDINBURGH LONDON MELBOURNE AND NEW YORK 1981
CHURCHILL LIVINGSTONE Medical Division of Longman Group Limited DiSlributed in the United States of America by Churchill Livingstone Inc., 19 West 44th Street, New York, N.Y. 10036, and by associated companies, branches and represematives throughout the world. Longman Group Limited 1981 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publishers (Churchill Livingstone, Robert Stevenson House. 1-3 Baxter's Place, Leith Walk, Edinburgh, EHI 3AF), Firsl published 1981 ISBN 0 443 02106 6
British Library Cataloguing in Publication DataGrieve. Gregory P. Common venebral joint problems.
1. Spine-Diseases1. Title 617'375 RC400
LIbrary of Congreu Catalog Card Number 81-67465
Printed in Great Britain by Butler & Tanner Ltd. Frome and London
Foreword
Modern advance in prevention and treatment has elimi nated or brought under control many of the severe illnesses which, a generation or so ago, afflicted man. The medical profession now has greater opportunity to pay attention to the challenge of chronic arthritis and the effects of trauma, stress and strain and wear and tcar of the musculoskeletal system, The population of the Western world of today, its av erage age and demand for physical comfort gradually in creasing, presents an expanding and exacting problem. In hospital practice, to which the more difficult cases 3fC referred, it is the consultant who examines, investigates, attempts to diagnose and prescribes treatment and having excluded a serious cause or the need for inpatient treatment may refer the patient to the department of physical medi cine for supervision and care. The therapist who carries out these instructions spends much time with the patient and learning from experience develops an unparalleled understanding of the nature of skeletal pain. Greg Grieve has dedicated his professional life to an extensive study of these physical problems and has devoted his attention in particular to the multiple syn dromes arising from the intervertebral and sacroiliac joints. So impressed was he by the work of Mennell, Marlin, Cyriax, Stoddard and others that he energetically became involved, with other Chartered physiotherapists, in found ing a school of instruction in the basic sciences as applied to the spine and of the problems of derangement and to train physiotherapists in the art of treatment by manipu lation. Following the initial courses, with other teachers, between 1965 and 1967 he was the pioneer who carried the
torch of planning the curriculum and progressive develop ment of the annual courses during the eight especially formative years, 1968 to 1975. During this time Grieve delved deeply into the vast literature that has accumulated on this subject. The variety and extent of this field is aptly expressed in this book: 'The mountain of literature on spinal pathology is massive enough to have become all things to all men.' This book lists no less than 1400 references and its text is astoundingly reverent to the galaxy of opinions and conclusions and the conflicting hypotheses that they contain. Derangement of the vertebral column is covered in all its aspects and it soon becomes obvious that the value of this monograph is unique. It unfolds the nature of the problem as seen by a person who has spent much time communicating with and actively treating patients. There is much to learn both from a diagnostic and therapeutic angle which is not found in the many textbooks written by the medical profession. This is a comprehensive aggregation of the whole subject but there is nothing pedestrian in its teaching. It is prov ocative and doubtless the more conservative reader would now and again catch his breath. Above all it provides stimulation for thought on a subject which is apt to be bogged down by tradition and hampered by interdisciplinary contention. It is a brave and brilliant endeavour to translate the jargon of the various schools into a language with a scien tific basis. It cannot fail to appeal to all those interested in the vencbral column whatever their clinical status. Aldeburgh, Suffolk 1981 P.H.N.
Preface
Is there anything whcrcofit may be said, 'Sec, this is new? It hath been already of old times, which was before us.' (Ecclesiastes i, 10)
There is )jute new in this book, only a different voice saying the old things, yet gathered together in a form which I hope will be useful to my colleagues. A commonly expressed regrct of therapists who strive to improve their handling of common joint problems is that some of those whose prerogative it is to diagnose and pres cribe at times appear to have only a limited conception of the capabilities of modern therapists. Such is the speed with which the technology and capabilities of all disciplines has riscn, this circumstance probably now applies to all interdisciplinary relationships. Since it is incumbent upon us to keep our own house in order, therapists must do something about their own situation. We must provide opportunities for our peers and colleagues to know about our work, aspirations and capabilities. In any case, it is really no more than enlightened self interest to comprehend as much as we can about the context of our work because if we do not, its value and our worth will fall away. Wright and Hopkins (1978) "" have em phasised that some 30 per cent of physiotherapists' time is devoted to rheumatic and orthopaedic conditions. I have attempted to formulate a guide, a vocabulary of basic information for those spending much of the day handling vertebral joint conditions. As a foundation for improving our knowledge we must know something of this if we aspire to become competent in the conservative treat ment of common vertebral joint problems, and to know in which direction our knowledge must be expanded. The easily portable knapsack-and-bedroll information and rule-of-thumb clinical methods of times past are no longer enough. Today's workers must gather knowledge from many fields, and train themselves to apply it quickly and accurately when assessing the multitude of facts ob tained by a good clinical examination. As the more successful treatment of respiratory, nervous and metabolic disease, for example, has naturally evolved
from a deeper understanding of the nature of the functional abnormality concerned, it is surely axiomatic that abnor malities of the musculoskeletal system arc more effectively treated when the nature of the abnormal movement is understood, since bodily movement is the function con cerned. There is nothing incongruous or unacceptable in applying this basic law of progression in therapeutics equally to the treatment of diseases of the blood, for in stance, and degenerative joint disease of the vertebral column. To treat musculoskeletal pain, whether by manipulation, acupuncture, hydrocortisone injection, transcutaneous nerve stimulation, the 'back school', relaxation techniques, exercises, ultrasound or whatever, without first making a comprehensive attempt to understand the clinical nature of the musculoskeletal abnormality as it affects each patient, is the road to Erewhon. The basic physical examination of common vertebral and peripheral joint conditions has now been developed to the stage of a modern technology, and given this as increas ingly standard practice, the steady accumulation of further knowledge is certain. Without this basis, low back pain, fibrositis, muscular pains, sciatica and tension headache, etc., will remain classically associated with patent medicine advertisements, rubifacient unctions, generalised exer cises, other 'shot-gun' regimes like generalised relaxation or whatever piece of gleaming chromium-plated machinery happens currently to be in vogue. There is nothing sadder than yesterday'S machine. While we make no real effort to understand the myriad clinical presentations of joint abnormality, troublesome joint pains will thunder on unabated. Since the level of useful knowledge in the world increases horrendously, individuals have great difficulty in keeping up with advances in their own small sphere; there are the problems of assimilation and especially organisation of the available information. I have had in mind the need for a new structural framework, perhaps serving as a skeleton around which increasingly better-informed successors will build yet more meat, the whole remaining organised in the
viii
PREFACE
sense that the skeletal framework is never lost from sight. The volume of information requires that many contri butors are needed, and this implies my hope that others will share in formulating succeeding and bener forms of this text. Unless they be monsters of omniscience, indivi duals who singlehandedly attempt to write on the many and diverse aspects of vertebral joint conditions must deal with some aspects about which they have little or no first hand knowledge. Without divine dispensation one's own view of what is important cannOt be acceptable to more than a handful, and for this reason alone, I would be very grateful for information about omissions, contradictions and ambi guities; suggestions from like-minded colleages would help to make a more suitable bony framework for the new meat and help to eradicate the inevitable defects of a first attempt. One could have written entirely on 'Manipulation', yet this presupposes that manipulation is the primary interest. This is not so-the more we understand about the genesis of these conditions, the temperament and life-habits of the patients in whom they are occurring and more especially the infinite variety of presentation from patient to patient, the better we help them; 'manipulation' is but one of our treatments, albeit a subject in itself. The text is addressed to the members of no particular discipline other than like-minded professional colleagues, by whatever academic route they may have developed an interest in the conservative treatment of the ubiquitous, frustrating and depressing spinal joint problems suffered by such multitudes of people. I have not attempted to categorise, or elaborate on, the pathology and syndromes of common musculoskeletal ab normalities other than in a general way, for these excellent reasons: 1. I already know of at least three different solutions to the problem of syndrome classification, which is a highly artificial business, anyway. 2. There is not space for such a full dissertation, should I be competent to provide it, if there is also to be some general attention to treatment techniques. 3. Knowledge of the subject is expanding and changing with such speed that a text purporting to be up-to-date and written by even the best authorities has little chance of meeting such a claim. Hence, principles only arc important, and do not change with the years. In The History of ImpressionismlO29 Renoir is quoted as observing, '. . . though one should take care not to remain imprisoned in the forms we have inherited, one should neither, through love of progress, imagine that one can detach oneself completely from past centuries.' Further, if we look to our experience we find that it is by thoroughly familiarising ourselves with the inventions of
others that we learn to make inventions of our own, par ticularly in regard to clinical examination procedures and treatment techniques. While physiotherapists should not anempt [Q write com prehensively on problems of diagnosis, or the disciplines of pathology, medicine, surgery, neurology, radiology and epidemiology, etc., perhaps in the devotion of a profes sional lifetime to this field of minor orthopaedics one may have acquired the competence to touch upon these discip lines as they concern the group of conditions under dis cussion here. When students approach their training in 'clinical con ditions' as diseases of the various systems, the conditions tend to assume a sort of social pecking order in their minds. Regrettably, the largely benign and humble rheumatic dis orders have a habit of being relegated to the lower orders and boring peasants of this hierarchy. I believe this to be a profound mistake, since by meticulous examination and enlightened assessment each one of the 'old (and young) necks and backs' becomes an exciting detective stOry of absorbing interest and amply repays informed and accurate treatment, which need not be vigorous or aggressive. The ample repayment lies in the pure pleasure of relieving chronic and often disabling pain and other symptoms and in one's slowly increasing awareness of the infinite variety of ways in which movement-abnormalities of the vertebral column can present. Degenerative joint disease of the spine is perhaps best regarded as a family of physiological ageing processes, with pathological changes intervening sooner or later as a con sequence, the process being influenced by direct and indi rect trauma or stress, and coexistent disease. Patients rarely attend because their spines are undergoing gradual and silent degeneration with gradual diminution of movement, but because they have pain and other troublesome symp toms in a specified area, and sometimes two or three. 'There is in medicine a natural law that any single man ifestation, subjective or objective, may have behind it a multiplicity of organic causes, just as any single patho logical event is bound to project itself into a number of different clinical manifestations' (Steindler, 1962).1171 It is convenient to use generalised treatment procedures for 'the arthrosis' or 'the spondylosis' as the basic reason for the patient's attendance, yet always more rewarding to broaden an understanding of the infinite variety of ways in which patients can be troubled and try to perceive the nature of the causes and to adapt treatment for the unique form in which the disease affects each one. With regard to affections of the cranial nerves, for ex ample, Brodal (1965) has pointed out that it is somewhat unreliable to attempt fitting a given series of symptoms to one of the many syndromes described, since these syn dromes rarely occur in typical form. The same applies to migraine, of course (p. 218), and especially so to all clinical presentation of musculoskeletal joint problems.
PREFACE
ix
Attempts to eradicate this annoying untidiness, by seek ing to impose artificial order and regularity, where none can yet exist, are foolish. Plato observed that man never legislates, but destinies and accidents happening in all Sorts of ways, legislate in all sorts of ways (see p. 205). There are too many factors involved; very many of the so-called typ ical syndromes arc surprisingly uncommon. This becomes more apparent in direct relationship to the comprehen siveness of history-taking, initial examination and careful palpation. Because there appears to be a gross imbalance among the weight of literature on degenerative change, in that the lumbar disc has cornered a fashionable and ridiculously large share of anemion, I have devoted more space than may be customary to arthrosis, and to seemingly less-vis ited districts of the vertebral column. The subjects of ver tebral traction and the sacroiliac joint have also been given rather more space, since they currently attract considerable interest. The opposite end of the spine, in the form of therapy for headache, already suffers from an embarrasssment of riches-academic debates over migraine become more eru dite and the drugs more exotic with an increasing ball-and chain paraphernalia of side-effects. A very great deal more is being learned about what appears to a clinical therapist to be, in many cases, of little shopfloor clinical value, and we wistfully hope that more time will be devoted to comprehensively examining and palpating the bit that holds the headache up-the cervical spine and the craniovertebral junction. With regard to pathological changes, it has been neces sary to restrict discussion to those aspects which are of first importance in the field of musculoskeletal joint problems; where convenient to do so, reference as is necessary is made in the 'Clinical presentation' section rather than in the more detailed section on 'Pathological changes' (cf. anky losing spondylitis). Where it has seemed to me appropriate I have not hesi tated to cross the somewhat 'watertight' descriptive boun daries of aetiology, pathology and clinical features, for the more effective presentation of important aspects in parti cular spinal regions, e.g. in the section on 'whiplash' in juries, the discussion of surgical problems in the section on biomechanics of the cervical cord and meninges, and the discussion of soft tissue changes. Bourdillon (1973)'" expressed a salient feature of spinal musculoskeletal problems:The paucity of clinical signs and the diversity of symptoms produced by spinal join( disorders confused the medical profes sion[Q
it, or the facilities for help are not as adequate as desired, the patient is given a few generalised exercises and told to 'live with it'. There is the paradox that while musculo skeletal abnormalities are the most frequent cause of de pressing aches and pains, they tend to be regarded as the least rewarding to treat and thus may be the worst pro vided-for. The run-of-the-mill standard of clinical examin ation of these 'uninteresting' conditions is perhaps not always as painstaking as it might be, and the patience of patients is at times unbelievable. The amount of real need is calamitous, and the clinical wherewithal to cope with it ethically, knowledgeably, effectively and with a minimum of vigour, has been sadly thin on the ground. For this reason, the energetic attack with limited means on the important lumbar spine problems by the Society for Back Pain Research will do much good; the cervical region of the vertebral column, and the ubiquitous problems of cervical spondylosis, have also received an increasing vol ume of expert attention 1 11 and, together with the advances in the understanding of pain behaviour, today's clinical workers arc immeasurably better equipped than those of two decades ago. I t may be that the word 'manipulation' will conjure in the minds of many the 'rogue-elephant' manipulator, banging away in a vigorous manner at what ever joint condition may present itself; it may also be that (happily a small) minority of authors with a manipu lative bent, who have acquired authoritative voice and responsibility over the years, have tended to alienate the moderately minded by an habitual style of unbuttoned rhetoric and noisy self-aggrandisement. I quote F. Dudley Hart''':In medicine the authority in the past for some theory of ae tiology or drug action or pathological or physiological process was often some (often professorial) God-like figure and was sometimes based on precious little evidence, but it was accepted as true because (l) it seemed to explain things nicely and often relatively simply and
(2)
the gentleman who said or wrote it
was a great authority.... The God-like physician, proven repeatedly right in the past and venerated and respected ac cordingly, can hold back for years afterwards medical progress by an ... utterance based on inadequate evidence .... It is so much easier for us all to believe in somebody reputable than to work it out for ourselves and see if he was right. ... Most of us perform our medical duties acting on working hypotheses rather than on fixed beliefs, but it is very easy for the one gradually and very insidiously [0 become the other, particularly if one is teaching and lecturing. What I say three times is true, is true, is very true.
such an extent that they were not always recognised as
having their origin in spinal joints.
Occasionally, because the clinical therapist may only partially appreciate what the patient is complaining about, or fully appreciates it but docs not know what to do about
Having travelled the long road from cocksure ignorance to thoughtful uncertainty, I am mindful of the prime need for the younger clinical workers to develop their vocabu lary of anatomical information and their capacities for assessment, because superficial conclusions derived from casually observed phenomena are not always justified. The fact that most strip-clubs audiences are said to comprise
x
PREFACEthe occult nature of many visceral lesions; much efort f required[0
baldheaded old men should not lead to a 'logical' conclu sion that looking at ladies without any clothes on makes the hair fall out. The patient who presents as 'just another old disc lesion' may have a pain behaviour and more subtle clinical signs which only reveal themselves on careful examination. Those who have the wit and the stamina to adopt the attitude of intellectual explorers, rather than opting for an easier and safer pathway as passive recipients of orthodox knowledge, will get more interest and fun out of the pro ceedings and will find the work more absorbing; the overall profit exceeds the pain by a handsome margin. For myself, one of the hardest things I had to learn was concentration on treating the signs and symptoms and nOt unwittingly trying to treat the X-ray appearance, the textbook, the dogma or mechanical concepts of what was believed to have occurred, important though three of these may be. I plead that the medical and physiotherapy schools might devote much more attention to the teaching of ver tebral anatomy and the comprehensive management of benign articular pathology of the spinal column because, like the common cold, there's a lot of it about and its depredations interfere with our economic and social affairs to a sad extent. This is a pity, because a truly remarkable amount of the population's money syphons itself into re search of one kind and another and it is plain that a minor proportion of it might acquire considerable cost-effective ness by being channelled into teaching very many more clinicians and therapists how to recognise and treat by relatively simple means the early painful manifestations of vertebral degenerative joint disease. A summary (Wood, 1980)"'" of the proceedings of a Workshop on undergraduate education in rheumatology, suggests that while the musculoskeletal system is one of the major systems of the body, its status is only infre quently recorded in patients' casenotes.Although considerable progress has been evident since the
encourage all medical colleagues to examine joints
properly ...
It has been suggested that because the conundrum of rheumatoid arthritis will probably be solved within the decade, rheumatology must look to new fields and should turn its main energies to backache. Together with these logical and reasonable observations is included:Suferers f whose pains arc severe will seek help, some from family doctors and some from heterodox healers, the osteopaths, chiroprac tors, manipulating physiotherapists, unqualified bonesetters or others of the host described as 'fringe medicine'.
1971 survey) nevertheless there were still grounds for concernabout the adequacy of rheumatological teaching in many undergraduate medical schoolsj the situation in regard to rehabilitation is less satisfactory. Under the heading of 'Educational objectives' is suggested the fostering of an attitude of 'cooperation in regard to the con tributions that can be made by various health professionals and other members of the team'.
The summary also observes that:... the persisting neglect of the musculoskeletal system is cause for serious concern, and tends to be encouraged by the fact that patients are usually aware of their problem, in contrast to
The writer of such phrases about ethical and competent paramedical workers in the health care team could nm have more plainly bared his deep anxieties. Those who profess to handle the vertebral column must be awake [Q all aspects at all times. Problems, a few of them highly disconcerting, have a habit of looming suddenly and the more so as one slides into an easy familiarity of handling after a 'routine' history-taking. The possibility of serious pathology, and somelimes malignancy, hangs over all clinical presenta tions of vertebral pain. That which presents as a simple joint problem can be the seemingly innocent augury of something more sinister. Not often, but often enough. For this reason alone, the therapist must be soundly and com prehensively informed, always awake and always eco nomical in the use of vigour. There is no other way to avoid serious or catastrophic manipulation accidents. Should there be a message in this book, it lies in the sections on assessmcnt. In its coordinated activity and usc of stored patterns the mind is like a group of prime movers and syncrgic muscles and its ability to grasp, sort and organise information can reach an artistry as perfect as an outfielder's leap for a back-hand catch. I n his essay on Sir Isaac Newton, J. M. Keynes describes the mind-muscle as much like a lens; the ability to gather unrelated bits of knowledge in a new pattern varies from person to person. This ability is an essential quality for the accurate and detailed assessment of joint problems. Anatomical infor mation, painstaking clinical method and basically simple things done carefully and well are more important than the facile acquisition of exotic manipulation techniques. Since we tend, at times, to take ourselves much toO seriously I hope the mild irreverence here and there in the text does not make my more sober colleagues too unhappy. The late Sir Winston Churchill once said that short words were better than long ones and the old words were best of all. I hope there are not too many long words. G.P.G.
Acknowledgments
We climb on the shoulders of those who have gone before, and those who follow will climb on OUf own; we also lean on the shoulders of colleagues and I express with pleasure a debt of gratitude to john Conway (from whom I learnt much about the value of treating patients in (he side-lying position) and joe jeans (whose friendly but incessant demands that I produce a book have now been met), also Freddie Preasrner, Brian Edwards, Peter Edgclow, Marjorie Bloor, Sue Adams, Freddy Kaltenborn, Beryl Graveling, Sue Barker, Shelia Philbrook, Chris Coxhead, and jill Guymer. I wish to acknowledge the fruitful working relationship between Geoffrey Maitland and myself, extending over eighteen years and dating from his visit to St Thomas' Hospital in London during 1961. We have both had the privilege of developing the usc of mobilisation and mani pulation techniques by physiotherapists in our respective countries, and the free exchange of information and ideas between us has afforded me pleasure as well as profit. Figures 2.18, 2.19 and 2.20 arc reproduced from Verte bral MalliplIlalioll (4E) by kind permission of Geoffrey Maitland, AVA FCSP MAPA, and Messrs Butterworth, London. There is an especial place in my regard for Mr P. H. Newman, in whose Tuesday clinics at the Royal National Orthopaedic Hospital I learnt so much about orthopaedic patients. He graciously lent his immense tcaching au thority to the 1973, 1974 and 1975 CSP Manipulation Courses, and has very kindly honoured me by writing the foreword to this book. All therapists will join me in recording our considerable debt to Professor R. E. M. Bowden, Dr D. A. Brewerton, Mr R. Campbell Connolly, Dr j. Ebbetts, Mr A. W. F. Lettin, Dr R. O. Murray, Dr A. Stoddard, Dr j. D. G. Troup, Professor P. D. Wall and Dr B. D. Wyke. To our debt I add my warm personal thanks, also to Dr Basil Christie, Dr Ian Curwcn, Dr Desmond Newton and Mr Hugh Phillips; they have more than once guided my wan dering notions. I am grateful to Professor D. L. Hamblen, Mr P. H.
Newman, Mr H. Phillips, Dr W. G. Wenley and Dr B. D. Wyke for kindly looking at sections of the text and advising mc; faults which remain are my own, of course. Dr A. Burnell's enthusiasm has been a constant encour agement to physiotherapists and we owe much to Dr J. Cyriax, who brought some order to the examination of musculoskeletal problems and upon whose work further developments have been based. Also to Mr W. j. Guest, Principal of the West Middlesex Hospital School of Physiotherapy; his capacity for doing good unobtrusively has benefited physiotherapy more than it knows and I take pleasure in publicly recording my appreciation of his en couragement and support of the CSP Manipulation Courses in the early days, and of myself over 30 years of professional association. Members of the Manipulation Association of Charlered Physiotherapists have been most fortunate to enjoy access to the great and important volume of continental medical literature in this specialist field, and for this are in major debt to the multilingual erudition of my classmate of years now sadly past, Mr H. j. C. Cooper, and to his unfailing willingness (Q burn the midnight oil on our behalf with French, German and if need be Russian translations. It is a pleasure to record my debt (Q the technical skills of Dr john Graves of the Graves Audiovisual Medical Library, Miss Vta Boundy, Medical Photographer to the Institute of Orthopaedics, London, Mr john Tydeman of the Department of Medicallllustration, Norfolk and Nor wich Hospital, and to Anglia Photographics, Halesworth; they have devoted much care and technical skill to the illustrations. To those who patiently modelled during the long and tedious photographic sessions, viz. the late Moira Pakenham-Walsh, Sarah Key, jenifer Horsfall, Kathleen \'\Iinter, Denise Poultney and Fiona Percival, J am very grateful. To Mrs M. Moore, Librarian of the Norfolk and Norwich Institute of Medical Education, and to Mr C. Davenport and Mr P. Smith, respectively the previous
xii
ACKNOWLEDGMENTS
and present Librarians of the Institute of Orthopaedics, London, I gratefully acknowledge the efficient help I have been given. I thank Mr G. T. F. Braddock for generously providing photographic evidence of a unique experiment, which raised my interest when described, and for allowing me to publish it. Professor Peter R. Davies has been especially generous with advice on expression of magnitudes in S-I units. Mrs J. Whitehouse, The CSP Journal Editor, has kindly
allowed me to reproduce very many figures and passages from my writings in Physiotherapy. I thank Mr B. Holden of Carters Ltd, Mr N. Peters of The Tru-Eze Co. Inc. and Mr J. Maley of the Chattanooga Pharmacal Co. for promptly sending me the illustrations I had requested. Every care has been taken to make the customary ac knowledgment to holders of copyright, but if any copyright material has inadvertently been used without due permis sion or acknowledgment, apologies are offered to those concerned.
Contents
1. Applied anatomy-regional
7. Clinical features
159 160 161 176 189 196 196 199 200 202
Cervical Thoracic Lumbar Pelvic Surface anatomy2. Applied anatomy-general
3 13 17 29 31 36 36 36 38 53 56 62 64 69 74 77 82 82 88 94 110 121
Articular cartilage Lubrication of synovial joints Vertebral movement Inrcrvcrtcbral foramen Biomechanics of spinal cord and meninges Venous drainage Autonomic nervous system Patterns of somatic nerve root supply3. Aetiology in general terms 4. Incidence 5. Pathological changes-general
Neurological changes Pain and tenderness The autonomic nervouS system in vertebral pain syndromes Referred pain Abnormalities of feeling Changes in muscle and soft tissue Deformity Functional disablement The psychological aspect of vertebral pain
8. Common patterns of clinical presentation
205 205 206 229 232 250 279 300 303 303 322 322 324 326 327 328 334 336 341
Arthrosis and spondylosis Upper cervical region Cervico-thoracic region Thoracic region Lumbar spine and pelvis The pelvic joints Neoplasms9. Examination
Synovial joints Symphyses (Intervertebral body joints) Nerve root involvement Soft tissues Neoplasms6. Pathological changes-combined regional degenerative
125 125 129 134 138 150 151 157
Cervical spine Cervico-thoracic region Thoracic spine Lumber spine Sphincter disturbance The pelvis Serious pathology simulating musculoskeletal pain
Introduction Regional Examination procedures Cervical region Shoulder and clavicular joints Thoracic region Lumbar region Pelvic joints Hip Passive physiological movement tests Recording examination10. Assessment in examination-Prognosis
350 369
11. Investigation procedures
xiv
CONTENTS
12. Principles of treatment
376 377 378 38 38
Aims of treatment Definition of passive movement techniques Manipulation in general terms Grouping of techniques13. Recording treatment and clinical method
Localised manipulation Regional manipulation Exercise Contraindications16. Supports and appliances and adjunct physiotherapy treatments 17. Medication and alternative methods of pain relief 18. Prophylaxis 19. Invasive procedures
463 464 464 465
435
468
Use of technique Selection of technique Assessment during treatment14. Exercises 15. Indications for passive movement techniques and exercise
441 442 444 45 1
483 496 51 4 5 14 525 535 559
460 460 460 46 1 462 462 462
General indications Softtissue techniques Localised mobilisation Regional mobilisation Stretching CA) Mechanical harness traction
Minor procedures Major surgery with indications for seeking surgical opinionReferences Index
For Barbara Grieve-the other half of the team
and lO our melltor, Ted Goldblatt, with affection alld regard
1. Applied anatomy-regional
A shore general summary of vertebral structures and their function may usefully precede descriptions of degenerative change and irs consequences. Where indivi dual features require morc extended discussion, this has been included in the appropriate sections throughout the text .
Because structural variations have considerable impor tance in this clinical field, and their likelihood always worth bearing in mind, some anomalies have been in cluded with regional descriptions; reference should sooner or later be made to fuller and more detailed accounts. )15,881,1274,109)
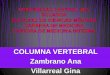
Fig. 1.1
(A) Anterior aspect ofthe venc:bral column. Note the variations in
length of transverse processes. (8) Lateral aspect. Note: the varying configuT8lions and size of spinous processes.
2
COMMON VERTEBRAL JOINT PROBLEMS
frequently, cardiac and renal abnormalities occur, and there may be congenital malformations of the gastro intestinal and respiratory system. lOGO
I. Symphyses, i.e. secondary cartilaginous JOints, between the vertebral bodies, with their interposed discs. The upper rwo synovial joint segments have no disc-;;d are therefore not symphyses, besides showing other atypi cal features. 2. .$.JJ1lovial joints, also called zygapnphyseal or facet joints, bctween the articular processes of the vertebral arches. The anterior symphysis together with the 2 pos terior facet joints typically form one of the 'mobile segments' of the spine, totalling 25 including the upper 2 atypical segments. 3. In the cervical spine only, a further group of small articulations rcquires consideration (Fig. 1.4): these are 1091 j the Q!ired oinlS of Luschka, the uncovertebral orneuro central articulauoQs. situated in the uncovertebral region on each side between the outer posterior margins of the vertebral bodies, at the five segments berween the second nd seventh yerrebrae.548
The join" of the vertebral column (Figs 1 . 1 , 1 . 2 and 1.3) at:! of three kinds:
Fig. t.2 Lateral aspect of cervical spine. Note the large and prominent spinous process of C2. the distance between the posterior tubercle of the arch of atlas and the C2 spinous process. and the somewhat depressed spinous processes of C3, C4 and C5. Tip of lateral mass of atlas is palpable between mastoid process and mandibular angle.
ArtICular facet on supenor ____ -= aspect -of atlas
Lateral t op ofatlas
---1'
Transverse
m-----,
--_ Cl--{;2ofC2Bifid
C2
facet joint
spflnous ocess
ofC2
Fig. 1.3 PoSterior aspect of the craniovertebral region. Note the lateral tip of atlas extending well beyond the transverse process of C2. The mastoid process of the temporal bone would lie laterally to the margins of the illustration.
APPLIED ANATOMY-REGIONAL
3
CERVICAL SPINEBecause the consequences of arthrotic and spondylorjc changes in the neck arc usually more marked and wjde_ spread than degeneration of other spinal regioos, the salient facts of anatomy and articular function in this area need careful consideration.''" 475,1)54,1)55.1)57,1364,967,1242A. UPPER CERVI C AL SPINE
(Fig. 1 .5)
T niovertebral re ion is of importance, as some 0 the most essential atwrcor jmpulses or the static and dynamic regulation of body posture arise from receptor sY stems in the connective tissue strucrutes and mpscles around the upper vertebral synovial joints. The impor tance of their func[tonal role is clearly demonstrated, for example, in consideration of the tonic neck reflexes. posture governs body posture and limb control; abnor malities of afferent impulse traffic from joint receptors, because of degenerative changes, can be expected to reduce the efficiency of postural control and produce the alarming symptoms of defective equilibration. Experimental cervical lesions jn monkeys jmm)ving u ilatera! section of u per cervical dorsa r duce bo y dysequilibrium; and positional n stagmus, in rabbits, IS cause y oc 109 the articular receptors in the intervertebral joints and ligaments. 586,587,188, U8, 136.J
F11r. 1.5 Anterior aspect of upper cervical region. There is chondro osteophytosis at C3-4 facet-joints on either side, and also at C4-5 on patient's left side.
OccipitoatlantaJ joint
verging anteriorly, with the lateral edges of the facets 00 . the atlas banked u a saucer, which somew IgS . , 1.5). stricts other than sagittal movs The r:QugblycirclJlar facetsofboth atlas and axis are not quite reciprocally curved; the convex upper axial surface receives the irregularly concave inferior facets of the atlas 'like the epaulettes on a pair ofsloping sho"lders'; the facet-planes being about]]0 totbeyertical Theposterior face of the anterior arch of atlas abuts against the front of the odontoid, a small synovial cavity intervening; a si!11ila all bursa or synovial oint intervenes between the posterior face 0 e odontoid and its strong retammg
The convex occipital condyles, and reciprocally concave articular surfaces of the atlas, have their long axes con-
Atlantoaxial j oint488 S58
Fig. 1.4 Anterior aspect of cervicothoracic region. The uncovenebral region at C5-6 level shows the sclerosis of bony margins and flanening of the C6 uncus on the patient's right side. Compare with uncovertebral region of C6-7 space.
Fl. 1.6
Frontal view of the atlas and the axis.
4
COMMON VERTEBRAL JOINT PROBLEMSPosterior Cranial Fossa
Antertor
Posterior
2 3 4
10"
12 13
Fig. t.,
Fig. 1.8 The lateral atlantoaxial joint appears biconvex. 2. 3. 4. 5. 6. 7. 8. 9. 10.
I. Anterior longitudinal ligament
Median and paramedian section of cervical structures.
(Figures 1.6 and 1.7 are reproducM from Hohl M, Baker HR 1964 The atlanto-axial joint-rntgenographic and anatomical study of normal and abnormal motion. Journal of Bone and Joint Surgery 56A: 1739. by kind permission of the authors and the Editor.)
fibrQus band Ihe Ir"D'Y'me ligament (see below) (Figs 1 . 5, 1 . 6, 1 . 7).
The craniovertebral ligaments These shared by both articulations are of much functional importance, as osteoarthrotic changes are common in this f re ion following stress and trauma and th yst possible Igamentous lOsufficiencym be bornein mind during treatment (Fig. 1 . 8).'98 From before backwards, they are: 1 . The anterior occjpitoatlantal membrarJe, continuous below with the anterior longitudinal ligament and blend ing laterally with the capsules of the facet-joints. l 2. The \pin qpica ligam!!,l, attaching the tip of the odontoid to the[Jor margin of the foramen magnum (Fig. 1.9). 3. The Q!ore laterallyplaced and tougher alar ligaments, attaching the posterior part of the odontoid tip to the lateral margin of the foramen magnum on each side. . 4. The transverse liggmem of the atlas, a strong fibrous band connecting each lateral mass across the front of the neural canal and passing behind the odontoid; it is a vital re..!,aining structure stabilising the odontoid in the bony ring of atlas, and is mainly responsible for the integrity of the atlantoaxial joi . TJle ligament has a cruciate form, w ertical bands of less functional imporrance ex!endjng"pward and dowmva. 5. The accessory atlqntOaxial ljgmueuu , w.!!ich pass upward and . f2 th bas QLlhl:jefcriNyertlcal ' 1D e band of the se of the odontoid process with the inferomedial art of the lateral he median atlantoaxial (or atlantodental)
II.12. 13.
Anterior atlanto-occipital membrane Synovial joint between anterior arch of atlas and odontoid Odontoid process Apical ligament of odontoid Synovial joint between transverse ligament and odontoid. NB. 3 and 6 comprise the median atlantoaxial joint (q.v.) Transverse ligament of atlas Membrane tectoria-the upward continuation of the posterior longitudinal ligament Posterior longitudinal ligament Foramen for first cervical nerve and vertebral artery Foramen for second cervical nerve Ligamentum nuchae Capsule of facet joint between the right side articular processes of C2 and C3.
(Reproduced from Kapandji IA 1974 The Physiology or the joints III (the trunk and vertebral column) p 187, by kind permission or the author and Librairic Maloine S.A. Paris.'
joint is very frequently the seat ofarthrotic change. more so than in the two lateral articulations.1174 \ 6. The membrana leeroo'a, being the upward prolonga tion of the posterior longitudinal ligament, covers the pc:cerljngstryctures posteriorl)' it is attached below to j the base of the odontoid, and above to the clivus of the basiocciput. 7. T.he posterior occipitoatlamal membrane completes
Apical l)9am"\-
2nd
. --j'--- 5th A.P.R.Fig. 1.13 Laleral aspect of upper five cervical verlebrae. The first two cervical roots emerge behind the facet-joints; all others emerge in front of the facet-joint. Arthrosis of the joint twr:en C2 and C3 frequently involves the nerve rOOt and rami by trespass upon il of degeneratively thickened tissues. (After Lazorthes G 1972 Ann. de Me-d. Physique 15: 192.)
8
COMMON VERTEBRAL JOINT PROBLEMS
other than pain (sec p. 299), some of which arc certainly due ta involvement of the autanamic system and which often accompany vertebral pain syndromes. At the u er two se menlS the spinal nerve roots emerge postero aterally behind the articular pillar an a ove the posterior arch at the numencatly correspondm vertebra' the first cerVlca nerve root s ares a foramen in the pos terior atlanta-occipital membrane with the vertebral artery and vein ( Fig. 1 . 1 3). All the orher spinal nerve ropts down to the level of the 5th lumbar eerge in front of the facet-jojnts Shore (1935)"" mentions that while the skin does not receive a direct supply from the first cervical nerve, because ofa communication with the second cervical nerve
C l has a share in supply of the cutaneous area to which the greater occipital nerve is distributed.
I5liiTrlg their passage towards the foramina, the fibres of the roots leaye thespjnalcordat the level of the numeric ally corresponding vertebral body, and do not pass later r all in such close relationship to the disc as do the I nerve roots see p. 24). onsequent y, although spinal cord and nerve root compression can occur by pathologi cal changes in the discs, its mode of production differs somewhat to that in the lumbar region. During their pass en t s are age through the interverte boun e 10 front and behjnd bygtrpcwres very likely tosympathetIC trunk
C2-C8
Fig. 1.14 Innervation of related cervical vertebral structures in transverse section. Muscular branches of the dorsal ramus supply the articular capsule. Pans of the vertebral plexus are seen within the foramen transversariuffi, together with vertebral vein and artery, and showing smaller but macroscopic ganglia in this situation. Communications of the plexus are seen with the spinal ganglion, dorsal and ventral rami, and the sympathetic trunk (and via this branch to the periosteum and marrow of the vertebral body and the anterior longi[Udinal ligament). Other branches are directed medially to the periosteum and spongy bone of the body and via the meningeal ramus to the dura mater and posterior longitudinal ligament. (After: Stillwell DL 1956 The nerve supply of the vertebral column and its associated struCtures in the monkey. Anatomical Record 125: 139. Reproduced by counesy of the Director, Wistar Press.)
APPLIED ANATOMY-REGIONALuce pressure or irritation by exos(Osis, these being the p fa e -'oint structures postero atera y and the 'neuro central joints' anterome la y. Cervical spine nerve roots have a rough segmental identity, i.e. after union of the ventral and dorsal rootlets, the roots emerging frow thejnteryertebral foramjna cor respond nymerically with the vertebra below (excepting that of the 8th cervical) and the appropriate segment of the spinal cord. Nevertheless, a few rootlets of the cord may ascend or descend to join and emerge with the spinal root numbered one above or one below the cord segment giving rise to them, and the lowest spinal cord rootlets contributing to a spinal root may be lower than the foramen for that nerve, and therefore have to ascend slightly to reach their exit from the neural cana1. 537 Paradoxically, the nerve supply to the vertebral column structures themselves is much I seqmentall ed, 1177 a rich netbem en work of fibres occupying the region of the somatic nerve roots and the sympathetic ganglia (Fig. 1.14). Wyke (1979)"'" observed that,articular branches of its own segmentally related spinal nerve Each cervical apophyseal joint
9
is
innervated not only through ut
.1.0 it and ascend to it from the caudally located nerve rOOt.
also by articular nerves that descend to it from the nerve root rostra
,
There are plentiful interconnections with the sympath etic grey rami communicantes, the inferior, middle and superior cervical ganglia, the spinal posterior root gan glion and the anterior and posterior primary rami. Mixed efferent autonomic fibres and afferent somatic fib
rived from this plex-us -fo-rm (ramus meningeus), usually compnslOg two or more branches which re-enter the foramen to supply structures ,\,ithin the vertebral canal (Fig. 1.15). Mixed branches from the paravertebral plexus also pass externally to the sides, front and back of the vertebral bodies, supplying periosteum and ligaments; many join with the medial branch of the posterior primary rami of each spinal root, thereby reaching and serving the rich and varied receptor population of the facet-joint structures (see p. 10). Each 'mobilit se ment' receives fibres derived from es together with sympathetic three a postganglionic fibres innervating the blood vessels therein, and these approach from a variety of directions; in addition to this segmental overlap, from outside, the branches of the sinuvertebral nerve within the neural canal may wander up and down for two or three or more segments before they terminate in receptor endings (Fig. 1.15). T.be extension of nerves supplyin g the vertebral column beyond their segment of or' . om arable to the mal innervation on the body s Ascending branches ofmixednenres withjn thenellra! canal, derived from the upoer three cervical segments, sli Iy the dura mater of the posterior cranial fossa, and may be concerne at urnes 10 the production of occipital headaches.657>
r
The autonomic nerve supply The supply to the head and neckis derived Cal from the three cervical sympathetic ganglia in this region, with (b)
Fi,. 1.15 Posterior aspect of spinal canal. The sinuvertebral nerve (ramus meningeus) may wander up and down for two, three at more segments before terminating in receptor endings. (After: Wiberg G 1949 Back pain in relation to the nerve supply of the intervertebral disc. Acta otthopaedica scandinavica 19: 211.)
10
COMMON VERTEBRAL JOINT PROBLEMS
parasympathetic connection,L contributed by cranial y nerves (particularl the glossopharyngeal and vagus) (Fig.1.14).",
4"
Although it is customary to regard the first thoracic segment as the uppermost level for emergence from the neuraxis of preganglionic sympathetic neurones, the work of Laruelle,699 Guerrier,4L Delmas and Laux2r-2
CoccyqeolFig. 2.13 The level of spinal cord segments i n .elalionlO
Cocc y xvertebral levels. The spinal cord ends a l L 1 - L2.
foramen varies between 1 2 and 19 mm, but the transverse diameter may be as little as 7 mm, and the opportunities for foraminal encroachment due to hon'zomal trespass are much greater. Diminution of the transverse diameter is more likely to embarrass the foraminal contents, and this space-occupy ing effect can be due to abnormalities of the disc and facet joints, so often the cause of acquired spinal stenosis. Nerve tissue will tolerate slow compression quite we1l282, )92 and marked trespass may not give rise to much detectable dis turbance of function, although repeated frictional trauma against encroaching degenerative thickening, and exos tosis, may be the more likely cause of reactive changes in the nerve and consequent development of signs and symptoms.
It is a curious fact that in both the lower cervical and lower lumbar regions, where spondylotic changes are very frequently responsible for a reduction in foraminal dimen sions, the foramina should be naturally smaller than in the middle and upper parts of these regions (see also 'Bio mechanics of spinal cord and meninges', below). When the transverse dimensions of the lumbar fora mina appear developmentally reduced, and this is detect able on plain lateral films in the absence of acquired foraminal encroachment by spondylosis and arthrosis, a narrow neural canal (spinal stenosis) is almost certainly present.
56
COMMON VERTEBRAL JOINT PROBLEMSDura mater (open sac) C7 ca Spmal cord
of their significance for those who treat vertebral de generative change :The primary source of meningeal and neural tension is the lengthening of the spinal canal on forward and lateral flexion. Normally, the soft tissues adapt freely to these skeletal move ments ; bUl in [he presence of space-occupying lesions involving the spinal cord or locatcd in the cord itself, and when there are sclerotic or fibrotic lesions that restrict the mobility or extensi bility of nervous and meningeal tissues, the tension may be much increased. Even when the pathological lesion appears to be exert ing an essentially compressive effect, the resulting deformation leads to a local increase in tension ; it is the effects of this raised tension that appear to be of primary neurophysiological signifi cance . . . excessive tension in the cord may produce measurablc changes in motor, sensory and autonomic function. These are accentuated whenever the cord is slretched, and may be reversed, and the symptoms relieved, if stretching can be eliminated and
T1
T2
T3
T4
the aff ected tissues are kepl relaxed. Even in the presence of irre versible myelopathic lesions, whether focal, sclerotic or space occupying. the existing symptoms and neural function can be improved significantly by surgical measures designed to prevent overstretching of the cord. In the course of clinical enquiry over nearly two decades I have found that many neurological disorders in which no mechanical component has ever been suspected do in fact have their origin in tension in the nervous tissue; we are at present only just beginning to recognise the histological and neurophysiological sequelae of this tension . . . . Biomechanical
T5
T7
m01foot Ventral rootlets
analyses were extended to the micToscopical level. These analyses have shown that tension in the nervous tissue that gives rise to symptoms is characterised by focaJ deformation of its complex three-dimensional fibre nerwork as seen in histological and microangiographical sections. It was evident that an important cause of functional disturbance both of the axis-cylinders and the blood-vessels lies in the reduction of their cross-section area resulting from tension. By slackening the nervous tissue the ten sion is relieved and the conductivity and circulation are restOred.
Cui edge of pedIcleAntenor aspect of dura mater
Fig. 2.14 Scheme of cervicothoracic root angulations-anterior aspect (sec leXt). (Afler Nathan H, Feuerstein M 1974 Angulated course of spinal nerve roots. Journal of Neurosurgery 32: 349.)
BIOMECHANICS OF SPINAL CORD AND MENINGESIn the presence of mechanical derangements such as disc pro lapse, or the bony and soft tissue hypertrophy of osteoarthrosis where there is encroachment upon the dura and nerve roots, and where adhesions may follow a local irritative state, there is need to distinguish between the possible causes of pain on movement. (Troup, 1979) 12'10b
I n his foreword to Breig's ( 1 978) " '" detailed observa tions on adverse mechanical tension in central nervous system tissues, Verbiest remarks that the observations are of much importance not only to specialists in the neurosciences and orthopaedic surgery, but also to anaesthetists, whose activities regularly involve the positioning of defenceless patients, and last but not least to physiotherapists, for reasons which need no elaboration. Breig introduces his study in words which leave no doubt
Nervous tissue and the meninges have different proper ties and therefore show different behaviour under mech anical stress ; this has important inferences when consider ing the effects of vertebral movement. Nerve tissue is almost semifluid-if cut transversely it tries to flow. The sciatic nerve, for example, can stretch, it is elastic.l Okf, 4 1 6 While a sudden stretch may interfere with it considerably, a slow stretching may be tolerated without undue reactive changes. The meninges differ. The more delicate of them can stretch and enlarge circumferentially, because much of the arrangement of their fibres is around the long axis, pre sumably to accommodate arterial pulsation, but they can not stretch very much along the longitudinal axis of the cord, e.g. when extended to around 5 per cent of their nor mal length they are taut. STRUCTUREThe outer layer of the dura marer) basically white fibrous tissue predominating over some elastic fibres, is con-
APPLIED ANATOMY-GENERAL
57
tinuous above through the foramen magnum with the in ner layer of the intracranial dura mater. The spinal canal continuation of the outer (endosteal) layer of the cranial dura mater is represented by the periosteum lining the vertebral canal. In the canal the space between the two layers is the epidural or extradural space, almost entirely occupied by fat, loose areolar tissue, and the rich plexus of vertebral veins,'n7 The caudal limit of the subdural cavity lies level with (he second sacral segment, the dural tissue then extending caudally, as an increment ofthe filum terminale of the spi nal cord, both of which structures end by blending with the periosteum on the back of the coccyx. In addition to these cephalic and caudal attachments the spinal dura mater is attached by fibrous slips to the back of the vertebral bodies of C2 and C3, ' " and also to the posterior longitudinal ligaments of the lumbar segments. In the lumbar region the binding of the dura is most firm along the lateral edges of the long superficial strap fibres of the posterior longitudinal ligament, with numerous cross connections of the epidural venous sinuses passing between the trabeculae of connective tissue which join the dura and ligament. cm Investments of dura mater are continued laterally through the intervertebral foramen (see p. 54) with the combined spinal nerve roots for a short and variable dis tance, as a root sleeve, or root ostia, blending with the con nective tissue perineurium.Variations occur with regard to angulation and maldevelop ment and/or malformation of cervical root pouches and root sleeves. }O2
the lower extremity of the subdural cavity at the second sacral segment. It lines the dural root sleeves, providing with the dura an investment of the ventral and dorsal spi nal nerve rootS but is not, like the dura, continued distally beyond the formation of the combined spinal root, i.e. it terminates by linking the adjacent layers of dura between the ventral and dorsal roots) thus contributing two laminae to the interradicular septum. In this situation both dura and arachnoid are sus ceptible to the repetitive, minor, mechanical trauma of stretching, and of impingement on adjacent foraminal margins as a consequence of degenerative change altering foraminal relationships; the resulting granulation tissue frequently leads to fibrosis and scarring, with the tethering effects of root sleeve fibrosis'" (see pp. 1 00, and 102).The innermosl /ayer, the pia maler, is a highly vascular and delicate membrane consisting of fine areolar tissue sup porting numerous small blood vessels, separated from the arachnoid by the subarachnoid space, which contains the cerebrospinal fluid. The spinal membrane is alto gether firmer and thicker than the intracranial pia mater, and it is intimately adherent to the spinal cord, lining the anterior median fissure and forming a sheath for the ventral and dorsal spinal roots as far distally as the inter radicular septum. It forms the ligamentum denticulatum, a series of tri angular tooth-like processes lying between ventral and dorsal roots and extending laterally to attach by their points to the inner aspect of the dura mater. The 21 pro cesses on each side begin at the level of the C I spinal nerve root and end between the levels of exit of T 1 2 and LI roots. The upper 'teeth' are almost perpendicular; the uppermost and stoutest of these is attached to the dura inside the posterior cranial fossa, behind the canal for the 1 2 th cranial nerve. The ligaments are organised to sustain a degree of tension, and when cut from their dural attachments they contract right down to the cord. The position and form of the dentate l igaments change during vertebral movement. ) 1 4 The pia mater ends with the termination of the spinal cord, the conus medullaris, at the level of L I-L2 vertebral segments, and thereafter a fine filament of connective tissue, the filum terminale, descends from the caudal apex of the conus to attach to the dorsum of the first coccygeal segment. The roots comprising the cauda equina therefore embrace the filum terminale. Particularly in {he cervical spine, the dural root sleeves are loosely attached to {he margins of the intervertebral foramen. I IQ]
Bowden, Abdullah and Gooding ( 1 967) ' " observe that the paired root sleeves of dura and arachnoid mater are loosely attached to the margins of the cervical foramina. These attachments increase in strength with advancing years and degenerative change. Sunderland ( 1 974),"" with regard to the remainder of the spine, describes the nerve complex as not attached to the wall of the foramen, the arrangement permitting the complex to move within and through the foramen ; Hollin shead ( 1 969)'" reports the first sacral nerve as attached to the margins of the intervertebral foramen. On leaving the foramen, the 4th, 5th, 6th and 7th cervical roots are more strongly attached to the vertebral column, each lodg ing in the gutter of the transverse process in which it is securely bound by its epineurial sheath and by reflections of the prevertebral fascia and other slips of connective tissue. 119lThe middle layer, o arachnoid macer, is a more delicate f membrane and is separated from the dura mater by a potential space which contains a trace of serous fluid. The arachnoid mater is continuous above with the in tracranial arachnoid membrane, and ends caudally with
EFFECTS OF VERTEBRAL MOVEMENT The coverings of the spinal cord permit it [0 move about within the limitations imposed by connective tissue tethering, the nerve roots, cranial and caudal attachments
58
COMMON VERTEBRAL JOINT PROBLEMS
and the ligamentum denticulatum. The dural sac changes its configuration considerably during exertion and strain ing. These effects are observed myelographically when the patent is asked to strain.'15 While the spinal cord, meninges and nerve roots are affected by vertebral movement, postures and pressure differences, 1 l 9 the cord does not slide up and down the neural canal to any appreciable degree-its movement in the cervical spine, for example, is only 2-3 mm at the most, although Reid ( 1 960) 00" refers to higher averages. The cord and its attachments deform like an accordion as the dimensions of its protective canal change with move ment. I l06 I t sustains tension, and its position relative to the anterior and posterior wall of the canal is changeable. The reason why cord and dura become taut together appears to lie in the nature and number of ligamenta den ticulata. Any small up-and-down movement of either cord or dura is quickly transmitted one to the other. Pull on nerve roots transmits its effects to the cord via the dural sheath and the dentate l igaments rather than via the root lets. Cephalic traction on the dura is found to be equally as effective in applying tension to the cord as is caudal traction. 1 024 I njuries to the cord and nerve roots may come about as a result of loss of plasticity, ischaemia induced by either local or more remote effects, pathological displacement of vertebra, degenerative trespass by structures forming the protective neural canal and by violent traumatic distrac tion of nerve root attachments. After degenerative change of the cervical intervertebral discs, for example, when the vertebral bodies settle like a pile of dishes, the neural canal is shortened and the relatively inelastic dura mater will fold. Since it is tough, in certain circumstances the folds may produce lesions due to trespass upon structures within the canal. 1 1 7Adhesions following haemorrhages, exudes and inflammation will cause shrinkage and stiffening of the tissues and loss of elas ticity of membranes. This, in turn, leads to abnormal tensions on the cord and nerve roots. . . .
rowing of the canal or by abnormal tethering of the cord in an anterior position. l20 A further and important factor is cord ischaemia due to trespass upon vessels sometimes remote from the site of its most potent effects.656, 426 The radicular arteries invariably lie on the anterior aspect of the nerve root. Active movements normally exert effects of tension and relaxation of the spinal cord, men inges and nerve roots.981 Whenever the cord shortens or lengthens, its cross-sectional area increases or decreases respectively. 1 20 During extension of the cervical spine, for example, the spinal cord and roots become relatively slack, l I7and the flaccid cord deviates according to gravity towards the front or back of the spinal canal, depending upon the prone or supine position. 120 The canal is nar rowed from front to back, and small ridges are raised over each disc on the anterior wall of the canal. 10201 The inelastic dura mater cockles up to a degree and the elastic ligamen tum flavum bulges forward into the neural canal. In flexion , the slack in cord and roots is taken up, and tension in them rises ; the stretched cord is strongly applied against any spondylotic ridges or protrusions which may be presenr. I )O Flexion of the cervical spine places tension on the lumbar and sacral nerve roots, as well as those of the cervi cal and thoracic region. l l 91 During rotation dorsal roots on the same side are stretched and anterior roots relaxed, and opposite effects are produced on the other side. Lateral flexion, as would be expected, shortens the neural canal on the same side and lengthens it on the opposite side. The inextensible dentate ligaments ofrhe pia mater can, during neck move ments, exert undue traction on the spinal cord when rela tionships have been disturbed by degenerative change. Microscopic studies s how that while the longitudinal neurones of the spinal cord are straight during flexion, they assume a wavy course when the cord is relaxed during extension. DO On cervical flexion, extension and rotation, the spinal cord follows the shortest route through the neural canal'" and consequently the form of the cord substance, its tracts and neurones and its blood vessels are modified by these tensions, distortions and relaxations. A bony protrusion, thickened soft tissue or a ventral neoplasm of the spinal cord will deftect the cord back wards as a flat bow, during cervical flexion. Further, a localised intramedullary haemorrhage, a glial scar of demyelinating disease, intramedullary tumours and con nective-tissue scars from cord injury will force the sur rounding tissue into a spindle-shaped formation. 1 2 1 The intensity of effect upon individual neurones increases with the size ofthe impinging structure and the degree of spinal cord tension. In a study of 42 unselected autopsy cases, Breig, Turn bull and Hassler (1 966)120 describe deformations of the cord induced by flexion and extension movements in those
It has been suggested that the dentate ligaments hold the cervical spinal cord against the spondylotic ridges, 62b bur division of these ligamentous 'teeth' does not have any effect on minimising cord pressure against the ridges. 1 024Cervical region Many authors have drawn attention to the discrepancy which may exist between the severity of signs and symp toms in cervical spondylosis and cervical myelopathy, and the minor nature of protrusions into the canal, or lack of evidence of cord compression. Elucidations of the factors underlying the discrepancy concentrate on the mechanical means whereby during certain movementS and postures the cord may be forcedly compressed against any pro trusion present, and its free mobility hampered by nar-
APPLIED ANATOMY-GENERAL
59
with and without spondylosis. The spinal cord speci mens were grooved anteriorly where it has been pulled taut over t he spondylotic bars in 1 3 of the 17 preparations fixed in cervical flexion. The spinal cord became flattened with the A-P dimensions reduced. The flattening was fre quently bilateral, although unilateral in some. The authors observe that pressure on the anterior spinal artery or arteries during cervical flexion may inhibit blood flow past a spondylotic ridge during life. Little blood would flow through the capillary network when it had been flat tened by the stresses which flatten the cord opposite a spondylotic ridge during flexion. Nervous tissue is highly vulnerable to anoxia. Circulatory depletion for around 1 0 minutes is enough to cause injury. Barre ( 1 924)" suggested that the myelopathy of cervical spondylosis was caused by ischaemia, noting that degenerative trespass upon radicular arteries would impair the blood supply of the cord. Freid, Doppman and Di Chiro ( 1970)'" studied the cervical cord blood supply in rhesus monkeys, and their findings indicated (a) that blood enters the cervical spinal cord mainly from the radicular arteries, and (b) it is doubtful that the vertebral arteries provide its main blood supply. Gooding ( 1 974)'" draws attention to the fact that the myelopathic cord is seldom compressed when seen at operation, and even when compression is present, there is often a disappointing lack of clinical improvement when the compression is relieved. 1200In less than half of the patients with this condition does the level of the neurological abnormality correspond to the radiological levels of the bony lesions. I I Z
uncommonly seen at operation and can be experimentally produced by trauma. In dogs, experimentally induced moderate cervical cord compression and ischaemia com bined, produced more severe loss of vascular autoregula tion, and more severe myelopathy, than either mechanism alone.425 In summary of the author's comments, degenerative change appears to remain the culprit, and possibly in the forms of spondylosis of the vertebral interbody joints IOgether with fibrosis of the meningeal lamella of the root sleeve. Whether cervical flexion, by exerting tension on the contents of the intervertebral foramen, or cervical extension, by approximating the margins of the foramen, be the more potent movement or posture exacerbating the condition is probably a factor varying between individual patients, but cervical flexion would appear to be the posture responsible for the two-fold effects postulated above. The probability that cervical myelopathy may be due to the combination of compressive and ischaemic factors is supported by the experimental findings of Hoff et al. ( 1 977)'" who discuss the multifactorial nature of the pathological changes. When the cord is relaxed, the cord tracts and neurones are no longer subjected to pressure and distortion, and in a variety of neurological disorders a striking reduction, and even abolition, of symptoms can be achieved by surgi cal immobilisation of the cervical spine in a position of slght extension. I Z l a iCervicothoracic region Nathan ( 1 970)"" observed that in a majority (76 per cent) of cases a variable number of spinal roots, more usually in the lower cervical and upper thoracic segments, fol lowed an angulated course. Within the dura, the rootlets proceeded downwards for a variable distance and on piercing the dura were sharply angulated upwards to reach the portal of the intervertebral foramen. Since the extra foraminal course is again downwards, a handful of spinal roots (commonly occupying a j unctional vertebral region prone to trespass by thickened degenerative tissues) have undergone two fairly marked angulations by the time of their emergence from the foramen. The degree of angula tions may be as much as 30 and can reach 45 (Fig. 2 . 1 4). Irregular and uneven development at the dural sac has been considered as the possible cause of these angulations which may, of course, be further distOrted by degenerative changes, particularly dural tethering within the neural canal and root-sleeve tethering at the foramen. The roots affected are those between C6 and T9, with T2 and T3 most frequently and severely angulated. The angulations are increased when the neck is extended. Thoracic spine Reid ( 1 960)'024 refers to the natural elasticity of the cord
There is the paradox of ischaemic myelopathy without an obvious vascular lesion. Spondylotic trespass is plain, compressive dis[Qrtion of the cord's normal configuration on neck flexion is plain and local interference with its vascularity is plain. Pathological studies of spinal cord lesions656 support the view that local ischaemia is the final step in pathogenesis of spinal myelopathy. l zo Yet atheroma of the spinal cord vessels, even in severe myelopathy, is very rare ; 704 also, Breig observed that no occluded radicu lar artery had ever been demonstrated postmortem in cases of cervical myelopathy. Gooding4Z5 comments that the radicular arteries form an important part of the cord's arterial supply184 and men tions that since they traverse the IVF they are almost always involved in fibrotic change of the dural and arach noid ostia of the root (Frykholm's root sleeve fibrosis, p. 102), associated with degenerative change. He observed that irritation of these vessels by trespass upon the fora mina by degenerative tissue, producing segmental vascular spasm of the pia mater arterial network, combined with moderate cervical-cord compression, may be the twofold mechanism underlying the production of myelopathy. Arterial spasm of the radicular and pial vessels is not
60
COMMON VERTEBRAL JOINT PROBLEMS
and the dura, describing the degree of dorsal lift in the cadaver when the spinal canal is unroofed, but not specify ing the degree of longitudinal distraction observed upon experimentally applied tension to a portion of it. Dorsal movement by free lifting, of about 1 cm, was found at the TS level in about one-third of the cases, although in others the dura seemed rather tight; in the aged, especially, the entire dura appeared crinkled and slack. He studied cord and dura movement in 1 8 necropsy cases with spines nor mal for their ages, i.e. I I males and 7 females between I S-S7 years, with an age average of 37 years. At all levels of roots C8 to TS, for example, movement took place both in flexion and extension with a total range of move ment of up to 1 .8 cm. It was not infrequent for the cervical dura to be quite taut in flexion, while that in the thoracic region was still loose and wrinkled, probably due to connective-tissue tethering and to a lesser extent the tethering effect of nerve roots. There were some differences between individuals. The amount of stretching was much less in the thoracic spine than in the neck, and the degree of compression against the anterior wall of the spinal canal varied in dif ferent areas. He reports that the amount of movement in man appears to be more cephalically, and most over the lowest cervical and upper three thoracic vertebrae, i.e. movements are minimal at the CS root and greatest at ca TS approximately, and stretch is greatest between roots C2 and T I . Should thoracic stretch be prevented or modi fied by fixation of dura to disc protrusions, then the full effect of flexion must be borne by such length of cord as is isolated above the area with adhesions.Average amplitudes during the total flexion-extension movement were as follows :Root levelC5 C6 C8 TI T3 T5 TIO
and broader. A slight posterior disc protrusion is evident at all lumbar segments, and the ligamentum flavum becomes slack and its cross-sectional area increases as the dimensions of the intervertebral foramen are reduced. The available space in the canal may be reduced to critical dimensions, this factor being more pronounced if a degree of developmental stenosis is present, together with acquired stenosis in the form of degenerative trespass by thickened sclerous and soft tissue. On flexion, the length ofthe posterior wall of the l umbar canal increases by about 25 per cent, the vertebral canal lengthening by up to 7 cm. 59). 4)4 Meningeal tissue is un able to stretch that much, hence the need for the cord and its coverings to possess a degree of anteroposterior mobility and the roots to move in and out of the foramina to a degree. In the cadaver, full flexion exerts traction on the dural sac, so that the roots are perforce drawn into the inter vertebral foramen for varying distances, i.e. : LI and L2 roots L3 root L4 root between 2-S mm less than 2 mm negligible movement4J4
Two points should be noted:
No. o obserfJaricm f3
Average (mm)3.3 9.0 12.7 6.6 2.3
3 3 3
N.B. Reference should be made to the full data W24 The author observes that any discussion of root direc tion, whether based on radiological, surgical or pathologi cal examination, must at the same time specify the position of the head and neck relative to the trunk.Lumbar region Sagittal and coronal plane movements of the lumbar spine exert broadly similar effects to those in the cervical spine, on the cauda equina, but rotation movements can have little effect since they are much more limited. Breig's ( 1 960) ' " studies of the cadaver indicated that on extension from flexion the lumbar intervertebral canal shortens and the neural contents also become s hortened
1 . Movements imposed upon the cadaver may not have the same mechanical effect on a living patient: a. bending forward from the neutral standing posi tion b. sitting with legs dangling over the plinth edge while one knee is passively extended. c. sitting on a horizontal surface with legs extended and then reaching forward to the toes. 2. The straight-leg-raising test does not induce the same mechanical disturbance of the dura and nerve roots as does lumbar flexion ; one essential difference is that in flexion, during clinical examination, the lumbar spine is bearing weight
(CI)
I f
Left eXL/side-flex/ rot. quadrant still pulls a trace Left ext. /side-flex/ rot. quadrant still pulls a trace Assess 7 daysw
2x
(CI) II
1 8. 1 1 . 74
'No problems'Signs. She's right !
Stop.
In retrospect, this patient is a good example of those who do not mention associated problems unless asked. This diffidence is sometimes due to unawareness that apparently disparate pains may indeed be associated, and at other times because the patient has in the past been sub jected to ridicule or had her reports brushed aside. The author has very frequently observed respected and able clinicians saying to the patient, 07 ru.s noted the successful application ofpassive-movte i ues in treatment of low-back P. in among the normal case-load of a general-hospital. Patientstre .ted with those techniques (Maitland, 1 977)'" were or better in about half the time taken for those treated by more traditional physiotherapy techniques. It is also believed by many that manipulation neces-
PRINCIPLES OF TREATMENT
383
than one treatment session, by orderly and logical method, an the ro ressive familiarisation of oneself with the salient clinical features which guide treatment procedures, and which differ so much fromJ'atient to patient. 0he degenerative changes of spondylosis, osteophytic trespass, fibrosis, acquired stenosis, spinal root irritation, secondary contracture of soft tissue, segmental instability and segmental stiffness (for one reason or another) provide the major bulk of what we might term a family of 'abnor malities of movement', and since only 1 in 1 0 000 subjects progresses to the stage of myelography and major surgical procedures, i.e. 0.0001 per cent,72] conservative treatment is of the utmost importance. Lewit ( 1 972)7J9 observes that when manipulative treatment relieves pain, it has succeeded in doing 50 purely O th the norntaJiliJiK..Q[ disturbed uncJjon. There are many ways of normalising the disturbed function of structures which comprise the moving parts of the body, and even the most superficial acquaintance with the many schools of manipulation makes it plain that while they all have their successes the basic premise, rationale and treatment procedures adopted by each seem to differ considerably. Greenman (1978) observes that:There is a wide and varying range of techniques that now fall under the term manipulation, or spinal manipulotherapy, and if onc picks up various tcxtbooks on the subject, one notes whole diferent f slight movements to various forms of massage, to gross nonspe
I t is plain that differing principles of approach, the con siderable varieties of methods and the many hypotheses about effects leave us with little that is common to all of them. If the technique and effects of simple massage are put to one side, then on further acquaintance, there appear to be only two factors which are common to all man!'pula tive disciplines, namely: (i) skilful and confident hand Itng; em joint movemeru. We might consider these factors as follows :
cific movement using femurs and shoulders and so on, to minute specific kinds of adjusting techniques which put a specific contact on either a transverse or a spinous process and give a very short, sharp thrust. So there is great variation in techniques by people never be made from a single qualified practitioner to the emire is often dismissed on the basis of one technique. field of manipulation. Nevertheless, all of manipulative therapy who claim to be spinal manipulators, and a generalisation can
Haldeman (1978)787 has tabulated some hypotheses, from times past to the present, of the nature of therapeutic effects of manipulative therapy:ThLory AuthorGalen Pare
1. 2. 3. 4. 5. 6. 7. 8. 9.
Restore vertebrae to normal position Straighten the spine Relieve interference with blood flow Relieve nerve compression Relieve irritation of sympathetic chain Mobilise fixated vertebral units Shift a fragment of intervertebral disc Mobilise posterior joints Remove interference with cerebrospinal fluid circulation
(1958)]95 (1958)969 Still (1899)1I7b Palmer (1910)966 Kunert (1965)686 Gillet (1968)408 Cyriax (1975)218 Mennell (1960)8 52De Jarnette Perl
(i) Skilful and confident handling Although adult patients are likely to stoutly reject the idea, most experienced practitioners might agree that those who present with varying degrees of painful damage to their locomotor apparatus, or who are temporarily disabled for their normal work and activity by pain, aTe actually in a state of mourning for their partial loss of physical func tion; many are also needlessly frightened of what the future may hold, in terms of an expected and fearful re striction of their locomotor freedom. Perhaps in a part of their psychic, emotional world they have unconsciously become children again, and in stinctively long for the omnipotent mother to take hold of the injured part, to handle it with loving care, skill and sympathetic interest; and to make them better--one way or another. Emotional maturity, social aspiration and in systems. T tellect notwithstanding, it is very common indeed for people with restricting aches and pains from joints in stinctively to seek out the therapeutic 'handler', whether orthopaedist, physiotherapist, osteopath, chiropractor, masseur, bonesetter or football team trainer,lJ8b C,?nfident, gentle and skilful handlin&J1.y whatever tech nique is a very powerful thereutic weapon. and thera pists who han iL.paticnts with insight and under standing, and examine them attentively with care (or detail,'" have already won half the battle; willy-nilly, they have already been polQllically cast by the arient in the role of 'the sympathetic handler who will make me bette?, and the confident and skilful therapist fulfils the . role, satisfying a deep and unconscious psychological need. Only so far as this powerful psychological need is concerned, the actual clinical method of handling pales into insignificance ; so much so that, even should the therapist not make the patient sign- and symptom-free, the burden of pain may be considerably relieved, and the patient calmed and reassured. U8bPhysical contact through the touch or cit al at in hands..of
(1967)2]7
10. Stretch contracted muscles, causingrelaxation
(1975)986
doctors or physiotherapists is
y patients as a E!!ticular
II. Correct abnormal somatovisceralreflexes
Homewood
12. Remove irritable spinal lesions 13. Stretching or tearing of adhesionsaround the nerve root
14. Reduce distortion of the annulus
(1964)174 Farfan (1973)]26
Chrisman I!t al.
(1963)566 Karr (1976)675
expression ofcare and concern for them.
alectric sensation about their neck and back, in the area at the very prospect ofphYSical contact, of massage, of attention. of the superficial trapezius muscle, or over
any acknowledge an
thelf arms or hands,
While phYSICians now largely express their concern and care by
384
COMMON VERTEBRAL JOINT PROBLEMS
sion of the impulse to help. The amount of physical contact with ati ents par kularly the lonely, the frigtened and the elderly t should never be reduced.)01
deep thought and the contemplation of the outcome of tests. ph sIOtherapIsts still represent the most direct ?"d natural expres
Y
So long as the human animal suffers benign but painful restriction of free bodily movement, so long will there be need for those skilled in therapeutic handling. All the more desirable that the handling should be informed, prudent and of tfie highest academic standard.(ii) Joint movementThe manual treatment of limbs and the spinal column has always maintained its place in official medical practice . . . wi an we are mechanically able to influence certain conditions of the tissues ; a ove alt the mobilj(YJ1fJ . s as ell as the relationship b b ni oint partners. However) we also set in motio" reflex !1IeclS I rfiy italics] and thereby the human hand may influence the regula tion and cont;ol mechanisms of postural and movement systems. Inana;:-rower sense, we mechanically try by manual therapy to restore disturbed jOlrll Jut/cliot/ (my italics] to normal, so far as is possible.4'"
joint to the different things we do in the way of treatment bY/itis sive movement-ofone kind I md another.
techniques. For example, Jones (I 964)'" described ttie technique of spontaneous release by positioningJ in which the patient is passively disposed in the pOSition of reatest ort c o,;,f and held there for some 90 seconds. After that i terval) the patient is very slowly returned to the neutral position. Muscular hypertonus is released and voluntary gu;;ding becomes unnecessary. The technique is applic a e to oth spinaP63 and peripheral joints, and is particu larly useful in treatment of the painful shoulde- r. Although treatment of a single segment is often suf ficient in the very early stages of dysfunction of that segment, where none existed before, the greater majority of joint problems present as a complex of chronic changes. There is no magic in the manipulator'S hand, there is no mystique of manipulation. But there is a centralmY.:; tery, and it lies in the variet 0 res omes o the abnormal f Joints cannot read books, or understand theories about technique; what suits one joint problem will not suit another. We must learn to be humble in the face of this mystery, we must learn to listen to what the abnormal joint istring to tell us-in short, we must learn to assess. b. NEUROPHYSIOLOGICAL EFFECTS In the business of getting the patient better, the technic ally desirable movement, the movement which is logically based on biomechanical concepts, on the orientation and configuration of facet-joint planes, for example, is by no means always the successfully curative movement ,. we can only learn which is the therapeutic movement from the initial responses of the joint, and it is the author's belief that the ultimate understanding of this central mystery can be served, among the study of other factors, by improving our appreciation of the neurophysiological aspect of our work.One essential point is that when applying the principles of mechanics to the prevention and management of back pai , the n other biological factors which are relevant must be taken into account; in particular, the epidemiological, neurophysiological and psychophysical aspects . . . . Pain implies neurophysiological dysfunction, and its relationship to the pathomechanics of lumbar spinal disorders dominates the interpretation of signs and symp toms . . . (Troup, 1979). 1 150b
There is ample evidence that nociceptor activity giving rise to pain also generates extensive reflex effects ; there is similar evidence (vide infra) that the simple passive movement of joints likewise generates reflex effects. It is untrue that treatment by mobilisation and manipu lati be ade uately discussed only on a mechanical cusc-and-cffect relationship; while we continue [0 regard musculoskeletal joint problems as simple mechanical ones, while we conceptualise only like mechanical engineers, our potential for better results will remain re stricted. Millions of as mtomatic individuals are walking about wit hanical joint .QI.oblems. Because of the work of B. D. WykelJS4 1 3,7, 136 1 . I16J and P. Polacek998 we have every reason for progressing to the point where we begin to think like telecommunication engineers-since the most basic acquaintance with spinal joint neurophysiology and recent research findings indi cate that the phenomenon of joint pain and its relief by mechanical techniques involve effects which transcend simple m