DISORDERS OF THE TEMPORO-MANDIBULAR JOINT (TMJ)Dr. Mohamed
ShokryBDS-MSc-PhDOral & Maxillofacial SurgeryFaculty of
Dentistry- Alexandria
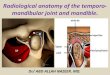
Unique joint, its structure allowing for three different groups
of movements: 1. The up and down, or elevation and depression, of
the jaw.2. The protraction &retraction of the mandible .3. Side
to side motion, or lateral deviation. Bony articulation and
interposed disc The condyle is roughly elliptical in cross section
with the medio-lateral dimension equal to about twice its
antero-posterior width.The articular surfaces are covered with
avascular fibrous tissue.The primary concave temporal articular
surface is limited anteriorly by the convex articular eminence and
posteriorly by the articular lip.Interposed between the osseous
structures is the meniscus (disc).It is composed of avascular,
aneural, fibrous connective tissue.
Disc And Its Attachments:The disc separates the superior and
inferior joint cavities.It is lined with synovial tissues that
produce fluid necessary for lubrication of articular surfaces.The
upper cavity is larger.The disc composed of three regions:-3 mm:
Posterior band.1 mm: Intermediate zone.2 mm: Anterior band.It is
thinnest centrally (1mm) and somewhat heavier along its
periphery.The greatest bulk is at the posterior attachment (the
bilaminar zone)The bilaminar zone consists of two strata of fibers
separated by loose areolar connective tissue Superior strata is
composed mainly of elastic fibersInferior strata is made up mainly
by fibrous tissue.The posterior attachment tissues are highly
innervated by the auriculo-temporal nerve.The superior surface of
the disc is concavo-convex, whereas the undersurface is concave
antero-posteriorly.The meniscus (disc) is attached tightly to the
medial and lateral poles of the condyle.Posteriorly the attachment
is elastic to allow it to translate forward with the
condyleAnteriorly, the disc is continuous with the capsule and the
lateral pterygoid fascia.
Capsule:Is a ligamentous structureIt extends from the temporal
portion of glenoid fossa , fuses with the margins of the disc,
reach the neck of condyle to invest the entire joint.It is
reinforced laterally by the TM ligament. The temporomandibular
ligament:It is composed of horizontal oblique and deep horizontal
connective tissue fibers.It reinforces the capsule laterally.It
acts to limit anterior and posterior condylar movements.It is
designed to prevent the mandible from opening too far on a pure
hinge rotation at the uppermost position.As the jaw opens on a pure
hinge movement, the floor of the mouth is directed back into the
airway.To prevent this the ligament reach its full length at about
15 to 20mm of the jaw opening.At this point, the site of attachment
of the TML to condyle becomes a pivot that initiate forward
translation of the rotating condyle.This requires the mandible to
move forward away from any airway obstruction during full
opening.The temporomandibular ligament: Normal function The condyle
disc interface of the joint is the site of primary hinge
movement.This is made possible by fixation of the disc to condyle
by the discal ligaments.Contraction of the inferior lateral
pterygoid muscle occurs during opening movement and result in
anterior condylar translation.During closure the inferior lateral
pterygoid releases contraction to allow the condyle to be pulled
back by the elevator muscles.During closure the superior lateral
pterygoid activate its contraction to hold the disc forward, to
oppose the pull of elastic fibers.The superior lateral pterygoid
muscle is essentially passive; contracting during forced closure,
or in the presence of occlusal interferences.Centric relation:The
relationship of the mandible to the maxilla when the properly
aligned condyle-disc assembly is in the most superior position
against the eminence, irrespective of tooth position or vertical
dimension.Centric Occlusion:The relationship of the mandible to
maxilla when the teeth are in maximum occlusal contact,
irrespective of position or alignment of condyle disc-
assembly.
The Temporomandibular Joint DisordersThe ADA classification of
TMJ disorders (developed by Weldon Bell)Masticatory muscle
disorders :1. Protective muscle splinting.2. Myofacial pain
dysfunction syndrome.3. Muscle hyper activity or spasm.4. Myositis
(muscle inflammation)Intra-articular problems: (internal
derangement):1. Anterior disc displacement with reduction
(clicking).2. Anterior disc displacement without reduction (closed
lock)
Degenerative joint disease Arthrosis. Arthritis.
Inflammatory joint disorders: Rheumatoid arthritisInfectious
arthritis.Metabolic arthritis.
Functional disorders:Dislocation & subluxation.TMJ
Ankylosis.
DIAGNOSIS OF TMJ DISORDERSDiagnosis of TMJ disease or
dysfunction depends upon thorough history and clinical examination,
plus radiographic imaging. TMJ disease / dysfunction are intimately
related to occlusion.History Taking History of the present
complaint (onset & course) is taken .Ascertain the effect of
function on the symptoms, its relation to daytime and stresses. The
general past history including medical, surgical, psychological,
occupational, social and family background.
Physical examination Examination of the joint itself.The range
of opening anteriorly is measured. Opening, closing, protrusive,
and lateral movements are evaluated. Direct examination of the
condyles both in the periauricular area and via external auditory
meatus (endaural).Sounds whether audible to the examiner or heard
by the stethoscope.Palpation of the muscles of mastication for
areas of tenderness, rigidity, or masses.Examination of dentition
and other hard and soft tissues of oral cavity.Radiographic
diagnosisPlain radiography; orthopantomogram (Panoramic x-ray),
oblique lateral transcranial views, and transpharyngeal views in
the open and closed positions.Tomography; Tomograms offer the best
results of plain radiography because of the elimination of
superimposition found in conventional radiographs.Tomographic
section of TMJ are done with mouth closed and opened.Arthrography;
Arthrograms, where radiographs are taken after a radio-opaque dye
has been injected into the synovial spaces, can demonstrate the
position of soft tissues within a joint by negative image. It has
the disadvantage of being invasive.Computed Tomography (CT Scan);
It is a non-invasive technique helpful in diagnosis of
abnormalities in hard / soft tissue components of the joint
Magnetic resonance imaging (MRI); it is an imaging procedure
with vast clinical potential, as it offers detailed views of
internal anatomy without ionizing radiation or invasion. More
helpful in diagnosis of soft tissue ( disk ) diseases. Arthroscopy;
it allows direct visualization .TMJ is a difficult joint for
arthroscopy; not only being small in size, but it has two
compartments with the line of entry of the instrument from the
lateral side shielded by the tip of the root of zygoma.
Radiographic diagnosis Ultrasound (US); the wavelengths available
for diagnostic ultrasound do not permit visualization of soft
tissues in close apposition to bone . Ultrasound in its present
form has no value.
Laboratory examination Laboratory examination; such as complete
blood cell count, serum calcium, phosphorous, and alkaline
phosphatase. Also serum uric acid, serum rheumatoid factor RF. The
ADA classification of TMJ disorders (developed by Weldon
Bell)Masticatory muscle disorders :1. Protective muscle
splinting.2. Myofascial pain dysfunction syndrome.3. Muscle hyper
activity or spasm.4. Myositis (muscle inflammation)
Protective muscle splintingThe lateral pterygoid muscles are
capable of holding the condyles in an advanced position during
protrusive function.The mechanism that forces this prolonged
contraction of the lateral pterygoid muscles is sensitive
protective reflex system that guards the teeth and their supporting
structures against excessive stress. This proprioceptive receptors
are designed to program the lateral pterygoid muscle to position
the jaw so that the elevator muscles can close directly into
maximum occlusal contact. This unique relationship between the
lateral pterygoid muscles and the proprioceptive periodontal
receptors is so definite that is even override the normal tendency
of the muscle to rest when it becomes fatigued. The muscles cannot
relax the protective bracing contraction as long as the occlusal
interference is present.The pattern of deviation is reinforced
every time the contact is made, and it is retained in the brains
memory bank (muscle engram) so that muscular closure into the
deviated jaw relationship becomes automatic One important fact of
the proprio-ceptive memory, however, is that it fades rapidly if
continual reinforcement of the pattern ceases.Elimination of
interfering contacts permits an almost immediate return to normal
muscle function The fatigue or spasm that occur from prolonged
hyperactivity often produces pain in the muscle. Sensory nerve
endings in the muscles are highly sensitive to lactic acid buildup
and also to ischemia. When the nerve endings are stimulated, they
report such stimulation as pain. Ischemia can occur in the muscle
because of the tight spastic contraction around its own blood
supply.Occlusal splints can perform one basic function. They can
prevent the existing occlusion from controlling the jaw to jaw
relationship at maximum intercuspation by providing a smooth
surface, which gives a chance for correcting the position of the
condyle-disk assemblies and relief of any spasm in the masticatory
muscles.Types of occlusal splints:Soft Occlusal Splint Hard
Occlusal SplintPermissive splint: Designed to unlock the occlusion
to remove the deviating tooth inclines from contact.Directive
splint: Designed to position the mandible in a specific relation to
maxilla.
MYOFASCIAL PAIN DYSFUNCTION SYNDROMEIt is not a disease entity
rather than a set of etiologically non-related disorders. Normal
TMJ / Muscle pain.This explains why this syndrome is defined on the
basis of the symptoms rather than on the basis or the principle
etiologic factor (cause and effect). MPDS :Signs and
symptoms:PainTenderness of the masticatory
muscles.Clicking.Limitation of mandibular movements.Absence of
clinical or radiographic evidence of organic changes in the
TMJ.Lack of tenderness in TMJ on endaural examination.
The Trigger points are signature mark of MPDS diagnosis. By spot
palpation of all muscles suspected pain is present.Painful limits
of the range of motion of opening. Etiology: Occlusal Disharmony
Psychological Disturbance TREATMENT: (it's multidisciplinary)1-
Pharmacological line of treatment : - NSAIDS (aspirin, ibuprofen) -
Tricyclic anti-depressant drugs in low doses - Potent muscles
relaxant (diazepam, skelaxin )2- Injection therapy : into trigger
points:a) local analgesic (bupivacaine, lidocaine )b) Skeletal
muscle relaxant ( botulinum toxin BO-TOX )as it cuts innervation
into muscles. 3- Role of Dentist : Breaking up bad habits (bruxism,
clinching, grinding). Treatment of occlusal disharmony / occlusal
adjustment.Occlusal splints : Occlusal splints can perform one
basic function. They can prevent the existing occlusion from
controlling the jaw to jaw relationship at maximum intercuspation
by providing a smooth surface, which gives a chance for correcting
the position of the condyle-disk assemblies and relief of any spasm
in the masticatory muscles.
Types of occlusal splints:1. Soft.2. Hard3. Permissive: Designed
to unlock the occlusion to remove the deviating tooth inclines from
contact.4. Directive: Designed to position the mandible in a
specific relation to maxilla.
4- Improvement of nutrition: - Soft diet - Increase of intake of
vitamins 5- Psychological line of treatment : The role of
psychiatric specialist will takes place in elimination of
stress.
Intra-articular problems: (internal derangement):1. Anterior
disc displacement with reduction (clicking).2. Anterior disc
displacement without reduction (closed lock)Internal
derangementInternal derangement of the TMJ can be defined as a
mal-relation of the meniscus to the condylar head and articular
eminence.It is categorized as:1. Anterior displacement of the disc
with reduction (reciprocal clicking of the joint)2. Anterior
displacement of the disc without reduction (locked joint). Anterior
disc displacement(With reduction)If the normally secure attachment
of the meniscus to the lateral condylar pole is slack or
detached.Or if the bilaminar zone has been destroyed or degenerated
from trauma or joint disease.As the interincisal opening increases;
a spontaneous reduction of the anteriorly displaced disc occurs
producing the characteristic click. The origin of the joint click
is related to the passage of the condyle over the thick posterior
meniscal band. On closure, a subsequent resumption of anterior
meniscal displacement occurs, a second click is noted (reciprocal
clicking). Anterior disc displacementwithout reduction(closed
lock)Closed lock is the result of unreduced, persistent anterior
displacement of the disc.When the posterior band of the deformed
disc is trapped anterior to the condyle, it forms a mechanical
barrier to normal condylar translation. Interincisal opening is
seldom greater than 25 mm.Translation is absent.Clicking phenomenon
is lost. The condition may progress to perforation of the disc
accompanied by osteoarthrosis of the condyle and articular
eminence.MRI done for diagnosis.Closed lock.No translation.No
clicking.Deformed disc.Painful joint.
Acute closed lockIt is the result of trauma in which the condyle
is driven posteriorly with subsequent injury to the posterior
attachment. The resultant pain/discomfort may be severe, and the
condition is sometimes identified as discitis. It is an
inflammation of the discal attachments rather than the relatively
avascular/aneural disc itself.
Treatment Of Internal Derangement Of TMJConservative
treatmentOcclusal therapy: This line of treatment consists of
occlusal splints, occlusal equilibration (selective grinding of
teeth) and dental reconstruction.A full occlusal splint harmonized
to the most comfortable joint position may produce acceptable
results. Physiotherapy !!!.Psychotherapy !!!.
surgical treatmentHigh condylar shave.Eminectomy.Capsular
rearrangement.Menisectomy.Subcondylar osteotomy.Meniscoplasty;
transaction and plication of posterior attachment.Recently
arthrocentesis.ArthrocentesisConsists of anesthezing the affected
TMJ with local anaesthetic followed by flushing the joint with a
sterile solution such as Lactate ringers solution anti-inflammatory
steroids.Used to lubricate the joint surfaces and reduce
inflammation.
Degenerative joint diseaseArthrosis. Arthritis.Inflammatory
joint disorders:Rheumatoid arthritisInfectious arthritis.Metabolic
arthritis.Degenerative (osteoarthritis).Traumatic.It is an
inflammatory systemic disease that produces destructive changes, in
more than a single joint. Clinically, there is pain, joint noise,
and limitation of motion.Obvious distortion of occlusion may be
seen Rheumatoid arthritisIn cases of juvenile rheumatoid arthritis
(JRA) there is such an extensive damage to the condyle that the
growth of the jaw may be seriously impaired by the development of
ankylosis. Diagnosis is established by both laboratory and
radiographic studiesA positive rheumatoid factor RF, particularly
in the presence of multiple joint involvement is fairly decisive in
establishing the diagnosis. The condyles are eroded, and flattened.
There is narrowing of the joint space . Arthritis urica (Gout)Is a
metabolic disease of unknown etiology.The joint tissue may be
inflamed owing to deposition of micro crystals of sodium urate.The
acute onset is very characteristic.The affected joint is reddened,
warm,swollen, and very tender.The pt. Feels ill and
fever.Degenerative arthritis(osteoarthritis)It can occur as the
result of prolonged functional abuse (closed lock). Diagnosis of
Osteoarthritis is made on the basis of clinical & radiographic
evidences Sclerosis of the interposed deformed discFacet on
antero-superior surface of condyle with loss of corex.Sclerosis of
cortex at summit and inferior surface of condyle.Cyst like
destruction posteriorlyFlattened eminenceSmall osteophyte on
superior surface of the condyle.Sclerosing of the condyle.The
intermediate zone and posterior band of the TMJ disc are ill
defined.Infectious arthritisBacterial or fungal disease of the
joint.It may be due to local extension of infections from the
middle ear, mastoid process, parotid gland and mandible.
Eventually, fibrous or even bony ankylosis can occur.Traumatic
arthritisIt the result of acute direct trauma and not micro-trauma
caused by repeated dental function and mechanical stress.
Hemarthrosis or traumatic svnovitis may be the major direct effects
of trauma to the joints. Dislocation and subluxationDislocation
i.e., luxation, is the displacement of condylar head completely out
of glenoid fossa anterior & superior to the summit of articular
eminence. It occurs when capsule (collateral ligaments) and
temporomandibular ligament are compromised. it cannot be reduced by
the patient. It may assume a chronic, recurrent form in which
patients suffer numerous episodes with resultant abnormal laxity of
the supporting capsule and ligaments (chronic subluxation). Reduced
by the patient. Etiology: Most dislocations occur spontaneously on
opening the mouth widely for yawning, dental work, during
seizure.Trauma may also produce dislocation.Clinical
findingsUncomfortable but not severely painful.Inability to close
the mouth.Dislocations may be unilateral or bilateralPrognathic
appearance to jaw when both are dislocated.Deviation of the
mandible to the opposite side in unilateral dislocation. Reduction
of TMJ dislocationReduction occurs through downward pressure with
the thumbs on the external oblique ridges, and upward pressure with
the fingers.Treatment of dislocation1- Eminectomy
2- Dautery operation Preauricular incision. The anterior part of
the eminence which is attached to the zygomatic arch is
exposed.This anterior portion of the eminence is
down-fractured.Because of the increase in eminence height, the
condyle is unable to dislocate. Other methods of eminence
augmentation have been described, for example bone graft
augmentation.
TMJ ankylosisAnkylosis is a chronic hypomobility or immobility
of movable articulation. It is considered as one of the most common
sequelae following infection or trauma. TMJ ankylosisIt has been
classified into:*Unilateral or bilateral*True (intra-articular) *
False (extra-articular).*Fibrous or bony.*Partial or complete.
CLINICAL FEATURES Inability to open the jaws. In unilateral
ankylosis, the lower jaws shifts towards the affected side on
opening of the mouth. In severe cases, there is complete
immobilization. Facial deformity (Bird Face). Other bones and
joints deformities may be associated.TREATMENT:1- Condylectomy
Pre-auricular incision. Horizontal cut carried is out at the level
of the condylar neck The head (condyle) should be separated from
the superior attachment3- Gap Arthroplasty.2- TMJ Interpositional
Arthroplasty : Interpositional arthroplasty using buccal pad of
fat4- Total Joint Replacement.
9