There are several interchangeable terms that have the same meaning. Terms change over time. For example, the term ‘mental deficiency’ (1940-1975) was replaced by ‘mental retardation’ (1975-2006), which in turn has been replaced by ‘intellectual disability’ (2006-present). This term is now being replaced by ‘intellectual and developmental disability’ (IDD) (2010-present). The terms ‘dual diagnosis,’ ‘dual disability,’ ‘co-occurring MI-ID,’ and ‘co-existing disorders’ are interchangeable terms and are all accepted in the professional community.
HISTORICAL SYSTEM SEPARATION: MH---------------------------------------IDD • Medical model • Episodic treatment • Strong individual rights • Embraces use of
WHO ARE THESE INDIVIDUALS? • Capable of significant skill development
• More like us than not.
• Experience the full range of emotions.
• Most medicated persons in society.
(Aman & Singh, 1998)
INCIDENCE AND PREVALENCE: ADULTS • Persons with ID/D are 3-4x more susceptible to psychiatric
disorders as per DM-ID and DSM 5; • Persons with I/DD can display a wide range of psychopathology; • Capable of significant skill development • Persons with ID/D receive less attention in the health care
system; • Minority cultures experience poorer health and more difficulty
with access and funding. • Most medicated persons in society.
(Aman & Singh, 1998)
Presenter
Presentation Notes
Compared with other populations, adults, adolescents, and children with MR experience poorer health and more difficulty in finding, getting to, and paying for appropriate health care. These challenges are even more daunting for people with MR from minority communities with many cultures and languages and whose culture and primary language may not be reflected in available health services. As with many other disabling conditions, the multiple disorders associated with MR are found disproportionately among low-income communities that experience social and economic disparities when they seek health care. Mental retardation compounds these disparities because many health care providers and institutional sources of care avoid patients with this condition. Without direct clinical experience, health care providers may feel incapable of providing adequate care. They may not value people with MR and their potential contributions to their own health and to their communities. Dykens “ a range of 10 to 70% indicates that there is limited research that helps us understand the higher risk of psychopathology for children with ID
• Communication • Home living • Community use • Health & safety • Leisure
• Self-care • Social skills • Self-direction • Functional academics • Work
AAIDD DEFINITION
IDD manifests before age 18
AAIDD DEFINITION • Substantial limitations in present functioning • Significantly sub-average intellectual functioning, existing concurrently with: • Related limitations in 2 or more of the applicable adaptive skill areas
Presenter
Presentation Notes
Fact Sheet: �Affects 1-3% population—Many causes but specific reason known in 25% of cases Four Assumptions Essential �to the Application of the Definition The following four assumptions must be considered when applying the definition. Valid assessment considers cultural and linguistic diversity, as well as differences in communications and behavioral factors. The existence of limitations in adaptive skills occurs within the context of community environments typical of the individual's age peers and is indexed to the person's individualized needs for supports. Specific adaptive limitations often co-exist with strengths in other adaptive skills or other personal capabilities. With appropriate supports over a sustained period, the life functioning of the person with mental retardation will generally improve.�
PROBLEM WITH IDD DEFINITION • Not a unifying concept—more correctly stated as intellectual/developmental disabilities • Not clinically helpful
• Must be diagnosed before age 18
• High level of medical co-morbidity
• IDD has >1300 causes
• 2 standard deviations from the norm
• Programmatic, social, legal, practical implications of IDD diagnosis
Presenter
Presentation Notes
During the Kennedy administration, MR was defined as one standard deviation from the norm. There were personal interestes in MR services. During the Nixon administration , it was raised to 2 standard deviations from the norm and with a pen stroke, thousands of people were cured of mental retardation
DSM 5 INTELLECTUAL DISABILITY • Onset during the developmental period that includes both intellectual and
adaptive functioning deficits in conceptual, social, and practical domains. Following 3 criteria must be met:
A. Deficits in intellectual functioning such as reasoning, problem solving , planning. Abstract thinking, academic learning and learning from experience, confirmed by both clinical assessment and individualized standardized testing;
B. Deficits in adaptive functioning that result in failure to meet developmental and sociocultural standards for personal independence and social responsibility. Without ongoing support, the adaptive deficits limit functioning in one or more activities of daily life, such as communication, social participation and independent living, across multiple environments such as home, school, work and community.
C. Onset of intellectual and adaptive deficits during the developmental period.
Specifiers of Mild, Moderate, Severe, Profound
Presenter
Presentation Notes
The term ID is equivalent to ICD 11 diagnosis of IDD. The federal statute in the US –Rosa’s law replaces the term mental retardation with ID signed by Obama 2010 The specifiers are based on adaptive functioning and not IQ scores because adaptive functioning determines the level of supports required.
• Communication Disorders • 315.39 (F80.9) Language Disorder • 315.39 (F80.0)Speech Sound Disorder • 315.35 (F80.81)Childhood onset Fluency Disorder (stuttering) • 315.39 (F80.89) Social Communication Disorder • 307.9 (F80.9) Unspecified Communication Disorder
Presenter
Presentation Notes
Mental Retardation has many different etiologies and may be seen as a final common pathway of various pathological processes that affect the functioning of the central nervous system. General intellectual functioning is defined by the intelligence quotient (IQ or IQ- equivalent) obtained by assessment with one or more of the standardized, individually administered intelligence tests (e.g., Wechsler Intelligence Scales for Children, 3rd Edition; Stanford-Binet, 4th Edition; Kaufman Assessment Battery for Children). Significantly subaverage intellectual functioning is defined as an IQ of about 70 or below(approximately 2 standard deviations below the mean). It should be noted that there is measurement error of approximately 5 points in assessing IQ, although this may vary from instrument to instrument (e.g., a Wechsler IQ of 70 is considered to represent a range of 65–75). Thus, it is possible to diagnose Mental Retardation in individuals with IQs between 70 and 75 who exhibit significant deficits in adaptive behavior. Conversely, Mental Retardation would not be diagnosed in an individual with an IQ lower than 70 if there are no significant deficits or impairments in adaptive functioning. The choice of testing instruments and interpretation of results should take into account factors that may limit test performance (e.g., the individual's sociocultural background, native language,and associated communicative, motor, and sensory handicaps). When there is significant scatter in the subtest scores, the profile of strengths and weaknesses, rather than the mathematically derived full-scale IQ, will more accurately reflect the person's learning abilities. When there is a marked discrepancy across verbal and performance scores, averaging to obtain a full-scale IQ score can be misleading.
DSM 5 NEURODEVELOPMENTAL DISORDERS
A. Autism Spectrum Disorder • Persistent deficits in social communication and social interaction across
multiple contexts • Restricted, repetitive patterns of behavior, interests, or activities • Symptoms are present in early developmental period • Symptoms must cause clinically significant impairment in social,
occupational or other important area of functioning • Disturbances not better explained by ID or global developmental delay
Presenter
Presentation Notes
Mental Retardation has many different etiologies and may be seen as a final common pathway of various pathological processes that affect the functioning of the central nervous system. General intellectual functioning is defined by the intelligence quotient (IQ or IQ- equivalent) obtained by assessment with one or more of the standardized, individually administered intelligence tests (e.g., Wechsler Intelligence Scales for Children, 3rd Edition; Stanford-Binet, 4th Edition; Kaufman Assessment Battery for Children). Significantly subaverage intellectual functioning is defined as an IQ of about 70 or below(approximately 2 standard deviations below the mean). It should be noted that there is measurement error of approximately 5 points in assessing IQ, although this may vary from instrument to instrument (e.g., a Wechsler IQ of 70 is considered to represent a range of 65–75). Thus, it is possible to diagnose Mental Retardation in individuals with IQs between 70 and 75 who exhibit significant deficits in adaptive behavior. Conversely, Mental Retardation would not be diagnosed in an individual with an IQ lower than 70 if there are no significant deficits or impairments in adaptive functioning. The choice of testing instruments and interpretation of results should take into account factors that may limit test performance (e.g., the individual's sociocultural background, native language,and associated communicative, motor, and sensory handicaps). When there is significant scatter in the subtest scores, the profile of strengths and weaknesses, rather than the mathematically derived full-scale IQ, will more accurately reflect the person's learning abilities. When there is a marked discrepancy across verbal and performance scores, averaging to obtain a full-scale IQ score can be misleading.
CONCEPT OF DUAL DIAGNOSIS FLETCHER 2005
• Co-existence of two disabilities: Intellectual Disability and Mental Illness
• Both Intellectual Disability and Mental Health disorders should be assessed
and diagnosed
• All needed treatments and supports should be available, effective and accessible
• Diagnostic Overshadowing must be considered. • (Reiss, Levitan & Szyko,1982)
Presenter
Presentation Notes
It is only within the past 35 years or so that professionals have recognized that it is possible for individuals to have both intellectual disability and mental illness. Trained professionals are needed to conduct mental health assessment in persons with ID. Services available for people with MI should also be available for people who have ID/MI. Availability is not enough; we need staff who have a level of competency in dual diagnosis. The services need to be conducted by professionals who are trained in dual diagnosis. This helps to achieve effectiveness.
IDD CAUSES • Genetic abnormalities ( >50%)
• 1995 285 causes of I/DD • 2015 1300+ Genetic Causes of I/DD
Infections (present at birth or occurring after birth) Congenital CMV, Congenital rubella, Congenital toxoplasmosis, Encephalitis, HIV infection, Listeriosis, Meningitis Chromosomal abnormalities Chromosome deletions (such as cri du chat syndrome) Chromosomal translocations (a gene is located in an unusual spot on a chromosome, or located on a different chromosome than usual) Defects in the chromosome or chromosomal inheritance (such as fragile X syndrome, Angelman syndrome, Prader-Willi syndrome), Errors of chromosome numbers (such as Down syndrome) Environmental Deprivation syndrome Genetic abnormalities and inherited metabolic disorders Adrenoleukodystrophy, Galactosemia, Hunter syndrome, Hurler syndrome, Lesch-Nyhan syndrome, Phenylketonuria, Rett syndrome, Sanfilippo syndrome, Tay-Sachs disease, Tuberous sclerosis Metabolic Congenital hypothyroid, Hypoglycemia (poorly regulated diabetes) Reye syndrome, Hyperbilirubinemia (very high bilirubin levels in babies) Nutritional --Malnutrition Toxic Intrauterine exposure to alcohol, cocaine, amphetamines, and other drugs Lead poisoning, Methylmercury poisoning Trauma (before and after birth) Intracranial hemorrhage before or after birth, Lack of oxygen to the brain before, during, or after birth Severe head injury Unexplained (this largest category is for unexplained occurrences of intellectual disability)
GENOTYPES AND PHENOTYPES
• Genotype: genetic constitution • Phenotype: behavioral manifestation and characteristics associated with
genetic disorders • Demonstrate the interaction between genes, brain structure and
organization and complex behaviors
Presenter
Presentation Notes
Monozygotic twins separated at birth demonstrate that genes are responsbile for 50% of personality traits
GENOTYPES AND PHENOTYPES • Behavioral phenotypes
• Are not set in stone • Look at syndromes rather than set diagnoses • Behavioral manifestations arise from the interaction of genes
and environment • Present a wide range of symptoms • Used as clues not as expectations
Presenter
Presentation Notes
A recent approach to studying the "mental retardation syndromes" (Accardo and Capute, 1998), which bears directly on people with a dual diagnosis, involves characterizing the behavioral phenotype of a specific genetic disorder (O'Brien and Yule, 1995; Finegan, 1998; Simonoff, Bolton, and Rutter, 1998). Advances in behavioral phenotype research occur in two ways: first by studying individuals with known genetic disorders such as Fragile X syndrome and developing syndrome characterizations, secondly by looking for a genetic marker in people with behavioral commonalities. Rett syndrome is a disorder which has long been thought to be genetically based, however, the genetic marker has not yet been found. The behavioral phenotype and developmental course of Rett syndrome has however been well documented (Hagberg and Witt-Engerstrom, 1986). As Rett syndrome has an identifiable phenotype without a genetic marker it remains in the DSM IV as an acceptable psychiatric diagnosis. When the genetic marker is found it will most likely be removed from the DSM IV, as other genetically based syndromes such as Down syndrome or Fragile X syndrome are not included. Once a diagnosis is made, the most critical test of its clinical utility is whether or not it will drive treatment. An etiologically based diagnosis can and should drive treatment. In many cases a biologically based syndromic diagnosis can serve as a unifying concept among those individuals designing individual supports for a person. It is much easier to develop a unified support system when professionals, the family and the individual are operating from a common unifying concept such as an etiological diagnosis. Aside from aiding in generating functional behavioral and psychiatric diagnoses, the family and individual support available at little or no cost through the many syndrome related support groups is good reason to pursue etiological diagnoses. Mental retardation, functional behavioral disorders, and mental illness are associated with hundreds of genetic disorders. The psychiatric, cognitive and behavioral profiles of these disorders are being better defined on a daily basis. As clinicians working to generate testable hypotheses in the areas of functional behavioral disorders and psychopathology it behooves us to become familiar with the characterizations of some of the more common syndromes.
ETIOLOGY VERSUS DESCRIPTION (DSM 5, AAIDD)
• Anticipates medical needs
• Allows insight • Vulnerabilities
• Behaviors
• Learning Styles
• Life span approach
Presenter
Presentation Notes
Ability to Study Vulnerabilities Ability to Study Strengths Predict medical predispositions Ability to Adapt to Learning Styles
GENETIC SYNDROMES
• Down Syndrome • Fragile X Syndrome • Smith-Magenis Syndrome • Prader-Willi Syndrome • Smith-Lemli-Optiz Syndrome • Williams Syndrome • Lesch-Nyhan Syndrome • Angelman Syndrome
Presenter
Presentation Notes
High visual memory Sequential processing intact Expressive language Articulation and grammar Hearing impairment and oral structure Prevalence of medical problems Language reception excellent (20 years) Good at breaking down tasks High social ability
GENETIC SYNDROMES
• Down Syndrome • Most Common & Well Known
• Fragile X Syndrome
• Most Inherited Form of ID
• Smith-Magenis Syndrome • Believed Rare ?
Presenter
Presentation Notes
Genetic Syndromes Down Syndrome Most Common & Well Known Fragile X Syndrome Most Inherited Form of ID Smith-Magenis Syndrome Believed Rare
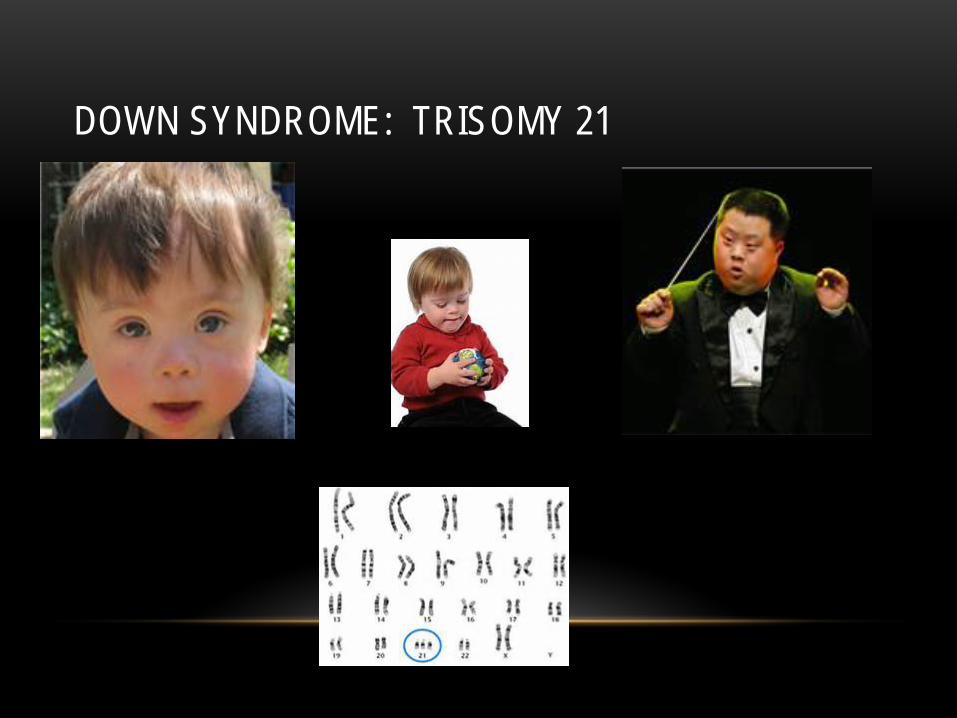
DOWN SYNDROME: TRISOMY 21
DOWN SYNDROME • 1/800 births worldwide, 1/1600 US
• Trisomy 21, extra chromosome 21
• 92% Trisomy 21
• 3%-5% Mosaic (Subsequent to first cell division)
• 3%-5% Robertsonian Translocation 21st on 14th (Transmittable)
• Prevalence
• Significant Increase > 45 years old (1:32)
• 80% Moms < 35 years old.
Presenter
Presentation Notes
Down Syndrome 1/800 births worldwide, 1/1600 US Trisomy 21, extra chromosome 21 92% Trisomy 21 3%-5% Mosaic (Subsequent to first cell diivision) 3%-5% Robertsonian Translocation 21st on 14th (Transmittable) Prevalence Significant Increase > 45 years old (1:32) 80% Moms < 35 years old.
Broad short hands, short fingers, with single palm crease
Short stature
Presenter
Presentation Notes
Down Syndrome – Physical Characteristics
• Down Syndrome • Noncompliance, stubbornness, inattention, overactivity, argumentative, withdrawn (depression and dementia among adults)
MALADAPTIVE VULNERABILITIES WITH GENETIC SYNDROMES
Presenter
Presentation Notes
TRISOMY 21-Down Syndrome Major malformations Cardiac GI Minor malformations Facial, skin, etc Developmental pattern MR Learning pattern TRISOMY 21 ADHD Autism ?~8% Developmental Medicine and Child Neurology November 2001 Alzheimer Dementia 16-50% depending on criteria for diagnosis May require different programs than typical for MR
DOWN SYNDROME: VULNERABILITIES
• Expressive Language
• Articulation and Grammar
• Hearing Impairment and Oral Structure
• Prevalence of Medical Problems
• Accelerated Aging Process
Presenter
Presentation Notes
Down Syndrome – Vulnerabilities Expressive Language Articulation and Grammar Hearing Impairment and Oral Structure Prevalence of Medical Problems Accelerated Aging Process
DOWN SYNDROME: STRENGTHS
High Visual Memory
Sequential Processing Intact
Language reception excellent
Good at Breaking down tasks
High sociability
Increased Life Expectancy 75+
Presenter
Presentation Notes
High Visual Memory Sequential Processing Intact Language reception excellent (20 years) Good at Breaking down tasks High sociability Increased Life Expectancy 75+
• Fragile X
• Social anxiety, shyness, gaze
aversion, perseveration, autism/PDD, inattention, hyperactivity, sadness or depression (primarily females)
MALADAPTIVE VULNERABILITIES WITH CERTAIN GENETIC SYNDROMES DYKENS 2000
Presenter
Presentation Notes
X-linked (carriers: F-1:259; M-1:800) 1:2000 males; 1:4000 females FMR1 gene on X chromosome (Xq27.3) Normal 0 to 25 repeats Premutation-25 to 200 repeats Mutation >200 repeats Diagnosis: DNA testing for mutation via PCR FRAGILE X SYNDROME Facial features Long face Large, protuberant ears Hyperextensible joints especially fingers Flat feet Large size Macroorchidism Cognition Males most with MR Females 1/3 to ½ with MR, others with LD ADHD (M-80-90%) Anxiety Disorders Mood disorders e.g. bipolar disorder/depression Autism (15-33%)/Autistic characteristics Handflapping/PICA Poor social judgement/interaction Sound/light/texture sensitivity Poor eye contact/perseverative speech
Presenter
Presentation Notes
Most common hereditary cause of developmental disability in all populations Occurs in males and females although males are more commonly affected Diagnosed through DNA blood testing Majority of those affected are undiagnosed 1 in 3,600 males 1 in 100 with ID, 1 in 36 ID males Hyperarousal—overreaction to sensory stimuli Enhanced cortisol release after stressors Delayed physiological recovery after hyperarousal Gaze aversion—distinctive form of poor eye contact—actively turning away versus looking through you Majority of males with fragile X exhibit gaze aversion—forced eye contact triggers abnormal cortisol response When eye contact goals are de-emphasized, eye contact often improves Many of males with fragile X meet criteria for an ASD and therefore are candidates for ABA ABA therapy needs to take into account gaze aversion, hyperarousal and anxiety issues therefore forced eye contact, discrete trail teaching and desensitization may be counterproductive
Anxiety—hyperarousal Early signs—self injury(hand wrist biting), mouthing objects, hand flapping Escalate to task refusal, leaving the area, verbal aggression with imitated phrases Triggers—forced eye contact, personal space issues, tactile defensiveness, emotional tone of peers/staff, changes in routine, auditory stimuli Other contributors—auditory processing deficits, delayed emotional processing, hypersensitivity to negative correction, poor concept of time A” Cure” for Fragile X targeted pharmaceutical treatments are undergoing human clinical trials—target the underlying biochemical pathway affected by the fragile X gene mutation Families diagnosed with Fragile X syndrome will be able to benefit from this medical breakthrough
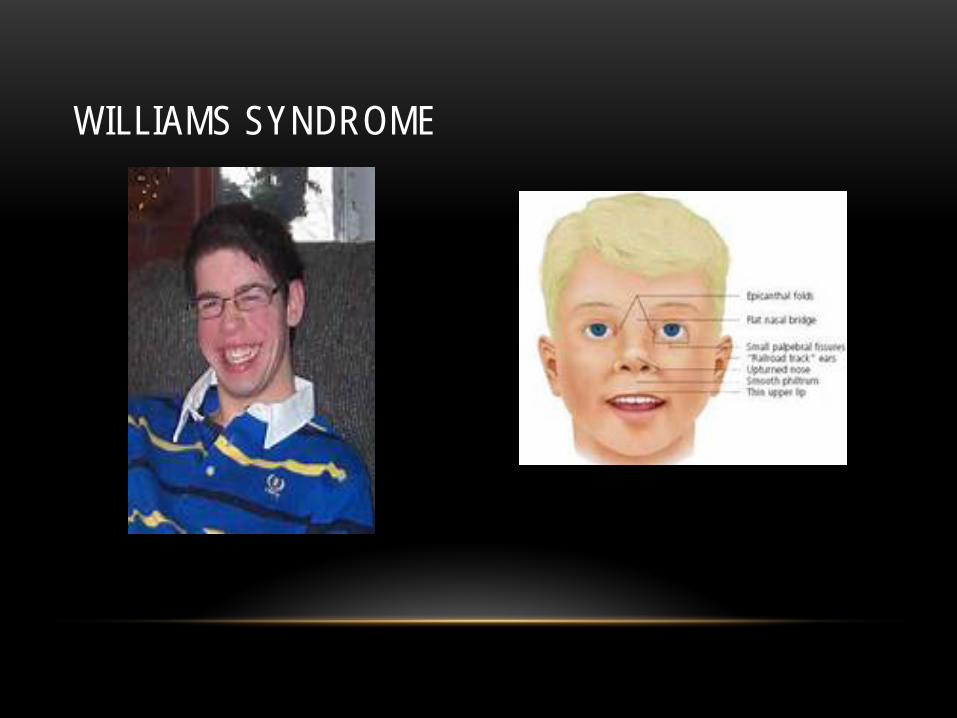
• Williams Syndrome
• Anxiety, fears, phobias,
inattention, hyperactivity, social disinhibition, overly friendly, indiscriminate relating, sensitive
MALADAPTIVE VULNERABILITIES WITH CERTAIN GENETIC SYNDROMES DYKENS 2000
Presenter
Presentation Notes
Highly characteristic Facial abnormalities, Cardiac abnormalities, Metabolic problems- high blood calcium levels Contiguous gene sequence , Deletion chromosome 7 1:20,000 births general pop, 1 in 100 with ID Associated DD, Mild to moderate MR Appealing face & engaging smile, auditory processing strength; strength in musical ability and facial recognition Short attention span/ADHD Cocktail party chatter—well developed verbal skills, no fear of strangers Obsessive compulsive characteristics e.g. topic of conversation Unusually sensitive to noise (hyperacusis), fear of heights Difficulty building friendships, poor visual motor integration, medically fragile Nail-biting, skin picking behaviors Anxiety/Anxiety Disorders Autism/Autistic features
MALADAPTIVE VULNERABILITIES WITH GENETIC SYNDROMES DYKENS 2000
Presenter
Presentation Notes
General pop 1 in 15,000 with ID, 1 in 100 Hypotonia in utero (decreased fetal movement) infancy with Failure to Thrive in first year of life; weak cry, delayed motor milestones –delayed walking until 2 years Short stature Hypogonadism Hyperphagia—food seeking behavior, hoarding, eating inedible, leading to morbid obesity Low muscle tone leads to exercise aversion Avg IQ around 70-good expressive language Skin picking Variable cognition—strength in visual processing Low tolerance for teasing, try to hide overeating, nurturing tends to get “stuck on topics”
Victor at 1 year Behavioral problems--low frustration tolerance, socialization difficulties, temper tantrums, OC tendencies, rituals, impulsivity, skin picking Weight control—obesity can be prevented 1000 to 1200 cal diet w 30 minutes exercise—locking up food—consider growth hormone since many have GH deficiency (as of 2000, GH becamre a treatment for PWS)—slightly controvertial
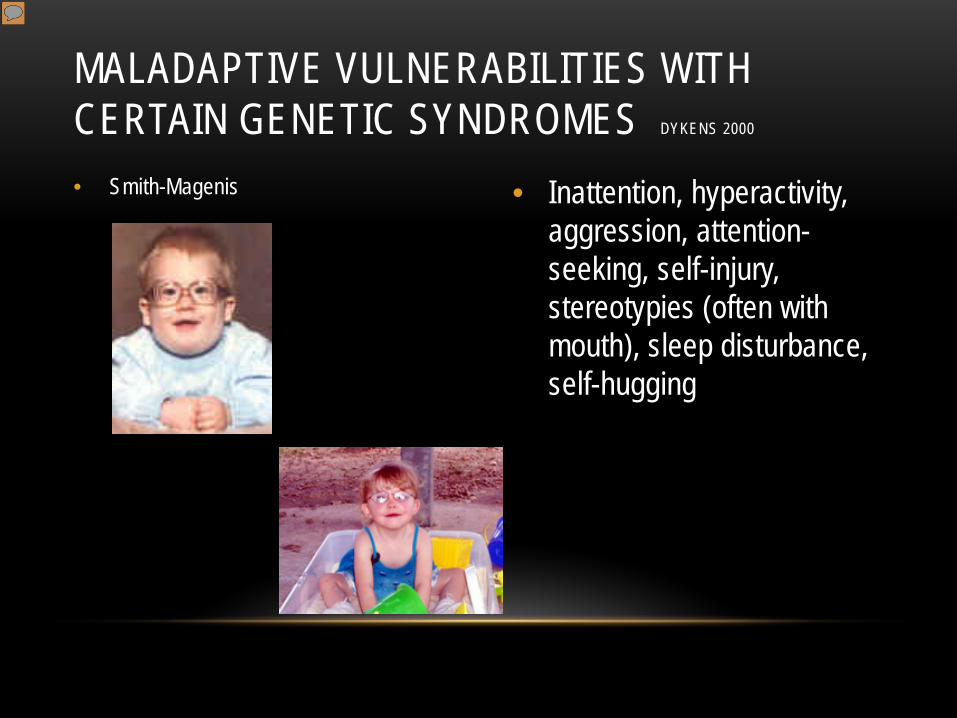
MALADAPTIVE VULNERABILITIES WITH CERTAIN GENETIC SYNDROMES DYKENS 2000
Presenter
Presentation Notes
Chromosome deletion 17p11.2 Nail yanking, oriffice stuffing Sleep disturbance—frequent awakenings at night, early wakeup sleep attacks during the day inversion of the melatonin cycle Perseveration—often asking the same questions Often in competition with peers/sibs for staff/parent attention Challenging behaviors: poor impulse control, aggressive hugging of others, prolonged tantrums, difficulty adjusting to change in routine, poor sense of time—cannot be rushed Positive aspects: engaging, endearing & full oif personality Appreciative of attention, Eager to please, sense of humor, communicative , responsive to structure, causes of outburst are often identifiable and outbursts can often be redirected if caught early
Relatively high cognitive and social abilities versus very young emotional development “Emotional toddler” iin SMS Low frustration tolerance, live in the moment, possessive attachment to caregivers, difficulty awaiting turns, Developmental Asynchrony—disparity occurs later in childhood & adulthood This does not mean treating older person with SMS as a child Professionals are generally not trained in early childhood special ed approaches and you need this early childhood approach grown up to adulthood use of day planner, computer reminders, phone reminders smorgasbord of school, work, tasks of short duration emphasis on hands-on apprach
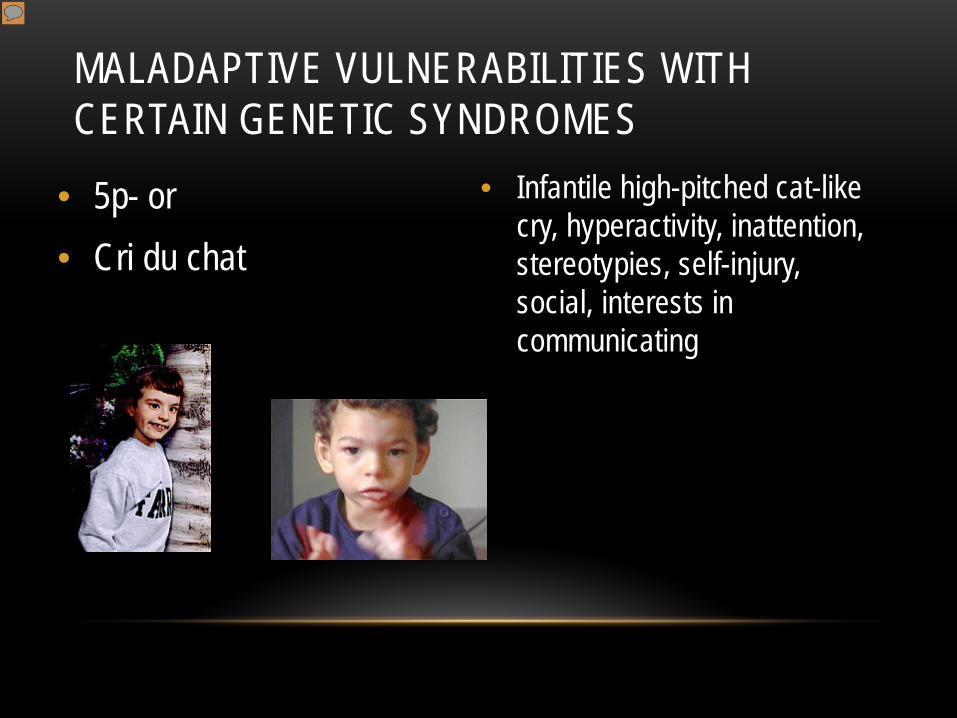
MALADAPTIVE VULNERABILITIES WITH CERTAIN GENETIC SYNDROMES
Presenter
Presentation Notes
Cri-du-chat (cat's cry) syndrome, also known as 5p- (5p minus) syndrome, is a chromosomal condition that results when a piece of chromosome 5 is missing. Infants with this condition often have a high-pitched cry that sounds like that of a cat. The disorder is characterized by intellectual disability and delayed development, small head size (microcephaly), low birth weight, and weak muscle tone (hypotonia) in infancy. Affected individuals also have distinctive facial features, including widely set eyes (hypertelorism), low-set ears, a small jaw, and a rounded face. Some children with cri-du-chat syndrome are born with a heart defect.
• Self-injurious behavior is seen in 4% to 16% • Recent studies integrate behavioral triggers with abnormalities
in the endogenous opioid and serotonin systems • 17% with ID have deafness • 30% with ID have visual impairments
Presenter
Presentation Notes
Different patterns of self-injury are associated with different syndromes Lesch-Nyan (extreme lip and finger biting), fragile X (hand-biting), Smith-Magenis (head banging, nail pulling, inserting objects into body orifices) These disorders may provide insight into biochemical anomalies associated with self-injury such as abnormal purine metabolism and dopaminergic functions in Lesch-Nyan.
Syndenham’s Chorea a CNS disease arising from Strepococcal infection (10% cases from rheumatic fever) characterized by involuntary, purposeless movements and there is no long term effects Cerebral palsy Cerebral palsy term used broadly to describe a number of motor disorders characterized by impaired voluntary movement resulting from prenatal developmental abnormalities or post natal CNS damage occurring before the age of 5 Spastic –involve motor functions, may have undeveloped limbs Athetoid-slow writhing movements, movements increase with emotional tension, results from basal gangliua involvement Ataxic-involvement of cerebellum, weakness, intention tremor, difficulty with rapid movements Muscular dystrophies-usually appear in boys 3 to 7y/o, confined to wheelchair by 10-12 and most die of respiratory complications by 20y/o
PSYCHOSOCIAL CONSIDERATIONSHEIMAN, 98
• Being different from peers • Losses rather than gains • Social isolation although mainstreamed • Rejected by peers • Failure experiences dominate school histories • Low social status
PSYCHOSOCIAL CONSIDERATIONS ZIGLER, 1999
• Outer directed personality orientation • look to others rather than selves for problem solution
• Aberrant social styles • Too wary or too disinhibited • Low expectancy or enjoyment of success
PSYCHOSOCIAL CONSIDERATIONS • Adolescents with ID are at a higher risk for developing
depression • Children & adolescents with ID are at heightened risk for
exploitation & physical or sexual abuse • Friendships with non-disabled peers show lack of shared play,
decision-making & laughter
Presenter
Presentation Notes
Kids with certain etiology may be susceptible to peer difficulties. Prader-Willi syndrome (with its related obesity and behavioral problems are more apt to be teased and disliked by peers Despite their sociability, children with Williams syndrome have difficulty with friends due to their anxiety, disinhibition and indiccriminate relating to others.
INDIVIDUAL AND FAMILY PREDICTORS OF PSYCHOPATHOLOGY DEKKER ET AL, 2003
• Inadequate daily living skills • Social incompetence • Chronic physical condition • High physical symptoms • Negative life events • Psychopathology of caregiver
VULNERABILITIES CHARLOT, 2011
• VULNERABILITIES commonly seen in people with IDD include challenges to learning and communication that can have a large influence on behavior • Also known as “risk factors” • Communication deficits • Learning challenges and teaching Implications
LEARNING CHARACTERISTICS OF PEOPLE WITH IDD CHARLOT, 2011
•WILLIAM I. GARDNER, PH.D. •49
• Learning occurs more slowly • Slower “information processing”
• Difficulty remembering information, especially recently learned materials
• Might repeat back when calm, then cannot remember when upset • Difficulty in working memory
• Has huge impact on problem solving • Difficulty in executive functions
• Planning, control over our emotions and behavior…using what we learned when we need it
LEARNING CHARACTERISTICS CHARLOT, 2011
•WILLIAM I. GARDNER, PH.D. •50
• Attention difficulties, both focus and span
• Yet may “perseverate” on some things • Much harder to focus on things that are too difficult
• Problems in learning abstract concepts • Problems with cognitive rigidity
• Difficulty changing from one task to another • Accepting alternative solutions or explanations • Shifting focus of attention
• This BRAIN BASED not being stubborn, or oppositional
LEARNING CHARACTERISTICS CHARLOT, 2011
•WILLIAM I. GARDNER, PH.D. •51
• Difficulty in generalizing skills acquired in one situation/at one time to other conditions/circumstances • Especially when there is stress or anxiety
• Difficulty planning - implementing complex behavioral chains/sequences of actions. • SEQUENCING deficits are common • May not understand time concepts well so its hard to wait for things
LEARNING CHARACTERISTICS CHARLOT, 2011
•WILLIAM I. GARDNER, PH.D. •52
• Demonstrates an outer-directedness and passive learning style (seeks cues/directions from others)
• Low expectations for being a successful learner due to excessive failure history ⇒ generalized learned helplessness
Unique Differences and Commomnalites
NUANCES OF ASSESSMENT
DM–ID: Two Manuals
•Diagnostic Manual – Intellectual Disability: A Clinical Guide for Diagnosis of Mental Disorders in Persons with Intellectual Disability
•Diagnostic Manual – Intellectual Disability: A Textbook of Diagnosis of Mental Disorders in Persons with Intellectual Disability
Presenter
Presentation Notes
Actually two diagnostic manuals were developed. We first developed the Diagnostic Manual – Intellectual Disability: A Textbook of Diagnosis of Mental Disorders in Persons with Intellectual Disability. This is a rather large book with over 550 pages. After we developed the textbook, it was suggested, by a large number of peer reviewers as well as our international advisory committee, that we develop a clinical manual that would be easily accessible to both psychiatrists as well as primary care physicians. We then embarked on the development of a second diagnostic manual entitled Diagnostic Manuel – Intellectual Disability: A Clinical Guide for Diagnosis of Mental Disorders in Persons with Intellectual Disability. Everything that is in the 350 plus pages clinical guide is also in the textbook. The textbook has a great deal of background information, a review of the research for each diagnostic category, as well as a section on pathogenesis and etiology for each diagnostic category. All of the diagnoses, diagnostic subcategories, and criteria modifications are identical in both books. Both books can be used to diagnose a specific psychThe DM-ID was developed by NADD in association with the APA and published in 2007. The work on the DM-ID began in 1997, and it took ten years to develop this diagnostic manual. There were approximately 100 psychiatrists and other clinicians from around the world who worked on the development of the DM-ID. Developing the DM-ID was a major project and was partially funded by the Joseph P. Kennedy Jr. Foundation. iatric disorder in persons with ID.
The Bio-medical Culprit
MEDICAL CONDITIONS
OVERVIEW OF I/DD AND PSYCHIATRIC DIAGNOSES • Always consider medical causes of behavior first
• Co-occurring medical disorders—importance of integrating medical conditions • Chronic Pain
• 21% higher prevalence vs. 1% in I/DD • Generalized seizures • Partial seizures • Pseudoseizures
Presenter
Presentation Notes
Dysphagia is common with cerebral palsy, malformations of the face, missing teeth, Parkinson's syndrome, poor motor skills, reflux and seizure disorders Is there continued weight loss? Is there a pattern of pneumonia or respiratory infection? Is there coughing during mealtimes? Are there difficulties chewing? GERD common—persons with moderate to severe ID have higher incidence of GERD as do people with cerebral palsy, scoliosis, non-ambulatory, on anti-convulsants Treatment is an anti- reflux diet and antacids or acid-reducer (prilosec, Nexium etc) Urological conditions--Long term use of psychotropics can cause neurogenic bladder and Downs syndrome has higher incidence of urinary track and renal hypoplasia Need to look for prostate problems as well Asthma—frequently undetected .. Signs are coughing at night, daytime fatigue, signs of URI, restlessness, itchy/watery eyes, wheezing Seizures—Generalized—all of brain affected with unconsciousness/convulsions Partial—abnormal electrical activity in part of brain—psychomotor or temporal lobe Pseudoseizures—psychogenic in nature but can easily be misdiagnosed and can co-exist with a true seizure disorder
ASSESSING FOR PAIN (MCGILVERY & SWEELAND, 2011 & ZWAKHALEN ET AL, 2004)
• Do not underestimate the effect of chronic pain on behavior • Observe for any pain-related behavior in non-verbal persons • Look for:
• Facial expressions • Moving in unusual ways • Not using part of body • Vocalizations such as moaning/ crying
• Assess for sleep, ambulation and sitting changes • Add pain management strategies to the treatment plan
Presenter
Presentation Notes
Advocate for the person to ensure that pain is treated Use pain management medications May need assessment from a pain management specialist with caregiver input
I/DD AND PSYCHIATRIC DIAGNOSES IN ADULTS
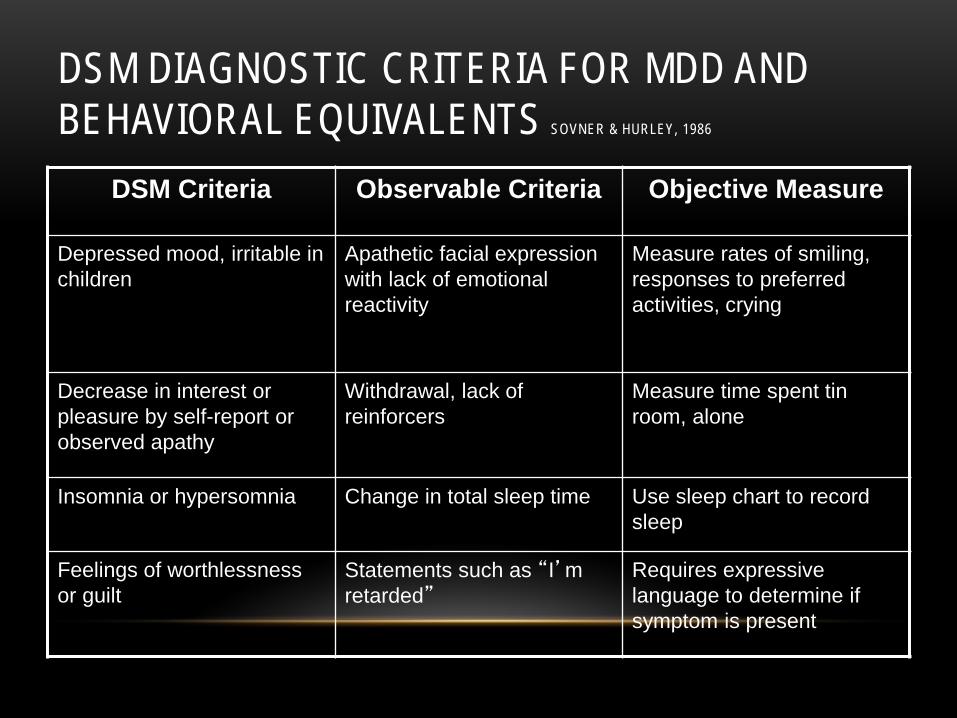
• Most Frequent DSM 5 mental illnesses in persons with ID/D • Depressive disorders
• Major depressive disorder • With psychotic features
• Bipolar disorder • Anxiety disorders
• Generalized anxiety disorder • Obsessive compulsive and related disorders
• Trauma and stressor related disorders • Personality disorders in persons with ID/DD • Major psychotic disorders
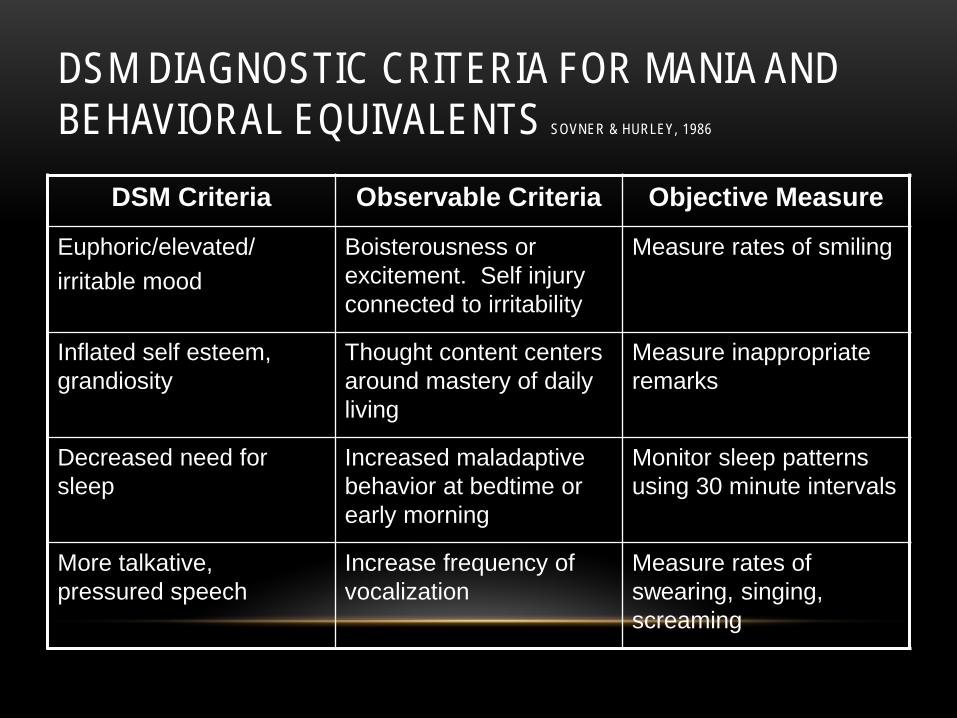
Boisterousness or excitement. Self injury connected to irritability
Measure rates of smiling
Inflated self esteem, grandiosity
Thought content centers around mastery of daily living
Measure inappropriate remarks
Decreased need for sleep
Increased maladaptive behavior at bedtime or early morning
Monitor sleep patterns using 30 minute intervals
More talkative, pressured speech
Increase frequency of vocalization
Measure rates of swearing, singing, screaming
COMMUNICATION (MCGILVERY & SWEELAND, 2011)
• Receptive language skills
• Expressive language skills
• Methods of communication
• May need to modify language
• Keep language simple
• Explain what you are doing
• Be sensitive to impact of medication on processing
• Use adult communication
Presenter
Presentation Notes
receptive language disorder may have difficulty understanding spoken language, responding appropriately, or both. This leads to substantial difficulty communicating. Thy have difficulty with language processing and the connection between words and ideas they represent. Some people may also have problems with pronunciation of words and speech / sound . Receptive language develops first Expressive Language Disorders - People with expressive language disorders may understand what is said to them or written in passages, but they have substantial difficulty communicating. They have difficulty with language processing and the connection between words and ideas they represent. Some people may also have problems with pronunciation of words. Expressive language may exceed their receptive skills—giving the appearance they understand more than they do With receptive communication—does he follow verbal requests and if so, how many Does he tell you yes or no when asked if he wants something , go somewhere etc? Simple & concrete language—point, gesture, model to assist in clarifying information Reduce words and do not use complex instructions Explanations are respectful Do not use child-like speech. People have years of life experience and deserve respect in verbal and non-verbal approaches
ENHANCING PERSON TO PERSON COMMUNICATION (MCGILVERY & SWEELAND, 2011)
• Developing therapeutic relationship • Active listening • Empathetic responses • Non-judgmental attitude • Avoid power struggles • Be aware of body language and position • Validate the person’s feelings • Offer choices and alternatives
Presenter
Presentation Notes
Can use reflective communication—to assist with understanding Empathy is the ability to understand another’s feelings and see how they perceive a situation An accepting attitude is important. This does not imply that problematic behavior is acceptable, but that at baseline, there is a non-critical relationship Avoid a physical stance or posture that can be viewed as challenging People in the state hospital are there involuntarily and already feel powerless—by presenting choices, this can assist in relationship development
WHAT INFLUENCES HOW WE BEHAVE?GARDNER
• “Multimodalities of Influence” Lots of different things will affect person’s tendency to become aggressive • Biomedical
• Medical – Neurological – People with IDD have problems and don’t self-report well • Psychiatric – Depression, anxiety etc impact on how we behave when stressed and
vice versa • Genetic - we are born with some areas of strength and weakness, temperament etc
• Psychological- • Cognitive (How we process information and our beliefs) • Emotional (feelings and how we manage our emotional states) • Motivational, behavioral (what we learn and what matters most to us)
• (Re)-Habilitation--to restore person to level prior to illness episode, e.g., pre-illness level of functioning ⇒ depressive episode ⇒ inappropriate self-harm ⇒ treatment of depression ⇒ return to pre-illness level of functioning+ absence of self-harm behaviors
• Habilitation-- to teach new or improved ways of successfully coping with a range of personal, interpersonal, and social expectations, demands, or requirements. No assumption that person with ID initially had skills but lost them due to illness.


![[PPT]Mental Retardationmrsashleymhelmsclass.wikispaces.com/file/view/Mental... · Web viewMental Retardation (Intellectual Disability) By: Cindy Infante Psychology (HONORS) Causes](https://img.pdfslide.us/doc/110x75/5ab8d3c77f8b9ad13d8cfa88/pptmental-retardation-viewmental-retardation-intellectual-disability-by-cindy.jpg)