Embed Size (px)
DESCRIPTION
The Jul/Aug 2009 issue of Clinical Oncology News
Citation preview

Oncology Practices Struggle ToWeather Financial StormNational Harbor, Md.—A few months ago, Cliff Goodman, PhD, senior vice pres-ident of the Lewin Group, was stressed out. He serves on the board of directors at a mid-size oncology practice in the Midwest and the practice was in “serious financial trouble.”
“We are having trouble securing enough reimbursement to cover costs. I have lost some of my workforce. The competition recently acquired some of this big-ticket technology and is marketing in the commu-nity. And my accountant is telling me that I can’t afford to buy that CT scanner our staff
is demanding,” Dr. Goodman said.His oncology practice is not alone—prac-
tices around the country are struggling.
Economic Woes
One big challenge is the purchase of big-ticket items when cash flow is a problem. This is particularly problemat-ic for oncology centers that have radia-tion oncology departments. “I think phy-sicians started out saying, ‘we are going to add this service.’ [They] struggled with the cost of a startup and, like a rat on the
One of the most anticipated pre-sentations at the annual meet-
ing of the American Society of Clinical Oncology (ASCO) was the long-awaited results of NSABP C-08 (abstract LBA4), which tested the efficacy of bevacizum-ab (Avastin, Genentech) as adjuvant therapy in stages II and III colon can-cer patients. In this Phase III trial, 2,710 patients were randomized to a standard arm of six months of adjuvant oxali-platin, 5-fluorouracil (5-FU) and leu-covorin (modified FOLFOX6) with or without bevacizumab (5 mg/kg), with
The Impact of LBA4 On Clinical Trials And Patient Care
Orlando, Fla.—PARP-1 inhibitors have shown strong potential to treat challeng-ing forms of cancer, according to three studies presented at the annual meet-ing of the American Society of Clinical Oncology (ASCO). In a Phase II study, PARP inhibitors increased overall sur-vival by roughly 50% in patients with metastatic, triple-negative breast can-cer. In another Phase II study of patients with BRCA-deficient advanced breast cancer, PARP-1 inhibitors resulted in a progression-free survival duration of 5.7 months, a PFS not usually seen in a population with very limited treatment options. And in a third study, PARP inhibitors showed promise for the treat-ment of relapsed ovarian cancer.
“[PARP inhibition] is an area that will explode in the next year or two,”
PARP-1 Inhibitors Touted as Next Big Breakthrough
Orlando, Fla.—Results from three Phase III trials have shown that maintenance thera-py provided after first-line chemotherapy, but before disease p r o g r e s s i o n , c a n improve progres-sion-free survival (PFS) in patients with advanced non-small celll u n g c a n c e r(NSCLC). In theone tr ia l that h a d a s u f f i -cient number ofevents to ana-l y z e o v e r a l lsurvival (OS), this was increased, too. In July, the results of this third trial sparked the FDA to approve pemetrexed (Alim-ta, Eli Lilly) as maintenance therapy for locally advanced or metastatic NSCLC,
specifically for patients with a non-squamous histology whose
disease has not progressed after four cycles of plat-
inum-based first-linechemotherapy. The
drug is not approvedfor the treatment of patients with s q u a m o u s c e l l NSCLC.
E a c h o f t h estudies, present-ed at the annu-al meet ing oft h e A m e r i c a n Society of Clin-i c a l O n c o l o g y (ASCO), met its
primary end point, leading at least one of the lead authors to characterize the results as a potential paradigm shift in care of advanced NSCLC. Although the discussant,
Maintenance Therapy in NSCLC:
Paradigm Shift in Care?
McMahon Publishing
Advances in Cancer CareCLINICALONCOLOGY.COM • JULY/AUGUST 2009 • Vol. 4, No. 3
see IMPACT, page 12 �
see PARP, page 9 �
see MAINTENANCE, page 6 �
POLICY & MANAGEMENT
ADVISORY BOARD EDITORIAL
see FINANCIAL STORM, page 3 �
Alimta from Eli Lilly approved
for maintenancetherapy in NSCLC.
See page 14.
NEW PRODUCT INDICATION
Targeted Cancer Therapy
Razelle Kurzrock; Maurie Markman
For more information, see page 13.
McMahonMedicalBooks.com
SOLID TUMORS
7 Maurie Markman, MD, discusses practice-changing ovarian cancer news.
10 Bevacizumab, pazopanib ripefor approval in RCC, says expert.
FDA NEWS
14 Pemetrexed gets fourth indication. Opioid gets green light.
SUPPORTIVE CARE
22 Is VKORC1 test needed in all patients receiving warfarin?
22 Interventional pain techniques effective in children
WWW.CMEZONE.COM
EDUCATIONAL REVIEWS
Treatment Options for Platinum-Sensitive Recurrent Ovarian Cancer
After page 6.
Guide to the Prevention Of Chemotherapy Medication Errors: Part 1
After page 14.
HEMATOLOGIC DISEASE
4 Richard Stone, MD, and Jennifer Brown, MD, PhD, highlight ASCO meeting news.

50004 18DEC07
YOUnique Insight
PharmacoDiagnostic® Breast Cancer ResourcesDako supports every breast cancer patient, oncologist, pathologist, and diagnostic lab with a sophisticated framework of pharmDx™ kits and resources that deliver uncompromising accuracy, allowing YOUnique Insight for better clinical interpretations with more certainty.
Dako offers proven reliability through both FDA-cleared and FDA-approved complete breast cancer kits and the widest selection, resulting in fewer reruns and increased productivity for a higher return on investment.
Knowledge that empowers. Resources that enable. YOUnique Insight from Dako.
www.dako.com.

CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 3
wheel, they have to replace their equipment because the guy down the street replaced his equipment and is now advertising that he has better equipment,” said Ed Braud, MD, a medical oncologist at ACT Medical Group in Rockford, Ill.
Other oncologists agree. “When a radiation oncol-ogist comes and asks you for $50,000, that is chump change to them—that is not chump change to any oth-er department in the hospital,” said Richard Reiling, MD, medical director of the Cancer Center at Presby-terian Hospital, Novant Health, in Charlotte, N.C.
Staffing Shortages
Another problem exacerbated by the current reces-sion is staffing shortages, a problem many might find odd given the growing unemployment crisis. In many cases, however, a cancer center staff member quits because his or her spouse has been laid off and the couple must relocate because of a dearth of jobs in the area. Oncology practices are left hanging—they can-not easily find replacements for credentialed staff, such as nurses and physiatrists. This is particularly true in oncology practices in the more remote areas of the United States, where skilled individuals with the degrees necessary to do the work are not available.
“In terms of the workforce, particularly in Rich-mond, Virginia, over the last several months, we have been hit very hard,” said Tom Gallo, executive direc-tor of the Virginia Cancer Institute, the largest medical oncology practice in Virginia. He said that Richmond-area companies, such as Circuit City, Land Ameri-ca Financial Group and Chesapeake Paper, are just a few of the casualties of the economic downturn. “Our unemployment rate has swung very dramatically,” Mr. Gallo said. Virginia Cancer Institute has experienced
a shortage of oncologists, nurses and other trained oncology staff.
“Nurse practitioners have cer-tainly been a tremendous com-plement to the practice, but finding those professionals who are trained in oncolo-gy is also difficult. One of the indirect things we have seen [from the recession] is los-ing staff because many of our employees are from two-earner families and their spouses have lost their job (forcing a relocation),” said Mr. Gallo.
Many oncologists echo this sentiment. “Radiation therapy technicians are hard to get,” said Dr. Reiling. “Physicists are hard to get.” At a presen-tation at the annual meeting of the American Associ-ation of Community Cancer Centers (ACCC) held in March, Dr. Braud asked the audience how many were looking for help in their office. Roughly 50% of the audience members raised their hands.
Solutions
So, how do cancer centers adjust to the changing economy? “That is a loaded question because the econo-my is a floating boat in a stormy sea and it’s going up and down,” said Dr. Reiling, speaking at the ACCC meeting. “I don’t think there is anyone in this group who has not cut off all travel and all capital expenditures.”
This will have serious implications for the future, especially in light of the fact that the cancer burden is only expected to increase. A recent study in the Jour-nal of Clinical Oncology revealed that over the next 20 years, the number of new cancer cases diagnosed annually in the United States will increase by 45% (2009; Epub ahead of print, PMID: 19403886). “We are not going to be able to handle this load when we
get all 40 billion people into the system and all the baby boomers are coming
in and testing for cancer,” Dr. Reil-ing said.
Mr. Gallo said his practice has responded to the economy and workforce shortage problem by pooling resources and relying on mid-level practitioners.
“One thing we have done is outsourced our lab service,” said
Mr. Gallo. “I am strictly a medical oncology practice with four offices
and we ran a lab internally for years. From a financial point of view, it was a
marginal or break-even [venture]. Eighteen months ago, we decided to contract with an outside provider to rent space in our office and provide for lab services. It’s a national program. They have train-ing programs and access to a much wider pool of tal-ent than we had individually.”
The second way his office has responded is by add-ing mid-level practitioners. “Over the last seven years, we have added mid-level practitioners. In 2001, we were probably a 12-doctor practice with no mid-levels and now we have 15 full-time doctors and six mid-lev-el practitioners in order to supplement the increased volume,” said Mr. Gallo.
Dr. Goodman said that, in these tough economic times, pooling resources and drawing on the capacity of larger organizations should provide practices with more flexibility and depth. Struggling clinics need to explore these and other alternatives to stay afloat and competitive right now.
To weigh in and discuss how your practice is reacting to the economic crisis, visit www.clinicaloncology.com and enter your thoughts in the comment section next to this story online.
—Kate O’Rourke
POLICY & MANAGEMENT
Finance
FINANCIAL STORMcontinued from page 1 �
ADVISORY BOARD
BioethicsJoseph P. DeMarco, PhDPaul J. Ford, PhD
Community OncologyMichael J. Fisch, MD, MPHJohn W. Finnie, MD
Hematologic MalignanciesJennifer R. Brown, MD, PhDAgnes Y.Y. Lee, MSc, MDRichard Stone, MD
Oncology Nursing Betty Ferrell, RN, PhD
PharmacyPolly E. Kintzel, PharmDMelvin E. Liter, MS, PharmD
Policy and ManagementMary Lou Bowers, MBABarbara Constable, RN, MBARhonda M. Gold, RN, MSN
Solid Tumors Bone Metastases
Allan Lipton, MD
Breast Cancer
Andrew Seidman, MD
Gastrointestinal Cancer
Edward Chu, MDCathy Eng, MDLeonard Saltz, MD
Gastrointestinal Cancer and Sarcoma
Ephraim Casper, MD
Genitourinary Cancer
Ronald M. Bukowski, MD
Gynecologic Cancer
Maurie Markman, MD
Lung, and Head and Neck Cancers
Edward S. Kim, MD
Lung Cancer, Emesis
Richard J. Gralla, MD
Infection ControlSusan K. Seo, MD, Director
Symptom Control and Palliative CareWilliam S. Breitbart, MD
Steven D. Passik, PhD
Joseph V. Pergolizzi Jr., MD
Russell K. Portenoy, MD
Charles F. von Gunten, MD
EDITORIAL STAFF
Kate O’Rourke, [email protected]
Sarah Tilyou, Senior [email protected]
James Prudden, Group Editorial Director
David Bronstein, Editorial Director, Hospital Group
Robin B. Weisberg, Manager, Copyediting Services
Elizabeth Zhong, Associate Copy Chief
SALES STAFF
Thomas Ciriacks, Group Publication [email protected]
Julianna Dawson, Associate Publication [email protected]
Nancy Parker, Executive Manager/Classified Advertising, [email protected]
ART AND PRODUCTION STAFF
Michele McMahon Velle, Creative Director, MAX Graphics
Frank Tagarello, Senior Art Director/Managing Director, MAX Graphics
Dan Radebaugh, Director of Production and Technical Operations
Diane Nielebock, Circulation Coordinatator
MCMAHON PUBLISHING
Raymond E. McMahon, Publisher & CEO, Managing Partner
Van Velle, President, Partner
Thomas Ciriacks, Vice President, Medical Education
Matthew McMahon, General Manager, Partner
Lauren Smith, Michael McMahon, Michele McMahon Velle, Rosanne C. McMahon, Partners
McMahon Publishing is a 36-year-old, family-owned medical publishing and medical education company. McMahon publishes seven clinical newspapers, seven special editions, and continuing medical education and custom publications.
Copyright © 2009 by McMahon Publishing, New York, NY 10036. All rights reserved. Clinical Oncology News (ISSN 1933-0677) is published monthly for $70.00 per year by McMahon Publishing. Postage paid at New York, NY, and at additional mailing offices.
www.mcmahonmed.com
POSTMASTER: Please send address changes to Clinical Oncology News, 545 W. 45th St., 8th Floor, New York, NY 10036.
Would you like to receive Clinical Oncology News or change your delivery address?All U.S. oncologists, hematologist/oncologists, surgical oncologists, oncology nurses and oncology pharmacists should re ceive Clinical Oncology News free of charge. If you are changing your address or name, you must notify the AMA at (800) 262-3211 or the AOA (if appropriate) at (800) 621-1773. To contin-ue receiving Clinical Oncology News, you need not be a member of either organization; however, they main-tain the ultimate source of our mailing addresses. For added assurance of uninterrupted receipt, you may also mail or fax a copy of your current mailing label along with your change of address and signature to:
Circulation Manager, Clinical Oncology News, 545 W. 45th St., 8th Floor, New York, NY 10036. Fax: (212) 977-3645.
If you are not a member of the groups listed above and would like to subscribe, please send a check pay-able to Clinical Oncology News. Please allow 8-12 weeks for delivery of the first issue. Subscription: $70.00 domestic, $90.00 international. Single copies $7.00 domestic, $10.00 international.
TM

4 CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009
Experts Highlight Hematology News From ASCO
Tweaking Induction Therapy for AML Increases Survival
A randomized trial of anthracycline dose intensification during induc-
tion of younger patients with acute myeloid leukemia has revealed that tweaking the dose can increase surviv-al by 8 months (abstract 7003). The study was conducted by the Eastern Cooperative Oncology Group (ECOG; study E1900).
Disappointingly, induction therapy for patients with acute myeloid leuke-mia (AML) has changed little in three decades. Adults of all ages with AML who are deemed treatment candidates are generally given an anthracycline for three days plus seven days of continu-ous infusional cytarabine. A Phase I study performed by the CALGB ded-icated to devising an induction ther-apy (including etoposide) that could be given with or without a drug resis-tance modulator showed that doses of daunorubicin over 90 mg/m2 for three days were well tolerated.
The ECOG thus sought to deter-mine whether high-dose daunorubicin might actually lead to a superior out-come compared with standard-dose daunorubicin. Adult patients with pre-viously untreated AML were random-ized to receive either daunorubicin at the standard dose (45 mg/m2 per day) or a high dose (90 mg/m2 per day), each for three days combined with standard-dose cytarabine (100 mg/m2 per day) for seven days by continuous
intravenous infusion. A second course of induction therapy was given (using standard-dose daunorubin in either arm) if leukemia persisted mid-cycle. Those achieving a complete remission were allocated to allogeneic stem cell transplantation or high-dose cytarabine prior to high-dose chemotherapy with peripheral blood stem cell rescue.
This study is one of the few trials to show a survival benefit based on a change in induction therapy. Those randomized to high-dose daunoru-bicin had a significantly higher com-plete remission rate (70.6% vs. 57.3%) and median overall survival (23.7 vs. 15.7 months; P=0.003) (Figure 1). This is a most striking result suggest-ing that the higher dose of daunoru-bicin was probably leading to a lower leukemia burden at the time of remis-sion and, therefore, a lower incidence of relapse. Fortunately, the benefit was not achieved at a higher cost—induc-tion death rates were similar in the two groups (about 5% in each arm). Subgroup analysis revealed that the patients who benefited from the high-er-dose daunorubicin were those with favorable or intermediate cytogenetics, those without FLT3 internal tandem duplication (ITD) mutations and those who were younger than age 55 years.
This is an important study that sug-gests that 45 mg/m2 per day of dauno-rubicin is an insufficient dose for induc-tion therapy in patients under the age of 60 years. However, it is not clear whether 90 mg/m2 is better than 60 mg/m2 per day, which is now probably the most commonly used dose (based on the CALGB trial) in induction thera-py for patients between the ages of 18 and 60 years. Another criticism of this trial is that the control group fared par-ticularly poorly compared with what might have been expected. None-theless, this trial answers a clinically important question only possibly asked by a cooperative group.
Wheat Grass: An Effective Iron Chelator in MDS?
A small study presented at the ASCO meeting (abstract 7012)
suggests that wheat grass may be an
effective iron chelator in patients with myelodysplastic syndromes (MDS). The juice is rich in oxalic and malic acids that could prevent intestinal dietary iron absorption as well as active ingre-dients that can chelate iron.
One of the major controversies in the management of patients with MDS is the optimal role of iron chelation therapy. Many patients with lower risk (International Prognostic Scoring Sys-tem low-risk or intermediate-1) are expected to survive at least five years and may require many red cell trans-fusions to maintain their hematocrit. These patients typically have high serum iron and ferritin levels. Wheth-er or not patients with MDS general-ly have complications of iron overload is unclear. Nonetheless, it has been the practice to provide chelation ther-apy for a selected group of patients with MDS. Historically, the available chelation therapy in this country, def-eroxamine, which must be adminis-tered subcutaneously for about 12 to 16 hours daily, is cumbersome and dis-liked by patients.
The recent approval of deferasirox (Exjade, Novartis), an oral iron chela-tion agent, has made it more feasible to treat a larger number of patients with MDS in an attempt to decrease iron stores. At the ASCO meeting, investigators from India reported on 20 patients with transfusion-depen-dent MDS who used five- to seven-day-old wheat grass (including stems) to make juice, of which 30 mL was given daily to each patient for six months. The mean serum ferritin lev-el of the patients was 2,250 mcg/L before wheat grass treatment and 950 mcg/L after treatment.
Although side effects of this ther-apy were not listed in the abstract, it appears that this natural remedy might be an effective iron chelator. How wheat grass compares to defera-sirox in terms of iron chelation ability is not clear. This study does not deal with the most important question: Is iron chelation therapy “worth it” in MDS? On the other hand, if a side effect–free, inexpensive and easy-to-administer regimen could reduce iron stores, it would certainly be easier to conduct a study that could answer the question.
Refining Prognostics In AML and Related Disorders
Several abstracts presented at the ASCO meeting dealt with new ways
to provide prognostic information for patients with acute myeloid leukemia and related disorders.
Two of the abstracts involved high-risk myeloid malignancies. Investiga-tors from the Cleveland Clinic (abstract 7016) showed that single nucleotide polymorphism (SNP) arrays could iden-tify gross chromosomal abnormali-ties with more resolution than stan-dard karyotyping and could detect copy-neutral loss of heterozygosity, a defect not detected by routine cytoge-netics. They found more chromosomal defects compared with standard cyto-genetics (71% vs. 47%) and showed that those with such SNP lesions had a worse median overall survival (41% vs.
not reached) than those without lesions. The prognostic significance of individual SNP abnormalities and how one should actually incorporate SNP abnormalities into our current prognostic scoring sys-tems for MDS is also unclear.
Marcucci and colleagues from Ohio State University (abstract 7000) showed that older adults with AML, known to fare poorly with available therapy, do somewhat better if they have normal cytogenetics and an NPM1 (nucleophosmin gene) mutation. Patients with an NPM1 mutation had a higher complete response (CR) rate (85% vs. 45%) and a better overall sur-vival (34% vs. 7% at three years) than similar patients without this genetic abnormality (Figure 2). Although these mutations predict a better outcome in this subgroup of adults with AML, the results are still inferior to what would be expected in a similar cytogenet-ics/genetic class of younger patients. Younger adults with cytogenetical-ly normal AML have been the focus of intense attempts to define prognos-tic subgroups. It is already recognized
Richard Stone, MD, highlights news on acute
leukemias, chronic myelogenous leukemia
and myelofibrosis. Dr. Stone is director of
the Adult Leukemia Program, Dana-Farber
Cancer Institute, and a professor of
medicine, Harvard Medical School,
both in Boston.
HEMATOLOGIC DISEASE
Multiple Cancers
25
20
15
10
5
0Me
dia
n O
ve
rall
Su
rviv
al, m
o
23.7
15.7
Cytarabine (100 mg/m2/d) + daunorubicin (90 mg/m2/d)
Cytarabine (100 mg/m2/d) + daunorubicin (45 mg/m2/d)
15.7
Figure 1. Comparison of induction therapies in patients with acute myeloid leukemia.
35
30
25
20
15
10
5
0Ove
rall
Su
rviv
al
at
Th
ree
Ye
ars
34
7
Patients with NPM1 mutations
Patients without NPM1 mutations
7
Figure 2. Comparison of survival in patients with acute myeloid leukemia.

CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 5
that patients with an FLT3 gene inter-nal tandem duplication (ITD) muta-tion (with or without an NMP1 muta-tion) have an inferior prognosis. This, however, was contradicted by a small study by M.D. Anderson Cancer Center investigators led by Santos (abstract 7015). Their study (481 patients) sug-gested that having an FLT3 mutation did not have prognostic importance in AML in those with either good- or poor-risk cytogenetics.
Marcucci and colleagues also showed (abstract 7001) that microRNA181a expression is associated with a good prognosis, including longer disease-free interval and overall survival, com-pared with those without microRNA- 181a expression. MIR181a expression was useful prognostically in the other-wise higher-risk group of cytogeneti-cally normal patients, those with FLT3 ITD or NPM1 wild-type disease. In this subgroup, those with higher MIR181a expression had a high rate of CR,
longer disease-free survival and better overall survival.
Finally, Marcucci and colleagues (abstract 7002) derived a prognos-tic classification system for younger patients with de novo cytogenetically normal AML which takes into account the FLT3 ITD, NMP1, CEBPα and WT1 mutational status, as well as ERG and BAALC expression.
A Bridge to Transplant Or a Bridge to Nowhere?
The study described in abstract 7032 analyzed the impact of aza-
citidine induction chemotherapy on post-transplant outcomes in patients with MDS.
Patients with MDS have no option for cure other than allogeneic stem cell transplantation. However, a major
controversy has been whether or not patients with excess marrow blasts would be better served by having some degree of cytoreductive therapy pri-or to transplant. Historically, there has been an aversion to giving aggressive induction chemotherapy to the large-ly older cohort of patients with demon-strated limited bone marrow reserve. The advent of DNA-hypomethylating agents such as azacitidine has made it possible to more safely treat patients with MDS in an attempt to reduce the blasts and, therefore, make transplant outcomes better.
It has been known for quite some time that patients who have a minimal disease burden fare better at the time of transplant. On the other hand, it is not known whether response to pre-transplant chemotherapy is a biolog-ical marker for better outcome after transplant or whether the pre-trans-plant chemotherapy actually “works” by lowering the disease burden. Cogle
et al tried to answer this question by analyzing post-transplant outcomes in 43 MDS patients, nine of whom received azacitidine before transplant and 34 who did not. It is important to point out that this was a retrospec-tive, nonrandomized study and that it is possible that 5-azacitidine patients were either better or worse candi-dates than their counterparts who did not receive this drug.
The group that received azacitidine before the transplant demonstrated better overall survival; however, the rates of acute and chronic graft-ver-sus-host disease and median over-all survival did not differ. There was a trend toward a higher relapse rate in the azacitidine group, suggesting that this was a population with a high-er original disease burden. Certainly, a randomized controlled trial would be necessary to prove or disprove the need to give hypomethylating agents prior to transplant.
Idiotype Vaccination Beneficial in Follicular Lymphoma
A Phase III trial has revealed that an idiotype vaccine can extend remis-
sion duration in certain patients with fol-licular lymphoma (FL; abstract 2). This is the third Phase III double-blind, ran-domized trial of an autologous tumor-derived patient-specific vaccine in FL.
The study enrolled previously untreat-ed advanced-stage FL patients and treated them with PACE chemo-therapy (prednisone, doxorubicin,
cyclophosphamide, and etoposide). Those patients who achieved a com-plete response/complete response unconfirmed (CR/CRu), 76% of the starting population, were random-ized. Of those 177 randomized, only 117 maintained their CR/CRu for six months as required to receive vaccine or placebo. Of the remaining 117 treat-ed with vaccine or placebo, at a medi-an follow-up of 57 months, the median time to relapse for the idiotype vac-cine group was 44 months, compared with 31 months for the control group (P=0.045; Figure 1). Thus, idiotype vac-cination extended remission duration in the subgroup of FL patients, about half the starting group, who were able to achieve a CR/CRu that persisted at least six months after chemotherapy.
The other two previously reported studies of idiotype vaccination failed to show a benefit, which may have been due to more relaxed criteria for the response required to move on to the vaccine phase, a shorter wait-ing time to vaccination or differenc-es in the vaccine. The most impor-tant problem with the study, however, is the absence of rituximab (Rituxan, Genentech/Biogen Idec), which is now a standard therapy for FL and which may alter responsiveness to or bene-fit from vaccine. Future studies will be required to address this question.
Long-term Follow-up Of FL Patients Receiving Rituximab
In the SAKK study (abstract 8512), FL patients received four weekly doses
of rituximab and then were random-ized to no further treatment or to four additional doses of rituximab at two-month intervals.
At a median follow-up of nine years and a minimum follow-up of five years in all patients, the median event-free survival (EFS) increased from 13 months in the observation arm to 24 months in the consolidation arm (Figure 2). Furthermore, those patients receiving consolidation ther-apy had a 25% and 18% chance of remaining in remission at five and eight years, respectively, suggesting remarkable sensitivity to rituximab in a subset of FL patients. The authors, however, were unable to identify a predictor of prolonged remission.
R-ICE Versus R-DHAP
In the CORAL study (abstract 8509), patients with diffuse large B-cell
lymphoma who were refractory to ini-tial therapy or in first relapse were ran-domized to salvage therapy with R-ICE (rituximab, ifosfamide, etoposide and carboplatin) or R-DHAP (rituximab, dexamethasone, aracytine and cisplat-inum). The overall response rate was 63%, with 38% complete remissions. No difference was observed between the arms in response rate or in three-year EFS or overall survival.
Utilization of Radiation Therapy in Early-Stage Hodgkin’s Disease
In recent years, the efficiacy of chemo-therapy in Hodgkin’s disease, as well
as increasing awareness of the long-term complications of radiation ther-apy, have led to increased interest in treating early stage Hodgkin’s disease with chemotherapy alone. In the study described in abstract 8511, researchers set out to assess the use of RT.
Investigators used the Surveillance, Epidemiology and End Results pro-gram registry to analyze patients diagnosed with early-stage Hodg-kin’s disease between 1990 and 2004, to look at the effect of RT on surviv-al (abstract 8511). Subgroup analy-ses were performed by era of treat-ment, sex and patient age. Receiving RT was associated with a significant improvement in overall survival and cause-specific survival (HR, 0.537 and 0.437, respectively) in all sub-groups. These results are intriguing and suggest that we should perhaps be circumspect in the current trend toward chemotherapy-only regimens, although the risks for long-term com-plications related to RT do need to be considered.
Jennifer R. Brown, MD, PhD, highlights news
regarding chronic lymphocytic leukemia
(CLL), Hodgkin’s disease, non-Hodgkin’s
lymphoma (NHL) and multiple myeloma (MM).
Dr. Brown is an attending physician with the
CLL & Lymphoma Program, Dana-Farber
Cancer Institute, and an assistant professor
of medicine at Harvard Medical School, both in Boston.
HEMATOLOGIC DISEASE
Multiple Cancers
50
40
30
20
10
0Me
dia
n T
ime
to
Re
lap
se, m
o
31
44
Patients receiving placebo
Patients receiving idiotype vaccination
Figure 1. Comparison of median time to relapse in patients with follicular lymphoma.
13
2450
40
30
20
10
0Me
dia
n E
ve
nt-
Fre
e S
urv
ival, m
o
Patients not receiving consolidation therapy
Patients receiving consolidation therapy with rituximab
Figure 2. Comparison of event-free survival in patients with follicular lymphoma.

Nasser H. Hanna, MD, invited to critique the three stud-ies at the meeting remained circumspect about their relevance to routine care in all patients because of a lack of reported quality-of-life (QoL) data, others saw the results as highly meaningful to extending the benefit of first-line chemotherapy. Dr. Hanna is an associate pro-fessor of medicine in the Department of Medicine and Division of Hematology/Oncology at the Simon Cancer Center, Indiana University, Indianapolis.
Pemetrexed Proves Potent
In a trial (abstract CRA8000) presented by Chan-dra P. Belani, MD, deputy director of Penn State Can-cer Institute, Hershey, Pa., 663 patients with stage IIIb/IVa NSCLC who had not progressed after four cycles of platinum-based chemotherapy were ran-domized to 500 mg/m2 pemetrexed plus best sup-portive care (BSC) or BSC plus placebo. Overall, the PFS was increased by almost two months (4.3 vs. 2.6 months; P<0.0001); OS was increased by almost three months (13.4 vs. 10.6 months; P=0.012). How-ever, the relative benefits of pemetrexed mainte-nance were even greater in nonsquamous cell his-tologies. Although there was no OS advantage in the squamous cell tumors (9.9 vs. 10.8 months; P=0.678), the survival advantage exceeded five months (15.5 vs. 10.3; P=0.007) when the squamous cell cancers were removed from the analysis. This translated into a highly significant reduction in the hazard ratio for death (hazard ratio [HR], 0.47; P<0.0001).
The survival advantage, however, was not without side effects. These included fatigue and neutropenia, and overall, 16% of patients on pemetrexed versus 4% on BSC alone (P<0.001) experienced a grade 3 adverse event (AE). According to Dr. Belani, however, AEs can be considered relatively modest in the context of one of the largest survival benefits yet observed in advanced NSCLC. He believes that these results are meaningful to routine patient care. Although he did not report QoL data, he said that such data were
collected and will be made available with the pub-lished manuscript.
ATLAS
A second study reported at the ASCO meeting was called ATLAS (abstract LBA8002). The largest of the three studies, ATLAS was stopped early by the Data and Safety Monitoring Committee because the prima-ry end point of PFS was met in a second planned inter-im analysis. In this study, 768 patients with stage IIIb/IV NSCLC who had achieved an objective response or stable disease on a combination of bevacizumab (Avas-tin, Genentech) and a platinum-containing doublet che-motherapy were randomized to 150 mg of erlotinib plus 15 mg/kg of bevacizumab administered every three weeks or bevacizumab plus placebo in the same sched-ule. At the time the study was stopped, the PFS advan-tage on the combination of erlotinib plus bevacizumab was a month greater than on bevacizumab alone (4.8 vs. 3.7 months). The difference was highly significant (HR, 0.72; 95% confidence interval [CI], 0.59-0.81; P=0.0012).
“The improvement in PFS was seen across multiple subgroups, including those defined on gender, histol-ogy, age and smoking status,” said the first author, Vin-cent A. Miller, MD, a thoracic oncologist at Memori-al Sloan-Kettering Cancer Center, New York City. He
reported that the safety profile was consistent with previous studies of the combination and indicated an acceptable level of tolerability. Survival data are not yet mature but are being collected.
SATURN
In a third study, called SATURN, 489 patients with stage IIIb (25%) or stage IV (75%) stable NSCLC who achieved stable disease or an objective response after a first-line, platinum-based che-motherapy were randomized to 150 mg erlotinib once daily or placebo (abstract 8001). At 24 weeks, the pro-portion of patients in PFS was 32% ver-sus 18%, favoring erlotinib (HR, 0.71; 95% CI, 0.62-0.82; P<0.0001), according to senior author Federico Cappuzzo, MD, Department of Medi-cal Oncology, Instituto Clinico Humanitas, Milan, Italy. The PFS was greater in the 45% of patients with ade-nocarcinoma (HR, 0.60; 95% CI, 0.48-0.75; P<0.0001) than in those with squamous cell histology (HR, 0.76; 95% CI, 0.60-0.95; P=0.0148).
“Erlotinib met the primary end point of PFS with a high degree of statistical significance, and significant improvement was seen in the secondary end points of response and disease control,” Dr. Cappuzzo said. He added that AEs were consistent with those previous-ly associated with erlotinib. Most importantly, “there was no deterioration in quality of life for erlotinib ver-sus placebo.” Again, survival data are not yet available, but are being collected.
Putting It in Perspective
Asked to discuss these three papers together, Dr. Hanna focused on the absence of QoL data. He was not sure if the gains in PFS for ATLAS and SATURN and
even the gain in OS with the pemetrexed study war-ranted a switch to this strategy in all patients.
“The questions I think patients are most interest-ed in are: does the earlier initiation of these agents in
my care result in me living longer and/or living better?” suggested Dr. Nasser. Although he
conceded that some patients may bene-fit from maintenance therapy, such as those who gain symptom control from maintenance therapy and have a good QoL before their disease progresses, he recommended that this approach must be used selectively.“It is clear from these strategies that
maintenance therapy improves pro-gression-free survival, but in my opin-
ion, improvement in progression-free surviv-al alone is less meaningful unless it also results in patients experiencing fewer cancer symptoms, fewer complications of their cancer or somehow measur-ing an improved quality of life, and none of that has been demonstrated by any of these trials,” Dr. Han-na said. Although maintenance therapy “does have great value” in the right patient, he noted that “most patients’ life expectancy is very short and you real-ly do not know whether exposing them to even the mild toxicities of longer-duration therapy is really benefiting them.”
This view was not well accepted by Dr. Belani, who stressed that the improvements in OS in his study were not only highly statistically significant, but clinically significant for a therapy that was reasonably well tol-erated. He believes that the data validate the concept of maintenance therapy in advanced NSCLC, and he expects this concept to be widely embraced.
—Ted Bosworth
6 CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009
MAINTENANCEcontinued from page 1 �
SOLID TUMORS
Lung
‘Most patients’ life expectancy is very short and you really do not know whether exposing them to even the mild toxicities of longer- duration therapy is really benefiting them.’
—Nasser H. Hanna, MD
5
4
3
2
1
0
Ove
rall
Su
rviv
al, m
o
4.3
2.6
Pemetrexed plus best supportive care (BSC)
BSC plus placebo
2.6
Figure 1. Comparison of overall survival with two different maintenance therapies.
5
4
3
2
1
0
Pro
gre
ssio
n-f
ree
Su
rviv
al, m
o
4.8
3.7
Erlotinib plus bevacizumab
Bevacizumab plus placebo
Figure 2. Comparison of overall survival with two different maintenance therapies.

CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 7
In the plenary session, Gordon J. Rus-tin, MD, et al. reported the long-await-ed results of the randomized Phase III trial that examined the impact on sur-vival associated with a CA-125 monitor-ing strategy in women with advanced ovarian cancer who had achieved a clinically defined complete response
to primary platinum-based chemother-apy (abstract 1). The study found that while routine monitoring of asymptom-atic women on an every-three-month schedule resulted in a median five-month earlier initiation of therapy for recurrent disease, there was no effect of this somewhat earlier treatment on overall survival. When ultimately pub-lished in the peer-reviewed literature, it will be important for these study results to be discussed by clinicians with their patients, as they may influence an indi-vidual ovarian cancer patient’s desire to undergo intensive routine CA-125 sur-veillance following completion of the primary treatment regimen.
Eric Pujade-Lauraine, MD, PhD,
presented the results of a second practice-changing abstract, the results of the CALYPSO trial (LBA5509). This trial directly compared a regimen of car-boplatin plus pegylated lipo-somal doxorubicin to carbo-platin plus paclitaxel when used for treatment of recurrent (potentially platinum-sensitive) ovarian cancer. The study revealed an improvement in progression-free sur-vival in favor of the pegylated liposomal
doxorubicin-containing regimen (median, 11.3 vs. 9.4 months;
hazard ratio, 0.82; P=0.005). Another interesting finding was the lower risk for car-boplatin-associated hyper-sensitivity reactions asso-
ciated with the pegylated liposomal doxorubicin pro-
gram (grade >2; 18% vs. 5%). This factor may have influenced
the amount of carboplatin that could be delivered to a substantial number of
patients, subsequently affecting the time of disease progression.
—Maurie Markman, MD
Ovarian Cancer News at ASCO To Impact PracticeTwo abstracts presented at the annual meeting of the American Society of Clinical Oncology can be deemed to be practice-changing news for patients with gynecologic malignancies. Both impact clinicians treating patients with ovarian cancer.
SOLID TUMORS
Ovarian
While routine monitoring of asymptomatic women on an
every-three-month schedule resulted in a median
five-month earlier initiation of therapy for recurrent
disease, there was no effect of this somewhat earlier
treatment on overall survival.
What’s Your View?
How will the results from the Rustin et al study impact how you care for patients? How have your patients
responded to the news?
Send replies [email protected]
Maurie Markman, MD
Vice President for Clinical ResearchUniversity of TexasM.D. Anderson Cancer Center, Houston, Texas
ADVISORY BOARD EDITORIAL
GEMZAR� (GEMCITABINE HCl) FOR INJECTIONBRIEF SUMMARY (OVARIAN). For complete safety please consult the package insert for completeprescribing information.
INDICATION AND USAGE: THERAPEUTIC INDICATION—Ovarian Cancer—Gemzar in combination withcarboplatin is indicated for the treatment of patients with advanced ovarian cancer that has relapsed atleast 6 months after completion of platinum-based therapy.
CLINICAL STUDIES: Ovarian Cancer—Gemzar was studied in a randomized Phase 3 study of 356 patientswith advanced ovarian cancer that had relapsed at least 6 months after first-line platinum-based therapy.Patients were randomized to receive either Gemzar 1000 mg/m2 on Days 1 and 8 of a 21-day cycle andcarboplatin AUC 4 administered after Gemzar on Day 1 of each cycle or single-agent carboplatin AUC 5administered on Day 1 of each 21-day cycle as the control arm. The primary endpoint of this study wasprogression free survival (PFS).
The addition of Gemzar to carboplatin resulted in statistically significant improvement in PFS and overallresponse rate. Approximately 75% of patients in each arm received poststudy chemotherapy. Only 13 of120 patients with documented poststudy chemotherapy regimen in the carboplatin arm received Gemzarafter progression. There was not a significant difference in overall survival between arms.
CONTRAINDICATION: Gemzar is contraindicated in those patients with a known hypersensitivity to the drug(see Allergic under ADVERSE REACTIONS).
WARNINGS: Caution—Prolongation of the infusion time beyond 60 minutes and more frequent thanweekly dosing have been shown to increase toxicity (see CLINICAL STUDIES in the full Prescribing Information).
Hematology—Gemzar can suppress bone marrow function as manifested by leukopenia, thrombocytopenia,yyand anemia (see ADVERSE REACTIONS), and myelosuppression is usually the dose-limiting toxicity.Patients should be monitored for myelosuppression during therapy. See DOSAGE AND ADMINISTRATIONin the full Prescribing Information for recommended dose adjustments.
Pulmonary—Pulmonary toxicity has been reported with the use of Gemzar. In cases of severe lung toxicity,Gemzar therapy should be discontinued immediately and appropriate supportive care measures instituted(see Pulmonary under Single-Agent Use and under Post-marketing experience in ADVERSE REACTIONSin the full Prescribing Information).
Renal—Hemolytic Uremic Syndrome (HUS) and/or renal failure have been reported following one or moredoses of Gemzar. Renal failure leading to death or requiring dialysis, despite discontinuation of therapy,has been rarely reported. The majority of the cases of renal failure leading to death were due to HUS (seeRenal under Single-Agent Use and under Post-marketing experience in ADVERSE REACTIONS in the fullPrescribing Information).
Hepatic—Serious hepatotoxicity, including liver failure and death, has been reported very rarely inpatients receiving Gemzar alone or in combination with other potentially hepatotoxic drugs (see Hepaticunder Single-Agent Use and under Post-marketing experience in ADVERSE REACTIONS in the fullPrescribing Information).
Pregnancy—Pregnancy Category D. Gemzar can cause fetal harm when administered to a pregnant woman.yyGemcitabine is embryotoxic causing fetal malformations (cleft palate, incomplete ossification) at dosesof 1.5 mg/kg/day in mice (about 1/200 the recommended human dose on a mg/m2 basis). Gemcitabineis fetotoxic causing fetal malformations (fused pulmonary artery, absence of gall bladder) at doses of0.1 mg/kg/day in rabbits (about 1/600 the recommended human dose on a mg/m2 basis). Embryotoxicitywas characterized by decreased fetal viability, reduced live litter sizes, and developmental delays. There areno studies of Gemzar in pregnant women. If Gemzar is used during pregnancy, or if the patient becomespregnant while taking Gemzar, the patient should be apprised of the potential hazard to the fetus.
PRECAUTIONS: General—Patients receiving therapy with Gemzar should be monitored closely by aphysician experienced in the use of cancer chemotherapeutic agents. Most adverse events are reversibleand do not need to result in discontinuation, although doses may need to be withheld or reduced. Therewas a greater tendency in women, especially older women, not to proceed to the next cycle.
Laboratory Tests—Patients receiving Gemzar should be monitored prior to each dose with a completeblood count (CBC), including differential and platelet count. Suspension or modification of therapy shouldbe considered when marrow suppression is detected (see DOSAGE AND ADMINISTRATION in the fullPrescribing Information).
Laboratory evaluation of renal and hepatic function should be performed prior to initiation of therapyand periodically thereafter (see WARNINGS).
Carcinogenesis, Mutagenesis, Impairment of Fertility—Long-term animal studies to evaluate thecarcinogenic potential of Gemzar have not been conducted. Gemcitabine induced forward mutations invitro in a mouse lymphoma (L5178Y) assay and was clastogenic in an in vivo mouse micronucleus assay.Gemcitabine was negative when tested using the Ames, in vivo sister chromatid exchange, and in vitrochromosomal aberration assays, and did not cause unscheduled DNA synthesis in vitro. Gemcitabine IP dosesoof 0.5 mg/kg/day (about 1/700 the human dose on a mg/m2 basis) in male mice had an effect on fertilitywith moderate to severe hypospermatogenesis, decreased fertility, and decreased implantations. In femalemice, fertility was not affected but maternal toxicities were observed at 1.5 mg/kg/day IV (about 1/200 thehuman dose on a mg/m2 basis) and fetotoxicity or embryolethality was observed at 0.25 mg/kg/day IV(about 1/1300 the human dose on a mg/m2 basis).
Pregnancy—Category D. See WARNINGS.Nursing Mothers—It is not known whether Gemzar or its metabolites are excreted in human milk.
Because many drugs are excreted in human milk and because of the potential for serious adversereactions from Gemzar in nursing infants, the mother should be warned and a decision should be madewhether to discontinue nursing or to discontinue the drug, taking into account the importance of the drugto the mother and the potential risk to the infant.
Elderly Patients—Gemzar clearance is affected by age (see CLINICAL PHARMACOLOGY in the fullPrescribing Information). There is no evidence, however, that unusual dose adjustments (i.e., other thanthose already recommended in DOSAGE AND ADMINISTRATION section in the full Prescribing Information)are necessary in patients over 65, and in general, adverse reaction rates in the single-agent safety databaseof 979 patients were similar in patients above and below 65. Grade 3/4 thrombocytopenia was morecommon in the elderly.
Gender—Gemzar clearance is affected by gender (see CLINICAL PHARMACOLOGY in the full PrescribingInformation). In the single-agent safety database (N=979 patients), however, there is no evidence thatunusual dose adjustments (i.e., other than those already recommended in DOSAGE AND ADMINISTRATIONsection in the full Prescribing Information) are necessary in women. In general, in single-agent studies of Gemzar, adverse reaction rates were similar in men and women, but women, especially older women,were more likely not to proceed to a subsequent cycle and to experience Grade 3/4 neutropenia andthrombocytopenia.
Pediatric Patients—The effectiveness of Gemzar in pediatric patients has not been demonstrated. Gemzarwas evaluated in a Phase 1 trial in pediatric patients with refractory leukemia and determined that themaximum tolerated dose was 10 mg/m2/min for 360 minutes three times weekly followed by a one-weekrest period. Gemzar was also evaluated in a Phase 2 trial in patients with relapsed acute lymphoblasticleukemia (22 patients) and acute myelogenous leukemia (10 patients) using 10 mg/m2/min for 360 minutesthree times weekly followed by a one week rest period. Toxicities observed included bone marrow suppression,febrile neutropenia, elevation of serum transaminases, nausea, and rash/desquamation, which were similarto those reported in adults. No meaningful clinical activity was observed in this Phase 2 trial.
Patients with Renal or Hepatic Impairment—Gemzar should be used with caution in patients withpreexisting renal impairment or hepatic insufficiency as there is insufficient information from clinicalstudies to allow clear dose recommendation for these patient populations. Administration of Gemzar inpatients with concurrent liver metastases or a preexisting medical history of hepatitis, alcoholism, or livercirrhosis may lead to exacerbation of the underlying hepatic insufficiency.
Drug Interactions—No specific drug interaction studies have been conducted. For information onthe pharmacokinetics of Gemzar and cisplatin in combination, see Drug Interactions under CLINICALPHARMACOLOGY.
Radiation Therapy—A pattern of tissue injury typically associated with radiation toxicity has beenreported in association with concurrent and non-concurrent use of Gemzar.
Non-concurrent (given >7 days apart)—Analysis of the data does not indicate enhanced toxicity whenGemzar is administered more than 7 days before or after radiation, other than radiation recall. Datasuggest that Gemzar can be started after the acute effects of radiation have resolved or at least one weekafter radiation.
Concurrent (given together or ≤7 days apart)—Preclinical and clinical studies have shown that Gemzarhas radiosensitizing activity. Toxicity associated with this multimodality therapy is dependent on manydifferent factors, including dose of Gemzar, frequency of Gemzar administration, dose of radiation,radiotherapy planning technique, the target tissue, and target volume. In a single trial, where Gemzar at adose of 1000 mg/m2 was administered concurrently for up to 6 consecutive weeks with therapeutic thoracicradiation to patients with non-small cell lung cancer, significant toxicity in the form of severe, andpotentially life-threatening mucositis, especially esophagitis and pneumonitis was observed, particularly inpatients receiving large volumes of radiotherapy [median treatment volumes 4795 cm3]. Subsequent studieshave been reported and suggest that Gemzar administered at lower doses with concurrent radiotherapyhas predictable and less severe toxicity. However, the optimum regimen for safe administration of Gemzarwith therapeutic doses of radiation has not yet been determined in all tumor types.
ADVERSE REACTIONS: Combination Use in Ovarian Cancer—In the Gemzar plus carboplatin versuscarboplatin study, dose reductions occurred with 10.4% of Gemzar injections and 1.8% of carboplatininjections on the combination arm, versus 3.8% on the carboplatin alone arm. On the combination arm,13.7% of Gemzar doses were omitted and 0.2% of carboplatin doses were omitted, compared to 0% ofcarboplatin doses on the carboplatin alone arm. There were no differences in discontinuations due toadverse events between arms (10.9% versus 9.8%, respectively).
Table 1 presents the adverse events (all grades) occurring in ≥10% of patients in the ovarian cancer study.
In addition to blood product transfusions as listed in Table 1, myelosuppression was also managed withhematopoetic agents. These agents were administered more frequently with combination therapy thanwith monotherapy (granulocyte growth factors: 23.6% and 10.1%, respectively; erythropoetic agents:7.3% and 3.9%, respectively).
The following are the clinically relevant adverse events, regardless of causality, that occurred in >1% and<10% (all grades) of patients on either arm. In parentheses are the incidences of Grade 3 and 4 adverseevents (Gemzar plus carboplatin versus carboplatin): AST or ALT elevation (0 versus 1.2%), dyspnea(3.4% versus 2.9%), febrile neutropenia (1.1% versus 0), hemorrhagic event (2.3% versus 1.1%),hypersensitivity reaction (2.3% versus 2.9%), motor neuropathy (1.1% versus 0.6%), and rash/desquamation(0.6% versus 0).
No differences in the incidence of laboratory and non-laboratory events were observed in patients65 years or older, as compared to patients younger than 65.
Post-marketing experience—The following adverse events have been identified during post-approvaluse of Gemzar. These events have occurred after Gemzar single-agent use and Gemzar in combination withother cytotoxic agents. Decisions to include these events are based on the seriousness of the event,frequency of reporting, or potential causal connection to Gemzar.
Cardiovascular—Congestive heart failure and myocardial infarction have been reported very rarely withthe use of Gemzar. Arrhythmias, predominantly supraventricular in nature, have been reported very rarely.
Vascular Disorders—Clinical signs of peripheral vasculitis and gangrene have been reported very rarely.Skin—Cellulitis and non-serious injection site reactions in the absence of extravasation have been rarely
reported. Severe skin reactions, including desquamation and bullous skin eruptions, have been reportedvery rarely.
Hepatic—Increased liver function tests including elevations in aspartate aminotransferase (AST),alanine aminotransferase (ALT), gamma-glutamyl transferase (GGT), alkaline phosphatase, and bilirubinlevels have been reported rarely. Serious hepatotoxicity including liver failure and death has been reportedvery rarely in patients receiving Gemzar alone or in combination with other potentially hepatotoxic drugs.
Pulmonary—Parenchymal toxicity, including interstitial pneumonitis, pulmonary fibrosis, pulmonaryedema, and adult respiratory distress syndrome (ARDS), has been reported rarely following one or moredoses of Gemzar administered to patients with various malignancies. Some patients experienced the onsetof pulmonary symptoms up to 2 weeks after the last Gemzar dose. Respiratory failure and death occurredvery rarely in some patients despite discontinuation of therapy.
Renal—Hemolytic-Uremic Syndrome (HUS) and/or renal failure have been reported following one ormore doses of Gemzar. Renal failure leading to death or requiring dialysis, despite discontinuation oftherapy, has been rarely reported. The majority of the cases of renal failure leading to death were due to HUS.
Injury, Poisoning, and Procedural Complications — Radiation recall reactions have been reported (seeRadiation Therapy under PRECAUTIONS).
Dosage and administration: Gemzar is for intravenous use only. Please consult full prescribing informationfor complete dosage and administration guidelines.
Literature revised May 7, 2007
PV 4067 AMP PRINTED IN USA
Eli Lilly and CompanyIndianapolis, IN 46285, USA
Copyright © 1996, 2007, Eli Lilly and Company. All rights reserved.
GEMZAR� (GEMCITABINE HCl) FOR INJECTION PV 4067 AMP GEMZAR� (GEMCITABINE HCl) FOR INJECTION PV 4067 AMP
CTC Grades (% incidence)Gemzar plus Carboplatin (N=175) Carboplatin (N=174)All Grades Grade 3 Grade 4 All Grades Grade 3 Grade 4
Laboratoryb
HematologicNeutropenia 90 42 29 58 11 1Anemia 86 22 6 75 9 2Leukopenia 86 48 5 70 6 <1Thrombocytopenia 78 30 5 57 10 1RBC Transfusionsc 38 15Platelet Transfusionsc 9 3
Non-laboratoryb
Nausea 69 6 0 61 3 0Alopecia 49 0 0 17 0 0Vomiting 46 6 0 36 2 <1Constipation 42 6 1 37 3 0Fatigue 40 3 <1 32 5 0Neuropathy-sensory 29 1 0 27 2 0Diarrhea 25 3 0 14 <1 0Stomatitis/pharyngitis 22 <1 0 13 0 0Anorexia 16 1 0 13 0 0
a Grade based on Common Toxicity Criteria (CTC) Version 2.0 (all grades ≥10%).b Regardless of causality.c Percent of patients receiving transfusions. Transfusions are not CTC-graded events. Blood transfusionsincluded both packed red blood cells and whole blood.
Table 1: Adverse Events From Comparative Trial of GemzarPlus Carboplatin Versus Single-Agent Carboplatin in Ovarian Cancera
38358_elonps_ov1p_con7_fa.indd 2 7/7/09 2:09:07 PM

1
Treatment Options for Platinum-Sensitive
Recurrent Ovarian CancerBRADLEY J. MONK, MD
Associate ProfessorDivision of Gynecologic Oncology
Department of Obstetrics and GynecologyChao Family Comprehensive Cancer Center
University of California, IrvineOrange, California
For almost 2 decades, the
traditional management of
women with recurrent epithelial
ovarian cancer has dichotomized
therapeutic recommendations based
on the platinum-free interval (PFI)
and the probability of response
to platinum retreatment.
These recommendations have defined much of the current clinical “standard of care” for these patients. It also has formed the basis for a research agenda, which, until recently, has explored nonplatinum agents in women considered at low probability for response to platinum retreatment, and platinum-based therapy in those with a higher probability of response. This paradigm is now in question as Phase III trials investigate newer agents and unique combinations. This monograph reviews the historical development of these contemporary practice patterns and suggests alternative strategies that may further improve efficacy among women with “platinum-sensitive” relapsed ovarian cancer.
The Concept of “Platinum Sensitivity”In the late 1980s and early 1990s, Blackledge,1 Gore,2
and Markman3 reported on the increasing success of retreating recurrent epithelial ovarian cancer with plat-inum compounds based on the length of the PFI; the response rate (RR) to platinum retreatment approached 60% as the PFI reached 2 years and beyond (Table 1).
These findings became the foundation for the current
paradigm of treating relapsed ovarian cancer with a sec-ond platinum-based regimen if the PFI was longer than 6 months. This was largely reinforced by the Gynecologic Oncology Group (GOG), which evaluated serial nonplat-inum agents in successive clinical studies of women with recurrent measurable disease who had recurred in 6 months or less.4
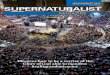
Blackledge, Gore, and Markman made their observa-tions before active nonplatinum drugs had been iden-tified or well studied (circa 1990). In 1992, the FDA approved paclitaxel as a new chemical entity for patients with metastatic carcinoma of the ovary after failure of first-line or subsequent therapy. Data from 5 noncon-trolled Phase I and II studies led to the regular approval of this compound based on durable RRs between 20% and 30% in both platinum-resistant (PFI <6 months) and platinum-sensitive (PFI >6 months) patients.5,6 It is now well appreciated that PFI is prognostic to the expected RR and duration of response (Figure 1).7
This effect appears to be somewhat linear, and it may be independent of specific chemotherapeutic agents, including platinum compounds. It is important to com-pare agents in formal Phase III trials rather than making
INDEPEND ENT LY DEVELOPED BY MCMAHON PUBL ISHING CL IN ICAL ONCOLOGY NEWS • JULY/AUGUST 2009
PRINTER-FRIENDLY VERSION AT CLINICALONCOLOGY.COM

INDEPENDENT LY DEVELOPED BY MCMAHON PUBL ISHING2
inferences from cross-trial assessments. One randomized trial has assessed the impact of plati-
num versus nonplatinum treatment in women with recur-rent ovarian cancer.8 This Phase II crossover trial between single-agent paclitaxel and the platinum triplet, cyclo-phosphamide, doxorubicin, and cisplatin (CAP), demon-strated that RRs were higher in those receiving CAP than in those receiving paclitaxel. All patients were platinum-sensitive using a PFI greater than 12 months. Although the generalizability of these results is limited by the study’s
small sample size, Phase II design, and nearly 50% “drop-out” at crossover, this trial has been cited as support that platinum should be considered first in women with plat-inum-sensitive recurrent cancer.9
The New Era of Novel AgentsBeginning in the mid-1990s, the development of new
compounds provided alternative mechanisms of action to the platinum and taxane portfolio. Positive results in 2 trials in recurrent ovarian cancer and 3 positive trials in platinum-sensitive recurrent ovarian cancer led to adjust-ment of the traditional treatment algorithm. The first was a challenge to single-agent platinum or paclitaxel in patients (“resistant” and “sensitive”) failing one regimen. ten Bokkel Huinink et al compared paclitaxel to topote-can (Hycamtin, GlaxoSmithKline) in relapsed disease and suggested that topotecan had efficacy at least equiva-lent to that of paclitaxel, as manifested by a higher RR and significantly longer time to progression.10 Not only did this trial include patients with platinum-resistant dis-ease, but it also used a nonplatinum drug to treat women with a PFI greater than 6 months; in this study, topotecan resulted in an increase in RR with longer PFIs that was similar to the increase Blackledge,1 Gore,2 and Markman3 observed when they retreated with platinum compounds (Table 1). This study was not persuasive enough to con-vince most clinicians to use nonplatinum compounds in platinum-sensitive patients, but it did lead to the 1996 regulatory approval of topotecan in the United States.
Gordon et al reported a second positive Phase III trial comparing topotecan with pegylated liposomal dox-orubicin (PLD; Doxil, Ortho Biotech), which led to the accelerated FDA approval of PLD in 1999 and full FDA approval in 2005.11 This trial also was performed in a mixed population of both platinum-sensitive and plati-num-resistant patients and, like the ten Bokkel Huinink trial, showed a greater RR as the PFI increased (Table 1). The FDA recognized this by not restricting the label
Table 1. Effect of Platinum-free Interval on Second-Line Response
Platinum-free Interval, mo
Response Rate in Trials, %
Platinum TherapyNon-platinum Therapy
19891a 19902 19913 199710 200111
0-6 10 17 — 10-16.7 12
7-12 29 27b 12.5-20 28
13-18 63 27 33 20-28.8
19-24 94
>24 57 59
a First-line therapy included platinum agents and other agents in Phase II investigation
b Platinum-free interval 5 to 12 months
Figure 2. OVA-301: study schema.
PLD, pegylated liposomal doxorubicina Premedication with dexamethasone is required.
Based on reference 14.
PLD 50 mg/m2 90-min infusion every 4 wk
PLD 30 mg/m2 90-min infusion followed by trabectedina 1.1 mg/m2 3-h infusion every 3 wk
RANDOMIZATION
Inclusion criteria:
Ovarian cancer•
Fallopian tube • cancer
Peritoneal • cancer
Measurable • disease
1 prior front-line • platinum-based regimen
1000
800
600
400
200
0
1.0
0.8
0.6
0.4
0.2
0
Days
Platinum-Resistant Platinum-Sensitive
Pe
rce
nt
Figure 1. Line and bar graphs showing the linear relationship between PFS, OS and RR, and PFI.
OS, overall survival; PD, progressive disease; PFI, platinum-free interval; PFS, progression-free survival; RR, response rate
Based on reference 6.
0-3 mo Pro-
gression
0-3 mo Non-PD
3-12 mo
12-18 mo
18+ mo
PFS, d 90 176 174 275 339
OS, d 217 375 393 657 957
RR, % 0.09 0.24 0.35 0.52 0.62

INDEPENDENTLY DEVELOPED BY MCMAHON PUBL ISHING 3
to use in platinum-resistant patients, but few clinicians use PLD over a platinum compound if the PFI is greater than 6 months. Perhaps this is because of the emerging evidence that doublets are superior to single agents in treating platinum-sensitive patients.
ICON 4 (International Collaborative Ovarian Neo-plasm 4) was the first trial to definitively show that platinum doublets (in this case with paclitaxel) were more effective than single-agent platinum compounds when the PFI was longer than 6 months.12 This obser-vation that doublets are superior to single agents was confirmed by an intergroup trial of the Arbeitsgemein-schaft Gynaekologische Onkologie-OVAR, the National Cancer Institute of Canada Clinical Trials Group, and the European Organisation for Research and Treatment of Cancer Gynecologic Cancer Group, leading to the FDA approval of gemcitabine (Gemzar, Eli Lilly) plus carbo-platin in platinum-sensitive second-line ovarian cancer in 2006.13
However, the “addiction” to platinum in this set-ting has been called into question based on the most recent positive Phase III trial in recurrent ovarian cancer, which compared PLD with PLD plus trabectedin (Yon-delis, Centocor Ortho Biotech; Figure 2).14 This is the first randomized Phase III trial in relapsed ovarian cancer to include a nonplatinum doublet. It is not surprising that this study, like the Gordon and the ten Bokkel Huinink studies, showed increasing activity with increasing PFI (Table 2).
[Editor’s Note: On July 15, the FDA’s Oncology Drugs Advisory Committee (ODAC) recommended that the combination of tra-bectedin administered with doxorubicin HCI liposome injection not be approved because it did not provide a sufficient benefit-risk profile for the treatment of relapsed ovarian cancer. However, the FDA is not bound by the ODAC’s recommendation. Centocor Ortho Biotech has stated that they are continuing trials with the drug and are working to address the concerns that were raised. Look for in-depth coverage of the ODAC meeting in an upcoming issue and at clinicaloncology.com.]
Perhaps more acceptable alternatives to paclitaxel plus carboplatin in treating platinum-sensitive relapsed ovarian cancer are gemcitabine plus carboplatin and PLD plus carboplatin because only paclitaxel is replaced in these regimens. Gemcitabine plus carboplatin is being studied in the Phase III OCEANS (Ovarian Cancer Evalu-ation of Avastin and Safety) trial.15 The date for final data collection for the primary outcome measure of progres-sion-free survival is June 2010. PLD plus carboplatin is being studied in the CALYPSO (CAELYX in Platinum Sen-sitive Ovarian Patients) study (Figure 3).16 Preliminary results of this trial, the largest in relapsed ovarian can-cer, showed superiority of the PLD-carboplatin combina-tion in terms of progression-free survival (median after 824 events, 11.3 vs 9.4 months; hazard ratio, 0.821; 95% confidence interval, 0.72-0.94; P=0.005) (Table 2). Com-pared with paclitaxel-carboplatin, PLD-carboplatin was well tolerated, with lower rates of severe and long-lasting (neuropathy) toxicities, but thrombocytopenia and skin reactions occurred at higher rates in the PLD group.
Replacing Paclitaxel, Carboplatin, or Both The question of whether nonplatinum doublets can be
used in preference to the commonly used platinum dou-blets of carboplatin plus paclitaxel or carboplatin plus gemcitabine remains unanswered because Phase III tri-als comparing PLD plus trabectedin or other active non-platinum doublets versus platinum doublets are lacking. However, the level of activity of the PLD plus trabectedin doublet suggests that it is an acceptable alternative in treating platinum-sensitive ovarian cancer (Table 2). This combination is especially appealing because, like gem-citabine-carboplatin,13 it is not associated with adverse effects of paclitaxel (bone pain, neuropathy, and alope-cia) or carboplatin (risk for allergy).14 However, PLD plus trabectedin is associated with more bone marrow sup-pression and gastrointestinal toxicity compared with PLD
Table 2. Platinum-Sensitive Recurrent OC: Positive Trials in Perspective
Study Treatment NPrior Taxane
% PFI >12 Mo
Measurable DiseaseRequired RR,a % PFS, mo OS, mo
Gordon11 PLD 123 NS NS Measurable 28 6.6 24.7
Parmar12 Carboplatin + paclitaxel
392 43 77 Italy (not MRC CTU or AGO)
66 12b 29
Pfisterer13 Carboplatin + gemcitabine
178 70 60 SWOG (measurable or assessable)
47 8.8b 18
Monk14 PLD + trabectedin
218 80 44 RECIST 47 9.2b 20.5 (not mature)
Pujade-Lauraine16
Carboplatin + PLD
466 99 65 RECIST or CA125 NA 11.3b (not mature)
AGO, Arbeitsgemeinschaft Gynaekologische Onkologie; CA125, cancer antigen 125; MRC CTU, Medical Research Council Clinical Trials Unit; OC, ovarian cancer; OS, overall survival; PFI, platinum-free interval; PFS, progression-free survival; PLD, pegylated liposomal doxorubicin; RECIST, Response Evaluation Criteria In Solid Tumors; RR, response rate; SWOG, Southwestern Oncology Groupa By independent radiologist; b By investigator

INDEPENDENT LY DEVELOPED BY MCMAHON PUBL ISHING4
alone,11,14 similar to how carboplatin plus gemcitabine is associated with more toxicity than single-agent carbo-platin.13 On the other hand, the dose of PLD (30 mg/m2 every 3 weeks) used with trabectedin is less intensive than the single-agent dose of PLD (50 mg/m2 every 4 weeks) and is associated with less skin toxicity (stomatitis and hand–foot syndrome).14 The preferential use of PLD-carboplatin over paclitaxel-carboplatin is easier to eval-uate given the recently reported CALYPSO study above. However, PLD-carboplatin has not been compared with gemcitabine-carboplatin.
Future Developments The future will likely involve the addition of bevaci-
zumab (Avastin, Genentech)15,17 and/or other targeted agents18 to chemotherapy, including nonplatinum doublets, in this setting. As the use of maintenance and consolidation chemotherapy increases, the inci-dence of clinically evident recurrent disease will likely increase, making the term platinum-free interval pref-erable to treatment-free interval because the activity of retreatment with platinum or even a nonplatinum agent most likely will depend on when the patient completed front-line platinum-based therapy. Addi-tionally, because some front-line Phase III trials are employing non–taxane-based platinum doublets, it is likely that future trials also may need to consider tax-ane naïvete when making treatment decisions.19 Fur-thermore, because other agents, such as topotecan, bevacizumab, PLD, and trabectedin have shown clear activity in women with platinum-sensitive disease, it may be that the term chemotherapy-sensitive disease
is the most appropriate characterization for patients who experience a relapse after 6 months.
References
Blackledge G, Lawton F, Redman C, Kelly K. Response of patients 1. in phase II studies of chemotherapy in ovarian cancer: implications for patient treatment and the design of phase II trials. Br J Cancer. 1989;59(4):650-653, PMID: 2713253.
Gore ME, Fryatt I, Wiltshaw E, Dawson T. Treatment of relapsed car-2. cinoma of the ovary with cisplatin or carboplatin following initial treatment with these compounds. Gynecol Oncol. 1990;36(2):207-211, PMID: 2404837.
Markman M, Rothman R, Hakes T, et al. Second-line platinum therapy 3. in patients with ovarian cancer previously treated with cisplatin. J Clin Oncol. 1991;9(3):389-393, PMID: 1999708.
Bookman MA. Developmental chemotherapy and management of 4. recurrent ovarian cancer. J. Clin Oncol. 2003;21(10 suppl):149s-167s, PMID: 17633784.
Trimble EL, Adams JD, Vena D, et al. Paclitaxel for platinum-refrac-5. tory ovarian cancer: results from the first 1,000 patients registered to National Cancer Institute Treatment Referral Center 9103. J Clin Oncol. 1993;11(12):2405-2410, PMID: 7902426.
Ozols RF. USA update on paclitaxel in ovarian cancer. 6. Ann Med. 1995;27(1):127-130, PMID: 7741991.
Pujade-Lauraine E, Paraiso D, Cure H, et al. Predicting the effective-7. ness of chemotherapy (Cx) in patients with recurrent ovarian cancer (ROC): a GINECO study. J Clin Oncol. 2002;21: abstract 829.
Cantù MG, Buda A, Parma G, et al. Randomized controlled trial of 8. single-agent paclitaxel versus cyclophosphamide, doxorubicin, and cisplatin in patients with recurrent ovarian cancer who responded to first-line platinum-based regimens. J Clin Oncol. 2002;20(5):1232-1237, PMID: 11870165.
Cannistra SA. Is there a “best” choice of second-line agent in the 9. treatment of recurrent, potentially platinum-sensitive ovarian cancer? J Clin Oncol. 2002;20(5):1158-1160, PMID: 11870154.
ten Bokkel Huinink W, Gore M, Carmichael J, et al. Topotecan versus 10. paclitaxel for the treatment of recurrent epithelial ovarian cancer. J Clin Oncol. 1997;15(6):2183-2193, PMID: 9196130.
Gordon AN, Fleagle JT, Guthrie D, Parkin DE, Gore ME, Lacave AJ. 11. Recurrent epithelial ovarian carcinoma: a randomized phase III study of pegylated liposomal doxorubicin versus topotecan. J Clin Oncol. 2001;19(14):3312-3322, PMID: 11454878.
Parmar MK, Ledermann JA, Colombo N, et al. Paclitaxel plus plat-12. inum-based chemotherapy versus conventional platinum-based chemotherapy in women with relapsed ovarian cancer: the ICON4/AGO-OVAR-2.2 trial. Lancet. 2003;361(9375):2099-2106, PMID: 12826431.
Pfisterer J, Plante M, Vergote I, et al. Gemcitabine plus carboplatin 13. compared with carboplatin in patients with platinum-sensitive recur-rent ovarian cancer: an intergroup trial of the AGO-OVAR, the NCIC CTG, and the EORTC GCG. J Clin Oncol. 2006;24(29):4699-4707, PMID: 16966687.
Monk BJ, Herzog T, Kaye S, et al. A randomized phase III study of 14. trabectedin with pegylated liposomal doxorubicin versus PLD in relapsed, recurrent ovarian cancer. In: Proceedings of the 33rd annual meeting of the European Society of Medical Oncology, Stockholm, Sweden, 2008; abstract LBA3.
Ovarian Cancer Evaluation of Avastin and Safety: ClinicalTrials.gov 15. Identifier: NCT00434642.
Pujade-Lauraine E, Mahner S, Kaern J, et al. A randomized, phase III 16. study of carboplatin and pegylated liposomal doxorubicin versus car-boplatin and paclitaxel in relapsed platinum-sensitive ovarian cancer (OC): CALYPSO study of the Gynecologic Cancer Intergroup (GCIG). J Clin Oncol. 2009;27(18 suppl); abstract LBA5509.
Fallopian Tube Cancer. Gynecologic Oncology Group Protocol 213: 17. ClinicalTrials.gov Identifier: NCT00565851.
ICON6. ClinicalTrials.gov Identifier: NCT00544973.18.
Pignata G, Scambia A, Savarese R, et al. Carboplatin plus paclitaxel 19. (CP) versus carboplatin plus stealth liposomal doxorubicin (CLD) in patients with advanced ovarian cancer (AOC): activity and safety results of the MITO-2 randomized multicenter trial. J Clin Oncol. 2009;27(15 suppl); abstract LBA5508.
Figure 3. CALYPSO: study schema.
AUC, area under the curve; CALYPSO, CAELYX in Platinum Sensitive Ovarian Patients; CD, carboplatin plus PLD; CP, carboplatin and paclitaxel; PLD, pegylated liposomal doxorubicina or on progression Based on reference 16.
Experimental arm: CD
PLD 30 mg/m2 IV day 1 and carboplatin AUC 5 day 1, every 28 d for 6 coursesa
Control arm: CP
Paclitaxel 175 mg/m2 day 1 and carboplatin AUC 5 day 1, for 21 d for 6 coursesa
RANDOMIZATION
Inclusion criteria:
Ovarian cancer • in late relapse (>6 mo) after first- or second-line platinum-based therapy (previous taxane required)
Stratification:
Therapy-free • interval (6-12 mo vs >12 mo)
Measurable dis-• ease (yes vs no)
Treating center•
Randomization•

CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 9
predicted Merrill J. Egorin, MD, professor of medi-cine and pharmacology, University of Pittsburgh Can-cer Institute, in Pittsburgh. He was not involved in any of the studies.
As a member of the PARP (poly [ADP-ribose] poly-merase) family, which includes at least 17 proteins, PARP-1 is particularly promising as a target because
of its role in DNA repair. The hypothe-sis, now substantiated by results from clinical trials, is that inhibition of PARP-1 can greatly potentiate the activ-ity of conventional cytotoxic agents in malignancies where inhibiting DNA repair is likely to be impor-tant. The considerable interest in PARP-1 inhibition, despite the fact that support so far is limited to Phase II data, is driven by the level of activity.
Success in Triple-Neg-ative Breast Cancer
In the larger of the two studies in patients with metastatic triple-negative breast cancer, the surviv-al advantage of adding the PARP-1 inhibitor BSI-201 (BiPar Scienc-es) to a combination of gemcitabine (Gemzar, Eli Lilly) and carboplatin versus the cytotoxic agents alone was 9.2 months compared with 5.7 months (hazard ratio [HR], 0.348; 95% confidence interval [CI], 0.19-0.65; P=0.0005). Joyce O’Shaughnessy, MD, director of the Breast Cancer Prevention Program at Baylor-Charles A. Sammons Cancer Center in Dallas, presented these data on behalf of the U.S. Oncology Group at the ASCO annual meeting (abstract 3).
In the initial analysis of 116 randomized patients, other outcomes measured also showed improve-ment with the addition of the PARP drug, includ-ing objective response rate (ORR; 48% vs. 16%), pro-gression-free survival (PFS; 6.9 vs. 3.3 months; HR, 0.342; P<0.0001) and clinical benefit rate (ORR plus stable disease; 62% vs. 21%; P=0.0002). Also encour-aging, Dr. O’Shaughnessy reported that there were no significant differences between the study arms for either hematologic or nonhematologic adverse events. The addition of BSI-201 did not lead to any dose reductions in chemotherapy.
The final data from this study are expected at the end of 2009. At that time, information will be made available on patients who were initially randomized to the chemotherapies alone but crossed over to che-motherapy plus BSI-201 at the time of progression. In the treatment protocols, all patients received gem-citabine (1,000 mg/m2) and carboplatin (area under the curve = 2) on days 1 and 8 of a 21-day cycle. For patients who received the PARP-1 inhibitor, the dose was 5.6 mg/kg on days 1, 4, 8 and 11. The median age of the study population was about 55 years. Approx-imately 60% of the patients received the PARP-1 inhibitor as first-line therapy, while the remaining were treated as second- or third-line.
BRCA-Linked Breast Cancer and Ovarian Cancer
Similar promise was demonstrated in a much small-er study of 54 patients with BRCA-deficient advanced breast cancer treated with the oral PARP-1 inhibitor, olaparib (AstraZeneca) (ASCO abstract CRA501). Two doses, 400 and 100 mg, both given twice dai-ly, were evaluated without a control arm. All patients were treatment-experienced. The median number of previous regimens was three. Most patients had received a taxane or an anthracycline or both, and
about 30% had been previously exposed to a plati-num-containing agent. Although almost 70% demon-strated BRCA1 deficiency, a substantial minority had a BRCA2 deficiency, and one patient had both.
Despite advanced disease and substantial exposure to previous regimens, 41% of those on the higher dose and 22% on the lower dose had an objective response. In the higher-dose arm, 4% of these were complete responses. The PFS in the higher-dose arm was 5.7 months (3.8 months for the lower dose), which is highly encouraging for a population with very limit-ed treatment options.
“This is the first report of a Phase II study employ-ing a PARP-1 inhibitor to target BRCA1- and BRCA2-deficient advanced breast cancer. It provides a proof of concept of the activity and tolerability for PARP-1 as a target of treatment,” said senior author Andrew Tutt, MD, Breakthrough Breast Cancer Research Unit, Kings College, London School of Medicine. He noted that the results were consistent with a second, similar multicenter study in BRCA-deficient, chemo-therapy-refractory ovarian cancer that was conduct-ed by many of the same investigators. In that series of 57 patients, the ORR was 33%.
The activity in these Phase II studies, which is consistent with the promise of PARP-1 inhibition in experimental studies, may just be the beginning success stories in a very promising path of clin-ical research. For example, it is conceivable that PARP-1 inhibition might prevent cancer in patients with inherited BRCA1 or BRCA2 mutations. It may also be possible to inhibit other PARPs important to cell survival.
Dr. Egorin said that the activity seen in these stud-ies is particularly promising at a stage when several key variables that might affect activity, particularly the optimal timing of PARP-1 inhibition in relation to cytotoxic effects, remains incompletely understood. A greater understanding of this area may lead to even more efficacious use of drugs that act on this target.
—Ted Bosworth
SOLID TUMORS
Breast
PARPcontinued from page 1 �
‘[PARP inhibition] is an area that will explode in the next year or two.’
—Merrill J. Egorin, MD
15
12
9
6
3
0
Pro
gre
ssio
n-f
ree
Su
rviv
al, m
o
9.2
5.7
Gemcitabine + Carboplatin (GC)
GC + PARP-1 inhibitor BSI-201
5.7
Figure 1. Comparison of treatments for metastatic triple-negative breast cancers.
100 mg olaparib (PARP-1 inhibitor)
400 mg olaparib (PARP-1 inhibitor)50
40
30
20
10
0
Ob
jecti
ve
Re
spo
nse
Rate
, %
41
22
Figure 2. PARP-1 inhibitors for BRCA-deficient advanced breast cancer.
Poly (ADP-ribose) polymerase family, member 1

The National Cancer Coalition (NCC) recently announced its Angel Grant recipients. The NCC implemented the Angel Grant program to provide seed funding to innovative projects that ben-efit and further cancer research, edu-cation and programs. Grants also are awarded to act as a catalyst for scientists to secure additional funding from U.S. government agencies and other sources.
Steven S. Brem, MD, is the director of neurosurgery and the division chief of the Neuro-Oncol-ogy Department at H. Lee Moffitt Cancer Center in Tampa. He will use the Angel Grant to pursue the devel-opment of new ant i-angiogenic therapies for pedi-atric brain tumors. Dr. Brem is a mem-ber of the Scientific Advisory Board of the American Brain Tumor Association and the Florida Brain Tumor Association and is vice president of the U.S. Central Brain Tumor Registry. He has served on
several national committees and Nation-al Institutes of Health (NIH) review panels. He is chairman of the National Comprehensive Cancer Centers Neuro-Oncology Guideline Committee.
Julie Blatt, MD, is chief of pediatric hematology/oncology at the Universi-ty of North Caroli-na (UNC) at Cha-pel Hill. Her award furthered UNC’s study demonstrat-ing no overall link between autism and cancer in chil-dren, as well as a teaching program for childhood can-cer survivors and health care providers. Dr. Blatt is a consultant to the Childhood Cancer Survivor Study, a multicenter NIH-funded study that is examining late effects in more than 20,000 survivors of childhood cancer. She also is a past mem-ber of the Strategy Group of the Surveil-lance and End Results Committee of the Children’s Oncology Group, which gen-erates late effects study components of therapeutic trials.
J e f f r e y W. T a u b , M D , i s t h e d i re c t o r o f t h e He m a t o l o -gy/Oncology Fel-lowship program at the Children’s Hospital of Mich-igan, Detroit. Dr. Taub plans to use the grant to pro-vide a new visi-ble wavelength microplate reader, which is integral to his innovative research and treatment of acute leukemias. Dr. Taub’s primary research focus, funded by the National Cancer Institute and the Leukemia and Lymphoma Society, is the mechanism of chemotherapy sensitivity in children with Down syndrome who have acute myeloid leukemia (AML), drug resis-tance in childhood acute lymphoblas-tic leukemia and AML, and the molecu-lar epidemiology of childhood leukemia. Dr. Taub has won numerous awards including Scholar in Clinical Research (2002-2007) from the Leukemia and Lymphoma Society and the 1994 Young
Investigator Award from the American Society of Clinical Oncology.
Eric C. Beyer, MD, PhD, is the chief of pediatric hema-tology/oncology at the University of Chicago’s Com-er Children’s Hos-pital. The Angel Grant will be used to further his investigations of the biology of pedi-atric glioblastoma multiforme brain tumors and their treatment. Dr. Bey-er heads an internationally recognized molecular and cellular biology labora-tory funded through grants awarded by the NIH and other government and private agencies. He and his colleagues are investigating the process of inter-cellular communication, specifically the direct exchange of ions and small molecules between cells through chan-nels formed of proteins called connex-ins. Their studies of this process may lead to new pharmacologic or molec-ular approaches to cancer therapy by manipulating exchange of drugs and drug metabolites between cells and the growth and viability of blood vessels. These studies also have major implica-tions for other clinical areas, including cardiac arrhythmias and cataracts.
Around the Water CoolerThis new section will bring you news about people and places in the field of oncology. If you have news to share (a new job, an award, a cancer center closure or expansion, etc), please send information to [email protected].
Nearly half of U.S. hospitals have reported no instances of disciplinary action against their physicians, despite a 17-year-old law requiring them to make disclosures, according to the report by the advocacy group Public Citizen.
Public Citizen claims that hospitals use loopholes to evade the spirit of the report-ing law, which mandates that the name of any doctor who has had his or her admit-ting privileges revoked or restricted for at least 30 days must be entered into the National Practitioner Data Bank.
The group said hospitals are plagued by “lax peer review, including a cul-ture among doctors of not wanting to ‘snitch’” on colleagues. Hospital admin-istrators also impose light penalties on transgressors, keeping sanctions under the threshold that would trigger a report or offering leaves of absence instead of suspensions, Public Citizen said.
Before launching the database, federal health officials projected that hospitals would submit 5,000 reports of privilege actions each year. “However, the aver-age number of hospital reports per year has been 650,” Public Citizen said in a
letter to Kathleen Sebelius, secretary of the Department of Health and Human Services. “As of December 2007, there was a total of only 11,221 such reports.”
“It is impossible to justify the fact that thousands of hospitals, which collec-tively have granted admitting privileges
to hundreds of thousands of doctors, have not reported a single discipline case in 17 years,” said Sidney Wolfe, MD, acting president of Public Citizen, in a statement. “Our report shows there is an urgent need for the Obama admin-istration to step in and hold hospital administrators accountable, as well as ensure that hospital medical staffs hold their own physicians accountable for patient safety.”
Failure to report disciplinary action against physicians prevents state med-ical boards from learning about such cases, creating the potential for harm to patients, the group said.
Public Citizen has called for changes to the Health Care Quality Improvement
Act of 1986, including imposing fines on hospitals that fail to report disciplinary actions against doctors. The group also would like the government to make com-pliance with the reporting law a compo-nent of hospital accreditation, as well as of participation in the Medicare program.
Elizabeth Lietz, a spokesperson for the American Hospital Association, dis-missed the Public Citizen report. “Hos-pitals, physicians and caregivers all work together to provide patients the right care in the right place at the right time and take seriously their respon-sibility for patient care,” Ms. Lietz said. “The premise that the number of reports received by the National Prac-titioner Data Bank correlates to jeopar-dized patient care is inaccurate.”
Reporting to the practitioner data bank is one of several disciplinary actions hospitals can take against phy-sicians, Ms. Lietz added. Others include requiring counseling and reporting offenders to state medical boards.
—Adam Marcus
Nearly Half of Hospitals Flunk Reporting Rule for Problem DocsThousands of hospitals in the United States may be shirking their responsibility to report cases of wrongdoing by physicians to a national data bank, a new report has found.
A CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 • DIGITAL EDITIONPEOPLE AND PLACES
‘It is impossible to justify the fact that thousands of hospitals, which collectively have granted admitting privileges to hundreds of thousands of doctors, have not reported a single discipline case in 17 years.’
—Sidney Wolfe, MD

Although most people cannot conceive of life without a stomach, those in the know understand that life and nourish-ment are in fact manageable without that major organ. The lifestyle changes may be inconvenient, but the alternative for people with the germline CDH1 (E-cad-herin) gene mutation is a very high risk for a very deadly cancer.
Prophylactic gastrectomy is “pret-ty much the standard recommendation for patients who have CDH1, if they’re healthy,” said Sam Yoon, MD, Division of Surgical Oncology, Massachusetts Gener-al Hospital and assistant professor of sur-gery, Harvard Medical School, Boston. Dr. Yoon performed the gastrectomies on the North Carolina family members.
The CDH1 mutation, which is thought to affect about 100 families worldwide,
was originally described among some Maori families in New Zealand. In peo-ple with CDH1, the risk for developing gastric cancer by the age of 80 is about 83% in women and about 67% in men. Women with CDH1 also have a high risk for lobular breast cancer.
Screening has proven fairly ineffective at identifying hereditary diffuse gastric cancer early enough to effectively treat the patient. “This diffuse-type gastric cancer often does not form a solid mass—it’s kind of an infiltrative tumor,” Dr. Yoon said. “The lesions start just underneath the visible mucosa. By the time screen-ing picks it up, it’s often lethal.”
The whole field of prophylactic sur-gery after genetic identification of hereditary cancer risk is on the rise, said Daniel Coit, MD, attending surgeon at
Memorial Sloan-Kettering Cancer Cen-ter (MSKCC), New York City, citing in particular thyroidectomy in patients with the RET mutation, which is a sure indi-cator the patient will develop medullary thyroid cancer.
“If you do a thyroidectomy in a child [with the RET gene mutation], you’ll find early signs of it. The BRCA1 gene is not as penetrant. Not 100% of people with a BRCA1 gene get breast cancer or ovarian cancer,” Dr. Coit said. “We believe that in CDH1-mutated patients, close to 90% will develop cancer if it is left untreated.”
It is unlikely, however, that awareness of CDH1 from publicity around the North Carolina family will result in a rush of concerned patients demanding prophy-lactic gastrectomies. Genetic counselors use fairly rigorous criteria to determine who is at inherent risk for this hereditary syndrome, Dr. Yoon explained.
“You’d have to have two or more cas-es of diffuse hereditary cancer in first- or second-degree relatives, with one case under age 50; or three family members of any age with diffuse gastric cancer,” Dr. Yoon said. Family members who meet
those criteria have a 30% to 50% chance of carrying the mutation.
Even if patients have genetic informa-tion about their cancer risk, the decision to undergo any type of prophylactic surgery is difficult, to say the least. “It’s extreme-ly gratifying to prevent cancer before it becomes incurable, but these are tough decisions for patients—whether to have it and when to get it,” Dr. Coit said. He listed the extensive team of medical profession-als any CDH1 patient will see at MSKCC for guidance in reaching a decision.
“I don’t want to belittle the loss of a thyroid or the loss of a breast, but there are reconstructive options that work toward restoration of quality of life after breast surgery; after thyroidectomy, replacement of the thyroid hormone is a pill that you take every day for the rest of your life,” Dr. Coit said. “But in gastrec-tomy patients, not only is there a risk for dying from the operation itself and from acute complications of it, there are also the long-term sequelae of it that patients need to adjust to, and that’s a big issue.”
—Monica J. Smith
The American Society of Clinical Oncology (ASCO) has commissioned
a new study to investigate how nonphy-sician practitioners, such as nurse prac-titioners (NPs) and physician assistants (PAs), can be used to address projected future oncology workforce shortages.
According to a 2007 ASCO workforce study, demands for oncology visits will increase 48% by 2020 and there will be a shortage of 4,000 oncologists. A recent study in the Journal of Clinical Oncology revealed that over the next 20 years, the number of new cancer cases diagnosed
annually in the United States will increase by 45% (2009; Epub ahead of print, PMID: 19403886). Cancer specialists are expect-ed to face a difficult challenge in dealing with this patient load.
“ASCO and the Workforce Adviso-ry Group continue to explore a variety of solutions to the anticipated oncolo-gy workforce shortage,” said Douglas W. Blayney, MD, ASCO president, in a press statement. “We believe collabor-ative practice models will help cancer care professionals cope with the reali-ties of having too many patients and not
enough doctors.”Oncology Metrics will conduct the
comprehensive analysis of how oncol-ogists, NPs and PAs collaborate to pro-vide patient care. Up to 40 private and hospital-based oncology practices will be involved, and researchers will specifical-ly examine the satisfaction, efficiency and productivity of each collaborative care team in order to establish “best practic-es.” Researchers will survey practices that vary in size, patient population and loca-tion. Results are expected in early 2011.
According to ASCO’s 2007 workforce
study, 56% of oncologists work with NPs or PAs, and providers who use these pro-fessionals have higher visit rates than those who do not. NPs and PAs provide services such as ordering and adminis-tering routine chemotherapy, as well as patient education and counseling.
The study is part of a collaboration between the ASCO Cancer Foundation, ASCO and Susan G. Komen for the Cure, in which Komen is providing $10 mil-lion in support of projects and programs designed to improve the quality of can-cer care in the United States.
Genetic Predisposition to Cancer Presents Difficult Choices
Addressing Oncology Workforce Shortage
A family in Charlotte, N.C. been getting a lot of press lately: Since September 2008, three of the family members have undergone prophylactic gastrectomies to avoid developing the gastric cancer that took the lives of two first-degree relatives. The youngest family member to take this preemptive step is 26.
CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 • DIGITAL EDITION BPRN
Genetics
Staffing
POLICY & MANAGEMENT
Cancer Therapeutic Agents Guide Now Available
The “Guide to the Administration and Use of Cancer Therapeutic Agents 2009” is available. Brought to you by Clinical Oncology News, the guide is authored by Val R. Adams, PharmD,
associate professor at the University of Kentucky College of Pharmacy in Lexington, and Susanne E. Liewer, PharmD, clinical pharmacy specialist, Stem Cell Transplant, Children’s Mercy Hospital in Kansas City, Mo. The drug information in this review is based on the most recent product literature at the time of printing; see the package insert for each product for complete prescribing information. To request a hard copy of this pocket guide, please visit www.clinicaloncology.com/copyorderform.asp.
All pocket guides are free to MDs in oncology and hematology/oncology, oncology nurses and oncology pharmacists, plus shipping and handling of $5.99 for the first copy and $1.00 for each additional copy. For bulk orders of up to 10 copies, pay only $15.99 and $1.00 for each additional copy shipping and handling (U.S. orders only).

Now, significant revisions to the Advanced Medi-cal Technology Association (AdvaMed) Code of Eth-ics aim to restrict some practices that may have led to abuses in the past.
“The goal is always to make sure that every time a doctor makes a decision, it is in the best interest of the patient, and not because of a relationship with a device company,” said Andrew Van Haute, AdvaMed’s dep-uty general counsel. According to its Web site, AdvaMed’s member companies pro-duce nearly 90% of the medical technolo-gy purchased in the United States.
The revised code of ethics (www.advamed.org/MemberPortal/About/code) includes a number of changes to how indus-try representatives can interact with health care professionals. There now is an explic-it prohibition from providing entertainment to physicians, and the provision of meals is allowed only under specific circumstances.
There also are changes to the guidelines regarding consulting and other relationships between industry and physicians. AdvaMed specifies that the need for a consultant must be legitimate, and selection of the consul-tant should be based on his or her qualifica-tions and expertise to meet that predefined need. Furthermore, the code states that the compensation in such an agreement needs to be consistent with fair market value, and should not in any way be dependent on the volume of the consultant’s potential busi-ness with the company.
“I think the revised guidelines are an improve-ment,” said Jaimie Henderson, MD, professor of neu-rosurgery at Stanford University Medical Center, in Stanford, Calif., and president of the North American Neuromodulation Society. “I think it is very important for industry and physicians—especially in the area of neuromodulation—to have a very well-defined rela-tionship, and that needs to follow very clear-cut eth-ical principles.”
Backlash to Major Abuses
Dr. Henderson said that some recent high-profile cases involving inappropriate relationships between medical device companies and doctors have increased scrutiny of the field. One notable case involved five major orthopedic device companies (Zimmer, DePuy Orthopaedics, Stryker, Biomet and Smith & Neph-ew) and an investigation into whether consulting agreements with physicians violated the federal anti-kickback statute. The case was settled with the U.S. Department of Justice in September 2007, with the companies agreeing to pay more than $300 million in penalties.
“Those situations aren’t necessarily what made us decide to revise the code, but they did in a way
inform some of the decisions that we made on the revisions,” Mr. Van Haute said. AdvaMed first wrote its code of ethics in 1991, and undertook a first major revision in 2003 that went into effect in 2004. The new revisions officially took effect on July 1, 2009.
Some think that the reaction to such public and costly issues is leading to practices that may hinder the development of new technologies and efforts to better treat patients.
“Before, maybe there was too little scrutiny of rela-tionships between physicians and industry, but now there’s too much,” said David Schultz, MD, medical director of Medical Advanced Pain Specialists med-ical pain clinics in Minneapolis and president of the American Society of Interventional Pain Physicians. “I think that was a minority of cases; I don’t think that it is a common, epidemic problem. There is a kind of overreaction now, to the point where almost
any relationship between a physician and industry is suspect, which I think is very unfortunate. I cer-tainly believe in transparency and compensation that is commensurate for actual work performed. But if physicians are stigmatized for collaborating with industry, then medical progress will be hindered and patients will suffer.”
The End of the Free Pen?
The changes to AdvaMed’s code go beyond con-sulting and other financial relationships. Under the
new rules, companies also will not be per-mitted to provide gifts of any type to health care professionals, regardless of value. This includes “noneducational” brand-ed promotional items such as pens, note-books or mugs.
Some believe that such prohibitions go beyond making sure that the patient’s well-being is the first priority, but Dr. Hen-derson said eliminating any possibility of unconscious bias is important.
“Everybody says that they won’t be influ-enced by industry gifts and that they take conscious steps to distance themselves from any individual company even if they do provide something of value,” he said. “But I think the supposition that we can eliminate our own biases is a false one. I think we need to have strict guidelines, like the AdvaMed guidelines, in order to help us with that.”
Dr. Schultz disagreed, saying that the effect of the high-profile settlements and abuses causes unnecessary changes to stan-dard practice. “I think physicians can real-ize that and actively prevent [bias] from entering into their decision-making pro-cess,” he said. “I think we’re sophisticat-
ed professionals, and I don’t think that we’re going to be influenced by that type of thing to actually take an action. I don’t buy that subconsciously I’m going to be prescribing things because of some lunch that some-body gave me. I find it insulting, actually.”
Whether or not a pen or a lunch would influence a physician into using a device or prescribing a drug is not explicitly addressed in the revised code of ethics, but Mr. Van Haute said the perception of impropriety is important to avoid. Branded promotional items, he said, are “rightly or wrongly seen as putting a cloud over the physician’s decision making. And we thought it best to just eliminate that entirely.”
Although Dr. Henderson said the revisions are a step forward in improving the relationship between industry and health care professionals, it will require some new thinking on how to continue some of the collaborative efforts that help to push technology in the right direction.
“The evolution is toward ever-stricter rather than looser guidelines,” he said. “I think that, overall, these guidelines are proper, they’re good and they’re help-ful, but there are some areas where they may in fact impact patient care negatively.”
—Dave Levitan
Revised Code of Ethics Seeks To Balance Physician–Industry TiesThe relationship between industry and the physicians who use their products is always a delicate balancing act, and both perceived and real conflicts of interest must be carefully monitored.
C CLINICAL ONCOLOGY NEWS DIGITAL EXCLUSIVE • JULY/AUGUST 2009PRN
Ethics
Under the new rules, companies will not be permitted to provide gifts of any type to physicians, regardless of value, including the perennial favorite, the free pen.

Dr. Pass selects the papers based on a variety of issues. “When you PubMed ‘breast cancer 2008,’ there are almost 8,000 papers,” she said. “So I try to lim-it it to any landmark studies, studies that when you go home might change what you are going to do, or [topics] that [were] highlighted in the news that patients seem to ask about.”
Dr. Pass came up with the idea of a Top 10 presentation in 2003, when she was program chair of the ASBS meet-ing. “Trying to keep up with the wealth of literature out there is all-consuming,” she said. “I always wanted somebody to tell me, ‘here, read this.’ ” At that time, she was also the editor of a review jour-nal, for which reading all of the breast research papers was a requirement. “It was a natural marriage. That journal has ceased to exist, but I still do this paper every year.”
The Top 10 Breast Cancer Papers of 2008
1. Azimm A, Constantini- Ferrando M, Oktay K. Safety of fertility preser-vation by ovarian stimulation with letrozole and gonadotropins in patients with breast cancer: a pro-spective controlled study. J Clin Oncol. 2008;26:2630-2635, PMID: 18509175.
Fertility issues are becoming more important as more breast cancer patients are being diagnosed at younger ages. Recent American Society of Clin-ical Oncology guidelines now encour-age the assessment of desire for fertili-ty preservation and emphasize the need for appropriate referral, and patients are increasingly aware of this issue.
Fertility preservation makes surgeons apprehensive, however, due to the hor-monal component of breast cancer and the fact that the supraphysiologic levels of estradiol that occur with convention-al ovarian stimulation may increase the risk for recurrence. The purpose of this trial was to determine if letrozole plus standard fertility medication affect-ed the disease-free survival of women undergoing treatment.
In this nonrandomized trial, 215 wom-en were prospectively evaluated for in vitro fertilization (IVF); 79 patients underwent IVF with letrozole and stan-dard agents, and 136 did not receive IVF.
At post-chemotherapy follow-up (medi-an, 23.4 months for the letrozole group and 33.1 months for the control group), there were no differences in disease-free status or overall survival rate between the two groups. Conclusion: IVF with letrozole and standard agents does not seem to increase the risk for recurrence in women with breast cancer who under-go fertility treatment.
The short follow-up gave Dr. Pass some concern. Although a large percentage of cancers will recur within two years, can-cer may recur later in life. “But IVF stim-ulation with letrozole did work and was effective,” she said.
Application for practice: Women of childbearing age should be offered referral for counseling about fertility preservation.
“I hate to tell you this, but as the sur-geon this is now one more obligation,” along with referral or counseling for the genetic component of the disease, con-sidering the patient’s molecular pro-file and having a meaningful discussion about breast reconstruction before they see the plastic surgeon, Dr. Pass said.
“We are the first line of education for our patients. If they are interested in fer-tility preservation, you need to be the one to start this conversation.” She rec-ommended that surgeons identify near-by fertility clinics with the expertise to deal with women with breast cancer so that this information is readily avail-able. “I do think this challenge is falling on us and the best way to [face] it is to be prepared.”
2. Thompson M et al. Intraopera-tive radioisotope injection for sen-tinel lymph node biopsy. Ann Surg Oncol. 2008;15:3216-3221, PMID: 18777194.
Preoperative injection of techne-tium sulfur colloid (Tc-99) is painful for patients and can cause problems with scheduling and operating room (OR) delays. This study was conducted to determine if intraoperative injection of Tc-99 is feasible.
This was an IRB-approved, prospec-tive study of patients with operable breast cancer who were candidates for sentinel lymph node (SNL) biopsy. The patients underwent subareolar injection of 1 mCi Tc-99 after general anesthesia. The
236 patients underwent 252 SNL biop-sies; time from injection to incision was 25.5±16.2 minutes; identification rate was 96%; average number of SNLs was 1.6±0.8; 20% of patients had a positive SNL; radi-ation exposure to surgical staff was well below established acceptable limits; and cost savings were $1,325 per patient. Con-clusion: Intraoperative subareolar injec-tion of Tc-99 is pain-free for patients, sim-plifies surgical scheduling, avoids surgical delays and is less costly.
Application for practice: “This paper caught my eye because it’s a dream of mine,” Dr. Pass said. This study provides evidence that there is no magical time window for Tc-99, and that the injection can be given in a pain-sparing way.
“I know my nuclear medicine col-leagues cringe because they don’t like inflicting pain,” Dr. Pass said. She rec-ommended surgeons discuss the study with their nuclear medicine colleagues, and ask them to consider coming to the OR to provide the service or, if regula-tory issues can be resolved, turning the performance of that service over to the surgeons themselves.
3. Arora S et al. Atypical ductal hyperplasia at the margin of breast biopsy—is re-excision indicated? Ann Surg Oncol. 2008;15:843-847, PMID: 17987337.
Atypical ductal hyperplasia (ADH) warrants surgical excision when it is found on a core biopsy. It is not so clear, however, what to do when ADH is found at the border of a lumpectomy. Dr. Pass herself questions the biologic relevance when there is not a frank malignancy, but her pathologist’s concerns—“ ‘this one is bad, that one is OK’ ”—have made her wonder. “I think it’s the extent of volume in all of the margin, but I want the pathologist to come up with the clin-ical relevance to these problems.”
This study was a retrospective review of the pathology database of Mount Sinai Medical Center, New York City, over five-and-a-half years. Of 44 lumpectomy specimens with ADH involving the sur-gical margin, 24 patients (55%) under-went re-excision at the surgeon’s dis-cretion. The re-excisions revealed no additional disease in nine and ADH in two, and more ductal carcinoma in situ (DCIS) or invasive ductal carcinoma
(IDC) in four patients. Of the 15 patients originally diagnosed with ADH, four (27%) were upstaged, and of the eight with a known diagnosis of malignancy, four (50%) had additional cancer at re-excision even when there was no cancer present at the margin. Conclusion: ADH at the margin of a lumpectomy is asso-ciated with a high rate of residual ADH and cancer; re-excision of all patients with ADH is recommended.
“I wish medicine were that simple,” Dr. Pass said, noting the study consist-ed of a highly selected, small retrospec-tive cohort with modest long-term fol-low-up. Critical examination of the data reveals that in patients with a diagnosis of ADH alone, upgrading was most like-ly if there was a residual mammographic abnormality indicating a mass or calcifi-cations, which would imply that the orig-inal lesion wasn’t adequately sampled with surgical excision, she explained.
Application for practice: “If I have ADH on a core and I remove the area and find ADH at the margin but remove the vast majority of the mammograph-ic abnormality, those patients don’t nec-essarily have to go on for re-excision,” Dr. Pass said. “They need to be treated as high-risk patients and have a discus-sion about chemoprevention.”
In patients with a cancer diagno-sis, however, the extent and amount of ADH should be considered. “One duct with ADH at the margins is very differ-ent than a ton of ADH at multiple mar-gins,” Dr. Pass said. “Maybe we need to be thinking more critically [whether] we could re-excise those patients much like we do for DCIS at the margin, especially if they still have a [cosmetically] accept-able outcome.”
4. Ciocca R, Li T, Freedman G, Mor-row M. Presence of lobular car-cinoma in situ does not increase local recurrence in patients treat-ed with breast-conserving therapy. Ann Surg Oncol. 2008;15:2263-2271, PMID: 18506537.
Surgeons usually perform an excision when lobular carcinoma in situ (LCIS) is found on core biopsy. This study was con-ducted to determine the need for re-exci-sion if LCIS is present in the lumpectomy specimen, especially at the margin.
The study was a retrospective database review of 894 early-stage (0-II) cancer patients treated at a single institution over 27 years. Of 290 patients with LCIS, 84 had LCIS at the final margin; 2,604 patients without LCIS served as con-trols. Median follow-up duration was 5.2 years.
“Top 10” Breast Cancer Studies Reviewed at MeetingExpert Discusses Potential Practice-Changing Research
In what has become one of the most popular presentations at the annual meeting of the American Society of Breast Surgeons (ASBS), Helen Pass, MD, assistant professor of clinical surgery at Columbia University in New York City, and attending surgeon at NewYork-Presbyterian/Columbia University Medical Center and Lawrence Hospital in Bronxville, N.Y., discusses what she considers the top 10 breast cancer papers of the year.
see TOP 10, page E �
CLINICAL ONCOLOGY NEWS DIGITAL EXCLUSIVE • JULY/AUGUST 2009 DSOLID TUMORS
Breast

In patients with LCIS at the margin, the local recurrence rate at five to 10 years was 6%. When LCIS was present in the specimen but not in the margin, the local recurrence rate was 1% and 15% at five and 10 years, respectively. In the absence of LCIS, the local recurrence rate was 2% and 6% at five and 10 years, respective-ly. Conclusion: The presence of LCIS in the margin of breast-conserving thera-py specimens does not affect local recur-rence and does not mandate re-excision.
Application for practice: “Not all high-risk lesions are equal—what you do for ADH may not extrapolate to LCIS, and we have no information on ALH [atyp-ical lobular hyperplasia],” Dr. Pass said. “But we know that the presence of DCIS at the margin is an indication for re-exci-sion, so even all in situs are not the same. This is an evolving field and one to stay tuned to and to begin to monitor in your own practice.”
5. Julian T et al. Novel intraoperative molecular test for sentinel lymph node metastases in patients with early-stage breast cancer. J Clin Oncol. 2008;26:3338-3345, PMID: 18612150.
For intraoperative SNL evaluation, most surgeons currently use frozen sec-tion and touch prep cytology. The authors of this study conducted a beta trial and a validation trial to validate use of the intra-operative molecular sentinel node test (aka, the breast lymph node [BLN] assay).
The beta trial consisted of 304 patients to determine the threshold of mamma-globin and cytokeratin 19, which correlate with metastases within the sentinel node greater than 0.2 mm. The validation trial of 416 patients was done to corroborate this threshold. The BLN assay required 36 to 46 minutes to complete. Conclusion: The BLN assay allows rapid evaluation of the sentinel node that is more accurate than conventional techniques.
Compared with frozen section analy-sis, the BLN assay “had a superior sensi-tivity and negative predictive value,” Dr. Pass said. “The negative predictive value is important because none of us wants to do a completion axillary lymph node dis-section [and find out] the sentinel node really wasn’t positive.”
Application for practice: The technol-ogy is yet not widely available, but “if it’s something your pathology department is interested in pursuing, the fact that it is molecularly based instead of pathologi-cally based should not give you pause for concern,” Dr. Pass said. “In very busy cen-ters, since this is a [technologist–depen-dent] rather than a pathologist-depen-dent assay, this may allow for ease and greater simplicity in cases where they’re
doing multiple frozen sections.”
6. Martelli G et al. Elderly breast can-cer patients treated by conservative surgery alone plus adjuvant tamox-ifen. Cancer. 2008;112:481-488, PMID: 1809826.
Elderly patients with breast can-cer often do not receive treatment in compliance with national guidelines. Many surgeons individualize care of the elderly because of their comorbid-ities, their reduced life expectancy, the presumed favorable biologic behavior of their tumors and the effectiveness of adjuvant hormonal therapy. This study evaluated the need for SNL biopsy and radiation therapy in elderly patients with breast cancer.
The prospective study followed 354 women older than 70 years with oper-able breast cancer for a median of 15 years. The patients had margin-nega-tive breast-conserving therapy and no axillary procedures or radiation, and all received adjuvant tamoxifen. The crude cumulative index of axillary dis-ease was 4.2%, in-breast recurrence was 8% and distant metastasis was just under 8.8%. Overall mortality was 76%, with 17% from breast cancer–specif-ic causes. Conclusion: Elderly patients with clinically node-negative disease can be treated with conservative sur-gery and hormone therapy, without an axillary procedure or radiation.
Application for practice: Surgeons often face an unsettling conundrum when deciding how much treatment to subject their elderly patients to. “You always feel guilty if you withhold one form of treatment or another,” Dr. Pass said. “This study justifies the art of medi-cine that we practice every day and [sup-ports] this approach in a selected patient population.”
If the surgeon and patient decide to forgo radiation, obtaining negative mar-gins is critical and the delivery of adju-vant hormonal treatment is important to increase local control. Surgeons should keep in mind the original National Sur-gical Adjuvant Breast and Bowel Project studies showing that if patients have an axillary relapse, surgery performed at a later date is still effective. Also, elderly patients vary greatly in fitness; chrono-logic age should not be the main factor determining treatment.
7. Hooning M et al. Roles of radio-therapy and chemotherapy in the development of contralat-eral breast cancer. J Clin Oncol. 2008;26:5561-5568, PMID: 1885457.
Women who have breast cancer have a threefold to fourfold increase in the risk for developing contralateral breast cancer. This study examined the role of modern radiation and chemothera-py—which are constantly evolving—in the risk for contralateral breast cancer
development.In this Dutch registry review of 7,425
patients with a follow-up rate of 95%, the risk for contralateral breast cancer increased in women under 35 years of age receiving radiation (hazard ratio [HR], 1.78); in women over 45, HR approached 1; there was little comment on women aged 35 to 45. Conclu-sion: Women under 45 irradi-ated with tangential fields have an increased risk for contralat-eral breast cancer, especially if they have a positive fami-ly history. Chemotherapy in the first five years may mit-igate this risk (thereafter, it makes no difference).
Application for practice: “We have to counsel these women regarding the risk of contralateral breast cancer and discuss surgical options,” Dr. Pass said. “It’s very diffi-cult to tell a woman who has a lumpectomy option that she might want to consider mastectomy or bilateral mas-tectomy, but women need to be apprised of their risk of contralateral disease.”
This also calls into question postop-erative surveillance. “We tend to take for granted that once these women are five years out, they’ll be followed by their primary care providers; but may-be as their breast surgeon, we need to be more aware of their risk for contralater-al breast disease,” Dr. Pass said.
8. Mortimer J et al. Tamoxifen, hot flashes, and recurrences in breast cancer. Breast Cancer Res Treat. 2008;108:421-426, PMID: 17541741.
In this study, 864 women on tamox-ifen, diagnosed between 1995 and 2005, filled out an extensive questionnaire on a variety of topics, including their expe-rience of hot flashes. The women were staged I-IIIa breast cancer. Those who reported hot flashes had a recurrence rate of 12.9%, while those who did not report hot flashes had a recurrence rate of 21%. Conclusion: Hot flashes are a stronger predictor of recurrence than age, hormone receptor status or wheth-er the patient is stage I or II.
Application for practice: “In our prac-tice, compliance with hormonal therapy is variable—many women get discour-aged and want to stop,” Dr. Pass said, noting that she herself has always been nervous when patients breeze through chemotherapy. “In the back of my mind, I wonder if anything is really being bio-logically affected. This study is evidence for surgeons to share with patients who complain bitterly about hot flashes. That means the drug is really working and they [will have] a better outcome.”
9. Goss P et al. Late extended adju-vant treatment with letrozole
improves outcome in
women with ear-ly-stage breast can-
cer who complete 5 years of tamoxifen. J Clin Oncol.
2008;26:1948-1955, PMID: 18332475.The Oxford overview of hormonal
therapy for early-stage breast cancer indi-cates that more than half of all breast can-cer recurrences or deaths happen after five years of adjuvant tamoxifen; longer duration of tamoxifen use has not been shown to be beneficial. “What happens to women who have been off tamoxifen for a substantial period of time?” Dr. Pass asked. “Many women who took tamox-ifen for five years were told that it was time to stop it and sent on their way. Should they now initiate a separate round of treatment?”
In the National Cancer Institute of Canada Clinical Trials Group MA.17 tri-al, patients were initially randomized to receive placebo versus letrozole after five years of tamoxifen. The trial reached stopping criteria after 2.5 years, and treat-ment was unblinded. There was a signif-icant improvement in women who were on letrozole, and women on placebo were offered the option of switching to letro-zole. Consequently, 1,579 patients switched and 804 patients remained on placebo. The median follow-up was 5.3 years.
In the letrozole group, disease-free survival improved impressively (HR, 0.37), as did distant disease–free sur-vival (HR, 0.39). Conclusion: Letrozole improves disease-free survival and dis-tant disease–free survival even if sub-stantial time has passed since the dis-continuation of tamoxifen.
Application for practice: “Not only do you have to do more pre-diagnosis in these women, but I’m asking you to do more post-diagnosis as well,” Dr. Pass said. “It’s important that we disseminate this information to our primary care pro-viders,” and alert them that the algorithm has changed. “After five years of tamox-ifen, women need to be either started on another agent or referred back to their medical oncologist, breast surgeon or another provider for consideration of additional treatment.”
E CLINICAL ONCOLOGY NEWS DIGITAL EXCLUSIVE • JULY/AUGUST 2009SOLID TUMORS
Breast
TOP 10continued from page D �

10. Cady B, Nathan R, Michelson J. Matched pair analyses of stage IV breast cancer with or without resection of primary breast site. Ann Surg Oncol. 2008;15:3384-3395, PMID: 18726129.
“We’ve heard a lot about women with stage IV breast cancer who have a sur-vival benefit when the primary tumor is resected, but this is still debated,” Dr. Pass said. The authors of this study sought to determine if selection bias accounts for the improved survival of women with stage IV breast cancer who undergo resection of the primary tumor.
The study analyzed patients with stage IV breast cancer, matching cases on age, date of diagnosis, location of metastat-ic disease, estrogen receptor (ER) status and use of adjuvant and systemic therapy. Of 622 patients, 388 (62%) had no prima-ry site surgery, 234 (38%) underwent sur-gery of their site. Survival was significant-ly improved in patients who underwent surgery (P=0.0001).
Survival, however, was better in patients who received chemotherapy before sur-gery; there was no benefit for those who received chemotherapy and surgery with-out a time delay. Conclusion: The case
selection bias of stage IV patients who undergo surgery explains most of the apparent survival benefit seen with this approach. There is no biologic explana-tion for the improved outcome.
Application for practice: Resecting primary patients with stage IV disease is still not a standard of care, but it is no longer taboo. “We used to be told, if you operate on these patients you’re breaking some sort of rule,” Dr. Pass said. But “on a case-by-case basis, there are probably several selected patients who will bene-fit from what we used to term the ‘effort effect.’ ” The patients most likely to
benefit from this resection of the prima-ry tumor are those who have “a dramat-ic response to chemotherapy, have oli-gometastases, have a good performance status and are highly motivated.”
Keeping up with the literature is a Sisy-phusian task for most. “Given the vast quantity of published material, staying current is a challenge for the practicing physician, which is why I review articles such as these,” Dr. Pass said. “Attendance at meetings can [also] help highlight important advances and keep the practi-tioner up to date.”
—Monica Smith
O. Carl Simonton, MD, DiesO. Carl Simonton, MD, a radiation oncologist who advo-cated treating the emotional and psy-chological needs of cancer patients, has died. He was 66. Dr. Simonton popular-ized the mind–body connection in fighting cancer and helped push this notion into mainstream medi-cine. He advocated for treating patients through techniques such as meditation and image-guided therapy.
In the early 1970s, he founded the Can-cer Counseling and Research Center in Fort Worth, Texas. In 1978, he co-wrote the book “Getting Well Again.” In 1984, he moved his practice to California, where he founded the Simonton Cancer Coun-seling Center, currently located in Mal-ibu. He died suddenly, choking during a meal at his home in Agoura Hills, Calif.
Oncologist Files Lawsuit
According to an article in the Peninsula Daily News, a regional paper in
Washington state, cancer specialist
Robert Witham, MD, has filed a federal lawsuit against Olympic Medical Center (OMC), in Port Angeles, arguing that the hospital is a monopoly and violates the federal Sherman Antitrust Act. The suit resurrects accusations of unfair competi-tion that he first made in 2004.
In his suit, Dr. Witham alleges that the medical center and its public hospi-tal is illegally driving him out of business and violating the law by directly employing doctors to unfairly compete with private physicians. He claims that the hospital’s intention to hire a second medical oncol-ogist will virtually drive him out of busi-ness. “OMC has now obtained monopoly power over the delivery of most profes-sional medical services in Clallam Coun-ty,” the lawsuit states.
According to the Peninsula Daily News, Dr. Witham claims the hospital’s actions including disparaging his repu-tation have cost him hundreds of thou-sands of dollars in losses. He has also experienced a precipitous decline in new
cancer patient referrals, because of the hospital’s aggressive hiring of doctors and specialists and the hospital inten-tionally diverting referrals away from him to generate profit.
According to a spokesman for OMC, the lawsuit is without merit and the business practices of the hospital are legal and ethical.
Cancer Survivors Launch Company
Cancer survivors in Wisconsin
have launched a company to offer an online nutri-tional service and meal-planning pro-gram for cancer patients. The com-pany, called TherapEase Cuisine, Inc., can be accessed at www.therapease-cuisine.com. According to the compa-ny’s Web site, their program is based on accepted oncology-dietetic practice and was developed by registered dieti-tians. It is available to cancer patients and health care systems treating can-cer patients to assist in maintaining
nutrition throughout treatment. Nutritional support for cancer outpa-
tients is often limited to minimal advice from their oncologists and some spe-cific cookbooks that are on the market. “Studies have shown that customized nutritional modifications to comple-ment a patient’s course of treatment can be very beneficial before, during and after treatment,” said James Her-mann, president and CEO of Thera-pEase Cuisine. “That’s why we’ve devel-oped a program for cancer patients that they can individually sign up for or that health care systems can purchase and offer to their patients.”
Program participants receive individ-ualized and detailed food recommenda-tions, as well as direct support via e-mail or phone from staff dietitians. The pro-gram features expert advice custom-ized to each patient’s diagnosis, treat-ment and criteria; regular reassessment and modifications based on symptoms and side effects as they materialize; and a library of educational information including updates for new studies and developments in the field of oncology dietetics. The company’s headquarters is in Greenfield, Wis.
Around the Water CoolerPEOPLE & PLACES
CLINICAL ONCOLOGY NEWS DIGITAL EXCLUSIVE • JULY/AUGUST 2009 FSOLID TUMORS
Breast
CME Opportunity Available: Cutaneous T-Cell Lymphoma
Are you in need of continuing medical education (CME) credits? The CME activity, “Cutaneous T-Cell Lymphoma: Early Diagnosis and Optimal Management Strategies,” is available at www.clinicaloncology.com. The review covers categorization and clinical-histologic features of CTCL, diagnosis and staging, and optimal medical management. The activity is valid for CME credits for physicians, pharmacists and nurses until Aug. 1, 2010.

Physicians and scientists submitted more than 100 abstracts, of which 49 were chosen for either oral or poster presentation. Several of these were notable for the information provided and their potential influ-ence on patient care. These abstracts can be divid-ed into three categories: clinical trial updates, nov-el agent development for therapy of metastatic RCC (mRCC) and toxicity management.
Bevacizumab News
During the ASCO 2008 meeting, the final overall survival (OS) update for the Phase III trial compar-ing sunitinib (Sutent, Pfizer) to interferon (IFN)-α in patients with treatment-naïve mRCC was present-ed (J Clin Oncol 2008;26: abstract 5024). A clinical-ly significant improvement in median OS for patients receiving the tyrosine kinase inhibitor (TKI) sunitinib was noted (26.4 vs. 21.8 months; hazard ratio [HR], 0.818; stratified log rank P=0.0491).
This year, two large Phase III studies comparing bev-acizumab (10 mg/kg IV every two weeks) plus subcuta-neous IFN-α (9 mU three times per week) or the same dose of IFN-α monotherapy in untreated patients were updated, and final survival analyses discussed. Previ-ously reported results from both trials had revealed a significant improvement in progression-free surviv-al (PFS) and overall response rate (ORR) for patients receiving bevacizumab plus IFN-α. At ASCO, Rini and colleagues presented results from the Cancer and Leu-kemia Group B (CALGB) trial in which 732 patients were randomized in open-label fashion to either treat-ment (J Clin Oncol 2009;27: LBA5019); 369 patients received the combination and 363 received IFN-α. The median OS for the cohort receiving combination ther-apy was 18.3 months (95% confidence interval [CI], 16.5-22.5) compared with 17.4 months for IFN-α treat-ed patients (HR, 0.86; 95% CI, 14.4-20.0; stratified log rank P=0.068) (Figure 1). The data for MSKCC prog-nostic subgroups were also presented. The median OS in the favorable-risk group receiving bevacizumab plus IFN-α versus IFN-α was 32.5 versus 33.5 months (P=0.524); in the intermediate-risk group, 17.7 versus 16.1 months (P=0.174); and in poor-risk patients, 6.6 versus 5.7 months (P=0.245). It was noted that 53% of patients had received secondary therapy following dis-ease progression.
The AVOREN trial, updated by Escudier and col-leagues, also compared bevacizumab plus IFN-α with IFN-α alone (J Clin Oncol 2009;27: abstract 5020). In this double-blind, placebo-controlled study, 648 patients were randomized to either bevacizumab plus IFN-α (n=327) or placebo plus IFN-α (n=322). The final median OS for patients receiving bevacizumab was 23.3 months, compared with 21.3 months (HR, 0.86; stratified log rank P=0.1291) for patients treated with IFN-α and pla-cebo. Secondary therapy including TKIs, mTOR inhib-itors, cytokines and chemotherapy was administered to 180 patients (55%) in the bevacizumab plus IFN-α arm and 202 patients (63%) in the placebo plus IFN-α arm. A subset analysis of patients receiving subsequent
TKIs (96 and 81 patients, respectively) demonstrated a median OS of 38.6 months for those initially treat-ed with bevacizumab plus IFN-α versus 33.2 months for the placebo plus IFN-α group (HR, 0.77; P=0.1948). Survival data for the various MSKCC subsets was not presented.
These two very important trials were different in design and eligibility criteria, but represent the cur-rent data set for patients receiving bevacizumab plus IFN-α. The previously reported improvements in PFS and ORR have been maintained; however, no significant differences in survival were identified. It is possible that secondary therapy with agents such as sunitinib, sorafenib or temsirolimus confounded these analyses, but the subset data presented could not demonstrate this effect. A second interesting finding in the CALGB study was the lack of OS differ-ence in the favorable MSKCC subgroup, something that was also noted in the sunitinib versus IFN-α tri-al (J Clin Oncol 2009;27:1-7). It may well be that this group of patients with few symptoms and limited dis-ease experiences major effects with secondary treat-ments, or patients with indolent disease experience different clinical outcomes. Further analyses of these studies hopefully will clarify some of these issues. Finally, based on the available information, it seems likely that the FDA will approve the combination of bevacizumab and IFN-α for treatment of patients with advanced RCC. The significant improvement in PFS associated with bevacizumab and IFN admin-istration supports this approval, and the supportive
findings from the CALGB trial provide additional evidence for this effect.
Novel TKIs
A second set of presented abstracts described a series of TKIs with significant antitumor effects in metastatic clear cell RCC. Sternberg and colleagues presented an initial report of a blinded, placebo-controlled Phase III trial in which patients with mRCC were randomized (2:1) to either the multi-kinase inhibitor pazopanib (GlaxoSmithKline) at 800 mg daily (n=290) or a placebo (n=145) (J Clin Oncol 2009;27: abstract 5021). Therapy was contin-uous, and at progression, patients receiving place-bo were permitted to cross over to pazopanib. The study included both untreated (n=233) and cytokine-refractory patients (n=202).
Investigators found that PFS was significant-ly prolonged by pazopanib compared with placebo (9.2 vs. 4.2 months; HR, 0.46; P<0.0000001). A simi-lar effect was seen in both the treatment-naïve (11.1 vs. 2.8 months; HR, 0.40; P<0.0000001) or cytokine-refractory groups (7.4 vs. 4.2 months; HR, 0.54; P<0.001). The ORR with pazopanib was 30% com-pared with 3% in the placebo arm (Figure 2). The median response duration was 58.7 weeks. Adverse events were described as mild; however, 12% of pazopanib-treated patients experienced grade 3 or greater hepatic toxicity.
These data clearly demonstrate the effectiveness of pazopanib in mRCC, and suggest regulatory approv-al of another novel agent for mRCC therapy is likely in the near future. An ongoing Phase III study comparing pazopanib with sunitinib in first-line mRCC patients will provide additional clinical information on this agent.
Three additional presentations highlighted prelim-inary data with the novel TKIs AVI-951 (J Clin Oncol 2009; 27: abstract 5032), BAY 73-4506 (J Clin Oncol 2009; 27: abstract 5033), and ABT-869 (J Clin Oncol 2009;27: abstract 5036). This series of Phase II tri-als reported the activity of these multi-kinase inhibi-tors, and a noted investigator assessed ORR between 19.6% (ABT-869) and 27.2% (AVI-951). These studies highlight the sensitivity of clear cell RCC to vascular endothelial growth factor (VEGF) receptor TKIs, and suggest a variety of other agents with different toxic-ity and efficacy patterns will be tested in clinical tri-als in the near future.
Sunitinib Toxicity
The final area of interest for RCC at the ASCO annual meeting included two presentations that focused on pharmacogenetic factors influenc-ing sunitinib toxicity in patients with mRCC. The two studies used analysis of patients’ single nucle-otide polymorphisms (SNPs) and correlated this
Bevacizumab, Pazopanib Ripe for Approval in RCCRonald Bukowski, MD, Highlights What You Need To Know From the ASCO Meeting
Orlando, Fla.—At the 2009 annual meeting of the American Society of Clinical Oncology (ASCO), significant new information and data on renal cell carcinoma (RCC) was presented.
10 CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009SOLID TUMORS
Kidney
Ronald M. Bukowski, MD
Director of Experimental Therapeutics ProgramTaussig Cancer CenterCleveland Clinic FoundationCleveland, Ohio
ADVISORY BOARD EDITORIAL
This series of Phase II trials reported the activity of these multi-kinase inhibitors, and a noted investigator assessed ORR between 19.6% (ABT-869) and 27.2% (AVI-951).
30
20
10
0Ove
rall
Re
spo
nse
Rate
, %
Pazopanib
Placebo
30
3
Figure 2. Comparison of response rate in RCC patients.

CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 11
information with toxicity. A presentation by Kim
et al reported a group of 62 patients with mRCC who were treated with suni-tinib, in whom the fre-quency of VEGF SNPs (–634 C/C and –1478 T/T) were then correlat-ed with the development of hypertension (J Clin Oncol2009;27: abstract 5005). The data demonstrated a significant associa-tion of VEGF SNP–634 G/G with suni-tinib-induced hypertension, but no asso-
ciation with ORR or PFS. A presentation by van Erp et al highlighted a multicenter study in which 31 SNPs in 12 candidate genes were assessed in 219 patients
receiving sunitinib (J Clin Oncol 2009;27: abstract
5006). A variety of SNPs from genes encoding metabolizing enzymes (CYP1A1), efflux trans-porters (ABCB1) and drug targets (VEG-FR-2) appeared to pre-
dispose patients to developing toxicities such
as leukopenia, hand–foot syndrome, mucosal inflamma-
tion, and in a nonspecific fashion any tox-icity greater than grade 2.
These two presentations require
confirmation, but suggest that genetic determinants can influence the devel-opment of sunitinib toxicity. This approach may be used in the future to optimize therapy and decrease toxicity for individual patients.
In summary, the ASCO 2009 meet-ing continued the recent trend for a large number of significant new
presentations dealing with mRCC. Data from the Phase III trials may ultimately influence the treatment of this patient group. Finally, the possibility that phar-macogenomic analyses will assist in optimizing therapy with a TKI such as sunitinib seems reasonable.
—Ronald M. Bukowski, MD
SOLID TUMORS
Kidney
These data clearly demonstrate the effectiveness of pazopanib in mRCC, and suggest regulatory approval of another novel agent for mRCC therapy is likely in the near future.
These two presentations require confirmation, but
suggest that genetic determinants can influence
the development of sunitinib toxicity.
Did you receive the August Digital Exclusive issue of Clinical Oncology News?
If you didn’t, you missed the following articles.
• Study Says Off-Label Resources Are Outdated, Flawed
• Standard of Care Established For Inoperable Biliary Cancer
• Immunotherapy Increases Cure Rate in Neuroblastoma
• Will Second-Gen TKIs Move to First-Line Therapy for CML?
• Sorafenib Dosing Poses Problem for Asian Patients
• High Risk For Parainfluenza Virus Infection Identified In Leukemia and HSCT Patients
To read these and other stories, visit www.clinicaloncology.com and click on the appropriate department head-ing. To register for the Digital Edition of Clinical Oncology News, click on the banner at the top of the page.
Micrograph of papillary renal cell carcinoma, showing vascular papillae with foam cells.
CHEMOTHERAPY FOUNDATION SYMPOSIUM XXVIIINNOVATIVE CANCER THERAPY FOR TOMORROW
November 11-13, 2009New York City
Register on line at chemotherapyfoundationsymposium.orgContact: [email protected]
CME Accredited by the Mount Sinai School of Medicine
The Greenspan Meeting
WEDNESDAY, NOVEMBER 11Hematology: Therapeutic Advances in Myeloproliferative & Myelodysplastic Syndromes, AML, CML, CLL, NHL, MM, JAK2, AML in the Elderly, HDAC Inhibitors, Anti-Myeloma Agents, Acute Leukemia, Mayo Risk Stratification MM. Lymphomas, Proteasome InhibitorsGI Cancers: Colorectal, Gastric Cancer, Pancreatic Cancer, Biliary Tract, Appendiceal, New Agents, TOGA, SPARC, AVANT Trials, VEGF Inhibitor, Recurrence Risk Prediction, Screening Advances, Hedgehog Pathway, mTOR Inhibition, C-Met Inibitors, Neuroendocrine Tumors
THURSDAY, NOVEMBER 12GYN Cancers: PARP, Recurrent Ovarian, Current Trials, Novel Treatments, Relapse Therapy, BRCA and Outcomes, Targeted Therapy, Melanoma: Biomarker Links, Analysis of Brain Metastases, Prognostic IndicatorHead & Neck Cancer: Targeted TherapySarcoma: Monotherapy and Chemotherapy in Tumor HypoxiaBreast Cancer: Gene Expression Profile, Triple Negative Breast Cancer, PARP, Novel Target, Mechanisms of Resistance to HER2, Novel HER2 Therapy Update, HER3 Measurement & Outcomes, Targeted Therapies in HER2 Negative Cancer, Anti-estrogen TherapyThyroid: Treatment in Advanced Disease
FRIDAY, NOVEMBER 13Immunotherapy: Vaccines, Blockage in Myeloma TherapyGU Prostate: Combination Therapy, Vaccine Therapy in PC, Phase II Clinical Trials, Neoadjuvant Therapy in High Risk PCRenal: Sarcomatoid Features, Novel AKT InhibitorLung Cancer: Novel Agents, PARP, Combination Chemotherapy, KRAS Mutatations and Targeted Therapy in NSCLC, EGFR Resistance, Biomarkers, Personalized Chemotherapy, Mesotheoloma Diverse Presentations: Unknown Primary, New Agents in Solid Tumors, Neuroendocrine Tumors, Recurrent Glioma, Dendritic Cells, CTEP Clinical Trials, Practice Patterns, EHRS

12 CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009
single-agent bevacizumab continued for an additional six months in the investigational arm. At the meeting, the investigators provided details of how the trial failed to meet its primary end point of three-year disease-free survival (DFS). What remains to be seen is what this study means for ongoing clinical trials and the drug’s future in patient care.
High Hopes
Bevacizumab, an anti-VEGF (vascular endotheli-al growth factor) antibody, is the first FDA-approved anti-angiogenic agent in the treatment of metastat-ic colorectal cancer following a significant improve-ment in overall survival noted in the pivotal trial of irinotecan, bolus 5-FU, and leucovorin (IFL), with or without bevacizumab. To date, the majority of bevaci-zumab trials in metastatic colorectal cancer have dem-onstrated an improved response rate, progression-free survival and overall survival. The drug has since been approved for the treatment of metastatic breast and lung cancers, as well as for glioblastoma.
Bevacizumab is the most commonly used biologic agent in metastatic colorectal cancer patients with-out contraindications to anti-angiogenic therapy. Investigators have not identified any markers that predict patient resistance to anti-VEGF therapy, and data regarding resistance to therapy are scarce. Given its well-documented efficacy in advanced colorectal cancer in conjunction with chemotherapy and pre-clinical data suggesting an impact of anti-VEGF ther-apy on preventing the development of metastatic dis-ease in animal models, bevacizumab appeared to be an appropriate biologic agent for investigation in the adjuvant setting. Reported safety data suggest that prolonged use of bevacizumab is not associated with significant toxicity.
Failure To Meet End Point
When Genentech announced in a press release that NSABP C-08 had failed to meet its primary end point in April, many oncologists were in disbelief. Given the success of bevacizumab in previous metastatic colon cancer trials, it did not seem possible that bev-acizumab would not have a role in the adjuvant set-ting, and some oncologists held out hope that the drug could benefit a subset of patients given a statement by Roche/Genentech. “Our initial review of the data leads us to continue to believe Avastin may be active in patients with early-stage colon cancer and look for-ward to NSABP’s presentation at ASCO,” said Hal Bar-ron, MD, senior vice president of development and chief medical officer at Genentech. “We remain fully committed to the ongoing Avastin adjuvant programs in early-stage colon, breast and lung cancers.”
The announcement caused many investigators to express concerns about ongoing trials in which bevaci-zumab was being utilized in the adjuvant colon cancer setting, notably AVANT (Roche) which had complet-ed patient accrual and ECOG 5202 which continued to accrue patients. Clinicians are keenly aware that to change the treatment paradigm in the adjuvant set-ting, thousands of patients must be accrued and fol-lowed extensively to identify any minute improvement in median disease-free or overall survival.
Appropriately enough, the press release resulted in the immediate temporary closure of ECOG 5202 for an amendment in its consent form informing patients of the preliminary negative results of NSABP C-08.
The negative DFS results were discussed in detail one month later at the ASCO plenary session on May 31, 2009. After a median follow up of 35.6 months, no difference in DFS was noted (hazard ratio [HR], 0.89) regardless of substratification by stage. Yet, the senior author of the trial suggested that the bene-fit of bevacizumab was present at the first year and implied that bevacizumab may need to be provided for a longer interval for optimal outcome (HR, 0.60; DFS first year only). What remained unanswered, however, was the potential impact on future patient care and how the results of the trial will affect ongo-ing adjuvant trials not only in colon cancer but also other malignancies.
Criticisms of Trial Design
One of the greatest criticisms of NSABP C-08 may lie in its clinical trial design. As a clinical investi-gator, when considering clinical trial design for an investigational agent, the objective is to establish superiority of the agent versus the standard of care with the ultimate goal of changing the existing treat-ment paradigm. Yet, NSABP C-08 required patients to receive an additional six months of bevacizum-ab when previous studies failed to demonstrate any benefit with single-agent bevacizumab in metastat-ic colorectal cancer.
Of greater interest is that stringent surveillance for tumor recurrence, computed tomography (CT) scans and carcinoembryonic antigen (CEA) levels at predefined intervals were not mandated in NSABP C-08. Given the primary end point of DFS, how were patients to be captured for recurrence of disease if only at the discretion of the treating physician? This point is of particular importance given the different duration of bevacizumab therapy in both arms of the trial, six months in the control arm versus 12 months in the experimental arm. Temporal imbalances in the timing of CT scans, and thus detection of recurrent disease, could have greatly influenced the reported results. This obvious oversight in trial design is sur-prising, because the study was considered a potential registration trial for bevacizumab in the adjuvant set-ting and would have been scrutinized by the National Cancer Institute and the Cancer Therapy Evaluation Program (CTEP) as well as the FDA.
Impact on Clinical Trials
So, how will the results of NSABP C-08 impact clin-ical trials? AVANT is a three-arm, randomized Phase III trial of FOLFOX versus FOLFOX plus bevacizumab
versus oxaliplatin and capecitabine (CapeOX) plus bevacizumab in high-risk stage II and stage III patients with a primary end point of DFS. Because AVANT completed accrual (N=3,451) in June 2007, the impact of NSABP C-08 is less in question. It is of note, howev-er, that AVANT mandated routine CT scans and CEA levels for both treatment arms.
The impact on ECOG 5202, however, is uncertain. It continues to accrue patients (1,889/3,610 patients as of May 16, 2009), and is the first prospective tri-al of its kind being conducted solely in stage II colon cancer patients with treatment stratification based on molecular prognostic markers. The trial hopes to address the ongoing dilemma for many treating phy-sicians in deciding treatment for the heterogenous stage II patient. Results of the Phase III INT-0035 and IMPACT B2 trials noted no additional benefit for adjuvant 5-FU in patients with stage II colon cancer. The recent QUASAR trial noted a minor benefit in five-year overall survival of 2.9% with adjuvant 5-FU. Yet, results from the adjuvant MOSAIC trial noted an improvement in DFS (HR, 0.74) for high-risk stage II patients who received six months of FOLFOX com-pared with 5-FU/LV (leucovorin) alone. The com-plexity of the decision of whether or not to treat the stage II patient population is reflected by ASCO’s nondirectional recommendation that adjuvant che-motherapy may be considered and can be discussed with the stage II patient. As a result, definitive treat-ment for the stage II patient is currently at the dis-
cretion of the treating physician. Unlike other clinical trials that define a high-risk
stage II patient as one with poorly differentiated his-tology, T4 disease, lymphovascular invasion or subop-timal lymph node dissection (<10 lymph nodes), ECOG 5202 is a unique trial comprised only of stage II colon cancer patients who are treated based on low risk (MSI-H or no 18q loss of heterozygosity [LOH], surveillance arm) or high-risk molecular markers (MSI-S or MSI-L, plus 18q LOH), and are treated with six months of FOLFOX with or without bevacizumab for 12 months, which is analogous to the design of NSABP C-08 with the primary end point of DFS. ECOG 5202 is 88% pow-ered to detect a 37% difference in median DFS (absolute difference of 5% in three years).
So, should the negative results of NSABP C-08 cause the closure of ECOG 5202 or should we believe that bevacizumab can benefit patients if it is continued for a longer duration? If the latter, should bevacizumab be continued for more than three years to achieve a dif-ference in three-year DFS? What refinements in the number of patients accrued would be needed to dem-onstrate a statistical difference in median DFS, given
SOLID TUMORS
Colon Cancer
IMPACTcontinued from page 1 �
Cathy Eng, MD
Associate ProfessorDepartment of Gastrointestinal Medical OncologyUniversity of TexasM.D. Anderson Cancer CenterHouston, Texas
ADVISORY BOARD EDITORIAL
The results of NSABP C-08 have significant implications for patient care, since they highlight that experimental therapies should not be used outside of a clinical trial setting.
see IMPACT, page 15 �
Micrograph of a tubular adenoma, a type of colonic polyp and a precursor of colorectal cancer.

Visit our site to get a FREE financial planning audio CD!
CO0809
THE BOOK PAGE
MCMAHONMEDICALBOOKS.COMAn Online Bookstore
ORDER ONLINEFor pricing, a more completereview and easy orderingwith a credit card, go toMcMahonMedicalBooks.com.
We can supply any medicalbook in print, so if you don’tfind the book you want,e-mail your request withbilling information [email protected].
If you are an author andwould like your medical book featured in this booksection, contactRay McMahon, Publisher, at [email protected].
TOP TEN BEST SELLERS ON MCMAHONMEDICALBOOKS.COMThese books and thousands more...
09876
54321
Abeloff's Clinical OncologyMartin D. Abeloff; James O. Armitage; John E. Niederhuber;Michael B. Kastan; W. Gillies McKenna
Carrying on the tradition established by its founding editor, the late Martin Abeloff,MD, the fourth edition of this respected reference synthesizes all of the latest oncol-ogy knowledge into one practical, clinically focused, easy-to-use volume. It incorpo-rates basic science, pathology, diagnosis, management, outcomes, rehabilitation andprevention—all in one convenient resource—equipping you to overcome your tough-est clinical challenges. What's more, you can access the complete contents of thisExpert Consult title online, and tap into its unparalleled guidance wherever and when-ever you need it most!
Financial Fund of KnowledgeMichael Reiman, CFS, RFC, DIA; Max Adams, Esq, LUTCF, CRFA
This book shares practical and insightful business and financial tips for residents andphysicians. You'll find suggestions for managing medical school loans to your ad-vantage, negotiating your employment contract, choosing asset protection strategies,taking steps to reduce tax liabilities, determining the best insurance products andinvestment tools, and avoiding typical missteps taken by physicians in their financialand business decisions.
For Doctors Only: A Guide to Working Less & Building MoreChristopher R. Jarvis, MBA; David B. Mandell, JD, MBA;Jason M. O’Dell, CWP; Claudio A. DeVellis, JD, CPA
For Doctors Only teaches doctors how to efficiently practice so they can get moreout of a medical practice. More specifically, For Doctors Only will help doctors protecttheir personal and practice assets from lawsuits, taxes and bad investments, whileshowing them the secrets to building wealth through the leverage of people, assetsand effort.
Medical Practice Management in the 21st CenturyMarjorie A. Satinsky, MBA; Randall T. Curnow, Jr., MD, MBA
This book will help physicians understand the breadth of practice management, learnthe essentials about start-up, organization and management; managing finances;recruiting and managing staff and outside resources; improving health care delivery andclinical outcomes; and ensuring compliance.
Targeted Cancer TherapyRazelle Kurzrock; Maurie Markman
Emerging technologies in target identification, drug discovery, molecular markers andimaging are rapidly changing the face of cancer. Targeted Cancer Therapy provides afoundation of knowledge in targeted cancer therapeutics.
Textbook of Lung Cancer, 2nd EditionHeine Hansen
Textbook of Lung Cancer, 2nd Edition, published in association with the EuropeanSociety of Medical Oncology, is a comprehensive and multidisciplinary text, whichexamines all aspects of this disease, with contributions from a multinational team ofauthors on etiology, epidemiology, molecular biology, pathology, smoking, detectionand management, clinical features, staging and prognostic factors, surgery, radio-therapy, and chemotherapy.
The Molecular Basis of Cancer With Expert ConsultJohn Mendelsohn; Peter M. Howley; Mark A. Israel; Joe W. Gray;Craig B. Thompson
Successfully fighting cancer starts with understanding how it begins. This thoroughlyrevised third edition explores the scientific basis for our current understanding of malig-nant transformation, and the pathogenesis and treatment of cancer. A team of leadingexperts thoroughly explains the molecular biologic principles that underlie the diag-nostic tests and therapeutic interventions now being used in clinical trials and practice.
The Washington Manual® of Oncology, Second EditionRamaswamy Govindan
This book presents the latest, most authoritative cancer management recommenda-tions in the famous fast-access Washington Manual® outline format. This edition hasbeen reorganized into three major sections: principles of oncology, site-specific dis-eases and supportive therapy.
TNM Staging AtlasPhilip Rubin; John T. Hansen
The TNM Staging Atlas presents cancer staging in a highly visual, rapid-referenceformat, with clear full-color diagrams and TNM stages by organ site. The illustrations—some original and some derived from Grant's Atlas of Anatomy—are three-dimension-al, three-planar, cross-sectional presentations of primary anatomy and regional nodalanatomy. They show the anatomic features identifiable on physical and/or radiologicexamination and the anatomic extent of cancer spread which is the basis for staging.
Wealth Protection MDChristopher R. Jarvis, MBA; David B. Mandell, JD, MBA;Celia R. Clark, JD, LLM; Glenn M. Terrones, Esq.
This book teaches doctors how to protect their personal and practice assets from law-suits, taxes, bad investments, bankruptcy and divorce by combining the expertise of afinancial planner, asset protection attorney and estate planning attorney. This compre-hensive guide explains domestic and offshore asset protection, tax-saving vehicles,captive insurance companies and more.
0
9
8
7
6
5
4
3
2
1
OR
DE
R B
OO
KS
ON
LIN
E
The bookstore division of

14 CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009
Pemetrexed Approved for Fourth Indication
The FDA has approved pemetrexed for injection (Alimta, Eli Lilly) as main-
tenance therapy for locally advanced or metastatic non-small cell lung cancer (NSCLC), specifically for patients with a nonsquamous histology whose disease has not progressed after four cycles of platinum-based first-line chemotherapy. The drug is not indicated for treatment of patients with squamous cell NSCLC. This is the fourth approval for the drug.
The drug was approved based on results from a multicenter, double-blind Phase III trial that compared efficacy with regard to overall survival of peme-trexed plus best supportive care (BSC) versus placebo plus BSC in 663 patients with stage IIIB/IV NSCLC, whose disease had not progressed after four cycles of platinum-based induction chemother-apy. The trial supported previous stud-ies looking at the use of histopathology
to tailor treatment for patients with advanced non-squamous NSCLC.
Patients in the trial were treated with pemetrexed (500 mg/m2 on day 1 of each 21-day cycle) or placebo, plus BSC. All patients were sup-
plemented with vitamin B12, folic acid and dexamethasone.
Overall, pemetrexed increased pro-gression-free survival by almost two months (4.3 vs. 2.6 months; P<0.0001) and overall survival (OS) by almost three months (13.4 vs. 10.6 months; P=0.012). However, the relative benefits of pem-etrexed maintenance were even great-er in nonsquamous cell histologies. Although there was no OS advantage in the squamous cell tumors (9.9 vs. 10.8 months; P=0.678), the survival advan-tage exceeded five months (15.5 vs. 10.3; P=0.007; hazard ratio, 0.47; P<0.0001) when the squamous cell cancers were removed from the analysis.
Opioid Pain Reliever Approved
The FDA has approved fentanyl buc-cal soluble film (Onsolis, Aveva
Drug Delivery Systems) to help man-age breakthrough pain in certain can-cer patients. Onsolis is in a class of drugs that deliver the potent opioid fenta-nyl through the mouth’s mucous mem-branes. Onsolis delivers fentanyl via an absorbable film that adheres to the inside of the cheek.
The drug is indicated for the manage-ment of breakthrough pain in patients with cancer, aged 18 and older, who already use opioid pain medication around the clock and who need and are able to safely use high doses of an addi-tional opioid medicine. Such patients are considered opioid-tolerant because of their current opioid medication use.
Because fentanyl is subject to abuse and misuse, this new drug was approved with a Risk Evaluation and Mitigation
Strategy, or REMS, which is a required plan for managing risks associated with a drug or biological product. The Food and Drug Administration Amendments Act of 2007 gave the FDA the author-ity to require that drugs and biological products have a REMS to ensure that the benefits of a drug or biological product outweigh its risks.
As part of the REMS, Onsolis will only be available through a restricted distri-bution program called the FOCUS pro-gram. Under this program, only those prescribers, patients and pharmacies reg-istered with the program will be able to prescribe, dispense and receive Onsolis. The FOCUS program will provide training
and educational materials to prescribers and pharmacy personnel, and a counsel-ing call will be placed to patients before dispensing to ensure they have been ade-quately educated about the appropriate use of the drug. Prescription orders will be filled only by participating pharmacies
that will send the medication directly to the patients’ homes.
Onsolis was approved with a boxed warning, which states that the medica-tion should not be used for the manage-ment of migraines, dental pain, or post-operative pain or by patients who use opioids intermittently, or on an as-need-ed basis. It also warns that the drug should be kept out of the reach of chil-dren and should not be substituted for other fentanyl products.
Onsolis is manufactured by Aveva Drug Delivery Systems, and marketed under license from BioDelivery Sciences International Inc., by Meda Pharmaceu-ticals Inc.
FDA NEWS
ABRAXANE® delivers
ABRAXANE for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) (albumin-bound) is indicated for the treatment of breast cancer after failure of combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy. Prior therapy should have included an anthracycline unless clinically contraindicated.
WARNING: ABRAXANE for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) (albumin-bound) should be administered under the supervision of a physician experienced in the use of cancer chemotherapeutic agents. Appropriate management of complications is possible only when adequate diagnostic and treatment facilities are readily available.ABRAXANE therapy should not be administered to patients with metastatic breast cancer who have baseline neutrophil counts of less than 1,500 cells/mm3. In order to monitor the occurrence of bone marrow suppression, primarily neutropenia, which may be severe and result in infection, it is recommended that frequent peripheral blood cell counts be performed on all patients receiving ABRAXANE.Note: An albumin form of paclitaxel may substantially affect a drug’s functional properties relative to those of drug in solution. DO NOT SUBSTITUTE FOR OR WITH OTHER PACLITAXEL FORMULATIONS.
IMPORTANT SAFETY INFORMATIONThe use of ABRAXANE has not been studied in patients with hepatic or renal dysfunction. In the randomized controlled trial, patients were excluded for baseline serum bilirubin >1.5 mg/dL or baseline serum creatinine >2 mg/dL.ABRAXANE can cause fetal harm when administered to a pregnant woman. Women of childbearing potential should be advised to avoid becoming pregnant while receiving treatment with ABRAXANE. Men should be advised to not father a child while receiving treatment with ABRAXANE.It is recommended that nursing be discontinued when receiving ABRAXANE therapy.ABRAXANE contains albumin (human), a derivative of human blood.Caution should be exercised when administering ABRAXANE concomitantly with known substrates or inhibitors of CYP2C8 and CYP3A4.ABRAXANE therapy should not be administered to patients with metastatic breast cancer who have baseline neutrophil counts of less than 1,500 cells/mm3. It is recommended that frequent peripheral blood cell counts be performed on all patients receiving ABRAXANE.
nab® defi ned: nab® technology exploits the natural properties of albumin, facilitating the delivery of water-insoluble compounds to the tumor.

CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 15
that the trial has thus far accrued more than 50% of its patients? Once open for accrual, will participating sites be will-ing to continue to enroll patients or will physicians defer enrollment altogeth-er due to the negative results of the tri-al presented at the ASCO meeting? Will an investigator be able to explain this complex trial to patients in such a way as to enhance enrollment while incor-porating the recent data from NSABP C-08, or will it be too difficult to explain
these issues so that it actually dissuades patient enrollment?
Although duplicity in a trial is not ideal, the advantage to the AVANT trial is that it may firmly establish whether there is any role for adjuvant bevacizumab in high-risk stage II or stage III patients. As men-tioned before, strict radiographic surveil-lance is required in this trial. The results of AVANT will not be available until late 2010 or early 2011, but unless AVANT fails to meet its primary end point, it is likely ECOG 5202 will remain open giv-en its unique trial design. Unfortunate-ly, for any large cooperative group tri-al such as ECOG 5202, any revisions will
require significant delays by the coop-erative group of origin, CTEP, followed by each institution’s institutional review board. This will only further delay patient accrual and our ability to answer wheth-er prognostic markers have a role in determining a plan of care for the stage II patient population and whether there is a role for bevacizumab in the high-risk stage II patient population.
Conclusion
NSABP C-08 demonstrated that we can successfully and rapidly accrue patients to a Phase III adjuvant trial. The results have significant implications for patient
care, since they highlight that experi-mental therapies should not be used out-side of a clinical trial setting. The con-trasting negative data for bevacizumab in the adjuvant (micrometastatic) setting in comparison to its well-documented effi-cacy in (macro)metastatic disease may eventually help us better understand the role and actual mechanism of action of anti-VEGF therapy in malignant tumors. This may open the door for future clini-cal trial design based on a better under-standing of the biologic implications of anti-angiogeneic therapy.
—Cathy Eng, MD
SOLID TUMORS
Colon
IMPACTcontinued from page 12 �
Patients should not be retreated with subsequent cycles of ABRAXANE until neutrophils recover to a level >1,500 cells/mm3 and platelets recover to a level >100,000 cells/mm3.In the case of severe neutropenia (<500 cells/mm3 for 7 days or more) during a course of ABRAXANE therapy, a dose reduction for subsequent courses is recommended. Sensory neuropathy occurs frequently with ABRAXANE. If grade 3 sensory neuropathy develops, treatment should be withheld until resolution to grade 1 or 2 followed by a dose reduction for all subsequent courses of ABRAXANE.Severe cardiovascular events possibly related to single-agent ABRAXANE occurred in approximately 3% of patients in the randomized trial. These events included chest pain, cardiac arrest, supraventricular tachycardia, edema, thrombosis, pulmonary thromboembolism, pulmonary embolism, and hypertension. In the randomized metastatic breast cancer study, the most important adverse events included alopecia (90%), neutropenia (all cases 80%; severe 9%), sensory neuropathy (any symptoms 71%; severe 10%), asthenia (any 47%; severe 8%), myalgia/arthralgia (any 44%; severe 8%), anemia (all 33%; severe 1%), infections (24%), nausea (any 30%; severe 3%), vomiting (any 18%; severe 4%), diarrhea (any
27%; severe <1%), and mucositis (any 7%; severe <1%). Other adverse reactions have included ocular/visual disturbances (any 13%; severe 1%), fl uid retention (any 10%; severe 0%), hepatic dysfunction (elevations in bilirubin 7%, alkaline phosphatase 36%, AST [SGOT] 39%), renal dysfunction (any 11%; severe 1%), thrombocytopenia (any 2%; severe <1%), hypersensitivity reactions (any 4%; severe 0%), cardiovascular reactions (severe 3%), and injection site reactions (<1%). During postmarketing surveillance, rare occurrences of severe hypersensitivity reactions have been reported with ABRAXANE.Reference: 1. ABRAXANE [prescribing information]. Los Angeles, Calif: Abraxis Oncology, a division of Abraxis BioScience, Inc; August 2007. Please see the Brief Summary of the ABRAXANE full prescribing information on the next page.ABRAXANE, Abraxis, Abraxis Oncology, nab, and ARC of Support are registered trademarks, and Abraxis Oncology Resource Center is a service mark, of Abraxis BioScience, LLC. Abraxis Oncology® is a division of Abraxis BioScience, LLC.©2009 Abraxis BioScience, LLC. All Rights Reserved. AO 1305 06/09Printed in USA
®
SM
efficacy* to make more possible
BOUND AND DETERMINED
In a pivotal phase III trial in metastatic breast cancer patients,
ABRAXANE® delivered nearly double the overall response rate* vs solvent-based paclitaxel1
15.5% vs 8.4%(P=NS) for study patients who failed combination chemotherapy or relapsed within 6 months of adjuvant chemotherapy.1
95% Cl, 9.3% to 21.8% for ABRAXANE95% Cl, 3.9% to 12.9% for solvent-based paclitaxel
21.5% vs 11.1%(P=.003) for all study patients.1
95% Cl, 16.2% to 26.7% for ABRAXANE95% Cl, 6.9% to 15.1% for solvent-based paclitaxel

16
Longer Time Between Neoadjuvant Therapy, Surgery Recommended For Rectal Cancer
Hollywood, Fla.—Surgeons should wait at least eight weeks after neoadju-vant therapy before resecting rectal can-cers, according to a new study.
In the study, waiting more than eight weeks after neoadjuvant therapy resulted in higher pathologic complete response (CR) rates and lower rates of recur-rence, without any increase in postoper-ative complications, investigators found. The study results were presented at the American Society of Colon and Rectal Surgeons annual meeting (abstract S1).
In the analysis, 177 patients with stage II and III rectal cancer undergoing neo-adjuvant chemoradiation and surgery were identified from a prospectively maintained database of patients with col-orectal cancer. Adjuvant chemotherapy was 5-FU-based and median radiother-apy dose was 5,040 cGy (range 4,000-6,100 cGy). The operations included both abdominoperineal resections (29%) and low anterior resections (71%).
Patients were retrospectively divided into two groups based on time to surgery (median, eight weeks); 86 patients under-went surgery at four to seven weeks and 91 patients at eight to 14 weeks. The inves-tigators’ primary outcomes were com-plete pathologic response, disease recur-rence and survival rates, and short-term surgical outcomes.
None of the surgical outcomes were statistically different between the groups; in particular, rates of blood loss, anasto-motic leaks and wound infections all were similar regardless of the time of surgery. Oncologic outcomes, however, were significantly better in several mea-sures among the patients who under-went resection at more than eight weeks. In particular, both pathologic CR (17% vs. 31%; P=0.03) and three-year local recur-rence rates (11% vs. 1%; P=0.04) were bet-ter. Five-year disease-free and overall sur-vival rates were better in the group that had surgery later as well, but neither was statistically significant.
“An interval of greater than eight weeks resulted in higher patholog-ic complete response rate, lower local recurrence, regardless of the tumor response, with no changes in perioper-ative complications,” said Luiz F. Cam-pos-Lobato, a surgeon in the Division of Colorectal Surgery at Cleveland Clinic in Ohio, and lead author of the study. “We recommend an interval between neoadjuvant [therapy] and surgery of at least eight weeks due to its safety and oncological benefits.”
—Gabriel Miller
SOLID TUMORS
Rectal

Guide to the Prevention of Chemotherapy
Medication ErrorsCauses of Chemotherapy Errors
DWIGHT D. KLOTH, PHARMD, FCCP, BCOPDirector of Pharmacy
Fox Chase Cancer CenterPhiladelphia, Pennsylvania
Medication error prevention
is a critical goal for
pharmacists, nurses,
and physicians in all treatment
settings—especially in oncology.
Antineoplastic agents have a lower therapeutic index and safety margin than do other drug classes. Addition-ally, in cancer chemotherapy, the dose, dosing interval, and even the route of administration may vary as a function of the tumor type and the stage of disease. Chemotherapy-related medication errors, such as the administration of a 10-fold higher dose as a result of a transcription error, or the intrathecal administration of drugs that only should be administered by IV infusion, are potentially fatal.1-4
In 2006, the Institute of Medicine (IOM) released the landmark report Preventing Medication Errors,5 which stated that “medication errors harm at least 1.5 million patients every year in hospitals, long-term facilities, and outpatient clinics, resulting in billions of dollars in addi-tional medical costs.” To help prevent medication errors, the committee recommended that all organizations
implement an electronic prescribing and dispensing system by 2010. Additionally, the report contained sev-eral other important recommendations pertinent to facilities that treat patients with cancer:
monitor medication safety literature; • develop and implement a structured error-avoidance • plan; establish a routine procedure for double-checking • filled prescriptions; designate a practice-wide medication safety offi-• cer with widespread authority and responsibility to improve care; create a safer work environment by looking at light-• ing and noise levels, minimizing distractions, and improving drug storage areas by separating look-alike and sound-alike medications;
Part 1 of a 2-Part Series
1INDEPEND ENT LY DEVELOPED BY MCMAHON PUBL ISHING CL IN ICAL ONCOLOGY NEWS • JULY/AUGUST 2009
PRINTER-FRIENDLY VERSION AT CLINICALONCOLOGY.COM

continuously evaluate technology and automation to • reduce medication errors; be assertive in requesting resources to promote • accurate medication prescribing, processing, dis-pensing, and administration; and involve patients in an aggressive education and rec-• onciliation program.This 2-part educational review is intended to help
clinicians develop practical strategies to recognize and prevent chemotherapy medication errors. Part 1 includes information on selected publicized chemo-therapy errors and their outcomes as well as exam-ples of potential causes of errors, such as look-alike/sound-alike drug names and the use of handwritten orders. Part 2, which will be published in an upcom-ing issue, discusses how health care professionals can assess the risk for medication errors at their institu-tions and practice sites and offers strategies to help prevent such errors. Because nearly all authorities rec-ommend implementation of an electronic order entry system, this guide discusses the use of technology and computerization (eg, computerized prescriber order entry [CPOE] and bar coding) in medication error pre-vention, including the advantages of and caveats to these technologies.
Causes of Chemotherapy ErrorsThe consequences of antineoplastic drug errors can be
devastating because these agents have one of the lowest therapeutic indices and safety margins of any drug class. Combination chemotherapy regimens are very complex and intensive. Doses can vary tremendously for different diseases. For example, a “normal” dose of methotrexate can range from 10 to 20,000 mg, and appropriate total doses and infusion durations of regimens for 5-fluoroura-cil (5-FU) for colorectal cancer can vary widely, even for the same tumor type and stage of disease. Similarly, tar-geted agents such as bevacizumab (Avastin, Genentech) now include FDA-approved labeling at substantially dif-ferent dose intensities, even within the colorectal cancer arena—that is, 5 mg/kg every 14 days if given with FOLFIRI (a chemotherapy regimen for colon cancer comprising irinotecan [Camptosar, Pfizer Oncology], 5-FU, and leu-covorin)6,7 and 10 mg/kg every 14 days if given in conjunc-tion with FOLFOX (a chemotherapy regimen for colon cancer combining oxaliplatin [Eloxatin, Sanofi-Aventis], 5-FU, and leucovorin).8 This 100% dose variation is yet another potential opportunity for errors, although the clinical risks for such errors are not as clearly defined as with conventional cytotoxic anticancer therapies.
Several publicized accounts of chemotherapy med-ication errors have appeared in the scientific and lay press within the past decade9-26 (Table 1), reflecting the small to nonexistent margin of error that health professionals have when ordering, dispensing, and administering cytotoxic agents. Medication safety was recently evaluated in the ambulatory chemother-apy setting, where most antineoplastic drug doses are administered. Gandhi and colleagues24 reviewed
10,112 medication orders in 1,606 patients (15% pedi-atric) and found an error rate of 3%, including 2% of orders with the potential to cause harm. Pharmacists and nurses intercepted 45% of potential adverse drug events before they reached the patient.
Errors occur not only at private practice oncology offices and smaller, nonspecialty hospitals but also at renowned teaching and research centers. Although some errors involve only one practitioner, in clinical experience most errors occur when several staff mem-bers are involved. These incidents often are the result of a lack of critical information or the presence of inac-curate data.25 Significant potential causes of chemo-therapy errors are highlighted in Table 2.6,8,27
LOOK-ALIKE/SOUND-ALIKE DRUG NAMES
One of the most common causes of medication errors is the similar-sounding names of drugs used in oncology practice.28 For example, fatal errors have occurred when the dose for one drug was mistaken for the dose of another (eg, when vincristine was dis-pensed instead of vinblastine, when docetaxel [Tax-otere, Sanofi-Aventis] was administered instead of paclitaxel, and when cisplatin was administered instead of carboplatin).11,12,26 A theoretical risk is the poten-tial for confusion between conventional paclitaxel (eg, Taxol, Bristol-Myers Squibb) and the new albu-min-bound paclitaxel, Abraxane (Abraxis Oncology), because the doses for these 2 versions of paclitaxel are not identical. One could argue that the risk for con-fusion between the albumin-bound paclitaxel and con-ventional paclitaxel is even greater than the risk for confusing cisplatin with carboplatin or vincristine with vinblastine. Additionally, concerns have been raised because the official generic name for Abraxane, pacli-taxel protein-bound particles for injectable suspension (albumin bound), is neither intuitive or manageable for paper-based systems nor feasible for computer data-base entries. Thus, this medication, like liposomal dox-orubicin (Doxil, Tibotec Therapeutics), is an example of an instance where the trade name may be the most practical and feasible drug name to use to maximize safety in everyday practice. Oncology treatment cen-ters (hospitals and practices) recognize that doxo-rubicin dosing and liposomal doxorubicin dosing are not the same and should not be substituted for each other. The same concern exists for conventional pacli-taxel and albumin-bound paclitaxel and the same level of precautions should be taken. In fact, the package insert for Abraxane carries the following warning29: Note: An albumin form of paclitaxel may substantially affect a drug’s functional properties relative to those of drug solution. DO NOT SUBSTITUTE FOR OR WITH OTHER PACLITAXEL FORMULATIONS.
One method practitioners can use to differentiate chemotherapeutic drugs with similar-sounding names is to use TALL MAN lettering on labels and electronic records: CISplatin versus CARBOplatin; vinBLASTine ver-sus vinCRISTine or vinORELbine; DOXOrubicin versus
INDEPENDENT LY DEVELOPED BY MCMAHON PUBL ISHING2

LIPOSOMAL DOXOrubicin; DOCEtaxel versus PACLI-taxel; and mitoMYCIN versus mitoXANTRONE. However, as stated above, in some cases the trade name actually may be the best choice available.
At Fox Chase Cancer Center (FCCC), in Philadelphia, the pharmacy computer system allows use of both TALL MAN lettering and scalable fonts for chemotherapy IV bag or syringe labels, enabling further differentiation
of drug names. Additionally, use of supplemental labels or stickers in different bright colors highlights and dis-tinguishes between various agents of a particular drug class (eg, a neon green DOCETAXEL sticker sharply dis-tinguishes a docetaxel dose from a paclitaxel dose with a neon purple PACLITAXEL sticker)—an important distinc-tion when these drugs sound alike, are used for the same tumor types, and may be given to patients seated next to each other in a busy infusion center, but have signifi-cantly different dosing regimens and toxicity profiles.
HANDWRITTEN PRESCRIPTION DRUG ORDERS
Some consider a CPOE system to be the best preven-tion for medication errors; however, most oncologists still handwrite orders, often because commercially available
INDEPENDENTLY DEVELOPED BY MCMAHON PUBL ISHING 3
Table 2. Examples of Potential Causes Of Chemotherapy Medication Errors
Miscommunicated verbal orders
Total course (or cycle) dose given every day
Lack of pertinent patient health care information (eg, lab data and patient demographics such as age, height, and weight)
Use of incorrect patient information/lab data or the information/lab data for a different patient
Excessive interruptions during order processing or dose preparation
Substantial distance between the pharmacy and the patient treatment area, which inhibits communication between pharmacy, nursing, and medical staff
Poor packaging and labeling by manufacturers
Use of abbreviations of drug names
Similar-sounding drug names within the therapeutic class
Lack of a proper copy of the physician order or use of a fax copy, which might be illegible
Use of trade names, which may vary even for generically available agents, rather than generic names
Lack of procedures (eg, using larger volumes for vincristine doses) and warning stickers/labels to prevent inadvertent intrathecal administration of drugs such as vincristine, doxorubicin, and daunorubicin
Failure to round drug doses to the nearest whole integer, potentially leading to a 10-fold overdose if the decimal point is not seen
Widely differing dosing regimens for the same drug even for the same tumor type and stage (eg, various regimens of 5-fluorouracil and bevacizumab in colorectal cancer)
Use of outdated lab data (eg, outdated serum creatinine or liver function tests)
Adapted from references 6, 8, and 27.
Table 1. Selected Publicized Chemotherapy Medication Errors And Outcomesa
Drug Error and Outcome
Amphotericin B and liposomal amphotericin9
Conventional amphotericin B administered at liposomal amphot-ericin doses: multiple patient deaths
Carboplatin10 Overdose administered to 2 chil-dren: possible deafness in 1 child
Carboplatin and cisplatin11
Confusion of proper dose ranges; cisplatin administered at dose intensity appropriate for carboplatin: consistently fatal outcome (numerous examples prior to labeling changes in 1996)
Docetaxel and conventional paclitaxel12
An incorrect dose of 260 mg docetaxel (Taxotere, Sanofi-Aventis) was administered instead of 260 mg conventional paclitaxel (Taxol, Bristol-Myers Squibb): patient died 5 days later, although the error may not have caused the death
Doxorubicin hydrochloride and liposomal doxorubicin13,14
Liposomal doxorubicin adminis-tered instead of doxorubicin hydro-chloride: increased morbidity and possible cause of patient death
Lomustine13,15 Serious errors have occurred when this oral agent was administered daily rather than every 6 weeks: patient harm, prolonged hospital-ization, and death
Methotrexate16-18 Multiple cases of accidental daily administration of oral methotrexate when weekly dosing was intended: at least 25 fatalities and an equal number of incidents of serious patient harm
Vincristine19-25 Accidental intrathecal administra-tion: multiple patient deaths over many years (universally fatal when this error occurs): patient harm
Vincristine and vinblastine26
Vincristine accidentally given at dose appropriate for vinblastine; patient death
a Not all-inclusive; selected examples are given here to illustrate the nature of the error. Some examples have occurred numerous times in the literature.

software simply is not available; when it is available it often is poorly written, incompatible with other existing computer systems, or otherwise unreliable. As a result, other safety steps remain vital.
In one such example, FCCC banned chemotherapy drug name abbreviations (eg, CPT-11, which might indi-cate irinotecan or cisplatin) from all chemotherapy order forms in 1995. Trade names are still permitted and in some cases encouraged (eg, Doxil to indicate liposomal dox-orubicin) in response to such recommendations by the Institute for Safe Medication Practices (ISMP; www.ismp.org). The ISMP has a comprehensive list of error-prone
abbreviations, symbols, and dose designations that can be used as a benchmark to improve patient safety (Table 3).30 Table 4 lists antineoplastic ordering terms and shows some potentially problematic names and abbrevi-ations. In the absence of a CPOE system, strict enforce-able rules for medication orders should be in place (eg, write “daily” instead of “qd” and “units” instead of “U”). “If in doubt, write it out” is a mantra adopted by many leading health systems. The Joint Commission also rec-ognizes the risks associated with various error-prone abbreviations and mandates that hospitals and health systems create and periodically review and update a list of error-prone abbreviations that are not permitted in any component of the medical record.31
CLARIFYING TERMS
Another problem is a “disconnect” in the commu-nication system, in which prescribers think of antineo-plastic drug therapy as a “course” or a “cycle,” which is usually several doses, whereas pharmacists and nurses evaluate, prepare, and administer a single dose. Addi-tionally, a decimal point can be missed if the prescriber fails to round doses of more than 5 or 10 mg to the nearest whole number, which can potentially cause a 10-fold overdose.30 Similarly, the unwise use of a “trail-ing zero” or “leading decimal” also has the potential to cause a 10-fold dosage error.30
DEADLY DRUG ADMINISTRATION ERRORS
The inadvertent intrathecal administration of drugs such as vincristine, doxorubicin, and daunorubicin con-tinues to occur and almost always is fatal. From an order-entry standpoint, these errors could be avoided if all pharmacy computer systems had an automatic “dead stop” whenever a pharmacist tried to enter one of these drugs to be administered intrathecally. All manufactur-ers of vincristine include auxiliary warning labels that state: “Fatal if given intrathecally, for IV use only. Do not remove covering until moment of injection.”32 Tragic deaths ensue because some practitioners choose not to use this United States Pharmacopeia-required label; and in some cases, the labels have been used by the phar-macy department but with no protective effect at the patient bedside.21,33,34 For example, in 2003, a patient at a university hospital in New Jersey died after mis-takenly being injected intrathecally with vincristine—by a board-certified radiologist—despite the warning label that the drug is fatal if administered this way.21
Because pharmacists are not routinely at the bed-side when lumbar puncture procedures are performed, pharmacy CPOE warnings and/or syringe labeling can-not ensure the prevention of this error. Some researchers have suggested routinely diluting all vincristine doses in 50-mL IV piggyback (IVPB) bags to prevent recurrences of this type of error.35,36 Before employing this approach, one is encouraged to consider the possible morbidities associated with increased extravasation risk. This pres-ents a struggle for balance between the prevention of fatal errors versus the prevention of more frequent
INDEPENDENT LY DEVELOPED BY MCMAHON PUBL ISHING4
Table 3. Error-Prone Medical Transcription
AVOID…(Error-Prone Transcription)
USE…(Strongly Recommended Transcription)
qd or QD daily
qn, qhs, hs, BT (bedtime) at bedtime
q 6pm 6 p.m. nightly
qod or QOD every other
×3d × 3 days
tiw or TIW 3 times weekly
μg or Ug mcg (for micrograms)
U, IU, u units
cc mL
SS sliding scale
per os (misread as “left eye”)
PO, by mouth, or orally
SC, subQ, SQ subcutaneous
od right eye
os left eye
AU both ears
terminal zeros for doses expressed in whole num-bers (eg, AVOID 1.0 mg …)
instead USE 1 mg
failure to use a zero before a decimal point when the dose is less than a whole unit (eg, AVOID .1 mg …)
instead USE 0.1 mg
lack of a space between the drug name, dose, and unit of measure (eg, AVOID vinblastine10mg …)
instead USE vinblastine 10 mg
Adapted from reference 30.

INDEPENDENTLY DEVELOPED BY MCMAHON PUBL ISHING 5
Table 4. Antineoplastic Ordering Terms and Routes of Administration
Ideal Generic Drug Names
Not Ideal Branda/Generic Drug Names and Abbreviations
Most Common Administration Route(s)
Albumin-bound paclitaxel Abraxane Intravenous
Aldesleukin Proleukin, interleukin-2 (IL-2) Intravenous, subcutaneous
Alemtuzumab Campath, mono clonal antilymphocyte antibody Intravenous
Altretamine Hexalen, hexamethylmelamine (HMM) Oral
Amifostine Ethyol, Ethiofos, Gammaphos, WR2721 Intravenous
Aminoglutethimide Cytadren, Elipten Oral
Anastrozole Arimidex Oral
Arsenic trioxide Trisenox intravenous
Asparaginase Elspar, Colaspace, ASN-ase Intramuscular, intravenous
Azathioprine Imuran Intravenous, oral
Bendamustine Treanda Intravenous
Bexarotene Targretin Oral
Bicalutamide Casodex Oral
Bleomycin Blenoxane, Bleo Intravenous, intramuscular, subcutaneous
Busulfan Myleran, Busulfex Oral
Capecitabine Xeloda, Ro 09-1978 Oral
Carboplatin Paraplatin, CBDCA Intravenous
Carmustine BiCNU, bischloronitrosourea (BiCNU) Intravenous
Chlorambucil Leukeran Oral
Cisplatin Platinol, cis-diaminedichloro-platinum (CDDP) Intravenous, intraperitoneal
Cladribine Leustatin, 2-chlorodeoxyadenosine (2-CdA), CDA Intravenous, subcutaneous
Clofarabine Clolar Intravenous
Cyclophospha mide Cytoxan, Neosar, CTX, CPM, CYT Intravenous, oral
Cytarabine Cytosar-U, Tarabine, aytosine, cytosine arabinoside (Ara-C)
Intravenous, intrathecal
Dacarbazine DTIC-Dome, DIC, imid azole carboxamide Intravenous
Dactinomycin Cosmegen, Actinomycin-D (ACT-D) Intravenous
Dasatinib Sprycel Oral
Daunorubicin Cerubidine, Daunomycin, Rubidomycin, DNR Intravenous
Denileukin diftitox Ontak, LY-335348 Intravenous
Dexrazoxane Zinecard, ICRF-187, ADR-529 Intravenous
Docetaxel Taxotere, RP-56976 Intravenous
Doxorubicin Adriamycin, Rubex, Adria Intravenous, intraperitoneal
Doxorubicin liposome Doxil Intravenous
Epirubicin Ellence, 4'-epidoxorubicin (EPI) Intravenous
Erlotinib Tarceva Oral
Estramustine Emcyt Oral
Etoposide Etopophos, VePesid, VP-16, EPEG Intravenous, oral, intrapleural
(continued on next page)

INDEPENDENT LY DEVELOPED BY MCMAHON PUBL ISHING6
Table 4. Antineoplastic Ordering Terms and Routes of Administration
Ideal Generic Drug Names
Not Ideal Branda/Generic Drug Names and Abbreviations
Most Common Administration Route(s)
Everolimus Afinitor Oral
Exemestane Aromasin, Nikidess Oral
Floxuridine Fluorodeoxyuridine (FUDR) Intravenous
Fludarabine Fludara, FAMP Intravenous
Fluorouracil Adrucil, Efudex, 5-FU Intravenous, topical
Flutamide Eulexin, Niftolid Oral
Gemcitabine Gemzar, LY-18801 Intravenous
Goserelin Zoladex, ICI-118630 Subcutaneous
Hydroxyurea Hydrea, Droxia, Mylocel, hydroxycarbamide Oral
Idarubicin Idamycin, 4-demethoxydaunorubicin, IDR, IDA Intravenous
Ifosfamide Ifex, IFX Intravenous
Imatinib Gleevec, STI-571 Oral
Interferon alfa Roferon-A, Intron A, IFN Intramuscular, subcutaneous
Irinotecan Camptosar, CPT-11 Intravenous
Isotretinoin Accutane, 13-cis-retinoic acid (13-CRA) Oral
Ixabepilone Ixempra Intravenous
Lapatinib Tykerb Oral
Lenalidomide Revlimid Oral
Letrozole Femara Oral
Leucovorin Wellcovorin, citrovorum factor, folinic acid (FA), LV Intravenous, oral
Leuprolide Lupron, Lupron Depot, leuprorelin Intramuscular, subcutaneous
Levamisole Ergamisol, l-tetramisole, ICI-59623 Oral
LEVO-leucovorin Fusilev, leucovorin, L-leucovorin Intravenous
Lomustine CeeNU, CCNU, bis-chloro-nitrosourea Oral
Mechlorethamine Mustargen, Chlore thazine, HN2, nitrogen mustard Intravenous, topical
Medroxyprogesterone Provera, Depo-Provera Oral, intramuscular
Megestrol Megace Oral
Melphalan Alkeran, phenylalanine mustard, L-PAM Oral, intravenous
Mercaptopurine Purinethol, 6-MP Oral
Mesna Mesnex, sodium 2-mercaptoethane sulfonate Intravenous, oral
Methotrexate Amethopterin, MTX, Folex Intravenous, oral, intrathecal
Mitomycin Mutamycin, mitomycin-c Intravenous
Mitotane Lysodren, o,p'-DDD Oral
Mitoxantrone Novantrone, DHAD, DHAQ Intravenous, intraperitoneal
Nelarabine Arranon Intravenous
Nilotinib Tasigna Oral
This information is based on the prescribing information for each drug.a Brand names are listed in bold.
(continued)

non–life-threatening, albeit severe, adverse events (eg, vesicant drug extravasation when a drug is administered from an IVPB minibag into a peripheral IV line). In cases when a 50-mL IVPB vincristine, vinblastine, or vinorel-bine dose might present excessive risk for extravasation, some centers use 20- or 30-mL fixed-volume syringes for all vinca alkaloid medication doses, with warning stickers and label text, to achieve the same purpose—namely, making the drug volume too large to be acciden-tally administered intrathecally.
Prevention of vincristine administration errors was
reviewed in a 2005 Sentinel Event Alert issued by the Joint Commission.37 The alert was distributed to all health care organizations in the United States. More recently, the ISMP has recommended revised wording for sup-plemental stickers applied to vinca medication doses. Specifically, the ISMP no longer recommends “NOT for Intrathecal Use” based on the concern that the presence of the word “intrathecal” may contribute to confusion if the sticker is not read completely or becomes dam-aged.38 The ISMP now recommends supplemental warn-ing stickers that include the following text: “For IV Use
INDEPENDENTLY DEVELOPED BY MCMAHON PUBL ISHING 7
Table 4. Antineoplastic Ordering Terms and Routes of Administration
Ideal Generic Drug Names
Not Ideal Branda/Generic Drug Names and Abbreviations
Most Common Administration Route(s)
Octreotide Sandostatin, 1-cysteinamide, SMS Subcutaneous
Oprelvekin Neumega, interleukin-11 (IL-11), rIL-11 Subcutaneous
Oxaliplatin Eloxatin, diamino cyclohexane platinum Intravenous
Paclitaxel Taxol, TX, PCL, PCT, TX Intravenous
Pegaspargase Oncaspar, polyethylene glycol L-asparaginase Intramuscular
Pemetrexed Alimta Intravenous
Pentostatin Nipent, co-vidarabine, 2-deoxycoformycin (DCF) Intravenous
Plicamycin Mithramycin, Mithracin, aureolic acid Intravenous
Prednisone Deltasone Oral
Procarbazine Matulane, Natulana, N-methylhydrazine Oral
Rituximab Rituxan, IDEC-C2B8 Intravenous
Sorafenib Nexavar Oral
Streptozocin Zanosar Intravenous
Sunitib Sutent Oral
Tamoxifen Nolvadex Oral
Temozolomide Temodar Oral
Temsirolimus Torisel Intravenous
Thalidomide Thalomid Oral
Thioguanine Tabloid, 6-thioguanine (6-TG), TG, WR-1141 Oral
Thiotepa TESPA, Thioplex, WR-45312 Intravenous, intravesical
Topotecan Hycamtin, SKF-104864 Intravenous
Toremifene Fareston, EC-11570 Oral
Trastuzumab Herceptin, anti-HER2 antibody Intravenous
Tretinoin Vesanoid, all trans-retinoic acid (ATRA) Oral
Trimetrexate NeuTrexin, TMQ, TMTX Intravenous
Vinblastine Velban Intravenous
Vincristine Oncovin, Vincasar Intravenous
Vinorelbine Navelbine Intravenous
This information is based on the prescribing information for each drug.a Brand names are listed in bold.

For a pocket guide version of The Guide to the Prevention of Chemotherapy Medication Errors, visit www.CLINICALONCOLOGY.COM
Only: Fatal if given by other routes.”38 Recommendations for preparing, dispensing, and
administering IV vincristine and other vinca alkaloids (in addition to diluting vincristine and affixing the required warning labels) include conducting a “time out” with at least 2 licensed, qualified health care profession-als to independently review the drug, dose, and route at the time of pharmacy preparation, as well as separating the dispensing of vincristine from other antineoplastics that may be given by the intrathecal route as part of the treatment regimen. In Australia, pharmacists are lobby-ing the national governmental organization to abolish the syringe as a vehicle to administer vincristine.39
As this discussion illustrates, significant differences of opinion remain regarding the best (and safest) manner to avoid fatal accidental intrathecal administration of vin-cristine and other vinca alkaloids in light of the significant risk for severe local tissue injury if an IVPB dose of a vinca extravasates during a peripheral line administration.39
ReferencesBeckwith MC, Tyler LS. Preventing medication errors with antineo-1. plastic agents, part 1. Hosp Pharm. 2000;35(5):511-525.
Womer RB, Tracy E, Soo-Hoo W, Bickert B, DiTaranto S, Barn-2. steiner JH. Multidisciplinary systems approach to chemotherapy safety: rebuilding processes and holding the gains. J Clin Oncol. 2002;20(24):4705-4712, PMID: 12488417.
Müller T. Typical medication errors in oncology: analysis and 3. prevention strategies. Onkologie. 2003;26(6):539-544, PMID: 14704927.
Schulmeister L. Preventing chemotherapy errors. 4. Oncologist. 2006;11(5):463-468, PMID: 16720846.
Aspden P, Wolcott J, Bootman JL, Cronenwett LR, eds, for the 5. Committee on Identifying and Preventing Medication Errors. Pre-venting Medication Errors: Quality Chasm Series. Washington, DC: National Academy Press; 2006.
Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus 6. irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335-2342, PMID: 15175435.
Avastin [prescribing information] South San Francisco, CA: 7. Genetech; May 2009.
Giantonio BJ, Catalano PJ, Meropol NJ, et al. Bevacizumab 8. in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal can-cer: results from the Eastern Cooperative Oncology Group study E3200. J Clin Oncol. 2007;25(12):1539-1544, PMID: 17442997.
Institute for Safe Medication Practices. Urgent Drug Safety Message. 9. Medication errors with certain lipid-based products. http://www.ismp.org/newsletters/acutecare/articles/19980818.asp. Accessed July 16, 2009.
Chemotherapy overdoses for 2 Children at Johns Hopkins. 10. The New York Times. August 2, 2002. http://www.nytimes.com/2002/08/02/us/national-briefing-health-and-science-che-motherapy-overdoses-for-2-children.html?n=Top/Reference/Times%20Topics/Organizations/J/Johns%20Hopkins%20Univer-sity. Accessed April 15, 2009.
Fritsch J. Syracuse hospital admits causing death of patient. 11. The New York Times. May 13, 1992. http://www.nytimes.com/1992/05/13/nyregion/syracuse-hospital-admits-causing-death-of-patient.html. Accessed July 16, 2009.
ISMP Medication Safety Alert 2/7/01. FDA Advise-ERR: Medication 12. errors associated with taxotere and taxol. http://www.ismp.org/newsletters/acutecare/articles/20010207.asp. Accessed July 16, 2009.
ISMP Medication Safety Alert 10/21/04. http://www.ismp.org/13. MSAarticles/A4Q04Action.htm. Accessed July 16, 2009.
Hazard Medication Alert. 8/18/98. MSA Acute Care Edition 14.
Newsletter. http://www.ismp.org/hazardalerts/lipid.asp. Accessed July 16, 2009.
Institute for Safe Medication Practices. Medication Safety Alert 15. 7/15/04. Lowdown on lomustine: we’d hate CEENU make this mistake. http://www.ismp.org/newsletters/acutecare/arti-cles/20040715.asp. Accessed July 16, 2009.
Moore TJ, Walsh CS, Cohen MR. Reported medication errors 16. associated with methotrexate. Am J Health Syst Pharm. 2004;61(13):1380-1384, PMID: 15287234.
National Patient Safety Agency. Reducing the harm caused by 17. oral methotrexate. http://www.nacc.org.uk/downloads/factsheets/npsaMethotrexateAlert.pdf. Accessed July 16, 2009.
Institute for Safe Medication Practices. Medication Safety Alert 18. 12/3/02. http://www.ismp.org/hazardalerts/ha.pdf. Accessed July 16, 2009.
Institute for Safe Medication Practices. Medication Safety Alert 19. 4/5/00. Pain, paralysis, and knowledge of impending death marks intrathecal vincristine. http://www.ismp.org/ newsletters/acute-care/articles/20000405.asp. Accessed July 16, 2009.
Berwick DM. Not again! Preventing errors lies in redesign—not 20. exhortation. BMJ. 2001;322(7281):247-248, PMID: 11157508.
Narayanan A. Family tells of tragedy following fatal injection. 21. The Home News Tribune. April 17, 2003. http://www.thnt.com/thnt/story10,21282,723614,00.html. Accessed April 15, 2009.
Bennett C. Is jail the answer for fatal negligence?22. Guardian (UK). September 25, 2003. http://www.guardian.co.uk/uk/2003/sep25/ukcrime.comment. Accessed April 15, 2009.
Cohen MR. Vincristine therapy: days “4-11” misunderstood as days 23. 4 through 11. Hosp Pharm. 2006;41(9):811-815.
Gandhi TK, Bartel SB, Shulman LN, et al. Medication safety in the 24. ambulatory chemotherapy setting. Cancer. 2005:104(11):2477-2483, PMID: 16245353.
Alcaraz A, Rey C, Concha A, Medina A. Intrathecal vincristine: fatal 25. myeloencephalopathy despite cerebrospinal fluid perfusion. J Toxi-col Clin Toxicol. 2002;40(5):557-561, PMID: 12215050.
Twedt S. Deadly hospital mistakes are doomed to be repeated. 26. Pittsburgh Post-Gazette. October 24, 1993;section A,1.
Kloth DD. Prevention of chemotherapy medication errors. 27. J Pharm Pract. 2002;15(1):17-31.
Joint Commission. Sentinel Event Alert. Look-alike, sound-alike 28. names. 2001. http://www.jointcommission.org/SentinelEvents/Sen-tinelEventAlert/sea_19.htm. Accessed July 16, 2009.
Abraxane [prescribing information]. Los Angeles, CA: Abraxis 29. Oncology; August 2007.
Institute for Safe Medication Practices. ISMP’s List of Error-Prone 30. Abbreviations, Symbols, and Dose Designations. http://www.ismp.org/Tools/errorproneabbreviations.pdf. Accessed April 15, 2009.
The Joint Commission. Official “Do Not Use” list. http://www.31. jointcommission.org/NR/rdonlyres/2329F8F5-6EC5-4E21-B932-54B2B7D53F00/0/dnu_list.pdf. Accessed July 16, 2009.
Vincristine [product label]. http://patient.cancerconsultants.com/32. druginserts/vincristine.pdf. Accessed July 20, 2009.
Dyer C. Junior doctor charged with manslaughter after medical 33. error [news item]. BMJ. 2002;325(7365):616, PMID: 12269306.
Dyer C. Doctor sentenced for manslaughter of leukaemia patient 34. [news item]. BMJ. 2003;327(7417):697, PMID: 14512453.
Davis NM. The preparation of vincristine in minibags will prevent 35. deadly medication errors. Hosp Pharm. 2001;36(7):707.
Trissel LA, Zhang Y, Cohen MR. The stability of diluted vincris-36. tine sulfate used as a deterrent to inadvertent intrathecal injection. Hosp Pharm. 2001;36(7):740-745.
Joint Commission. Sentinel Event Alert. Preventing vincristine 37. administration errors. http://www.jointcommission.org/sentinelEv-ents/SentinelEventAlert/sea_34.htm. Accessed July 16, 2009.
Institute for Safe Medication Practices. Medication Safety Alert 38. Nurse Advise-ERR. 2008;6(10).
Gilbar PJ, Carrington CV. The incidence of extravasation of vinca 39. alkaloids supplied in syringes or mini-bags. J Oncol Pharm Pract. 2006;12(2):113-118, PMID: 16984750.
8

McMahon Publishing was founded in
1972 by Raymond E. McMahon. McMahon
Publishing has grown to become one
of the nation’s largest family-owned
medical publishers, with a projected
2009 annual revenue of roughly
$23 million across all product categories.
Today, McMahon publishes a broad array of medical
newsmagazines in various specialties, including oncol-
ogy, anesthesiology, gastroenterology, general surgery,
hospital pharmacy, infectious diseases, and pain medi-
cine. McMahon publications are at or near the top of
their markets in independent readership scores. The
combined circulation of McMahon Publishing publica-
tions approaches 330,000 doctors and pharmacists.
Clinical Oncology News was launched in September
2006 and has become a rising star among oncology
publications. The mission of the publication is threefold:
to improve the quality of oncology care, to increase its
cost-effectiveness and to facilitate the job of the oncolo-
gist. To achieve these goals, the editorial staff of Clinical
Oncology News follows developments in the field, both in
the academic and private-practice settings. The majority
of the news coverage comes from major oncology meet-
ings, roughly 10 to 15, including the annual meetings of the
American Society of Clinical Oncology, American Society
of Hematology, European Society for Medical Oncology
and American Society of Pediatric Hematology/Oncol-
ogy. Each month, Clinical Oncology News also provides
in-depth educational reviews.
McMahon Publishing also produces a wide variety
of Special Editions, compendia of educational reviews
written by thought leaders in various specialties. These
include oncology, anesthesiology, gastroenterology and
endoscopy, hospital pharmacy, general surgery, infec-
tious disease, and pain medicine. The Special Projects
division of McMahon Publishing produces educational
reviews, wall charts and custom pocket guides and Spe-
cial Reports and Literature Reviews. The educational
reviews, written by authorities in a given treatment area,
are comprehensive summaries of state-of-the-art thinking
on a specific disease state.
These often are published as wall charts and pocket
guides that serve as on-the-spot educational tools for
health care providers. Special Reports are individual,
custom-written monographs that are bound inside Clinical
Oncology News or other McMahon publications. Special
Reports can be based on symposium coverage, interviews
with experts, the medical literature and any combination
of these. Special Reports can be CME/CE accredited.
Literature Reviews also are individual, custom-written
monographs that are bound inside Clinical Oncology
News or other McMahon publications and distributed to
the newsmagazine’s full readership. We conduct a lit-
erature search for all peer-reviewed, published studies
on a given subject and compile a detailed, scientifically
sound review of these articles. Literature Reviews also
can be CME/CE accredited.
McMahon PublishingAT A GLANCEAddress
545 W. 45th Street, 8th Floor
New York, NY 10036
Phone: (212) 957-5300
Fax: (212) 957-7230
www.mcmahonmed.com
www.clinicaloncology.com
www.cmezone.com
Products
Medical newsmagazines, custom
medical publications, educational
reviews, educational and instruction-
al pocket guides, special editions.
Publisher, CEO and Managing Partner
Raymond E. McMahon
President, PartnerVan Velle
Clinical Oncology News Staff
Vice President, Medical Education; Group Publication Director
Thomas Ciriacks
Associate Publication Director
Julianna Dawson
Executive Manager, Classifieds
Nancy Parker
Managing Editor
Kate O’Rourke
Senior Editor
Sarah Tilyou
Art Director
Frank Tagarello

Abraxis BioScience is a
fully integrated global
biotechnology company
dedicated to the discovery,
development and delivery
of next-generation thera-
peutics and core technolo-
gies that offer patients safer
and more effective treat-
ments for cancer and other
critical illnesses.
The company’s portfolio includes the world’s first and only protein-bound nanoparticle chemotherapeutic compound (ABRAXANE), which is based on the company’s proprietary tumor targeting technology known as the nab® platform. The first FDA-approved product to use this nab platform, ABRAX-ANE was launched in 2005 for the treatment of metastatic breast cancer and is now approved in 36 countries. The company continues to expand the nab platform through a robust clini-cal program and deep product pipeline. Abraxis trades on the NASDAQ Global Market under the symbol ABII. For more infor-mation about the company and its products, please visit www.abraxisbio.com.
Abraxis BioScience
18 Corporate Profile 2009 Special Advertising Section Clinical Oncology News
AT A GLANCE
Address
11755 Wilshire Blvd., 20th Floor
Los Angeles, CA 90025
Phone: (310) 883-1300
Fax: (310) 998-8553
www.abraxisbio.com
Executive Committee
Lonnie Moulder
Patrick Soon-Shiong, MD
Mary Lynne Hedley, PhD
Rick Rodgers
Bruce Wendel
Board of Directors
Patrick Soon-Shiong, MD
Lonnie Moulder
Kirk K. Calhoun
David S. Chen, PhD
Stephen D. Nimer, MD
Leonard Shapiro

Scientists at Amgen pursue fundamental cellular
signaling pathways. Following these uncharted
molecular trials can lead to important discover-
ies about the root causes of grievous illnesses,
as well as to new targets for drug development.
Amgen researchers have found pathways that
play a role in various types of cancer, bone loss
and immune system and inflammatory disorders.
The result is a robust pipeline that currently con-
tains more than 50 molecules from late discov-
ery research through Phase III clinical trials.
The Principled Pursuit of Innovation
Amgen’s research and development teams follow four guiding principles:
1. Focus on grievous illnesses
Patients suffering from the greatest unmet needs are Amgen’s first priority. The majority of new molecules that Amgen is bring-ing into the clinical target pathways have never previously been addressed in humans. Many of these are aimed at cancer, an area in which Amgen is conducting clinical trials in more than a dozen tumor types.
2. Be modality-independent
In other words, choose the right tool for the task. Amgen scien-tists look first at the disease process, then seek to determine the most advantageous therapeutic approach, be it large-molecule biologic, antibody, peptibody or small-molecule (oral) therapy.
3. Study disease in people
Studying disease in people is the best way to develop medi-cines for people. Experimental models often have little predictive value, and promising preclinical studies too often lead to high-cost clinical failures. Amgen seeks to identify safe and effective disease intervention methods as early as possible in the develop-mental process, using biomarkers and other tools.
4. Seamless integration
Amgen is structured to incorporate perspectives from health economics, regulatory and government affairs, clinical develop-ment and basic research into all development programs. Being rigorous in its prioritization, clear in its focus and attentive to all aspects of therapeutic intervention enables Amgen to develop medicines that address important unmet medical needs while also presenting a compelling value proposition for society.
Pathways in Cancer Research
Amgen oncology researchers are fighting cancer on multiple fronts, including:
Growth Regulation: Identifying and block-ing the pathways that regulate the abil-ity of cancer cells to proliferate, migrate, invade and survive.Angiogenesis: Preventing tumors from stim-ulating the formation of new blood vessels to feed them.Apoptosis: Enabling programmed cell death, or “cancer cell suicide.”Bone Metabolism and Metastases: Control-ling the signals that trigger bone buildup and breakdown, in an effort to treat and prevent the spread of cancer to the bones.
Amgen: Bringing the Promise of Biotechnology to Life
Amgen uses innovative research to improve the health of patients. As pioneers in bio-technology, Amgen applies its expertise to discover, create and deliver vital medicines that so far have helped more than 15 million people in their fight against cancer, kidney dis-ease, rheumatoid arthritis and other serious illnesses. With a deep and broad pipeline of potential new medicines, Amgen is working to continue to bring the promise of biotechnology to life—to help many more.
Amgen: Pioneering Science Delivers Vital Medicines
Amgen explores several oncology research areas including tumor angiogenesis, the abnormal process of new blood vessel formation.
In the United States, one out of every two women over age 50 will suffer an osteoporotic fracture. Bone biology is an important area of exploration where Amgen scientists work to address unmet needs.
Special Advertising Section Clinical Oncology News Corporate Profile 2009 19
AT A GLANCE
Address
One Amgen Center Drive
Thousand Oaks, CA
91320-1799
Phone: (805) 447-1000
Fax: (805) 447-1010
www.amgen.com
For information about
Amgen medicines,
including important
safety information, visit
www.amgen.com/medpro/
products.html

Dako is a global leader
in tissue-based cancer
diagnostics. Hospital and
research laboratories
worldwide use Dako’s
know-how, reagents,
instruments and software
to make precise diagnoses
and determine the most
effective treatment for
patients with cancer.
With more than 1,000 employees and operations in more than 70 countries, Dako covers essentially all of the global anatomic pathology markets. Headquartered in Denmark, Dako’s focus is to become first choice for patholo-gists around the globe.
Drug-Diagnostic Codevelopment
In an effort to improve patient care, the FDA encourages the use of companion diagnostics to enable identification of patients who are eligible for a particular cancer therapy.1 Through the pharmDx™ program, Dako offers partner-ship opportunities to pharmaceutical and biotechnology companies that wish to codevelop their drug with a companion diagnostic test. Dako’s approach is uniquely suited to complement the entire pharmaceu-tical value chain, from preclinical research through clinical trials, regulatory approval and commercialization.
About the Dako pharmDx™ Program
Dako’s pharmDx™ products are predictive tests that enable targeted therapeutics by providing tools to accomplish the following:
Identify potential responders to a • specific drug;Aid in differential diagnosis or identifica-• tion of patient subsets;Permit data mining and re-evaluation of • previously studied drugs; and Identify patients at risk for adverse events
In 1998, Dako pioneered this field with the introduction of HercepTest as a companion diagnostic for Herceptin®. Since then, Dako has commercialized the following companion diagnostics: HER2 FISH pharmDx™ for Herceptin® treatment, EGFR pharmDx™ for Erbitux treatment, ER/PR pharmDx™ for antihormonal or aromatase inhibitor therapies and c-Kit pharmDx™ for diagnosis of gastrointestinal stromal tumors and treatment with Gleevec/Glivec™. Currently, Dako is work-ing with several pharmaceutical and biotechnology companies,
and has numerous new pharmDx™ products in the pipeline.
Dako’s pharmDx™ Capabilities
Dako’s exceptional track record demonstrates the company’s unique ability to collaborate with pharmaceutical companies to develop, manufacture and commercialize predictive tests for ana-tomic pathologists worldwide. Dako’s unique pharmDx™ capabili-
ties include the following: Basic research and pharmDx™ assay devel-• opment capabilities for both immunohis-tochemistry and in situ hybridization assays in manual and automated formats; Development of image-analysis algorithms • to enable more uniform interpretation; FDA- and ISO-certified manufacturing • facilities; Regulatory filing and approval in the United • States, Europe and Japan; and Access to global markets through worldwide • sales, marketing and distribution channels.
Partnership Opportunities
Dako is strongly committed to developing and maintaining successful partnerships for the long term. Dako is actively seeking new partners for drug-diagnostic codevelopment opportunities. As a partner, Dako will leverage its industry-leading diagnostic and pharmDx™ expertise to facilitate successful discovery, development and commercialization of new
targeted therapies and companion diagnostics.
For press releases and further information, please see www.dako.com.
1. “Drug-Diagnostic Co-Development Concept Paper (Draft)” published by the
FDA’s Department of Health and Human Services (HHS), April 2005.
Dako
Lars Holmkvist, President and CEO
Dako subsidiary in North America.
20 Corporate Profile 2009 Special Advertising Section Clinical Oncology News
AT A GLANCE
Address
6392 Via Real
Carpinteria, CA 93013
Phone: (805) 566-6655
Fax: (805) 566-6688
www.dako.com
Products
HercepTest
HER2 FISH pharmDx
EGFR pharmDx
ER/PR pharmDx
c-Kit pharmDx

Every door opened could be a discovery made.
Lilly Oncology Making science personal.
GC58648 0709 PRINTED IN USA © 2009, Lilly USA, LLC. ALL RIGHTS RESERVED.
38358_elonps_lilcorp_con8_fa.indd 1 7/20/09 4:02:10 PM

22 CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009
Phillip C. Phan, MD, director of inter-ventional pain management at The Uni-versity of Texas M.D. Anderson Cancer Center, in Houston, said interventional pain management strategies can reduce pain without increasing the use of oral analgesics that cause side effects in pediatric patients.
“There are two problems with using pain medicine in children. They are very susceptible to side effects, so they get sleepy, drowsy and nauseated. Tol-erance also develops much more rap-idly with children,” said Dr. Phan, a co-author of the study.
Interventional strategies, such as blocking a nerve plexus, can disrupt the transmission of pain, said Dr. Phan, who presented the findings at the 2009 annu-al meeting of the American Academy of Pain Medicine, in Honolulu (abstract 153). “With cancer, the location of the cancer is the source of the pain. So we can dampen it by local blocking, or we can put a cath-eter into that area and infuse medicine to block the pain signal.”
In the retrospective review of 58
children treated at the center between 2006 and 2008 for a range of cancer diagnoses, the most commonly used procedures were neural blockade, neu-rolytic blockade, intrathecal therapy, neurostimulation and vertebral aug-mentation. The techniques reduced pain scores by 68.7% and opioid con-sumption by 65.0%. Dr. Phan stressed that these therapies augment tradition-al pain control methods.
“You may have a patient with an osteo-sarcoma of the lower leg who is on ade-quate pain medication, but once in a while the kid moves the leg and causes a pain flare-up,” he said. “In that case, the medication would not help, so we would go in and do a temporary nerve block, injecting a local anesthetic and a ste-roid. That would give the patient relief for 24 to 48 hours.” Thus, interventional pain therapy can optimize pain control while pediatric patients are receiving
definitive cancer treatment.Christina Ullrich, MD, MPH, a spe-
cialist in pediatric oncology and pedi-atric palliative care at the Dana-Farber Cancer Institute, in Boston, said the study adds to a growing body of litera-ture showing interventional pain man-agement strategies to be effective, “par-ticularly when dealing with refractory pain and medications that are caus-ing side effects, and in the setting of
advanced illness.” She was particular-ly encouraged by the results in pediat-ric patients—few pain control studies are conducted in children. She added, however, that the availability of home care must be considered up front for patients undergoing such procedures. “If a patient is going to be discharged with an implanted pump or port, it can be challenging to find a home care agency that is able to support that technology in the outpatient setting,”
Dr. Ullrich said.Arthur D. Zepeda, MD, director of
pain management at the University of California at Irvine College of Med-icine, noted that neuroaxial opioids have long been used for postoperative pain in pediatric patients and that treat-ing pediatric cancer patients with sim-ilar procedures is a next step. “They can be at least as beneficial as they have been in adults,” he said. Concerns about
device management, however, need to be addressed during patient selection. “Even with adults, we have to make sure the patients have the resources and psy-chosocial capability to handle the post-operative and maintenance part of this therapy,” Dr. Zepeda said.
Complications reported in the study included postdural puncture headaches in two patients who received intrathecal therapy.
—David Jakubiak
But whether such testing should become routine is still a matter for debate.
At the 2009 annual conference of the Hematology/Oncology Phar-macy Association (HOPA), Rowena N. Schwartz, PharmD, direc-tor of oncology phar-macy at The Johns Hopkins Hospital, Balti-more, argued that pharmacogenom-ic testing for vita-min K epoxide reductase (VKORC1), the gene that codes for the enzyme that is the site of action where warfarin exerts its effect, should be done in all patients receiving warfarin.
Kelly Nystrom, PharmD, assistant pro-fessor of pharmacy practice at Creigh-ton University, Omaha, Neb., took the opposite view, telling HOPA delegates
that testing for VKORC1 should not be done in all patients because it is still not known whether the information from the test will actually affect clin-
ical outcomes.
The Evidence for VKORC1 Testing
There is a single nucleotide poly-morphism (SNP) in the VKORC1
gene that influenc-es the pharmacody-
namics of warfarin. The pharmacokinet-ics of warfarin are influenced by an SNP in the cytochrome P450 C29 (CYP2C9) gene. Together, these genetic factors account for 30% to 35% of the variability in warfa-rin dosing. However, it is very difficult to determine which individuals have these variants, Dr. Schwartz said.
“A study by Limbi [Pharmacotherapy 2008;28:1084-1097] found that the fre-quency of the VKORC1 allele 1173C/T was 10.6% among African Americans, 36.5% in Euro-Americans and 87% in
Hong Kong Chinese. But you can no longer say for certain which patient will have the variation. So even though this data is really helpful, it doesn’t help us make the adjustment in individual patients,” she said.
Adding to the case for testing is the abundant evidence that the 1173C/T allele affects the variability of the dose requirement in patients who are receiv-ing warfarin. Carriers of this allele need a longer time to reach a stable
international normalized ratio (INR) than individuals with homozygous wild-type alleles, according to a study by Stehle and colleagues (Clin Pharma-cokinet 2008;47:565-594).
Dr. Schwartz said that to date, the most convincing data for the benefit of VKO-RC1 testing comes from the Internation-al Warfarin Pharmacogenetics Consor-tium, which pooled data from 21 research groups from nine different countries (N Engl J Med 2009;360:753-764). The consortium used data from 4,043 patients to create a dose algorithm based on clini-cal variables alone, or on genetic informa-tion plus clinical variables. Consortium researchers concluded that the algorithm
Interventional Pain Techniques Effective in Children
Case for Genetic Screen Debated
Is VKORC1 Test Needed in All Warfarin Patients?
Interventional pain manage-ment can reduce pain scores in pediatric cancer patients, a new study reveals.
Miami—Genetic testing to determine an individual patient’s sensitivity to warfarin would make dosing of the agent more efficient and reduce the risk for bleeding or clotting events.
Pain
‘If a patient is going to be discharged with an implanted pump or port, it can be challenging to find a home care agency that is able to support that technology in the outpatient setting.’
—Christina Ullrich, MD, MPH
SUPPORTIVE CARE
Thromboembolism
‘We know that VKORC1 affects the dosing of warfarin that we are going to use, but what we don’t know is how that affects clinical outcomes. I don’t think that we have adequate information yet to tell us this.’
—Kelly Nystrom, PharmD

CLINICAL ONCOLOGY NEWS • JULY/AUGUST 2009 23
that contained the genetic information provided a significantly better prediction of the appropriate dose of warfarin than the algorithm containing just clinical vari-ables. The pharmacogenetic algorithm was also better than a fixed-dose approach based on 35 mg per week of warfarin.
The consortium also found that 1,711 (33.9%) of the total cohort of patients in their review required a low dose—less than 21 mg per week of warfarin, and that the pharmacogenetic algorithm provid-ed better prediction, with fewer overesti-mations of dose. Similarly, for 625 (12.4%) individuals requiring high doses (>49 mg per week of warfarin), the pharmacoge-netic algorithm provided better predic-tion, with fewer underestimations.
“The data from the consortium shows that if you use a fixed dose, you are not right often. You can make up for this if you have very close monitoring. But frequent monitoring and patient visits and the time it takes to evaluate those measures is not cheap either,” Dr. Schwartz said.
She concluded, “There is clear evidence that there is a difference in response to warfarin in patients with different genetic variants. If we can know those and make more knowledgeable decisions about what the dosing should be, especially the initiation dosing, I think that we save peo-ple time and problems.”
Jury Still Out
Dr. Nystrom disagreed that evidence justifies VKORC1 testing in all patients receiving warfarin. “We know that VKORC1 affects the dosing of warfa-rin that we are going to use, but what we don’t know is how that affects clinical outcomes. I don’t think that we have ade-quate information yet to tell us this.”
She cited a study by Schwartz et al. (N Engl J Med 2008;358:999-1008) that showed the risk for bleeding com-plications in 297 patients was the same regardless of VKORC1 genotype. “Their take-home message was that the patients with the VKORC1 *A/*A variant had a higher INR than patients with the VKORC1 *non-A/*non-A variants, even with empiric dose adjustments, but that serious bleeding effects were not signif-icantly affected by the VKORC1 haplo-type or CYP2C9 status.”
In addition to genetic testing, Dr. Nystrom said other factors to consider when it comes to dosing warfarin include smoking, alcohol use, comorbidities, weight, height, vitamin K intake, age, gen-der, medications and amount of exercise.
Cost-effectiveness is another factor that needs to be examined when recom-mending universal VKORC1 testing, Dr. Nystrom said. A study by Eckman and colleagues (Ann Intern Med 2009;150:73-83) studied the cost-effectiveness of pharmacogenetic-guided warfarin dos-ing and found that, in comparison with standard warfarin dosing, the strategy cost $144,000 per quality-adjusted life
year. The researchers concluded that there is a small group of patients who might benefit, and that the cost-effec-tiveness may improve as the cost of peforming the test decreases. “Still, it is not cheap,” Dr. Nystrom said.
Finally, the Centers for Medicare & Medicaid Services (CMS) released a statement in May announcing that it would not reimburse warfarin genet-ic testing, noting a lack of evidence that such testing improves health outcomes in Medicare beneficiaries.
The CMS also released statements from major medical groups, includ-ing the American College of Chest
Physicians, the American College of Medical Genetics, the Association for Molecular Pathology and the American Society of Hematology, calling for more randomized data from clinical trials before they could support routine VKO-RC1 testing.
“Once we have this information, we can make a better judgment on whether this is something that should be offered to all patients, but currently, I don’t think there is enough information available to offer testing to all patients who are receiving warfarin,” Dr. Nystrom concluded.
—Fran Lowry
WARFARINcontinued from page 22 �
SUPPORTIVE CARE
Thromboembolism
What’s Your View?
Should VKORC1 testing be done in all patients receiving
warfarin therapy?
Send replies [email protected]

INDICATION: Vectibix® is indicated as a single agent for the treatment of EGFR-expressing, metastatic colorectal carcinoma (mCRC) with disease progression on or following fluoropyrimidine-, oxaliplatin-, and irinotecan-containing chemotherapy regimens.
The effectiveness of Vectibix® as a single agent for the treatment of EGFR-expressing mCRC is based on progression-free survival. Currently, no data demonstrate an improvement in disease-related symptoms or increased survival with Vectibix®.
Important Safety Information including Boxed WARNINGS:Safety data are available from 15 clinical trials in which 1467 patients received Vectibix®; of these, 1293 received Vectibix® monotherapy and 174 received Vectibix®
in combination with chemotherapy.
WARNING: DERMATOLOGIC TOXICITY and INFUSION REACTIONSDermatologic Toxicity: Dermatologic toxicities occurred in 89% of patients and were severe (NCI-CTC grade 3 and higher) in 12% of patients receiving Vectibix® monotherapy. Withhold Vectibix® for dermatologic toxicities that are grade 3 or higher or are considered intolerable. If toxicity does not improve to ≤ grade 2 within1 month, permanently discontinue Vectibix®. The clinical manifestations included,but were not limited to, dermatitis acneiform, pruritus, erythema, rash, skin exfoliation, paronychia, dry skin, and skin fissures. Subsequent to the development of severe dermatologic toxicities, infectious complications, including sepsis, septic death, and abscesses requiring incisions and drainage were reported.
Infusion Reactions: Severe infusion reactions occurred in approximately 1% of patients. Severe infusion reactions included anaphylactic reactions, bronchospasm, and hypotension. Although not reported with Vectibix®, fatal infusion reactions have occurred with other monoclonal antibody products. Stop infusion if a severe infusion reaction occurs. Depending on the severity and/or persistence of the reaction,permanently discontinue Vectibix®.
Vectibix® is not indicated for use in combination with chemotherapy. In an interim analysis of a randomized (1:1) clinical trial of patients with previously untreated metastatic colorectal cancer, the addition of Vectibix® to the combination of bevacizumab and chemotherapy resulted in decreased overall survival and increasedincidence of NCI-CTC grade 3-5 (87% vs 72%) adverse reactions.
In a single-arm study of 19 patients receiving Vectibix® in combination with IFL, the incidence of NCI-CTC grade 3-4 diarrhea was 58%; in addition, grade 5 diarrhea occurred in 1 patient. In a single-arm study of 24 patients receiving Vectibix® plus FOLFIRI, the incidence of NCI-CTC grade 3 diarrhea was 25%.
Pulmonary fibrosis occurred in less than 1% (2/1467) of patients enrolled in clinical studies of Vectibix®. Following the initial fatality, patients with a history of interstitial pneumonitis, pulmonary fibrosis, evidence of interstitial pneumonitis, or pulmonary fibrosis were excluded from clinical studies. Therefore, the estimated risk in such patients is uncertain. Permanently discontinue Vectibix® therapy in patients developing interstitial lung disease, pneumonitis, or lung infiltrates.
In the randomized, controlled clinical trial, median magnesium levels decreased by 0.1 mmol/L in the Vectibix® arm. Additionally, hypomagnesemia (NCI-CTC grade 3 or 4) requiring electrolyte repletion occurred in 2% of patients 6 weeks or longer after the initiation of Vectibix®. In some patients, both hypomagnesemia and hypocalcemia occurred. Patients’ electrolytes should be periodically monitored during and for 8 weeks after the completion of Vectibix® therapy, and appropriate treatment instituted, as needed.
Exposure to sunlight can exacerbate dermatologic toxicity. It is recommended that patients wear sunscreen and hats and limit sun exposure while receiving Vectibix®.
Dermatologic, mucosal, and ocular toxicities were also reported.
Adequate contraception in both males and females must be used while receiving Vectibix® and for 6 months after the last dose of Vectibix® therapy.
The most common adverse events of Vectibix® are skin rash with variable presentations, hypomagnesemia, paronychia, fatigue, abdominal pain, nausea, and diarrhea, including diarrhea resulting in dehydration. The most serious adverse events of Vectibix® are pulmonary fibrosis, severe dermatologic toxicity complicated by infectious sequelae and septic death, infusion reactions, abdominal pain, hypomagnesemia, nausea, vomiting, and constipation.
Please see brief summary of Prescribing Information on next page.
References: 1. Vectibix® (panitumumab) prescribing information, Amgen. 2. Van Cutsem E, Peeters M, Siena S, et al. Open-label phase III trial of panitumumabplus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol. 2007;13:1658-1664.
©2009 Amgen. All rights reserved. 4-09 45904
*Correlation with safety and efficacy is unknown
The first fully human*
anti-EGFR monoclonalantibody
Based on independent review of disease progression, a statistically
significant prolongation in PFS was observed in patients receiving
Vectibix® plus BSC vs those patients receiving BSC alone1,2
Weeks
Prop
orti
on E
vent
Fre
e
0%
10%
20%
30%
60%
70%
100%
90%
80%
50%
40%
0 4 10 12 14 16 40 42 44 46 4832 34 36 388 186 20 302 50 5222 24 26 28
Kaplan-Meier Plot of PFS Time as Determined by the Independent Review Committee1,2
Treatment Group
Vectibix® + BSC (n=231)
BSC Alone (n=232)
P < 0.0001
Subjects at risk:
Vectibix® + BSCBSC Alone
231 217 209 197 118 85 76 65 49 41 40 40 31 22 19 19 13 8 8 8 5 2 2 1 1 1
232 209 175 149 75 41 31 20 17 11 7 7 7 4 4 3 3 3 2 1 1 1 1 1 1 0
Statistically significant prolongation in PFS time vs BSC alone1,2
The recommended dose of Vectibix® is 6 mg/kgadministered over 60 minutes (for doses over1000 mg infuse over 90 minutes) as an intravenous infusion every 14 days1
The use of premedication was not standardized in clinical trials (the utility of premedication in preventing infusional toxicity is unknown)1
~1% incidence of severe infusion reactions reported1
- See Important Safety Information includingBoxed WARNINGS for infusion reactions
Infusionreactions
Q2Wdosing
ProlongedPFS