Embed Size (px)
Citation preview

Child HealthChild HealthNursingNursing
Partnering withPartnering withChildren & FamiliesChildren & Families
Chapter 30Chapter 30
Alterations in Alterations in Gastrointestinal Gastrointestinal FunctionFunction
Jane W. BallJane W. BallRuth C. BindlerRuth C. Bindler
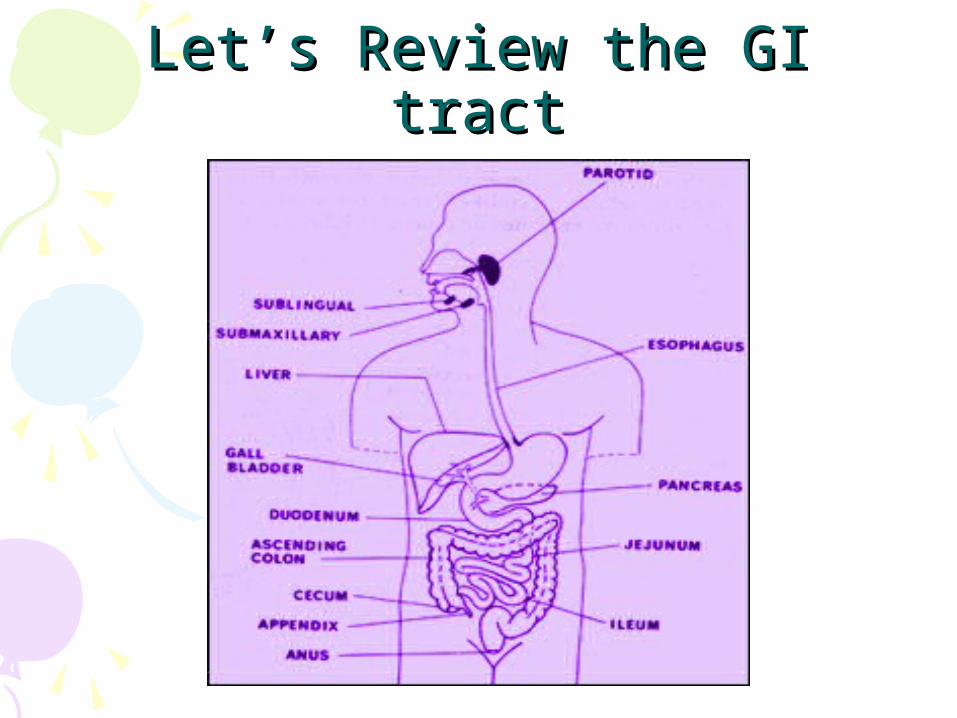
Let’s Review the GI tractLet’s Review the GI tract

FIGURE 30–1FIGURE 30–1 The internal anatomic structures of the stomach, The internal anatomic structures of the stomach, including the pancreatic, cystic, and hepatic ducts; the pancreas; including the pancreatic, cystic, and hepatic ducts; the pancreas; and the gallbladder.and the gallbladder.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.

Pediatric Differences in Pediatric Differences in Anatomy and PhysiologyAnatomy and Physiology
• Duodenum: digestion takes place• Enzymes that aid in digestion:
– Amylase ( saliva; digests carbs)– Lipase (enhances fat absorption)– Trypsin (which breaks down protein into
polypeptides and some amino acids)(Infants are deficient in these enzymes until
around 4-6 mos…therefore abdominal distention from gas is common)

Pediatric Differences in Pediatric Differences in Anatomy and PhysiologyAnatomy and Physiology
• GI sx immature at birth– Process of absorption and secretion do
not take place until after birth– Sucking primitive reflex– Voluntary swallow (at 6 weeks)– Newborn’s stomach capacity is small at
birth ??? Implications..• (frequent feedings, freq bowel movements,
and intestinal motility is greater than in older kids (peristalsis) therefore greater emptying time)
Pediatric Differences in Pediatric Differences in Anatomy and Physiology Anatomy and Physiology
• Liver function immature at birth and next few weeks
• During first year of life– Gluconeogenesis (formation of glycogen from noncarbs)– Plasma protein– Ketone formation– Vitamin storage– Deamination
• GI structures in second year of life more mature– Enlarged stomach capacity (to 3m/day)– Sphincter control (mylination of sc)
What What would be some signs/ would be some signs/ symptoms of GI disorders in symptoms of GI disorders in
infants/ children?infants/ children?• Vomiting/ regurgitation• Irritability/ fussiness• Abdominal pain/ distension• FTT• Weight loss• Stool changes• Abdominal pain

GI Assessment TechniquesGI Assessment Techniques• Subjective
– Lifestyle and family factors• Including family hx
– Diet• ? Gaining weight• Thorough h/o feeding pattern, ? Any problems• Allergies (lactose intolerant, celiac disease)
– Elimination patterns• I/O’s • Encorpresis/ constipation

GI Assessment TechniquesGI Assessment Techniques• Objective
– Observe• Abdominal distension• Symmetry, bumps, bulges or masses• Umbilicus• Peristaltic waves
– Visible rippling waves= bowel obstruction
GI Assessment TechniquesGI Assessment Techniques• Objective (con’t)
– Auscultation• Hyper/hypo bowel sounds
– Percussion• Tympany vs dullness
– Palpation• Light vs deep • Rebound tenderness…peritoneal
inflammation• McBurney’s point
Disorders of the GI SystemDisorders of the GI System• Structural defects• Disorders of motility• Intestinal parasitic disorders• Inflammatory disorders• Disorders of malabsorption• Hepatic disorders• Injuries to the GI system

Structural DefectsStructural Defects• Cleft Lip and Cleft Palate• Esophageal atresia and
tracheoesophageal fistula• Pyloric Stenosis• Insussusception• Abdominal Wall Defects• Anorectal malformations• Umbilical hernia
Cleft Lip and Cleft PalateCleft Lip and Cleft Palate• Congenital malformation (failure of
the maxillary processes to fuse) occurring during weeks 6-12 gestation
• Each abnormality may appear by itself or may be seen together
• Varying degrees of severity• Most common craniofacial deformities
overall in US• Multifactoral causes

Cleft Lip and Cleft PalateCleft Lip and Cleft Palate• Complication Associated with Cleft
Lip or Cleft Palate (see Table 30-1)– Feeding problems– Speech development– Otologic– Dental and orthodontic– Developmental

Cleft LipCleft Lip• Opening between the nose and lip• Apparent at birth• Should be documented during
newborn assessment• Assess child’s ability to suck and
swallow• Cleft lip repair is performed during
first month of life• Special feeding techniques if surgery
is delayed
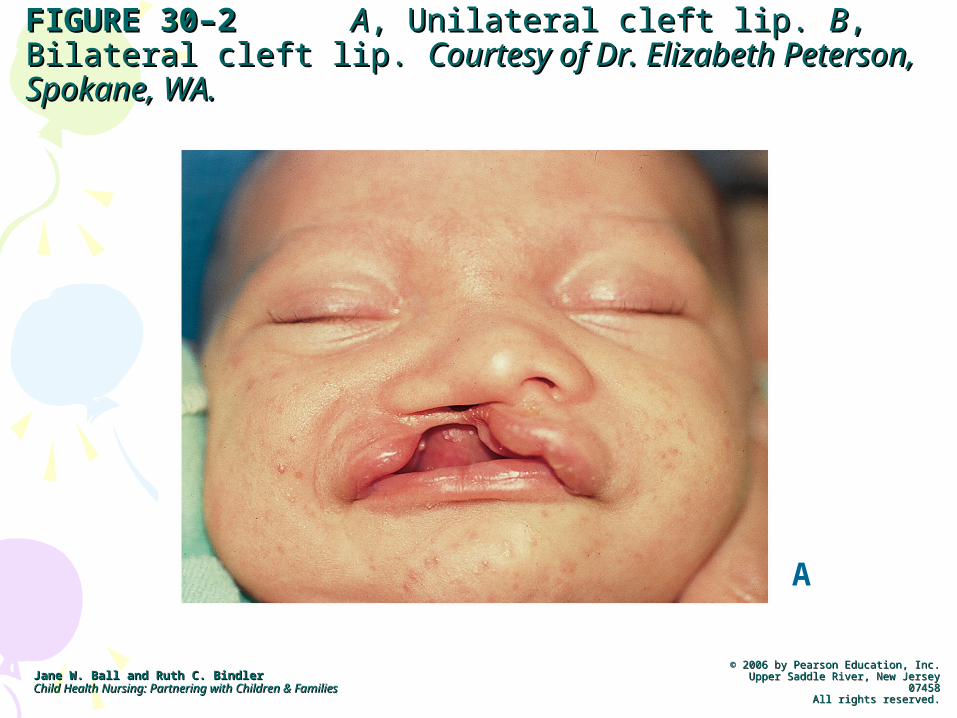
FIGURE 30–2FIGURE 30–2 AA, Unilateral cleft lip. , Unilateral cleft lip. BB, Bilateral cleft , Bilateral cleft lip. lip. Courtesy of Dr. Elizabeth Peterson, Spokane, WA.Courtesy of Dr. Elizabeth Peterson, Spokane, WA.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
A
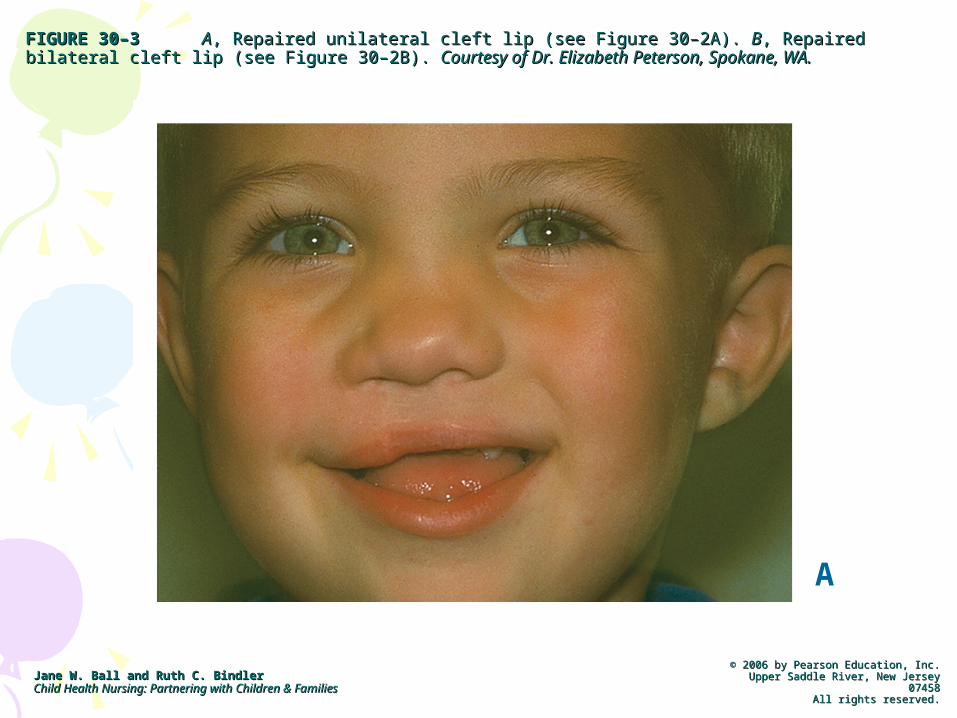
FIGURE 30–3FIGURE 30–3 AA, Repaired unilateral cleft lip (see Figure 30–2A). , Repaired unilateral cleft lip (see Figure 30–2A). BB, Repaired bilateral cleft lip (see , Repaired bilateral cleft lip (see Figure 30–2B). Figure 30–2B). Courtesy of Dr. Elizabeth Peterson, Spokane, WA.Courtesy of Dr. Elizabeth Peterson, Spokane, WA.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
A
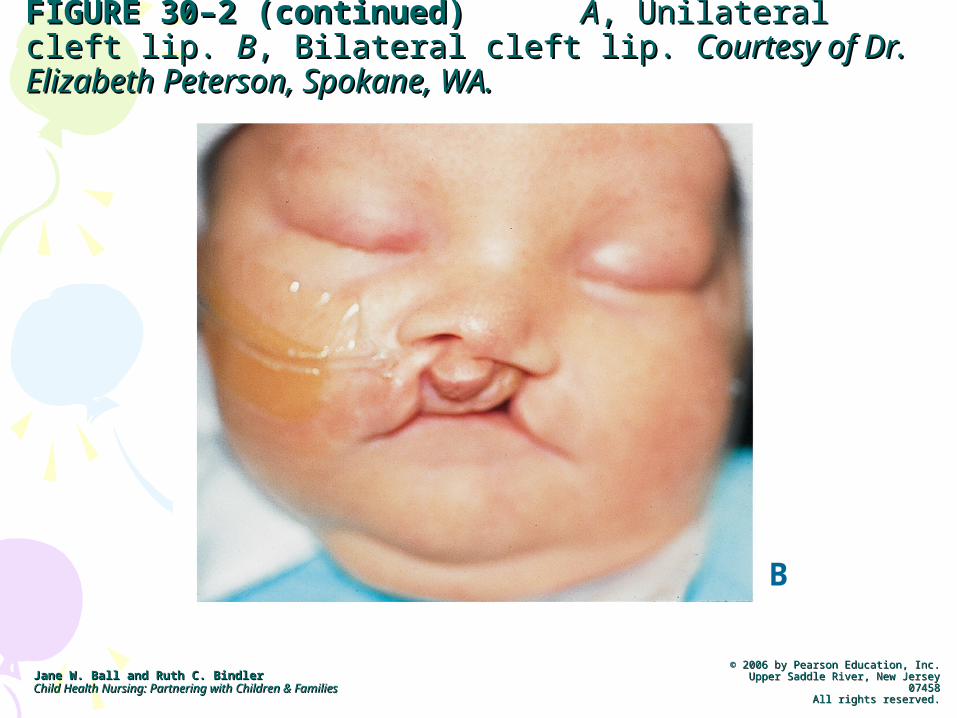
FIGURE 30–2 (continued)FIGURE 30–2 (continued) AA, Unilateral cleft lip. , Unilateral cleft lip. BB, , Bilateral cleft lip. Bilateral cleft lip. Courtesy of Dr. Elizabeth Peterson, Courtesy of Dr. Elizabeth Peterson, Spokane, WA.Spokane, WA.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
B

FIGURE 30–3 (continued)FIGURE 30–3 (continued) AA, Repaired unilateral cleft lip (see Figure 30–2A). , Repaired unilateral cleft lip (see Figure 30–2A). BB, Repaired bilateral , Repaired bilateral cleft lip (see Figure 30–2B). cleft lip (see Figure 30–2B). Courtesy of Dr. Elizabeth Peterson, Spokane, WA.Courtesy of Dr. Elizabeth Peterson, Spokane, WA.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
B
Cleft LipCleft Lip• Feeding a Child before Cleft Lip
Repair• Bottle with special nipple – longer and
narrower• Hold infant in upright position• Large cross-cut hole in nipple to allow the
child to get food into back of throat without strong sucking
• Stimulate sucking by rubbing nipple on infant’s lower lip
• Allow child to swallow and burp frequently• ESSR method – Enlarge nipple, Stimulate
sucking, Swallow, Rest
Cleft LipCleft Lip• Surgery for Cleft Lip Repair
– Usually done early (first few days to 1st month of life) to improve parental bonding and improve feeding
– Plastic surgery with a staggered suture line (often in shape of letter “Z” to minimize scarring)
– After surgery Logan Bar over child’s mouth to reduce tension on suture line

Logan BarLogan Bar
Cleft Lip RepairCleft Lip Repair• Pre-Op Care of the Child and Parents• Explain pre-op procedures to
parents• Provide support and information• Keep accurate record of child’s
growth and feeding schedule• Infant:
– NPO X 4-6 hours pre-op– IVs
Cleft Lip RepairCleft Lip Repair• Nursing Diagnosis
– Pre-Op• Imbalanced Nutrition: Less than body
requirements• Risk for aspiration• Altered parenting
Cleft Lip RepairCleft Lip Repair• Post-Op Care of Child and Family• Encourage rooming-in• Incision care: clean sutures with sterile
cotton swab and ½ strength H2O2 followed by saline to prevent crusting (esp. after feeding). May apply antibiotic ointment to suture line
• DO NOT DISPLACE LOGAN BAR• Special feeder – syringe with rubber tubing
into side of mouth, Breck feeder• Diet advance from clear to diet for age over
48 hours• Elbow restraints

Cleft Lip RepairCleft Lip Repair• Nursing Diagnosis
– Post-Op• Risk of injury & Infection• Pain • Altered feeding patterns
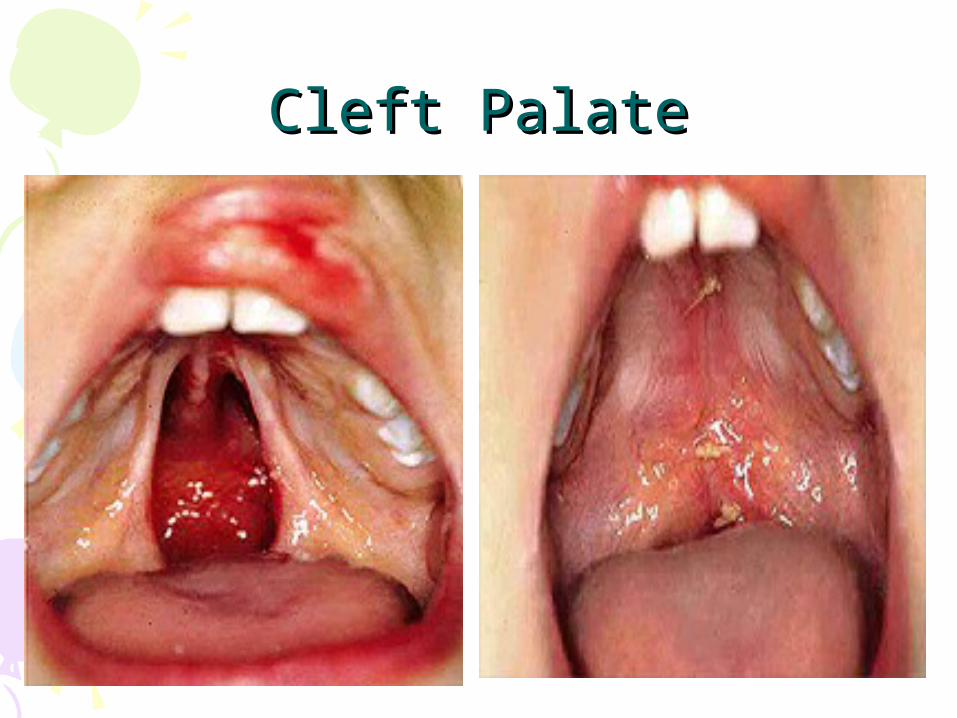
Cleft PalateCleft Palate• Repaired surgically between 6
months to 2 years prior to talking• Parents will care for child at home
until surgical repair• Altered dentition and speech
dysfunction may also occur• Frequent episodes of otitis media
– (due to opening into nasopharynx)
Cleft PalateCleft Palate
Cleft Palate RepairCleft Palate Repair• Post-op: sutures in child’s mouth• Keep straws, pacifiers, spoons away
from child’s mouth for 7-10 days post-op
• Elbow restraints and mittens• Feeding – soft foods: baby food. Short
nipples may be used• All feeding followed by rinsing mouth
with water to clean suture line• No brushing teeth X 1-2 weeks
Cleft Palate RepairCleft Palate Repair• Nursing Diagnoses
– Pre-Op:• Parental Knowledge Deficit• Risk for Infection• High Risk for Altered Family Processes
– Post-Op:• Altered Skin Integrity• Child: Pain
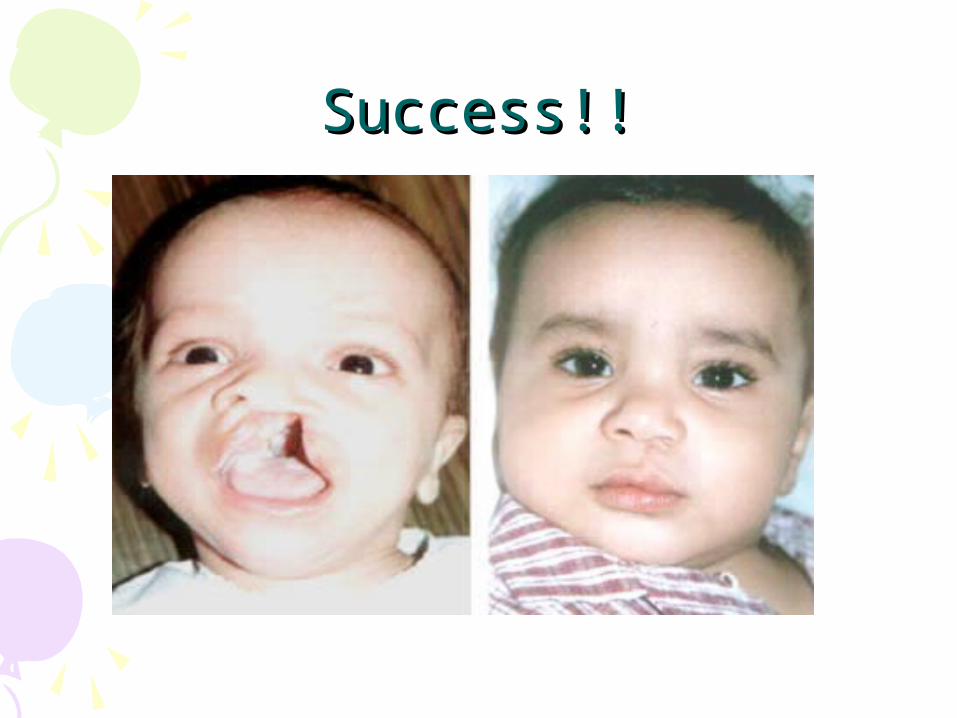
Success!!Success!!
Esophageal Atresia & Esophageal Atresia & Tracheoesophageal Fistula Tracheoesophageal Fistula
(TEF)(TEF)
• Esophageal atresia and TEF– a malformation that results from failure
of the esophagus to develop as a continuous tube
– Foregut fails to lengthen, separate and fuse into 2 parallel tubes (at 4-5 weeks gestation)
– Associated with maternal polyhydramnios
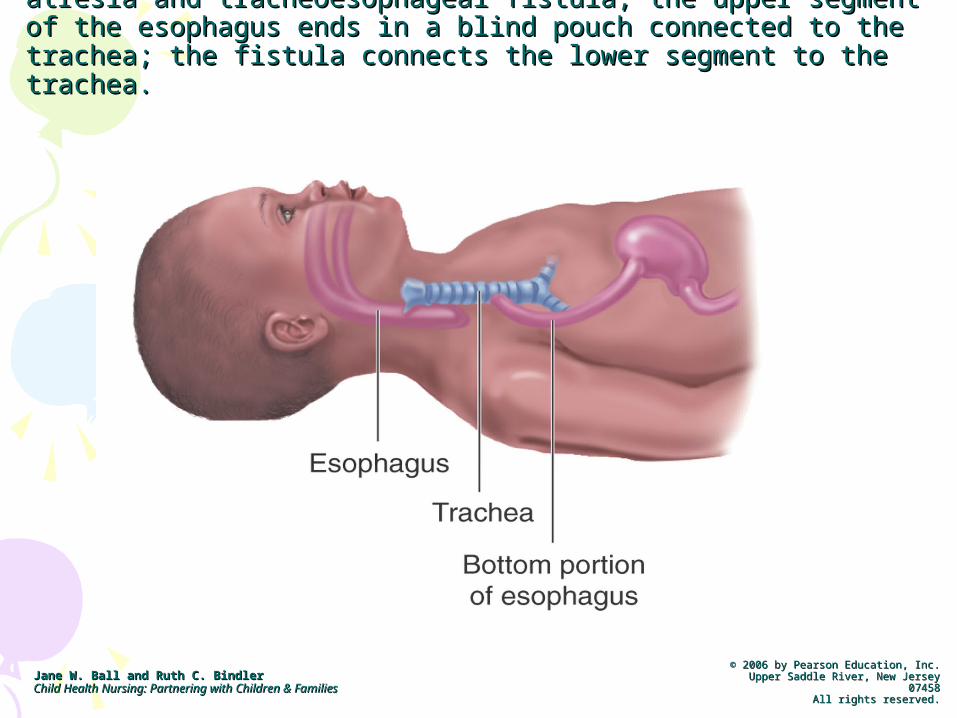
FIGURE 30–4FIGURE 30–4 In the most common type of esophageal atresia In the most common type of esophageal atresia and tracheoesophageal fistula, the upper segment of the and tracheoesophageal fistula, the upper segment of the esophagus ends in a blind pouch connected to the trachea; the esophagus ends in a blind pouch connected to the trachea; the fistula connects the lower segment to the trachea.fistula connects the lower segment to the trachea.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
EA and TEF EA and TEF • Signs/Sx: • Apparent in immediate newborn period
– Respiratory Distress – Difficulty feeding– Excessive drooling– Choking, coughing– Cyanosis
• Esophageal Atresia is a surgical emergency!
• Tx: Surgical correction
EA and TEFEA and TEF• Diagnosis
– Confirmed by attempting to pass an NG Tube into stomach• Usually a 5 or 8 French tube
• Nursing Care– ID signs/symptoms of disease– Careful Physical Assessment

EA and TEFEA and TEF• Pre- and Post- Operative Care• Pre-Op:
– NG tube to suction– Prevent aspiration complication
• (increase HOB, NPO)
– Establish IV access: IVFs & IV abx
• Post-Op:– Care of G-Tube– Family teaching
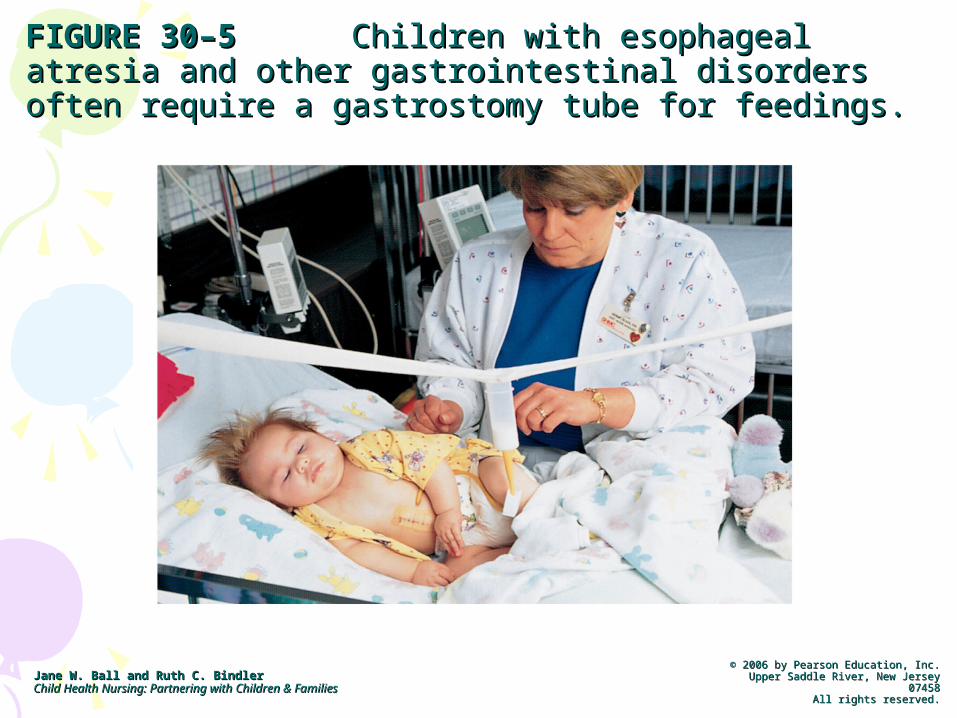
FIGURE 30–5FIGURE 30–5 Children with esophageal atresia and Children with esophageal atresia and other gastrointestinal disorders often require a other gastrointestinal disorders often require a gastrostomy tube for feedings.gastrostomy tube for feedings.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
Pyloric StenosisPyloric Stenosis• AKA Hypertrophic Pyloric Stenosis• Etiology unknown, but often affects first-
born males• Affects males 2-5 X more than females,
especially white males• Present at birth• Diagnosis by ultrasound• Stenosis occurs b/t stomach and
duodenum
Pyloric StenosisPyloric Stenosis• Pathophysiology:
– Obstruction of the pyloric sphincter by hypertrophy of the circular muscle of the pylorus
– With the enlarged muscle, there is severe narrowing of the pyloric canal between the stomach and duodenum
– With food, the muscle is irritated and becomes further edematous thus causing the opening to become narrower
– Usually there is a slow progression of edema and narrowing of the opening into the duodenum

Pyloric StenosisPyloric Stenosis

Pyloric StenosisPyloric Stenosis• Clinical Manifestations:
– Initially, regurgitation after meals– Within one week - projectile vomiting– Vomiting occurs shortly after meals– Vomiting is forceful and may spew 2-4 feet– Infant constantly hungry– Fails to gain weight or loses weight– Stools decrease in number– Dehydration results/ electrolyte imbalances

Pyloric StenosisPyloric Stenosis• Clinical Manifestations:
– Upper abdomen distended– Olive-shaped mass palpable in RUQ– Left-to-right peristaltic waves noticeable on
abdomen– Best time to palpate mass is when infant is
relaxed during feeding– S/Sx of dehydration – sunken anterior fontanel,
sunken eyes, decreased elasticity of skin (tenting)
• Tx:– Surgery – Pyloromyotomy

Pyloric StenosisPyloric Stenosis• Nursing Care Pre- and Post-Op
– Fluid and electrolyte management– IV – NG Tube– Analgesics– Prevent Infection– Support family– Teaching

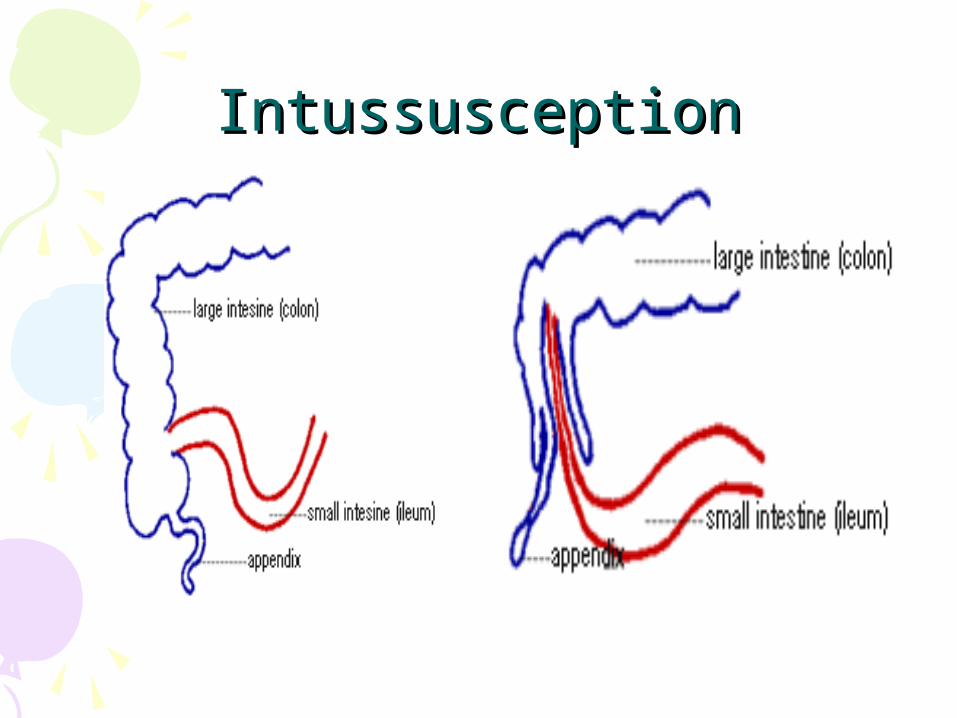
IntussusceptionIntussusception• Invagination (telescoping) of one
portion of intestine into another – (like a sock).
• Multifactoral causes• Commonly occurs in children b/t 3
months-6 years• 3x more likely in boys than girls• Common in children w/ CF, Celiac
Disease and gastroenteritis

IntussusceptionIntussusception• Mechanical Bowel Obstruction Occurs:
– Walls of the segments of the intestine press against each other causing inflammation, edema and decreased blood flow.
– As incarceration occurs, necrosis results with hemorrhage, perforation and peritonitis.
• Classic Triad:– Severe episodic pain– “Currant jelly” stool– Transverse tubular abdominal mass

IntussusceptionIntussusception
IntussusceptionIntussusception
IntussusceptionIntussusception• Clinical Manifestations:
– Sudden onset of abdominal pain in a healthy child
– Child screams and draws knees up to abdomen
– Pain is intermittent, child is relaxed between pain intervals - paroxysmal
– Vomiting occurs and increases over time– Stool changes from brown to blood-
tinged and mucousy - “currant jelly” in 50% of cases
IntussusceptionIntussusception• Clinical Manifestations:
– Most patients (75%) will test + for occult blood in stools
– Abdomen tender and distended– Sausage-shaped mass in RLQ (vertically-
oriented)– As obstruction progresses, child
becomes acutely ill with fever, and signs of peritonitis

IntussusceptionIntussusception• Diagnosis:
– Often based on history and physical examination alone
– Barium Enema is definitive (in 75% of cases). It is therapeutic and curative in most cases with less than 24-hour duration.
– Digital rectal exam reveals mucous, blood and sometimes the intussusception
– Laboratory tests – CBCD, Lytes
IntussusceptionIntussusception• Treatment:
– 10% will have spontaneous reduction of bowel
– Barium or contrast enema– Manual Reduction (if unsuccessful or
bowel is strangulated or s/sx of peritonitis= surgery)
– Surgical intervention is a last resort and must be done if there are signs of perforation and peritonitis
IntussusceptionIntussusception• Assessment – subjective parental
history of child’s physical and behavioral SxS
• Nursing Diagnoses– Altered GI Tissue Perfusion– Pain– Fluid Volume Deficit– Parental Knowledge Deficit– Parental Anxiety
IntussusceptionIntussusception• Nursing Management:
– VS– Pain – Abdominal exam (distention,
tenderness, auscultate BS Q4H)– I/O’s
• Fluids/ electrolytes
– Note: admission is indicated for all pts b/c up to 10% of reduction cases recur w/in 24 hrs
Abdominal Wall Defects: Abdominal Wall Defects: Gastroschisis & OmphaloceleGastroschisis & Omphalocele
• A congenital defect of the ventral abdominal wall, characterized by herniation of abdominal visceral outside the abdominal wall– Gastroschisis= occurs to the side (usually
right) of the umbilicus– Omphalocele= through the umbilical cord
• Occurs in week 11 of gestation – When abd contents fail to return to the abd
• Multifactoral causes
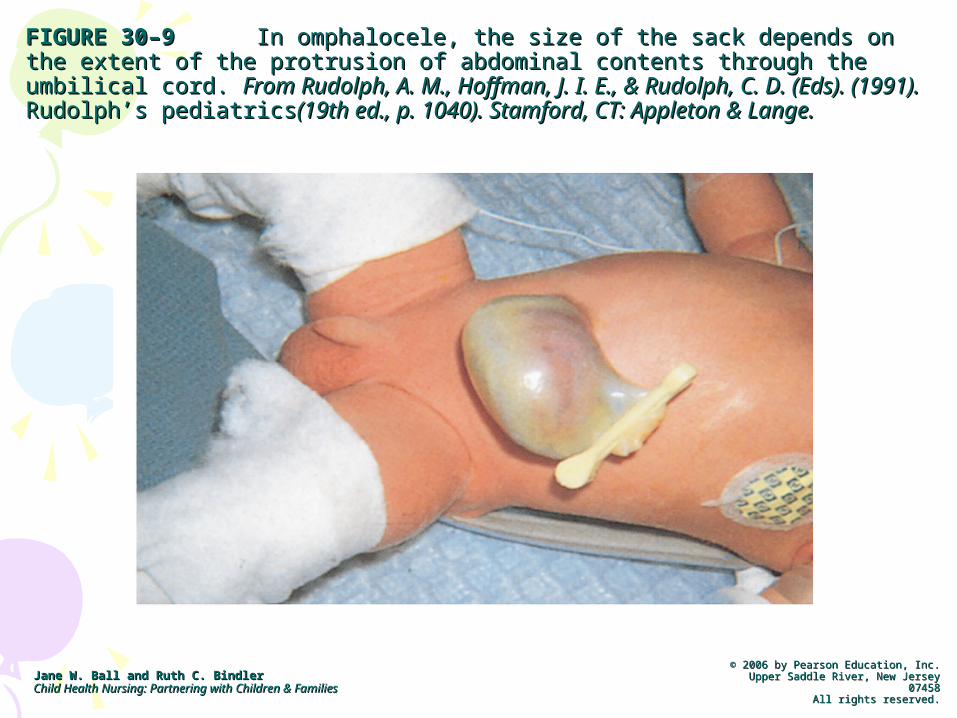
FIGURE 30–9FIGURE 30–9 In omphalocele, the size of the sack depends on the extent In omphalocele, the size of the sack depends on the extent of the protrusion of abdominal contents through the umbilical cord. of the protrusion of abdominal contents through the umbilical cord. From From Rudolph, A. M., Hoffman, J. I. E., & Rudolph, C. D. (Eds). (1991). Rudolph, A. M., Hoffman, J. I. E., & Rudolph, C. D. (Eds). (1991). Rudolph’s Rudolph’s pediatricspediatrics(19th ed., p. 1040). Stamford, CT: Appleton & Lange.(19th ed., p. 1040). Stamford, CT: Appleton & Lange.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.

Anorectal Malformations: Anorectal Malformations: Anal Stenosis & Anal AtresiaAnal Stenosis & Anal Atresia• Anal stenosis:
– A thickened and constricted anal wall– s/sx=characteristic ribbon-like stools
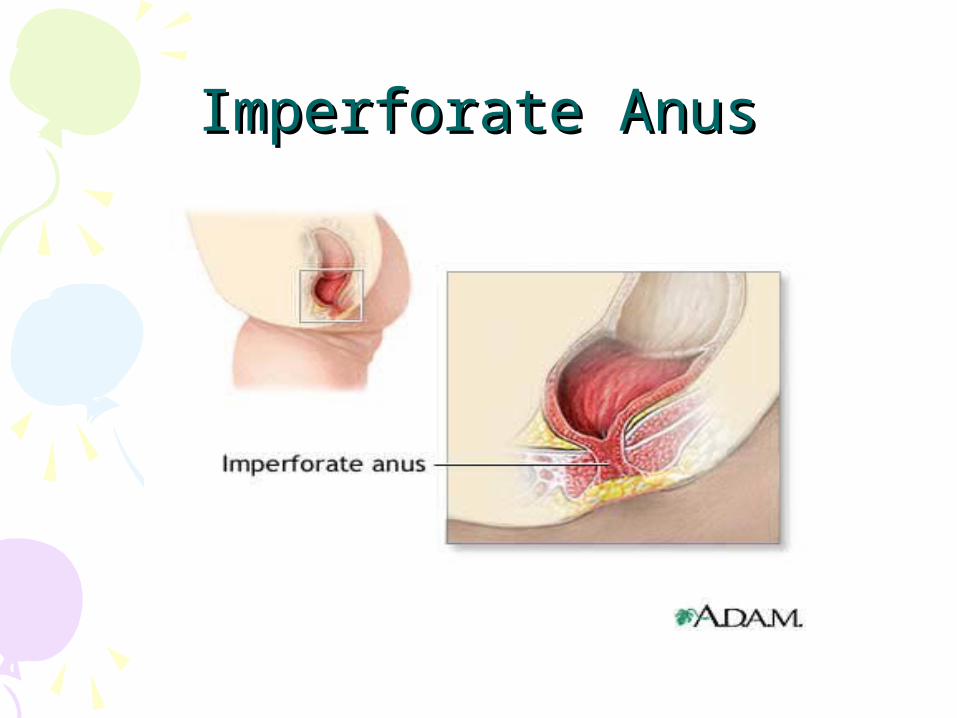
• Anal Atresia, aka Imperorate Anus– PE reveals absent anal opening– Failure to pass meconium also diagnostic
• Associated anomalies up to 70% of the time

FIGURE 30–10FIGURE 30–10 Imperforate anus, which is often obvious at birth, can Imperforate anus, which is often obvious at birth, can range from mild stenosis to a complex syndrome that includes associated range from mild stenosis to a complex syndrome that includes associated congenital anomalies.congenital anomalies.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
Imperforate AnusImperforate Anus
• Clinical Manifestations:– Failure to pass meconium during the
first 24 hours– Absence or stenosis of rectal canal– Stool in urine due to fistula to perineum– Stool in vagina due to fistula
Anorectal Malformations: Anorectal Malformations: Anal Stenosis & Anal AtresiaAnal Stenosis & Anal Atresia

Anorectal Malformations: Anal Anorectal Malformations: Anal Stenosis & Anal Atresia Stenosis & Anal Atresia
• DX=– Digital Rectal Exam– Ultrasound– Abdominal X-Rays– CT Scans
• Treatment= – For low lesions with just an anal membrane,
serial rectal digital dilations are effective– For higher lesions – 2 stage surgical repair
• Temporary colostomy• Abdominal pull-through
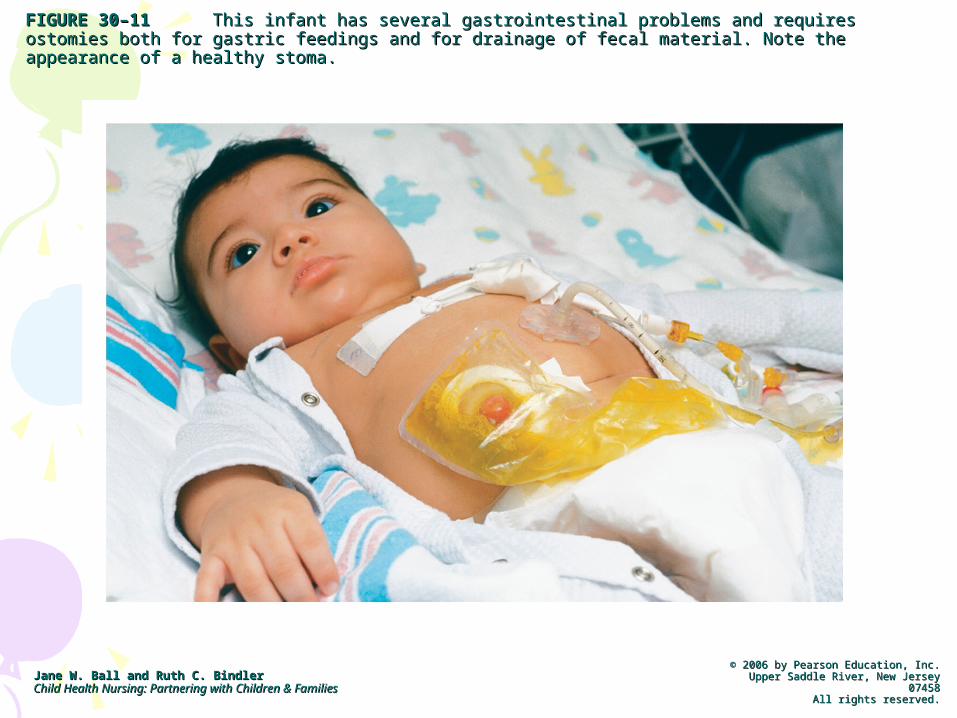
FIGURE 30–11FIGURE 30–11 This infant has several gastrointestinal problems and requires ostomies both for This infant has several gastrointestinal problems and requires ostomies both for gastric feedings and for drainage of fecal material. Note the appearance of a healthy stoma. gastric feedings and for drainage of fecal material. Note the appearance of a healthy stoma.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
Umbilical HerniaUmbilical Hernia• Hernia= protrusion or projection of an organ or a
part of an organ through the muscle wall of the cavity that normally contains it.
• Results from imperfect closure of the umbilical muscle ring
• Often associated with diastasis recti (lateral separation of the abdominal muscles)
• Etiology unknown• Around week 11 gestation and obliterated
umbilical vessels occupy the space in the umbilical ring
Umbilical HerniaUmbilical Hernia• Clinical Manifestations:
– Herniated umbilicus protrudes with coughing, crying or straining
– Hernia can be reduced by pushing contents back into fibrous ring
– Most defects spontaneously resolve by 3-4 years of age as the muscular ring closes
– Surgery indicated in cases of strangulation, increased protrusion after 2 years of age or no improvement in large defect after 4 years.
Disorders of MotilityDisorders of Motility• Vomitting/ diarrhea• Gastroesophageal Reflux• Constipation and encorpresis• Hirschsprung disease• Parasitic disorders• Gastroenteritis
Gastroesophageal RefluxGastroesophageal Reflux• GER is the regurgitation of stomach
contents into the esophagus d/t an incompetent lower esophageal sphincter.
• Three mechanisms allow reflux to occur– Lower esphageal relaxations– Incompetent LES– Anatomic disruption of esophagogastric
junction (aka hiatal hernia)

Gastroesophageal RefluxGastroesophageal Reflux• What's the difference between GER
and GERD? • Gastroesophageal reflux (GER)
– is the backward flow of stomach contents up into the esophagus or the mouth. It happens to everyone. In babies, a small amount of GER is normal and almost always goes away by the time a child is 18 months old.
• Gastroesophageal reflux disease (GERD)– occurs when complications from GER arise,
such as failure to gain weight, bleeding, respiratory problems or esophagitis

How is GERD diagnosed?How is GERD diagnosed?• S/Sx include:
– presence of vomiting, pain associated with regurgitation, arching back (Sandifer syndrome) and feeding refusal.
– However, in very young infants, it may be difficult to differentiate GERD from normal GER or colic because some of the symptoms are similar—constant or sudden crying, spitting up or vomiting, hiccups, irritability or pain and refusal to eat. Infants with GERD can also have atypical symptoms, including respiratory problems.
GERDGERD• A small degree of reflux is common in all
infants• Incidence
– up18% of all infants– up to 70% w/ co-existing medical conditions
• Anatomy– Shorter intra-abdominal Esophagus– Immature LES– Swallow less while asleep
How is GERD diagnosed?How is GERD diagnosed?• Diagnoses: on hx alone (mild) or pH probe
or upper GI endoscopy• Tests include:
– endoscopic studies or – measuring the amount of reflux with pH-probes – A trial of medications may also be a useful
diagnostic tool. – In infants less than 3 months, try changing the
formula, if allergy is suspected.

Nonpharmacological Nonpharmacological TreatmentTreatment
• Try smaller, more frequent feedings. • Thickening the formula also helps. Adding rice
cereal makes the liquid less likely to slosh up out of the stomach into the esophagus. Studies show that even though the total amount of reflux may not change, the symptoms improve after the formulas are thickened.
• Keeping the baby upright before and after feedings will also decrease the amount of reflux.
• Burp several X’s during feeding• If bottle feeding, find a nipple that makes a good
seal to prevent air into mouth• If child is overweight, consult PCP to set weigh loss
goals
Medications for GERDMedications for GERD• The two major pharmacotherapies are H2-
blockers and proton pump inhibitors (PPIs), both of which are effective in decreasing acid secretion and have been used safely in children.
• Another group of drugs, prokinetics, can be prescribed to increase motility. – These are usually given with medications that
inhibit the acid. Examples are metaclopramide (Reglan) and cisapride (Propulsid).
• Antacids may be tried first in children with mild symptoms.
Medications for GERDMedications for GERD• H2 receptor blockers:
– help decrease the amount of acid the stomach makes, which, in turn, will cut down on the heartburn associated with reflux.• H2-blockers include:
– cimetidine (Tagamet) – ranitidine (Zantac) – famotidine (Pepcid) – nizatidine (Axid).
Medications for GERDMedications for GERD• Proton-Pump inhibitors:
– Prevent excess acid secretion in the stomach• omeprazole (Prilosec) • lansoprazole (Prevacid) • pantoprazole (Protonix) • rabeprazole (Aciphex).

SurgerySurgery• Management of severe GERD:
– Nissen fundoplication—the fundus of the stomach is wrapped around the distal esophagus to increase LES pressure.
GERDGERD• Nursing Care
– Risk for Aspiration related to reflux– Fluid Volume deficit related to reflux– Imbalanced nutrition, less than body
requirements• Teaching
– Feeding techniques– Positioning– Medication administration
ConstipationConstipation• Constipation is a common complaint
and accounts for 25% of GI referrals• Affects 3% of preschool-age children
and 1-2% of school-age children– (For Infants) Defined by criteria of
• Pebble-like hard stools for a majority of BM’s X 2 weeks
• Firm stools more than twice/week x 2 weeks
Constipation Constipation • Constipation…think hardness, not
frequency• Constipation may result from defects
in filling, or more commonly emptying, or the rectum.
• Please refer to Table 30-5 in text.
ConstipationConstipation• Constipation can be caused by
underlying disease, diet or psychological factors
• Three types of constipation– Normal-Transit constipation (functional
constipation)– Defecation Disorders– Slow-transit constipation
• Fewer than 1/week BM’s

ConstipationConstipation• Nursing Care• Important Education
– Dietary– Medications– Fluids
Medical Management of Medical Management of ConstipationConstipation
• Usually involves 2 stages (for severe constipation)– Soften stool (Lactulose)– Evacuate stool (laxative)
• Meds:– Osmotic Laxatives= lactulose, sorbitol, MOM,
Polyethylene glycol (Miralax)– Lubricants= Mineral Oil– Stimulant Laxatives= Dulcolax, Senna– Stool Softeners= Colace
EncorpresisEncorpresis• Abnormal elimination pattern
characterized by the recurrent soiling or passage of stool at inappropriate times.
• 1% of school-age children• Primary vs Secondary encorpresis• Retention of stool of lower bowel/ rectum,
leads to constipation, dilation of lower bowel and incompetence of the inner sphincter
EncorpresisEncorpresis• Dx:
– made on hx and PE, may perform barium enema to r/o organic causes
• Tx:– Behavior modification– Dietary changes– Clear out impacted stool– Bowel program
• Nursing care:– Centered around educating the child and
parents about the disorder and its tx– Reassurance/ emotional support
Hirschsprung’s DiseaseHirschsprung’s Disease• Congenital aganglionic megacolon• Absence of ganglion cells in the colon
results in mechanical obstruction due to inadequate motility
• Most common area affected is rectosigmoid colon
Hirschspung’s DiseaseHirschspung’s Disease• Etiology? Usually congenital, often a
familial defect. – Also associated w/ Down’s Syndrome– And anomalies of urinary tract
• As stool enters the affected area, it remains there until additional stool pushes it through. The affected part of the colon dilates; a mechanical obstruction may result

Hirschsprung’s DiseaseHirschsprung’s Disease

Hirschsprung’s DiseaseHirschsprung’s Disease• Clinical Manifestations:
– Failure to pass meconium within 24 hours– Constipation during first month of life– Bile-stained emesis– Abdominal distension– Distended abdomen– Reluctance to eat– Failure to thrive– V/D; stool w/ ribbon-like appearance
Hirschsprung’s DiseaseHirschsprung’s Disease• Diagnosis:
– Digital examination of rectum reveals absence of stool followed by explosive release of gas
– Barium enema– Rectal biopsy makes definitive diagnosis
– absence of ganglion cells
Hirschsprung’s Disease Hirschsprung’s Disease TreatmentTreatment
• Surgery to remove aganglionic bowel– Usually 2 stagesSurgery – (if complete obstruction)– First stage – temporary colostomy (until infant weighs 8-
10kg or 10mos-1yr)—to decompress the colon– Second stage – Abdominal pull-through with excision of
aganlionic segment and reanastomosis
• NG tube is generally inserted preop• Milder cases
– Dietary modification, stool softeners, and isotonic irrigation to prevent impaction

Hirschsprung’s DiseaseHirschsprung’s Disease• Nursing Care
– Monitor F/E balance– Maintain nutrition– Pre- and Post-Op care– Pain relief– Promote bowel program
• Nursing Diagnoses– Constipation related to aganglionic bowel– Post-op: Altered skin integrity– Post-op: Risk for Infection– Post-op: Pain– Post-op: Risk for Fluid volume deficit/altered
nutrition < body requirements
GastroenteritisGastroenteritis
• Gastroenteritis– inflammation of the stomach and small and
large intestines. It is an infection caused by viruses, bacteria or parasites.
– Commonly manifested as diarrhea– Children under 5 years, 2 cases/year average
• Gastroenteritis caused by viruses may last 1-2 days. – Viral Gastroenteritis accounts for 70-80% of
acute diarrhea in North America. • Bacterial cases can last a week or more.• Complications include: Dehydration,
electrolyte and acid base disturbance, bacteremia and sepsis and malnutrition
DiarrheaDiarrhea• What is it?
– Watery stool, increased frequency or both
• Acute vs Chronic Diarrhea– Acute: lasting less than 2 weeks, which is
usually r/t bacterial or viral infections; most common childhood reason for Diarrhea= Rotavirus
– Chronic: lasting longer than 2 weeks, usually r/t functional disorders, such as IBS, or diseases such as UC or Crohn’s disease
DiarrheaDiarrhea• What causes Diarrhea?
– Bacterial, viral or parasitic infection– Food intolerances or allergies– Reaction to medications– Diseases such as Chron’s Disease or UC– Refer to Table 30-6 for Other causes of
Diarrhea in Children
• Meds used to tx Diarrhea– Metronidazole (Flagyl)- anerobic bacteria,
some parasites and in combination for H pylori– Imodium (an anti-diarrheal)
Parasitic DisordersParasitic Disorders• Chart on page 1132 reviews major
parasites
Inflammatory DisordersInflammatory Disorders• Peptic Ulcer• Appendicitis• Necrotizing Enterocolitis• Meckel’s Diverticulum• Recurrent Abdominal Pain• Inflammatory Bowel Disease
Peptic UlcerPeptic Ulcer• Definition: peptic ulcer is erosion in the
lining of the stomach or duodenum (the first part of the small intestine). The word “peptic” refers to pepsin, a stomach enzyme that breaks down proteins.
• Small ulcers may not cause any symptoms. Large ulcers can cause serious bleeding . Most ulcers occur in the first layer of the inner lining. A hole that goes all the way through is called a perforation of the intestinal lining.

What causes Peptic Ulcers?What causes Peptic Ulcers?• Something damages the stomach lining.• The most common cause of such damage is a
bacterium called Helicobacter pylori (H.pylori) . • Most people with peptic ulcers have this organism
living in their gastrointestinal (GI) tract.• Other factors can make it more likely for you to
get an ulcer , including: – Using aspirin, ibuprofen, or naproxen – Drinking alcohol excessively – Smoking cigarettes and using tobacco

Peptic UlcersPeptic Ulcers• Symptoms • Abdominal pain is a common symptom
but it may not always be present. • Other possible symptoms include:
– Nausea , vomiting – Weight loss – Fatigue – Heartburn , indigestion , belching – Chest pain– Blood-tinged emesis – Bloody or dark tarry stools
Peptic UlcersPeptic Ulcers• Dx: upper GI, or esophagogastroduodenoscopy,
and Guiac of stool and CBC w/ diff• Tx: A combination of medications to kill the H
pylori, reduce acid levels, and protect the GI tract.
• Medications include:– Antibiotics to kill Helicobacter pylori– Acid blockers (like cimetidine, ranitidine, or
famotidine) – Proton pump inhibitors (such as omeprazole)– Bismuth (may help protect the lining and kill the
bacteria)
AppendicitisAppendicitis• Appendicitis= inflammation of the
appendix• Occurs most often in adolescent males
(10-19yr)• Caused when the opening from the
appendix into the cecum becomes blocked. – The blockage may be due to a build-up of thick
mucus within the appendix or to stool that enters the appendix from the cecum.
– As edema continues, vascular supply is compromised, bacteria followed by an immune response…can lead to rupture.

Appendicitis Appendicitis • Appendicitis should be suspected in any
child with pain in the RLQ• Symptoms• Two types of presentation: typical and atypical.
– The typical history includes pain starting centrally (periumbilical) before localizing to the right iliac fossa (the lower right side of the abdomen)
– Pain is usually associated with loss of appetite and fever– Nausea or vomiting– Lethargy– Atypical symptoms may include pain beginning and
staying in the right iliac fossa, diarrhea and a more prolonged, smoldering course.

AppendicitisAppendicitis• Signs
– These include localized findings in the right iliac fossa.
– Periumbilical tenderness– Abdominal tenderness– rebound tenderness – digital rectal examination elicits tenderness – Coughing causes point tenderness at
McBurney's point – Guarding upon palpation, suspect Peritonitis
II
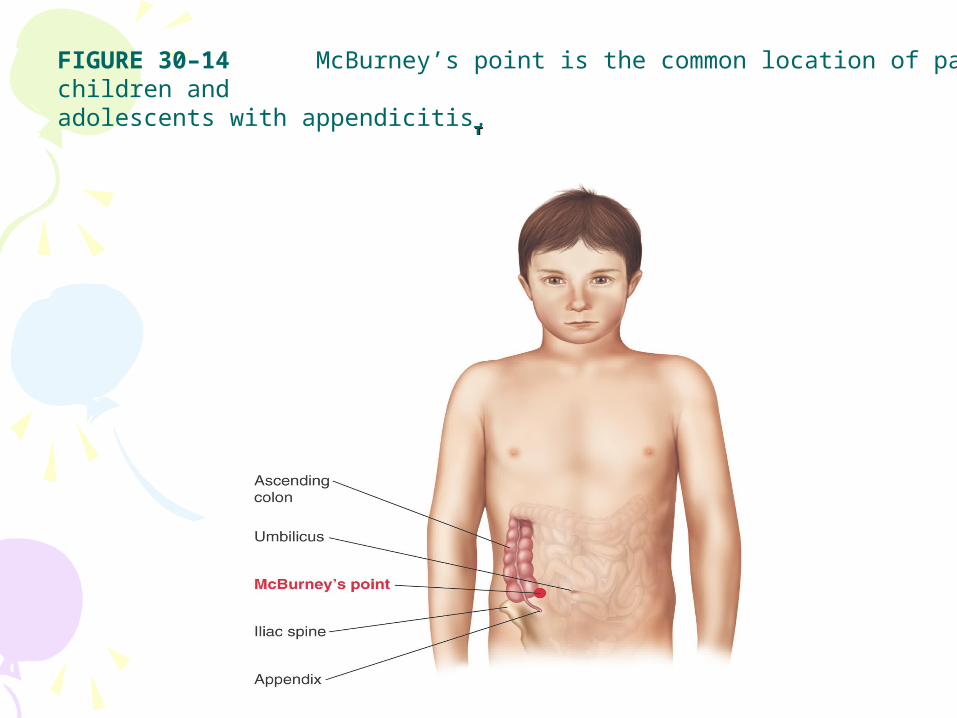
FIGURE 30–14 McBurney’s point is the common location of pain in children and adolescents with appendicitis.
AppendicitisAppendicitis• Other signs include:
– Rovsing's sign• Deep palpation of the left iliac fossa may cause pain
in the right iliac fossa. – Psoas sign
• Occasionally, an inflamed appendix lies on the psoas muscle and the patient will lie with the right hip flexed for pain relief.
– Obturator sign• If an inflamed appendix is in contact with the
obturator internus, spasm of the muscle can be demonstrated by flexing and internally rotating the hip. This Maneuver will cause pain in the hypogastrium.

AppendicitisAppendicitis• Diagnosis is based on Hx and PE• Abdominal CT or ultrasound
– For atypical presentation
• Labs: CBC w/ diff– Also an elevation of neutrophilic white
blood cells. – Pregnancy test to r/o ectopic pregnancy
AppendicitisAppendicitis• Nursing Care• Pre and Postoperative care
– NPO, IVFs– Correction of fluid and electrolyte deficits– Surgical incision– Antibiotics
• Nursing Diagnosis– Pain– Risk for Infection

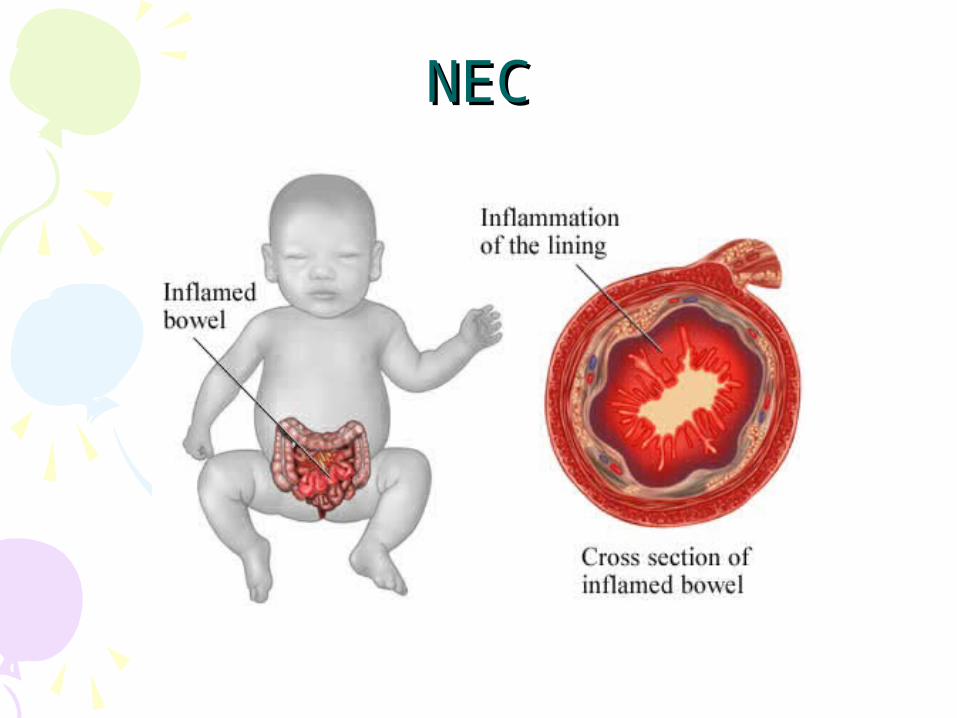
Necrotizing Enterocolitis Necrotizing Enterocolitis (NEC)(NEC)
• A medical condition primarily seen in premature infants, where portions of the bowel undergo necrosis. Potentially life-threatening inflammatory disease.
• Most common GI emergency occurring during the neonatal period
• Etiology is multifactorial:– Intestinal ischemia– Bacterial or viral infection– Immaturity of the GI mucosa
NECNEC
NECNEC• Clinical manifestations occur b/t 3-14 doa,
but can occur as early as the first day of life and as late as 3 months of age.Initial symptoms include: – feeding intolerance (increased gastric
residuals, vomitting, irritability, and abdominal distension)
– Bloody stools– Decreased UO– Bile-stained emesis – Symptoms may progress rapidly to abdominal
discoloration with intestinal perforation and peritonitis and systemic hypotension requiring intensive medical support.

NECNEC• Clinical Triad:
– Abdominal distension– Bilious vomiting– Bloody stools
• Dx: – PE – the presence of free peritoneal gas, and abd
wall changes on X-ray– Heme + stool– Labs: anemia, leukopenia, leukocytosis,
thrombocytopenia, electrolyte imbalances
NECNEC
NECNEC• Nursing care:
– Observe for feeding intolerance– Abdominal exam: Measure abdominal
circumference, and assess BS Q-8 Hrs– Monitor VS and I/O’s– Pre and Post Op care
• Nursing Dx– Risk for Infection– Ineffective Tissue Perfusion– Imbalanced Nutrition

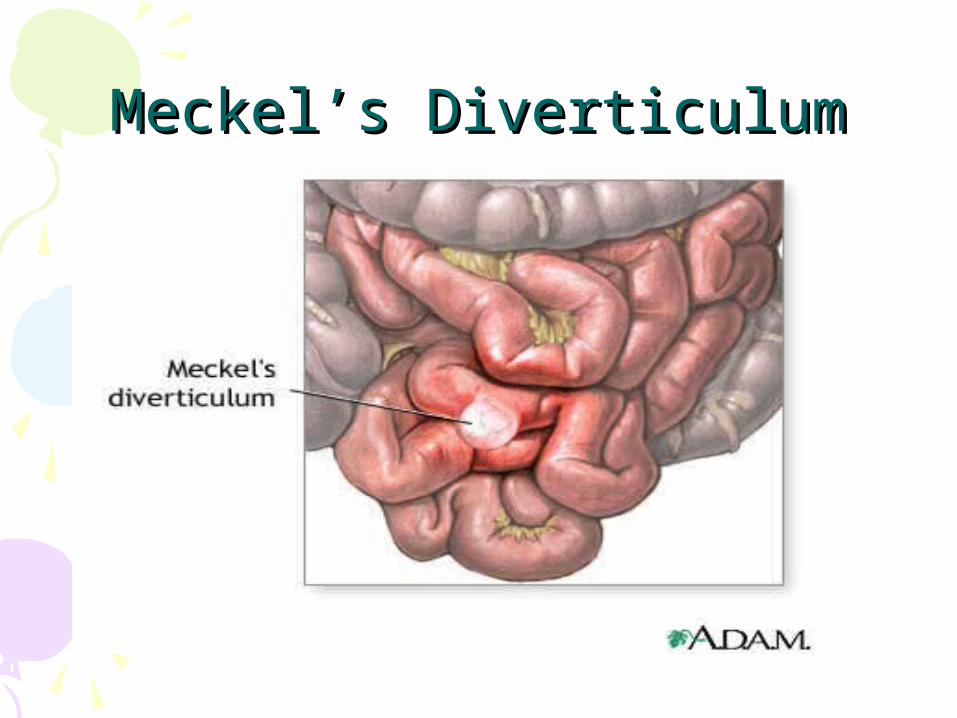
Meckel’s DiverticulumMeckel’s Diverticulum• Meckel's diverticulum is one of the most common
congenital abnormalities. • It occurs when the connection between the
intestine and the umbilical cord doesn't completely close off during fetal development.
• This results in a small outpouching of the small intestine.
• In some cases, the diverticula can become infected (diverticulitis) cause an obstruction of the instesitne, or cause bleeding from the intestine.
• The most common symptom of Meckel's diverticulitis is painless bleeding from the rectum. The stools may contain fresh blood or may look black and tarry.
Meckel’s DiverticulumMeckel’s Diverticulum• Omphalomesenteric duct fails to
atrophy• Outpouching of the ileum remains
and contains gastric contents causing ulceration
• Bowel obstruction, perforation or peritonitis can occur
Meckel’s DiverticulumMeckel’s Diverticulum
Meckel’s DiverticulumMeckel’s Diverticulum• Rule of 2’s• Bowel obstruction is the most
common complication • Dx: made on hx• Tx: surgical incision• Nursing Care:
– Pre and Postoperative care (similar to other abdominal surgery)
Recurrent Abdominal PainRecurrent Abdominal Pain• Frequent problem among young children
and adolescents, especially school-aged girls
• Organic causes uncommon, but need to be r/o.
• Pain is generally in periumbilical area and occurs on a regular basis
• The hx should examine the pressure’s and stresses in child’s life
• Nursing care: centered around supporting child during assessment and dx tests
• ? Mental health referral
Inflammatory Bowel DiseaseInflammatory Bowel Disease• Crohn’s Disease and Ulcerative Colitis
– Faulty regulation of the immune response of the intestinal mucosa
– Usually genetically triggered– Crohn’s disease can cause inflammation
and ulcers anywhere throughout the GI tract• Mouth to anus
– Ulcerative colitis effects large intestine and rectal mucosa
Crohn’s DiseaseCrohn’s Disease• Clinical Manifestations:
– Abdominal pain (esp RLQ)– Rectal bleeding – Diarrhea– Fever– Weight loss– Arthritis – Skin problems– Delayed growth
• Lesions are full-thickness, extend into bowel wall• Affects anywhere in GI tract (illeum, colon and
rectum most common sites)• More common in whites, age 15-25
Crohn’s DiseaseCrohn’s Disease• Complications:
– Intestinal Blockage:• Thickening of the intestinal wall w/
swelling= freq diarrhea; also leads to scar tissue
– Fistulas• Tunnels through affected area to
surrounding tissues of bladder, vagina, skin
– Nutritional complications• Deficiencies of proteins, calories, vitamins

Crohn’s DiseaseCrohn’s Disease• Treatment of Crohn’s Disease:
– may include drugs, nutrition supplements, surgery, or a combination of these options.
– The goals of treatment are to control inflammation, correct nutritional deficiencies, and relieve symptoms like abdominal pain, diarrhea, and rectal bleeding.

Ulcerative ColitisUlcerative Colitis• A form of colitis that causes inflammation
and ulcers in the lining of the rectum and colon
• Surgery can cure the disease– Illeostomy– Illeoanal anastomosis “pull through”
• More common in Jewish descent• Average onset b/f 20 yr; peak onset 12 yrs• 5% of UC develop colon cancer
Ulcerative ColitisUlcerative Colitis• Clinical Manifestations:
– Cramping abdominal pain– Rectal bleeding– Diarrhea– Fever– Anorexia– Growth failure– Malaise – Extraintestinal manifestations: joint pain
and swelling, skin lesions, arthritis, uveitis
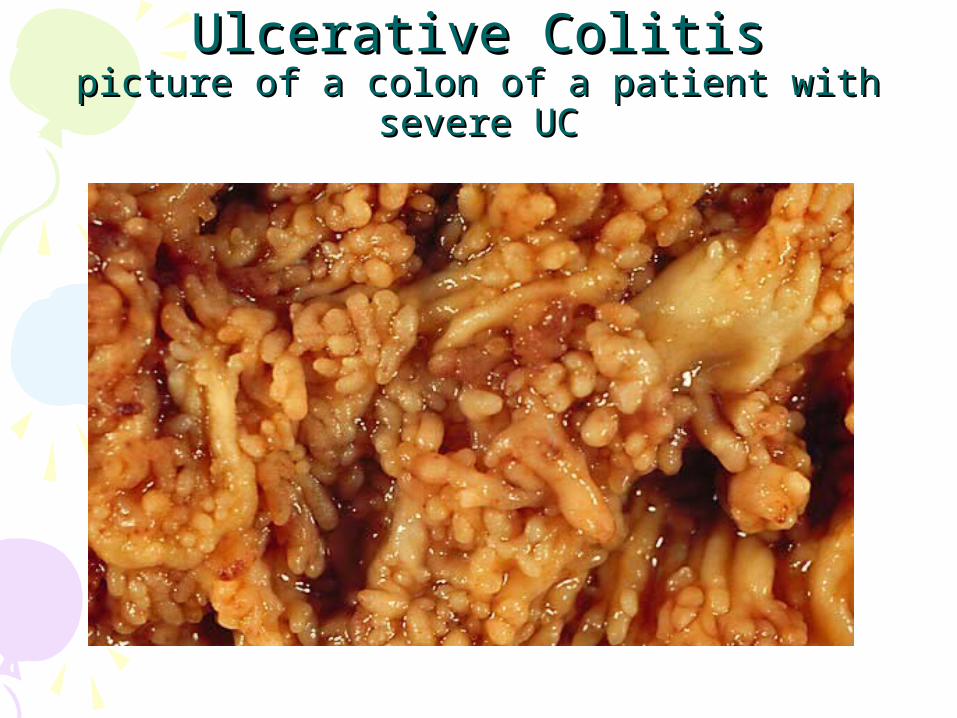
Ulcerative ColitisUlcerative Colitispicture of a colon of a patient with severe UCpicture of a colon of a patient with severe UC
IBDIBD• Treatment:
– Includes pharmacologic interventions (abx, antiinflammatory, immunosuppressive and antidiarrheal meds)
– Nutrition modification– Surgery– Pharmacologic Therapy: see Table on p
1142

IBDIBD• Nursing care:
– Help child/ family adjust to chronic disease– Help family to find community support– Educatate family/ child on
• s/sx of flare-ups• Med teaching• Monitor nutritional status
• Nursing Assessment:– Assess for abdominal distension, tenderness
and pain– Monitor BS, measure abdominal girth
Disorders of MalabsorptionDisorders of Malabsorption• Malabsorption occurs when a child is
unable to digest or absorb nutrients in the diet. Disorders of malabsorption– Short Bowel Syndrome– Celiac Disease– Lactose Intolerance– (Cystic Fibrosis)
Short Bowel SyndromeShort Bowel Syndrome• Due to shortened
intestine after surgical resection of a portion of the intestines
• Sxs depend on which area of the bowel was resected
Illeum Bile salts, f/e’s, absorption decrease cuasing diarrhea, statorrhea, decreased absorption of fat soluble vits
Colon f/e mgmt is impaired
Jejunum Mostly compensated for by other bowel
Short Bowel SyndromeShort Bowel Syndrome• The symptoms of short bowel
syndrome can include:– Abdominal pain – Diarrhea and steatorrhea (oily or sticky
stool, which can be particularly foul-odored)
– Fluid retention – Weight loss and malnutrition– Fatigue
Celiac DiseaseCeliac Disease• Also known as celiac sprue or gluten-
sensitive enteropathy • A chronic malabsorption syndrome
more common in white Europeans• Immunologic disorder characterized
by intolerance for gluten found in wheat, barley, rye and oats. Affects fat absorption
• ? Genetic factors
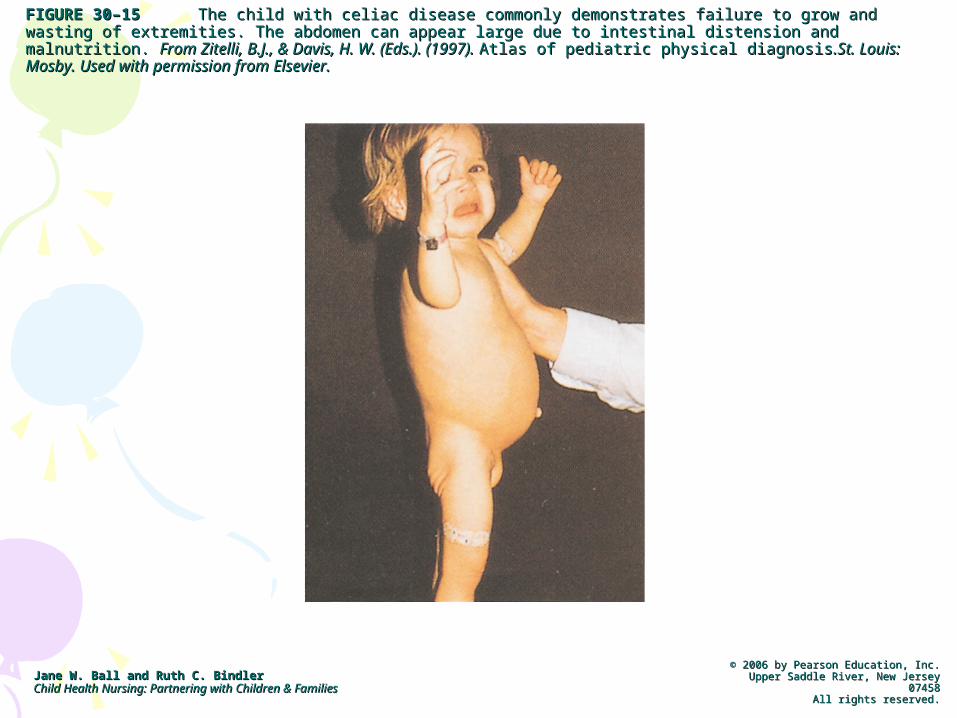
FIGURE 30–15FIGURE 30–15 The child with celiac disease commonly demonstrates failure to grow and wasting of The child with celiac disease commonly demonstrates failure to grow and wasting of extremities. The abdomen can appear large due to intestinal distension and malnutrition. extremities. The abdomen can appear large due to intestinal distension and malnutrition. From Zitelli, B.J., & From Zitelli, B.J., & Davis, H. W. (Eds.). (1997). Davis, H. W. (Eds.). (1997). Atlas of pediatric physical diagnosisAtlas of pediatric physical diagnosis.St. Louis: Mosby. Used with permission from .St. Louis: Mosby. Used with permission from Elsevier.Elsevier.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
Celiac DiseaseCeliac Disease• Clinical manifestations:
– Diarrhea– FTT– Abdominal pain– Large quantities of fat in stool– Stools are greasy, foul smelling, frothy, and
excessive– Eventually may develop protein deficiency
with wasted musculature, and abd distension

Celiac DiseaseCeliac Disease• Diagnostic Tests
– Fectal fat content– Duodenal biopsy– Trial of gluten free diet– Serum screening for IgA
• Tx– Diet modification: Gluten-free diet– Do not eat anything that contains the following grains:
wheat, rye, and barley. – The following can be eaten in any amount: corn,
potato, rice, soybeans, tapioca, arrowroot, carob, buckwheat, millet, amaranth and quinoa.
Lactose IntoleranceLactose Intolerance• Inability to digest lactose d/t deficiency of
enzyme Lactase, which is produced by the cells that line the small intestine
• Lactose is a disaccharide found in dairy products
• Symptoms include:– Explosive, watery diarrhea– Abdominal pain, distension– Excessive flatus
• Dx– Hx– Hydrogen breath test– Stool acidity test (lactic acid buildup)

Lactose IntoleranceLactose Intolerance• Treatment and nursing care:
– Reduce/ eliminate lactose in diet– Infants switch to soy-based formula– Switch to soy-based formula– Lactaid tablets for older children (aid in
digestion of lactose)– Assure enough calcium in diet– Nursing care: supportive tx
Hepatic DisordersHepatic Disorders• Hyperbilirubinemia of the newborn• Biliary atresia• Viral hepatitis• Cirrhosis

Hepatic DisordersHepatic Disorders• Signs of Hepatic Disorders
– Jaundice– Easy bruising, intense itching– White or clay-colored stools– Tea-colored urine
Hyperbilirubinemia of the Hyperbilirubinemia of the NewbornNewborn
• Bilirubin: a yellow pigment produced from the breakdown of RBCs
• Newborns have more RBCs/kg than adults• They produce more bilirubin than their
livers are capable of metabolizing• Preterm infant more at risk for hyperbilirub
d/t an even shorter RBC lifespan, and impaired bilirubin conjugation d/t liver immaturity
HyperbilirubinemiaHyperbilirubinemia• Majority of newborns experience
some degree of jaundice in the 1st week of life– Self-limiting– Bilirubin levels peak b/t the 3-5th dol– Hyperbilirubinemia: a level of bilirubin in
the blood that requires intervention to prevent CNS damage

HyperbilirubinemiaHyperbilirubinemia• Pathophysiology• Neonatal physiologic jaundice results from
simultaneous occurrence of the following 2 phenomena: – Bilirubin production is elevated because of
increased breakdown of fetal erythrocytes. This is the result of the shortened lifespan of fetal erythrocytes and the higher erythrocyte mass in neonates.
– Hepatic excretory capacity is low both because of low concentrations of the binding proteins responsible for making bilirubin water soluble (conjugation).
HyperbilirubinemiaHyperbilirubinemia• Bottom line:
– Unbound, free and unconjugated bilirubin is not water soluble…therefore it can’t be excreted from circulation…it moves to fatty tissue, leading to jaundice.
– How is it removed from the system?• Uncong. Bili. Attaches to albumin, then
moves to the liver, where it b/c “conjugated” into direct bilirubin
• Direct bilirubin= water soluble, and excreted into small intestine
HyperbilirubinemiaHyperbilirubinemia• Clinical Manifestations of newborn
jaundice:– 1st evident on the face, and progresses
downward to trunk etc.• Symptoms of hyperbilirubinemia
– Visible jaundice heat to toe, including sclerae– Lethargy or irritability– Poor breastfeeding or bottle feeding
• Symptoms of acute bilirubin encephalopathy:– Lethargy– Hypotonia– Poor sucking ability
HyperbilirubinemiaHyperbilirubinemia• Nursing care:
– ID newborn’s at risk/ observe s/sx of jaundice– Promote successful BF/ refer for lactation
support– Educate parents re: newborn jaundice
• Nursing assessment: refer to Table 30-5 in text
• Tx:– Phototherapy– Hydration– IV y-Globulin– Exchange transfusion– Tin-mesoporphyrin (med)
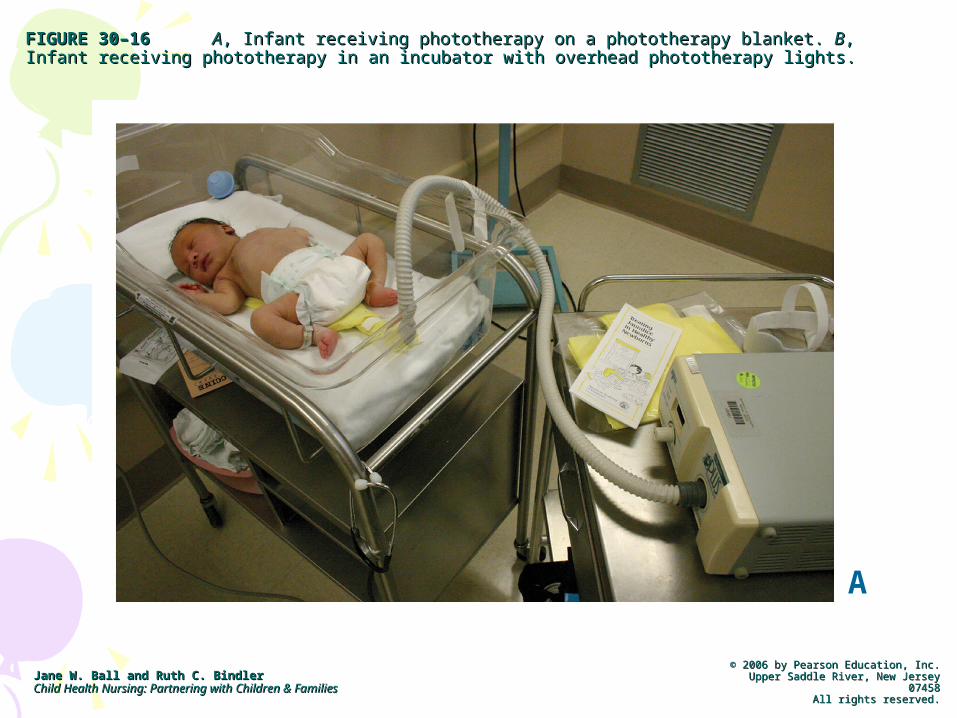
FIGURE 30–16FIGURE 30–16 AA, Infant receiving phototherapy on a phototherapy blanket. , Infant receiving phototherapy on a phototherapy blanket. BB, Infant receiving , Infant receiving phototherapy in an incubator with overhead phototherapy lights. phototherapy in an incubator with overhead phototherapy lights.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
A
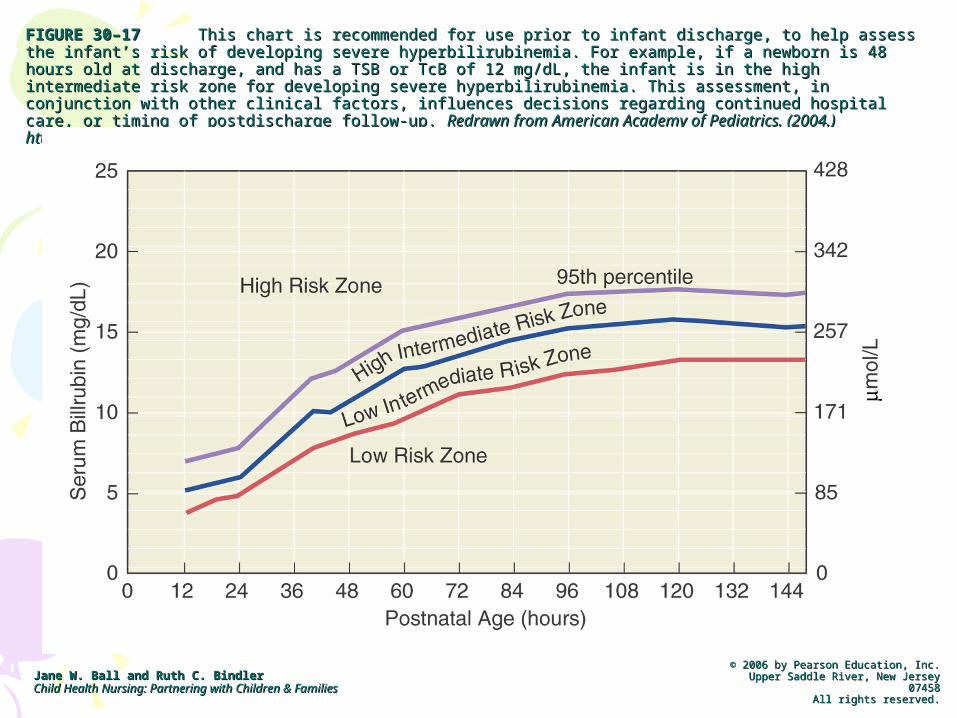
FIGURE 30–17FIGURE 30–17 This chart is recommended for use prior to infant discharge, to help assess the infant’s risk This chart is recommended for use prior to infant discharge, to help assess the infant’s risk of developing severe hyperbilirubinemia. For example, if a newborn is 48 hours old at discharge, and has a TSB of developing severe hyperbilirubinemia. For example, if a newborn is 48 hours old at discharge, and has a TSB or TcB of 12 mg/dL, the infant is in the high intermediate risk zone for developing severe hyperbilirubinemia. or TcB of 12 mg/dL, the infant is in the high intermediate risk zone for developing severe hyperbilirubinemia. This assessment, in conjunction with other clinical factors, influences decisions regarding continued hospital This assessment, in conjunction with other clinical factors, influences decisions regarding continued hospital care, or timing of postdischarge follow-up. care, or timing of postdischarge follow-up. Redrawn from American Academy of Pediatrics. (2004.) Redrawn from American Academy of Pediatrics. (2004.) http://aappolicy.aappublications.org/cgi/content/full/pediatrics; 114/1/297.pdf, accessed 1/20/05.http://aappolicy.aappublications.org/cgi/content/full/pediatrics; 114/1/297.pdf, accessed 1/20/05.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
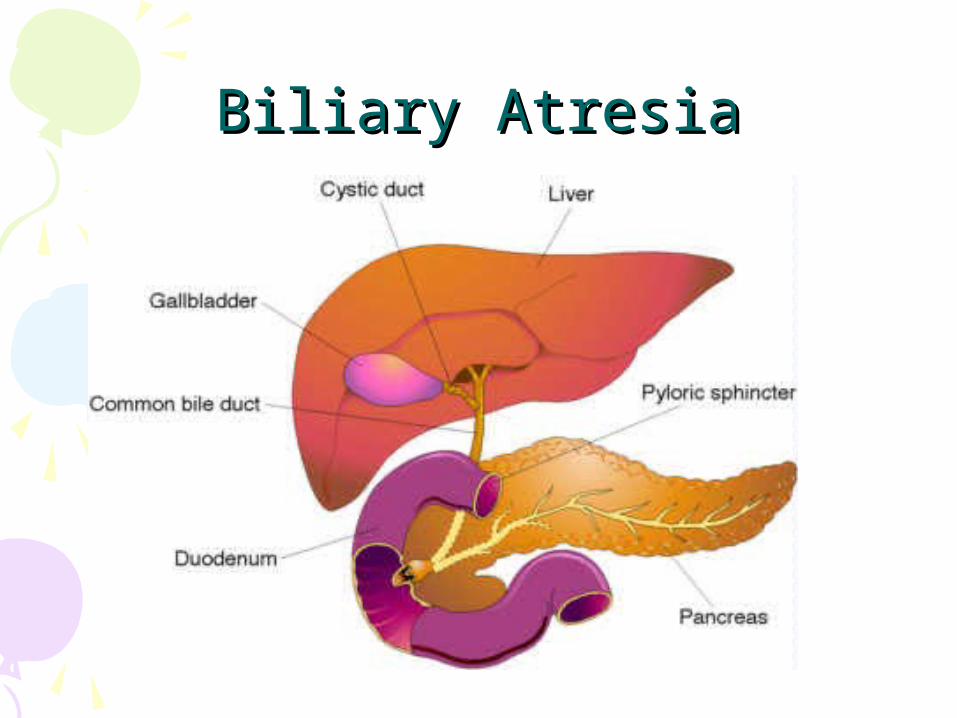
Biliary AtresiaBiliary Atresia• The pathologic closure or absence of
hepatic or common bile ducts at any point from the porta hepatic to the duodenum
• The disorder leads to cholestasis, fibrosis, and cirrhosis
• Most common pediatric liver disease necessitating transplantation and the most common cause of infant jaundice
Biliary AtresiaBiliary Atresia• Etiology: unknown• Blockage of bile flow from the liver to
duodenum causes inflammation and fibrotic changes.
• Lack of bile acids also interferes with digestion of fat-soluble vits (K,A,D,E), leading to steatorrhea and nutritional deficits
• Without tx, disease is fatal
Biliary AtresiaBiliary Atresia

Biliary AtresiaBiliary Atresia• Clinical Manifestations:
– Newborn is initially asymptomatic– Jaundice around 2-3 weeks– Abdominal distension– Increase in bilirubin levels– Splenomegaly– Easy bruising, prolonged bleeding time and
intense itching– Tea-colored urine– Clay-colored stools– Ftt/ malnutrition

Biliary AtresiaBiliary Atresia• Dx: hx, PE and labs• Tx: surgery to correct obstruction• Liver Transplantation• Nursing care: pre and postoperative,
teach the family, and prepare for organ transplant

Viral HepatitisViral Hepatitis• An inflammation of the liver caused
by a viral infection– Can be acute or chronic disease– Acute: rapid onset, can dev into chronic– Hep A (HAV)– Hep B (HBV)– Hep C (HCV)– Hep D (HDV)– Hep E (HEV)
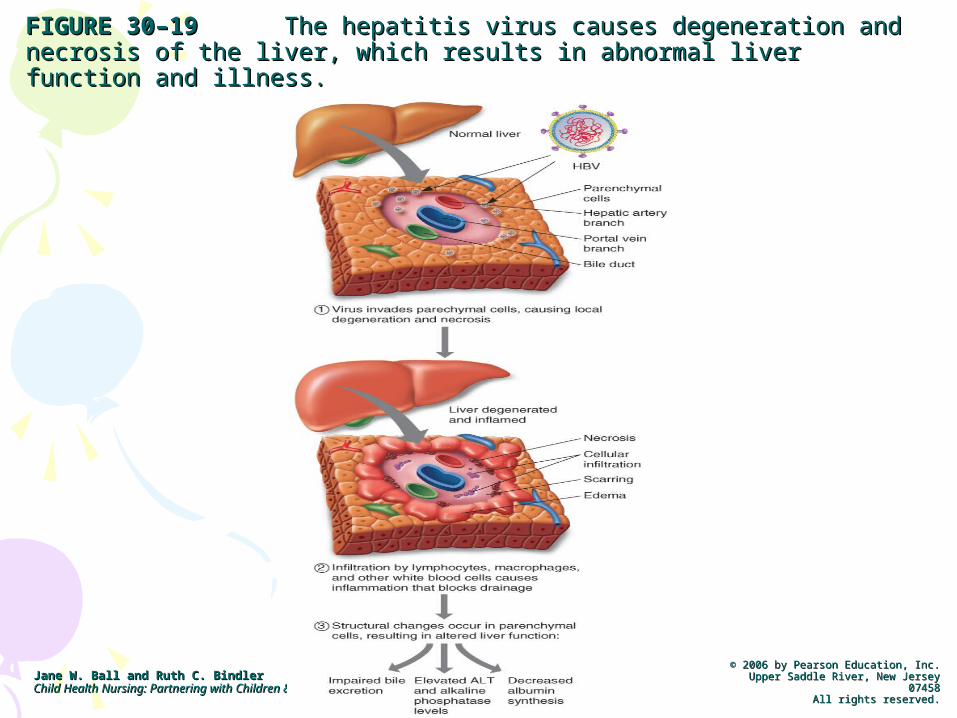
FIGURE 30–19FIGURE 30–19 The hepatitis virus causes degeneration and necrosis The hepatitis virus causes degeneration and necrosis of the liver, which results in abnormal liver function and illness.of the liver, which results in abnormal liver function and illness.
Jane W. Ball and Ruth C. BindlerJane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & FamiliesChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458Upper Saddle River, New Jersey 07458
All rights reserved.All rights reserved.
Viral HepatitisViral Hepatitis• Nursing Care:
– Prevent spread of disease– Provide fluid and nutritional support– Promote G&D– Reduce risk of complications– Support child and family
• Refer to Table 30-8 for Comparison of major types Hepatitis Types
• Refer to Table 30-9 for transmission, immunization and prophylaxis for hepatitis
CirrhosisCirrhosis• Degenerative disease process that
results in fibrotic changes and fatty infiltration in the liver
• Clinical Manifestations of cirrhosis vary
• End-stage liver failure• Tx: liver transplant

Injuries to the Injuries to the Gastrointestinal SystemGastrointestinal System
• Trauma• Ingestion of foreign objects• Lead poisoning
Abdominal TraumaAbdominal Trauma• May be caused by blunt or penetrating
trauma• Type of injury determines extent of organ
damage• Dx: Hx, PE, CTscan, FAST (focused abd
sonogram for trauma)• Nursing care:
– Provide emotional support– Follow care orders– Prevention teaching once stabilized
Poisons IngestionPoisons Ingestion• Poisonings are the 2nd leading cause
of unintentional home-injury • Do not use ipecac• Airway, hemodynamic stability,
remove toxin and support• Education on prevention• Most common poison????• Refer to Table 30-8 for Emergency Management
of Poisoning
Lead PoisoningLead Poisoning• A medical condition caused by increased
levels of the metal lead in the blood. • Lead may cause irreversible neurological
damage as well as renal disease, cardiovascular effects, and reproductive toxicity.
• Healthy People 2010 goal: eliminate childhood lead poisoning as a public health issue in the U.S.
Lead PoisoningLead Poisoning• Routes of exposure:
– Mostly through lead-based paint in older homes
– Pain can chip and flake into dust which settles on the floor
– Children explore through putting things in their mouths.
Lead PoisoningLead Poisoning• Other sources of lead exposure:
– Water from lead pipes– Lead solder on canned foods– Lead ammunition– Pool cue chalk– Collectible toys– Jewelry
Lead poisoningLead poisoningWhy are children at greater risk?Why are children at greater risk?
• Children are at greater risk of lead poisoning because they absorb and retain more lead in proportion to their weight than adults do.
• Causes problems with normal cell function:– Nervous system—can cause irreversible
damage to developing brain– Blood cells—displaces Iron, which decreases
Heme production– Kidneys—excreted through kidneys– Has an adverse affect on vitamin D and
calcium metabolism.
Lead PoisoningLead Poisoning• Toxicology/ Distribution• At least 99% of absorbed lead is
bound to erythrocytes upon entry into the bloodstreatm– 70% is stored in the bone
• Accumulates throughout life, but can be released during stress
• Can have a ½ life of as many as 20 years
– 30% moves to major soft tissue storage sites•Liver, kidney, bone marrow and BRAIN !

Lead PoisoningLead Poisoning• Pathophysiology: Lead toxicity can affect
any soft tissue of the body including:– Hematological – Renal – GI– Skeletal– Endocrine– CNS*** (Neurotoxicity w/in the Pediatric CNS is
most detrimental pathology)

Lead poisoningLead poisoning
• Three routes for absorption of lead in children’s body:– GI, Inhalation and Transplacental
• Clinical Manifestations:– Depend upon the degree of toxicity:
• Decreased IQ scores.• Cognitive deficits.• Loss of hearing.• Growth delays.

Lead PoisoningLead Poisoning• S/Sx:• Acute Lead Poisoning:
– N/V– Anorexia– Constipation– Abdominal Pain

Chronic Lead Poisoning Chronic Lead Poisoning • Neurocognitive effects
– Developmental delay
– Lower IQ– Speech and
language problems– Reading skills
deficits– Learning disabilities– Lowered academic
success
• Behavioral effects– Aggression– Hyperactivity– Impulsivity– delinquency– Disinterest– Withdrawal
Lead Poisoning TreatmentLead Poisoning Treatment• Primary Prevention• Secondary Prevention• Depending upon Lead levels:
– Recent studies suggest that adverse health effects exist in children at blood lead levels less than10 µg/dL (CDC)
– Pb-B 10 to 19 micrograms/dL – need to remove identifiable sources
– Chelation tx is indicated if BLL greater than 45ug/dl• (Succimer, EDTA, and BAL)

Lead PoisoningLead Poisoning• Nursing Assesment:• Obtain a complete medical history.
– Developmental progress.– Problems with attention.
• Obtain Lead level results.
Foreign Object IngestionForeign Object Ingestion• Assessment important• Prepare child and parents for x-rays
and possible removal• Education on prevention
The End!!The End!!





























