Embed Size (px)
Citation preview

Health Alterations IIManagement of Clients
with Problems of the Gastrointestinal System
Lecture 2.2Lecture 2.2Disorders of the Esophagus

The main symptoms of the esofageal disorders:
Dysphagia (difficulty swallowing)
Odynophagia (acute pain on swallowing)

Achalasia
Achalasia is an absent or ineffective peristalsis of the distal esophagus, accompanied by failure of the esophageal sphincter to relax in response to swallowing

Clinical Manifestations
difficulty in swallowing both liquids and solidssensation of food sticking in the lower portion of the esophagusregurgitation of foodchest pain or heart-burn (pyrosis). This pain may or may not be assotiated with eating

Assessment and Diagnostic Findings
X-ray (dilatation above the narrowing). CT of the esofagus, barium swallowing, endoscopy may be used too diagnosis is confirmed by manometry

Management
The patient should be instructed to eat slowly and to drink fluids with meals. As a temporary measure, calcium channel blockers and nitrates have been used to decrease esophageal pressure and improve swallowing. Injection of botulinum toxin (Botox) to quadrants of the esophagus via endoscopy has been helpful because it inhibits the contraction of smooth muscle. Periodic injections are required to maintain remission. If these methods are unsuccessful, pneumatic (forceful) dilation or surgical separation of the muscle fibers may be recommended

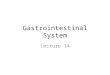
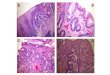
Achalasia may be treated conservatively by pneumatic dilation to stretch the narrowed area of the esophagus (fig. 1)
Pneumatic dilation has a high success rate. Although perforation is a potential complication, its incidence is low
The procedure can be painful; therefore, moderate sedation in the form of an analgesic or tranquilizer, or both, is administered for the treatment
The patient is monitored for perforation. Complaints of abdominal tenderness and fever may be indications of perforation

Fig. 1. Pneumatic dilation of the lower part of the esophagus

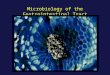
Achalasia may be treated surgically by esophagomyotomy (Fig. 2). The procedure usually is performed laparoscopically, either with a complete lower esophageal sphincter myotomy and an antireflux procedure, or without an antireflux procedure
The esophageal muscle fibers are separated to relieve the lower esophageal stricture.
Although patients with a history of achalasia have a slightly higher incidence of esophageal cancer, long-term follow-up with esophagoscopy for early detection has not proved beneficial

Fig. 2. Esophagomyotomy

Diffuse Spasm
Diffuse spasm is a motor disorder of the esophagusThe cause is unknown, but stressful situations can produce contractions of the esophagusIt is more common in women and usually manifests in middle age

Clinical Manifestations
Difficulty or pain on swallowing (dysphagia, odynophagia) Chest pain similar to that of coronary artery spasm

Assessment and Diagnostic Findings
Esophageal manometry, which measures the motility of the esophagus and the pressure within the esophagus, indicates that simultaneous contractions of the esophagus occur irregularlyDiagnostic x-ray studies after ingestion of barium show separate areas of spasm

Management
Conservative therapy includes administration of sedatives and long-acting nitrates to relieve pain
Calcium channel blockers have also been used to manage diffuse spasm
Small, frequent feedings and a soft diet are usually recommended to decrease the esophageal pressure and irritation that lead to spasm
Dilation performed by bougienage (use of progressively sized flexible dilators), pneumatic dilation, or esophagomyotomy may be necessary if the pain becomes intolerable

Hiatal Hernia
In a condition known as hiatus (or hiatal) hernia, the opening in the diaphragm through which the esophagus passes becomes enlarged, and part of the upper stomach tends to move up into the lower portion of the thorax
Hiatal hernia occurs more often in women than men

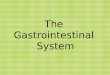
There are two types of hiatal hernias: sliding and paraesophageal
Sliding, or type I, hiatal hernia occurs when the upper stomach and the gastroesophageal junction (GEJ) are displaced upward and slide in and out of the thorax (Fig. 3a). About 90% of patients with esophageal hiatal hernia have a sliding hernia.
A paraesophageal hernia occurs when all or part of the stomach pushes through the diaphragm beside the esophagus (see Fig. 3b)

Fig. 2. The Hiatal Hernia Types

Clinical Manifestations
Sliding hernia: heartburn, regurgitation, and dysphagia, but at least 50% of patients are asymptomatic. Sliding hiatal hernia is often implicated in reflux
Paraesophageal hernia: sense of fullness after eating or asymptomatic. Reflux usually does not occur, because the gastroesophageal sphincter is intact
The complications of hemorrhage, obstruction, and strangulation can occur with any type of hernia

Assessment and Diagnostic Findings
Diagnosis is confirmed by x-ray studies, barium swallow, and fluoroscopy

Management
Management for an axial hernia includes frequent, small feedings that can pass easily through the esophagus. The patient is advised not to recline for 1 hour after eating, to prevent reflux or movement of the hernia, and to elevate the head of the bed on 4- to 8-inch (10- to 20-cm) blocks to prevent the hernia from sliding upward. Surgery is indicated in about 15% of patients
Medical and surgical management of a paraesophageal hernia is similar to that for gastroesophageal reflux; however, paraesophageal hernias may require emergency surgery to correct torsion (twisting) of the stomach or other body organ that leads to restriction of blood flow to that area

DiverticulumClinical Manifestations
Symptoms experienced by the patient with a pharyngoesophageal pulsion diverticulum include difficulty swallowing, fullness in the neck, belching, regurgitation of undigested food, and gurgling noises after eating. When the patient assumes a recumbent position,undigested food is regurgitated, and coughing may be caused by irritation of the trachea. Halitosis and a sour taste in the mouth are also common because of the decomposition of food retained in the diverticulum
Symptoms produced by midesophageal diverticula are less acute. One third of patients with epiphrenic diverticula are asymptomatic, and the remaining two thirds complain of dysphagia and chest pain
Dysphagia is the most common complaint of patients with intramural diverticulosis

Assessment and Diagnostic Findings
A barium swallow may be performed to determine the exact nature and location of a diverticulum
Manometric studies are often performed for patients with epiphrenic diverticula to rule out a motor disorder
Esophagoscopy usually is contraindicated because of the danger of perforation of the diverticulum, with resulting mediastinitis
Blind insertion of a nasogastric tube should be avoided

Management
Because pharyngoesophageal pulsion diverticulum is progressive, the only means of cure is surgical removal of the diverticulumPostoperatively, the patient may have a nasogastric tube inserted at the time of surgery. The surgical incision must be observed for evidence of leakage from the esophagus and a developing fistula. Food and fluids are withheld until x-ray studies show no leakage at the surgical siteThe diet begins with liquids and progresses as tolerated
Surgery is indicated for epiphrenic and midesophageal diverticula only if the symptoms are troublesome and becoming worseTreatment consists of a diverticulectomy and long myotomy
Intramural diverticula usually regress after the esophageal stricture is dilated

Perforation
Perforation may result from stab or bullet wounds of the neck or chest, trauma from motor vehicle crash, caustic injury from a chemical burn, or inadvertent puncture by a surgical instrument during examination or dilation

Clinical Manifestations
The patient has persistent pain followed by dysphagia
Infection, fever, leukocytosis, and severe hypotension may be noted
In some instances, signs of pneumothorax are observed

Assessment and Diagnostic Findings
Diagnostic x-ray studies and fluoroscopy are used to identify the site of the injury

Management
Broad-spectrum antibiotic therapyA nasogastric tube is inserted to provide suction and to reduce the amount of gastric juice that can reflux into the esophagus and mediastinumNothing is given by mouthSurgery may be necessary to close the wound, and postoperative nutritional support then becomes a primary concernDepending on the incision site and the nature of surgery, the postoperative nursing management is similar to that for patients who have had thoracic or abdominal surgery

Gastroesophageal Reflux Disease (GERD)
Some degree of gastroesophageal reflux (back-flow of gastric or duodenal contents into the esophagus) is normal in both adults and children
Excessive reflux may occur because of an incompetent lower esophageal sphincter, pyloric stenosis, or a motility disorder
The incidence of reflux seems to increase with aging

Clinical Manifestations
pyrosis (burning sensation in the esophagus)dyspepsia (indigestion)regurgitationdysphagia or odynophagia (difficulty swallowing, pain on swallowing)hypersalivationesophagitisthe symptoms may mimic those of a heart attack

Assessment and Diagnostic Findings
endoscopy or barium swallow to evaluate damage to the esophageal mucosa
ambulatory 12- to 36-hour esophageal pH monitoring is used to evaluate the degree of acid reflux
bilirubin monitoring (Bilitec) is used to measure bile reflux patterns

Management
Teaching the patient to avoid situations that decrease lower esophageal sphincter pressure or cause esophageal irritation
The patient is instructed to eat a low-fat diet; to avoid caffeine, tobacco, beer, milk, foods containing peppermint or spearmint, and carbonated beverages; to avoid eating or drinking 2 hours before bedtime; to maintain normal body weight
To avoid tight-fitting clothes; to elevate the head of the bed on 6- to 8-inch (15- to 20-cm) blocks; and to elevate the upper body on pillows
Medications such as antacids or histamine receptor blockers, proton pump inhibitors, prokinetic agents, which accelerate gastric emptying
If medical management is unsuccessful, surgical intervention may be necessary

Barrett’s EsophagusIt is believed that long-standing untreated GERD may result in a condition known as Barrett’s esophagus. This has been identified as a precancerous condition that, if left untreated, can result in adenocarcinoma of the esophagus, which has a poor prognosis
It is more common among middle-aged white men; however, the incidence is increasing among women and among African Americans

Clinical Manifestations
The patient complains of symptoms of GERD, symptoms related to peptic ulcers or esophageal stricture, or both

Assessment and Diagnostic Findings
EGD is performed. This usually reveals an esophageal lining that is red rather than pink. Biopsies are taken, and the cells resemble those of the intestine

Management
Monitoring varies depending on the amount of cell changes. Some physicians may recommend a repeat EGD in 6 to 12 months if there are minor cell changes
Medical and surgical management is similar to that for GERD

Nursing ProcessAssessment
Emergency conditions of the esophagus (perforation, chemical burns) usually occur in the home or away from medical help and require emergency medical care
The patient is treated for shock and respiratory distress and transported as quickly as possible to a medical facility
Foreign bodies in the esophagus do not pose an immediate threat to life unless pressure is exerted on the trachea, resulting in dyspnea or interfering with respiration, or unless there is leakage of caustic alkali from a battery
Educating the public to prevent inadvertent swallowing of foreign bodies or corrosive agents is a major health issue

For nonemergency symptoms, a complete health history may reveal the nature of the esophageal disorder The nurse asks about the patient’s appetite. Has it remained the same, increased, or decreased?
Is there any discomfort with swallowing? If so, does it occur only with certain foods? Is it associated with pain? Does a change in position affect the discomfort?
The patient is asked to describe the pain. Does anything aggravate it? Are there any other symptoms that occur regularly, such as regurgitation, nocturnal regurgitation, eructation (belching), heartburn, substernal pressure, a sensation that food is sticking in the throat, a feeling of becoming full after eating a small amount of food, nausea, vomiting, or weight loss? Are the symptoms aggravated by emotional upset?

If the patient reports any of these symptoms, the nurse asks about the time of their occurrence, their relationship to eating,and factors that relieve or aggravate them (eg, position change, belching, antacids, vomiting)
This history also includes questions about past or present causative factors, such as infections and chemical, mechanical, or physical irritants; the degree to which alcohol and tobacco are used; and the amount of daily food intake
The nurse determines whether the patient appears emaciated and auscultates the patient’s chest to determine whether pulmonary complications exist

Nursing Diagnosis
Based on the assessment data, the nursing diagnoses may include the following:
• Imbalanced nutrition, less than body requirements, related to difficulty swallowing
• Risk for aspiration related to difficulty swallowing or to tube feeding
• Acute pain related to difficulty swallowing, ingestion of an abrasive agent, tumor, or frequent episodes of gastric reflux
• Deficient knowledge about the esophageal disorder, diagnostic studies, medical management, surgical intervention, and rehabilitation

Planning and Goals
The major goals for the patient may include attainment of adequate nutritional intake, avoidance of respiratory compromise from aspiration, relief of pain, and increased knowledge level

Nursing Interventions
Encouraging adequate nutritional intakeDecreasing risk of aspirationRelieving painProviding patient educationPromoting home and community-based care:
Teaching patients self-careContinuing care

Evaluation
Expected patient outcomes may include:1. Achieves an adequate nutritional intake
a. Eats small, frequent mealsb. Drinks water with small servings of foodc. Avoids irritants (alcohol, tobacco, very hot beverages)d. Maintains desired weight
2. Does not aspirate or develop pneumoniaa. Maintains upright position during feedingb. Uses oral suction equipment effectively

3. Is free of pain or able to control pain within a tolerable levela. Avoids large meals and irritating foodsb. Takes medications as prescribed and with adequate fluids(at least 4 ounces), and remains upright for at least10 minutes after taking medicationsc. Maintains an upright position after meals for 1 to 4 hoursd. Reports that there is less eructation and chest pain
4. Increases knowledge level of esophageal condition, treatment,and prognosisa. States cause of conditionb. Discusses rationale for medical or surgical managementand diet or medication regimenc. Describes treatment programd. Practices preventive measures so injuries are avoided