Embed Size (px)
Citation preview
1
Gastrointestinal
Alterations
Nancy Thompson, RN, MS, AOCNS
Swedish Cancer Institute
GI Alterations
Nausea & Vomiting
Mucositis
Taste Alterations
Anorexia / Cachexia
“The Chinese do not draw any distinction between
food and medicine.”
Lin Yutang
Case Study: Sarah Hogan
A 44 year old female, diagnosed
with extensive stage small cell
lung cancer.
She is told by her oncologist that
she will be receiving etoposide
100 mg/m2 and cisplatin 100
mg/m2.
She is worried about side effects
because she had a friend who
had a lot of nausea and vomiting.
2
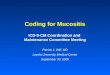
Therapy-Related Emesis Patterns
Anticipatory: Occurs before or during treatment from associated
stimuli; a conditioned response
> 25% incidence
Acute: Occurs within 24 hours
> Incidence determined by agents
Delayed: Occurs at least 24 hours after therapy and may persist up
to 6 days
> Cisplatin associated with highest incidence
CINV: Prevalent With Common Regimens Even Today Despite 5-HT3 Use
TAC=docetaxel + doxorubicin + cyclophosphamide;
FOLFOX 6=oxaliplatin + leucovorin + 5-fluorouracil.
Site of Cancer
Breast
Lung
Colorectal
Ovarian
Regimen Vomiting Nausea
TAC 44.5% 80.5%
Carboplatin +
paclitaxel 33.3% 44.3%
FOLFOX 6 42% 67%
Carboplatin +
docetaxel 37% 78%
Risk Factors for CINV: Chemotherapy-Specific Factors
Use of moderately or highly emetogenic regimens, such as:
> Cisplatin-based regimens
> Cyclophosphamide-based regimens (e.g. CHOP)
> AC (anthracycline + cyclophosphamide)
> Carboplatin-based regimens
> ABVD (doxorubicin + bleomycin + vinblastine + dacarbazine)
> FOLFOX/FOLFIRI (oxaliplatin + leucovorin + 5FU/irinotecan +
leucovorin + 5FU)
Short IV infusion time
Repeated cycles of chemotherapy
Hesketh PJ. Oncologist. 1999;4:191–196.
Navari RM. J Support Oncol. 2003;1:89–103. NCCN Guidelines. v.3.2008: antiemesis.
Risk Factors for CINV: Patient Characteristics
Female
Age < 50 years
History of low alcohol intake (<1.5 oz/day)
History of motion sickness
History of morning sickness during pregnancy
History of prior CINV
Extreme anxiety
Other factors
> pain, constipation, medications
Navari RM. J Support Oncol. 2003;1:89–103.
3
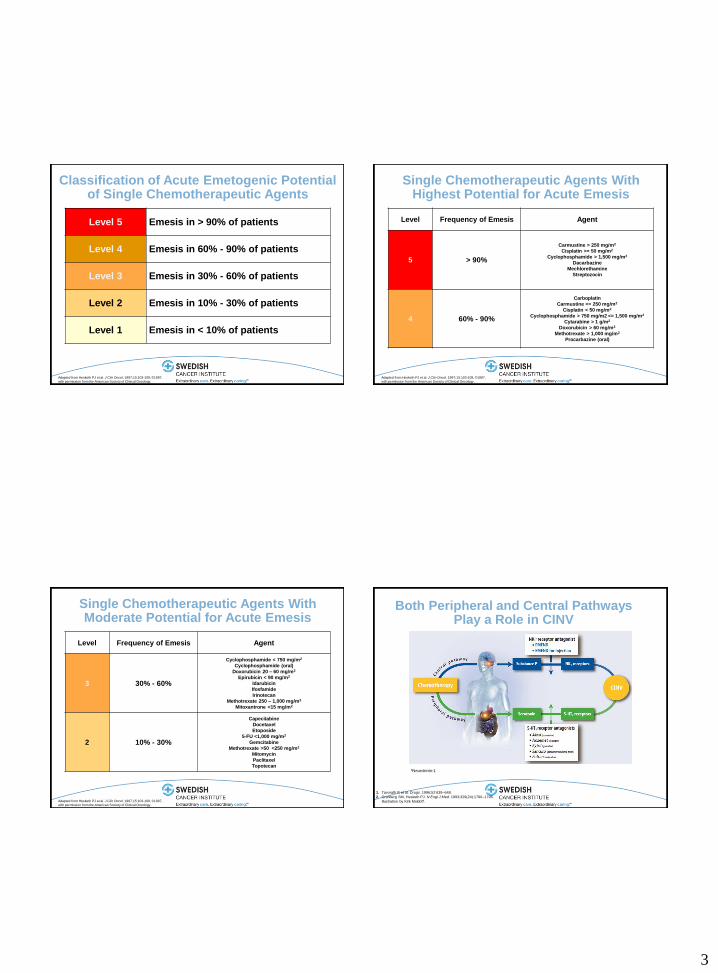
Classification of Acute Emetogenic Potential of Single Chemotherapeutic Agents
Level 5 Emesis in > 90% of patients
Level 4 Emesis in 60% - 90% of patients
Level 3 Emesis in 30% - 60% of patients
Level 2 Emesis in 10% - 30% of patients
Level 1 Emesis in < 10% of patients
Adapted from Hesketh PJ et al. J Clin Oncol. 1997;15:103-109, ©1997,
with permission from the American Society of Clinical Oncology.
Single Chemotherapeutic Agents With Highest Potential for Acute Emesis
Level Frequency of Emesis Agent
5 > 90%
Carmustine > 250 mg/m2
Cisplatin >= 50 mg/m2
Cyclophosphamide > 1,500 mg/m2
Dacarbazine
Mechlorethamine
Streptozocin
4 60% - 90%
Carboplatin
Carmustine <= 250 mg/m2
Cisplatin < 50 mg/m2
Cyclophosphamide > 750 mg/m2 <= 1,500 mg/m2
Cytarabine > 1 g/m2
Doxorubicin > 60 mg/m2
Methotrexate > 1,000 mg/m2
Procarbazine (oral)
Adapted from Hesketh PJ et al. J Clin Oncol. 1997;15:103-109, ©1997,
with permission from the American Society of Clinical Oncology.
Single Chemotherapeutic Agents With Moderate Potential for Acute Emesis
Level Frequency of Emesis Agent
3 30% - 60%
Cyclophosphamide < 750 mg/m2
Cyclophosphamide (oral)
Doxorubicin 20 – 60 mg/m2
Epirubicin < 90 mg/m2
Idarubicin
Ifosfamide
Irinotecan
Methotrexate 250 – 1,000 mg/m2
Mitoxantrone <15 mg/m2
2 10% - 30%
Capecitabine
Docetaxel
Etoposide
5-FU <1,000 mg/m2
Gemcitabine
Methotrexate >50 <250 mg/m2
Mitomycin
Paclitaxel
Topotecan
Adapted from Hesketh PJ et al. J Clin Oncol. 1997;15:103-109, ©1997,
with permission from the American Society of Clinical Oncology.
Both Peripheral and Central Pathways Play a Role in CINV
1. Tavorath R et al. Drugs. 1996;52:639–648.
2. Grunberg SM, Hesketh PJ. N Engl J Med. 1993;329(24):1790–1796.
Illustration by Kirk Moldoff.
bNeurokinin-1
4
Nausea & Vomiting Pharmacologic Management
Prevention, prevention, prevention!!
Select appropriate antiemetic based on treatment regimen
Consider cumulative effects
Administer through entire anticipated period of nausea & vomiting
Oral and IV antiemetics have equivalent effectiveness
Consider other potential causes of emesis
ONS: Putting Evidence into Practice
Serotonin Antagonists
Indications:
> High & moderate to high emetogenic chemotherapy
Common side effects:
> Headache, diarrhea, constipation, fever
Examples:
> ondansetron, granisetron, dolasteron
> Palonosetron (2nd generation)
NK-1 Antagonist
Indications:
> Acute and delayed nausea / vomiting
> Highly emetogenic chemotherapy
Common side effects:
> Diarrhea, hiccups, fatigue
Examples:
> Aprepitant (oral)
> Fosaprepitant (IV)
5
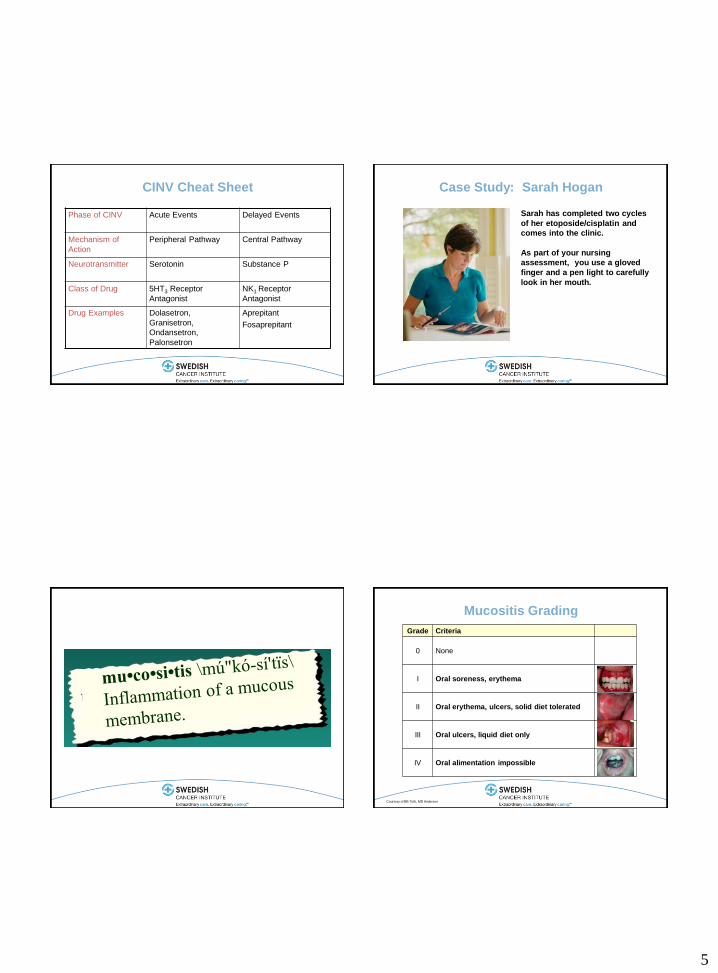
CINV Cheat Sheet
Phase of CINV
Acute Events Delayed Events
Mechanism of
Action
Peripheral Pathway Central Pathway
Neurotransmitter Serotonin Substance P
Class of Drug 5HT3 Receptor
Antagonist
NK1 Receptor
Antagonist
Drug Examples Dolasetron,
Granisetron,
Ondansetron,
Palonsetron
Aprepitant
Fosaprepitant
Case Study: Sarah Hogan
Sarah has completed two cycles
of her etoposide/cisplatin and
comes into the clinic.
As part of your nursing
assessment, you use a gloved
finger and a pen light to carefully
look in her mouth.
Mucositis Grading
Grade Criteria
0 None
I Oral soreness, erythema
II Oral erythema, ulcers, solid diet tolerated
III Oral ulcers, liquid diet only
IV Oral alimentation impossible
Courtesy of BB Toth, MD Anderson
6
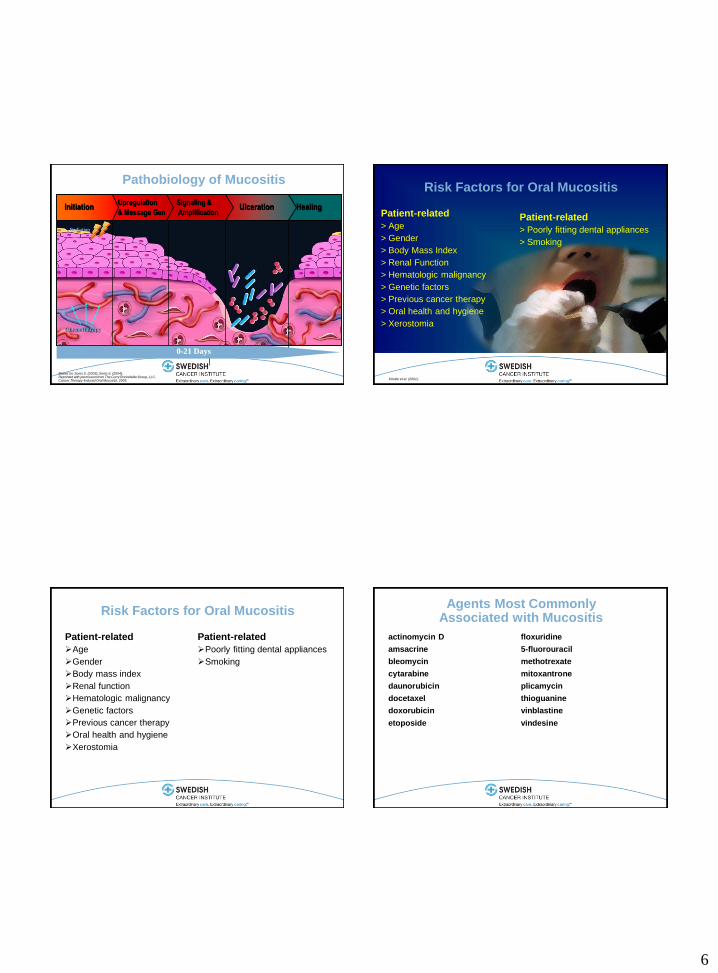
Radiation
Healing Ulceration Signaling &
Amplification
Upregulation
& Message Gen Initiation
Chemotherapy
0-21 Days
Based on: Sonis S. (2003); Sonis S. (2004); Reprinted with permission from The Curry Rockefeller Group, LLC, Cancer Therapy-Induced Oral Mucositis, 2005.
Pathobiology of Mucositis Risk Factors for Oral Mucositis
Patient-related
> Age
> Gender
> Body Mass Index
> Renal Function
> Hematologic malignancy
> Genetic factors
> Previous cancer therapy
> Oral health and hygiene
> Xerostomia
Patient-related
> Poorly fitting dental appliances
> Smoking
Köstler et al. (2001).
Risk Factors for Oral Mucositis
Patient-related
Age
Gender
Body mass index
Renal function
Hematologic malignancy
Genetic factors
Previous cancer therapy
Oral health and hygiene
Xerostomia
Patient-related
Poorly fitting dental appliances
Smoking
Agents Most Commonly Associated with Mucositis
actinomycin D
amsacrine
bleomycin
cytarabine
daunorubicin
docetaxel
doxorubicin
etoposide
floxuridine
5-fluorouracil
methotrexate
mitoxantrone
plicamycin
thioguanine
vinblastine
vindesine
7
Impact of Oral Mucositis
Clinical Consequences
> Dose reduction
> Dose/Treatment delay
> Morbidity – increase fever, increase infection
> Mortality – 4 fold increase in risk
Economic
> Increase resource utilization
> Increase cost -- $4,500 per day
Sonis et al. (2001); Ruescher, et al. (1998); Elting et al. (2003).
Mucositis: Assessment
Subjective:
> pain, burning, increased sensitivity, altered taste
Objective:
> erythema, ulceration, saliva, bleeding, cracked lips, hoarse
voice
Functional:
> Ability to chew, difficulty swallowing or speaking
“Systematic oral assessment at least daily or at each patient
visit”
ONS Putting Evidence Into Practice, 2009
Mucositis: Management
Prevention
> Collaborate with a
multidisciplinary team
> Oral care products
> Patient education (written, verbal,
demonstration)
> Treat dental problems before
cytotoxic therapy
> High protein diet
> Fluid intake > 1500 ml/day
> Cryotherapy for bolus 5-FU
Treatment
> Oral agents & hygiene
> Systemic pain medications
> Culture lesions
Mucositis: Oral Hygiene Program
Routine oral care protocol
> Daily oral self-exam, report signs of mucositis
> Oral hygiene after each meal and at bedtime, increase to q 2 hours as
needed
> Floss daily with dental tape
> Brush with soft toothbrush, 90 seconds bid
> Swish after each meal, at bedtime, at other times with water or mouth
rinse (Normal Saline, sodium bicarbonate)
Avoid oral irritants including tobacco and alcohol
Maintain adequate hydration
Use water based moisturizers to protect the lips
ONS Putting Evidence Into Practice, 2009
8
Magic Mouthwash
Dodd MJ, Dibble SL, Miaskowski C, et al.. (2000).
Randomized Double-blind, Placebo-controlled study
23 outpatient settings, 142 patients
No differences in effectiveness among 3 groups in outcome
(pain relief or time to resolution)
Salt and soda rinses were least costly
Pro-Self Mouth Aware Program
Magic Mouthwash
Chlorhexidine
Salt/Soda Rinses 2 tsp baking soda
1 tsp salt
1 liter of water
Rinse oral cavity every 2-4 hours or more often as needed.
Make a fresh solution every 24 hours.
Salt and Soda Rinse
Cryotherapy for Bolus Mucotoxic Chemotherapy with Short Half Life
Bolus 5-fluorouracil (5-FU) & Melphalan
Instruct patients to hold ice chips in their mouth starting 5 minutes
prior and for 30 minutes after.
The effectiveness of this intervention is based on vasoconstriciton
of the circulation in the oral cavity and the short half life of these
agents.
Evidence is lacking to support the benefit with other chemotherapy
agents.
Do not use in patients receiving oxaliplatin.
ONS Putting Evidence Into Practice, 2009
Case Study: Sarah Hogan
Sarah complains that food does
not taste the same and that
everything tastes like cardboard,
especially red meat.
She asks you if this is “normal”.

9
Taste Alterations: Defined
An actual or perceived change in taste sensation or loss of taste
> Hypogeusethesia:
• A decrease in the acuity of the taste sensation
> Dysgeusia:
• An unusual taste perception, perceived as unpleasant
> Ageusia:
• An absence of the taste sensation, “mouth blindness”
True or False? (Hint: Only one is true)
1. Taste changes associated with chemotherapy often resolve
once therapy is completed.
2. Approximately one in three cancer patients receiving
chemotherapy report taste changes.
3. The most commonly reported intervention to manage metallic
taste is to ingest sour candies.
4. Metallic taste changes are often reported with platinum-based
chemotherapy regimens.
Taste Alterations: Causes
Disease related
> Invasion of the tumor
> Oral infections
> Excretion of amino acid-like
substances from the tumor cells
Treatment related
> Specific surgical sites
> Radiation
> Chemotherapy:
• Lowered threshold for bitter taste
• Increased threshold for sweet, sour
and salty taste
• Aversion to meats
• Metallic taste
Taste Alterations: Consequences
Anorexia/poor appetite
Decreased oral intake
Reduced energy levels
Poor quality of life
Altered or perverted sense of taste for certain foods
* Can persist for hours, weeks or months after treatment
10
Taste Alterations: Management
Experiment with spices and flavorings
Use the aroma of foods to stimulate taste
Encourage oral hygiene before and after meals
Add increased sweeteners
Substitute other sources of protein (non-meat)
Marinate meats in sweet marinades
Avoid the sight and smell of foods causing unpleasantness
Avoid alcohol, commercial mouthwashes, smoking
Consume hard candies and / or chew gum to change taste before meals and
before chemotherapy treatment to reduce metallic taste
Use plastic eating utensils to manage the metallic taste
Refer to dietitians for nutritional counseling
Assess for weight loss
Case Study: Sarah Hogan
Before beginning her 4th cycle of
etoposide/cisplatin,
Sarah comes in to the clinic for
her assessment.
You notice that she has lost 15
pounds since her baseline
weight.
She tells you that she has no
appetite.
Common Nutritional Challenges
Anorexia
Malnutrition
Weight Loss
Muscle mass loss
Cachexia
At diagnosis: 50% of patients
present with nutritional issues
Malnutrition is the most common
secondary diagnosis to cancer
Anorexia: Defined
Involuntary loss of appetite accompanied by decreased food
intake
Often accompanied by weight loss
May be insidious and may only be obvious by weight loss
Can lead to cachexia
Often is not treated or diagnosed
11
Malnutrition: Defined
A state of nutrition in which a deficiency,
excess or imbalance of energy, protein, and
other nutrients causes measurable adverse
effects on body function and clinical outcome.
Anorexia and Malnutrition: Causes
Physiologic: Concurrent symptoms
> Nausea/vomiting
> Early satiety
> Pain
> Dysphagia
> Mucosisits
> Ascites
> Fatigue
Structural problems
> Abdominal tumors
> Surgical and dental changes
Medications
> Narcotics, iron, antibiotics
Psychological
> Anxiety, depression
> Loss of pleasure associated with food
Social factors
> Companionship
> Eating environment
> Issues associated with food preparation
Cachexia: Defined
A multifactorial syndrome characterized by an ongoing loss of skeletal muscle mass (with or without loss of fat mass) that
cannot be fully reversed by conventional nutritional support and leads to progressive functional impairment
1. Pre-cachexia - Weight loss of less than 5%. Anorexia and metabolic change
2. Cachexia - Weight loss of more than 5% or BMI less than 20 and weight loss greater than 2% or sarcopenia and weight loss more than 2%. Reduced food intake and systemic inflammation.
3. Refractory Cachexia – Variable degree of cachexia. Cancer disease both pro-catabolic and not responsive to anticancer treatment. Low performance status. Less than 3 months expected survival.
Fearon K., Lancet Oncol. 2011; 12(5) 489 – 495)
Patients with weight loss have worse outcomes
Chemotherapy dose reductions
Increase dose limiting toxicity
Decreased treatment response
Decreased quality of life and performance status
Shorter survival
Andreyev HJN, Eur J Cancer, 1998/34(4) 503-509
12
“Malnourished cancer patients do not live as long as their counterparts who
remain well nourished”
Dewys, WD et al. Am J Med, 1980, 69: 491-497
Malnutrition’s Effect on Oncology Patients
Just a small loss of weight may be a sign of a nutritional decline
that leads to:
> Treatment Delays
> Complications
> More frequent hospitalizations
> Reduced key outcomes such as quality of life
Dewys, WD et al. Am J Med, 1980, 69: 491-497
Early Assessment and Intervention is Critical
Dietary factors
> Diet history
> Ability to purchase & prepare food
> Food preferences / aversions
> Calorie count / food diary
> Educational needs
Physical Exam
> Weight loss
> Functional status
Laboratory Data
> Pre-albumin, albumin, transferrin
Laboratory Results
Serum albumin
> Measures visceral protein stores
> Less than 3.5 g/dl shows recent
protein depletion
Serum prealbumin
> Less than 15 mg/dl
> Indicates protein depletion
Serum transferrin
> Less than 200 mg/dl
> Reflects a decrease in the body’s
ability to make serum proteins
13
Anorexia / Cachexia: Management
Treat the tumor (keep patients on treatment!)
Early and regular assessment (weight % and time)
Early intervention prior to a crisis
Manage anorexia causes (N & V, Mucositis, pain)
Consider appetite stimulants
> Corticosteroids, progestins
Consider nutritional supplements with Revigor™
> Ensure clinical Strength or Juven®
Dietary Counseling
Non-pharmacological
> small, frequent meals, oral hygiene, exercise, high calorie, high protein
foods & supplements
Recommended Appetite Stimulants
Corticosteroids: Prednisolone, Dexamethasone
> Improve appetite, food intake, sense of well-being and performance
status
> Most effective type, dose or route not established
> Benefit is significant yet short in duration
> Long term use is associated with significant toxicities
Megestrol acetate (Megace) -160 - 1600 mg daily
> Most widely studied
> Dose related benefit on appetite, caloric intake and body weight and
sensation of well-being.
> Not to be used in patients at risk for thromboembolic disease, heart
disease or serious fluid retention
Individualized Dietary Counseling
Improved nutritional intake and body weight
Reduction in the incidence of anorexia
Improved quality of life
PUTTING EVIDENCE INTO PRACTICE, 2009
Non-pharmacological
Exercise/strength training -
improved lean muscle mass
Refer to cancer rehabilitation or PT
One of the most effective things we
can do!

14
Nutritional Alterations
Nausea & Vomiting
Mucositis
Taste Alterations
Anorexia / Cachexia