Embed Size (px)
Citation preview
Alterations in Respiratory Function
Ball and Bindler
Spring 2007
Donna Hills EdD APN
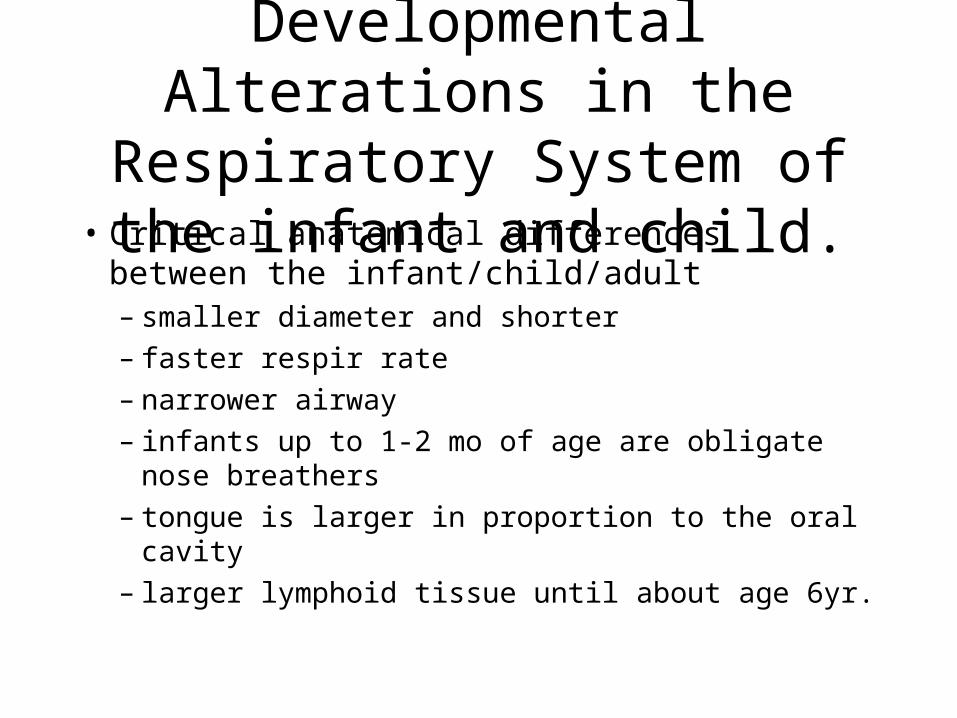
Developmental Alterations in the Respiratory System of the infant
and child.• Critical anatomical differences between the
infant/child/adult – smaller diameter and shorter– faster respir rate– narrower airway – infants up to 1-2 mo of age are obligate nose
breathers– tongue is larger in proportion to the oral cavity– larger lymphoid tissue until about age 6yr.
Critical anatomical differences between the infant/child/adult
• Lower airway– children up to 6yr are primarily diaphragmatic
breathers– intercostal muscles are immature and less
effective in aiding respir before age 6.– Chest wall is flexible due to ribs being
primarily cartilage; more prone to movement
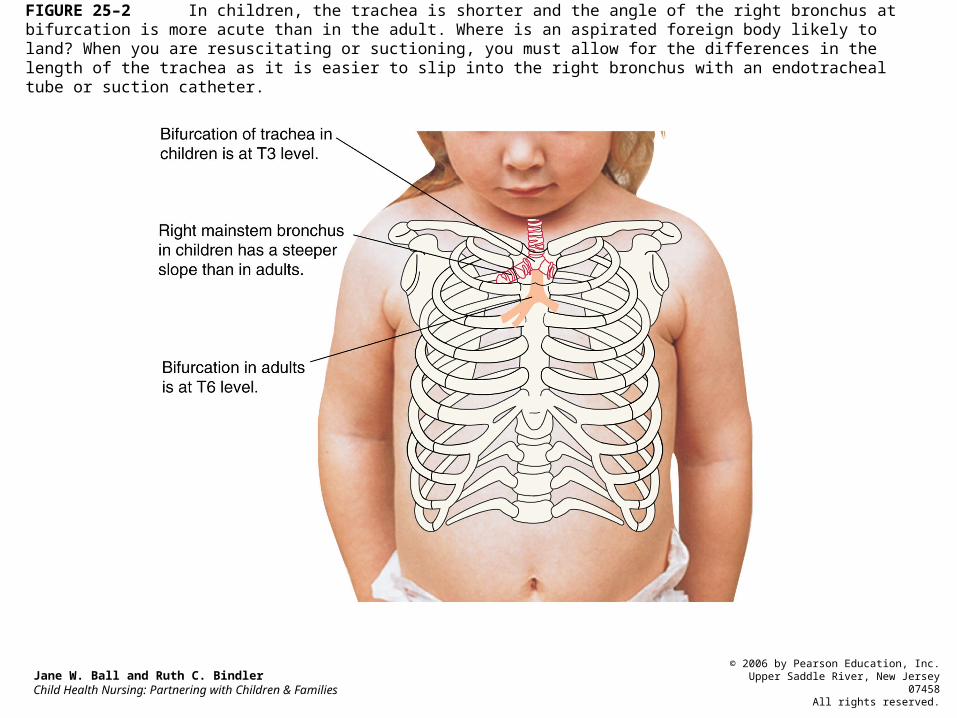
FIGURE 25–2 In children, the trachea is shorter and the angle of the right bronchus at bifurcation is more acute than in the adult. Where is an aspirated foreign body likely to land? When you are resuscitating or suctioning, you must allow for the differences in the length of the trachea as it is easier to slip into the right bronchus with an endotracheal tube or suction catheter.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
Assessment Guidelines for a Child in Respiratory Distress
• Ball & Bindler: Box 25-1, p. 825
• Quality of respirations
• Quality of pulses
• Color
• Cough
• Behavior changes
• Signs of dehydration
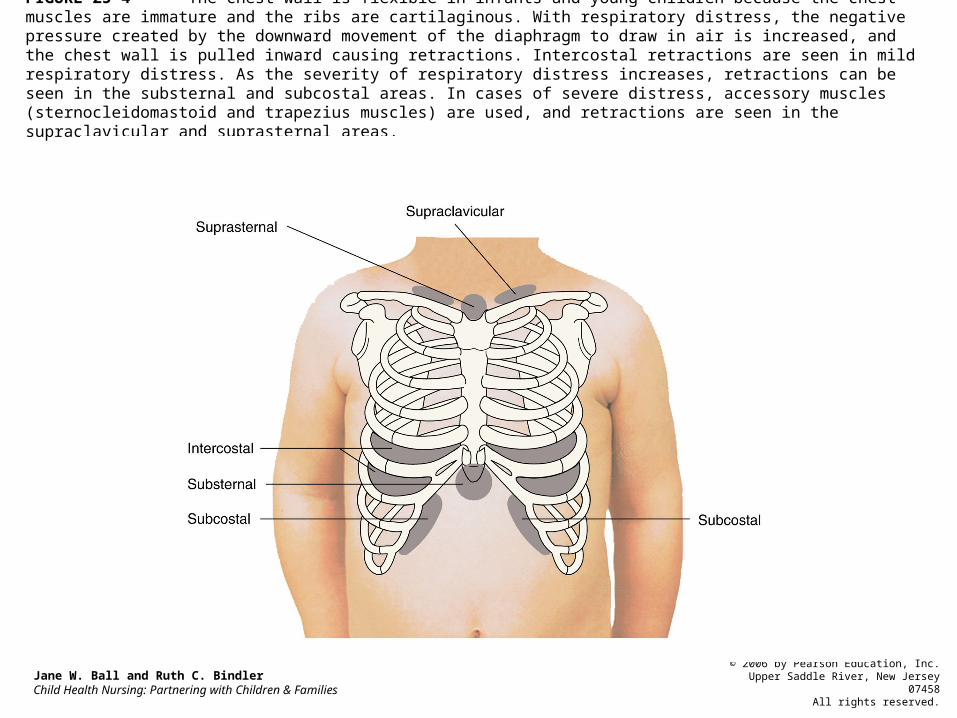
FIGURE 25–4 The chest wall is flexible in infants and young children because the chest muscles are immature and the ribs are cartilaginous. With respiratory distress, the negative pressure created by the downward movement of the diaphragm to draw in air is increased, and the chest wall is pulled inward causing retractions. Intercostal retractions are seen in mild respiratory distress. As the severity of respiratory distress increases, retractions can be seen in the substernal and subcostal areas. In cases of severe distress, accessory muscles (sternocleidomastoid and trapezius muscles) are used, and retractions are seen in the supraclavicular and suprasternal areas.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
Abnormal Alterations in the Respiratory System of the infant
and child.• Apnea: cessation of respir >20 sec.
– May or may not be accompanied by cyanosis, pallor, hypotonia, bradycardia.
– Apnea may be the first sign of distress in the infant; respir dysfunction,, sepsis, meningitis/encephalitis.
– Apnea of prematurity: occurs in preterm infants due to lack of maturity of the neuro/respiratory systems.
• episode of apnea accompanied by color change, hypotonia, choking, gagging, occuring in a near term infant (>37wks).
• May occur during sleep or wakefulness, or feeding.
• Child is usually admitted for monitoring
Apparent Life Threatening Event
• sudden death of an infant <1yr of age that remains unexplained after a complete autopsy, death scene investigation and review of the history.
• Leading cause of death in infants (1mo-1yr), with 90% occurring before 6mo..
• Rarely occurs in infants <2wks.
• Unpredictable and unpreventable.
• First sign is cardiopulmonary arrest.
Sudden Infant Death Syndrome: SIDS
• hypoxemia;low O2 level in the blood; assessed by O2 saturation or ABG/VBG.
• Hypercapnia: high CO2 level in the blood: ABG/VBG
• irritability, lethargy, cyanosis, dyspnea (flaring, grunting, retracting), tachypnea.
• Any of the above signs needs action and needs to be reported immediately to the Instr, RN or MD.
Signs of Respiratory Distress
• If O2 sats are less than 95%, confirm that the tracing is believable; (sine wave form and correlates with heart rate).
• At the same time, raise the HOB or sit child up if able.
• Determine O2 sat probe is functioning
• open airway
• administer O2 by blow-by first, then face mask, then bag/valve if sats <90.
Nursing Management of Respiratory Distress
• assess the child for changes in:– vital signs, esp. HR, RR and BP.– mentation/responsiveness– tone,– color
• alert the appropriate person to communicate changes in O2 sat and responses to treatment; obtain order for O2 or any other actions. Transfer child if required.
Nsg. Management Resp Dist. (cont)
• occur as a response to invasion by a virus, bacterium, allergen or irritant.
• Response includes inflammation, edema, increased mucous production and bronchospasms– AKA the 3 S’s: secretions,swelling, spasm.
• Can involve both the upper and lower airways• include croup, asthma and bronchiolitis
Reactive Airway Disorders
• classified as upper airway syndrome• can have swelling of :epiglottis, larynx, trachea,
and/or bronchi.• 3 viral syndromes:
– acute spasmodic laryngitis (spasmodic croup)– laryngotracheitis– laryngotracheobronchitis (LTB)
• 2 bacterial syndromes:– bacterial tracheitis and epiglottitis
Croup Syndromes
• Ball and Bindler, p. 838
• Acute spasmodic laryngitis
• Laryngotracheitis
• Laryngotracheo-bronchitis
• Bacterial tracheitis
• Epiglottitis
Summary of Croup Syndromes
• Acute spasmodic croup peaks at night, resolves by morning but reoccurs
• High fevers are associated with the bacterial syndromes: Bacterial Tracheitis and Epiglottitis, which are treated with antibiotics
• The child with LTB sounds worse than they look: the child with Epiglottitis is worse than they sound.
Classic parameters that distinguish each condition:
LTB: Laryngotracheobronchitis
• most common: 3mo-8yrs
• potential for airway obstruction esp in younger age group
• Influenza,Parainfluenza types I and II, RSV; esp seen in winter.
• barking cough, inspiratory stridor, retractions.
• inflammation and subsequent edema of the epiglottis causing airway obstruction within minutes to hours.
• Causes: HIB, staphylococcus and streptococcus• Recent decreased incidence with increased
immunization rates of HIB vaccine.• Avoid making the child cry to avoid desat and
increased laryngospasm.
Epiglottitis: Supraglottitis
• life threatening with rapid progression
• drooling, incr HR/RR, prefer sitting upright, with chin thrust
• avoid throat culture, tongue depressor or palpation of the tonsillar fossa, as this manipulation could produce severe laryngospasm
• if suspected, keep pt calm, transport in sitting position with O2: alert ENT.
Epiglottitis: Special Considerations
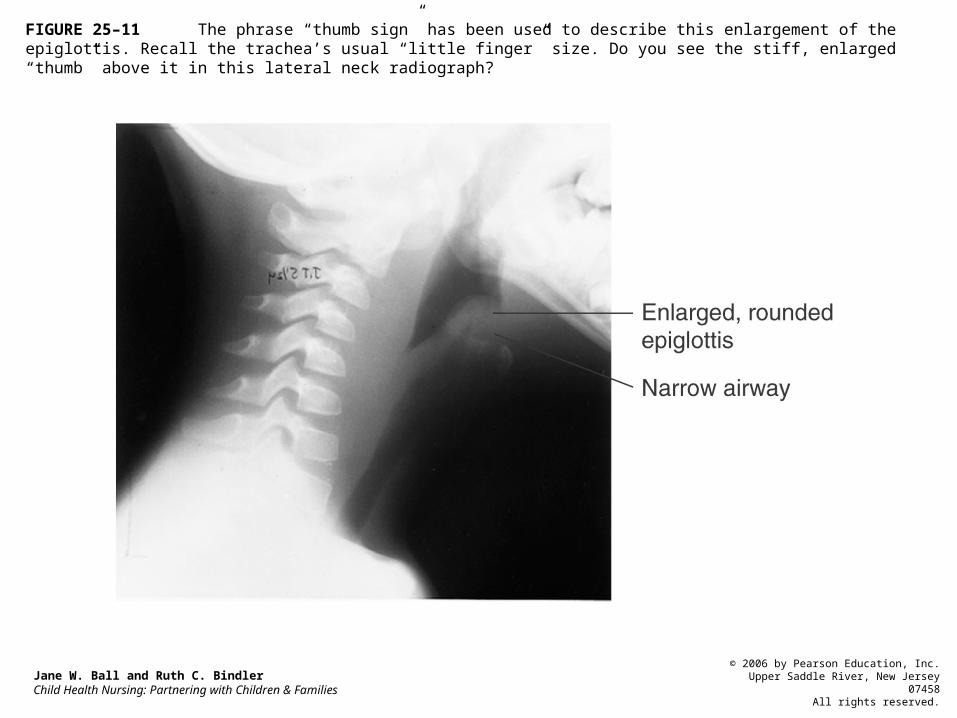
FIGURE 25–11 The phrase “thumb sign” has been used to describe this enlargement of the epiglottis. Recall the trachea’s usual “little finger” size. Do you see the stiff, enlarged “thumb” above it in this lateral neck radiograph?
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
Case Presentation
• Three yr old presents with a few days of URI symptoms with low grade fever (<102), now develops hoarseness and barking cough. Appetite less than usual but still drinking clear liquids and voiding 5x/day. Clear nasal discharge which he clears with his sleeve; wakes up at night coughing. Is cranky but consolable. Temp 100 ax, HR 130, RR 28, sat 95% RA in no distress. Color good. Chest coarse; no retr.
Assessment of Case Presentation
• What other questions would you like to ask the parent to determine data needed?
• Any further assessment or tests needed?
• What behaviors in the child might signal that the child was experiencing increased airway distress?
• What do you think the child has and why?
Management for Case Presentation
• Might give a trial neb of Albuterol 2.5mg in 2cc NS over 5-10min. Reassess response.
• Monitor for signs of stridor, F/G/R, activity, ability to take fluids, breath sound quality.
• If sats are > or = 95% on RA even with activity, there is no suspicion of epiglottitis or air way narrowing on lateral neck xray (steeple sign), and good aeration, would give parameters for home management.
• Assess parents ability to assess child, and obtain emergency help if needed
• If child awakes with barking cough and stridor, and/or has coughing with increased work of breathing, either bring into the bathroom with shower on and door closed (fan off) or bring outside in cool night air (wrap in a coat or blanket) for a few minutes. Distress usually subsides.
Parameters for Home Management
• If coughing subsides with this cool humidification treatment, offer clear liguids and settle back to sleep. Can give a home neb of Albuterol or even just mist. Episode my reoccur.
• If respiratory distress continues despite these efforts, bring to the nearest ER or call 911 if color poor, child is limp or lethargic, child drooling, quiet and wants to sit up.
Home Management continued
• chronic inflammatory disorder with acute exacerbations or persistent symptoms
• effects the large and small airways with increased mucous production, swelling and bronchospasm
• triggers: exercise, infection, allergies and environmental irritants (second-hand smoke abrupt change in weather).
Asthma
• Multiple allergic pathways may be stimulated: IgE, Leukotrienes, Compliment.
• Airway swelling and spasm results in airway narrowing, particularly significant in children with smaller airways.
• Air trapping occurs distal to mucus plugs
• Bronchospasm/coughing can feed into the cycle of anxiety which further increases the bronchospasm.
Pathophysiology
• Assess for degree of respiratory distress: RR, HR, color/O2sat, F/G/R, cap refill.
• Breath sounds, air movement, I/E ratio, peak flow (if able).
• Nebulizer with O2 via mask of Albuterol/Atrovent, (or Xopenex); use Epinephrine if respiratory distress is severe.
• Start steroids at 1-2mg/Kg/day divided BID.
Acute Care Management
Acute Care Management( cont):
• assess fluid status; increased RR leads to increased insensible loss of water, dries out mucous airways and risk of aspiration.
• Monitor output: number of wet diapers/day, number of voids or actual measurement
• provide emotional support for child and parents.
• promote rest to conserve energy, decrease O2 need and decrease bronchospasm
FIGURE 25–17 Acute exacerbations of asthma may require management in the emergency department. The child is placed in a semisitting position to facilitate respiratory effort. Providing support to both the child and parent is an important part of nursing care during these acute episodes. The mother is exhausted after a sleepless night of caring for her son.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
FIGURE 25–18 Medications given by aerosol therapy allow children to get optimal therapy without injections and their associated pain and stress.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
• Primary goal is prevention
• use peak flow meter to monitor degree of obstruction; divided into zones
• avoid triggers: – refer to allergist to determine if candidate for
desensitization (shots)– maintenance meds to avoid histamine and/or
leukotriene stimulation
• rescue agent for acute symptoms: Albuterol
Management at Home
• Determine need for a home nebulizer vs spacer used with an MDI (metered dose inhaler).
• Keep a home log of need for treatment and adjustments in the environment, activity, diet, etc.
• Determine need for steroids for maintenance and prevention
• Determine a clear follow-up plan.
Home management cont.
Revised Asthma Severity Classification
• 2002 National Asthma Education and Prevention Program Classification System of Asthma Severity
• brief exacerbations < 2x/wk
• night time symptoms < 2x/month
• PEFR > or = 80%
• quick relief with bronchodilators PRN, but if needed > 2x/wk then moves to the next level.
Mild Intermittent
• exacerbations > 2x/wk but < 1x/day.
• Night time sx > 2x/month
• May affect activity
• PEFR > or = 80%
• daily anti-inflammatory med.
• Quick relief bronchodilator PRN
Mild Persistent
• daily symptoms• daily short-acting beta-agonist• exacerbations >2x/wk; lasts for days• night time sx > 1x/wk• affects activity• PEFR >60% but <80%• daily anti-inflammatory meds; medium dose• bronchodilator up to 3x/day
Moderate Persistent
• continuous symptoms
• limited physical activity
• frequent exacerbations
• frequent night time sx
• PEFR ,60% but >30%
• daily anti-inflammatory; high dose
• bronchodilator up to 3x/day
Severe Persistent
Status Asthmaticus
• severe, unrelenting respiratory distress with bronchospasm
• persists despite medication and supportive interventions
• medical emergency requiring endotracheal intubation with assisted ventilation
• Bronchopulmonary Dysplasia
• Bronchiolitis
• Pneumonia
• Cystic Fibrosis
• Foreign body aspiration
Lower Airway Disorders
• acute lung injury with abnormal xray findings and persistent oxygen need beyond 36wks gestational age.
• Seen more often in preterms and those treated with long term ventilatory support
• results in fibrosis and edema of the bronchioles with smooth muscle hypertrophy
Bronchopulmonary Dysplasia: Patho
• sx resp distress: tachypnea, wheezing, crackles/rales, irritability, F/G/R, pulmonary edema, FTT, barrel chest.
• Cyanosis if severe or accompanied by cardiac anomalies
• Normal activities such as feeding, playing or a mild URI, increases oxygen demands and therefore can precipitate respiratory distress
BPD: clinical manifestations
• symptomatic treatment and support• humidified 02 to keep sats 90-92% even during
feeding and sleeping• CPT 3-4x/day or as needed, preceeded by
bronchodilator nebs (Albuterol,Xopenex), diuretics (Lasix, Aldactone), Anti-inflammatories(steroids:Dexamethasone,Methylprednisolone, Prednisone/Prednisolone), inhaled steroids (Pulmocort, Flovent).
BPD: medical management
FIGURE 25–14 Many children with BPD are cared for at home, with the support of a home care program to monitor the family’s ability to provide airway management, oxygen, and support. This premature infant girl, who is now 4 months old but weighs only about 5 pounds, requires respiratory support with oxygen.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
• promote respiratory function, nl G+D. • preparing the family for home care needs• close monitoring of RR, HR, color, behavior
changes, and how the family unit is coping with caring for this child with special needs.
• Clear parameters for follow up in an acute exacerbation:readmission to the hosp is common and become ill very quickly.
BPD: nursing management
• inflammation of the trachea and bronchi
• usually follows a URI esp in children <4yr.
• Usually viral but can be bacterial: xray may be indicated
• treatment usually supportive with close monitoring for worsening of symptoms.
• Coarse breath sounds, wheezing, hacking cough, worse at night, fatigue, decreased appetite and interest in play.
Bronchitis
• variation of severity of respir distress• <2mo hospitalized; ,6mo more severe disease
than older infant• inflammation and destruction of smaller airways• caused by viruses: Influenza type A & B,
Parainfluenza, RSV.• Can also be caused by bacteria or mycoplasma
(but less likely).
Bronchiolitis
• transmitted through close or direct contact
• viruses act like parasites and invade the mucosal cells
• cells die, bursts and the resultant debris clogs and obstructs the bronchioles
• in response, airways swell, produce excess secretions causing obstruction and bronchospasm.
• Apnea and pulmonary edema may occur
Respiratory Syncytial Virus: RSV
• URI, fever, clear rhinitis progressing to wheezing/coarse breath sounds, increased work of breathing, F/G/R.
• Appear progressively more ill as sx of resp distress develop
• less po intake, less energy/activity, incr sleepiness or irritability.
RSV: clinical manifestations
• chest xrays are not specific unless the child has a pneumonia as well
• viral cultures are done on the nasal secretions and child is put on contact precautions until cultures come back neg (if positive, precautions continue)
• respirations are supported with humidified 02 to keep sats by oxymetry >93%
• CPT, sx VS, contact prec, hand washing.
RSV: clinical therapy
• Ribavirin:only antiviral drug available .Questionable effectiveness; reserved for severe, life-threatening cases.
• Evidence that RSV in early childhood increases the risk of asthma in later childhood and COPD later in life.
• Recomm premies and children with underlying medical conditions during their first RSV season (Oct-Mar) with Synagis.
RSV: medical management

• passive immunity with monoclonal antibody specific to RSV
• IM inj given 1x/mo Oct-April to those born <37 wks, and/or have cong heart disease, asthma, BPD, or immunosuppression (and other chronic diseases).
• Day care, shelters, high density group living and older siblings also increase the risk of the child contracting RSV.
Synagis for children at risk
• inflammation or infection of the bronchioles and alveolar spaces of the lungs
• viral, bacterial or mycoplasma in origin(latter two are treated with A/B)
• end result from all causes is exudate that fills alveolar spaces, creating areas of plugging and consolidation that can interfere with gas exchange.
Pneumonia
• similar to bronchiolitis• in addition, use of Tylenol or Ibuprofen for fever
and pain control• frequent persistent coughing can cause muscle
strain and interrupted sleep for both child and parent.
• Cough suppressants are not routinely advised for young children
• supportive therapy: fluids/nutr/02 if indic.
Pneumonia:clinical manifestations and nursing
management
• common inherited autosomal recessive disorder
• involves the exocrine glands which excrete a thick fluid that affects functioning of the respiratory, GI, endocrine, skin and reproductive systems.
• Predominantly seen in the white population
• equal distribution among gender
• median life span is 30yrs.
Cystic Fibrosis
FIGURE 25–20 Cystic fibrosis is an inherited autosomal recessive disorder of the exocrine glands, so it is not uncommon to see siblings with it such as this brother and sister.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
• 600 mutations with variation of severity
• all types affect multiorgan systems:
• lungs become plugged with thick mucous that can not be expectorated, causing atelectasis and air trapping. Secondary infections are common and are combatted by scheduled hosp. admissions for “clean outs”
CF: clinical manifestations
• pancreatic ducts become blocked: enzymes can’t adequately digest food– poor absorption of nutrients; weight loss, FTT, resulting in
foul smelling, frothy, floating and fat containing stools.– Insulin dependent diabetes is not uncommon as the child ages
(adolescence).
• Sterility or decreased fertility is common due to increased mucous secretions
• metabolic imbalance d/t excess electr loss• .
CF: clinical manifestations
• meconium ileus in the new born
• small bowel obstruction as a young infant
• fecal impaction and/or intussusception
• steatorrhea (fatty stools)
• productive cough, frequent URI’s, weight loss
• elevated Chloride on a Sweat Test (>50-60)
CF: Primary presentation and diagnosis
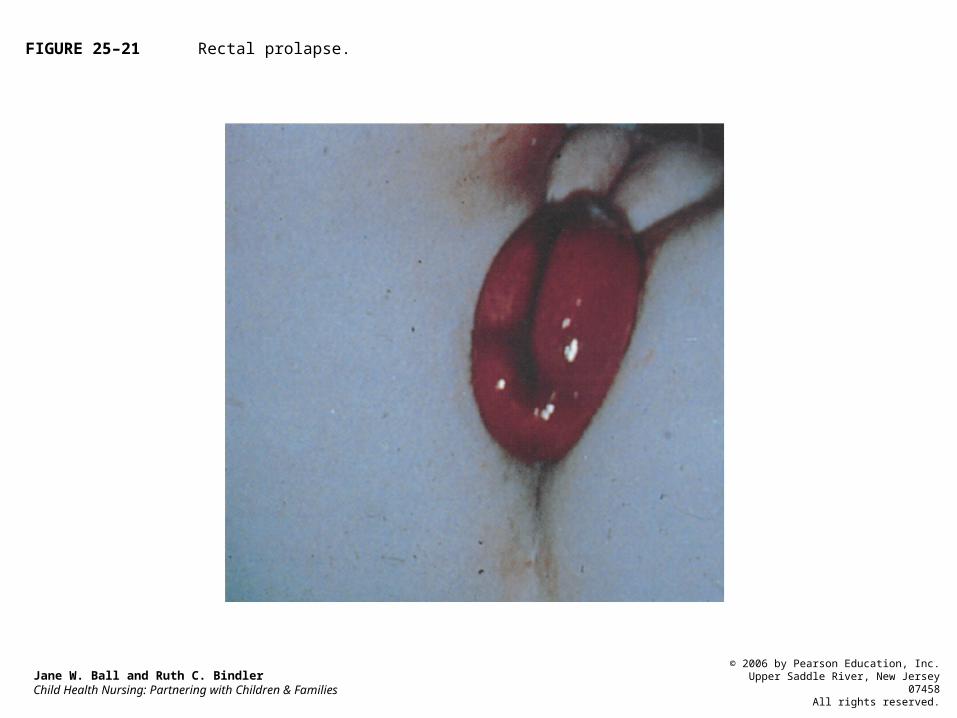
FIGURE 25–21 Rectal prolapse.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
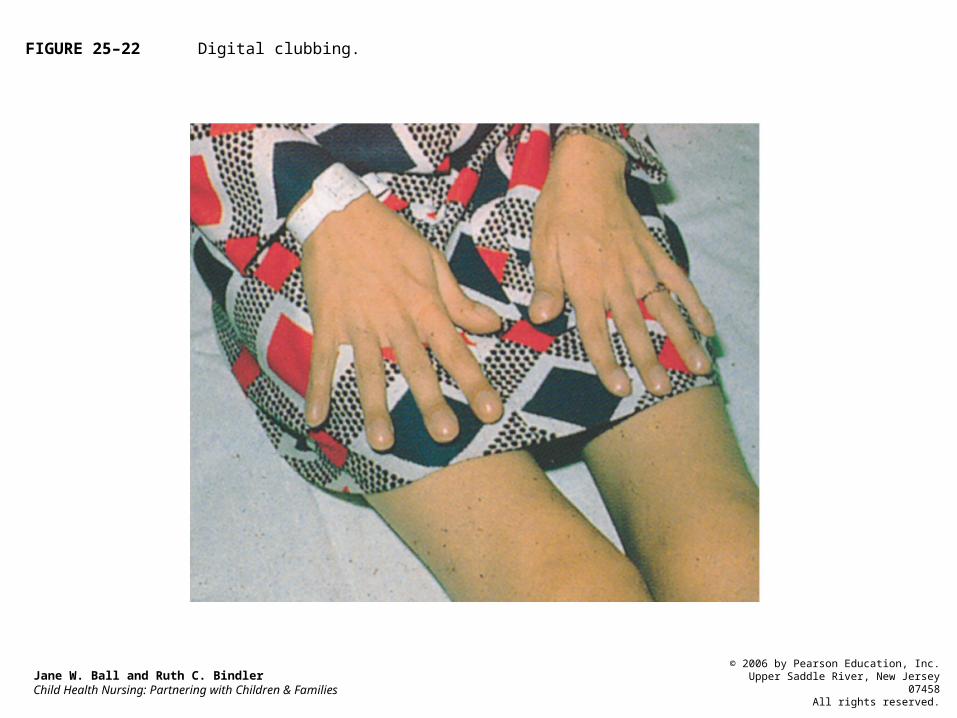
FIGURE 25–22 Digital clubbing.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
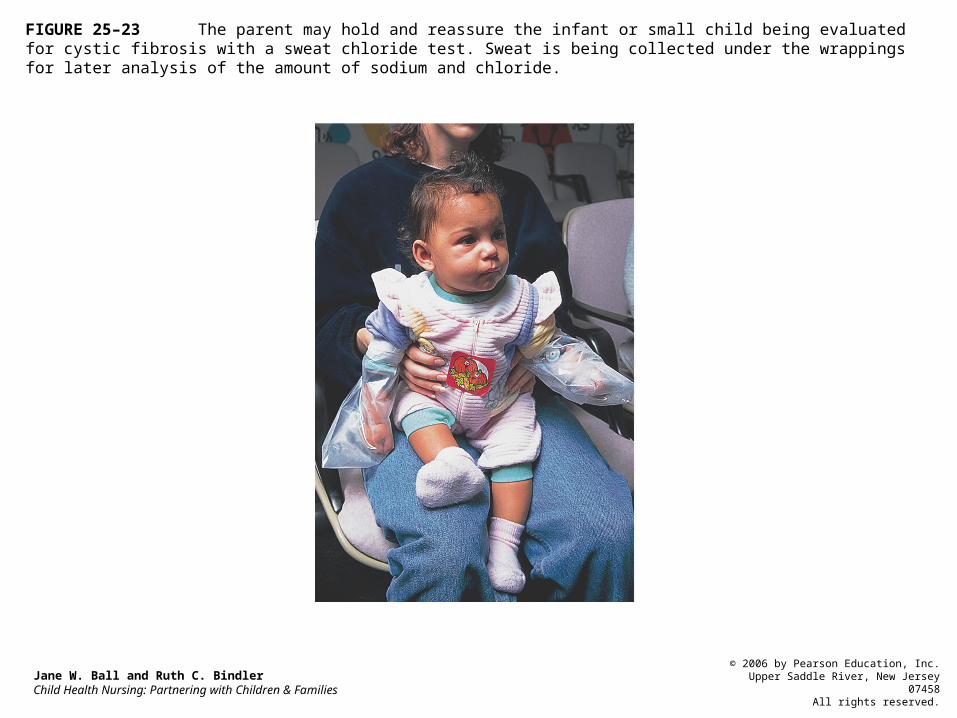
FIGURE 25–23 The parent may hold and reassure the infant or small child being evaluated for cystic fibrosis with a sweat chloride test. Sweat is being collected under the wrappings for later analysis of the amount of sodium and chloride.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
• maintaining respiratory function: nebs/CPT TID/PD/vibration/expectoration
• supportive 02 as needed• managing infection:maintenance A/B, then clean
outs and high dose antibiotics when hospitalized. • Avoid colonization and cross contamination with
other Cystic Fibrosis kids.• Optimal GI absorp and avoid obstruction
CF: Clinical Therapy
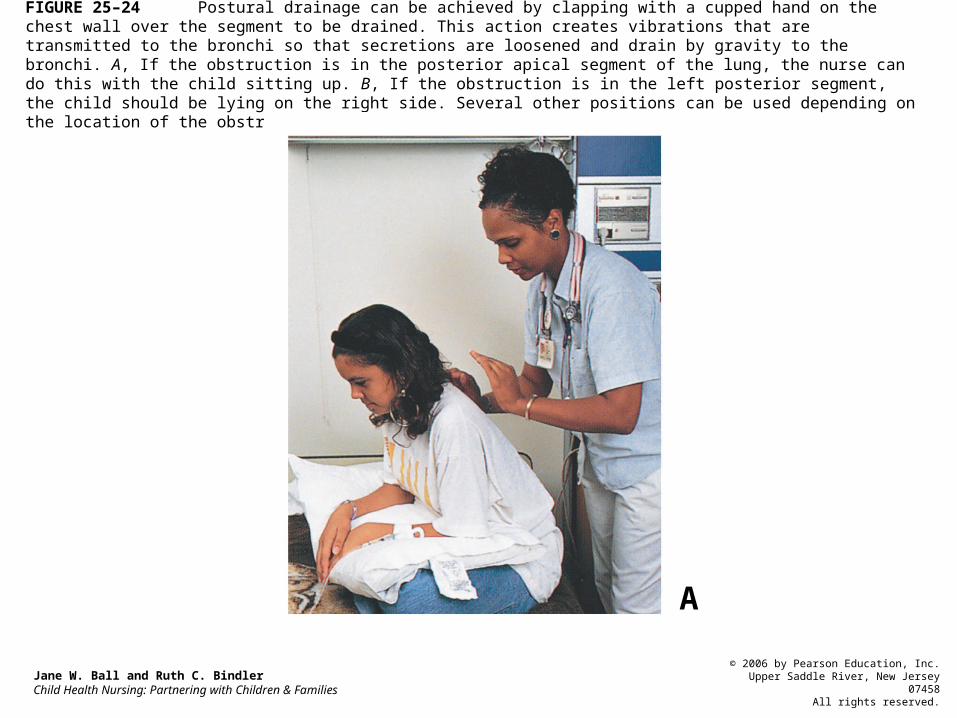
FIGURE 25–24 Postural drainage can be achieved by clapping with a cupped hand on the chest wall over the segment to be drained. This action creates vibrations that are transmitted to the bronchi so that secretions are loosened and drain by gravity to the bronchi. A, If the obstruction is in the posterior apical segment of the lung, the nurse can do this with the child sitting up. B, If the obstruction is in the left posterior segment, the child should be lying on the right side. Several other positions can be used depending on the location of the obstruction. See the Skills Manual.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
A
Foreign Body Aspiration
• at risk: infants>6mo, toddlers, preschoolers during exploration and experimentation
• schoolage and teens d/t activity while eating, too much in the mouth or eating too fast.
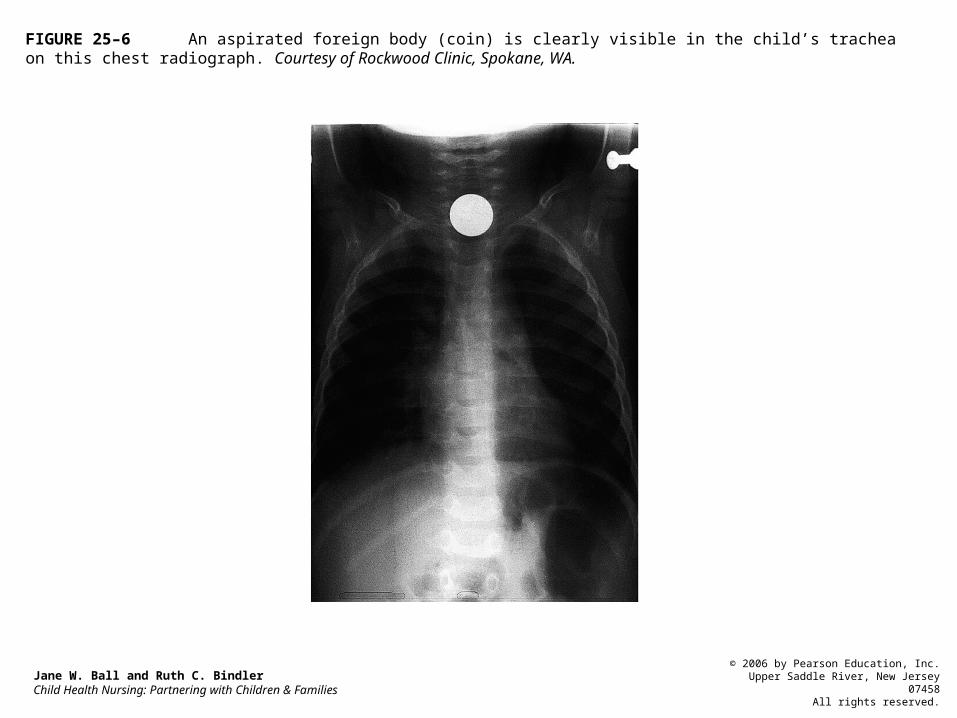
FIGURE 25–6 An aspirated foreign body (coin) is clearly visible in the child’s trachea on this chest radiograph. Courtesy of Rockwood Clinic, Spokane, WA.
Jane W. Ball and Ruth C. BindlerChild Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.Upper Saddle River, New Jersey 07458
All rights reserved.
• coughing, choking, gagging, dyphonia and wheezing; decreased breath sounds on one side, stridor and possible respiratory distress.
• FB in bronchus is better tolerated; in trachea is life threatening
• can migrate to R main stem bronchus to R lung d/t anatomical slope.
FBA: clinical manifestations
• in air way obstruction: chest thrusts and back blows in the infant.
• Abdominal thrusts in the child over 8 yrs.• if partially obstructed: xray indic of chest (A/P
& lateral) and lateral film of the neck.• Bronchoscopy under sedation may be necessary
to remove object or sometimes, surgery.• Best therapy is prevention.
FBA: clinical management