Embed Size (px)
Citation preview

Chapter 5Chapter 5
Care of the Patient with aGastrointestinal Disorder
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Digestive System
2Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Slide 3Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Digestive system (Alimentary canal) Organs and their functions
• Mouth: Beginning of digestion
• Teeth: Bite, crush, and grind food
• Salivary glands: Secrete saliva
• Esophagus: Moves food from mouth to stomach
• Stomach: Churn and mix contents with gastric juices
• Small intestine: Most digestion occurs here
• Large intestine: Forms and expels feces
• Rectum: Expels feces
Peristalsis: coordinated, rhythmic, serial contraction of smooth muscle that forces food through digestive tract, bile through bile duct and urine through ureter

Slide 4Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Accessory organs of digestion Organs and their functions
• Liver: Produces bile; Manages blood coagulation Detoxifies poisons; activates Vitamin D Stores glycogen; breaks down nitrogenous waste to urea
• Pancreas: Produces pancreatic juice
• Regulation of food intake Hypothalamus
• One center stimulates eating and another signals to stop eating

Digestion in the Small Intestine
5Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Slide 6Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Laboratory and Diagnostic ExaminationsLaboratory and Diagnostic Examinations
• Upper GI series: NPO & expulsion of barium
• Gastric analysis: determine presence of acid
• Esophagogastroduodenoscopy (EGD): NPO, IV Capsule endoscopy
• Barium swallow: more thorough esophageal exam; barium or gastrografin
• Bernstein test: acid-perfusion test (reproduce acid reflux)
• Stool for occult blood: Guaiacoccult, Hemoccult, Hematest
• Sigmoidoscopy: lower GI tract
• Barium enema: radiographic images of colon
• Colonoscopy: clear liquid diet; cleansing of colon
• Stool culture and sensitivity; stool for ova and parasites
• Flat plate of the abdomen: detect air-fluid levels within intestine

Slide 7Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the MouthDisorders of the Mouth
• Dental plaque and caries Etiology/pathophysiology
• Erosive process that results from the action of bacteria on carbohydrates in the mouth, which produces acids that dissolve tooth enamel
Medical management/nursing interventions• Remove affected area of tooth and replace with dental
material
• Periodontal – remove plaque
• Encourage brush teeth min. 2x/ day
• Frequent oral care for NPO patients

Slide 8Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the MouthDisorders of the Mouth
• Candidiasis Etiology/pathophysiology
• Infection caused by a species of Candida, usually Candida albicans
• Fungus normally present in the mouth, intestine, and vagina, and on the skin
• Also referred to as thrush and moniliasis Clinical manifestations/assessment
• Small white patches on the mucous membrane of the mouth
• Thick white discharge from the vagina

Slide 9Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the MouthDisorders of the Mouth
• Candidiasis (continued) At risk: immune suppressed, DM2, alcoholism, people
on antibiotics, inhaled steroid treatments Medical management/nursing interventions
• Pharmacological management Nystatin Ketoconazole oral tablets Diflucan (fluconazole)
• Half-strength hydrogen peroxide/saline mouthwash
• Meticulous hand washing
• Comfort measures – soft brush, cool/warm foods

Slide 10Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the MouthDisorders of the Mouth
• Carcinoma of the oral cavity Etiology/pathophysiology
• Malignant lesions on the lips, oral cavity, tongue, or pharynx
• Usually squamous cell epitheliomas Clinical manifestations/assessment
• Leukoplakia (biopsy if present >2 wks)
• Roughened area on the tongue
• Difficulty chewing, swallowing, or speaking
• Edema, numbness, or loss of feeling in the mouth
• Earache, face ache, and toothache
• Lip with non-healing lesion

Slide 11Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the MouthDisorders of the Mouth
• Carcinoma of the oral cavity (continued) Diagnostic tests
• Indirect laryngoscopy• X-ray of mandible• Excisional biopsy is most accurate
Medical management/nursing interventions• Stage I: Surgery or radiation• Stage II & III: Both surgery and radiation• Stage IV: PalliativeSurgical complications possible: nerve damage, airway
obstruction, hemorrhage, aspiration, edema, dysphagiaPEG tube insertion may be requiredPrognosis: dependent on staging

Slide 12Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the EsophagusDisorders of the Esophagus
• Gastroesophageal reflux disease What medication would Arisha B. Perez be taking? Etiology/pathophysiology
• Backward flow of stomach acid into the esophagus due a weak sphincter
• If left untreated, can turn to Barrett’s esophagus Clinical manifestations/assessment
• Heartburn (pyrosis) 20 min to 2 hours after eating
• Regurgitation – warm fluid in throat
• Dysphagia or odynophagia (painful swallow)
• Eructation and flatulence
• Nocturnal cough, wheeze and hoarseness

Slide 13Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the EsophagusDisorders of the Esophagus
• Gastroesophageal reflux disease (continued) Diagnostic tests
• Esophageal motility and Bernstein tests• Barium swallow• Endoscopy
Medical management/nursing interventions• Pharmacological management
Antacids or acid-blocking medications• Dietary recommendations; small, frequent meals, reduce
caffeine/alcohol, avoid eating 2-3 hours before bedtime
• Lifestyle recommendations; smoking cessation, avoid heavy lifting,
straining, sleep with head of bed elevated • Comfort measures• SurgeryPrognosis: poor if left untreated

Slide 14Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Acid reducersAcid reducers
• H2 receptor antagonists (the -tidine family) Tagamet (cimetidine) Zantac (ranitidine) Pepcid (famotidine) Axid (nizatidine)
• Proton Pump Inhibitors (the –prazole family) Prilosec (omepraxole) Nexium (esomeprazole) * Protonix (pantoprazole) Prevacid (lansoprazole)

Antacids, H2-Receptor Antagonists, Proton Pump Inhibitors – Edmunds 303-304
Adverse Reactions Antacids: weakness, anorexia, diarrhea,
frequent burping, bowel obstruction, constipation, hypermagnesemia; Bind with many medications
H2-receptor antagonists: dizziness, headache, somnolence, mild/brief diarrhea, hematologic changes, muscle pain
Proton pump inhibitors: headache, diarrhea, abdominal pain, and nausea; rarely rash, vomiting, and dizziness
15Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Slide 16Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the EsophagusDisorders of the Esophagus
• Carcinoma of the esophagus Etiology/pathophysiology
• Malignant epithelial neoplasm that has invaded the esophagus
90% are squamous cell carcinoma associated with alcohol intake and tobacco use
6% are adenocarcinomas associated with reflux esophagitis
Typically discovered at late stage making prognosis poor and palliative treatment common
Clinical manifestations/assessment• Progressive dysphagia over a 6-month period
• Sensation of food sticking in throat

Slide 17Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the EsophagusDisorders of the Esophagus
• Carcinoma of the esophagus (continued) Medical management/nursing interventions
• Radiation: May be curative or palliative
• Surgery: May be palliative, increase longevity, or curative
Types of surgical procedureso Esophagogastrectomyo Esophagogastrostomyo Esophagoenterostomy o Gastrostomy

Slide 18Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the EsophagusDisorders of the Esophagus
• Achalasia Etiology/pathophysiology
• Cardiac sphincter of the stomach cannot relax
• Possible causes: Nerve degeneration, esophageal dilation, and hypertrophy
Clinical manifestations/assessment• Dysphagia
• Regurgitation of food
• Substernal chest pain
• Loss of weight; weakness
• Poor skin turgor

Slide 19Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the EsophagusDisorders of the Esophagus
• Achalasia (continued) Diagnostic tests
• Radiologic studies; esophagoscopy Medical management/nursing interventions
• Pharmacological management Anticholinergics, nitrates, and calcium channel blockers
o Reduce pressure of the tight sphincter
• Dilation of cardiac sphincter (like in angioplasty)
• Surgery Cardiomyectomy – cut the muscle of the sphincter a little
on the outside to allow stretch of mucosa

Slide 20Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Acute gastritis Etiology/pathophysiology
• Inflammation of the lining of the stomach
• May be associated with alcoholism, smoking, and stressful physical problems
• Interferes with acid & pepsin secretion Clinical manifestations/assessment
• Fever; headache
• Epigastric pain; nausea and vomiting
• Coating of the tongue
• Loss of appetite

Slide 21Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Acute gastritis (continued) Diagnostic tests
• Stool for occult blood; WBC; electrolytes; Hct Medical management/nursing interventions
• Pharmacological management Antiemetics Antacids Antibiotics IV fluids
• NG tube and administration of blood, if bleeding
• NPO until signs and symptoms subside
• Monitor intake and output

Slide 22Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
AntiemeticsAntiemetics
• Compazine (prochlorperazine)
• Phenergan (promethazine)
• Tigan (trimethobenzamide)
• Zofran (ondansetron)
• Dramamine (dimenhydrinate)
• Causes drowsiness; Avoid CNS depressant drugs while on anti-emetics. Do not operate machinery until you know how the medication will affect you.

Slide 23Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Peptic UlcersPeptic Ulcers
• Gastric ulcers and duodenal ulcers Ulcerations of the mucous membrane or deeper
structures of the GI tract Most commonly occur in the stomach and duodenum Result of acid and pepsin imbalances H. pylori
• Bacterium found in 70% of patients with gastric ulcers and 95% of patients with duodenal ulcers

Digestion in the Stomach
24Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Slide 25Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Gastric ulcers (continued) Etiology/pathophysiology
• Gastric mucosa are damaged, acid is secreted, mucosal erosion occurs, and an ulcer develops
• Stress Ulcers Stress causes ulcers to form: prophylactic use of acid
reducers before surgery to prevent erosion
• Duodenal ulcers (continued) Etiology/pathophysiology
• Excessive production or release of gastrin, increased sensitivity to gastrin, or decreased ability to buffer the acid secretions

Slide 26Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Gastric and duodenal ulcers (continued) Clinical manifestations/assessment
• Pain: Dull, burning, boring, or gnawing, epigastric
• Dyspepsia
• Hematemesis
• Melena Diagnostic tests
• Esophagogastroduodenoscopy (EGD)
• Breath test for H. pylori

Slide 27Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Gastric and duodenal ulcers (continued) Medical management/nursing interventions
• Pharmacological management Antacids to neutralize pH Histamine H2 receptor blockers Proton pump inhibitor Mucosal healing agents, like Carafate Antibiotics for H. pylori
• Dietary recommendations small frequent meals; limit coffee, spicy foods, tobacco,
alcohol, and aspirin use

Slide 28Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Gastric and duodenal ulcers (continued) Medical management/nursing interventions
• Surgery Antrectomy Gastroduodenostomy (Billroth I) Gastrojejunostomy (Billroth II) Total gastrectomy Vagotomy Pyloroplasty
May require NG tube placement

Slide 29Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
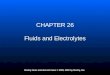
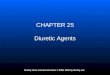
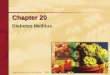
Figure 5-7Figure 5-7
Types of gastric resections with anastomoses.
A, Billroth I. B, Billroth II.
Removes antrum; connectstomach to duodenum
Attach rest of stomach to Jejunum; Close duodenal end

Slide 30Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Gastric and duodenal ulcers (continued) Complications after gastric surgery
• Dumping syndrome Rapid dump of food from stomach to duodenum leads to
diarrhea
• Pernicious anemia Missing stomach = missing intrinsic factor
• Iron deficiency anemia Nutritional deficit – poor absorption time

Slide 31Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Antidiarrheal medicationsAntidiarrheal medications
• Antidiarrheal Pepto-Bismol (bismuth subsalicylate) Lomotil (diphenoxylate with atropine) Kaopectate (kaolin-pectin) Imodium (loperamide)
• Anticholinergic (dry you up) Donnatol, Bentyl (anti-spasmotics)

Anticholinergics and Antispasmodics –Edmunds 306-307
Action and Uses Anticholinergic-antispasmodic preparations reduce GI
tract spasm and intestinal motility, acid production, and gastric motility, thus reducing pain Use: peptic ulcer, pylorospasm, biliary colic, hypermotility,
irritable colon, and acute pancreatitis Antidiarrheals reduce the fluid content of the stool and
decrease peristalsis and motility of the intestinal tract; increase smooth-muscle tone and diminish secretions Use: treatment of nonspecific diarrhea or diarrhea caused by
antibiotics
32Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Slide 33Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Cancer of the stomach Etiology/pathophysiology
• Most commonly adenocarcinoma
• Primary location is the pyloric area
• Risk factors: History of polyps Pernicious anemia Hypochlorhydria Gastrectomy; chronic gastritis; gastric ulcer Diet high in salt, smoked foods, preservatives, and
carbohydrates Diet low in fresh fruits and vegetables

Slide 34Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Cancer of the stomach (continued) Clinical manifestations/assessment
• Early stages may be asymptomatic
• Vague epigastric discomfort or indigestion
• Postprandial fullness
• Ulcer-like pain that does not respond to therapy
• Anorexia; weight loss
• Weakness
• Blood in stools; hematemesis
• Vomiting after fluids and meals

Slide 35Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the StomachDisorders of the Stomach
• Cancer of the stomach (continued) Diagnostic tests
• GI series• Endoscopic/gastroscopic examination• Stool for occult blood• RBC, hemoglobin, and hematocrit
Medical management/nursing interventions• Surgery
Partial or total gastric resection
• Chemotherapy and/or radiation
Prognosis: usually poor due to lack of clinical signs and metastasis

Slide 36Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Infection Etiology/pathophysiology
• Invasion of the alimentary canal by pathogenic microorganisms
• Most commonly enters through the mouth in food or water
• Person-to-person contact
• Fecal-oral transmission
• Long-term antibiotic therapy can cause an overgrowth of the normal intestinal flora (C. difficile)

Slide 37Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Infection (continued) Clinical manifestations/assessment
• Diarrhea
• Rectal urgency
• Tenesmus (ineffective, painful strain to defecate)
• Nausea and vomiting
• Abdominal cramping
• Fever

Slide 38Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Infection (continued) Diagnostic tests
• Stool culture Medical management/nursing interventions
• Let the body rid itself of causative agent
• Antibiotics if stool culture has WBCs
• Fluid and electrolyte replacement – oral first
• Kaopectate and Pepto-Bismol will thicken the stool and decrease the volume.

Slide 39Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Irritable bowel syndrome Etiology/pathophysiology
• Episodes of alteration in bowel function
• Spastic and uncoordinated muscle contractions of the colon
Clinical manifestations/assessment• Abdominal pain
• Frequent bowel movements
• Sense of incomplete evacuation
• Flatulence, constipation, and/or diarrhea

Slide 40Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Irritable bowel syndrome (continued) Diagnostic tests
• History and physical examination Medical management/nursing interventions
• Pharmacological management Anticholinergics Milk of magnesia Mineral oil for constipation Opioids slow bowel motility Antianxiety agents if panic attacks also occur
• Dietary recommendations • Bulking agents; increase fiberPrognosis: good with good diet and stress managment

Slide 41Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Ulcerative colitis
• What types of treatments may have been available to Pierre 60 years ago? Etiology/pathophysiology
• Ulceration of the mucosa and submucosa of the colon
• Tiny abscesses form that produce purulent drainage, slough the mucosa, and ulcerations occur
• Twice the incidence of Crohn’s disease Clinical manifestations/assessment
• Diarrhea—pus and blood; 15 to 20 stools per day
• Abdominal cramping
• Involuntary leakage of stool
• Exacerbations and remissions

Slide 42Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Ulcerative colitis (continued) Diagnostic tests
• Barium studies, colonoscopy, stool for occult blood Medical management/nursing interventions
• Pharmacological management Azulfidine, Dipentum, Rowasa, corticosteroids, Imodium
• Dietary recommendations: No milk products or spicy foods; high-protein, high-calorie; total parenteral nutrition during bowel rest
• Stress control
• Assist patient to find coping mechanisms

Slide 43Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Ulcerative colitis (continued) Medical management/nursing interventions
• Surgical interventions Colon resection Ileostomy Ileoanal anastomosis Proctocolectomy Kock pouch
Maintain periostomal skin integrity; provide emotional support

Slide 44Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
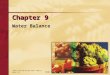
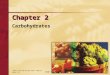
Figure 5-9Figure 5-9
Kock pouch (Kock continent ileostomy).

Slide 45Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 5-10Figure 5-10
Ileostomy with absence of resected bowel.

Slide 46Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Crohn’s disease Etiology/pathophysiology
• Inflammation, fibrosis, scarring, and thickening of any/all layers bowel wall
• Can occur anywhere in the intestines Clinical manifestations/assessment
• Weakness; loss of appetite
• Diarrhea: 3 to 4 daily; contain mucus and pus
• Right lower abdominal pain
• Steatorrhea
• Anal fissures and/or fistulas

Slide 47Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Crohn’s disease (continued) Medical management/nursing interventions
• Pharmacological management Corticosteroids Azulfidine Antibiotics Antidiarrheals; antispasmodics Enteric-coated fish oil capsules B12 replacement

Slide 48Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Crohn’s disease (continued) Medical management/nursing interventions
• Dietary recommendations High-protein Elemental (basic level of nutrition – readily absorbed) Hyperalimentation (IV) Avoid
o Lactose-containing foods, brassica vegetables, caffeine, beer, monosodium glutamate, highly seasoned foods, carbonated beverages, fatty foods
• Surgery Segmental resection of diseased bowel
Prognosis: chronic condition with high rates of recurrence

Slide 49Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Appendicitis Etiology/pathophysiology
• Inflammation of the vermiform appendix
• Lumen of the appendix becomes obstructed, the E. coli multiplies, and an infection develops
Clinical manifestations/assessment• Rebound tenderness over the right lower quadrant of
the abdomen (McBurney’s point)
• Vomiting
• Low-grade fever
• Elevated WBC

Slide 50Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Appendicitis (continued) Diagnostic tests
• WBC
• Roentgenogram
• Ultrasound
• Laparoscopy Medical management/nursing interventions
• Appendectomy

Slide 51Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Diverticular disease When would Therese discover that she had
diverticuli? She also has something secondary to them___________________?
Etiology/pathophysiology• Diverticulosis
Pouch-like herniations through the muscular layer of the colon
• Diverticulitis Inflammation of one or more diverticula

Slide 52Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 5-11Figure 5-11
Diverticulosis.

Slide 53Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Diverticular disease (continued) Clinical manifestations/assessment
• Diverticulosis May have few, if any, symptoms Constipation, diarrhea, and/or flatulence Pain in the left lower quadrant
• Diverticulitis Mild to severe pain in the left lower quadrant Elevated WBC; low-grade fever Abdominal distention Vomiting Blood and/or pus in stool

Slide 54Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Diverticular disease (continued) Medical management/nursing interventions
• Diet high in fiber (fresh fruit and vegetables)• Decreased intake of fat and red meat• Increase physical exercise• Weight reduction for the obese• Avoid increasing intra-abdominal pressure
Stool softeners Prevent hemorrhoids
• Check for signs of peritonitis

Slide 55Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Diverticular disease (continued) Medical management/nursing interventions
(continued)• Surgery
Hartmann’s pouch Double-barrel transverse colostomy Transverse loop colostomy
Prognosis is good.

Slide 56Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Peritonitis Etiology/pathophysiology
• Inflammation of the abdominal peritoneum
• Bacterial contamination of the peritoneal cavity from fecal matter or chemical irritation
Clinical manifestations/assessment• Severe abdominal pain; nausea and vomiting
• Abdomen is tympanic; absence of bowel sounds
• Chills; weakness
• Weak rapid pulse; fever; hypotension

Slide 57Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines• Peritonitis (continued)
Diagnostic tests• Flat plate of the abdomen• CBC
Medical management/nursing interventions • Pharmacological management
Parenteral antibiotics Analgesics IV fluids
• Position patient in semi-Fowler’s position• Surgery
Repair cause of fecal contamination Removal of chemical irritant
• NG tube to prevent GI distention

Slide 58Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• External hernias Etiology/pathophysiology
• Congenital or acquired weakness of the abdominal wall or postoperative defect
Abdominal Femoral or inguinal Umbilical

Slide 59Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• External hernias (continued) Clinical manifestations/assessment
• Protruding mass or bulge around the umbilicus, in the inguinal area, or near an incision
• Incarceration
• Strangulation Diagnostic tests
• Radiographs
• Palpation

Slide 60Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• External hernias (continued) Medical management/nursing interventions
• If no discomfort, hernia is left unrepaired, unless it becomes strangulated or obstruction occurs
• Truss (supportive garment)
• Surgery Synthetic mesh is applied to weakened area of the
abdominal wall

Slide 61Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Hiatal hernia Etiology/pathophysiology
• Protrusion of the stomach and other abdominal viscera through an opening in the membrane or tissue of the diaphragm
• Contributing factors: obesity, trauma, aging Clinical manifestations/assessment
• Most people display few, if any, symptoms
• Gastroesophageal reflux

Slide 62Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
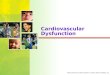
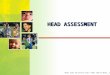
Figure 5-15Figure 5-15
Hiatal hernia. A, Sliding hernia. B, Rolling hernia.

Slide 63Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Hiatal hernia (continued) Medical management/nursing interventions
• Head of bed should be slightly elevated when lying down
• Do not eat before going to bed
• Surgery Posterior gastropexy Transabdominal fundoplication (Nissen)

Slide 64Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Intestinal obstruction Etiology/pathophysiology
• Intestinal contents cannot pass through the GI tract
• Partial or complete
• Mechanical
• Non-mechanical Clinical manifestations/assessment
• Vomiting; dehydration
• Abdominal tenderness and distention
• Constipation

Slide 65Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 5-17Figure 5-17
Intestinal obstructions. A, Adhesions. B, Volvulus.

Slide 66Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Intestinal obstruction (continued) Diagnostic tests
• Radiographic examinations - flat plate
• BUN, sodium, potassium, hemoglobin, and hematocrit Medical management/nursing interventions
• Evacuation of intestine NG tube to decompress the bowel Nasointestinal tube with mercury weight
• Surgery Required for mechanical obstructions

Slide 67Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Colorectal cancer Etiology/pathophysiology
• Malignant neoplasm that invades the epithelium and surrounding tissue of the colon and rectum
• Second most prevalent internal cancer in the United States
Clinical manifestations/assessment• Change in bowel habits; rectal bleeding
• Abdominal pain, distention, and/or ascites
• Nausea
• Cachexia

Slide 68Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Cancer of the colon (continued) Diagnostic tests
• Proctosigmoidoscopy with biopsy
• Colonoscopy
• Stool for occult blood Medical management/nursing interventions
• Radiation
• Chemotherapy

Slide 69Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Cancer of the colon (continued) Medical management/nursing interventions
(continued)• Surgery
Obstructiono One-stage or two-stage resectiono Two-stage resection
Colorectal cancero Right or left hemicolectomyo Anterior rectosigmoid resection

Slide 70Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Hemorrhoids Etiology/pathophysiology
• Varicosities (dilated veins) External or internal
• Contributing factors Straining with defecation, diarrhea, pregnancy, CHF,
portal hypertension, prolonged sitting and standing
Clinical manifestations/assessment• Varicosities in rectal area
• Bright red bleeding with defecation
• Pruritus
• Severe pain when thrombosed

Slide 71Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Hemorrhoids (continued) Medical management/nursing interventions
• Pharmacological management Bulk stool softeners Hydrocortisone cream or Preparation H Topical analgesics
• Sitz baths
• Ligation
• Sclerotherapy; cryotherapy
• Infrared photocoagulation
• Laser excision
• Hemorrhoidectomy

Slide 72Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Anal fissure Linear ulceration, crack or laceration of the skin of the
anus Usually caused by trauma Lesions usually heal spontaneously May be excised surgically
• Anal fistula Abnormal opening on the surface near the anus Usually from a local abscess Common in Crohn’s disease Treated by a fistulectomy or fistulotomy

Slide 73Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the IntestinesDisorders of the Intestines
• Fecal incontinence Potential causes Medical management/nursing interventions
• Biofeedback training
• Bowel training
• Patient education
• Dietary recommendations

Laxatives – Edmunds 311, 6th ed
Aid in the elimination of stool from the rectum
Bulk-forming agents - Metamucil Fecal softeners -Colace Hyperosmolar or saline solutions – Fleet’s Lubricants – Mineral oil Stimulant or irritant laxatives - Ducolax
74Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Laxatives (cont.)
Action and Uses Bulk-forming laxatives absorb water and expand,
increasing the bulk and moisture content of the stool; peristalsis increases, and absorbed water softens the stool
Fecal softeners lower the surface tension, which allows the fecal mass to be softened by intestinal fluids
Hyperosmolar laxatives produce an osmotic effect by drawing water into the bowel, thereby promoting peristalsis and bowel movement
75Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Laxatives (cont.)
Action and Uses (cont.) Lubricant laxatives create a barrier between
feces and the colon, preventing colon reabsorption and causing softening of the stool
Stimulant or irritant laxatives work according to the agent
76Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Laxatives (cont.)
Adverse Reactions Nausea and vomiting, obstruction,
hypersensitivity Cramping, diarrhea Electrolyte disturbances
77Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Laxatives (cont.)
Drug Interactions Reduced effectiveness of antibiotics,
anticoagulants, digitalis, and salicylates when combined with laxatives
Nursing Implications and Patient Teaching Assessment (CHF)
78Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Disulfiram - Antabuse
Used in the management of alcoholism
Unpleasant reaction when combined with alcohol – severe nausea, vomiting and diarrhea; severe headache, SOB, hyperventilation, tachycardia and can lead to death
79Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Other Intolerances or Allergies
Not genetic inborn errors of metabolism Rather, caused by food intolerances or
allergies Lactose intolerance: deficiency of any of the
disaccharidases in small intestine• Insufficient lactase to break down milk
• Abdominal cramping and diarrhea
Produces containing lactose must be avoided
80Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Small Intestine – review of anatomy and absorption
81Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Absorption Processes (p. 71)
Simple diffusion: particles move outward in all directions toward areas of lesser concentration
Facilitated diffusion: uses a protein channel for carrier-assisted movement of larger particles
Active transport: carrier partner (e.g., sodium) moves particles across a membrane
Pinocytosis: larger materials are engulfed by a cell
82Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Transport (p. 73) Vascular system: veins and arteries
Carry water-soluble nutrients, oxygen, other vital substances
Transport wastes for removal Portal circulation first carries nutrients to liver for cell
enzyme work Lymphatic system
Carries non–water-soluble fatty materials Lymph vessels in villi absorb materials Route to larger lymph vessels Eventually to blood stream through thoracic duct
83Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Stored Energy (p. 74)
Energy beyond that needed at present is stored for future
Glucose is converted to glycogen via glycogenesis, stored in liver or muscles
When glycogen reserves are full, excess is stored as fat via lipogenesis
Excess protein/amino acids converted to glucose via gluconeogenesis
84Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Errors in Digestion and Metabolism (p. 75)
Genetic defects: cell is missing enzyme controlling metabolism of a specific nutrient Phenylketonuria (PKU)
• Enzyme responsible for metabolizing essential amino acid phenylalanine is missing
• Untreated, causes permanent mental retardation and CNS damage
• With proper treatment, affected children may have normal and healthy lives
85Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Errors in Digestion and Metabolism (cont’d) (p. 75)
Genetic defects (cont’d) Galactosemia
• Enzyme responsible for metabolizing galactose to glucose is missing
• All sources of lactose must be eliminated from diet
• Untreated, can cause brain and liver damage
• Screening and treatment can enable normal life
86Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.

Errors in Digestion and Metabolism (cont’d) (p. 77)
Genetic defects (cont’d) Glycogen storage diseases (GSD)
• Group of rare genetic defects
• Absence of enzymes required for synthesis or breakdown of glycogen
• Form of disease depends on enzyme missing
87Copyright © 2013 Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.