Embed Size (px)
Citation preview

CHAPTER
16Schizophrenia and OtherPsychotic Disorders
EILEEN TRIGOBOFF
KEY TERMSanhedonia 7
avolition 7
blunted affect 16
catatonic type 8
delusional disorder 10
delusions 4
dopamine hypothesis 11
expressed emotion (EE) 14
flat affect 6
hallucination 3
illusions 15
negative symptoms 3
positive symptoms 3
poverty of speech 6
relapse 8
schizoaffective disorder 9
schizophrenia 3
schizophrenia, catatonictype 8
schizophrenia,disorganized type 8
schizophrenia, paranoidtype 8
schizophrenia, residualtype 9
schizophrenia,undifferentiated type 9
schizophreniform disorder 9
thought blocking 16
waxy flexibility 8
LEARNING OUTCOMESAfter completing this chapter, you will be able to:
1. Describe the central features of schizophrenia.2. Distinguish among the subtypes of schizophrenia.3. Compare and contrast the various biopsychosocial theories that address the
possible causes of schizophrenia.4. Explain how psychological and social pressures can influence the course of
schizophrenia.5. Discuss the major nursing implications in caring for clients with difficult and
chronic illnesses such as schizophrenia.6. Discuss the major nursing implications in supporting the families of persons with
schizophrenia.7. Describe methods to prevent or minimize relapses in schizophrenia.8. Identify the personal characteristics you bring to the care of clients with
schizophrenia that might cause you to distance yourself or fail to understandtheir experience and difficulties.
MEDIALINK www.prenhall.com/kneisl
Go to the Prentice Hall Nursing MediaLink CD-ROM and the Companion Website atwww.prenhall.com/kneisl for interactive resources.
2
CRITICAL THINKING CHALLENGE
Like most individuals with schizophrenia, Alicia is extremely sensitive to herenvironment. When stressed, she often runs the risk that her symptoms will worsen. Inthe course of living in usual ways, everyone experiences stress related to conducting day-to-day activities. Alicia’s nurse at the mental health clinic has been preparing her to copewith working at a local store. Specific environmental features, such as noise and visualdistractions, are particularly difficult for Alicia to deal with.
1. Why do mental health care providers advocate that people with schizophreniainteract with the larger community in treatment programs, jobs, and living in thecommunity?
2. Would people with schizophrenia be better off in protected environments such assemistructured group homes or structured and sheltered workshops?
3. How would you help Alicia deal with noise and visual distractions?4. How do most working people create an environment that suits their strengths and
weaknesses? Can these methods be useful for Alicia?
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 2

SYMPTOMS OF SCHIZOPHRENIAThe diagnosis of schizophrenia requires not only the pres-ence of distinct symptoms but also the persistence of thosesymptoms over time. Symptoms must be present for at least6 months, and active-phase symptoms (called Criterion Asymptoms in the DSM-IV-TR) must be present for at least 1 month during that time, before schizophrenia can be diag-nosed. The diagnostic criteria for schizophrenia are pre-sented in the DSM-IV-TR feature below.
The symptoms of schizophrenia are conceptually sepa-rated into positive symptoms, which represent an excess ordistortion of normal functioning, or an aberrant response; andnegative symptoms, which represent a deficit in functioning.
Positive SymptomsPositive symptoms include the three most pronounced out-ward signs of the disorder: hallucinations, delusions, and dis-organization in speech and behavior.
HallucinationsHallucinations are the most extreme and yet the most commonperceptual disturbance in schizophrenia. A hallucination is a
Schizophrenia is a complex disorder with an extremelyvaried presentation of symptoms. It affects cognitive, emo-tional, and behavioral areas of functioning. According to theNational Institute of Mental Health the prevalence rate forschizophrenia is approximately 1.1% of the population overthe age of 18. The age of onset is typically between the lateteens and mid-thirties, although there are cases outside thatrange. For example, there is a rarely seen childhood schizo-phrenia as well as a late-onset schizophrenia (referred to asLOS) that is diagnosed after age 45 and seen more often inwomen. The illness is diagnosed most frequently in the earlytwenties for men and late twenties for women. The progres-sion of the disease is as variable as its presentation. In somecases, the disease progresses through exacerbations and re-missions; in other cases, it takes a chronic, stable course;while in still others, a chronic, progressively deterioratingcourse evolves. The National Institute of Mental Healthwebsite on schizophrenia (www.nlm.nih.gov/medlineplus/schizophrenia.html ), which can be accessed through a directlink on the Companion Website for this book, will also serveas a resource on schizophrenia for you, your clients, and theirfamilies.
Chapter 16 • Schizophrenia and Other Psychotic Disorders 3
USING DSM-IV-TRHealth care providers often use language unfamiliar to clients and their families. Reword this DSM statement to make it easier for clients andfamily members to understand: “Two (or more) of the following, each present for a significant portion of time during a 1-month period (or lessif successfully treating): delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior, or negative symptoms.”
of prodromal or residual symptoms. During these prodromal orresidual periods, the signs of the disturbance may be mani-fested by only negative symptoms or two or more symptomslisted in Criterion A present in an attenuated form (e.g., oddbeliefs, unusual perceptual experiences).
D. Schizoaffective and Mood Disorder exclusion: Schizoaffective Disorder and Mood Disorder with psychotic features have been ruled out because either (1) no Major Depressive, Manic, or Mixed Episodes have occurred concurrently with the active-phase symptoms; or (2) if mood episodes have occurred during active-phase symptoms, their total duration has been brief rela-tive to the duration of the active and residual periods.
E. Substance/general medical condition exclusion: The distur-bance is not due to the direct physiological effects of a sub-stance (e.g., a drug of abuse, a medication) or a generalmedical condition.
F. Relationship to a Pervasive Developmental Disorder: If there is ahistory of Autistic Disorder or another Pervasive DevelopmentalDisorder, the additional diagnosis of Schizophrenia is madeonly if prominent delusions or hallucinations are also presentfor at least a month (or less is successfully treated).
Source: Reprinted with permission from the Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition, Text Revision(Copyright 2000). American Psychiatric Association.
Diagnostic Criteria for SchizophreniaDSM-IV-TRA. Characteristic symptoms: Two (or more) of the following, each
present for a significant portion of time during a 1-month pe-riod (or less if successfully treated):1. delusions2. hallucinations3. disorganized speech (e.g., frequent derailment or incoher-
ence)4. grossly disorganized or catatonic behavior5. negative symptoms, i.e., affective flattening, alogia, or
avolition Note: Only one Criterion A symptom is required if delusions are bizarre or hallucinations consist of a voice keeping up arunning commentary on the person’s behavior or thoughts, ortwo or more voices conversing with each other.
B. Social/occupational dysfunction: For a significant portion of thetime since the onset of the disturbance, one or more majorareas of functioning such as work, interpersonal relations, orself-care are markedly below the level achieved prior to theonset (or when the onset is in childhood or adolescence, failureto achieve expected level of interpersonal, academic, or occu-pational achievement).
C. Duration: Continuous signs of the disturbance persist for at least6 months. This 6-month period must include at least 1 monthof symptoms (or less if successfully treated) that may meet Cri-terion A (i.e., active-phase symptoms) and may include periods
MED
IALIN
KN
ational Institute of Mental H
ealth
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 3

4 Unit IV • CLIENTS WITH MENTAL DISORDERS
FIGURE16-1 ■ Distorted perceptions. The distorted visual percep-tions indicated by this figure exemplify what is experienced bysomeone during visual hallucinations.
subjective sensory experience that is not actually caused byexternal sensory stimuli. One or more of the five senses are in-volved in hallucinations. Hallucinations may be auditory(heard), visual (seen), olfactory (smelled), gustatory (tasted),or tactile (touched). FIGURE 16-1 ■ represents how someone withvisual hallucinations may distort a scene.
The most common form of hallucination in schizophre-nia, at least in the western hemisphere, is hearing voices orsounds that are distinct from the person’s own thoughts. If avoice is heard, it (or they) may be friendly or hostile andthreatening. It is particularly characteristic of schizophrenia ifthe person hears two or more voices conversing with eachother, or hears a voice that provides continuous comments onthe train of thought.
Having auditory hallucinations does not necessarilymean that the individual hears human speech. As you willsee in Table 16-3, several other sounds made by clocks, ani-mals, insects, and so on may be hallucinated. Do not con-fuse hallucinatory experiences with synesthesia, which isthe experience of having multiple senses involved in a sin-gle event; synesthesia is not a disease or disorder. Distin-guishing between synesthesia and hallucinations can beaccomplished by ensuring that there is no external stimula-tion to the sensations. Examples of synesthesia include see-ing sounds, seeing colors when in pain, and hearing smells.
This knowledge must, necessarily, influence the way yougather information during assessment.
Hallucinations also occur in several other illnesses be-sides schizophrenia. Dementia (Chapter 14 ), substanceabuse (Chapter 15 ), and depression (Chapter 17 ) aresome of them. TABLE 16-1 ■ links hallucinations with com-monly associated disease processes. Hallucinations can alsobe experienced under extreme physiologic stress or as a sideeffect of medications.
DelusionsDelusions are mistaken or false beliefs about the self or theenvironment that are firmly held even in the face of discon-firming evidence. Delusions may take many forms. Indelusions of persecution, the person may think that othersare following him, spying on him, trying to damage or takesomething of value like a reputation, or trying to tormenthim (e.g., “They have misters in my apartment that sprayLSD onto me when I walk around.”). In another commonform, delusions of reference, the person thinks that publicexpressions, like a story on the television or a newspaper ar-ticle, are specifically addressed to him or her or that theevent occurred because of his or her thoughts or actions(e.g., “When the newscaster wears navy blue, she is speakingmy thoughts to the world.”). Specific delusions are discussedin TABLE 16-2 ■ .
Disordered Speech and BehaviorOther positive symptoms represent excesses of language orbehavior. Disorganized speech is the outward sign of disor-dered thoughts and may range from less severe forms (theperson moves rapidly from one topic to another), to severeforms (the person’s speech cannot be logically understood).Positive symptoms include low-level behavioral responsesto the environment characterized by such disorganized be-havior as agitated, nonpurposeful, or random movements,and waxy flexibility (discussed and defined later in thischapter). The positive symptoms of schizophrenia are dis-cussed in TABLE 16-3 ■.
TABLE 16-1 ■ Types of Hallucinations
Perceptual Disturbance
Commonly Associated Disease Process
Auditory Schizophrenia
Visual Dementia
Tactile* Acute alcohol withdrawal
Somatic* Schizophrenia
Olfactory* Seizure disorders
Gustatory* Seizure disorders
*Also referred to as “proprioceptive hallucinations,” associated with infec-tions and tumors.
MED
IALI
NK
Cas
e St
udy,
Sch
izop
hren
ia w
ith A
udito
ry H
allu
cina
tions
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 4

Chapter 16 • Schizophrenia and Other Psychotic Disorders 5
TABLE 16-2 ■ Types of Delusions
Disturbances in Thinking Definition Example
Delusions of persecution Belief that others are hostile or trying to harm theindividual
A woman notices a man looking at her and believesthat he is trying to follow her.
Delusions of reference False belief that public events or people are directlyrelated to the individual
A man hears a story on the evening news and believesit is about him.
Somatic delusions Belief that one’s body is altered from normal structure or function
An elderly woman believes that her bowel is filled withcement and refuses to eat.
Thought broadcasting Belief that one’s unspoken thoughts can be heard A young client believes that everyone around himknows he’s attracted to a nurse although he has saidnothing.
Delusions of control Belief that one’s actions or thoughts are controlled by an external person or force
A woman believes that her neighbor controls herthoughts by means of his home computer.
TABLE 16-3 ■ Positive Symptoms
Positive Symptom Examples
Hallucinations
Auditory Human speech (speaking clearly, mumbling, whispering, singing, yelling, screaming, one voice, several voices,voice speaking to client, voices speaking to each other, male, female, both, indistinguishable, imitatingnonhuman sounds)Mechanical sounds (clocks, metal clanging, clicking)MusicAnimal soundsInsect soundsWind through the treesGrating sounds made by walking on sandCrinkling sound from plastic or aluminum wrapsThe sound of the earth moving or heaving as during an earthquake
Visual Blood PeopleAnimals Movement of large objectsDistortions of everyday sights Auras
Olfactory Green peppers BloodFumes Burning materialsGarlic Urine or fecesSemen Rotting meatSulfur
Gustatory Metallic flavor BloodUrine or feces Semen
Tactile Being pregnant Giving birthBeing beaten ElectrocutionBeing raped Band around headGrease on hands Moving tumorsInternal movements
Delusions
Persecutory “I cannot leave my apartment more than once a month. I have to have this cardboard in my pockets when I goout so the CIA can’t take pictures of me.”
Referential “I didn’t mean to do it. I was just thinking what would happen if the train derailed. I’m sorry I killed all thosepeople.”
—Continued
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 5

6 Unit IV • CLIENTS WITH MENTAL DISORDERS
TABLE 16-3 ■ Positive Symptoms
Positive Symptom Examples
Delusions—Continued
Somatic “I am going to be hemorrhaging, bleeding to death through my mouth.”Or: “I have an alien gestating in my belly. When he is mature he’ll drip from my palms like sweat.”
Religious “My daughter is the devil, saturated with evil, because her age of ascendancy is 666 (June 6, 2006).”
Substitution “It looks just like my wife but it’s really a robot.”
Thought insertion “These thoughts are being put in my head by the alien conspiracy.”Or: “When I get angry it’s because the NSA is altering my brain waves.”
Nihilistic “Everything is falling apart. My insides are rotting away and so is everything else.”
Grandiose “I made $7 million from a software program I developed and they’re keeping it from me until I tell them mysecret programming wizardry.”Or: “I am not who you think I am. I work midnights at all the top law firms so I can get all their work done for them.”
Disorganized Speech
Loose associations “I came here by bus, but bussing is kissing, I wasn’t kissing but if you keep it simple that is a business tenet forKISS. That was a great group that played on and on, but I’m not playing with you. You are youthful looking. Look out for yourself too.”
Word salad “Wimple sitting purple which the twilighted cheshire, for then frames of silver ticking bubble and.”
Clanging “I want to eat neat treat seat beat.”“I’m fine it’s a sign fine whine wine pine dine.”
Echolalia Client repeats pieces of what is said or entire phrases: Nurse asks, “How are you today?” and the client states,“You today.” Or client states, “I love smelling roses. I love smelling roses.”
Behavior
Disorganized Client walks around aimlessly picking up everything available to him and touching all objects and surfaces.
Catatonic Excited catatonia: A client in the ER is repeatedly assaultive, hyperactive, or cannot sit still.Waxy flexibility: Client maintains a rigid position, allows another to move him or her into new positions andmaintains the new position.
Thinking
Lack of planning skills Indecisiveness Lack of problem-solving skills
Concrete thinking Blocking Difficulty initiating tasks
Negative SymptomsNegative symptoms of schizophrenia are less dramatic butjust as debilitating as positive symptoms. TABLE 16-4 ■ givesexamples of negative symptoms of schizophrenia. Negativesymptoms include the “four As” of schizophrenia:
1. Flat affect and apathy2. Alogia3. Avolition4. Anhedonia
Flat AffectPeople with schizophrenia often appear to have unemotionalor very restricted emotional responses to their experiences.Flat affect “is the absence or near absence of any signs of
affective expression” as well as poor eye contact (AmericanPsychiatric Association [APA], 2000). To see how flat affectdiffers from a normal range of affect, imagine someone re-sponding to winning a prize (“This is great! I’m so happy!”).Now imagine that same person with much less emotion inher response and no emotion showing on her face (“Oh.”).The difference between the two responses is the flattening ofaffect.
AlogiaBrief, empty verbal responses are known as alogia. Ratherthan saying a few sentences in response to a question, clientswith alogia reply with a single word or a very limited numberof words. This poverty of speech is thought to be sympto-matic of diminished thoughts and is different from a refusal
—Continued
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 6

Chapter 16 • Schizophrenia and Other Psychotic Disorders 7
TABLE 16-4 ■ Negative Symptoms
Negative Symptom Examples
Flat Affect The client maintains the sameemotional tone when told his motherhas died as when told it is time toattend programs. “OK.”
Apathy The client has feelings of indifferencetoward people, events, activities, andlearning.
Avolition The client does not get to the job hereally wanted because he couldn’t getup and take the bus.
Anhedonia The client apparently derives nopleasure from bowling when, prior togetting sick, he used to enjoy it.
Alogia Rather than using a series of sentencesor several words, the client, whenasked about his day, speaks sparsely ina limited, stilted manner: “Fine.”
to speak. Under these circumstances, the client does not usemany words to express experiences or thoughts.
AvolitionA symptom that is frequently misunderstood by families andmembers of the larger community is avolition, an inability topursue and persist in goal-directed activities. You may see evi-dence of this negative symptom when a client fails to go for a jobinterview or fails to become involved in an easily available activ-ity. The schizophrenic person’s experience of avolition is oftenmisinterpreted as laziness or an unwillingness to support him- orherself, rather than as a symptom of this chronic disorder. Thismisunderstanding often affects the ability of family membersand friends to stay involved in relationships with the client. Theymay feel frustrated, as if their efforts have been wasted, or per-sonally rejected because their suggestions have gone unheeded.
AnhedoniaAnhedonia, the inability to experience pleasure, is an impor-tant symptom that challenges many nurses. It is difficult toimagine, and even more arduous to empathize with, someonewho cannot seem to enjoy even small aspects of life. It is im-portant to remember that people who have schizophrenia can-not enjoy experiences because of a physiologic reason overwhich they have no control.
Negative symptoms of schizophrenia are difficult to as-sess because they differ in degree, but not in form, fromeveryday experience. While few of us have experienced truehallucinations, many of us know what it is like to have a daywithout the energy to pursue goal-directed activities. Anotherdifficulty in recognizing the presence of negative symptomsstems from the fact that people with schizophrenia often livein difficult situations that may lead to restricted emotionalexpression and disturbed goal-directed activities. Living inpoverty or in unsettled circumstances—homelessness, forexample—can induce feelings of desperation or despair,
which may mimic the negative symptoms of schizophrenia. Itis important to try to separate environmental influences onexperience from the disease process, and to note the persist-ence of the symptoms over time across a variety of circum-stances. For example, if a client is living in a rooming housewhere others around him are likely to steal, that client willnot be safe talking excitedly about having received a giftfrom his parents. If, however, the client is not excited whenin his own home in front of his parents and trusted others, thepresence of a negative symptom of schizophrenia is likely.
Another important criterion for recognizing schizophre-nia is detecting an impaired ability to perform and completesocial and work obligations. It is diagnostic of schizophreniawhen the person has difficulty performing in one or moreareas of life including work, school, social relationships, andthe maintenance of everyday activities such as dressing andproviding food for oneself.
Somatic TreatmentsPrior to the 1950s—which is referred to as the pre-neurolep-tic age—insulin coma, drug or electrically induced shocktreatments, and psychosurgery, including prefrontal loboto-mies, were used to treat schizophrenia. The impact of theseextreme somatic treatments did make a difference, for a time,in symptomatology but were not durable or beneficial andoften not ethical. Many hoped these treatments were the long-sought-after cure for schizophrenia because they were rela-tively quick and inexpensive compared to lengthy and costlyanalytic therapies. This hope was not realized.
Contemporary psychosurgery has been refined from agross assault on cranial tissue (the lobotomy of decades past)to procedures in which specific involved areas of the brain aredelicately shaped to reduce repetitive and destructive behav-iors (amygdalotomy, cingulotomy). Electroconvulsive therapy(ECT) has been improved upon and crafted to an impressivedegree in the last 20 years. Effective treatment with minimalrisks has been offered mostly for mood-disordered clients.
The introduction of psychoactive drugs in the1950s provided new alternatives for the treatment ofschizophrenia. Psychotropic medications, which in-fluence the thoughts, mood, and behavior of clients, madepreviously uncontrolled symptoms manageable. In the periodfollowing the introduction of psychotropic medications, theuse of seclusion and restraints declined dramatically, as didthe duration of hospital stays and numbers of clients in statemental hospitals.
A new optimism arose regarding the possible outcomesof mental illness. Because they controlled the most difficultsymptoms of psychosis, psychotropic medications made psy-chosocial or behavioral treatments possible for a muchgreater percentage of psychiatric clients. The major tranquil-izers did not live up to their promise of providing a cure forschizophrenia and other chronic psychiatric illnesses. How-ever, these drugs relieved the most debilitating symptoms formany clients and were the first step toward recovery or ahigher level of functioning.
Refer to Chapters 5, 6, 7, and 32 for more details on the history and the science behind somatic treatments.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 7

Ethical and legal aspects of somatic treatments are discussedin Chapter 13.
RelapseA client with schizophrenia is vulnerable after a period of sta-bility, however brief or extended, partial or complete, to a re-turn of symptoms. This is referred to as a relapse, and thedisease itself has a pattern of relapse and recovery. As achronic disorder, schizophrenia is characterized by relapsesalternating with periods of full or partial remission.
Although antipsychotic medication is effectivein reducing relapse rates, 30% to 40% of clients re-lapse within 1 year after hospital discharge even ifthey are receiving maintenance medication. This is a tremen-dous difficulty for the client to overcome; therefore, acknow-ledge the sense of demoralization likely with such a recurrentand debilitating course that cannot be altered significantly. Thecurrent hope is that the relapse rate will be reduced fromaround 35% to about 15% to 20%. The need to improve meth-ods for relapse prevention is clear (van Meijel et al., 2006).The following clinical examples detail how relapses can occurunder certain circumstances.
CLINICAL EXAMPLEDaryl, a 26-year-old with a diagnosis of paranoid schizophre-nia, decided to stop taking his quetiapine (Seroquel) becausehe didn’t think he needed it anymore. Within a few days ofstopping the medication, he was unable to leave the house forfear of someone harming him. Although he liked his job at thelocal cannery and knew that he had the chance to earn moremoney in the near future, he refused to go to work for fearthat he would be hit by a bus on his way there. He was even-tually fired because of poor attendance. The loss of a struc-tured schedule furthered his deterioration and Daryl relapsed,requiring hospitalization.
8 Unit IV • CLIENTS WITH MENTAL DISORDERS
CLINICAL EXAMPLEJeanne, 22, lived with her divorced mother and younger sisterMaura since her release from the hospital after her second psy-chotic episode. She found living alone too frightening and wasmore comfortable staying in her old room at home. WhenMaura began preparing to leave home for college, Jeanne be-came increasingly anxious, demanding to sleep in Maura’sroom at night and hiding Maura’s belongings. As Maura’s de-parture grew near, Jeanne began actively hallucinating andwithdrew to her room, refusing to talk to her mother or sister.
In this instance, a decrease in medication increasedDaryl’s biologic vulnerability, with marked behavioral, andeventually environmental, consequences. His relapse beganwith a medication issue and could have been prevented.
In this case, the client did not have sufficient copingskills to deal with her sister’s departure from the household,and her psychosis reemerged. Jeanne’s relapse may have been
averted had she been taught coping skills and had the oppor-tunity to practice them. However, learning is unfavorably af-fected by schizophrenia, motivation and energy are problems,and even a competent program of teaching cannot remove allthe negative consequences in response to life stress. Subtypesof schizophrenia are used to designate which symptoms areprominent. The subtypes are discussed below and in theDSM-IV-TR Diagnostic Criteria feature on page 9.
Paranoid TypeProminent hallucinations and delusions are present in theparanoid type of schizophrenia. Delusions are often persecu-tory or grandiose, and they often connect into a somewhat or-ganized story. Delusions may also be varied and includesomatic or religious delusions. Hallucinations often link withthe delusions, although this is not necessary. For example, aperson who believes he is being monitored by the FBI mayhear the voices of people he identifies as FBI agents laughingat him or talking to him.
Disorganized TypeThe central features present in the disorganized type ofschizophrenia are disorganized speech and behavior and flator inappropriate affect. The client appears disorganized andunkempt because basic everyday tasks like dressing oneselfcannot be accomplished. The client may have all the neces-sary clothing on, but the order of putting on each item ofclothing or the steps required to accomplish dressing (e.g.,buttoning, zipping, tying) may be too much to handle. Emo-tional expression may be either inappropriate to the contentof what the client is saying (e.g., laughing when discussingbeing thrown out of the house by roommates) or restrictedand flat. Hallucinations and delusions are typically more frag-mentary and disorganized than in the paranoid type. This sub-type has been referred to as potentially being the most severeform of the disease.
Catatonic TypeAlthough not seen frequently in the United States, thecatatonic type of schizophrenia is a distinctive type charac-terized by extreme psychomotor disruption. The client maydisplay substantially reduced movement to the point of stu-por, accompanied by negativism and resistance to any inter-vention. A client could display a type of posturing known aswaxy flexibility, a feature of catatonic motor behavior inwhich, when clients are placed in peculiar positions, they re-main almost completely immobile in the same position forlong stretches of time. Alternatively, extremely active andpurposeless movement (excitement) that is not influenced bywhat is going on around the person may be present. Addi-tional signs of the catatonic type of schizophrenia are repeat-ing what others say or mimicking their movements.
Undifferentiated TypeWhen a client is in an active psychotic state, meaning thatCriterion A symptoms for schizophrenia are met and theclient does not have prominent symptoms that match any of
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 8

Chapter 16 • Schizophrenia and Other Psychotic Disorders 9
tic criteria are the same as the Criterion A symptoms forschizophrenia. The main difference is that the client has expe-rienced the symptoms for at least 1 month and either recov-ered from the symptoms before 6 months, or 6 months havenot yet elapsed since the original symptoms began. Under thelatter set of circumstances, the diagnosis of schizophreniformdisorder is provisional until the 6 months have elapsed andthen a diagnosis is set. A second difference, besides duration,is that the client may show no impairment in social and workfunctioning.
Schizophreniform disorder may occur just prior to theonset of schizophrenia (i.e., be prodromal to [precede] schiz-ophrenia), yet approximately one third of clients diagnosedwith this disorder recover. The other two thirds go on to haveeither schizophrenia or schizoaffective disorder.
Schizoaffective DisorderIn schizoaffective disorder, two sets of symptoms—psychotic and mood symptoms—are present concurrently inthe same period of illness episode: Criterion A symptoms ofschizophrenia and symptoms of a mood disorder (either amajor depressive or manic disorder; see Chapter 17 ).Schizoaffective disorder is less common than, and has aslightly better prognosis than, schizophrenia, but it has a sub-stantially worse prognosis than mood disorders. Interactingwith a client who has schizoaffective disorder may requirethe same skills you would employ with a client who has
the prior subtypes, then undifferentiated type is diagnosed.Remember that a client’s diagnosis may also change over theyears as symptoms form and re-form. The particular subtypediagnosed at one point in time may not match what is cur-rently happening to a client. The subtype of schizophreniamay have shifted, with the undifferentiated subtype now mostrepresentative of the course of the disease.
Residual TypeThe residual type of schizophrenia is a subtype diagnosis re-served for a client who has had at least one documentedepisode of schizophrenia but now has no prominent positivesymptoms of the illness. Negative symptoms such as flat af-fect and inability to work are present, but prominent halluci-nations, delusions, and disorganized thoughts and behaviorare not. When a client has these characteristics, the client isconsidered to have residual features of the illness and re-ceives this subtype diagnosis.
OTHER PSYCHOTIC DISORDERSPsychosis occurs in a number of disorders in addition to schiz-ophrenia. The problems with symptoms can be short-lived ormay extend into significant periods of time with disability.
Schizophreniform DisorderSchizophreniform disorder is very similar to schizophreniaexcept the person has not been ill for very long. The diagnos-
DSM-IV-TR
USING DSM-IV-TRHealth care providers often use language unfamiliar to clients and their families. Reword this DSM statement to make it easier for clients andfamily members to understand: “Preoccupation with one or more delusions or frequent auditory hallucinations.”
Diagnostic Criteria for Schizophrenia Subtypes
PARANOID TYPEA type of Schizophrenia in which the following criteria are met:A. Preoccupation with one or more delusions or frequent auditory
hallucinations.B. None of the following is prominent: disorganized speech, disor-
ganized or catatonic behavior, or flat or inappropriate affect.
DISORGANIZED TYPEA type of Schizophrenia in which the following criteria are met:A. All of the following are prominent:
1. disorganized speech2. disorganized behavior3. flat or inappropriate affect
B. The criteria are not met for Catatonic Type.
CATATONIC TYPEA type of Schizophrenia in which the clinical picture is dominatedby at least two of the following:1. motoric immobility as evidenced by catalepsy (including waxy
flexibility) or stupor2. excessive motor activity (that is apparently purposeless and not
influenced by external stimuli)3. extreme negativism (an apparently motiveless resistance to all
instructions or maintenance of a rigid posture against attemptsto be moved) or mutism
4. peculiarities of voluntary movement as evidenced by posturing(voluntary assumption of inappropriate or bizarre postures),stereotyped movements, prominent mannerisms, or prominentgrimacing
5. echolalia or echopraxia
UNDIFFERENTIATED TYPEA type of Schizophrenia in which symptoms that meet Criterion Aare present, but the criteria are not met for the Paranoid, Disorga-nized, or Catatonic Type.
RESIDUAL TYPEA type of Schizophrenia in which the following criteria are met:A. Absence of prominent delusions, hallucinations, disorganized
speech, and grossly disorganized or catatonic behavior.B. There is continuing evidence of the disturbance, as indicated by
the presence of negative symptoms or two or more symptomslisted in Criterion A for Schizophrenia, present in an attenuatedform (e.g., odd beliefs, unusual perceptual experiences).
Source: Reprinted with permission from the Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition, Text Revision(Copyright 2000). American Psychiatric Association.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 9

schizophrenia. Disorganized speech may be an expression ofthis client’s psychosis. The Rx Communication box aboveprovides examples of therapeutic communication with aclient with the clang association form of disorganized speech.
One of the defining characteristics of schizoaffectivedisorder is when the hallucination or delusion occurs. A per-son who has schizoaffective disorder is likely to have halluci-nations or delusions regardless of mood state. In other words,if the person were delusional only when he or she had ex-treme problems with mood (mania or depression), it is likelythe diagnosis would be mood disorder with psychotic featuresrather than schizoaffective disorder.
Delusional DisorderDelusional disorder is diagnosed when the client holds one ormore nonbizarre delusions for a period of at least 1 month. Theclient must never have met the Criterion A symptoms for schiz-ophrenia. Although it is sometimes difficult to differentiatebizarre from nonbizarre delusions, the key is that the nonbizarredelusions could conceivably arise in everyday life. A nonbizarredelusion is the focus of the clinical example that follows.
RX COMMUNICATION
CLIENT WITH CLANG ASSOCIATIONSCLIENT: “The dining room lining trying to eat forever.”
NURSE RESPONSE 1: “Jack, are you having a problem getting yourfood?”
RATIONALE: Direct question allows the client with clang associationsto answer with a “yes” or “no” response, models how the communi-cation can be stated, and labels the situation as a problem.
NURSE RESPONSE 2: “Come with me and let’s get you set up.”
RATIONALE: This response reinforces the appropriateness of theclient’s coming to the nurse with a problem and concretely showsthe client how to resolve the problem.
CLINICAL EXAMPLEMartin holds the delusional belief that the police are trying toentrap him. He goes to extremes to protect his home with sur-veillance and security equipment. At the same time, he be-lieves that the police won’t bother him at work because hisboss, with whom he gets along well, is the son of a policeman.
10 Unit IV • CLIENTS WITH MENTAL DISORDERS
People with delusional disorders may function quitewell in areas of their life not affected by the delusion, yet be-have oddly in activities touched by the delusion. Delusionaldisorders are not common and arise predominantly duringmiddle and late adulthood.
A subtype of delusional disorder, the erotomanic type,occurs when clients believe that another person is in lovewith them. Typically this other person has no relationshipwhatsoever to the client, or the relationship is superficial atbest. Contacting the person, stalking the person, and displaysto impress the imagined lover, have involved celebrities,politicians, and even the man or woman next door.
Brief Psychotic DisorderIn a brief psychotic disorder, at least one of the Criterion Asymptoms for schizophrenia are present (hallucinations, delu-sions, disorganized speech or behavior) for at least 1 day, butfor less than 1 month. Upon remission of these symptoms,clients return to their level of functioning prior to the onset ofthe illness. This disorder may be brought on by a particularstressful event in the person’s life, including childbirth. Inother instances, a stressful life event cannot be specificallyidentified. Brief psychotic disorder is an unusual and seldom-seen phenomenon.
Additional Psychotic DisordersSeveral additional psychotic disorders are specified in theDSM-IV-TR:
■ Shared psychotic disorder■ Psychotic disorder due to a general medical condition■ Substance-induced psychotic disorder■ Psychotic disorder not otherwise specified (NOS)
Consult the DSM-IV-TR for diagnostic criteria for thesedisorders. However, in diagnosing any psychotic disorder, thediagnostician must explore the alternative explanation thatsymptoms may be caused by an underlying medical disorderor by substance use.
BIOPSYCHOSOCIAL THEORIESBeliefs about the causes of schizophrenia have changedover the centuries since schizophrenia was equated withearly senility. Theories about the treatment for schizophre-nia have also undergone change. For example, at one pointit was erroneously believed (based on the writings of Sig-mund Freud) that people with schizophrenia could not betreated because they were unable to form a therapeutic rela-tionship with a psychoanalyst. At another point, a nowdiscredited theory pointed to the behavior of parents, espe-cially mothers, causing schizophrenia in their offspring. It islikely that several factors interrelate to cause schizophreniaand several forces influence the effectiveness of treatment.A multifactorial cause and a varied approach to treatment,responsive to the individual’s needs, seem to be the bestapproach.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 10

Biologic TheoriesIt is unlikely that schizophrenia is caused by one specific bio-logic abnormality. Scientists have searched unsuccessfullyfor a unique biologic marker consistently present in peoplewith schizophrenia but absent in healthy people. At the sametime, evidence suggests that the disorder is not merely psy-chological and that biologic alterations are present. Particu-larly convincing is the fact that the symptoms associated withschizophrenia, such as delusions or hallucinations, are foundin healthy people only when they are in a state of metabolicimbalance or suffer from organic diseases. Individuals whohave brain tumors, have infections, or have ingested certaindrugs, for example, may experience hallucinations.
Genetic TheoriesPeople with schizophrenia inherit a genetic predisposition tothe disease rather than inheriting the disease itself. What sup-ports this theory is the fact that relatives of people with schizo-phrenia have a greater chance of developing the disease than domembers of the general population. While 1.1% of the popula-tion develops schizophrenia, 10% of the first-degree relatives(parents, siblings, children) of persons with schizophrenia arediagnosed with the disease during their lifetimes (Brookes etal., 2006; Karayiorgou & Gogos, 2006; Kessler, Chiu, Demler,& Walters, 2005). The risk of developing schizophrenia in-creases with the closeness of one’s relationship to a diagnosedperson. Siblings have a greater risk of developing the diseasethan do half-siblings or grandchildren, and these have a greaterrisk than more distant relatives, such as cousins.
There is no clear genetic marker for schizophrenia at thistime, although several research projects are involved in thesearch for susceptibility genes. The most promising develop-ment has been the Human Genome Project. The Project’s com-pletion of the sequence of the human genome has been guidingthe study of the genetic variations implicated in human dis-ease. The quest for the schizophrenia gene is exciting news forpsychiatric–mental health nurses. On the other hand, Josephand Leo (2006) make a strong argument that much of what wehave assumed is genetic can also be explained by environmen-tal factors. The risk of susceptibility may remain the same, butthe notion that there is one specific schizophrenia gene mayhave weaker support than previously thought.
In fact, it is becoming obvious that a single gene is notresponsible for schizophrenia (Paz et al., 2006; Riley &Kendler, 2006). This illness resists easy genetic codificationdue to its complexity and its variety of forms. It has beensuggested that schizophrenia may be a collection of disordersrather than a single disease entity. The current front-runneramong possible susceptibility genes for schizophrenia isneuregulin 1 (NRG1), a very complex gene (Harrison &Law, 2006). It has six known types but only two may be rele-vant to schizophrenia.
Research examining the occurrence of schizophrenia intwins indicates that both environmental and genetic factors areimportant. Rates of concordance (in which both twins either ex-press or do not express the trait) for schizophrenia are consis-tently higher for monozygotic twins than for dizygotic twins.
Interestingly, monozygotic, or identical, twins need not bothhave schizophrenia, but the chance of both twins having schizo-phrenia is 25% to 39%. This finding supports the hypothesis ofsome level of genetic transmission. The fact that both twins are not always affected when they are genetically identical,however, indicates that environment plays a large part in the ex-pression of the illness. If the disease were solely genetically de-termined, the concordance rates in this group would be close to100%. (See also pages 000–000 in Chapter 6 for anotherdiscussion of genetics in schizophrenia.)
Brain Structure AbnormalitiesAs a group, people with schizophrenia differ in their brainstructure from people who do not have schizophrenia. Peoplewith chronic schizophrenia show changes to their frontotem-poral cortical gray matter, among other areas. Magnetic reso-nance imaging (MRI) studies show hippocampal structuraldifferences between people who have schizophrenia andthose who do not. When the hippocampus is formed, brain-derived neurotrophic factor (BDNF) is involved. Checkingfor abnormalities in BDNF may be able to tell us who is atrisk for developing schizophrenia (Szeszko et al., 2005).
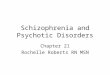
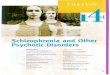
Altered brain structures may be genetically based andcould represent a marker of vulnerability to schizophrenia thatprecedes any other symptomatology. How the brain structureabnormalities influence the progress of the disease is not wellunderstood and requires further study. An example of PETscan differences between identical twins where one has schiz-ophrenia and the other is unaffected is seen in FIGURE 16-2 ■ .
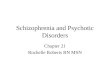
Biochemical TheoriesThe biochemical basis of schizophrenia is captured in thedopamine hypothesis, which states that schizophrenic symp-toms may be related to overactive neuronal activity that isdependent on dopamine (DA). In other words, positive psychoticsymptoms are associated with excessive DA transmission.
The hypothesis was supported by numerousstudies demonstrating that DA blockers, which aremedications that decrease DA activity, alleviatesymptoms. The traditional antipsychotic medications wereshown to be effective because of their ability to antagonizeDA receptors; however, this causes undesirable side effectssuch as extrapyramidal symptoms. The relief of positivesymptoms with these traditional agents was not complete, andthe negative symptoms of the disorder were much less re-sponsive to DA blockers. See FIGURE 16-3 ■ for a graphic rep-resentation of this concept.
Research suggests that the relationships between DA ac-tivity and schizophrenic symptoms are much more complexthan originally hypothesized. It is now known that there aremultiple types of DA receptors, and different types of recep-tors are concentrated in different regions of the brain. Anotherfeature of this theory is catechol-O-methyltransferase(COMT), a catecholamine-metabolizing enzyme involved indopamine flux and the dopaminergic regulation problems seenin schizophrenia (Tunbridge, Weinberger, & Harrison, 2006;Meyer-Lindenberg et al., 2006). The regulation of DA activity
Chapter 16 • Schizophrenia and Other Psychotic Disorders 11
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 11

continues to be thoroughly studied, as DA dysregulation fromevery source is recognized as being inherently involved in thepathology of schizophrenia (Eastwood & Harrison, 2006).
Further evidence that supports a biochemicaltheory is the physical impact that atypical antipsy-chotic agents have on clients with schizophrenia(Kelly et al., 2006; Kelly & Conley, 2006). These medica-tions block DA as well as serotonin. This may help lessen ex-trapyramidal side effects such as dystonia and akathisia(uncomfortable or painful side effects, explained in detail inChapter 32 ), and may be the reason they are so useful inreducing negative symptoms.
Psychological TheoriesMost psychological theories focus on the processing of infor-mation as well as attention and arousal states in schizophrenia.
Information ProcessingMany clients with schizophrenia have information-processingdeficits. Two central types of information processing havebeen identified:
1. Automatic processing2. Controlled or effortful processing
Automatic processing occurs when you take informationin unintentionally. Automatic processing can occur withoutyour being aware of it and does not interfere with consciousthought processes that occur at the same time. An example ofautomatic information processing is being aware of the phys-ical features of a new environment, such as a room beinglarge and spacious as opposed to small and confined.
People with schizophrenia are deficient in controlled in-formation processing (Lee, Lee, Lee, & Kim, 2007; Nicode-
12 Unit IV • CLIENTS WITH MENTAL DISORDERS
FIGURE16-2 ■ Schizophrenia scans. PET scans of discordant monozygotic twins taken during a test to provoke activity and measure regionalcerebral blood flow. (A) Arrows indicate areas of normal blood flow and brain activity in the unaffected twin. (B) Arrows indicate areas of lowerblood flow and brain activity in the twin with schizophrenia.
Source: Courtesy of Dr. Karen F. Berman, Clinical Brain Disorders Branch, National Institute of Mental Health.
FIGURE16-3 ■ The dopamine hypothesis of schizophrenia holds that the amount of dopamine in various areas of the brain creates the vari-ous symptoms of the disease. Note how too much dopamine in the mesolimbic area (the middle of the limbic system) is thought to causepsychosis, while too little dopamine in the mesocortical area (the middle of the cortex of the brain) is thought to cause the negative symp-toms of schizophrenia.
A B
MED
IALI
NK
Extr
apyr
amid
al S
ide
Effe
cts
Vide
os
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 12

Chapter 16 • Schizophrenia and Other Psychotic Disorders 13
mus et al., 2006). Their ability to perform directed, conscious,sequential thinking—for example, making comparisonsbetween two stimuli or organizing a set of stimuli—is consis-tently inferior to that of people who do not have schizophre-nia. Someone with schizophrenia would not easily be able toperform the series of steps necessary to organize a classroomdebate. Any level of cognitive dysfunction creates ripple ef-fects in treatment and quality of life. See the Rx Communica-tion feature for an example of an interaction with a client whois unfocused and having a problem processing information.
We do not know whether the inability of a person withschizophrenia to sustain conscious, directed thought is theprimary problem or the result of a primary deficit in auto-matic thinking. If the primary deficit is in automatic pro-cesses, then the person is forced to complete automatic tasksat the conscious level, inhibiting and slowing controlled in-formation processing. There is research support for the pres-ence of attention and cognitive impairments (Donohoe et al.,2006) and the presence of negative impacts on working mem-ory in the current literature. Sufficient evidence to resolvethis question is not yet available.
Attention and ArousalAttention and arousal are measured by physiologic states andalterations, such as galvanic skin response, heart rate, bloodpressure, skin temperature, and pupillary response. Physio-logic studies of attention and arousal in clients with schizo-phrenia show promise in identifying clinically significantsubgroups.
One subgroup of clients exhibits abnormally low re-sponse levels to novel, or different, stimuli. This finding sug-gests that these clients are less adept than healthy people atattending to and responding to novel situations. An exampleof this state can be seen when a client with schizophreniadoes not register that a ball is being thrown at him during agame of catch. The ball may even strike him, drop to theground, and roll away before the client looks at it.
A second group of clients with schizophrenia demon-strates a state of hyperarousal evidenced by elevated electro-dermal activity, heart rate, and blood pressure. Hyperarousalhas been noted during both symptomatic and nonsympto-matic periods. These clients demonstrate symptoms of irritability, excitement, and anxiety rather than apathy and
withdrawal. An example of this state occurs when a clientwith schizophrenia angrily and loudly criticizes someone forusing incorrect grammar in a sentence.
Family TheoriesNumerous theories implicating family interaction alone as acause of schizophrenia have been proposed and unsupported.Research has failed to support the theory that dysfunctionalfamily interaction alone causes the illness.
Suggestions have been supported that disordered familycommunication (the inability to focus on and clearly share anobservation or thought) causes schizophrenia only in thepresence of a genetic predisposition to the disease. For exam-ple, the communication taking place at the dinner table maybe chaotic and constant. No one finishes a sentence and noth-ing is discussed to its logical conclusion. Living with this pat-tern of family communication during early development isthought to impair the ability of the person with schizophreniato perceive the environment and communicate with othersabout it. People with schizophrenia are more likely to showsymptoms of thought disorder when they are raised by peoplewho have dysfunctional communication.
Individuals with schizophrenia who are raised by adop-tive parents, who themselves showed elevated levels ofcommunication deviance, demonstrate as much thought dis-order as those raised in birth families. In contrast, adopteeswho were raised by adoptive parents with more functionalcommunication were less likely to show thought disorder. Inone study, this pattern was not evident in control adoptees—there was no discernible relationship between thought disor-der in the adoptees and communication deviance in theadoptive parents. In other words, these findings did not de-tect the presence of a “schizophrenogenic” environment forindividuals without a preexisting genetic liability. These ex-amples support the view that genetic factors alone do notexplain the development of schizophrenia, and that interac-tions with the environment are important. Individuals wholive in aversive environments tend to have higher rates ofschizophrenia, suggesting there may be a neighbor-hood and social context to development of the dis-ease (Allardyce & Boydell, 2006).
A second theory is that the family’s emotional tone caninfluence the course of schizophrenia over time. Researchers
RX COMMUNICATION
UNFOCUSED CLIENTCLIENT: “I went to the ballgame and I had great seats and I saw the whole game and I saw all the home runs and all the hits and all thestrikeouts and I saw the pitcher throw all the pitches, fast ball, curve ball, change up, and . . .“
NURSE RESPONSE 1: “Keith, tell me about this more slowly so Ican keep up with you.”
RATIONALE: This response is structured to be brief, focused, and todirect the client’s attention to the speed with which he speaks.
NURSE RESPONSE 2: “How about if I ask you some questionsabout the game? If you give me a chance to ask questions I’ll havea better idea of what you saw.”
RATIONALE: This response defines the special skills required for aconversation.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 13

14 Unit IV • CLIENTS WITH MENTAL DISORDERS
found that individuals with schizophrenia from families whoare highly critical, hostile, overprotective, or overinvolvedtend to relapse more often. Families exhibiting such charac-teristics have been described as having high expressed emo-tion (EE). There is some evidence that family expressedemotion, life events, and biological factors combine with theindividual’s genetic liability to the disorder to cause schizo-phrenia. In other words, the disorder is responsive to psy-chosocial attributes such as the emotional climate of thefamily (Kymalainen, Weisman, Rosales, & Armesto, 2006).Recent research on schizophrenia can be found on the Na-tional Alliance for Research on Schizophrenia and Depres-sion website at www.mhsource.com/narsad/ and through adirect link on the Companion Website for this book.
Humanistic–Interactional TheoriesAn interactional model of schizophrenia integrates many ofthe biologic and psychosocial theories already discussed. Inthis view, schizophrenia is due to the interaction of a ge-netic predisposition or biologic vulnerability, stress orchange in the environment, and the individual’s socialskills and supports. In an interactional model, the influ-ences are multidimensional. A biologic vulnerability mayinhibit the individual’s capacity to cope with even minorstressors such as the loss of a primary source of support.Similarly, the symptoms of schizophrenia may worsenupon entering an environment that demands coping skillsthe person with schizophrenia may not have developed.
A precursor to present-day interactional theories is theenduring interpersonal-psychiatric theory of Harry Stack Sul-livan (discussed in detail in Chapter 5 ). Sullivan, a psy-chiatrist, emphasized modes of interaction and the role ofanxiety as the real focus of psychiatric inquiry in his workwith people with schizophrenia. Hildegard Peplau (known asthe “mother” of psychiatric nursing) based her interpersonalpsychiatric nursing approach on the work of Sullivan. How-ever, Peplau had more to say than Sullivan about the socialand cultural conditions that influence behavior. The ideas ofSullivan and Peplau continue to influence our practice withclients who are schizophrenic.
Stress–Vulnerability ModelAn interactional model for understanding schizophrenia thathas received wide acceptance is the stress–vulnerabilitymodel, which suggests that people with schizophrenia have agenetically based, biologically mediated vulnerability to per-sonal, family, and environmental stress. In this model, riskfactors and protective factors interact in any of three ways:
1. Stressors, risk, and vulnerability factors combineand potentiate each other.
2. As long as stress is not excessive, it enhancescompetence.
3. Protective factors modulate or buffer the impact ofstressors by improving coping and adaptation.
People with schizophrenia have a potentially increasedvulnerability to stress. High-EE relatives may cause them
great stress, resulting in an exacerbation of symptoms and/ora relapse. It is now almost standard practice to aim to reducehigh EE and criticism in the family system of persons withschizophrenia. However, as one study indicates, while somefamilies are identified by researchers as having a criticalhome environment, the clients themselves do not necessarilyperceive their relatives as critical (Weisman, Rosales, Ky-malainen, & Armesto, 2006).
As we know, the stressors a client with schizophreniaexperiences can overwhelm the resources available, andsymptoms result. Psychobiologic stressors include the stressof living with schizophrenia itself. Altered attention and per-ception, as well as problems with motivation and energy, cre-ate stresses for people with schizophrenia. Environmental andinterpersonal stressors include those we all encounter; how-ever, a person with schizophrenia is particularly sensitive tothem. These include stressful life events, environments thatare highly demanding or stimulating, and family or living en-vironments that are highly negative.
It is not unusual for clients to make statements that pointto the validity of the stress–vulnerability concept, especiallythe protective qualities. One client said, “I’m not saying it[referring to an antipsychotic medication] is a perfect solu-tion. It’s not. There are painful side effects. But I know I cancount on it when the going gets rough. If things get stressful itwill help me through it.” A second client said: “I feel raw in-side and out when I’m off it [referring to an antipsychoticmedication]. Everything bothers me. So it cushions the blowsthat are my life.”
Resources That Moderate StressResources that can moderate stress (and are thought to affectthe development of symptoms in schizophrenia) include:
■ Skill in symptom recognition and management■ Social support■ Antipsychotic medication
The capacities to self-monitor the waxing and waningof schizophrenia and to develop coping strategies to influ-ence symptoms at the first sign of trouble show promise ininfluencing the longer-term course of the illness. An exam-ple of how you can help a client to self-monitor symptomsand develop coping strategies is in the Evidence-BasedPractice feature that follows. This capacity to detect prodro-mal symptoms and acute symptoms and institute self-carebefore completely decompensating is a resource that maywork to mediate the stress that occurs in the person, family,or environment.
Social support has proven helpful in moderating stressfor general populations and for people with schizophrenia inparticular. Supportive others who provide empathy, interper-sonal contact, financial aid, problem solving, and other formsof support help to mitigate the difficulties of schizophrenia(Montgomery, Tompkins, Forchuk, & French, 2006). Finally,antipsychotic medications moderate some, and some-times most, symptoms of the disease, and thus someof the stressors induced by the disease.
MED
IALI
NK
Nat
iona
l Alli
ance
for
Rese
arch
on
Schi
zop
hren
ia a
nd D
epre
ssio
n
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 14

Chapter 16 • Schizophrenia and Other Psychotic Disorders 15
ceptual changes are sufficient to cause the client to mistakethe stimulus for something else (see the example of an illu-sion in Figure 10-1 on page 000). Hallucinations are the mostextreme and yet the most common perceptual disturbance inschizophrenia. Auditory hallucinations are the most commonform of hallucination. Although hallucinations are a hallmarkof schizophrenia, their presence alone does not establish thepresence of the disorder. Refer back to Table 16-1 on page 4,which lists various types of hallucinations.
Assess perceptual disturbances by asking the clientabout the experience and by observing for behaviors that in-dicate the client is frightened or attending to internal stimuli.Ask the client, “What are you seeing and hearing?” Note thedegree to which this description differs from your perceptionsof the environment.
Clients may be reluctant to discuss the extreme percep-tual disturbance of hallucinations. One of the ways you canintroduce the topic is to discuss physical symptoms such aspain or discomfort. Then ask about hearing and vision skills.From there it is a smooth transition to asking about unusualexperiences with hearing and seeing.
A classic sign of auditory hallucinations is placing thehands over the ears when clients are frightened by the voicesand attempt to block them out. Less obvious signs of halluci-nations are inappropriate laughing or smiling, difficulty fol-lowing a conversation, and difficulty attending to what ishappening at the moment. Fleeting, rapid changes of expres-sion that are not precipitated by events in the real world canbe another sign. The degree to which clients believe the hallu-cinatory experience is real and their ability to verify the real-ity of the experience by checking with others have importantimplications for interventions. Note the client’s emotional re-sponse to hallucinations. Some clients experience depressionor despair about the continued presence of voices; others maybe comforted or kept company by their voices. Client coping
EVIDENCE-BASED PRACTICE
ASSESSING THE PARENTING SKILLS OF A CLIENT WITH SCHIZOPHRENIA
Jane is a 33-year-old female, mother of two small children, whohas paranoid schizophrenia. She is one of the people with whomyou work in an outpatient clinic for moderately ill people whohave schizophrenia. Your education and experience have taughtyou that schizophrenia is a complex illness that requires more thanjust medications to address it adequately.
Jane typically hides her illness from her children. She wants toprotect them from the stress and stigma of a mentally ill mother,and she wants her role as mother to be unsullied by illness andincapacitation. In order to achieve this, she watches what she saysand masks her troubles. Jane has appointments at the clinic onlywhen her children are otherwise occupied. They do not know she
is in therapy or takes medications. What happens as a result is thatJane gets very symptomatic from the stress of pretending she isnot ill.
This situation suggests the need to be sensitive to mothers whohave a serious mental illness. Carefully and accurately assess andreassess the mothering skills needed to make sure the children arenurtured, their relationship is healthy, and the mother receives thecare she needs. Action should be based on more than one study,but the following is a study that would be helpful in this situation.
Montgomery, P., Tompkins, C., Forchuk, C. & French, S.(2006). Keeping close: Mothering with serious mental illness.Journal of Advanced Nursing 54(1), 20–28.
CRITICAL THINKING APPLICATION1. Is it possible for Jane to truly hide her illness from her children?2. How will you know if Jane’s relationship with her children is a nurturing one?
NURSING PROCESS Clients with Schizophrenia
Schizophrenia is a difficult and chronic illness requiring un-derstanding and competent care in every facet of the client’slife. In addition to the discussion that follows, a nursing careplan for the client with schizophrenia is presented at the endof the chapter.
AssessmentAssessing clients who have schizophrenia occurs at individ-ual, family, and environmental levels. Be aware of the client’sstatus and of changes in the client’s personal life, family situ-ation, and environment in order to plan care and intervene ef-fectively. In addition, care that addresses multiple levels ofthe client’s life is consistent with the interactional theory ofschizophrenia because it is assumed that changes in any as-pect of the client’s environment influence all other aspects ofthe personal environmental balance.
Subjective DataThese data describe the client’s inner experience of schizo-phrenia.
Perceptual Changes The perceptions of clients with schizo-phrenia may be either heightened or blunted. These changesmay occur in all the senses or in just one or two. For example,a client may see colors as brighter than normal or may beacutely sensitive to sounds. Another may have a heightenedsense of touch and therefore be extremely sensitive to anyphysical contact. Illusions occur when the client misper-ceives or exaggerates stimuli in the external environment. Aclient with schizophrenia may mistake a chair for a person orperceive that the walls of a hallway are closing in. The per-
MED
IALIN
KLearning from
Clients: Schizop
hrenia Video
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 15

16 Unit IV • CLIENTS WITH MENTAL DISORDERS
strategies, and their effectiveness or ineffectiveness, are alsoan important aspect of assessment. Finally, clients may talk tothemselves, presumably in answer to the voices they hear.Specific guidelines for assessing hallucinations are given inthe Your Assessment Approach feature.
Objective DataThese data are the observable symptoms and manifestationsof schizophrenia that you, as a nurse, will assess.
Disturbances in Thought and Expression Clients with schizo-phrenia find that their thinking is muddled or unclear. Theirthoughts are disconnected or disjointed, and the connectionsbetween one thought and another are vague.
The clarity of the client’s communication often reflectsthe level of thought disorganization. Client responses may besimply inappropriate to the situation or conversation. Theymay have difficulty responding or stop in midsentence, as ifthey are stuck, a sign of thought blocking.
Note the rate and quality of the client’s speech. Is it un-usually loud, insistent, and continuous? Does the client wan-der from topic to topic or have tangential communication(communication with only a slight or tenuous connection tothe topic)? An example is, “You want to know how I camehere? I came here by bus, but bussing is kissing, I wasn’tkissing but if you keep it simple that is a business tenet forKISS. That was a great group that played on and on but I’mnot playing with you.” Does the client bring up minute detailsthat are irrelevant or unimportant to the topic at hand(circumstantial communication)? An example is, “You wantto know how I came here? I came here on a blue and yellow
bus with a lady bus driver. There were three teenage kids anda blind man with a seeing-eye dog on the bus. It didn’t haveto make a stop at the corner of Main and 9th.” Are the client’sresponses slow and hesitant, reflecting difficulty in taking instimuli and responding to them?
Clients with schizophrenia also have difficulty thinkingabstractly. Their responses may be inappropriate because theyinterpret words literally rather than abstractly. For example,when told to prepare to have his blood drawn, a young manreadied some paper and marking pens. You can assess abstractthinking by asking clients the meaning of proverbs, a test re-quiring the client to abstract a general meaning from a specificor metaphysical statement, for example, “People who live inglass houses shouldn’t throw stones.” Clients with schizophre-nia are more likely to give concrete (“If you throw a stone theglass will break”) rather than abstract (“Don’t criticize some-one else if you behave the same way”) responses.
Disruptions in Emotional Responses Tone of voice, rate ofspeech, content of speech, expressions, postures, and bodymovements indicate emotional tone. Many individuals withschizophrenia demonstrate inappropriate affect—emotionalresponses that are inappropriate to the situation. For exam-ple, a client may smile or laugh while relating a history ofhaving been abused as a child. Or, a client may becomeangry or anxious when asked to join a group of other clientsfor dinner. The degree to which a client’s emotions are inap-propriate is a prognostic indicator. Clients whose emotionalresponse is preserved and generally appropriate have a morefavorable prognosis than clients who demonstrate inappro-priate affect.
A marked decrease in the variation or intensity of emo-tional expression is called blunted affect. The client may ex-press joy, sorrow, or anger, but with little intensity. In flataffect, there is a total lack of emotional expression in verbaland nonverbal behavior; the face is impassive, and voice rateand tone are regular and monotonous. The absence of emo-tion and the presence of anhedonia are also often indicative ofschizophrenia.
Motor Behavior Changes Disruptions seen in schizophrenia in-clude disorganized behavior and catatonia. Disorganized behav-ior lacks a coherent goal, is aimless, or is disruptive. Catatonicbehavior is manifested by unusual body movement or lack ofmovement. This activity disturbance includes catatonic excite-ment (the client moves excitedly but not in response to environ-mental influences), catatonic posturing (the client holds bizarrepostures for periods of time), and stupor (the client holds thebody still and is unresponsive to the environment).
Changes in Role Functioning An important factor in predictingthe course of schizophrenia is the client’s level of functioningbefore the symptoms of the disease became pronounced. As-sessment should therefore include a complete history of theclient’s success at completing developmental tasks. The prog-nosis is best if the client functioned at a high level prior to theonset of schizophrenic disturbance. Assess how well the clientfulfilled role responsibilities in the family, in school, in relation
A complete assessment of hallucinations should identify thefollowing:
■ Whether the hallucinations are solely auditory or includeother senses
■ How long the client has experienced the hallucinations, whatthe initial hallucinations were like, and whether they havechanged
■ Which situations are most likely to trigger hallucinations, andwhich times of day they occur most frequently
■ What the hallucinations are about (Are they just sounds, orvoices? If the client hears voices, what do they say?)
■ How strongly the client believes in the reality of thehallucinations
■ Whether the hallucinations command the client to dosomething, and if so, how potentially destructive thecommands are
■ Whether the client hears other voices contradictingcommands received in hallucinations
■ How the client feels about the hallucinations■ Which strategies the client has used to cope with the
hallucinations and how effective the strategies were
YOUR ASSESSMENT APPROACHHallucinating Client
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 16

Chapter 16 • Schizophrenia and Other Psychotic Disorders 17
to peers, and in work. Obtain a history of the rate of decline inthese various roles. The onset of schizophrenia may be rela-tively acute, or degeneration may be slow.
Drug Use Clients with drug toxicity or withdrawal may havebehavior disturbances similar to those seen in clients withschizophrenia. They may have auditory or visual hallucina-tions and may be confused, illogical, and highly anxious. Forthis reason, it is essential to obtain a detailed drug history. As-sess both long-term and recent use of chemical substances. Ifthe client is not a reliable historian, interview family orfriends. In addition, both blood and urine should be tested fordrugs if reliable information cannot be obtained.
Family Health History Part of a thorough and complete assess-ment is noting any history of mental disorder in the client’sfamily (Chafetz, White, Collins-Bride, Nickens, & Cooper,2006). Of particular interest is a history of schizophrenia or anythought disorder, mood disorders (such as cyclical highs or de-pressions), or alcoholism in any family member. Note any re-port that family members had “nervous breakdowns” or anyother colloquial descriptions of mental or emotional disorders.
Family Cohesion and Emotion In families of people withschizophrenia, enmeshment (see Chapter 30 ), combinedwith a negative emotional tone, is thought to be detrimentalto the ill member’s well-being. However, the presence of ac-quaintances and family members showing emotional warmthin low expressed emotion (EE) situations can have a protec-tive function.
Much of the nursing assessment of family cohesion andemotion can be carried out unobtrusively. Chapter 30 hasspecific guidelines for assessment of these and other familydynamics. The nursing staff, in conjunction with the interdis-ciplinary team, can also arrange formal family assessment interviews (also discussed in Chapter 30 ). When you areobserving interactions, note signs of dysfunction.
Family Overinvolvement and Negativity At present there areno clear-cut clinical determinants of exactly how much over-involvement and negative emotion in families is problematic.Note families who seem excessively bonded emotionally. Theinability of family members to maintain emotional, social, orphysical separateness is a clear sign of this problem. Also as-sess for the presence of a high level of criticism among fam-ily members. Discuss families that seem seriously enmeshedor hypercritical with the treatment team.
Family Communication Problems Unclear or incompletecommunication is frequent in families of people with schizo-phrenia. This area requires nursing assessment. Unclear com-munication may result from continual interaction with the illmember or may contribute to the disorder. Clinicians mustevaluate how effectively the family communicates to deter-mine the potential need for intervention.
Assess these aspects of family communication:
■ Ability to focus on a topic■ Ability to discuss a topic in a meaningful way with
other family members
■ Ability to maintain the discussion without wanderingfrom the subject or becoming distracted
■ Use of language and explanations that are generallyunderstandable (not peculiar to that family alone)
Also note who in the family seems to do the talking,who talks to whom, and whether members talk for, or inter-rupt, one another. Communication problems that commonlyoccur with the diagnosis of schizophrenia and interfere withinterpersonal relationships, especially family communication,are discussed in Box 16-1.
Family Burden Most families of individuals with schizophre-nia report that caring for the ill member places a burden onthe family unit. Ask about the challenges the family is facingso that you can determine the information and support needsto be met. See Chapter 30 for examples of common fam-ily burdens.
Environment Assess the availability of support and servicesbeyond the bounds of the family, including extended familyand friends, as well as community groups and organizationsthat support people with schizophrenia. Assess also the avail-ability of mental health programs that address the specificmental health needs of people with schizophrenia.
Nursing Diagnosis: NANDANursing diagnoses with clients with schizophrenia focus on al-terations in the patterns of activity, cognition, emotionalprocesses, interpersonal processes, and perception. Alterations
BOX 16-1 Problematic Communication PatternsCommon in Schizophrenia
BlockingThe client has trouble expressing a response or stops inmidsentence, as if stranded without a thought.
Clang AssociationsWords that rhyme or sound alike are distributed throughoutconversations without necessarily making sense.
EcholaliaPhrases, sentences, or entire conversations said to the client arerepeated back by the client.
NeologismsWords or meanings are invented by the client. This can includemultisyllabic, pseudo-scientific words or simple words.
PerseverationThe client maintains a particular idea regardless of the topicbeing discussed or attempts to change the subject.
Word SaladAn incoherent medley of words is emitted in conversation as ifit was a sensible and articulate phrase.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 17

18 Unit IV • CLIENTS WITH MENTAL DISORDERS
and inactivity. Inactivity induced by ambivalence is associ-ated with higher levels of emotion. Anxious about choosingone course of action and rejecting another, the client is immo-bilized. The following clinical examples describe the experi-ence of intolerance to activity.
CLINICAL EXAMPLEJim is ambivalent about taking a pass to go out alone from theinpatient unit for the first time. He is undecided about takingthe risk of leaving the hospital setting without a staff member,yet yearns for the freedom of walking the streets alone. Indeci-sion leaves him standing, immobilized, by the doorway to theunit.
Extreme ambivalence can manifest itself in even themost automatic of behaviors.
CLINICAL EXAMPLEMelissa cannot eat because of ambivalence about where to sitor what to eat. She stands in the center of the dining room,turning first to one chair and then another, unable to choosewhere to sit so that she can begin eating.
Clients who are inactive because of apathy demonstratelittle emotional tone. Such clients may spend long hours lyingin bed staring into space or listening to music. Often, but notalways, apathetic individuals prefer isolation. You might findseveral clients sitting in the same room, engaged in no appar-ent activities, and interacting with one another only when ab-solutely necessary.
Social IsolationExtreme anxiety about relating to others often leads clientswith schizophrenia to withdraw from interaction and to iso-late themselves. Some clients tolerate only a few moments ofdirect communication, whereas others can manage extendedperiods of contact. Assess the client’s tolerance of brief peri-ods of contact with staff and other clients. Document patternsof relating and withdrawal, also noting in which activities theclient engages when in contact with others and which activi-ties the client undertakes when alone. Nurses who work inskilled nursing facilities also need to be able to diagnose so-cial isolation as a symptom of schizophrenia (see the WhatEvery Skilled Facility Nurse Should Know feature).
Decisional ConflictDecisional conflict in schizophrenia is probably due to bio-chemical alterations in the brain that make it difficult forclients to take in, synthesize, and respond to information. De-cisional conflict may be evident both in the mundane activitiesof daily life (e.g., selecting one’s diet) and in major life deci-sions. This can be frustrating for caregivers and for clients.The following clinical example shows how decisional conflictcan remove what is a pleasant aspect of life from the client.
in ecologic, physiologic, and valuation processes are assessedas well; however, the central nursing problems relate to theformer five processes.
Impaired CommunicationSchizophrenia interferes with the ability to communicate, acomplex and demanding function.
Verbal Clients with schizophrenia may communicate in a disorganized, sometimes incomprehensible fashion. Someclients, because their thinking is disorganized, speak very lit-tle (alogia, or poverty of speech). Also note there may be apoverty of content in speech, in that the client converses butactually says very little.
Often, clients with schizophrenia communicate in waysthat are overly concrete (a sign of an inability to think andcommunicate abstractly) or overly symbolic (a sign of preoc-cupation with unreal or delusional material). The symbols areusually difficult to decipher because their meanings are idio-syncratic to that particular individual.
Nonverbal The facial and bodily expressions that accompanythe verbal communication of people with schizophrenia fre-quently do not match the content of the verbal message. Thislack of congruence is primarily due to the blunting of emotionsfound in schizophrenia. Expected facial expressions—smiles,looks of concern or disgust—may not accompany the client’sstatements. In addition, clients with motor or behavioral ab-normalities—posturing, unusual movements, or grimacing—convey a confusing mix of verbal and nonverbal messages.
Self-Care DeficitsPeople with schizophrenia frequently appear indifferent totheir personal appearance. They may neglect to bathe, changeclothes, or attend to minor grooming tasks such as combingtheir hair. Some show little awareness of current fashion styles,and many wear clothing that makes them look out of place. Ofgreater concern are those who wear clothing that is inappropri-ate to the current season and weather conditions.
Although lack of attention to grooming might be a sim-ple annoyance to those who must live in close proximity tothe person with schizophrenia, health risks related to pro-longed poor hygiene can arise. Assess immediate problems,such as inadequate nutrition, fluid intake, and elimination, aswell as long-term problems, such as dental caries and in-creased susceptibility to infections.
Disregard for appearance and hygiene may extend to theclient’s environment. The client may fail to maintain a cleanand safe living space. He or she may not take good care ofpersonal belongings and may misplace them. Self-care defi-ciencies may result from consistently disturbed thought andperceptual processes. For example, a client whose chronichallucinations are only partly relieved by medication mayhave difficulty concentrating for long periods and paying at-tention to grooming.
Activity IntoleranceThe emotional disturbances of ambivalence and apathy, com-mon in schizophrenic disorders, can result in lack of interest
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 18

Chapter 16 • Schizophrenia and Other Psychotic Disorders 19
CLINICAL EXAMPLEMurray refuses to take medications, even though not takingthem means that he will be evicted from the residential treat-ment program he likes.
Disturbed Sensory PerceptionAlterations in the five senses (sound, sight, smell, taste,touch) create an altered perception of the world.
Hallucinations Hallucinations are both a clinical diagnosticsign of schizophrenia and a focus for nursing care. You need toknow the extent and nature of clients’ hallucinations so thatyou can document the hallucinatory experience. Discuss withthe client, if the client is able to, the details of his or her symp-toms. Look for major themes in the content of the hallucina-tions, particularly whether the hallucinations command theclient to take action. Command hallucinations such as “Jumpup and down. Jump up and down. Don’t look at her, she hascancer and you’ll catch it,” can be difficult for the client tocope with and can affect the client’s behavior. The client maynot be able to withstand pressured commands to say things orperform acts that could include violence or a refusal to remainin a housing situation (which could lead to homelessness).
Illusions Illusions make the client vulnerable to emotionaland physical injury. The level of misperception may varyfrom day to day and even throughout the day. Misperceptionsof the social environment make the client vulnerable to inap-propriate responses that may be ridiculed by others. Misper-ceptions of the physical environment, such as misjudging thespeed of an oncoming car, may lead to physical harm.
Disturbed Body ImageA body image disturbance is common in people with schizo-phrenia. Clients may lose the sense of where their bodiesleave off and where inanimate objects begin. They may be-come dissociated from various body parts and believe, for ex-ample, that their arms and legs belong to someone else. Theymay worry about the normalcy of their sexual organs. Clientsoften verbalize this altered sense of self directly, saying “Idon’t feel like myself” or “I feel like I am looking at my bodyfrom somewhere else in the room.”
Excess Fluid VolumeExcess fluid intake, or water intoxication, is a problem that isobserved primarily in clients who reside in institutions suchas state mental hospitals. This physiologic state is brought on by excessive drinking, characterized by hyponatremia,confusion, and disorientation, and progresses to apathy andlethargy. In severe cases, seizures and death may result. Thisbehavior can lead to irreversible brain damage. Polydipsia ap-pears to be significantly associated with male gender, smok-ing, celibacy, and psychiatric chronicity. Polydipsia inschizophrenia has been treated effectively with clozapine(Margetic, Aukst-Margetic, & Zarkovic-Palijan, 2006). Forclients suspected to be at risk because of frequent drinking,preventive measures include regular measures of urine spe-cific gravity, and regular weights designed to screen for in-creases in the body’s fluid volume.
Disturbed Thought ProcessesSchizophrenia changes the way thoughts are processed bydistorting logic and organization.
Delusions Clients express delusional thinking in direct interac-tions and, to a lesser extent, through behaviors. When asked,many clients willingly describe their delusional beliefs in de-tail. They seldom withhold this information because they be-lieve firmly in the validity of the delusion, no matter howbizarre it seems to others. Clients’ actions reflect the fixednessof their beliefs.
CLINICAL EXAMPLEGerry has the somatic delusion that her body is riddled withholes. She flatly refuses to drink, convinced that the fluid willflow directly out of the holes and soil her dress.
The content of delusions varies: delusions of persecu-tion, reference, and so on (see Table 16-3). Reality-baseddelusions may seem plausible because they could, undersome circumstances, actually occur. Bizarre delusions, morecommon among clients with schizophrenia, have no possiblebasis in reality. On the other hand, the false belief that one’shusband is having an affair with a neighbor has a possiblebasis in reality, and is called a reality-based delusion. In con-trast, the belief that one’s thoughts are directed by a televisionannouncer, or that one’s unspoken thoughts can be heard byothers, are known as bizarre delusions.
WHAT EVERY SKILLED NURSINGFACILITY NURSE SHOULD KNOW
A skilled nursing facility (SNF) nurse needs to befamiliar with the primary symptoms of schizophrenia—
delusions, hallucinations, agitation, and general decompensation.There are two reasons SNF nurses should be familiar with thesesymptoms:
1. These symptoms are part of a disease process that requiretreatment.
2. The presence of these symptoms can distort or mask thepresentation of symptoms of physical illnesses, and severepsychiatric distress can impair healing from medical andsurgical procedures and injuries.
When an SNF resident represents symptoms that appear to in-clude behavioral and psychiatric features, the SNF nurse shouldbe prepared and able to document, classify, and report thesesymptoms correctly, and to help ensure the resident receivesnecessary treatment. Knowing the interventions, pharmacologi-cal and nonpharmacological, can speed stabilization and im-prove the quality of life your residents’ experience.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 19

20 Unit IV • CLIENTS WITH MENTAL DISORDERS
Delusions often reflect the client’s fears, particularly aboutpersonal inadequacies. For example, a man’s grandiose delusionthat he is the mayor of New York City could be a defenseagainst feelings of inferiority. Similarly, persecutory delusionsdefend against the person’s own feelings of aggression. Aggres-sive feelings are projected onto a person or organization—forexample, the police, whom the client then fears.
Magical Thinking Magical thinking is the belief that eventscan happen simply because one wishes them to. Some peoplewith schizophrenia claim they can exert their will to make peo-ple take certain actions or make specific events occur, like win-ning the lottery.
Thought Insertion, Withdrawal, and Broadcasting Hallmarksof schizophrenic thought are the beliefs that others can putideas into one’s head (thought insertion) or take thoughts outof one’s head (thought withdrawal). In addition, some clientsbelieve that their thoughts are transmitted to others via radio,television, or other means but not directly by the client. Thisbelief is known as thought broadcasting.
Dysfunctional Family ProcessesWhen a family has a member with a significant illness, regard-less of whether it is a mental or physical illness, that family’sfunctioning and dynamics change. The operations of the familymust change to accommodate the ill family member as well ashow the rest of the family deals with the illness. The symptomsof the illness may be alien to family members, and they maynot know how they should respond. See the Partnering withClients and Families feature for guidelines on how to teachfamilies about the negative symptoms of schizophrenia.
Interrupted Family ProcessesFamilies burdened with the long-term responsibility of caringfor a relative with schizophrenia may suffer disruptions in
their household routine, work, social interactions, and physi-cal well-being. The household may be disrupted by theclient’s insistence that the family act on and accommodatedelusional beliefs. The family may bend to the client’s wish,fearing an increase in the client’s anxiety and possible fight-ing or shouting if they do not comply.
CLINICAL EXAMPLEThe Walker family built an extra bathroom rather than fightwith Tim, their son with schizophrenia, who spends hours inthe bath completing elaborate washing rituals.
The Sherman family must eat out several times a weekbecause Suzanne, their daughter with schizophrenia, refusesto allow anyone in the room when she eats.
The family social life may be disrupted. For instance,the family may fear leaving the ill person alone, or they mayfear that the ill person will embarrass visitors if friends areinvited in. Some families are willing to be open about the ad-justments they make in living with a loved one with schizo-phrenia, whereas others choose to live isolated lives.
Family members’ work can suffer because of the emo-tional strain of living with an ill member. They must take timeoff to accompany the schizophrenic person to doctors’ ap-pointments, make hospital visits, and help during interviewswith social agencies or the police. Family health may sufferbecause of general inattention or because of prolongedstresses within the home.
Outcome Identification: NOCThe outcome criteria established for a client with schizophre-nia need to be flexible and include the option to acknowledgea partial behavior change as success. For example, the out-
PARTNERING WITH CLIENTS AND FAMILIES
TEACHING ABOUT THE NEGATIVE SYMPTOMS OF SCHIZOPHRENIA
Families and caregivers have a difficult time understanding that symptoms of an illness include not just those experiences that are unusualand extra, such as hallucinations and delusions, but also those aspects of being human that are missing, such as enjoyment and motiva-tion. You need to evaluate the family’s current level of awareness of negative symptoms and provide important information.
Suggestions Rationale
Discuss how not having motivation and not seeming to care aboutsurroundings are part of the illness.
Families may be comforted to know that their loved one is notchoosing to behave in this way.
Inform the family members about how these symptoms look andfeel to the client.
Frequently, family members may blame medication for causing theclient to be “zoned out” or “just sitting and staring.”
Help families identify their responses to the negative symptoms. Families often misinterpret negative symptoms as laziness orrefusing to cooperate, and communicate this to the client. Thisincreases the negativity to which the client is exposed.
Talk about when and how negative symptoms respond to medica-tions.
The time frame of 18–24 months before negative symptomsrespond to atypical antipsychotics may seem a long time to familymembers, and they will need support so their expectations arerealistic.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 20

Chapter 16 • Schizophrenia and Other Psychotic Disorders 21
come for Body Image Distortion may include (a) recognizessymptom regularly, (b) speaks often with important other per-son regarding body feelings, and (c) manages to function de-spite symptomatology much of the time. Setting realisticgoals and continually reevaluating expectations based onyour client’s current desires and status is imperative with out-comes development. Other issues for outcomes with this pop-ulation are an awareness of the client’s multiple functionaldeficits, your personal response to working with this popula-tion, cultural differences, and lethality factors (Griner &Smith, 2006; Muñoz & Hilgenberg, 2006; Netto, 2006). Seethe Caring for the Spirit box above for cultural awarenesscontributions to outcomes.
Planning and Implementation: NICNursing interventions are most effective when they focus onthe needs and wants of the client to maximize functioning. Inorder to accomplish this, you must attend to the issues thatare important to the client. The client’s perspective is themost valuable tool you have to create competent and mean-ingful treatment interventions. Box 16-2 discusses the issuesmost important to the client with schizophrenia, from theunique perspective of the client.
When planning care for any client with a chronic ill-ness, nurses must be careful to set realistic goals for clientchange. Particular care must be taken with clients who areschizophrenic because they are extremely sensitive tochange and failure. Deterioration in all aspects of function-ing is characteristic of the disease. Focus on the most trou-blesome areas of client functioning and set incremental,short-term goals that pave the way for successes in achiev-ing long-term goals. Answering the questions in the YourSelf-Awareness: Working with Clients Who Have Schizo-phrenia feature on page 22 will increase your effectivenessin working with a psychotic client.
Preventing RelapseCombining maintenance antipsychotic medicationtherapy with psychosocial approaches has beenfound to be more effective than pharmacotherapyalone in delaying or preventing relapse. It has been suggestedthat early intervention would be effective in preventing re-lapse in clients with schizophrenia. This could be accom-plished through close clinical or family monitoring for theclient’s particular prodromal symptoms (those symptoms thatoccur early in the relapse process for that client). Once identi-
CARING FOR THE SPIRITCan Culturally Adapted Interventions Make a Difference in Outcome?
Schizophrenia is a difficult illness with many presenta-tions. The distress people experience during symptomexacerbation motivates the search for treatments thatare effective and useful in fulfilling the needs of theclient. The search for answers has taken a variety ofpathways, including the realm of spirituality and cul-tural sensitivity.
The quality of mental health services available topeople who have schizophrenia are greatly enhancedwhen the relevant content of both psychoeducationaland mental health interventions are culturally linked.Think about the last time you spoke with somebodyabout a problem you were having. If that person hadan understanding of both your culture and your valuesystem, such as spirituality, you probably had an easier
time explaining your problem. Now think about a timewhen you spoke with somebody about a problem youwere having and that person had no idea what youwere talking about. How would you describe that ex-perience? As you can imagine, this happens quite oftenwith people who have schizophrenia when their symp-toms are unusual or they are not able to articulatethem clearly.
Culture, spirituality, and a value system are intri-cately interwoven. They form the fabric for a system of meaning. Symptom expression, stressors, copingmechanisms, and interactions with others arise fromthis system. Keeping the cultural and spiritual contextof a client’s experience in mind while interactingaround psychiatric symptoms and treatment reducesthe client’s frustrations and increases the effectivenessof your communication.
BOX 16-2 Important Issues for the Client with Schizophrenia
People who have schizophrenia have to deal with an illnessdifferent from any other disease. The symptoms are unlikeanything else, and anosognia (unawareness of the illness) canfurther complicate their lives. Imagine not knowing you havean illness and not, therefore, needing help. It makes acceptingtreatment and staying in treatment particularly challenging.Developing meaningful treatment and conducting effectiveinterventions incorporate these vital aspects into effectivenursing care:
■ Personal power and efficacy■ Interpersonal relationships■ Social expectations■ Differences between what one hoped for oneself and what
one has now■ Connecting with people■ Personal growth■ Stability■ Coping with relapses■ Expression of spirituality■ Understanding the symptoms of the illness
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 21

22 Unit IV • CLIENTS WITH MENTAL DISORDERS
fied, prompt clinical intervention with antipsychotic medica-tion may reduce the overall frequency of the relapse event.
Programs for relapse prevention typically combinestandard doses of maintenance antipsychotic medicationwith psychosocial treatment and result in lower relapserates. Weekly group therapy for clients is an opportunity tomonitor prodromal symptoms. Such clinical scrutiny mayprevent or minimize relapse and rehospitalization. A multi-family group component is helpful to support and educatethe families as well as provide peer contacts and here-and-now experiences.
For clients residing with their families, educational andsupportive family interventions have an important effect onrelapse prevention. Those clients who live more independ-ently and experience relapses could benefit from a commu-nity treatment contact. Prevention is more effective whenclients and their families understand the likely relapse trig-gers, as outlined in TABLE 16-5 ■ .
Other aspects of relapse prevention have been imple-mented clinically with good results. Clients with a psychosisthat is not responsive to pharmacotherapy may benefit fromspecific cognitive–behavioral therapies (see Chapter 31 ),while persons with persistent negative symptoms and limitedsocial competence may find social skills training useful. In ad-dition, new programs of supported employment may enablesome clients to maintain competitive employment. The impactsof regularly scheduled employment and improved skills can be
To increase self-awareness about working with a person with ac-tive psychosis, ask yourself:
■ How do I feel about approaching a person who is havinghallucinations?
■ How do I feel about talking to someone who has delusionsthat frighten him?
■ Have I ever encountered someone in public who waspsychotic?
■ Do I fear that I might do something that might make theperson’s illness worse?
■ What kinds of understanding and knowledge do I need tofeel comfortable working with clients with psychosis?
To increase self-awareness about working with clients withdisrupted ability to care for themselves, ask yourself:
■ Do I react negatively when I think about someone my agewho has never worked?
■ What goes through my mind when I see someone who isdisheveled, unclean, or oddly dressed?
■ How can I find a point of connection between myself andsomeone whose life is so dramatically different from myown?
YOUR SELF-AWARENESSWorking with Clients Who Have Schizophrenia
TABLE 16-5 ■ Relapse Triggers in Schizophrenia
Physiological Stressors
Infection Pain
Acute illness Fatigue
Chronic illness Side effects of medications
Dehydration Appetite changes
Insomnia Injury
Rape Surgery
Personal Stressors
Exacerbation/relapse of illness Financial difficulties
Depression An increase in responsibility
Negative symptoms of schizophrenia A decrease in access to resources
Spiritual distress Recreational activity choice/access
Pet loss/illness/aging Maturational/developmental changes
Interpersonal Stressors
Perceived rejection/abandonment Loss of job or status within a job
Conflict, anger Altered contact with another or others
Relationship changes (family, intimate relationships, friendships, etc.) High expressed emotion
Community Stressors
Difficulties making living arrangements Disruption of living situation
Roommate/family stressors Transportation
Community disruption
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 22

Chapter 16 • Schizophrenia and Other Psychotic Disorders 23
a helpful distracter from the onslaught of psychosis if it doesnot tax the client’s coping abilities.
Promoting Adequate CommunicationClients with schizophrenia try to communicate, even thoughtheir statements may be difficult to understand. Close atten-tion to what the client is saying and honest attempts to under-stand the real and symbolic aspects of the message areimportant. The client will perceive nuances of your behavior.Therefore, one of the most direct and successful ways todemonstrate caring and respect is to attend seriously to theclient (this is discussed in depth in Chapter 10 ).
Clients make valid observations about their environ-ment, needs, and concerns. Some, if not all, of their observa-tions and sensations exist in reality and are not to be treatedas if they are all totally psychotic symptoms. The sensitivityto the environment that can overwhelm someone with schizo-phrenia also clues him or her into aspects to which othersmay not have access. A client may make observations aboutevents or situations that are beyond your awareness. For ex-ample, take seriously a client’s statement about anotherclient’s drug use or suicidal threats. If a client complains of aphysical symptom such as stomach distress, consider thesymptom as real until there is evidence otherwise. It is easy todismiss a client’s statements, particularly those of a delu-sional client. Doing so, however, shows lack of respect forthe client’s intact capacities to see and respond to what is hap-pening in the environment.
Promoting Adherence with Medication RegimenPsychotropic medications play an important part in thetreatment of schizophrenic disorders. Drugs that di-minish focal symptoms (hallucinations and delusions)and yet produce relatively few untoward effects are now avail-able. Complying with treatment, which for schizophreniameans medications, is a complex demand. You will need to becreative and ever-mindful of your client’s specific barriers tolearning and maintaining specific behaviors. The disease itselfcauses difficulty in adhering to a treatment regimen when aclient lacks the ability to recognize the illness. This is calledpoor insight and can be compared to the unawareness or lack ofinsight into neurological deficits following a stroke. Recognizethat individuals respond to their illness, their circumstances,and their medications in different ways.
The idea of adherence can be expressed through a num-ber of terms such as treatment adherence, role reliability, col-laboration for health behaviors, and cooperation. Interviewsand clinical contacts tell us that clients are able to participatein the treatment if they are included and made an integral partof the design of their care (Haynes et al., 2006; Isherwood,Burns, & Rigby, 2006; Rosenberg & Rosenberg, 2006). SeeBox 16-3 for a description of the barriers and challenges totreatment adherence.
Consistent adherence in taking medications as pre-scribed is not common among this client population. Re-searchers estimate that as few as 68% of psychiatric clientsadhere to medication regimens while in the hospital (Uko-
Ekpenyong, 2006). When these clients return to the commu-nity, 37% or fewer adhere to drug regimens. Clients may stoptaking their medications for these reasons:
■ They don’t understand the administrationinstructions.
■ They are too disorganized to follow the instructions.■ The side effects of major tranquilizers are too
uncomfortable.■ They do not wish to be stigmatized as having
schizophrenia so they reject treatment.■ They begin to feel better and believe the medication
is no longer necessary.■ They don’t have easy access to pharmacies because
of transportation, financial, or interpersonaldifficulties.
Clients who do not take medications are more vulnera-ble to stressors and risk more frequent relapse of symptoms.Efforts to educate clients about their medications and to havethem practice self-medication prior to discharge have in-creased the rate of adherence only marginally. Client attitudestoward the medications prescribed also influence their will-ingness to comply. You must be an active participant in as-sessing adherence and fostering a positive attitude towardmedications. Commonly used antipsychotic medications andside effects are presented in Chapter 32.
Clients are often ambivalent about taking medications.Maintaining adequate blood levels of therapeutic medicationsis important for clients with schizophrenia. To help themovercome ambivalence, give them time to think about takingthe medications. Set a time limit. For an inpatient who fails tocomply, come back later and try again. Two useful strategiesare reminding clients of the positive effects of the medicationand framing the action as a way for them to help themselvesget better. The Your Intervention Strategies: Adherence En-hancers feature on page 24 is a compendium for increasingtreatment adherence for clients with schizophrenia.
BOX 16-3 Challenges to Adherence
■ Difficulties with prescribed psychotropic medications■ Severe level of symptomatology■ Cognitive difficulties secondary to thought disorder■ Motivational problems secondary to negative symptoms■ Motivational problems secondary to flight into health
(wanting to be “normal”)■ Unpleasant side effects■ Persistence of positive symptoms (delusions) mitigating
against adherence■ Financial issues■ Misperceptions and misunderstanding of the information
presented in medication teaching■ Cursory or minimal medication teaching that lacks relevance
to all areas of the client’s life■ Unresolved issues with treatment providers■ Cultural impacts
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 23

24 Unit IV • CLIENTS WITH MENTAL DISORDERS
Assisting with Grooming and HygieneHelping clients establish and maintain personal care habits is acomplex process. If the client clearly lacks the skills, then teachthe skills. If, however, the client has learned grooming skillsbut does not practice them, focus on ways to motivate theclient. Intervention begins by establishing clear expectationsabout essential grooming habits. The frequency and timing ofall aspects of grooming—including bathing, dressing, hair care,oral hygiene, and room care—can be specified in writing if thatwould be a useful learning device for your client.
Formal training programs for helping chronically men-tally ill clients improve their grooming skills can be applied ininpatient as well as outpatient settings. These programs arewell developed and tested. They systematically help clients inall steps of personal grooming, including collecting grooming
supplies, moving to the grooming area (a bathroom or bed-room with sink and mirror), completing each grooming step,completing appropriate dressing, and storing grooming mate-rials. Nursing interventions at each step can progress fromsimple verbal coaching, to modeling, to gentle physical guid-ance. Acknowledge client efforts during each phase with real-istic encouragement and praise. The success of these programsprobably depends on daily staff attention to the client’s train-ing, along with consistent, meaningful rewards. Avoid powerstruggles regarding the completion of tasks. If initial promptsdon’t work, leave the client alone for a short period.
Promoting Organized BehaviorClients whose behavior is disorganized require direction andlimits to make their actions more effective and goal-directed.
YOUR INTERVENTION STRATEGIESAdherence Enhancers
Make a figure of a hub of a wheel with adherence as the huband each feature a spoke in the wheel or a target with each fea-ture/strategy as an arrow hitting the center of the target.
■ Involve the client as a partner in medication-based treatmentplanning decisions.
■ Change to another medication with a differentneurotransmitter action with lower or different side effectsthat may be more tolerable. Atypical antipsychoticmedications have a lower side-effect profile and can increaseadherence because they’re not so hard to take.
■ Teach the client how to report side effects, including theirseverity (from dry mouth to priapism). This may require role-playing or assertiveness training.
■ Teach the client how to manage the side effects he doesget—if possible, with such solutions as hard candy and arubber pillow case liner. It may make it tolerable to continueon the medication.
■ Instruct, educate, and arrange for reminders well beforedischarge (especially with geriatric recipients) to maximizeboth knowledge and adherence (knowledge can be thenumber-one factor determining adherence).
■ Simplify the medication regimen.■ Match the medication dosing strategy to the client’s
schedule, preferences, work situation, and recreationalpursuits.
■ Discuss the client’s expectations of the medication—are theyrealistic?
■ Take cultural impacts into account during comprehensivetreatment planning.
■ Use concrete educators. The tried-and-true cognitionenhancers are: pamphlets, booklets, handbooks, workbooks,sheets, cards, videos, audiotapes, posters, magnets, logs,journals, etc.
■ Assess the client’s perception of control over the treatmentregimen.
■ Assess the client’s self-administration of medications.■ Help the client take action to prevent untoward effects, such
as maintaining fluid intake to avoid postural hypotension.
■ Teach coping efforts involving problem solving, whichincreases adherence.
■ Peer support is important. Hearing from peers how a newmedication could help with symptoms, and asking theprescriber to consider it, improves adherence.
■ Give hope—it pays to be well. It takes all the small steps torecovery in addition to medications to get better.
■ Repetition—say the same thing over and over, with patience,especially if clients have schizophrenia or depression.
■ Develop reminders, cues to remembering (visual cues—when I see this I need to take my pills, when I eat lunch Itake my pills, rubber band on wrist, calendars, to-do lists;auditory cues—alarm clocks or watches).
■ Depot medications given weekly, biweekly, or monthly cancontribute to adherence because the client does not have toremember to take pills. The marketing of an atypicalantipsychotic in depot form (risperidone) adds to thechoices.
■ Pill boxes—come in many shapes, sizes, and organizationalstyles (multiple daily doses, layers for time of day, Braillemarkings, timer with small alarm clock feature that opens compartment). If the medication can’t be taken outof its original container without affecting the potency,place a small button or candy in the pill box to serve as areminder.
■ Keep all medications and information about them in one dry,cool place. Use plastic products such as containers andbags—not in the bathroom or by a dishwasher in thekitchen.
■ Involve the family.■ Match the degree of client autonomy in treatment to the
needs of the individual client.■ Financial assistance might be available.■ Have clients teach about their medications (after they have
learned sufficiently) to other recipients or to significantothers. Nothing speeds learning as much as teachingothers.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 24

Chapter 16 • Schizophrenia and Other Psychotic Disorders 25
In working with a disorganized client, proceed slowly and re-main calm. The client’s perception of the environment may bedistorted, but your calmness can help calm the client. Try to di-rect the client in simple, safe activities. Nursing goals and in-terventions for a disorganized client must focus on manageablesteps. A clinical example of one such intervention follows.
CLINICAL EXAMPLEGeorge is moving quickly yet aimlessly from the refrigerator tothe cupboard. He pulls a box of cereal from the cupboard,opens it, and then wanders away. Next he goes to the refrig-erator, opens the door, peers in, and closes the door. Rum-maging through all his pockets, he locates a comb, combsthrough his hair, sets the comb on the counter, and wandersback to the cupboard. This effortful yet unproductive behaviorcontinues for several minutes when the nurse enters.
Nurse: George, are you trying to get some cereal foryourself?
George: Sort of. I was going to . . . brush . . . no . . .comb. . . no . . . eat something. Yeah, I wantedsomething to eat.
Nurse: Try to concentrate on one thing. First, put thecomb back in your pocket. (He does so.) Now,come over here and get the cereal box. Here’s abowl. Here’s a spoon. (She hands him the utensils.)Why don’t you sit right here? (She seats him sothat he has his back to the rest of the activity in theroom.) Can you sit still for a bit?
George: I think so.Nurse: Pour yourself some cereal. I’ll get the milk for you.
(She does so.)
George begins to eat his cereal quietly. The nurse stays withhim for a few minutes and directs him to continue eatingeach time he becomes distracted by others who come intothe room.
Promoting Social Interaction and ActivityThe client’s efforts to withdraw from social contact stemfrom past relationship failures and fear of rejection. Clientsoften find their internal world less risky and therefore moreattractive than a world that requires interpersonal relating.When making efforts to help the client become less with-drawn, respect the client’s sometimes overwhelming anxietyabout human contact.
After establishing a basic level of trust, encourage theclient to try out new behaviors within the relationship. Thegoal is to have the client experience success; therefore, en-courage even small increments of change. If, for example, theclient has difficulty initiating conversation, encourage theclient to practice this skill once a day. Similarly, if the clientavoids any activity in the environment because of fear of re-lating to groups, structure an activity involving the client,yourself, and one other client. Reinforce the client when he orshe approaches you to communicate, even if that communica-tion contains problematic patterns (refer back to the Rx Com-munication feature on page 13).
Promoting Social Skills and ActivitiesAddress social skills that are essential to functioning in theenvironment: introducing oneself, starting a conversation,ending a conversation, saying no, asking for assistance, andlistening. Staff members can model these skills and helpclients role-play each skill. Focus discussion on situations inwhich clients might need the skill. If they see its applicabilityto dilemmas in their personal lives, they will be motivated tolearn the skill. Praise and, if available, material rewards canalso motivate clients. Social skills training can also be donein small groups (see Chapter 30 ).
Schizophrenia can disturb a person’s will and capacity toaccomplish meaningful activity. Clients with distorted per-ceptions and thinking expend considerable energy merelytaking in and interpreting their immediate worlds. In addition,major tranquilizers, which control the positive symptoms ofthe disease, can further inhibit a client’s active in-volvement and interest in activities. Be aware of howmuch work it takes to cope with schizophrenic symp-toms. Do not assume that periods of quiet or inactivity aredue to laziness or lack of interest. Rather, assess each individ-ual’s need for quiet periods in which to organize perceptionsand thoughts.
At the same time, clients with schizophrenia livein a culture in which action and accomplishment arehighly prized and rewarded. They are not immune tothe pressure for personal productivity as a measure of personalworth (Thomas, Seebohm, Henderson, Munn-Giddings, &Yasmeen, 2006). For this reason, they feel better about them-selves when they are involved in meaningful activities. Yourtask is to help clients find activities that are intrinsically re-warding or that bring some social or tangible reward, yet arewithin their capacities.
Learning clients’ personal interests is a first step. Provid-ing opportunities for the client to actively engage in an activ-ity of interest (by providing records, books, craft materials, oraccess to newspapers and television) is the next intervention.In addition, activities within the therapeutic milieu, such asattending groups and completing unit “jobs,” can provide theexternal rewards of praise from staff and peers (Connor &Wilson, 2006). These activities give clients confidence anddevelop and promote their work habits. Success in these ac-tivities can lead to success in volunteer or paid work in thecommunity after discharge.
Intervening with Hallucinations and DelusionsDelusions or hallucinations often frighten clients. You can in-tervene by:
■ Reassuring clients that they are safe■ Protecting them from physical harm as they respond
to their altered perceptions■ Validating the feelings they are having in response to
their experience■ Validating reality■ Helping them distinguish what is real from what is a
hallucination or a delusion
MED
IALIN
KC
are Plan, Paranoid Schizophrenia
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 25

26 Unit IV • CLIENTS WITH MENTAL DISORDERS
Hallucinations are especially frightening if the client hasnever experienced them before or if their content is threateningor angry. Attempt to alleviate this anxiety by describing yourperception of the frightened behavior and asking clients to dis-cuss what they are experiencing. Make simple reassuring re-marks, such as “I hear what you’re telling me. This soundsvery frightening. No one means to harm you.” See the Your In-tervention Strategies feature above for intervention strategiesthat help a client manage hallucinations.
Protect clients from harm and reassure them aboutsafety. A client may take impulsive action to escape the fright-ening experience or to obey voices in the hallucination. Pre-vent this by:
■ Closely observing client behavior during activehallucinations
■ Using calming techniques and one–to–oneinteractions to shape and guide the situation
■ Reducing excess noise and distractions. One personspeaks to the client at a time.
■ Intervening quickly by giving additionaldoses of psychotropic medications or placingthe client in a quiet room
■ If necessary, securing the unit so that the client cannotleave and take self-destructive or impulsive action
Make every effort to help the client attend to real ratherthan internal stimuli, orient the client to the real situation, andencourage the client to focus on you rather than on the hallu-cination (England, 2006; Grant, 2006). “George, listen to merather than to the sounds you hear. Remember, you are in thehospital and I am your nurse. I will help you find your shoes.Come with me.” Active involvement in some activity, such asfinding shoes, will help the client maintain a focus on realevents and perceptions.
General guidelines for working with delusional individ-uals are to avoid arguing with their false beliefs, to focus onthe reality-based aspects of their communication, and to pro-tect them from acting on their delusions in a way that mightharm themselves or others (Hunt et al., 2006). It may also beimportant to teach clients that sharing their delusional contentdirectly with others in community settings such as the work-place or the social club may frighten others and lead tostigmatization. Keeping delusional content to oneself in thesesituations can improve interpersonal relationships. See theYour Intervention Strategies feature above for suggestednursing interventions that contain or manage delusions.
Promoting Congruent Emotional ResponsesWorking with clients who display blunted or flat affect can beconfusing for nurses who are accustomed to reading emo-tional responses that fall within a more normal range. Beaware that these clients have feelings about events aroundthem, including their interaction with you and other staffmembers, yet may have difficulty expressing those feelings.
Note any lack of congruence between the person’s affectand the content of the message. If your relationship with theclient is well established, you might comment on the incon-gruity and explore it with the client. (“Malcolm, what you aretelling me is sad but you are laughing. What shall I pay atten-tion to?”) Modeling clear, congruent communication is help-ful. Little can be done to change the client’s anhedonia, yetempathic listening might comfort the client.
Ambivalence, the simultaneous experience of contradic-tory feelings about a person, object, or action, can troubleclients with schizophrenia. Ambivalence can become greatenough to immobilize a client. Such clients cannot express
■ Determine the kind of hallucinations (auditory, visual, etc.).■ Can the symptom be managed with current coping?■ Access resources (advocacy groups, peers, staff, literature) for
fresh ideas, better management techniques.■ Discuss options and success rate with professionals.■ Select options for coping with the stimuli:
DistractionResistingCalmingTreatment (such as medication)
■ Practice using an option to cope.■ Use a technique based on the success you have with it.■ Be ready to replace coping styles when they don’t work
anymore.
YOUR INTERVENTION STRATEGIESHelping a Client ManageHallucinations
■ Determine if the client can tell the difference between thedelusion (“I don’t drink the water because it’s poisoned”)and a personal preference (“I’m not drinking water because Iprefer orange juice”).
■ Work with advocacy groups, peers, and professional staff toclearly demarcate what constitutes delusional thinking.
■ Suggest options to cope with delusional thoughts:Support from othersConcrete tasksCaretaking activitiesRefocusing thoughtsDetermined efforts to steer thinking in another direction
■ Make sure client understands how important it is to besurrounded by people who reinforce the client’s efforts.
■ Encourage clients to self-validate the struggle they are in andany level of effectiveness they achieve at coping.
YOUR INTERVENTION STRATEGIESHelping a Client ManageDelusions
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 26

Chapter 16 • Schizophrenia and Other Psychotic Disorders 27
one emotion or the other, or choose one action over the other.You may be able to partially alleviate the client’s unease byidentifying aloud the emotions the client may be experienc-ing. (“Lily, I think you might be feeling both very happy tosee your father and at the same time very angry.”) Namingthe conflicting emotions gives the client the opportunity totalk about them, although many times he or she may not beable to do so.
Immobility due to ambivalence is extremely uncomfort-able. One way of intervening is to limit the number ofchoices the indecisive client has to make. For example, aman may be immobilized by his inability to decide whetherto go out alone for the first time. You can help by telling himthat it seems too soon for him to go out alone and that, fortoday, he must be accompanied. Another example is a youngwoman who is undecided about where to sit. You can removeextra chairs at the table in the dining room so that she hasonly one choice.
Promoting Family Understanding and InvolvementWhen a person with schizophrenia is hospitalized, encouragethe family and help them remain involved in the client’s care.Except for unusual circumstances, share information on theclient’s status, treatment program, and future treatment plans,including discharge plans. Nurses may need to be active ad-vocates for families’ rights to information about, and involve-
ment in, the care of their loved one with schizophrenia. Ofcourse, nurses need to comply with the client’s wishes andwith the laws governing disclosure of information, whichvary by state and by institution.
Referral to Psychoeducation Programs If assessment suggeststhat family members need information about the disease andtreatment, refer the family to education programs, if they areavailable. Family psychoeducation programs are preferable todirect teaching because they often combine education withmutual support. In such groups, families can meet others whoshare their life difficulties. These peers can provide informalsupport and information to help the family deal with the tasksthat lie ahead. You can reinforce the formal teaching that oc-curs in such programs when you meet with individual families.See the Partnering with Clients and Families: Teaching aboutSchizophrenia feature above.
Referral to NAMI Without exception, families should knowabout a national family support group with many local andstate affiliates. The National Alliance on Mental Illness(NAMI) serves families through educational programs, localsupport groups, and political activism. Most local organiza-tions are listed in telephone directories or can be reachedthrough the local community mental health agency responsi-ble for information and referral. For a resource link to NAMI,go to the Companion Website for this book.
PARTNERING WITH CLIENTS AND FAMILIES
TEACHING ABOUT SCHIZOPHRENIA
Suggestions Rationale
Discuss the basic nature of the disorder: Schizophrenia is a diseaseof the brain, like any other biologic disease.
Families misunderstand mental illness to be a personal failing andare comforted by the fact that it has a biologic basis.
Help families identify their responses to the early ambiguous signsof the illness and notice how their responses have changed nowthat the diagnosis has been made.
Families often misinterpret early signs of the disorder as acting outor developmentally appropriate behavior. On learning that thesesigns are part of the illness, they feel guilty for not seeking helpsooner.
Reinforce families for supporting the ill member in seekingtreatment.
Stigma about mental illness persists, and families need support fortaking action and engaging with treatment systems.
Refer families to structured educational or psychoeducationalprograms in which they can learn about the disease and itstreatment, as well as receive support.
Schizophrenia is extremely complex, and its treatment is multifac-eted. Families can benefit from structured classes. Programs thatoffer support to families in addition to education have provenefficacy in improving the illness course for the ill member.
Inform families about how to reach the local branch of theNational Alliance on Mental Illness (NAMI). Hand out fliers thatprovide telephone numbers and people to contact.
NAMI is a nationwide family support organization that providespeer support, education, and advocacy for the seriously mentallyill and their families.
Provide families with access to information such as:
Mueser, K. T., & Gingerich, S. (1994). Schizophrenia: A guide for families. New York: Harbinger.
Torrey, E. F. (1995). Surviving schizophrenia: A manual for families, consumers, and providers (3rd ed.). New York: Harper Collins.
To assist families, you need to evaluate the family’s current responses to living with and caring for a family member with schizophrenia.The following suggestions apply to the time period shortly after the disorder has been diagnosed.
MED
IALIN
KN
ational Alliance on M
ental Illness
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 27

28 Unit IV • CLIENTS WITH MENTAL DISORDERS
ery in mind, as every client can improve and recover to a cer-tain extent. The National Library of Medicine MEDLINEpluswebsite at www.nimh.nih.gov/publicat/schizmenu.cfm offerssearch options on schizophrenia and other topics.
CommunicationClients will, with greater regularity, express their thoughtsclearly and congruently. They will feel sufficient trust to talkto the nurse about troublesome symptoms or experiences. Be-cause clients will probably continue to experience somesymptoms even after medications have taken effect, this trustallows them to express what has changed and what is stilltroublesome.
Self-CareClients will consistently appear clean and well groomed andwill independently manage personal grooming and hygiene.Clients will have clean and reasonably appropriate clothes, interms of both fashion and season. Individual styles of dress,which are the client’s way of expressing or presenting theself, will be supported by nurses. The means for maintainingself-care after discharge from acute care are identified.
Activity IntoleranceClients will participate in goal-directed activities with mini-mal intervention. Clients will complete the activities theybegin. Clients will demonstrate a broader range of interestand activities than they did on admission.
Social IsolationClients will demonstrate the capacity to interact, at least forbrief periods, with nursing staff, with other clients, and in smallgroups. They will consistently demonstrate socially requiredinteractions, such as greeting and starting a conversation with astranger, asking for assistance, saying no, and listening to an-other’s conversation. Clients will be inactive for shorter peri-ods and spend more time engaged in interesting or meaningfulactivity. They will demonstrate the capacity to function outsidethe protective environment of acute or sheltered care.
Sensory/Perceptual AlterationsClients will have fewer episodes of attending to internal stim-uli. If hallucinations or delusions persist, clients will begin toidentify stressors or situations that precipitate them. Clientswill identify and practice personal coping strategies that de-crease the hallucinations, delusions, or their effects, such asgoing to a quiet room, engaging in social activities, and per-forming activities that demand concentration.
Thought ProcessesClients will engage in reality-based discussions. If delusionspersist, clients will not act on delusions in ways that areharmful or detrimental to themselves or others. They will alsoidentify significant others in their current living environmentwho can help them limit their hallucinations via distraction orsocial contact.
CLINICAL EXAMPLEThe Oldstads were worried about their daughter’s failinggrades at college for the last semester and were surprised tolearn that she had ended a relationship with her boyfriend.When she came home for spring break, she seemed disinter-ested and uncommunicative and wouldn’t eat or socializewith the family. Her parents found her burning incense andchanting to herself in the mirror at 3:00 A.M. In a panic, theytook her to the local emergency room. After a completeworkup, they were shocked to learn that the probable diagno-sis was schizophrenia. Furthermore, the physician wantedtheir daughter to begin taking medication.
The rapidity of the decline in their daughter’s function-ing, and the fact that she had hidden many of her symptomsfrom them, left the Oldstads feeling guilty, sad, and disbeliev-ing. They could not fathom how this had happened to theirbeautiful daughter. A nurse at the emergency room had giventhem the number of a local NAMI support group and hotline.In their anguish, they called and were able to speak with otherparents, who helped them begin to deal with their emotionsand directed them to helpful books that explained schizo-phrenia and its treatment.
The importance of NAMI to families and the NAMI ed-ucation program are discussed in detail in Chapter 30.
Promoting Community ContactsAn awareness of a client’s community supports and potentialtreatment programs can guide nurses in preparing clients fordischarge. For example, the client’s most important peer sup-port group might be the clientele at a local day treatment pro-gram or social club. If so, several visits prior to discharge willhelp the client make the transition back to the community.
Preparing clients for the residence they will enter afterhospital discharge is a central nursing task. Often, placementdepends on how the client functions in the hospital (Stroupet al., 2006). If the client is able to manage medications, par-ticipate in a variety of groups, and live cooperatively withother clients, then placement in a residential care facility thatsupports independent functioning is appropriate. In contrast,clients who need assistance with structuring free time, resisttaking medications, or cannot be responsible for self-care re-quire a more structured and supervised environment (Wil-son, 2006).
Nurses work with clients to help them achieve theirhighest level of functioning. They document clients’ abilitiesto perform various tasks and make recommendations to thetreatment team about appropriate placements.
EvaluationTo complete the nursing process, nurses evaluate changes inclient status and behavior in response to nursing interven-tions. Evaluation criteria are linked to nursing goals and re-flect an understanding of the limitations of clients withschizophrenia. However, you must keep the concept of recov-
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 28

Chapter 16 • Schizophrenia and Other Psychotic Disorders 29
Emotional ResponsesClients will have increased awareness that their emotional ex-pressions at times do not match their verbal communications.They will monitor others’ responses to them to learn cuesabout how they are varying their emotional expressions.Clients will experience fewer episodes of extreme discomfortdue to ambivalence about people, events, or actions.
Family FunctioningFamilies will be involved in all aspects of client care, includ-ing assessment, planning and carrying out interventions, inpa-tient treatment choices, and planning for discharge. Familyunderstanding of the illness trajectory and the client’s capaci-ties and limits will improve (Segrin, 2006). Family difficultiesin caring for clients will be considered in treatment and dis-charge planning, and adequate resources will be identified tosupport family needs. Families will report that their questionsabout the schizophrenic disease process, and about varyingmodes of treatment for the disorder, have been answered.
There are a number of services necessary and availablein the community to maximize both quality of life and moreindependent functioning for people with schizophrenia andother psychotic disorders. Examples are:
1. Continuing day treatment programs2. Independent living centers3. Day hospitals4. Community mental health centers5. Social clubs6. Wellness centers
These various settings are described in Chapter 12.Counseling, psychotherapy, medication management,
and other treatments are part of the care delivered in the com-munity. In addition, remember that recreation is a quality-of-life issue. Community-based care can be instrumental inproviding the guidance needed for clients to integrate intocommunity living with an illness that can be debilitating anddifficult.
HOME CAREYou may conduct different roles in delivering clinical serv-ices and care to clients with schizophrenia in a home setting.For example, you may function as a case manager and makehome visits. This can be particularly important for clientswith schizophrenia who often have great difficulty success-fully meeting daily responsibilities and maintaining inde-pendence in a healthy home environment.
An important function of the nurse, whetheror not you are a case manager, is to assist clientswho have schizophrenia with medication adher-ence. Clients with schizophrenia are at high risk for re-lapse because they may stop taking their antipsychoticmedications. This can happen because of side effects(those reported and not reported to the prescriber), confu-sion about medication administration schedules, environ-mental factors that do not encourage adherence to amedication regimen, or any number of other factors. Youcan play an important role in reducing the likelihood of re-lapse during home care visits. The home will shape adher-ence practices because the home is the environment inwhich most doses of their medications are taken.
Home interventions by nurses, however, are not limitedto case management or medication adherence issues. Somepeople with schizophrenia can benefit from supportive psy-chotherapeutic interventions delivered by you in the client’shome. These interventions can help generalize what theyhave learned beyond the confines of the nurse’s office or theclinic. When people who have schizophrenia live with sig-nificant others, it is sometimes possible for you to deliverpsychoeducational interventions for everyone living to-gether as a unit. This allows the significant others and theclient the opportunity to increase their skills in living to-gether and coping with this serious illness in a way that low-ers the probability of client relapse.
CASE MANAGEMENTKnowledge of the impact schizophrenia has on the way an in-dividual thinks and functions is the underpinning of a compe-tent case management program. In order to carry out anyparticular task, an individual with this illness must have spe-cific duties coupled with realistic expectations. The casemanagement strategies that work best with schizophrenia andother psychotic disorders include:
1. Tasks broken into manageable steps2. Concrete actions3. Structured environment4. Routines and schedules5. Dependable professionals6. Flexibility to accommodate the shifts of the illness
Intensive Case Management (ICM) assists people withschizophrenia in outpatient settings (discussed in Chapter12 ). With a smaller caseload, you have greater involve-ment with clients who require more supervision and care.You would orchestrate appointments and daily functioningissues to enhance the client’s abilities to remain in the com-munity and to foster a more independent lifestyle. Whetheryour assignment involves case management or intensive casemanagement, the difficulties with thought processing andcommunication mentioned earlier in the chapter will shapeyour management of the case.
COMMUNITY-BASED CAREPeople who have schizophrenia can have repetitive inpatienthospitalizations. The transition from an inpatient unit back tothe community setting must begin prior to the client’s dis-charge from the inpatient setting, forming a bridge from inpa-tient to outpatient care.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 29

30 Unit IV • CLIENTS WITH MENTAL DISORDERS
news events are always present at a lowlevel. He has lived with his mother since di-agnosis, attending day treatment and, forthe last 8 months, a structured work pro-gram. He occasionally attends client supportnetwork meetings. His work attendance hasbeen sporadic, and he has been on and offprobation for nonattendance in this struc-tured work environment. He receives med-ications and follow-up treatment at thecommunity mental health center.
Family HistoryThe Mays are both living and well. Theywere separated 3 years ago and divorced 2years ago. Jack’s father is an attorney, andJack sees him approximately once a month.Their relationship is pleasant but not close.His mother runs her own crafts store and isagreeable to having Jack live with her. Thereare no other children.
Psychosocial HistoryJack has completed high school and a fewcourses at the local community college. Hewas an above-average student and was al-ways involved in school and extracurricularactivities, until about 9 months before hisfirst psychotic episode. Since that time, hehas socialized primarily with his mother andrarely with a few acquaintances from theclient support group. He smokes a pack ofcigarettes a day and drinks beer occasion-ally. He denies any illicit drug use. Jack has a
keen interest in computers. He took exten-sive coursework in computers in school andhas collected considerable equipment andsoftware, primarily gifts from his father.Other pastimes are listening to rock musicand watching television.
Medical HistoryNo notable medical problems.
Current Mental StatusJack is a healthy-looking 24-year-old who isanxious, somewhat guarded, but coopera-tive in the interview. He is oriented to per-son, time, and place, and demonstratesgood memory and recall. Judgment is im-paired. His affect is anxious. Speech is rapid,pressured, tangential. He is hyperalert to hisenvironment and is notably startled by asiren outside. Persecutory delusions aboutpeople trying to take over his home andwork are present, and he has hallucinationsof unrecognizable voices and the voice ofhis father. No command hallucinations.Some loosening of associations present. Ab-stractions are concrete and self-referential.Insight poor; believes that his mother is“sick” and that she should not impede himin his important projects.
Other Clinical DataEvidence that Jack may have stopped takingmedications approximately 2 weeks ago.Suicide/violence potential minimal.
Nursing Diagnosis: Disturbed Thought Processes
Expected Outcome: Client will demonstrate the ability to cope competently with delusions.
Identifying InformationJack May is a 24-year-old single male who liveswith his mother and supports himself withSSI. He is brought to the psychiatric emer-gency service by his mother. He currently at-tends a structured work program 5 days aweek, but stopped attending 8 days ago.
Jack says that he does not need to be hos-pitalized and that his mother is the one withthe problem. He wants to be left alone towork on his computer projects. He admitsthat he has been hearing multiple voices inhis head for the past week. For the past 2weeks, Jack has been increasingly isolated,working on his personal computer in hisroom. He will not tell anyone what the workis about, but his mother has seen printoutsthat suggest it is a plan to soundproof andsecure his room. Jack stopped attending hiswork program a week ago, saying that hehad “more important work” to do at home.He refuses to eat or talk with his mother. Hismother believes he stopped taking his med-ications. An identifiable stressor is that 2weeks ago his father announced plans to re-marry in the near future.
Symptom HistoryTwo years ago, Jack had a serious psychosisprecipitated by his move to a college out ofstate. He was diagnosed with schizophrenia,paranoid type. He was hospitalized for 2weeks, stabilized on Haldol, and dischargedhome. Persecutory delusions that shift with
NURSING CARE PLANClient with Schizophrenia
Short-Term Goals Interventions Rationales
Client able to function in avariety of settings withoutintrusive delusional thoughtcontent.
■ Make frequent, supportive, and brief contacts.■ Allow description of delusional thoughts and
acknowledge emotional impact of same.
Some contacts can be overwhelming for a clientwith schizophrenia and need to be of amanageable length.
■ Focus discussions on the client’s feeling levelconcerning the delusions, and not the content.
■ Teach client how to cope with delusionalthinking through engagement in activities fordistraction, active self-talk promoting hisefforts, support from others, treatment.
The client must be taught how to cope with thesymptoms of the illness in an effective manner.
■ Reinforce adaptive efforts.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 30

Nursing Diagnosis: Anxiety related to delusions
Expected Outcome: Client will demonstrate decreased anxiety.
Chapter 16 • Schizophrenia and Other Psychotic Disorders 31
Short-Term Goals Interventions Rationales
Client able to describe areduction in his anxiety.Client participates in histreatment.
■ Make frequent, supportive, and brief contacts. Some contacts can be overwhelming for a clientwith schizophrenia and need to be of amanageable length.
■ Reassure client verbally, with a structuredroutine, and by giving explanations congruentwith client’s ability to understand.
People with schizophrenia often do not havetheir feelings acknowledged. Reassurancevalidates their feelings.
■ Prompt client to interact with others when ableto reduce feelings of isolation and alienation.
■ Provide an array of coping skills client may usewhen anxious.
You must teach a variety of coping skills to suitvarious situations.
Concept MapClient with Schizophrenia: Disturbed Thought Processes
Monitoringby through
rationale
Teaching
expected outcome
short-term goal
Mr. Jack May24 y.o. maleSchizophrenia
generates nursing diagnosis
Reinforce adaptive efforts.Make frequent, supportive,and brief contacts.
Some contacts can be overwhelmingfor a client with schizophrenia and needto be of a manageable length.
• Allow description of delusionalthoughts and acknowledge emotionalimpact of same.• Focus discussions on the client’sfeeling level concerning the delusions,and not the content.
• Teach client how to cope withdelusional thinking through engagementin activities for distraction, activeself-talk, promoting his efforts, supportfrom others, treatment.
The client must be taught how to cope with the symptoms of the illness in an effective manner.
rationale
Disturbed Thought Processes
Client will demonstrate the ability tocope competently with delusions.
Client able to function in a variety of settingswithout intrusive delusional thought content.
intervention
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 31

32 Unit IV • CLIENTS WITH MENTAL DISORDERS
Concept MapClient with Schizophrenia: Anxiety Related to Delusions
Monitoring
by
expected outcome
short-term goal
intervention
Monitoring intervention intervention
intervention
Mr. Jack May24 y.o. maleSchizophrenia
generates nursing diagnosis
People with schizophrenia often donot have their feelings acknowledged.Reassurance validates their feelings.
Make frequent, supportive,and brief contacts.
Provide an array of copingskills client may use whenanxious.
Some contacts can be overwhelmingfor a client with schizophrenia and needto be of a manageable length.
• Reassure client verbally, with astructured routine, and by givingexplanations congruent with client’sability to understand.
rationale
Anxiety related to delusions
Client will demonstrate decreased anxiety
Client able to describe a reduction in hisanxiety.Client participates in his treatment.
by
rationale
rationale
by
• Prompt client to interact with otherswhen able to reduce feelings ofisolation and alienation.
by
You must teach a variety of copingskills to suit various situations.
Teaching
Teaching
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 32

Chapter 16 • Schizophrenia and Other Psychotic Disorders 33
EXPLORE MEDIALINK
For NCLEX-RN® review questions, case studies, andother resources for this chapter see the Prentice Hall Nursing MediaLink CD-ROM thataccompanies this book and the Companion Website at www.prenhall.com/kneisl.
www.prenhall.com/kneisl
Companion WebsiteAudio GlossaryNCLEX-RN® Review QuestionsCase Study• Schizophrenia with Auditory HallucinationsCare Plan• Paranoid SchizophreniaVideo• Learning from Clients: SchizophreniaMediaLinksMediaLink Application
Prentice Hall Nursing MediaLink CD-ROMAudio GlossaryNCLEX-RN® Review QuestionsCritical Thinking Exercise• Client with SchizophreniaVideos and Animations• PET/SPECT Schizophrenia• Dystonia (Blepharospasm, Cervical Torticollis)• Bradykinesia (Shuffling Gait)• Akathisia (Legs)• Akinesia & Pill Rolling• Tardive Dyskinesia (Mouth, Trunk, Ambulation)
NCLEX-RN® REVIEW QUESTIONS1. Which of the following client statements demonstrates the
major symptoms of schizophrenia?1. “You can read my mind. This light of mine will shine, fine;
blinding world will end at nine.”2. “I’ve been depressed ever since our house was destroyed
by fire.”3. “I had too much to drink last night, started feeling all-
powerful, and stupidly drove my truck into a tree.”4. “ ‘A stitch in time saves nine’ means that prevention is
easier than fixing a real problem.”
2. A family member asks you, “Since both of my siblings haveschizophrenia, why is my brother’s presentation so differentfrom my sister’s? He withdraws when there’s a change in hisenvironment or routine. She starts cursing and yelling aboutthe Mafia and the CIA when I do something that’s less thanperfect.” Based on your knowledge, your response shouldaddress the:1. Differences in information processing among clients with
schizophrenia.2. Typical progression of symptoms within an individual over
time.3. Effect of gender on clinical presentation in schizophrenia.4. Significance of paranoid content in the differential
diagnosis of paranoid schizophrenia.
3. Which family member statements demonstrate recognition ofthe effects of social pressures associated with schizophrenia?Select all that apply.1. “I’m going to help my family member figure out what to
tell other family members, friends, and business associatesabout why he’s been on medical leave.”
2. “I’ll attend a support group, but I’m afraid my familymember will not go . . . s/he would rather try to ‘pass’ asnot mentally ill.”
3. “Maybe my family member can identify somebody who’sbelievable when that person says, ‘Your symptoms areworse. Let’s go to the psychiatrist’.”
4. “If my family member would just move in with me, itwould be a lot easier for me to maintain my household andcare for my children.”
5. “I used to protect my family member from a lot of the biginterpersonal conflicts in the family, but we need toincrease our expressed emotion.”
4. Which client statements demonstrate acknowledgment of theeffects of psychological pressures associated withschizophrenia? Select all that apply.1. “If I can’t stand the side effects, how will I ask my
psychiatrist to change my medication?”2. “I’m going to look for a job where I can use my college
degree but have less day-to-day stress.”
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 33

34 Unit IV • CLIENTS WITH MENTAL DISORDERS
3. “I have designed a weekly schedule so that I can get tasksdone and have planned time to relax.”
4. “Next month, my sister and I are going to write a grantproposal for a psychiatric day treatment/social center.”
5. “I just want to get back to what I was doing and put thiswhole episode behind me.”
5. You have presented your client with written aftercaremedication directions: “Take one capsule three times per day.”Your client informs you that s/he has reviewed the material.Which response specifically addresses the nurse’s concern foradherence?1. “What might get in the way of taking your medications?”2. “If you forget one dose, you can double the next one.”3. “This medication really works best if you take one capsule
three times per day.”4. “Do you understand everything?”
6. The client with schizophrenia is preparing for discharge. Tominimize relapse, which outcomes are the most important inplanning the client’s care?1. Describes medication regimen accurately and has a specific
plan for obtaining refills2. Identifies three new methods of spending leisure
time3. Lists three potential sources of social support4. Identifies two new ways to bolster self-esteem
7. While you are employed as a charge nurse on an inpatientpsychiatric unit, you recognize that you are choosing to spendless time interacting with the clients with schizophrenia. Yourfirst action is to:1. Reflect on your behavior.2. Force yourself to interact with the clients with
schizophrenia.3. Discuss your observation with your clinical supervisor.4. Request a transfer to another unit.
8. A peer approaches you and shares her frustration with herolder brother, who has had multiple hospitalizations withschizophrenia. “He used to show interest in me, but since hisdischarge 5 days ago, he just stares into space. I cannot get areaction out of him.” Which of the following statements impartaccurate information? Select all that apply.1. “He may be demonstrating flattening of affect and
anhedonia.”2. “He may have sedation or masked facial expressions from
his medications.”3. “Maybe he’s depressed about having a chronic illness.”4. “It’s sad when a loved one does not reciprocate.”5. “Have you confronted him with this?”
9. A nurse is designing a relapse-prevention inpatient group forclients with schizophrenia. Which statements address the twomain categories of nursing activities?1. “If you can increase your self-assessment skills, you’ll be
able to tell when you’re getting more stressed.”2. “We’re going to discuss current events.”3. “Let’s go around the room and have each person say
something positive about our group.”4. “We will go around the room and each person will state a
personal goal for today.”
10. You overhear a family member discussing medicationadherence with your client. Which of the following statementsdo you want to encourage the family member to reiterate?1. “Your support group encourages you to make healthy
choices. Taking your meds is a healthy thing you can doevery day, just like brushing your teeth.”
2. “Your children are getting tired of watching you get sickevery time you stop your meds.”
3. “If you stop taking your medication, I’ll take custody ofyour children.”
4. “You should let these healthcare providers get you well.Why do you fight that?”
See Appendix C for answers.
REFERENCESAllardyce, J., & Boydell, J. (2006). Review: The wider social environment
and schizophrenia. Schizophrenia Bulletin, 32(4), 592–8.American Psychiatric Association. (2000). Diagnostic and statistical manual
of mental disorders (4th ed., Text Revision). Washington, DC: Author.Brookes, K., Xu, X., Chen, W., Zhou, K., Neale, B., Lowe, N., et al. (2006).
The analysis of 51 genes in DSM-IV combined type attention deficit hy-peractivity disorder: Association signals in DRD4, DAT1 and 16 othergenes. Molecular Psychiatry, 11(10), 935–953.
Chafetz, L., White, M. C., Collins-Bride, G., Nickens, J., & Cooper, B. A.(2006). Predictors of physical functioning among adults with severe men-tal illness. Psychiatric Services, 57(2), 225–31.
Connor, S., & Wilson, R. (2006). It’s important that they learn from us formental health to progress. Journal of Mental Health, 15(4), 461–74.
Donohoe, G., Clarke, S., Morris, D., Nangle, J. M., Schwaiger, S., Gill, M.,et al. (2006). Are deficits in executive sub-processes simply reflecting
more general cognitive decline in schizophrenia? Schizophrenia Research,85(1-3), 168–173.
Eastwood, S. L., & Harrison, P. J. (2006). Cellular basis of reduced corticalreelin expression in schizophrenia. American Journal of Psychiatry,163(3), 540–542.
England, M. (2006). Cognitive intervention for voice hearers. Issues in Men-tal Health Nursing, 27(7), 735–751.
Grant, A. (2006). Cognitive remediation therapy for schizophrenia: Theory &practice. Journal of Mental Health, 15(2), 259.
Griner, D., & Smith, T. B. (2006). Culturally adapted mental health interven-tion: A meta-analytic review. Psychotherapy: Theory, Research, Practice,Training, 43(4), 531–548.
Harrison, P. J., & Law, A. J. (2006). Neuregulin 1 and schizophrenia: Genet-ics, gene expression, and neurobiology. Biological Psychiatry, 60(2),132–140.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 34

Chapter 16 • Schizophrenia and Other Psychotic Disorders 35
Haynes, R. B., Yao, X., Degani, A., Kripalani, S., Garg, A., & McDonald, H. P. (2006). Interventions for enhancing medication adherence. TheCochrane Library, 4–163.
Hunt, I. M., Kapur, N., Windfuhr, K., Robinson, J., Bickley, H., Flynn, S., etal.. (2006). Suicide in schizophrenia: Findings from a national clinical sur-vey. Journal of Psychiatric Practice, 12(3), 139–47.
Isherwood, T., Burns, M., & Rigby, G. (2006). A qualitative analysis of the‘management of schizophrenia’ within a medium-secure service for menwith learning disabilities. Journal of Psychiatric & Mental Health Nurs-ing, 13(2), 148–56.
Joseph, J., & Leo, J. (2006). Genetic relatedness and the lifetime risk forbeing diagnosed with schizophrenia: Gottesman’s 1991 figure 10 recon-sidered. Journal of Mind and Behavior, 27(1), 73–90.
Karayiorgou, M., & Gogos, J. A. (2006). Schizophrenia genetics: Uncover-ing positional candidate genes. European Journal of Human Genetics,14(5), 512–519.
Kelly, D. L., & Conley, R. R. (2006). A randomized double-blind 12-weekstudy of quetiapine, risperidone or fluphenazine on sexual functioning inpeople with schizophrenia. Psychoneuroendocrinology, 31(3), 340–346.
Kelly, D. L., Dixon, L. B., Kreyenbuhl, J. A., Medoff, D., Lehman, A. F.,Love, R. C., et al. (2006). Clozapine utilization and outcomes by race in apublic mental health system: 1994-2000. Journal of Clinical Psychiatry,67(9), 1404–1411.
Kessler, R. C., Chiu, W. T., Demler, O., & Walters, E. E. (2005). Prevalence,severity, and comorbidity of twelve-month DSM-IV disorders in the Na-tional Comorbidity Survey Replication (NCS-R). Archives of GeneralPsychiatry, 62(6), 617–627.
Kymalainen, J. A., Weisman, A. G., Rosales, G. A., & Armesto, J. C. (2006).Ethnicity, expressed emotion, and communication deviance in familymembers of patients with schizophrenia. Journal of Nervous & MentalDisease, 194(6), 391–396.
Lee, S., Lee, J., Lee, B., & Kim, Y. H. (2007). A 12-week, double-blind,placebo-controlled trial of galantamine adjunctive treatment to conven-tional antipsychotics for the cognitive impairments in chronic schizophre-nia. International Clinical Psychopharmacology, 22(2), 63–68.
Margetic, B., Aukst-Margetic, B., & Zarkovic-Palijan, T. (2006). Successfultreatment of polydipsia, water intoxication, and delusional jealousy in analcohol dependent patient with clozapine. Progress in Neuro-Psychophar-macology & Biological Psychiatry, 30(7), 1347–1349.
Meyer-Lindenberg, A., Nichols, T., Callicott, J. H., Ding, J., Kolachana, B.,Buckholtz, J., et al. (2006). Impact of complex genetic variation in COMTon human brain function. Molecular Psychiatry, 11(9), 867–877.
Montgomery, P., Tompkins, C., Forchuk, C., & French, S. (2006). Keepingclose: Mothering with serious mental illness. Journal of Advanced Nurs-ing, 54(1), 20–28.
Muñoz, C., & Hilgenberg, C. (2006). Ethnopharmacology: Understandinghow ethnicity can affect drug response is essential to providing culturallycompetent care. Holistic Nursing Practice, 20(5), 227–234.
Netto, G. (2006). Creating a suitable space: a qualitative study of the culturalsensitivity of counselling provision in the voluntary sector in the UK.Journal of Mental Health, 15(5), 593–604.
Nicodemus, K. K., Luna, A., Vakkalanka, R., Goldberg, T., Egan, M., Straub,R. E., et al. (2006). Further evidence for association between ErbB4 andschizophrenia and influence on cognitive intermediate phenotypes inhealthy controls. Molecular Psychiatry, 11(12) 1062–1065.
Paz, R. D., Andreasen, N. C., Daoud, S. Z., Conley, R., Roberts, R., Bustillo,J., et al. (2006). Increased expression of activity-dependent genes in cere-bellar glutamatergic neurons of patients with schizophrenia. AmericanJournal of Psychiatry, 163(10), 1829–1831.
Riley, B., & Kendler, K. S. (2006). Molecular genetic studies of schizophre-nia. European Journal of Human Genetics, 14(6), 669–680.
Rosenberg, J., & Rosenberg, S. (Eds.). (2006). Community mental health:Challenges for the 21st century. New York: Routledge.
Segrin, C. (2006). Family interactions and well-being: Integrative perspec-tives. Journal of Family Communication, 6(1), 3–21.
Stroup, T. S., Lieberman, J. A., McEnvoy, J. P., Swartz, M. S., Davis, S. M.,Rosenheck, R. A., et al. (2006). Effectiveness of olanzapine, quetiapine,risperidone, and ziprasidone in patients with chronic schizophrenia fol-lowing discontinuation of the previous atypical antipsychotic. AmericanJournal of Psychiatry, 163(4), 611–622.
Szeszko, P. R., Lipsky, R., Mentschel, C., Robinson, D., Gunduz-Bruce, H.,Sevy, S., et al. (2005). Brain-derived neurotrophic factor val66met poly-morphism and volume of the hippocampal formation. Molecular Psychia-try, 10(7), 631–636.
Thomas, P., Seebohm, P., Henderson, P., Munn-Giddings, C., & Yasmeen, S.(2006). Tackling race inequalities: Community development, mentalhealth and diversity. Journal of Public Mental Health, 5(2), 13–19.
Tunbridge, E. M., Weinberger, D. R., & Harrison, P. J. (2006). A novel pro-tein isoform of catechol O-methyltransferase (COMT): Brain expressionanalysis in schizophrenia and bipolar disorder and effect of Valsuper-script 1-sup-5-sup-8Met genotype. Molecular Psychiatry, 11(2),116–117.
Uko-Ekpenyong, G. (2006). Improving medication adherence with orallydisintegrating tablets. Nursing, 36(9), 20–21.
van Meijel, B., Kruitwagen, C., van der Gaag, M., Kahn, R. S., & Gryp-donck, M. H. F. (2006). In intervention study to prevent relapse in patientswith schizophrenia. Journal of Nursing Scholarship, 38(1), 42–49.
Weisman, A. G., Rosales, G. A., Kymalainen, J. A., & Armesto, J. C. (2006).Ethnicity, expressed emotion, and schizophrenia patients’ perceptions oftheir family members’ criticism. Journal of Nervous & Mental Disease,194(9), 644–649.
Wilson, W. H. (2006). Neuropsychiatric perspectives for community mentalhealth theory and practice. In J. Rosenberg & S. Rosenberg (Eds.),Community mental health: Challenges for the 21st century (pp. 83–100).New York: Routledge.
Kneisl booklet v4 QX6 11/30/07 6:17 PM Page 35

Accompanying the textbook are complete student and instructor learning packages to aid studentsin learning, retaining, and applying classroom presentations and aids for class preparation andmanagement. All student and instructor material is organized by chapter.
Student Assessment . . . Customized Study Plans . . .
The path to student success and nursing excellence in psychiatric-mental health!MyNursingLab is a user-friendly site that gives students the opportunity to test themselves on keyconcepts and skills in psychiatric-mental health nursing. By using MyNursingLab, students cantrack their own progress through the course and use the personalized, media-rich, study planactivities to help them achieve success in the classroom, in clinical, and ultimately on theNCLEX-RN®. MyNursingLab can also help instructors monitor class progress as students movethrough the curriculum.
To take a tour and see the power of go to www.mynursinglab.com
STUDENT RESOURCES
Prentice Hall Nursing MediaLink CD-ROM Accompanies your textbook andprovides review questions, video and animations, an audio glossary, and a concept mapping tool.
Companion Website Includes review questions, case studies, care plans, web links, andother exercises and resources.
INSTRUCTOR RESOURCES
Instructor’s Resource Manual This valuable resource provides classroom material linkedto each chapter in the textbook. It includes Concepts for Lecture, PowerPoint® lecture slides,Classroom Activities, and Clinical Activities for each learning outcome. Also contains a completetestbank with rationales, cognitive levels, level of client care, and step of the nursing process, allwritten in NCLEX-RN® style.
Instructor’s Resource CD-ROM Included on this faculty tool are PowerPoint® lectureslides with images and video embedded to accompany each chapter. Also on this disk are theTestGen testbank questions and video and animations from the student CD-ROM.
OneKey Online Course Management Available in WebCT, Blackboard, Angel, Moodle,and other applications is this useful resource for online course learning and management. Includedare interactive modules with PointPoint® lecture slides, review questions, case studies, care plans,and more.
RESOURCES FOR STUDENT AND INSTRUCTOR SUCCESS
Kneisl booklet v4 QX6 11/30/07 6:33 PM Page 36