Embed Size (px)
Citation preview

Schizophrenia and OtherPsychotic Disorders
SCHIZOPHRENIAThe Epidemiology of SchizophreniaOrigins of the Schizophrenia Construct
THE CLINICAL PICTURE IN SCHIZOPHRENIADelusionsHallucinationsDisorganized SpeechDisorganized and Catatonic BehaviorNegative Symptoms
WHAT CAUSES SCHIZOPHRENIA?Genetic AspectsPrenatal ExposuresGenes and Environment in Schizophrenia:
A SynthesisA Neurodevelopmental PerspectiveBiological AspectsNeurocognitionPsychosocial and Cultural Aspects
SUBTYPES OF SCHIZOPHRENIAParanoid TypeDisorganized TypeCatatonic TypeUndifferentiated TypeResidual Type
TREATMENT AND CLINICAL OUTCOMEPharmacological ApproachesPsychosocial Approaches
UNRESOLVED ISSUES:Can Schizophrenia Be Prevented?

SCHIZOPHRENIAWhen we think of severe mental illness, in all probabilitywe think of schizophrenia. Schizophrenia occurs in peoplefrom all cultures and from all walks of life, and its charac-teristic symptoms have long been recognized. The disorderis characterized by an array of diverse symptoms, includ-ing extreme oddities in perception, thinking, action, senseof self and manner of relating to others. However, the hall-mark of schizophrenia is a significant loss of contact withreality, referred to as psychosis. Although the clinical pre-sentation of schizophrenia differs from one patient toanother, the case of Emilio is quite typical.
Emilio: "Eating Wires andLighting Fires"
Emiliois a 40-year-old man who looks 10 years younger.He is brought to the hospital, his twelfth hospitalization,by his mother because she is afraid of him. He is dressedin a ragged overcoat, bedroom slippers, and a baseballcap, and he wears several medals around his neck. Hisaffect ranges from anger at his mother ("She feeds meshit ... what comes out of other people's rectums") to agiggling, obsequious seductiveness toward the inter-viewer. His speech and manner have a childlike quality,and he walks with a mincing step and exaggerated hipmovements. His mother reports that he stopped takinghis medication about a month ago and has since begun tohear voices and to look and act more bizarrely. Whenasked what he has been doing, he says "eating wires andlighting fires." His spontaneous speech is often incoher-ent and marked by frequent rhyming and clang associa-tions (speech in which sounds, rather than meaningfulrelationships, govern word choice).
Emilio's first hospitalization occurred after hedropped out of school at age 16, and since that time hehas never been able to attend school or hold a job. Hehas been treated with neuroleptics (medications used totreat schizophrenia) during his hospitalizations, but hedoesn't continue to take his medications when he leaves,so he quickly becomes disorganized again. He lives withhis elderly mother, but he sometimes disappears for sev-eral months at a time and is eventually picked up by thepolice as he wanders the streets. There is no known his-tory of drug or alcohol abuse. (Modified from Spitzeret aI., 2002, pp. 189-90.)
Source: Adaptedwithpermissionfromthe DSM-TR-Casebook:A Learning Companion to the Diagnostic and Statistical ManualofMental Disorders, FourthEdition,TextRevision(Copyright2002). AmericanPsychiatricPublishing,Inc.
This chapter describes the pieces of the schizophreniapuzzle as we now know them. It is important that you bearin mind from the outset that not all of the pieces or theirpresumed interconnections have been found, so our puz-zle is far from being solved. You will recognize just howchallenging and complex this disorder is-not only forpatients who suffer from it and for their families who try tocare for them, but also for the clinicians who attempt totreat it and the researchers who are determined to under-stand it.
The Epidemiology ofSchizophreniaMany people are surprised to learn that schizophrenia isabout as prevalent as epilepsy. The lifetime morbid risk fordeveloping schizophrenia is widely accepted to be around1.0 percent (Gottesman, 1991). What this means is that 1out of every 100 people born today who survive until atleast age 55 will develop the disorder. Of course, a statisticlike this does not mean that everyone has exactly the samerisk. This is an average lifetime risk estimate. As we shall seelater, some people (e.g., those who have a parent with
The internal suffering of the person with schizophrenia is oftenreadily apparent, as are bizarre behavior and unusualappearance.

Children whose fathers are older at the time of their birth have 2 to3 times the normal risk of developing schizophrenia.
schizophrenia) have a statistically higher risk of developingthe disorder than do others (e.g., people who come fromfamilies where there has never been a case of schizophre-nia). There are also other groups of people who seem tohave an especially high risk of developing schizophrenia.For example, people whose fathers were older (aged 45-50years or more) at the time of their birth have two to threetimes the normal risk of developing schizophrenia whenthey grow up (Byrne et al., 2003; Malaspina et al., 2001).Moreover, people of Afro-Caribbean origin living in theUnited Kingdom seem to have higher-than-expected ratesof schizophrenia (Harrison et al., 1997). Rates of schizo-phrenia also seem to be unexpectedly high in westernIreland and Croatia and especially low in Papua NewGuinea (Gottesman, 1991). The Hutterites, a Christian sectthat migrated to the United States from Europe in the late
1800s, also show a low prevalence of schizophrenia (Nim-gaonkar et al., 2000). At present, we have little idea aboutwhy this should be, although such differences are of greatinterest to researchers.
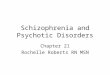
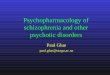
The vast majority of cases of schizophrenia begin inlate adolescence and early adulthood. Although schizo-phrenia is sometimes found in children, such cases are rare(Green et al., 1992; McKenna et al., 1994). Schizophreniacan also have its initial onset in middle age or later, butagain, this is not typical. Interestingly, schizophrenia tendsto begin earlier in men than in women. In men, there is apeak in new cases of schizophrenia between ages 20 and 24.The incidence of schizophrenia in women peaks duringthe same age period, but the peak is less marked than it isfor men. After about age 35, the number of men develop-ing schizophrenia falls markedly, whereas the number ofwomen developing schizophrenia does not. Instead, thereis a second rise in new cases that begins around age 40. Thisis shown in Figure 14.1. Overall, the average age of onset ofschizophrenia is around 25 years for men and around 29years for women (Jablensky & Cole, 1997).
In addition to having an earlier age of onset of schiz-ophrenia, many investigators believe that males develop amore severe form of the disorder (Leung & Chue, 2000).That belief is consistent with a brain-imaging study byNopoulos, Flaum, and Andreasen (1997) showing thatschizophrenia-related anomalies of brain structure (dis-cussed later) are more severe in male than in femalepatients. Gender-related differences in illness severitymay explain why some researchers have found that schiz-ophrenia is becoming more common in males than infemales (Iacono & Beiser, 1992). If women have a lesssevere form of schizophrenia, and if they also have moresymptoms of depression (see Leung & Chue, 2000), theymay either not be diagnosed at all or be diagnosed withother disorders.
30-Males n=117
25-Females n = 131
CLI 20ll/)III.•..c 15CLI...•..CLIc- 10
o12-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59
Age group
Age distribution of onset ofschizophrenia (first sign of mentaldisorder) for men and women.Source: Haffneret 01. (1998).

What might explain the better clinical outcome ofwomen with schizophrenia? One possibility is that femalesex hormones play some protective role. When estrogenlevels are low (as is true premenstrually) or are falling, psy-chotic symptoms in women with schizophrenia often getworse (Lindamer et al., 1997). The protective effect ofestrogen may therefore help explain the delayed onset ofschizophrenia in women. Declining levels of estrogenaround menopause might also explain why late-onsetschizophrenia is much more likely to strike women thanmen. And there is some evidence that this late-onset pat-tern in women is associated with a more severe clinicalpresentation (Haffner et al., 1998).
Origins of the SchizophreniaConstructThe first detailed clinical description of what we now rec-ognize to be schizophrenia was offered in 1810 by JohnHaslam, the apothecary at the Bethlem Hospital in Lon-don, England. Haslam described the case of James TillyMatthews, a married tea merchant with two children.Matthews was admitted to Bethlem in 1797, and heappears to have suffered from a variety of symptoms thatare typical of schizophrenia. He was delusional, andHaslam noted that Matthews believed that "in some apart-ment near London Wall, there is a gang of villains pro-foundly skilled in Pneumatic Chemistry who assail him bymeans of an Air Loom" (as cited in Carpenter, 1989). Fiftyyears later, the Belgian psychiatrist Benedict Moreldescribed the case of a 13-year-old boy who had formerlybeen the most brilliant pupil in his school but who gradu-ally lost interest in his studies; became increasingly with-drawn, lethargic, seclusive, and quiet; and appeared to haveforgotten everything he had learned. He talked frequentlyof killing his father. Morel thought the boy's intellectual,moral, and physical functions had deteriorated as a resultof brain degeneration of hereditary origin and hence wereirrecoverable. He used the term demence precoce (mentaldeterioration at an early age) to describe the condition andto distinguish it from the dementing disorders associatedwith old age.
It is the German psychiatrist Emil Kraepelin(1856-1926) who is best known for his careful descriptionof what we now regard as schizophrenia. In 1896, Krae-pelin (like Morel) used the term dementia praecox to referto a group of conditions that all seemed to feature mentaldeterioration beginning early in life. Kraepelin, an astuteobserver of clinical phenomena, described the patient withdementia praecox as someone who "becomes suspicious ofthose around him, sees poison in his food, is pursued bythe police, feels his body is being influenced, or thinks thathe is going to be shot or that the neighbours are jeering athim" (Kraepelin, 1896). Kraepelin also noted that the dis-order was characterized by hallucinations, apathy andindifference, withdrawn behavior, and an incapacity forregular work.
The term that has survived into today's diagnosti<;nomenclature was introduced in 1911 by a Swiss psychia-trist named Eugen Bleuler (1857-1939). Bleuler usedschizophrenia (from the German schizien, meaning "tosplit;' and phren, from the Greek root meaning "mind")because he believed the condition was characterized pri-marily by disorganization of thought processes, a lack ofcoherence between thought and emotion, and an inwardorientation away (split off) from reality. Although the termis often thought to reflect a "Jekyll and Hyde" split person-ality, this is a major misconception. The splitting does notrefer to multiple personalities (an entirely different form ofdisorder now called "dissociative identity disorder" anddiscussed in Chapter 8). Instead, in schizophrenia there is asplit within the intellect, between the intellect and emo-tion, and between the intellect and external reality. Inter-estingly, the subtitle of Bleuler's monograph (Bleuler,1911/1950) was "The Group of Schizophrenias;' indicatingthat he believed this disorder was not a single diagnosticentity.
In ReVIew~ What is the prevalence of schizophrenia?
What groups of people show lower or higherrates of schizophrenia than expected?
~ When does the initial onset of schizophreniausually occur? How does this vary by gender?
~ How does gender influence the severity ofschizophrenia? Why might this be?
~ What did Kraepelin mean by the termdementia praecox? How accurate is thisdescription?
~ What was Bleuler's use of the termschizophrenia meant to convey?
~ Is schizophrenia the same thing as splitpersonality?
THE CLINICAL PICTUREIN SCHIZOPHRENIAAs we have mentioned earlier, the DSM is a work inprogress. Diagnostic criteria are not fixed and immutablebut instead change subtly over time as new research find-ings become available. The current DSM -IV-TR criteriafor the diagnosis of schizophrenia are listed in the table onpage 493. These are very similar to the diagnostic criteria inthe ICD (WHO, 1992), which is the diagnostic system usedin Europe and other parts of the world. In isolation, how-ever, lists of symptoms convey little about the clinical

essence of schizophrenia. In the sections that follow, weelaborate on the hallmark symptoms of this major form ofpsychotic disorder.
A delusion is essentially an erroneous belief that is fixedand firmly held despite clear contradictory evidence. Theword delusion comes from the Latin verb ludere, whichmeans "to play." In essence, tricks are played on the mind.People with delusions believe things that others who sharetheir social, religious, and cultural backgrounds do notbelieve. A delusion therefore involves a disturbance in thecontent of thought. Not all people who have delusions suf-fer from schizophrenia. However, delusions are commonin schizophrenia, occurring in more than 90 percent ofpatients at some time in their illness (Cutting, 1995). Inschizophrenia, certain types of delusions or false beliefs arequite characteristic. Prominent among these are beliefsthat one's thoughts, feelings, or actions are being con-trolled by external agents (made feelings or impulses), thatone's private thoughts are being broadcast indiscrimi-nately to others (thought broadcasting), that thoughts arebeing inserted into one's brain by some external agency(thought insertion), or that some external agency hasrobbed one of one's thoughts (thought withdrawal). Alsocommon are delusions of reference, where some neutralenvironmental event (such as a television program or asong played on the radio) is believed to have special andpersonal meaning intended only for the patient. Otherstrange propositions, including delusions of bodilychanges (e.g., bowels do not work) or removal of organs,are also not uncommon.
A hallucination is a sensory experience thatoccurs in the absence of any external perceptualstimulus. This is quite different from an illusion,which is a misperception of a stimulus that actu-ally exists. Hallucinations can occur in any sen-sory modality (auditory, visual, olfactory,tactile, or gustatory). However, auditory halluci-nations (e.g., hearing voices) are by far the mostcommon, being present in up to 75 percent ofpatients with schizophrenia (Wing et aI., 1974).In contrast, visual hallucinations occur less fre-quently (15 percent of patients), and tactile hal-lucinations are even more rare (Cutting, 1995).Hallucinations often have relevance for thepatient at some affective, conceptual, or behav-ioral level. Patients can become emotionallyinvolved in their hallucinations, often incorpo-rating them into their delusions. In some cases,patients may even act on their hallucinationsand do what the voices tell them to do (Stern &Silbersweig,1998).
I 493
Criteria for the Diagnosis ofSchizophrenia
~ Two or more of the following symptoms, present for asignificant portion of time during a 1-month period (less ifsuccessfully treated):
(1) Delusions.
(2) Hallucinations.
C3) Disorganized speech.
(4) Grossly disorganized or catatonic behavior.
(5) Negative symptoms.
(Only one symptom is required if the delusions are bizarreor if the hallucinations consist of a voice keeping up arunning commentary on the person's behavior or thoughts,or two or more voices conversing with each other.)
~ Dysfunction in work, interpersonal relations, or self-care.
~ Signs of disturbance for at least 6 months, with at least 1month of symptoms listed above.
Source: Adapted with permission from the Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition, Text Revision(Copyright 2000). American Psychiatric Association.
In an interesting study of the phenomenology of audi-tory hallucinations, Nayani and David (1996) interviewed100 hallucinating patients and asked them a series of ques-tions about their hallucinatory voices. The majority ofpatients (73 percent) reported that their voices usuallyspoke at a normal conversational volume. Hallucinatedvoices were often those of people known to the patient in
The inner world of people with schizophrenia is often confused, punctuated byalien voices, paranoia, and illogical thoughts.

real life, although sometimes unfamiliar voices or thevoices of God or the Devil were also heard. Most patientsreported that they heard more than one voice and thattheir hallucinations were worse when they were alone.Most commonly, the hallucinated voices uttered rude andvulgar expletives or else were critical ("You are stupid"),bossy ("Get the milk"), or abusive ("Ugly bitch"), althoughsome voices were pleasant and supportive ("My darling").
Are patients who are hallucinating really hearingvoices? Neuroimaging studies of hallucinating patients arebeginning to provide some answers to this interestingquestion. Several research groups have used PET and fMRIto look at activity in the brains of patients when they areactually experiencing auditory hallucinations (Cleghornet al., 1992; McGuire et al., 1996). Although it might beexpected that patients hearing voices would show anincrease of activity in areas of the brain involved in speechcomprehension (e.g., Wernicke's area in the temporallobe), imaging studies show that hallucinating patientsshow increased activity in Broca's area-an area of thetemporal lobe that is involved in speech production. Insome cases, the pattern of brain activation that occurswhen patients experience auditory hallucinations is verysimilar to that seen when healthy volunteers are asked toimagine that there is another person talking to them(Shergill et al., 2000). Overall, the research findings suggestthat auditory hallucinations occur when patients misinter-pret their own self-generated and verbally mediatedthoughts (inner speech or self-talk) as coming fromanother source. Indeed, if trans cranial magnetic stimula-tion (where a magnetic field passing through the skulltemporarily disrupts activity in underlying brain areas) isused to reduce activity in speech production areas, halluci-nating patients actually show a reduction in their auditoryhallucinations (Hoffman et al., 200S)! Modern technol-ogy is thus supporting a very old idea: Auditory halluci-nations are really a form of misperceived subvocal speech(Gould, 1949).
Disorganized SpeechDelusions reflect a disorder of thought content. Disorga-nized speech, on the other hand, is the external manifesta-tion of a disorder in thought form. Basically, an affectedperson fails to make sense, despite seeming to conform tothe semantic and syntactic rules governing verbal commu-nication. The failure is not attributable to low intelligence,poor education, or cultural deprivation. Years ago, Meehl(1962) aptly referred to the process as one of "cognitiveslippage"; others have referred to it as "derailment" or"loosening" of associations or, in its most extreme form, as"incoherence."
In disorganized speech, the words and word combina-tions sound communicative, but the listener is left with lit-tle or no understanding of the point the speaker is trying tomake. In some cases, completely new made-up words
known as "neologisms" (literally, "new words") appear inthe patient's speech. An example might be the word detone,which looks and sounds like a meaningful word but is aneologism. Formal thought disorder is well illustrated inthe following example, which is taken from a letter writtenby a man with schizophrenia and addressed to QueenBeatrix of the Netherlands.
Disorganized Speech: ALetter to Queen Beatrix
I have also "killed" my ex-wife, [name), in a 2.5 to 3.0hours sex bout in Devon Pennsylvania in 1976, while twoPitcairns were residing in my next room closet, hearingthe event. Enclosed, please find my urology report, indi-cating that my male genitals, specifically my penis, arewithin normal size and that I'm capable of normal inter-course with any woman, signed by Dr. [name), a urologistand surgeon who performed a circumcision on me in1982. Conclusion: I cannot be a nincompoop in a physicalsense (unless Society would feed me chemicals for mypicture in the nincompoop book).
Disorganized and Catatonic BehaviorGoal-directed activity is almost universally disrupted inschizophrenia. The impairment occurs in areas of routinedaily functioning, such as work, social relations, and self-care, such that observers note that the person is not him-self or herself anymore. The picture is thus one ofdeterioration from a previously mastered standard of per-formance in everyday affairs. For example, the person mayno longer maintain minimal standards of personal hygieneor may exhibit a profound disregard of personal safetyand health. In other cases, grossly disorganized behaviorappears as silliness or unusual dress (e.g., wearing an over-coat, scarf, and gloves on a hot summer day). Manyresearchers attribute these disruptions of "executive"behavior to some sort of impairment in the functioning ofthe prefrontal region of the cerebral cortex (Lenzenweger& Dworkin, 1998).
Catatonia is an even more striking behavioral distur-bance. The patient with catatonia may show a virtualabsence of all movement and speech and be in what iscalled a catatonic stupor. At other times, the patient mayhold an unusual posture for an extended period of timewithout any seeming discomfort.
Negative SymptomsSince the days of Bleuler, two general symptom patterns orsyndromes of schizophrenia have been differentiated.These are referred to as positive- and negative-syndrome

schizophrenia (e.g., Andreasen, 1985; Andreasen et aI.,1995). Statistical procedures have further indicated thatsome symptoms like disordered speech and disorganizedbehavior that were previously thought to reflect positivesymptoms might be better separated from "true" positivesymptoms like hallucinations and delusions. A disorga-nized symptom pattern is now also recognized (Lenzen-weger et aI., 1991). These symptom types are illustrated inTable 14.l.
Positive symptoms are those that reflect an excess ordistortion in a normal repertoire of behavior and experi-ence such as delusions and hallucinations. Negative symp-toms, by contrast, reflect an absence or deficit of behaviorsthat are normally present. Important negative symptomsin schizophrenia include flat or blunted emotional expres-siveness, alogia (very little speech), and avolition (no abil-ity to initiate or persist in goal-directed activities). Instead,the patient may sit for long periods of time staring intospace or watching TV with little interest in any outsidework or social activities.
Although most patients exhibit both positive and neg-ative signs during the course of their disorders (Breieret aI., 1994; Guelfi et al., 1989), a preponderance of nega-tive symptoms in the clinical picture is not a good sign forthe patient's future outcome (e.g., Fenton & McGlashan,1994; McGlashan & Fenton, 1993; Milev et aI., 2005).
Not all negative symptoms are exactly what they seem,however. Kring and Neale (1996) studied unmedicatedmale patients with schizophrenia while they were watchingfilm clips. Three different types of film clips were used, thescenes in them being either very positive, negative, or neu-tral in terms of the emotions they were designed to elicit inthe viewers. Videotapes of how the patients looked whenthey were watching the films were then coded by trainedraters. As might be expected, the patients with schizophre-nia showed less facial expressiveness than a group ofhealthy controls.
What was surprising was that when the patientswere asked about their emotional experiences during thefilms, they reported as much emotional feelings as thecontrols-and sometimes slightly more. Measures of
Positive and negative symptoms can co-occur in the same patient.This woman appears to exhibit marked social withdrawal (anegative symptom) in addition to showing bizarre behavior (apositive symptom).
autonomic arousal also showed that when they werewatching the films, the patients exhibited more physio-logical reactivity than the controls did. What these find-ings suggest, therefore, is that even though patients withschizophrenia may sometimes not look very emotionallyexpressive, they are nonetheless experiencing plenty ofemotion.
In ReVIew~ Explain the difference between positive and
negative symptoms.~ What are the major symptoms of
schizophrenia?~ How is a hallucination different from a
delusion?
.' 'PositiveJ Negative, anc"Di~'brg~niz~d Symptoms . - .'~ ...·,"~f.Schiz~phrenia . 1.1 .~., [
Positive SymptomsHallucinationsDelusions
Negative SymptomsEmotional flatteningPoverty of speechAsocialityApathyAnhedonia
Disorganized SymptomsBizarre behaviorDisorganized speech

SUBTYPES OFSCHIZOPHRENIAWhat we call "schizophrenia" in all probability encom-passes a variety of disordered processes of varied etiology,developmental pattern, and outcome-perhaps more sothan in the case of any other psychiatric diagnosis. Thisleads to much heterogeneity at the clinical, observationallevel. Sociocultural factors also shape the clinical presenta-tion of the disorder. For example, compared to Mexican-American patients, Anglo-American patients withschizophrenia report fewer somatic symptoms, have moreblunted affect, and exhibit more self-neglect. They alsohave more persecutory delusions and delusions that have abasis in science fiction or the supernatural (Weisman et aI.,2000). Current classification systems have long attemptedto recognize the heterogeneity in the presentation of schizo-phrenia by describing clinical subtypes of the disorder.
The DSM -IV recognizes several subtypes of schizo-phrenia. However, questions have been raised about theoverall usefulness of subtyping patients. For example,there is no strong evidence that such information is helpfulwhen it comes to planning treatment. Despite this,researchers and clinicians remain interested in exploringand refining possible subtypes of schizophrenia, perhapsbecause they hope such an approach will eventually yieldinsights into the etiology of the disorder.
Paranoid TypeThe patient with paranoid schizophrenia shows a historyof increasing suspiciousness and of severe difficulties ininterpersonal relationships. The eventual clinical picture isdominated by absurd and illogical ideas and beliefs that areoften highly elaborated and organized into a coherent,though delusional, framework. Persecutory delusions arethe most frequent and may involve a wide range of bizarreideas and plots. An individual may become highly suspi-cious of relatives or associates and may complain of beingwatched, followed, poisoned, talked about, or influenced byvarious tormenting devices rigged up by "enemies." Delu-
, I
DSM-IV-TR,I
~ Preoccupation with delusions or frequent auditoryhallucinations.
~ No evidence of marked disorganized speech, disorganizedor catatonic behavior, flat or inappropriate affect.
sions of grandeur are also common in paranoid schizo-phrenia. Persons with such delusions may, for example,claim to be the world's greatest economist or philosopher,to have invented some impossible device, or to be a promi-nent person from the past. In some cases, this provides thejustification (in the mind of delusional persons) for theirbeing persecuted, followed, or spied upon, and it may pro-vide a sense of identity and importance not otherwiseattainable. Patients with the paranoid subtype of schizo-phrenia tend to function at a higher level overall and also tohave more intact cognitive skills than patients with othersubtypes, although the differences are not large and are notconsistent across all cognitive domains (Zalewski et aI.,1998). The prognosis for these patients is generally betterthan for patients with other types of schizophrenia (Fenton& McGlashan, 1991; Kendler, McGuire, et aI., 1994).
The next clinical example will give you some sense ofwhat a complex and highly elaborated delusional system islike. It was printed on a flier and handed to one of theauthors by a man who appeared to be in his thirties. Anyerrors of grammar are errors in the original flier.
Are You Being MindControlled?
Are you being or were you mind controlled to do some-thing very stupid? Twenty-five percent of our populationhave what is called electronic hearing. This twenty-fivepercent can hear a silent radio and do not hear it. Youmight be one. In hearing pitch the average person hearsfrom zero to sixteen thousand cycles. Twenty-fivepercentcan hear up to thirty thousand cycles. The silent radio canbe heard by these high hearing frequency persons. Thesilent radio sounds the same as thoughts in their minds.
This silent radio tricks these persons into everycrime imaginable. It tricks them into bad decisions, toquit jobs, to divorce, to run away, to be sheriff saled andany stupidity possible. The broadcasters over this silentradio are government, medical, psychiatrists, religiousand educational. This is an enormous budget used todestroy the innocent and helpless. The media is scared tocover this up.
This minority,which can be in any ethnic or race, haslost all rights under law because the Russians do it every-where. It is shocking to discover very large corporation andall college have mind control departments. Ifyou and yourfamily constantly make bad decisions and have ruinousproblems, you probably are mind controlled. Every yearthese mind controlled people are going down the eco-nomic ladder as they cannot be trusted. No companyknows when one will be selected as a guinea pig. Whocould risk a sizeable work force of persons with electronichearing for your competitor could easily wipe you out?

Disorganized TypeCompared with the other subtypes of schizophrenia,disorganized schizophrenia usually occurs at an earlierage and has a gradual, insidious onset. As you can see fromthe table for criteria for disorganized schizophrenia, it ischaracterized by disorganized speech, disorganized behav-ior, and flat or inappropriate affect. In the past (and cur-rently in the ICD) this subtype was called "hebephrenicschizophrenia." The case study of Emilio that you read ear-lier is an example of this subtype. Very gradually, the per-son becomes more reclusive and preoccupied withfantasies. As the disorder progresses, the clinical picture isone of emotional indifference and infantile behavior. Asilly smile and inappropriate, shallow laughter after littleor no provocation are common symptoms. Speechbecomes difficult to understand and may include consid-erable baby talk, childish giggling, and a repetitious use ofsimilar-sounding words. Hallucinations and delusionsmay be present, but in contrast to paranoid schizophrenia,
these are not coherentor organized into a"story." Patients withdisorganized schizo-phrenia may have severedisruptions in their abil-ities to take care of them-selves and be unable toperform routine tasks.They sometimes alsoshow peculiar manner-isms and other bizarreforms of behavior.These behaviors maytake the form of oddfacial grimaces, talkingand gesturing to them-selves, or sudden, inex-plicable laughter andweeping. The prognosis
is generally poor for individuals who develop disorganizedschizophrenia. At this stage of deterioration, no form oftreatment intervention yet discovered has a high likelihoodof effecting more than modest gains.
People with the disorganizedtype of schizophrenia becomeemotionally indifferent andinfantile and may display oddfacial grimaces, talk andgesture to themselves, andbreak into sudden, inexplicablelaughter and weeping.
Catatonic TypeThe central feature of catatonic schizophrenia (see thetable for criteria for catatonic schizophrenia) is pro-nounced motor signs, either of an excited or a stuporoustype. Some of these patients are highly suggestible and willautomatically obey commands or imitate the actions ofothers (echopraxia) or mimic their phrases (echolalia).Even if a patient's arm is raised to an awkward and uncom-fortable position, he or she may keep it there for minutesor even hours. Ordinarily, patients in a catatonic stuporstubbornly resist any effort to change their position, may
. I
DSM-IV-TR
~ Disorganized speech.
~ Disorganized behavior.
~ Flat or inappropriate affect.
•. No evidence of catatonic schizophrenia.
become mute, resist all attempts at feeding, and refuse tocomply with even the slightest request. Catatonic patientsmay pass suddenly from extreme stupor to a state of greatexcitement, during which they seem to be under great"pressure of activity" and may become violent, being inthese respects indistinguishable from some bipolar manicpatients. They may talk or shout excitedly and incoher-ently, pace rapidly back and forth, openly indulge in sexualactivities, attempt self-mutilation or even suicide, orimpulsively attack and try to kill others. The suddennessand extreme frenzy of these attacks make such patientsdangerous to both themselves and others. Though at onetime common in Europe and North America, catatonicreactions have become less prevalent in recent years,although 'they are still found in less industrialized regionsof the world (Cutting, 1995).
The matter is far from settled, but some cliniciansinterpret a catatonic patient's immobility as a way of cop-ing with his or her reduced filtering ability and increasedvulnerability to stimulation: It seems to provide a feeling ofsome control over external sources of stimulation, thoughnot necessarily over inner ones. Freeman (1960) has cited
, I, • I
DSMTIV-TRI
In catatonic schizophrenia, the clinical picture is dominated byat least two of the following:
~ Immobile body or stupor.
~ Excessive motor activity that is purposeless and unrelatedto outside stimuli.
•. Extreme negativism (resistance to being moved, or tofollow instructions) or mutism.
~ Assumption of bizarre postures, or stereotypedmovements or mannerisms.
~ Echolalia or echopraxia.

the explanation advanced by one patient: "I did not wantto move, because if I did everything changed around meand upset me horribly so I remained still to hold on to asense of permanence" (p. 932).
Anna, the Student withCatatonic Schizophrenia
Anna is a 22-year-old unmarried student of mathematics inFinland. She was brought to the psychiatric hospital by thepolice after she attacked a child. She had walked up to a 9-year-old girl at a bus stop and tried to strangle her. Somepassersby fortunately intervened, restraining Anna, andcalled the police. At first she fought violently and tried toget at the child, but then suddenly she became motionlessand rigid as a statue, with one arm stretched out towardthe child and a wild stare on her face. When the policearrived, it was very difficult to get her into the car, becauseshe would not move and resisted attempts to move her.
At the police station she said nothing, kept standingin an awkward position, and stared straight ahead. Aphysician decided that an immediate admission to thepsychiatric hospital was appropriate. Anna was put on alocked ward because she was under arrest for attemptedmurder. When she was brought to the ward, she remainedstanding just inside the entrance and resisted invitationsto go farther. She refused to have anything to eat andwould not go into the examination room. She remainedstanding rigid, with her right arm stretched out in front ofher, staring at her hand. She did not answer questions orrespond in any way to the ward assistants. After severalhours she finally had to be taken to her room and put inbed with the use of mild force. She lay in bed in the posi-tion where she had been placed, staring at the ceiling.She seemed tense, with an apprehensive and worriedlook on her face. She was given an injection of 10 mg ofhaloperidol and did not resist. Afterward she fell asleep.
During a clinical interview the next day, Annaappeared to be fully oriented. She knew she was in thehospital but would not or could not explain what had hap-pened. At times she suddenly stiffened and stared for halfa minute or so. At other times she just mechanicallyrepeated the questions that were asked of her.
Anna's sister arrived. She said that the family hadbeen concerned about Anna for some time. For the last 2or 3 months she had seemed reclusive and odd, withrecurrent episodes of muteness that lasted for severalminutes. Several times she made peculiar statementssuch as, "Children are trying to destroy mathematics"and "Rational figures have a hard time." She stoppedgoing to the university and stayed in her room, leaving itonly for a walk in the evening. She seemed to be preoccu-pied with writing numbers on pieces of paper. (Adaptedfrom UstOn et aI., 1996.)
Undifferentiated TypeAs the term implies, the diagnosis of undifferentiatedschizophrenia is something of a wastebasket category. Aperson with undifferentiated schizophrenia (see the tableon criteria for undifferentiated schizophrenia) meets theusual criteria for schizophrenia-including (in varyingcombinations) delusions, hallucinations, disorderedthoughts, and bizarre behaviors-but does not clearly fitinto one of the other types because of a mixed-symptompicture. People in the acute, early phases of a schizophrenicbreakdown frequently exhibit undifferentiated symptoms,as do those whose clinical picture may change enough overtime to warrant a change in diagnosis from a specific sub-type to the undifferentiated subtype.
Residual TypeA final subtype of schizophrenia contained in DSM-IVdeserves brief mention. Residual schizophrenia is a cate-gory used for people who have suffered at least one episodeof schizophrenia but do not now show any prominent pos-itive symptoms such as hallucinations, delusions, or disor-ganized speech or behavior. Instead, the clinical picturecontains mostly negative symptoms (e.g., flat affect),although some positive symptoms (e.g., odd beliefs, eccen-
. 1\' - ,.' ,
"DSM-N-TR .'I •
Criteria for UndifferentiatedSchizophrenia
~ Symptoms of schizophrenia that do not meet criteria forthe Paranoid, Disorganized, or Catatonic types.
1 .
, DSM.- IV-TRII. . •
Criteria for the Residual Type ofSchizophrenia
~ Absence of prominent delusions, hallucinations,disorganized speech, and grossly disorganized or catatonicbehavior.
~ Continued evidence of schizophrenia (e.g., negativesymptoms), or mild psychotic symptoms (e.g., odd beliefs,unusual perceptual experiences).

tric behavior) may also be present in a mild form (see thetable for criteria for residual type schizophrenia).
Other Psychotic DisordersSCHIZOAFFECTIVE DISORDER The DSM-IV recog-nizes a diagnostic category called schizoaffective disorder(see the table for criteria for schizoaffective disorder). Thisdiagnosis is conceptually something of a hybrid in that it isused to describe people who have features of schizophreniaand severe mood disorder. In other words, the person haspsychotic symptoms that meet criteria for schizophreniabut also has marked changes in mood for a substantialamount of time. Because mood disorders can be unipolaror bipolar in type, there also are two subtypes of schizo-affective disorder (bipolar and unipolar subtype).
It is still not entirely clear whether schizo affective dis-order is best regarded as a variant of schizophrenia or as aform of mood disorder. Reflecting this controversy,DSM -IV-TR lists schizoaffective disorder in the same sec-tion of the manual as schizophrenia but does not classify itas a formal subtype of schizophrenia. Instead, it is treatedas a separate disorder. In general, the prognosis for thesepatients is somewhere between that of patients withschizophrenia and that of patients with mood disorders(Walker et aI., 2004). Research suggests that the long-term(lO-year) outcome is much better for patients withschizoaffective disorder than it is for patients with schizo-phrenia (Harrow et aI., 2000).
SCHIZOPHRENIFORM DISORDER Schizophreniformdisorder is a category reserved for schizophrenia-like psy-choses that last at least a month but do not last for 6months and so do not warrant a diagnosis of schizophre-nia (see the table for criteria for schizophreniform disor-der). It may include any of the symptoms described in thepreceding sections but is probably most often seen in anundifferentiated form. Brief psychotic states of this sortmayor may not be related to subsequent psychiatric disor-der (Strakowski, 1994). At present, however, all recent-onset cases of true schizophrenia presumably must firstreceive a diagnosis of schizophreniform disorder. Becauseof the possibility of an early and lasting remission in a firstepisode of schizophrenic breakdown, the prognosis forschizophreniform disorder (where it is a manifestation ofrecent-onset schizophrenic symptoms) is better than thatfor established forms of schizophrenia.
DELUSIONAL DISORDER Patients with delusional dis-order, like many people with schizophrenia, give voice to,and sometimes take actions on the basis of, beliefs that areconsidered completely false and absurd by those aroundthem. Unlike individuals with schizophrenia, however,people given the diagnosis of delusional disorder may oth-erwise behave quite normally. Their behavior does notshow the gross disorganization and performance deficien-
I
DSM-IV-TR .. I'
~ An illness during which, at some time, there is either aMajor Depressive Episode, a Manic Episode, or a MixedEpisode that co-occurs with symptoms of Schizophrenia(delusions, hallucinations, disorganized speech,disorganized behavior, or negative symptoms).
~ During the illness, there must be a period of at least 2
weeks where delusions and hallucinations have beenpresent without mood symptoms.
~ The mood symptoms are present for a substantialproportion of the total illness time.
I
DSM-IV-TR
~ Symptoms of schizophrenia.
~ An episode of the disorder (including the prodromal,active, and residual phases) that lasts at least 1month butless than 6 months.
, I
DSM~IV-TRI
~ Nonbizarre delusions (i.e., involving situations that couldoccur in real life such as being followed or beingpoisoned) that last for at least 1month.
~ No evidence of full-blown schizophrenia.
~ Apart from the delusion, the person's functioning is notmarkedly impaired; neither is behavior obviously odd orbizarre.
cies characteristic of schizophrenia, and general behavioraldeterioration is rarely observed in this disorder, even whenit proves chronic (see the table for criteria for delusionaldisorder). One interesting subtype of delusional disorderis erotomania. Here, the theme of the delusion involvesgreat love for a person, usually of higher status. One studysuggests that a significant proportion of women who stalkare diagnosed with erotomania (Purcell et aI, 2001).

BRIEF PSYCHOTIC DISORDER Brief psychotic disor-der is exactly what its name suggests. It involves the sud-den onset of psychotic symptoms or grossly disorganizedor catatonic behavior. Even though there is often greatemotional turmoil, the episode is usually quite brief, oftenlasting only a matter of days (too short to warrant a diag-nosis of schizophreniform disorder). After this, the per-son returns to his or her former level of functioning andmay never have another episode again (see the table forcriteria for brief psychotic disorder). Cases of brief psy-chotic disorder are infrequently seen in clinical settings,perhaps because they remit so quickly. Brief psychoticdisorder is often triggered by stress, as illustrated in thefollowing case.
Four Days of Symptoms andRapid Recovery
A32-year-old lawyer, who has successfully practiced lawfor 6 years, who is married with two young sons and manyclose friends, and who is a popular Cub Scout leader,returns home from work to find his wife in bed with hisbest friend. Initially, he expresses much depression andanger, but within 2 days begins to speak of fusing withGod, of dispensing peace on Earth, and of needing tofight the "giant conspiracy." He hears voices calling hisname and saying, "Love, love, love." His affect becomesflat and he speaks slowly and distinctly. His sleep is notdisturbed. He is admitted to a hospital, where he istreated with medication. Within 4 days he begins maritaltherapy with his wife. He improves rapidly. He returns towork within 5 days of the onset of his initial symptoms.(Adapted from Janowsky et al., 1987, p. 1.)
DSM-IV-TR I
• Presence of one or more of the following: delusions,hallucinations, disorganized speech or grosslydisorganized or catatonic behavior.
• The episode lasts for at least 1day but less than1 month, with an eventual full return to normalfunctioning.
• A diagnosis of Mood Disorder with Psychotic Features;Schizoaffective Disorder or Schizophrenia is ruled out.
SHARED PSYCHOTIC DISORDER Finally, many peopleknow shared psychotic disorder by its French name,folie it deux. As the name suggests, it is a delusion thatdevelops in someone who has a very close relationshipwith another person who is delusional (see the table forcriteria for shared psychotic disorder). Over time, this sec-ond individual comes to believe in the delusions of theother person. In some cases, the contagion of thought mayspread even further and whole families may adopt thesame delusional beliefs.
IDSM-IV-TR
I
• A delusion develops in the context of a close relationshipwith another person who already has an establisheddelusion.
• The delusion is similar in content to that of the personwho already has the established delusion.
• Other Psychotic Disorders are ruled out.
r---=="'-------==~,In ReVIew• What are the five major subtypes of
schizophrenia recognized by the DSM?• What are the major differences between
schizophrenia and (a) schizoaffectivedisorder and (b) schizophreniform disorder?
WHAT CAUSESSCHIZOPHRENIA? _
Despite an enormous research effort going back manyyears and continuing to the present day, this question stilldefies a simple answer. In the sections that follow, we dis-cuss what is currently known about the etiology of schiz-ophrenia. In all probability, however, no one factor canfully explain why schizophrenia develops. The olddichotomy of nature versus nurture is as misleading as itis simplistic. Psychiatric disorders are not the result of asingle genetic switch being flipped. Rather, a complexinterplay between genetic and environmental factors isusually responsible.

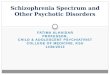
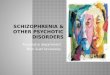
Genetic AspectsIt has long been known that disorders of the schizophrenictype are "familial" and tend to "run in families." The evi-dence for higher-than-expected rates of schizophreniaamong biological relatives of "index" cases (that is, thediagnosed group of people who provide the starting pointfor inquiry, also called "probands") is overwhelming.Figure 14.2 shows the percentage of the risk of developingschizophrenia given a specific genetic relationship withsomeone who has the disorder. As you can see, there is astrong association between the closeness of the blood rela-tionship (i.e., level of gene sharing or consanguinity) andthe risk for developing the disorder. For example, theprevalence of schizophrenia in the first-degree relatives(parents, siblings, and offspring) of a proband with schizo-phrenia is about 10 percent. For second-degree relativeswho share only 25 percent of their genes with the proband(e.g., half-siblings, aunts, uncles, nieces, nephews, andgrandchildren), the lifetime prevalence of schizophrenia iscloser to 3 percent.
Of course, that something runs in families does notautomatically implicate genetic factors. The terms familialand genetic are not synonymous, and a disorder can run ina family for nongenetic reasons (if I am obese and my dogis also obese, the reasons for this are clearly not genetic!).
General population
First cousins ].!!! Uncles/ AuntscCIl•....cc..
Nephews/Nieces0N:cuIII Grandchildren..c-.~c Half siblings0l!!CIlc..
Parents0-c..:c
SiblingsIIIc0'';::"' ChildrenQ)
a:::
Fraternal twins
Identical twins
As we have repeatedly emphasized, the interpretation offamilial concordance patterns is never completely straight-forward, in part because of the strong relationship betweenthe sharing of genes and the sharing of the environmentsin which those genes express themselves. Although they areindispensable in providing a starting point for researchers,family studies cannot, by themselves, tell us why a disorderruns in families. To disentangle the contributions of genesand environment, we need twin and adoption studies.
TWIN STUDIES We discussed twin studies in general inChapter 3 and more specifically in relation to anxiety andmood disorders in Chapters 6 and 7. As with the mood dis-orders, schizophrenia concordance rates for identical twinsare routinely, and over very many studies, found to be sig-nificantly higher than those for fraternal twins or ordinarysiblings. The most famous case of concordance for schizo-phrenia is the Genain quadruplets, summarized in TheWorld Around Us 14.1 on page 502.
Although being a twin does not increase one's risk fordeveloping schizophrenia (the incidence of schizophreniaamong twins is no greater than that for the general popu-lation), study after study has shown a higher concordancefor schizophrenia among identical, or monozygotic (MZ),twins over people related in any other way, including fra-ternal, or dizygotic (DZ), twins.
Genes shared
o 12.5% 3rd-degree relatives
25% 2nd-degree relatives
o 50% 1st-degree relatives
0100%
Lifetime age-adjusted, averagedrisks for the development ofschizophrenia-related psychoses inclasses of relatives differing in theirdegree of genetic relatedness.Source: Compiled from family and twinstudies in European populationsbetween 1920 and 1987. FromSchizophrenia Genesis:The Origins ofMadness (p. 96), by I. I. Gottesman.Copyright © 1991 by Irving I. Gottes-man. Used with permission ofWH. Free-man and Company/Worth Publishers.
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
Risk of developing schizophrenia

14.1
The Genain quadruplets were born sometimein the early 1930s. They immediately becamefamous in their hometown because they wererare MZ quadruplets. What makes the Genainsespecially interesting, however, is that each of
these genetically identical girls was to develop schizophre-nia, an outcome that would be expected to occur by chanceonly once in approximately 1.5 billion births.
The quadruplets were hospitalized at the NationalInstitute of Mental Health in the mid-1950S and becamea focus of intensive study. David Rosenthal, the leadresearcher, selected the pseudonym surname Genain forthe girls. The word was derived from the Greek for "dread-ful gene." Rosenthal also selected first names for the girlsin order of their birth, using the initials of the institution,NIMH. Accordingly, the women are known to us as Nora(the firstborn), Iris, Myra, and Hester. They are all concor-dant for schizophrenia. However, they are discordant withregard to the severity of their illnesses.
The most severely ill Genain is Hester, who was bornlast and had the lowest birth weight. Hester was alwaysthe slowest to develop, and she was removed from schoolafter eleventh grade. She has never held a job outside thehome and has suffered from chronic and unremittingsevere symptoms since age 18. Neurocognitive testing atNIMH revealed that, along with Nora, Hester showed agreat deal of evidence of brain disturbance.
Nora, the firstborn, was always considered by thefamily to be the best of the four girls. She had the highestIQ and was the first to get a job. Nonetheless, after she washospitalized at the age of 22 with hallucinations, delu-sions, and withdrawal, she had a long history of hospital-izations and was never able to live independently or hold ajob for an extended period of time.
In contrast, Myra, who was born third, though she hadsome problems in her twenties (when she was questionablydiagnosed as having schizophrenia), does not appear tohave experienced delusions and paranoia until her mid-for-ties. The only one of the Genains to marry and have chil-dren, she has a clinical picture that suggests schizoaffectivedisorder (a blend of psychotic symptoms and mood symp-toms). Although she was not psychiatrically well by anymeans, she was able to go off medications. She eventuallywent into remission and was diagnosed as having residualschizophrenia.
Finally, there is Iris. Like Nora, Iris had her first psychi-atric hospitalization at age 22. She spent 12 years in a statehospital and suffered from hallucinations, delusions, andmotor abnormalities. Although neurocognitive testing didnot reveal any obvious brain disturbance, it is clear thatshe has suffered from a severe form of schizophrenia.
Why do these identical quadruplets not have identi-cal illnesses? We simply do not know. Did Nora and Hes-ter, being born first and last, experience more traumaticbirth complications? Did Iris do less well than might havebeen expected from her neurocognitive test resultsbecause her parents insisted on treating the quads asthough they were two sets of twins-a superior and tal-ented set consisting of Nora and Myra, and an inferior,problematic set consisting of Iris and Hester? Did beingpaired with Hester somehow compromise Iris's develop-ment? Did Myra do so well (relatively) because she wasthe most favored and because she did not sustain anybrain damage?
Why did the quadruplets develop schizophrenia atall? In all probability, there was a family history of the dis-order. Mr. Genain's mother (the girls' grandmother) had anervous breakdown in her teens and appears to have had

some symptoms of paranoid schizophrenia. It is also clearthat the family environment was far from healthy and mayhave provided the stress that acted on the quadruplets'genetic predispositions to induce full-blown illness. Mr.Genain was very disturbed. He spent most of his timedrinking and expressing his various fears and obsessionsto his family. Prominent among these were fears thatbreak-ins would occur at the home unless he patrolledthe premises constantly with a loaded gun, and, espe-cially as the girls developed into adolescence, that theywould get into sexual trouble or be raped unless hewatched over them with total dedication. He imposedextreme restrictions and surveillance on the girls until thetime of their breakdowns. He was himself sexuallypromiscuous and was reported to have sexually molestedat least two of his daughters. Mrs. Genain, although sheapparently managed to see sexuality and sexual threats
in the most innocuous circumstances, seems to haveignored the real sexual exploitation occurring in thehome. In short, nothing about the family environment canbe considered to have been normal.
It is a tribute to the scientific diligence of the NIMHstaff and to David Rosenthal, who maintained both ahuman and a scientific interest in this unfortunate family,that we know so much about them (see Rosenthal, 1963;see also Mirsky & Quinn, 1988). In the Genain quadrupletswe have four genetically identical women, all of whom haveexperienced schizophrenia in one form or another. Theirdisorders, however, have been different in severity,chronicity, and eventual outcome. Although this case high-lights the likely role of environmental factors in the puzzleof schizophrenia, just how the combination of genes andenvironment shaped the destinies of Nora, Iris, Myra, andHester remains a mystery.
65 o Identical twins
o Fraternal twins50
41
31 33 28(97/341)
2418
1410 9
Study 2 Study 3 Study 4 Study 5 Study 6 Study 7 Study 8 Overall
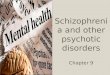
E. Fuller Torrey is a noted schizophrenia researcherwho has a sister with the disorder. He and his colleagues(1994) have published a review of the major literatureworldwide on twin studies of schizophrenia. Their find-ings are summarized in Figure 14.3. The overall pairwiseconcordance rate is 28 percent in MZ twins and 6 percentin DZ twins. This suggests that a reduction in shared genesfrom 100 percent to 50 percent reduces the risk of schizo-phrenia by nearly 80 percent. Also note that sharing 50 per-
CIl
~ 40•...cCIl
~ 30~
cent of one's genes with a co-twin with schizophrenia isassociated with a lifetime risk for schizophrenia of 6 per-cent. Although this is low in absolute terms, it is markedlyhigher than the baseline risk of 1 percent found in the gen-eral population.
If schizophrenia were exclusively a genetic disorder,the concordance rate for identical twins would, of course,be 100 percent. Although MZ concordance rates vary fromone twin study to another, and some researchers report
Pairwise twin concordance rates for schizophrenia found in eight methodologically adequate studies.
Source: From Schizophrenia and Manic Depressive Disorder by E. Fuller Torrey, Ann Bowler, Edward Taylor, and frving f. Gottesman. Copyright © 1994 byBasic Books. Reprinted by permission of Basic Books, a member of Perseus Books, L. L. C.

age-correctedincidence rate
Incidence is the number ot newcases that develop. An age-corrected incidence rate takes intoaccount predicted breakdowns torsubjects who are not yet beyondthe age ot risk tor succumbing tothe disorder.
MZ twin #1Well
higher rates than Torrey's 28 percent, they are never evenclose to 100 percent. Two conclusions can therefore bedrawn: First, genes undoubtedly play a role in causingschizophrenia. Second, genes themselves are not the wholestory. Twin studies provide some of the most solid evi-dence that the environment plays an important role in thedevelopment of schizophrenia. But why one MZ twinshould develop schizophrenia when his or her co-twindoes not remains a mystery.
A great deal of research attention is now beingdirected at studying people with a known genetic liabilityfor schizophrenia. The most important subjects to studyin this regard are MZ twins who are discordant forschizophrenia. This investigative strategy was pioneeredby Fischer (1971, 1973) in an ingenious study. Fischerreasoned that genetic influences, if pre-sent, would be just as likely to show upin the offspring of the well (nonschizo-phrenic) twins of discordant pairs (seeFigure 14.4) as they would be to showup in the offspring of the ill twins withschizophrenia (because they share alltheir genes in common). And, in asearch of official records in Denmark,Fischer found exactly that. Subsequentto this, in a follow-up of Fischer's sub-jects, Gottesman and Bertelson (1989)reported an age-corrected schizophre-nia incidence rate of 17.4 percent forthe offspring of the nonschizophrenic(i.e., well) MZ twins. This rate, whichfar exceeds normal expectancy, was not significantly dif-ferent from that for offspring of the schizophrenic mem-
MZ twin #2Schizophrenia
Because MZ twins have identicalgenes, the children ot even the welltwin have an elevated risk otschizophrenia, even it their parentdid not actually sutter trom thedisorder.
bers of discordant pairs, or from that for offspring of DZtwins with schizophrenia. Assuming that exposure to anaunt or uncle with schizophrenia (i.e, the "ill twin")would have, at most, limited etiologic significance, theseresults lend impressive support to the genetic hypothesis.They also, as the authors note, indicate that a predisposi-tion to schizophrenia may remain "unexpressed" (as inthe nonschizophrenic twins of discordant pairs) unless"released" by unknown environmental factors.
ADOPTION STUDIES One major assumption that twinstudies make is that any differences found between MZand DZ twins are attributable to genes. At the heart ofthis assumption is the idea that the environments of MZtwins are no more similar than the environments of
DZ twins. But it is very reasonable toexpect that, because they are identical,the environments of MZ twins willactually be more similar than the envi-ronments of DZ twins. To the extentthat this is true, twin studies will over-estimate the importance of genetic fac-tors (because some similarities betweenMZ twins that occur for nongeneticreasons will be attributed to geneticfactors). In some cases, of course,MZ twins go to a great deal of effort totry to be different from one another.The bottom line, however, is that theassumption that MZ and DZ twinshave equally similar environments can
create some problems when we try to interpret the find-ings of twin studies.

Several studies have attempted to overcome the short-comings of the twin method in achieving a true separationof hereditary from environmental influences by usingwhat is called the "adoption strategy." Here concordancerates for schizophrenia are compared for the biological andthe adoptive relatives of persons who have been adoptedout of their biological families at an early age (preferablyat birth) and have subsequently developed schizophrenia.If concordance is greater among the patients' biologicalthan adoptive relatives, a hereditary influence is stronglysuggested; the reverse pattern would argue for environ-mental causation.
The first study of this kind was conducted by Hestonin 1966. Heston followed up 47 children who had beenborn to mothers who were in a state mental hospital suf-fering from schizophrenia. The children had been placedwith relatives or into foster homes within 72 hours of theirbirth. In his follow-up study, Heston found that 16.6 per-cent of these children were later diagnosed with schizo-phrenia. In contrast, none of the 50 control children(selected from among residents of the same foster homeswhose biological mothers did not have schizophrenia)developed schizophrenia. In addition to the greater proba-bility of being diagnosed with schizophrenia, the offspringwhose mothers had schizophrenia were also more likely tobe diagnosed as mentally retarded, neurotic, and psycho-pathic (that is, antisocial). They also had been involvedmore frequently in criminal activities and had spent moretime in penal institutions (Heston, 1966). These findingsare often taken to suggest that any genetic liability con-veyed by the mothers is not specific to schizophrenia butalso includes a liability for other forms of psychopathol-ogy, but we must be careful about drawing such a conclu-sion. Heston's study provided no information aboutpsychopathology in the fathers of the children. We there-fore cannot know to what extent some of the problems thatthe children had were due to genetic liability conveyed bytheir fathers.
Heston's study began by identifying mothers withschizophrenia and then tracing what had happened totheir adopted-away offspring. An alternative approachinvolves locating adult patients with schizophrenia whowere adopted early in life and then looking at rates ofschizophrenia in their biological and adoptive relatives. Alarge-scale and multifaceted adoption study of this typewas undertaken in Denmark with Danish and Americaninvestigators working in collaboration (Kendler & Gruen-berg, 1984; Kendler et aI., 1994; Kety, 1987; Kety et aI.,1968, 1978, 1994; Rosenthal et aI., 1968; Wender et aI.,1974). As would be expected on the basis of a geneticmodel, the data showed a preponderance of schizophreniaand "schizophrenia-spectrum" problems (e.g., schizotypaland paranoid personality disorder) in the biological rela-tives of adoptees with schizophrenia. More specifically,13.3 percent of the 105 biological relatives had schizophre-nia or schizophrenia-spectrum disorders themselves. In
contrast, only 1.3 percent of the 224 adoptive parentsshowed such problems.
THE QUALITY OF THE ADOPTIVE FAMILY The Danishadoption studies did not include independent assessmentsof the child-rearing adequacy of the adoptive families intowhich the index children (those who developed schizo-phrenia) and the control children (those who did not) hadbeen placed. It remained for Tienari and his colleagues(Tienari et aI., 1987,2000,2004) to add this feature to theirresearch design. The Finnish Adoptive Family Study ofSchizophrenia, as it is known, has followed up theadopted-away children of all women in Finland who werehospitalized for schizophrenia between 1960 and 1979. Asthey grew to adulthood, the functioning of these indexchildren was compared with the functioning of a controlsample of adoptees whose biological mothers were psychi-atrically healthy. Over the course of a 21-year follow-up,the index adoptees developed more schizophrenia andschizophrenia-related disorders than did the controls(Tienari et aI., 2000; 2003). What sets this study apart,however, is what it tells us about the interaction betweengenes and environment.
One measure of the family environment that theresearchers looked at was communication deviance(Wahlberg et aI., 1997). Communication deviance is a mea-sure of how understandable and "easy to follow" the speechof a family member is. Vague, confusing, and unclear com-munication reflects high communication deviance. WhatWahlberg and colleagues found was that it was the combi-nation of genetic risk and high communication deviance inthe adopted families that was problematic. Children whowere at genetic risk and who lived in families where therewas high communication deviance showed high levels ofthought disorder at the time of the follow-up. In contrast,the control adoptees who had no genetic risk for schizo-phrenia showed no thought disorder, regardless of whetherthey were raised in a high- or a low-communication-deviance family. Perhaps what was most remarkable,though, was the outcome for the high-risk children whowere raised by adopted families low in communicationdeviance. These children were healthier at follow-up thanany of the other three groups! In other words, if they areraised in a benign environment, even children who are atgenetic risk for schizophrenia appear to do very well.
Tienari and his colleague have recently provided fur-ther evidence of a gene-environment interaction in schizo-phrenia (Tienari et aI., 2004). Using interviews, theresearchers first looked at the quality of the family envi-ronment in which the adopted children were raised. Theythen looked at what happened to the children who wereraised in healthy versus dysfunctional families. The degreeof adversity in the family environment predicted laterproblems in the adopted children. However, only thosechildren who were raised in dysfunctional families and hadhigh genetic risk for schizophrenia went on to develop

Child with geneticrisk of schizophrenia
Child with geneticrisk of schizophrenia
High risk ofdeveloping schizophrenia
Low risk ofdeveloping schizophrenia
Children at genetic risk for schizophrenia are more likely to develop the disorder if they are raised in dysfunctional family environments.Children who do not have a genetic risk have a low risk of developing schizophrenia, even if their family environment is not healthy.
schizophrenia-related disorders themselves. Children athigh genetic risk who were raised in healthy family envi-ronments did not develop problems any more frequentlythan children at low genetic risk (see Figure 14.5).
These findings are important because they suggestthat our genetic makeup may control how sensitive we areto certain aspects of our environments. If we have nogenetic risk, certain kinds of environmental influencesmay not affect us very much. But if we have high geneticrisk, we may be much more vulnerable to certain types of
environmental "risks" such as high communicationdeviance or adverse family environments. Findings such asthese also raise the exciting possibility that certain kinds ofenvironments may protect people with a genetic suscepti-bility to schizophrenia from ever developing the illness.
In summary, these findings indicate a strong interac-tion between genetic vulnerability and an unfavorablefamily environment in the causal pathway leading toschizophrenia. Of course, it could be argued that the chil-dren who went on to develop problems caused the dis-

organization of their adoptive families. However, there islittle support for this alternative interpretation (see Tienariet aI., 2004; WaWberg et aI., 1997). Some independent workreported by Kinney and colleagues (1997) also fails toshow diminished mental health in adoptive parents raisingchildren who later developed schizophrenia. Everythingconsidered, the Finnish Adoptive Family Study has pro-vided strong confirmation of the diathesis-stress model asit applies to the origins of schizophrenia.
MOLECULAR GENETICS Family, twin, and adoptionstudies have been immensely valuable in the study ofschizophrenia. Family studies tell us that schizophreniaruns in families, and twin and adoption studies help usexplore the relative contributions of genes and environ-ment. These approaches also tell us about the genetic het-erogeneity of schizophrenia. For example, in addition tohigher rates of schizophrenia, higher rates of schizotypalpersonality disorder are also found in the relatives ofpatients with schizophrenia (Kendler et aI., 1993). Thissupports the idea of the schizophrenia spectrum and sug-gests that a genetic liability to schizophrenia can some-times manifest itself in a form of pathology that is"schizophrenia-like" but not exactly schizophrenia itself(see Fowles, 2003, for more discussion).
Traditional genetic approaches have indeed taken us along way. But a paradigm shift is now taking place.Genetic researchers are moving away from family, twin,and adoption studies toward studies of molecular genet-ics. Although a detailed discussion of such approaches istechnical and beyond the scope of this textbook, effortsare now under way to answer two key questions: "What isthe mode of genetic transmission?" and "Where are thegenes located?" Using a complex mathematical modelingtechnique called "segregation analysis," researchers aretrying to determine whether there is a single major geneticlocus for schizophrenia. Progress in this area has beenfrustratingly slow, not least because schizophrenia appearsto be very complex genetically and because researchers arestill not sure exactly what phenotype they should be look-ing for (remember the idea of "the schizophrenias"?).Because segregation analysis requires that we know who is"affected" and who is not, this is clearly a big problem.
It is extremely unlikely that schizophrenia will, likeHuntington's disease (see Chapter 15), be explained by onemutated gene on one specific chromosome. Rather, schizo-phrenia probably involves several, or perhaps many, genesworking together to confer susceptibility to the illness(Faraone et aI., 1999; Gottesman, 1991). The individual's"dose" of schizophrenia genes may explain why one persondevelops schizophrenia and another develops a mildervariant within the schizophrenia spectrum such as schizo-typal personality disorder.
Currently, researchers are paying a lot of attention tospecific regions on chromosomes 22, 6, 8, and 1, amongothers (Brzustowicz et aI., 2000; Harrison & Owen, 2003;
Kendler, 1999a; Plomin & McGuffin, 2003). They are alsousing known DNA markers to try to learn where aberrantgenes might lie. As Faraone and colleagues (1999) aptlystate, DNA markers are the "milemarkers" on our chromo-somal highways. Molecular geneticists capitalize on thefact that we know the location of a few important genesthat are associated with observable traits (such as genes forcolor blindness, for blood group, and for the human leuko-cyte antigen). Because genes that are close together on thesame chromosome tend to stay together when geneticinformation is shuffled (as happens during reproduction),researchers can see whether a disorder like schizophreniatends to co-occur with any known DNA marker traits. Thisis the rationale behind linkage analysis. Linkage analysishas been very successful in helping locate the genes asso-ciated with diseases that have well-defined models ofinheritance. In schizophrenia research up to now, however,failures to replicate this success have been more the rulethan the exception.
Now the focus is on looking more closely forcandidate genes (Berry et aI., 2003; Harrison & Owen,2003). These genes are known to be involved in some ofthe processes that are thought to be aberrant in schizo-phrenia (e.g., genes implicated in dopamine metabolism).Although there are no definitive findings as yet, thisapproach holds a lot of potential.
Prenatal ExposuresGenes are clearly involved in the development of schizo-phrenia, but we also know that they are not the wholestory. In recent years, researchers have begun to exploreother factors that might either cause the disorder or triggerit in a genetically vulnerable person. These factors includeprenatal viral infection, rhesus incompatibility, earlynutritional deficiency, and perinatal birth complications.
The idea that schizophrenia might result from somekind of virus is not new. Kraepelin (1919) suggested that"infections in the years of development might have acausal significance" for schizophrenia. We also know thatin the Northern Hemisphere, more people with schizo-phrenia are born between January and March than wouldbe expected by chance (Waddington et aI., 1999). Couldsome seasonal factor, such as a virus, be implicated in caus-ing schizophrenia?
In 1957 there was a major epidemic of influenza inFinland. Studying the residents of Helsinki, Mednick andcolleagues found elevated rates of schizophrenia in chil-dren born to mothers who had been in their secondtrimester of pregnancy at the time of the influenza epi-demic (1988). The link between maternal influenza andsubsequent schizophrenia in the grown offspring has nowbeen well replicated using influenza epidemic informationfrom other countries (see Wright et al., 1999). Risk ofschizophrenia seems to be greatest when the mother getsthe flu in the fourth to seventh month of gestation.

Although the size of the effect is small and influenza clearlydoes not account for very many cases of schizophrenia, thefact that this association exists is very provocative. Howcan maternal influenza set the stage for schizophrenia inthe child two or three decades later? One possibility is thatthe mother's antibodies to the virus cross the placenta andsomehow disrupt the neurodevelopment of the fetus(Waddington et aI., 1999).
The idea that the mother's immune system mightsomehow damage the developing brain of the fetus is notas far-fetched as it might sound. Rhesus (Rh) incompati-bility occurs when an Rh-negative mother carries an Rh-positive fetus (Rhesus-positive or -negative is a way oftyping a person's blood). Incompatibility between themother and the fetus is a major cause of hemolytic (blood)disease in newborns. Interestingly, Rh incompatibility alsoseems to be associated with increased risk for schizophre-nia. Hollister, Laing, and Mednick (1996) have shown thatthe rate of schizophrenia is about 2.1 percent in males whoare Rh-incompatible with their mothers. For males whohave no such incompatibility with their mothers, the rateof schizophrenia is 0.8 percent-very close to the expectedbase rate found in the general population. Hollister isanother example of a schizophrenia researcher who has afamily member with the disorder, in this case a sister whowas Rh-incompatible with her mother.
How might Rh incompatibility increase the risk forschizophrenia? One possibility is that the mechanismmight involve oxygen deprivation, or hypoxia. This sugges-tion is supported by studies that have linked the risk forschizophrenia to birth complications. Research tells us thatpatients with schizophrenia are much more likely to havebeen born following a pregnancy or delivery that was com-plicated in some way (Cannon et aI., 2002). Although thetype of obstetric complication varies, many delivery prob-lems (for example, breech delivery, prolonged labor, or theumbilical cord around the baby's neck) affect the oxygensupply of the newborn. Although we still have a lot tolearn, the research again points toward damage to the fetalbrain at a critical time of development.
The last piece of evidence that supports the idea thatschizophrenia might be caused or triggered by environ-mental events that interfere with normal brain develop-ment comes from a tragedy that occurred in theNetherlands toward the end of World War II. In October1944, a Nazi blockade resulted in a severe famine thataffected people living in Amsterdam and other cities in thewest of the country. The Dutch Hunger Winter (as it wasknown) continued until the Netherlands was liberated inMay 1945. The population was severely malnourished dur-ing this time, and many died of starvation. Not surpris-ingly, fertility levels fell and the birthrate droppedprecipitously. However, some children were born duringthis time. It now appears that those who were conceived atthe height of the famine had a twofold increase in their
risk of later developing schizophrenia (Susser et aI., 1996).Early prenatal nutritional deficiency app~ars to have beenthe cause. Whether the problem was general malnutritionor the lack of a specific nutrient such as folate is not clear.But again, something seems to have compromised thedevelopment of the fetus during a critical stage.
Genes and Environment inSchizophrenia: A SynthesisWithout question, schizophrenia has a strong genetic com-ponent. But it is a genetically influenced, not a geneticallydetermined, disorder (Gottesman, 2001). Schizophrenia isalmost certainly polygenic and involves more than one ortwo genes. Current expert thinking emphasizes the notionof a multiplicity of genes that must somehow operate inconcert (Gottesman, 1991; Kendler & Diehl, 1993; Moldin& Gottesman, 1997). Moreover, in the case of a person whodevelops schizophrenia, the predisposing genetic factorsmust have combined in additive and interactive ways withenvironmental factors, some known and some stillunknown, that operate prenatally, perina tally, and alsopostnatally (see Gottesman, 2001).
It is also possible that the focus on MZ concordancerates has caused us to overestimate the heritability of schiz-ophrenia. This is because some MZ and all DZ twins donot have equally similar prenatal environments. Aroundtwo-thirds of MZ embryos are monochorionic, whichmeans that they share a placenta and their blood supply.The remaining MZ twins and all DZ twins are dichorionic;they have separate placentas and separate fetal circulations.This is shown in Figure 14.6. The higher concordance ratefor schizophrenia in MZ than in DZ twins might thereforebe a consequence, at least in part, of the greater potentialfor monochorionic MZ twins to share infections. Davis,Phelps, and Bracha (1995) have found that MZ twins whoare monochorionic are much more likely to be concordantfor schizophrenia (around 60 percent concordance) thanMZ twins who are dichorionic (around 11 percent concor-dance). The concordance figure for dichorionic MZ twinsis very similar to that generally reported for DZ twins.Monochorionic twins may therefore have inflated concor-dance rates in schizophrenia and may have caused us tooverattribute to genetics what might more accurately beattributed to environmental influences.
Finally, we need to keep in mind that genes get "turnedon" and "turned off" in response to environmentalchanges. Perhaps some environmental "hits" turn on thegenes for schizophrenia. Perhaps some environments cankeep the genes for schizophrenia from ever being turnedon at all. And perhaps being at genetic risk makes peoplemore susceptible to environmental insults. In a study look-ing at the consequences of birth complications, Cannonand colleagues (1993) found that only the people who hada parent with schizophrenia and who had birth complica-

tions were the ones who later had brain abnormalities inadulthood such as enlarged ventricles (fluid-filled spacesin the brain). Moreover, for people who had two parentswith schizophrenia, the problems were even worse. In con-trast, people with no family history of schizophrenia didnot show enlarged ventricles, regardless of whether theyexperienced delivery complications when they were born.The message seems to be clear: A genetic liability to schizo-phrenia may predispose an individual to suffer more dam-age from environmental insults than would be the case inthe absence of the genetic predisposition.
A Neurodevelopmental PerspectiveEarlier in this chapter you learned that schizophrenia typi-cally strikes people in late adolescence or early adulthood.Yet in the sections above, we saw that some of the factorsthought to cause schizophrenia occur very early in life-insome cases before birth. How can this be? A majority ofresearchers now accept that schizophrenia is a neurodevel-opmental disorder. The idea here is that vulnerability toschizophrenia stems from a brain lesion that occurs veryearly in development, perhaps even before birth. Thislesion then lies dormant until normal maturation of thebrain shows up the problems that result from the lesion.This may not occur until the brain is fully mature, typicallylate in the second decade of life (Conklin & Iacono, 2002;Weinberger, 1987).
What goes wrong? We cannot yet be certain. Braindevelopment is a complex process that involves a pro-grammed, orderly, and progressive sequence of events(Nowakowski, 1999). One possibility, however, is that thereis a disruption in cell migration, with some cells failing toreach their target destinations. If this were to happen, the"internal connectivity" of the brain could be greatlyaffected. Neuronal migration is known to occur during thesecond trimester-exactly the period in development dur-ing which the consequences of maternal influenza seem tobe most devastating.
Chorionic Arrangements inTwins(A) Dichorionic twins, who can beeither dizygotic or monozygotic,have separate placentas andseparate fetal circulation.(B) Monochorionic twins, who arealways monozygotic, have a singleplacenta and shared circulation.Source: Davis, Phelps, and Bracha (1995).
DEVELOPMENTAL PRECURSORS OF SCHIZOPHRENIAIf the seeds of schizophrenia are sown very early in life, canwe see early indications of vulnerability to the disorderbefore the illness itself strikes?
An ingenious series of studies reported by ElaineWalker and her colleagues nicely illustrates the associationbetween early developmental deviation and schizophreniarisk. These investigators gathered family home moviesmade during the childhoods of 32 persons who eventuallydeveloped schizophrenia. Trained observers made "blind"ratings (i.e., the observers were uninformed of outcomes)of certain dimensions of the emotional (Grimes & Walker,1994) and facial expressions (Walker et aI., 1993), motorskills, and neuromotor abnormalities (Walker et aI., 1994)of these children and of their healthy-outcome siblingsfrom the same movie clips. The facial and emotionalexpressions and the motor competence of the preschizo-phrenic and the healthy-outcome children were found bythe raters to differ significantly. The preschizophrenic chil-dren showed more motor abnormalities including unusualhand movements than their healthy siblings; they alsoshowed less positive facial emotion and more negativefacial emotion. In some instances these differences wereapparent by age 2. Of course, we need to keep in mind thatthese early problems do not characterize all preschizo-phrenic children. But they do tell us that subtle abnormal-ities can be found in children who are vulnerable toschizophrenia. We should also note that a major advantageof Walker's research design was that it avoided the problemof retrospective bias. Rather than asking parents or siblingswhat patients were like when they were growing up, thestudy used home movies to provide an objective behav-ioral record.
Another way to explore childhood indicators withoutthe problem of retrospective bias is to use a prospectiveresearch design. Jones et al. (1994) and Isohanni et al.(2001) studied whole cohorts of children born in particu-lar years and followed them up over time. Both groups ofresearchers found evidence of delayed speech and delayed

Ratings of clips of old home movies have revealed that childrenwho went on to develop schizophrenia showed more unusualhand movements than their healthy siblings, even when they werejust two years old.Source: E. E. Walker (1994). Developmentally moderated expressionsof the neuropathology underlying schizophrenia. Schisophrenia Bul·
letin, 20,453-480.
motor development at age 2 in children who later went onto develop schizophrenia.
Yet another approach is to follow children who areknown to be at high risk for schizophrenia by virtue oftheir having been born to a parent with the disorder. Thisstrategy, pioneered by Mednick and Schulsinger (1968),has led to several other studies of high-risk children (forreviews, see Cornblatt et al., 1992; Erlenmeyer-Kimling &Cornblatt, 1992; Garmezy, 1978a, 1978b; Neale & Olt-manns, 1980; Rieder, 1979; Watt et aI., 1984). Obviously,research of this kind is both costly and time-consuming. Italso requires a great deal of patience on the part ofresearchers, because children at risk have to be identifiedearly in their lives and then followed into adulthood.Moreover, because the majority of people with schizophre-nia do not have a parent with the disorder [in fact, 89 per-cent of patients have no first- or second-degree relativeswith schizophrenia (Gottesman, 2001)], high-risk samplesare not particularly representative. Nonetheless, they haveprovided us with some valuable information about whatpeople at risk look like prior to developing the full illness.
One of the most consistent findings from high-riskresearch is that children with a genetic risk for schizophre-nia are more deviant than control children on researchtasks that measure attention (Erlenmeyer-Kimling &Cornblatt, 1992). Adolescents at risk for schizophrenia arealso rated lower in social competence than adolescents atrisk for affective illness (Dworkin et aI., 1990, 1991, 1994).Some of the social problems that these high-risk childrenhave may result from underlying attentional problems(Cornblatt et aI., 1992). This is consistent with the follow-ing comments, which come from a patient who developedschizophrenia as a child:
It has always been hard for me to have friends. 1wantfrIends, but 1don1t know how to make them. I alwaysthink people are serious when they are just jokingaround, but I don't figure that out until a lot later. I justdon't know how to adapt. ... After I got back from [myfirst hospitalization], I really couldn't get along withanyone. That was when kids first began calling me"retard." I am not a retard, but I get confused and I can'tfigure out what is going on. (Anonymous, 1994, p. 587)
Echoing the findings from Walker's home movie studyis evidence that early motor abnormalities might be anespecially strong predictor of later schizophrenia. Usingdata from the New York High-Risk Study, Erlenmeyer-Kimling and colleagues (1998) reported that, of an initialgroup of 51 high-risk children, 10 developed schizophre-nia or schizophrenia-like psychosis as adults. Of these, 80percent showed unusual motor behavior when they werebetween 7 and 12 years of age. Although we might havesuspected that the schizophrenia would first begin to showitself via hallucinations or delusions, it may be that the firstsigns of the illness can instead be found in the way thatchildren move.
The original high-risk studies have given us manyinsights into the problems that characterize people at riskfor schizophrenia. But researchers are now changing theirstrategies. A new generation of high -risk studies is focusingon the young unaffected siblings of patients with schizo-phrenia, rather than following children who have a parentwith the disorder (Cornblatt et aI., 1998). Other researchgroups are studying currently well young people who are atexceptionally high risk because they have two close relativeswith the disorder (Miller et aI., 2002). Time will tell justhow informative these research designs will prove to be.
Finally, it is important to remember that studyingpeople with a family history of schizophrenia is not theonly way to study people at risk for schizophrenia. Analternative approach is to study endophenotypes (e.g.,Miller, 1995). These are discrete, measurable traits that arethought to be linked to specific genes that might be impor-tant in schizophrenia. Accordingly, researchers are inter-ested in people who score high on certain tests or measuresthat are thought to reflect a predisposition to schizophre-nia. One example is subjects who score high on a self-report measure of schizotypic traits involving perceptualaberrations and magical ideation (the Per-Mag Scale; seeChapman, Chapman, & Miller, 1982; Chapman et aI.,1994). An example of perceptual aberration is responding"True" to the statement "Sometimes people whom I knowwell begin to look like strangers." An example of magicalideation is endorsing the item "Things seem to be in differ-ent places when I get home, even though no one has beenthere" (see Green, 1997). Other endophenotypic riskmarkers for schizophrenia include abnormal performanceon measures of cognitive functioning such as tests ofworking memory (see Barch, 2005).

Biological AspectsResearch on the structural properties of the brain in livingsubjects was largely unproductive until the development ofmodern computer-dependent technologies such as com-puterized axial tomography (CAT), positron emissiontomography (PET), and magnetic resonance imaging(MRI). The use of these techniques in the study of thebrains of people with schizophrenia has accelerated inrecent years, with important results.
BRAIN VOLUME One of the most well-replicated find-ings concerns the brain ventricles, fluid-filled spaces thatlie deep within the brain. A large number of studies haveshown that, compared with controls, patients with schizo-phrenia have enlarged brain ventricles, with males possiblybeing more affected than females (see Lawrie & Abukmeil,1998). Figure 14.7 illustrates enlarged ventricles in identi-cal twins, one of whom suffers from schizophrenia. How-ever, we must also point out that enlarged brain ventriclesare apparent only in a significant minority of patients.Enlarged brain ventricles also are not specific to schizo-phrenia and can be seen in patients with Alzheimer's dis-ease, in those with Huntington's disease, and in chronicalcoholics.
Enlarged brain ventricles are important because theyare an indicator of a deficit in the amount of brain tissue.The brain normally occupies fully the rigid enclosure ofthe skull. Enlarged ventricles therefore imply that the brainareas that border the ventricles have somehow shrunk ordecreased in volume, the ventricular space becominglarger as a result. In fact, MRI studies of patients withschizophrenia show about a 3 percent reduction in wholebrain volume relative to controls (Lawrie & Abukmeil,1998). This decrease in brain volume seems to be presentvery early in the illness. Even patients with a recent onset ofschizophrenia have lower overall brain volumes than con-trols (Fannon et aI., 2000; Matsumoto et aI., 2001) or else
show evidence of enlarged ventricles (Cahn et aI., 2002).These findings suggest that some brain abnormalities maypredate the illness rather than develop as a result ofuntreated psychosis or as a consequence of taking neu-roleptic medications (Bogerts, 1993; Hoff et aI., 2000).Studies of neuropsychological test performance (Heatonet aI., 1994; Hoff et aI., 1992) lead' us to essentially the sameconclusion. Patients who have only recently become illperform about the same on neuropsychological tests aspatients who have been ill for many years (and both groupsobviously perform worse than controls). This suggeststhat many of the problems that characterize patients arepresent early in the illness. In other words, the neuropsy-chological data and the neuroanatomical data supportschizophrenia being a neurodevelopmental disorder ratherthan a neurodegenerative or progressively deterioratingdisorder (see Cannon, 1998a, 1998b; Heaton et aI., 2001).
The idea that brain abnormalities in patients withschizophrenia progressively get worse with time shouldnot be dismissed too readily, however. An MRI study of asmall sample of children with schizophrenia who receivedbrain scans on two separate occasions 2 years apartshowed that their brain volumes were smaller at the sec-ond assessment (Jacobsen et aI., 1998). A similar decreasein brain volume was not found in the healthy control par-ticipants. Other researchers have also reported that adultpatients with schizophrenia show more rapid declines intotal brain volume than healthy controls (Mathalon et aI.,2001). Moreover, evidence suggests that these brainchanges occur early in the illness. Cahn and colleagues(2002) measured changes in the overall volume of graymatter (which is made up of nerve cells) in patients whowere experiencing their first episode of schizophrenia.Thirty-four patients and 36 matched healthy comparisonsubjects received MRI brain scans at the start of the studyand then again 1 year later. The results showed that thevolume of gray matter declined significantly over time inthe patients but not in the controls. More specifically,
MRI scans of 28-year-old male identical twins,showing the enlarged brain ventricles in the twinwith schizophrenia (right) compared with his wellbrother (left).
Source: E. Fuller Torrey, M.D., The Treatment AdvocacyCenter.

there was almost a 3 percent decrease in the volume ofgray matter in the patients in the I-year period betweenthe first and the second scans. Although progressive brainchanges are not invariably found (e.g., Lieberman et aI.,2001), results like these suggest that, in addition to being aneurodevelopmental disorder, schizophrenia may also becharacterized by progressive brain changes. Kraepelin's
Compared with normal adolescents, young people withearly-onset schizophrenia show a progressive loss of graymatter in their brains over time. MRI scans repeated over a5-year period show a much greater loss of brain tissue inpatients with schizophrenia than in healthy controls.Graymatter loss occurs in many brain areas, beginning inparietal cortex and spreading to temporal cortex and frontalcortex.Source: Thompson et 01., 2000.
use of the term dementia praecox may have been highlyappropriate after all.
SPECIFIC BRAIN AREAS In recent years much researchhas focused on the question of what particular brain struc-tures are especially involved in schizophrenia. Althoughmuch remains to be learned, there is evidence of problems
4.~ Pain Insensitivity andSchizophrenia
Pain is a very familiar sensation for most ofus. Yet for some patients with schizophre-nia, this may not be true (Dworkin, 1994).A century ago, Kraepelin (1919(1989)observed that "the patients often become
less sensitive to bodily discomfort; they endure uncom-fortable positions, pricks of a needle, injuries, withoutthinking much about it" (p. 34); and Bleuler (1924(1988)similarly noted "an analgesia, which occurs not too rarelyand which is sometimes quite complete" (p. 400).
These observations of pain insensitivity in schizophre-nia are supported by anecdotal accounts and case reportsin the medical and surgical literatures. One case describeda male patient with schizophrenia who had a perforatedbowel and who reported only occasional mild discomfortand showed surprisingly little abdominal tenderness dur-ing a physical examination (Rosenthal et aI., 1990). Otherreports described patients with such medical problems asa perforated and gangrenous gallbladder (Bickerstaff et aI.,1988), a perforated ulcer, a broken ankle (Fishbain, 1982),and a ruptured appendix (Geschwind, 1977), who nonethe-less seemed to experience little pain. In some cases the
atypical presentations of some schizophrenia patients withrespect to physical pain put them at risk of being misdiag-nosed or of potentially serious medical problems beingoverlooked (Bickerstaff et aI., 1988).
Pain insensitivity in schizophrenia is not a ubiquitousphenomenon, and some patients do report pain(Delaplaine et aI., 1978; Torrey, 1989). What is especiallyinteresting, however, is that a significant minority of therelatives of patients with schizophrenia also appear tohave much higher pain tolerance than do controls with nofamily history of mental illness (Hooley & Chung, 2003;Hooley & Delgado, 2001). We have no idea as yet why thisshould be. However, several areas ofthe brain that areinvolved in pain perception are brain regions that havebeen implicated in schizophrenia. Included here are thethalamus and the anterior cingulate (Benes & Bird, 1987).The neurotransmitter glutamate is also involved in thetransmission of noxious stimuli. Although pain insensitiv-ity is a rather neglected topic in schizophrenia research(see Dworkin, 1994), it may provide us with some moreclues that will help us get closer to solving the puzzle ofschizophrenia.

not seem to be able to kick into action when patients per-form complex tasks (see Figure 14.9). Again, however, thisproblem characterizes only a minority (albeit a substantialminority) of patients with schizophrenia (e.g., Buchsbaumet a1., 1992; Heinrichs, 2001). Nonetheless, frontal lobedysfunction is believed to account for some of the negativesymptoms of schizophrenia and perhaps to be involved insome attentional-cognitive deficits (Cannon et a1., 1998;Goldman-Rakic & Selemon, 1997).
There is also evidence that the temporal lobes (whichhave many connections to and from the frontal lobes) andother medial temporal areas such as the hippocampus(which is involved in memory) and the amygdala (which isinvolved in emotion) are compromised in schizophrenia(C; Bogerts, 1997; Haber & Fudge, 1997; Nelson et a1.,1998). Here again, there are still many unresolved orunreconciled findings, and large numbers of patients havetemporal lobe volumes within normal limits (Crow, 1997;Heinrichs, 2001; Weinberger, 1997). But the consensusappears to be that these regions, perhaps especially on theleft side, are somehow implicated and that they may belinked to positive symptoms (Bogerts, 1997; Cannon et a1.,
in the frontal lobes and in the temporal lobes and suchneighboring (medial temporal) areas as the amygdala, hip-pocampus, and the thalamus (Ettinger et a1., 2001; Gur &Pearlson, 1993; Lawrie & Abukrneil, 1998; Tamminga et a1.,2002; Weinberger, 1997). Again, however, we must empha-size that most patients have brains that look essentiallynormal and that many of the differences reported are notspecific to schizophrenia. As you know from other chaptersin this book, some of these brain areas are implicated inother conditions (e.g., severe mood disorders) as well.Brain areas such as the thalamus are also involved in sensi-tivity to pain, which, interestingly, is greatly diminished inmany patients with schizophrenia, as well as in some oftheir relatives (see Developments in Research 14.2).
The importance of the frontal lobes is reflected intheir large size relative to the rest of the brain. Many stud-ies have demonstrated that patients with schizophreniashow abnormally low frontal lobe activation (known as"hypofrontality") when they engage in mentally challeng-ing tasks such as the Wisconsin Card Sorting Test (WCST)or in other tests generally thought to require substantialfrontal lobe involvement. Essentially, this brain area does
BASAL GANGLIAInvolved in movement andemotions and in integratingsensory information. Abnormalfunctioning in schizophrenia isthought to contribute toparanoia and hallucinations.(Excessive blockade ofdopamine receptors in the basalganglia by traditionalantipsychotic medicines leads tomotor side effects.)
AUDITORY SYSTEMEnables humans to hear and understand speech. Inschizophrenia, overactivity of the speech area (calledWernicke's area) can create auditory hallucination-the illusion that internally generated thoughtsare real voices coming from the outside.
OCCIPITAL LOBEProcesses information aboutthe visual world. People with
schizophrenia rarely have full·blown visual hallucinations, but
disturbances in this areacontribute to such difficulties as
interpreting complex images,recognizing motion, and reading
emotions on others' faces.
FRONTAL LOBE ~Critical to proble~~~lv,ing" ~insight and other high-levelreasoning. Perturbations inschizophrenia lead to difficultyin planning actions andorganizing thoughts.
HIPPOCAMPUSMediates learning and memory
formation, intertwinedfunctions that are impaired in
schizophrenia.LIMBIC SYSTEMInvolved in emotion.Disturbances are thought tocontribute to the agitationfrequently seen in schizophrenia.
The Brain in SchizophreniaMany brain regions and systems operate abnormally in schizophrenia, including those highlighted below. Imbalances in theneurotransmitter dopamine were once thought to be the prime cause of schizophrenia. But new findings suggest that impoverishedsignaling by the more pervasive neurotransmitter glutamate-or, more specifically, by one of glutamate's key targets on neurons (theNMDA receptor) -better explains the wide range of symptoms in this disorder.

1998; Woodruff et al., 1997). It is also interesting to notethat the left temporallob@ is thought to be the last brainregion to complete neuronal migration. Because of this, itmay be especially vulnerable to injury and insult (Satz &Green, 1999).
Finally, evidence is emerging that the volume of thethalamus is reduced in patients with schizophrenia relativeto controls (Andreasen et al., 1994; Ettinger et al., 2001).The thalamus receives virtually all incoming sensory input.This relay center of the brain connects with many differentareas. It is tempting to speculate that a thalamus reduced involume may be less able to do its job and to successfully fil-ter out, or "gate," irrelevant information. The result may bethat patients become flooded with sensory information.
CYTOARCHITECTURE As we have seen, one hypothesisabout schizophrenia is that genetic vulnerabilities, perhapscombined with prenatal insults, can lead to disruption ofthe migration of neurons in the brain. If this is true, somecells will fail to arrive at their final destinations, and theoverall organization of cells in the brain (the brain'scytoarchitecture) will be compromised. There are alsoother ways in which the organization of cells in the braincould be disrupted. For example, we all have an excess ofsynapses well into our late teens. This "neuronal redun-dancy" is eventually diminished by synaptic pruning,whereby unnecessary neuronal connections are essentiallydeleted. Programmed cell death (which involves the eradi-cation of surplus cells) is also a natural developmentalevent (see Weickert & Weinberger, 1998, for a usefuloverview). If any or all of these processes are disrupted, thedensity and positioning of the cells in the brain will be indisarray.
Although the brains of people with schizophrenia arealmost certainly different from the brains of people whodo not have schizophrenia, the precise nature of these dif-ferences is still under investigation. Using painstakingcounting techniques on postmortem brain slices, Benesand her colleagues have demonstrated that patients withschizophrenia have lower densities of neurons in certainbrain regions such as the prefrontal cortex than do con-trols (1986). Other researchers, using more complex,three-dimensional counting techniques have reported anincrease in neuronal density in the brains of patients withschizophrenia (see Selemon, 2004). There are also abnor-malities in the distribution of cells in different layers of thecortex and hippocampus (Arnold, 2000; Kalus et al., 1997;Selemon et al., 1995), as well as evidence that patients withschizophrenia are missing particular types of neuronsknown as "inhibitory interneurons" (Benes, 2000; Beneset al., 1991). These neurons are responsible for regulatingthe excitability of other neurons. Their absence may meanthat bursts of activity by excitatory neurons in the brain gounchecked. Again, research suggests that the brains ofpatients with schizophrenia may be less able to regulate ordampen down overactivity in certain key circuits (see
Daskalakis et al., 2002). As we will see shortly, patients withschizophrenia have difficulty handling even normal levelsof stress. Given what we have just learned, this makes agreat deal of sense.
SYNTHESIS The brain is clearly compromised in schizo-phrenia, although the compromise is often very subtle.Some of the brain abnormalities that are found are likelyto be genetic in origin. Others may reflect environmentalinsults. For example, Baare and colleagues used MRI tostudy the brains of MZ and DZ twins who were discordantfor schizophrenia and then compared the results for thesegroups to results from a group of healthy twins. Whatthese researchers found was that the patients with schizo-phrenia had smaller brain volumes than their well co-twins. What was interesting, however, was that these wellco- twins also had smaller brains than the healthy controltwins. Baare and his colleagues (2001) propose thatgenetic risk for schizophrenia may be associated withreduced brain development early in life. This is why thehealthy twins who had a co-twin with schizophrenia hadsmaller brain volumes than the healthy controls. Baareand his colleagues (2001) also hypothesize that patientswho develop schizophrenia suffer additional brain abnor-malities that are not genetic in origin. This explains whythey had smaller brain volumes than their discordant co-twins. In people at genetic risk for schizophrenia (but notin those without genetic risk), a history of fetal oxygendeprivation has been shown to be associated with brainabnormalities in later life (Cannon et al., 2002). In otherwords, what we may have here is an excellent example ofhow genes can create an enhanced susceptibility to poten-tially aversive environmental events. Moreover, even whenboth members of a twin pair have identical genes (as is thecase for MZ twins), if only one of them experiences theenvironmental insult (for example, a birth cord aroundthe neck, creating hypoxia), this would explain why onetwin might be pushed across the threshold into illnesswhile the co-twin remained healthy.
Finally, we emphasize that it is unlikely that schizo-phrenia is the result of anyone problem in anyone specificregion of the brain. The brain is comprised of functionalcircuits-regions that are linked to other regions by a net-work of interconnections. If there is a problem at any pointin the circuit, the circuit will not function properly. Thefocus now is on learning how the brain is wired and whatregions are functionally linked. The brain abnormalitiesassociated with schizophrenia are not massive, and thereare no specific brain abnormalities that invariably distin-guish patients with schizophrenia from healthy people. Itmay be, however, that subtle brain abnormalities in somekey functional circuits may wreak havoc with normalfunctioning (see Mendrek et al., 2004). As we gain moreknowledge about how the brain does its job, perhaps wewill understand more about how the brain is compro-mised in schizophrenia.

NEUROCHEMISTRY The idea that serious mental disor-ders are due to "chemical imbalances" in the brain is nowcommonplace. This phrase is often used to provide a gen-eral explanation of why someone has a disorder like schizo-phrenia. But the notion of "chemical imbalance" is vagueand imprecise. All it really conveys is the widely acceptednotion that alterations in brain chemistry may be associ-ated with abnormal mental states. This idea became veryclear to researchers shortly after LSD was first synthesizedin 1947. The profound mental changes associated withLSD prompted those interested in schizophrenia to con-sider the possible biochemical basis of the disorder.
The most important neurotransmitter implicated inschizophrenia is dopamine. The "dopamine hypothesis"(as it is called) dates back to the 1960s and was derivedfrom three important observations. The first is the phar-macological action of the drug chlorpromazine (Tho-razine). Chlorpromazine was first used in the treatment ofschizophrenia in 1952. It rapidly became clear that thisdrug was helpful to patients. Eventually, it was learned thatthe therapeutic benefits of chlorpromazine were linked toits ability to block dopamine receptors.
The second piece of evidence implicating dopaminein schizophrenia came from an entirely different direc-tion. Amphetamines are drugs that produce a functionalexcess of dopamine (i.e, the brain acts as if there is toomuch dopamine in the system). In the late 1950s and early1960s, it began to be seen that abuse of amphetamines led,in some cases, to a form of psychosis that involved para-noia and auditory hallucinations (Connell, 1958; Kalant,1966; Tatetsu, 1964). There was thus clinical evidence thata drug that gave rise to a functional excess of dopaminealso gave rise to a psychotic state that looked a lot likeschizophrenia.
The third piece of indirect evidence linking dopamineto schizophrenia came from clinical studies that actuallytreated patients by giving them drugs that increase theavailability of dopamine in the brain. An example here isParkinson's disease (see Chapter 15), which is caused by lowlevels of dopamine in a specific brain area (the basal gan-glia) and is treated with a drug called L-DOPA. Psychoticsymptoms are a significant complication of treatment withL-DOPA. Again, then, the circumstantial evidence pointedto the role of dopamine in inducing psychosis.
How could dopamine induce psychosis? Activity inthe dopamine system may playa role in determining howmuch salience we give to internal and external stimuli.Dysregulated dopamine transmission may actually makeus pay more attention to and give more significance tostimuli that are not especially relevant or important. Thisis called "aberrant salience" (see Kapur, 2003). If this is thecase, it is quite easy to see why patients might develop delu-sions or experience hallucinations and why psychoticexperiences might be so shaped by the patient's culture andhistory. In the early stages of their illnesses, patients oftenreport heightened sensory awareness ("My senses were
sharpened. I became fascinated by the little insignificantthings around me:') or increased meaning in events ("I feltthat there was some overwhelming significance in this"). Ifdopamine creates aberrant salience, the person will strug-gle to make sense of everyday experiences that were previ-ously in the background but that now have becomeinappropriately important and worthy of attention. In thisway, the hum of a refrigerator could become a voice talk-ing; or the arrival of a package could signal a threat, whichthen prompts the patient to look carefully at the subtlebehaviors of others to see who could be a source of harmand persecution.
But how might a functional excess of dopamine inthe system come about? One way is through too muchdopamine available in the synapse (the gap between nervecells that has to be "bridged" by a neurotransmitter for anerve impulse to be carried from one neuron to another).This could be accomplished by increasing the synthesis orproduction of dopamine, by releasing more of it into thesynapse, by slowing down the rate at which dopamine ismetabolized or broken down once it is in the synapse, or byblocking neuronal reuptake (the "recycling" of dopamineback into the neuron). Any or all of these could increasethe overall availability of dopamine. There is also anotherway in which a functional excess of dopamine could beproduced or, more accurately, mimicked. If the receptorsthat dopamine acts on (i.e., those on the postsynapticmembrane) are especially dense and prolific or if they areespecially sensitive, the effects of a normal amount ofdopamine being released into the synapse would be multi-plied. In other words, the system acts as though there weremore dopamine available even though there really isn't.This is what we call "receptor supersensitivity."
Researchers have been acutely interested in learningabout dopamine in the brains of people with schizophre-nia, but research is hampered by the fact that braindopamine can be measured only in the postmortem brainand then only with some technical difficulties. Because ofthis, researchers have largely had to be content to studydopamine indirectly by measuring its major metabolite(what most of it is converted into). The major metaboliteof dopamine is homovanillic acid, or HVA. However, HVAis best collected in cerebrospinal fluid (CSF). This requiresthat the patient agree to a lumbar puncture, which involvesa large needle being inserted into the spine to draw offfluid. Not only is this potentially dangerous, it also leavesthe patient with a violent headache.
Studies that have examined concentrations of HVA inthe CSF of patients with schizophrenia and in controls haveyielded generally negative results (see Heinrichs, 2001;Owen & Simpson, 1995). The same is true of postmortemstudies. In general, there seems to be no strong evidence tosupport the idea that patients with schizophrenia are pro-ducing more dopamine than controls are. In light of this, itis hardly surprising that more recent research efforts havemoved toward exploring the idea that the problem lies not

in overall dopamine levels (dopamine turnover) but inreceptor sensitivity.
Most of the research has concerned a type ofdopamine receptor called a D2 receptor although we knowthat there are at least five dopamine receptor subtypes(D1-D5) and that more may be discovered. In general,postmortem studies show that there are more D2 receptorsin the brains of patients with schizophrenia than in con-trols-in fact, some 60 to 110 percent more (McKenna,1997). Although this would seem to support the dopaminehypothesis of schizophrenia, there is a major problem: Thedrugs used to treat schizophrenia (known as "neurolep-tics") are also known to cause postsynaptic receptor super-sensitivity. Because virtually all patients with schizophreniareceive neuroleptics, it is impossible to know whether theincreased density of D2 receptors is associated with theschizophrenia or with the neuroleptic medications thepatients have received during their lives. Ironically, then,the drugs that played such a major role in the developmentof the dopamine hypothesis may have made it almostimpossible for us to determine whether that hypothesis iscorrect!
But modern technology has given us a way around theproblem. PET scans enable us to study the working brainand to look at the density of dopamine receptors in livingpatients. Even more important, PET studies can be donebefore patients receive any medications for their schizophre-nia (so-called drug-naIve patients). Several studies have nowbeen done. One group (Wong et al., 1986) found evidencefor a more-than-twofold increase in D2 receptors in patientswith schizophrenia, compared with controls, and later repli-cated these results (Gjedde & Wong, 1987). Another group(Farde et al., 1987, 1990) found no significant differencesbetween the patients and the controls. So far, the decisive testof the dopamine hypothesis has not yielded decisive results.Different methodological approaches used by the differentresearch teams may be one reason why.
What is the current status of the dopamine hypothe-sis? Certainly, there is support for the idea that schizophre-nia involves abnormal dopaminergic function. Althoughmuch of the evidence is still circumstantial, the prolifera-tion of dopamine receptors in the postmortem brains ofschizophrenia patients clearly suggests a biologically basedabnormality. Although some increase in receptor densitymay be the result of neuroleptic treatment, some PETstudies with drug-naIve patients support the idea of recep-tor supersensitivity in schizophrenia. Thus researchers donot yet have good reason to abandon the dopaminehypothesis. Current thinking, however, is that schizophre-nia also involves problems in other neurotransmitter sys-tems. Before leaving our discussion of the neurochemistryof schizophrenia we take a quick look at another key neu-rotransmitter that is attracting a lot of attention.
Glutamate is an excitatory neurotransmitter that iswidespread in the brain. As was the case for dopamine,there are a number of reasons why researchers have begun
to suspect that a dysfunction in glutamate transmissionmight be involved in schizophrenia. First, PCP, or angeldust, is known to block glutamate receptors. PCP alsoinduces symptoms (both positive and negative) that arevery similar to those of schizophrenia. Moreover, whenpeople with schizophrenia take PCP, it exacerbates theirsymptoms.
Second, physicians had to stop using ketamine, whichis an anesthetic, because when it is given intravenously tonormal subjects, it produces schizophrenia-like positiveand negative symptoms (see Krystal et al., 2005). Whengiven to patients whose schizophrenia is stable and wellcontrolled, ketamine exacerbates hallucinations, delu-sions, and thought disorder. But what is all the moreremarkable about ketamine is that it does not cause any ofthese problems when it is administered to children, forwhom it continues to be used as an anesthetic. This sug-gests that age (and brain maturity) determines whetherketamine causes psychosis.
Like PCP, ketamine blocks glutamate receptors.Researchers are now exploring concentrations of gluta-mate in postmortem brains of patients with schizophreniaand finding lower levels of glutamate in both the prefrontalcortex and the hippocampus, compared with control sub-jects (Goff & Coyle, 2001). Olney and Farber (1995) haveproposed that diminished activity at certain types of gluta-mate receptors (known as "NMDA" receptors) may notonly trigger schizophrenia-like symptoms but also causethe degeneration of neurons in key brain areas. In otherwords, if the NMDA receptors are not normally active(perhaps because glutamate levels are low), subtle braindamage may result.
The glutamate hypothesis of schizophrenia is nowattracting a lot of research attention. It is also promptingthe development of new experimental drugs such asglycine that are designed to activate glutamate receptors.This research is still in its early stages but holds muchpromise (Goff & Coyle, 2001).
Finally, does the importance of glutamate challengethe importance of dopamine in the neurochemistry ofschizophrenia? No. One action of dopamine receptors is toinhibit the release of glutamate. Simply stated, an overac-tive dopaminergic system could result in excessive sup-pression of glutamate, leading to the underactivity of theNMDA receptors. The dopamine hypothesis of schizo-phrenia is actually made all the more credible by discover-ies about glutamate.
NeurocognitionGiven all that you have learned about the brain abnormal-ities associated with schizophrenia, it should come as nosurprise that schizophrenia patients experience problemsin many aspects of their neurocognitive functioning (seeCornblatt et al., 1999, or Green, 1997, for reviews). In fact,the range of deficits is so broad that it is fair to say that

schizophrenia manifests itself more in defective cognitionthan in defective biology (Heinrichs, 2001). For example,in reaction time studies that require subjects to respond toa stimulus as quickly and appropriately as possible, schizo-phrenia patients do poorly compared with controls (seeNuechterlein, 1977). They also show deficits on the Con-tinuous Performance Task (CPT; e.g., Cornblatt et a!.,1989). This task requires the subject to attend to a series ofletters or numbers and then to detect an intermittentlypresented target stimulus that appears on the screen alongwith other letters or numbers (e.g., "Press when you see thenumber 7"). There are also problems with working mem-ory (Barch, 2005; Park et a!., 1995), which can be thoughtof as our "mental blackboard." Paralleling the findings forthe Wisconsin Card Sort Test that we described earlier,patients with schizophrenia show less prefrontal brainactivity than healthy controls when they engage in tests ofworking memory (Cannon et a!', 2005).
Somewhere between 54 and 86 percent of people withschizophrenia also show eye-tracking dysfunction and aredeficient in their ability to track a moving target such as apendulum (Cornblatt et a!., 1999). This is a skill referred toas smooth-pursuit eye movement (Holzman et a!., 1988,1998; Levy et a!., 1983, 1993; Lieberman et a!., 1993). Incontrast, only about 6 to 8 percent of the general popula-tion show problems with eye-tracking. Especially interest-ing is that around 50 percent of the first-degree relatives ofschizophrenia patients also show eye-tracking problemseven though they do not have schizophrenia themselves(e.g., Clementz et a!., 1992; Iacono et a!., 1992; Levy et a!',1993 Sporn et a!', 2005). This suggests that disturbances ineye-tracking have a genetic basis. Moreover, when healthyvolunteers are given ketamine (the NMDA receptor antag-onist, or blocker, that we described earlier), they developeye-tracking problems similar to those found in schizo-phrenia patients (Avila et a!., 2002). This provides us withanother clue that problems with NMDA receptors (whichdetect the neurotransmitter glutamate) are somehowinvolved in the pathophysiology of schizophrenia.
Perhaps the strongest finding in the area of neuro-cognition and schizophrenia, however, concerns a psy-chophysiological measure called "P50" (see Heinrichs,2001). When two clicks are heard in close succession, thebrain (receiving the auditory signal) produces a positiveelectrical response to each click. This response is called P50because it occurs 50 milliseconds after the click. In normalsubjects, the response to the second click is less markedthan the response to the first click because the normalbrain dampens, or "gates," responses to repeated sensoryevents. If this didn't happen, habituation to a stimuluswould never occur. Many patients with schizophrenia, incontrast, respond almost as strongly to the second click asto the first. This is referred to as "poor P50 suppression."First-degree family members of patients with schizophre-nia are also more likely than controls to have problemswith P50 suppression (Clementz et a!., 1998). It has been
suggested that poor P50 suppression is the result of prob-lems with specific receptors in the hippocampus of themedial temporal lobe (Adler et a!', 1998). As you mayrecall, the hippocampus is one brain region that appears tobe compromised in schizophrenia. Cells in the hippocam-pus are also especially susceptible to damage from hypoxiaduring brain development.
Taken together, the weight of the evidence suggeststhat patients with schizophrenia have problems with theactive, functional allocation of attentional resources. Whatthis means is that they are unable to attend well ondemand. Although many of the findings may not be highlyspecific to schizophrenia (some of the neurocognitivedeficits can be found in patients with mood disorders, forexample), attentional dysfunctions may be indicators of abiological susceptibility to at least some forms of schizo-phrenia (Cornblatt et a!', 1992).
INTEGRATION Biological factors undoubtedly play arole in the etiology of schizophrenia. But genetic predispo-sitions can be shaped by environmental factors such asprenatal exposures. We have also seen that when childrenat genetic risk for schizophrenia are adopted into familiesthat show maladaptive rearing styles or deviant communi-cation patterns, they are at increased risk of problems lateron. In contrast, children at genetic risk who are adoptedinto healthy family environments do very well (Tienariet a!., 2004; Wahlberg et a!., 1997). The diathesis-stressmodel, whose origins largely derive from schizophreniaresearch, predicts exactly these sorts of scenarios (e.g.,Walker & Diforio, 1997; Zubin & Spring, 1977).
Psychosocial and Cultural AspectsDO BAD FAMILIES CAUSE SCHIZOPHRENIA? Yearsago, parents were routinely assumed to have caused theirchildren's disorders through hostility, deliberate rejection,or gross parental ineptitude. Many professionals blamedparents, and their feedback to them was often angry andinsensitive. Mothers were particularly singled out for criti-cism. The idea of the "schizophrenogenic mother" whosecold and aloof behavior was the root cause of schizophre-nia was very influential in many clinical circles (Fromm-Reichman, 1948). Not surprisingly, this was a bad thingfor families. Not only were they faced with the difficultiesof coping with a son or daughter who had a devastatingillness (see The World Around Us 14.3 on p. 518 for adescription of what it is like to live with schizophrenia inthe family), but they suffered all the more because of theblame that was directed toward them by mental healthprofessionals.
Today, things are very different. Theories that werepopular 40 years ago have foundered for lack of empiricalsupport-for example, the idea that schizophrenia wascaused by destructive parental interactions (Lidz et aI.,1965). Another idea that has not stood the test of time is

14.3Schizophrenia is a disorder that easily captures
attention. Because of this, the difficulties facedby family members who must cope with the ill-ness in a loved one can sometimes be over-looked. Schizophrenia can wreak havoc in the
most healthy of families. It is hardto be the parent of a son or daugh-ter with the disorder, and growingup with a mother or father who suf-fers from schizophrenia is fraughtwith its own set of problems.
In her book Mad House, (leaSimon (a Boston author; 1997)describes what it was like for her togrow up with two older siblingswho developed schizophrenia. (leawas only 8 years old when her sis-ter, Katherine, succumbed toschizophrenia at age 16. Shortlyafter this, her older brother, Daniel,whom she adored, also dissolvedinto madness. He began to hearvoices while he was a freshman atHarvard, dropped out of school, and was diagnosed withschizophrenia. In her book C1eadescribes a happy child-
hood abruptly terminated by late-night phone calls fromthe police and from hospitals. She describes Katherine'sscreaming panics and how, powerless to prevent it, shewatched Katherine kill her beloved hamster in a fit of rage.She also speaks of her sadness at losing the brother who
doted on her and gave her piggy-back rides.
Like her parents, C1eatried tocope as best she could. She sensedher parents needed to see that shewas happy, and so she acted happy.Yet she felt alone and stranded. Asshe approached adolescence, shealso felt afraid. None of her siblingshad made it through adolescencewithout going crazy. Following inher father's footsteps and going toHarvard, she was also acutelyaware that she was retracing herbrother Daniel's steps too. Shemade it through, but not withouther own personal struggles. As the"well sibling," it has taken her
many years to come to terms with what happened to herbrother and sister.
Author Cleo Simon grew up with twoolder siblings who both developedschizophrenia in their teens.
the double-bind hypothesis (Bateson, 1959, 1960). A doublebind occurs when the parent presents the child with ideas,feelings, and demands that are mutually incompatible (forexample, a mother may complain about her son's lack ofaffection but freeze up or punish him when he approachesher affectionately). According to Bateson's etiologichypothesis, such a son is continually placed in situationswhere he cannot win, and he becomes increasingly anx-ious. Presumably, over time, such disorganized and contra-dictory communications in the family come to be reflectedin his own thinking. However, no solid confirmation of thepathogenicity of double-bind communications has everbeen reported.
Instead, research has taught us that disturbances andconflict in families that include an individual with schizo-phrenia (e.g., Hirsch & Leff, 1975) may well be caused byhaving a severely ill and psychotic person in the family. Inother words, rather than causing the schizophrenia, familycommunication problems could be the result of trying tocommunicate with someone who is severely ill and disor-ganized (Liem, 1974; Mishler & Waxler, 1968). Of course,
some families do show unusual communication patternsthat we now refer to as "communication deviance" (Singeret aI., 1978; Wynne et aI., 1979). Current thinking is thatthese amorphous and fragmented communications mayactually reflect genetic susceptibility to schizophrenia onthe part of the relative (Hooley & Hiller, 2001; Miklowitz& Stackman, 1992). However, as we know from theFinnish Adoption Study, adverse family environments andcommunication deviance probably have little pathologi-cal consequence if the child who is exposed has no geneticrisk for schizophrenia (Tienari et aI., 2004; Wahlberget aI., 1997).
FAMILIES AND RELAPSE Although schizophrenia isoften a chronic disorder, its symptoms may be especiallysevere at some times (i.e., when there is a relapse) and lesssevere at other times (for example, during a period ofremission). In 1958, George Brown and his colleagues(Brown et aI., 1958) observed that how patients withschizophrenia fared clinically after they left the hospitaldepended a lot on what kind of living arrangement they

returned to. Surprisingly, patients who returned home tolive with parents or with a spouse were at higher risk ofrelapse than patients who left the hospital to live alone orwith siblings. Brown reasoned that highly emotional fam-ily environments might be stressful to patients. Unlikeresearchers on the other side of the Atlantic, however, hesuspected that what might be important was not the pres-ence of markedly disturbed or pathological patient-family relationships (although those certainly existed insome families) but something much more ordinary andcommonplace. Brown's hunch was that researchers shouldfocus on "the range of feelings and emotions to be foundin ordinary families" (Brown, 1985, p. 22). This was anunusual insight at the time. As Brown himself remem-bers, "In 1956 there was little hint in the literature ofBritish psychiatry that the core symptoms of schizophre-nia might be importantly influenced by social experience"(1985, p. 10). Viewing his insight today in the context ofthe diathesis-stress model, we see just how prescientBrown was.
In a series of studies, Brown and his colleagues wenton to develop and refine the construct of expressed emo-tion, or EE. Expressed emotion is a measure of the familyenvironment that is based on how a family memberspeaks about the patient during a private interview with aresearcher. It has three main elements: criticism, hostility,and emotional overinvolvement (EOI). The most impor-tant of these is criticism, which reflects dislike or disap-proval of the patient. Hostility is a more extreme form ofcriticism that indicates a dislike or rejection of the patientas a person. Finally, EOI reflects dramatic or overcon-cerned attitude on the part of the family member towardthe patient's illness.
EE is important because it has been repeatedly shownto predict relapse in patients with schizophrenia. In ameta-analysis of 26 studies, Butzlaff and Hooley (1998)demonstrated that living in a high-EE home environmentmore than doubled the baseline level of relapse risk forschizophrenia patients in the 9 to 12 months after hospi-talization. Moreover, even though EE predicts relapseregardless of whether the patients studied have been ill fora short, medium, or long time, EE seems to be an espe-cially strong predictor of relapse for patients who arechronically ill.
Of course, it could be that families simply tend to bemore critical of patients who are more severely ill and thatthis is why EE and relapse are correlated. However, a reviewof the literature provides no strong support for thisassumption (see Hooley et al., 1995). Also, EE predictsrelapse even when potentially important patient variablesare controlled statistically (Nuechterlein et al., 1992).Finally, research shows that when EE levels in families arelowered (usually by clinical interventions), patients'relapse rates also decrease (Falloon et al., 1985; Hogartyet al., 1986; Lam, 1991; Leff et al., 1982; Jesus-Mari &
Patients with schizophrenia who live in families where there is ahigh level of emotional tension have more than twice the risk ofrelapse.
Streiner, 1994; McFarlane et al., 1995). This suggests thatEE may playa causal role in the relapse process.
But how might EE trigger relapse? There is a greatdeal of evidence that patients with schizophrenia arehighly stress-sensitive. Consistent with the diathesis-stressmodel, environmental stress is thought to interact withpreexisting biological vulnerabilities to increase the proba-bility of relapse (Nuechterlein et al., 1992). We know, forexample, that independent stressful life events occur morefrequently just prior to psychotic relapse than at othertimes (Ventura et al., 1989, 1992) and may exert theireffects over longer periods of time too. Furthermore, in athoughtful review, Walker and Diforio (1997) note thatone of the primary manifestations of the stress response inhumans is the release of cortisol (a glucocorticoid) fromthe adrenal cortex. Animal and human studies show thatcortisol release triggers dopamine activity (McMurrayet al., 1991; Rothschild et al., 1985). Glucocorticoid secre-tion also affects glutamate release (Horger & Roth, 1995;Walker & Diforio, 1997). In other words, two of the majorneurotransmitters implicated in schizophrenia (dopamineand glutamate) are affected by cortisol, which is releasedwhen we are stressed.
Along these lines, Hooley and Gotlib (2000) have sug-gested that, to the extent that high-EE behaviors exhibitedby family members are perceived as stressful by patients,these behaviors are likely to trigger the release of cortisol.In support of this idea, high-EE relatives have been foundto be more behaviorally controlling of patients thanlow-EE relatives are (Hooley & Campbell, 2002). Whenthey try to help, they seem to do so in rather intrusive ways(e.g., "She wouldn't go to sleep so I held her head downonto the pillow"). Furthermore, controlling behaviorssuch as these predict relapse in patients with schizophre-nia. Quite possibly, relatives' well-meaning attempts to getpatients to function better simply backfire. If patients are

stressed by what the relatives do) this could increase corti-sol levels, affect important neurotransmitter systems, andperhaps eventually lead to a return of symptoms.
At the present time, we have no direct evidence thatthis happens. However, one study is worthy of note. Agroup of researchers studied the behavior of patients withschizophrenia when they were involved in interactions withhigh-EE and low-EE relatives (Rosenfarb et al., 1995). Theresearchers observed that when patients said somethingstrange (e.g., "If that kid bites you, you'll get rabies"), high-EE relatives tended to respond by being critical of thepatient. What was interesting was that when this happened,it tended to be followed by another unusual remark fromthe patient. In other words, an increase in patients' unusualthinking occurred immediately after the patient was criti-cized by a family member. Although other interpretationsof the findings are possible, the results of this study are con-sistent with the idea that negative (stress-inducing) behav-iors by relatives can trigger increases in unusual thinking inpatients with schizophrenia. Although we have no way ofknowing what was happening to the cortisol levels of thesepatients, it is intriguing to speculate that increased cortisolrelease might somehow be involved.
URBAN LIVING Being raised in an urban environmentseems to increase a person's risk of developing schizophre-nia. Pederson and Mortensen (2001) studied a large sam-ple of 1.9 million people in Denmark, a country whereinformation about where people live is recorded in anational register and where people have to notify authori-ties when they change addresses in order to retain eligibil-ity for benefits. The researchers found that children whospent the first 15 years of their lives living in an urban envi-
Research suggests that growing up in an urban environmentincreases a person's risk of developing schizophrenia inadulthood.
rQnm~ t w~r~~ 7~ tim~s mor~ likely to dcvdop 5~hizo-phrenia in adulthood than were children who spent theirchildhoods in more rural settings. Other methodologicallysound studies also confirm this association (Sundqusistet al., 2004). Although the reasons for the link betweenurban living and the later development of schizophreniaare not clear, studies of this kind raise the possibility thatsome cases of schizophrenia may have environmentalcauses (van as, 2004). What is so problematic about urbanliving is still unknown, however.
IMMIGRATION The findings showing that urban livingraises a person's risk for developing schizophrenia suggestthat stress or social adversity might be important factors toconsider with respect to this disorder. Supporting this idea,research is also showing that recent immigrants have muchhigher risks of developing schizophrenia than do peoplewho are native to the country of immigration. Looking atthe results of 40 different studies involving immigrantgroups from many different parts of the world, Cantor-Grace and Selten (2005) found that first-generationimmigrants (i.e., those born in another country) had 2.7times the risk of developing schizophrenia; for second-generation immigrants (i.e., those with one or both par-ents having been born abroad) the relative risk was evenhigher at 4.5. In other words, there is something aboutmoving to another country that appears to be a risk factorfor developing schizophrenia. The following case studyillustrates this.
Schizophrenia in anImmigrant from China
Ayoung Chinese woman was sent by her parents to live inIreland after she lost her job in China and was unable tofind another. She enrolled in language school and subse-quently began to study for a master's degree in businessadministration. Initially she lived in a boarding house,moving later to live in a house with eight other young Chi-nese. Those who knew her described her as a private per-son who did not have many friends. She spent her timealone reading or playing solitary games.
After she learned of the unnatural deaths of twoyoung Chinese nationals in Dublin, the young Chinesewoman became extremely alarmed. She left the languageschool and moved back with her old landlady from theboarding house. She developed a belief that a "presence"was livingin her abdomen. She also reported that multiplevoices were coming from the "presence." The voicesspoke Chinese and English, and they included the voicesof her family, her landlady, and teachers in her languageschool. She also reported that the picture on a banknotethat she had recently received from her family in China

spoke to her, stating, "You are no longer welcome here."In addition, she developed the belief that the family withwhom she had grown up was not her real family. Sheimmediately cut off contact with them and expressed awish to contact her "real" mother. She also stated that theCIAwas looking for her but could provide no explanationof why this should be the case. (Adapted from Feeneyet aI., 2002.)
Why should immigration be associated with an ele-vated risk of developing schizophrenia? One possibility isthat immigrants are more likely to receive this diagnosisbecause of cultural misunderstandings (Sashidharan,1993). However, there is no convincing evidence that this isthe case (Harrison et al., 1999; Takei et al., 1998). Anotherhypothesis is that people who are genetically predisposedto develop schizophrenia are more likely to move to live inanother country. However, some of the impairments asso-ciated with the early stages of schizophrenia seem incom-patible with this because negative symptoms and frontallobe dysfunctions may make it harder to be organizedenough to emigrate (see Cantor-Grace & Selten, 2005).
Perhaps the strongest clue comes from the findingthat immigrants with darker skin have a much higher riskof developing schizophrenia than do immigrants withlighter skin (Cantor-Grace & Selten, 2005). This raises thepossibility that experiences of being discriminated againstcould lead some immigrants to develop a paranoid andsuspicious outlook on the world, which could set the stagefor the development of schizophrenia. In support of thisidea, the results of a prospective study showed that healthypeople who felt discriminated against were more likelyto develop psychotic symptoms over time than healthypeople who did not perceive any discrimination (Janssenet al., 2003). Another possibility suggested by animal stud-ies is that the stress that results from social disadvantageand social defeat may have an effect on dopamine releaseor dopamine activity in key neural circuits (Tidey &Miczek, 1996). Moreover, some of these biological changescould make people more sensitive to the effects of usingillicit substances (Miczek et al., 2004). This is especiallyinteresting in light of new evidence linking cannabis abuseto the development of schizophrenia (see Developmentsin Research 14.4). Although there are no definitive answersyet, environmental triggers of schizophrenia are nowreceiving a renewed focus of attention.
4. Cannabis Abuse andSchizophrenia
er he finding that people with schizophrenia aretwice as likely as people in the general popula-tion to smoke cannabis (van Os et al., 2002)
has prompted researchers to ask whether thereis a causal link between cannabis abuse and
the development of psychosis. A methodologically rigorousstudy of conscripts to the Swedish army suggests that thismay indeed be the case. Compared to those who had neverused cannabis, young men who were heavy cannabis usersby the time they were 18 were more than 6 times morelikely to have developed schizophrenia 27 years later(Zammit et aI., 2002). This association also remained evenafter people who had used other kinds of drugs wereremoved from the statistical analysis.
Other studies have replicated this link (Arsenaultet al., 2002; Fergusson et aI., 2003; van Os, 2002) andhighlighted early cannabis use as being particularlyproblematic. For example, Arsenault et al. (2002)
reported that 10.3 percent of those who used cannabisby age 15 were diagnosed with signs of schizophrenia byage 26, compared with only 3 percent of the controlswho did not use cannabis. Taken together, the researchfindings suggest that using cannabis more than doubles
a person's risk of developing schizophrenia at a laterstage of life.
A major methodological concern in studies of thiskind is whether people who are in the early stages of devel-oping psychosis are more likely to use cannabis. Ifthiswere the case, cannabis use would simply be a correlate ofschizophrenia and not a cause. However, even after child-hood psychotic symptoms are considered and accountedfor statistically, cannabis use has still been found to be apredictor of later schizophrenia (Fergusson et al., 2003).
Of course, the majority of people who use cannabisdo not develop schizophrenia. An important factor here isobviously how vulnerable a person is to developing psy-chosis in the first place. Those who already have some pre-existing psychotic symptoms or who have a family memberwith schizophrenia may be particularly at risk if they usecannabis, especially if they begin early. It has been sug-gested that removing cannabis abuse in ls-year-oldswould reduce the later development of schizophrenia inthe population by 8 percent (see Arsenault et aI., 2004). Atthe very least, parents, teachers, and health practitionersneed to alert teenagers to the risks associated withcannabis use and discourage them from using it.

Immigration has been found to be a risk factor for developingschizophrenia. People who leave their native land to live inanother country have almost 3 times the risk of developingschizophrenia compared to people who remain living in theirhome country. The stresses and social challenges thataccompany immigration may be important factors.
In ReVIew~ What evidence supports a genetic
contribution to schizophrenia?~ What is the dopamine hypothesis? Describe
the current status of this explanation forschizophrenia.
~ What neuroanatomical abnormalitiesdifferentiate people with schizophrenia frompeople who do not suffer from this disorder?
~ What role does the family play in thedevelopment of schizophrenia?
TREATMENT ANDCLINICAL OUTCOMEBefore the 1950s the prognosis for schizophrenia wasrather bleak. Treatment options were very limited andmost patients were sent away to remote, forbidding, andovercrowded public hospitals. Some were put in straitjack-ets or treated with electroconvulsive "shock" therapy.Other were simply left to adjust to institutions that theywere never expected to leave (Deutsch, 1948).
Dramatic improvement carne in the mid-19~Os whena class of drugs known as "antipsychotics" were intro-duced. Pharmacotherapy (treatment by drugs) with thesemedications rapidly transformed the environment ofmental hospitals by calming patients and virtually elimi-nating wild, dangerous, and out-of-control patient behav-iors. A new and more hopeful era had arrived.
CLINICAL OUTCOME The most recent studies of clini-cal outcome show that 15 to 25 years after developingschizophrenia, around 38 percent of patients have a gen-erally favorable outcome and can be thought of as beingrecovered (Harrison et aI., 2001). This does not mean thatpatients return to how they were before they became ill,however. Rather, it means that, with the help of therapyand medications, the patients function quite well. Unfor-tunately, only around 16 percent of patients recover tothe extent that they no longer need any treatment. More-over, for a minority of patients (around 12 percent), long-term institutionalization is necessary. Finally, around athird of patients show continued signs of illness, usuallywith prominent negative symptoms. In other words,although things now are a great deal better than they were50 or 60 years ago, a "cure" for schizophrenia has notmaterialized.
Sometimes, patients who have been very severelyimpaired by schizophrenia show considerable improve-ment late in the course of their illness. As illustrated in thecase below, these spontaneous improvements can occureven when there is no change in the medications thatpatients are taking.
From Impairment toImprovement
The patient is a 46-year-old man who first became illwhen he was 17 years old. At the time his illness began,he was hearing voices and he had grandiose delusions.He also had delusions of being persecuted.
By the time he was 30, he was living in the hospital.He experienced continuous symptoms including delu-sions, hallucinations, and incoherent speech. His self-care was also very poor. His symptoms showed onlyminimal improvement after he was treated with clozapine.
Spontaneous clinical improvement was noted whenthe patient was in his forties. He became less isolated andhe began to spend more time doing activities. Although hehad previously been in<;pherent when he spoke, he beganto speak rationally, although there was still some povertyin the content of his speech. His self-care also improved.However, hospital staff still needed to prompt him tobathe and change his clothes. (Adapted from Murrayet aI., 2004.)

Can we predict which patients will do better overtime? Milev and colleagues (2005) gave a comprehensivebattery of clinical assessments and cognitive tests to a sam-ple of 99 patients who were experiencing their first episodeof schizophrenia. They then followed up the sample for7 years. Although the outcome of any individual case isobviously difficult to forecast, the best predictor of overallpsychosocial functioning over time was the severity of thepatients' negative symptoms.
Finally, patients who live in less industrialized coun-tries do better than patients who live in more industrial-ized nations (Jablensky et aI., 1992). This may be becauselevels of expressed emotion are much lower in countriessuch as India than in the United States and Europe. Forexample, in highly industrialized cultures, more than 50percent of families are high in expressed emotion. In con-trast, studies with Mexican-American and Hindi-speakingIndian samples show that only 24 percent and 41 percentof families, respectively, are high in EE (see Kamo et aI.,1987; Leff et aI., 1987). These differences may help explainwhy the clinical outcome of patients is different in differ-ent parts of the world.
Pharmacological ApproachesFIRST-GENERATION ANTI PSYCHOTICS First-gener-ation antipsychotics are medications like chlorpro-mazine (Thorazine) and haloperidol (Haldol) that wereamong the first to be used to treat psychotic disorders.Sometimes referred to as neuroleptics (literally, "seizingthe neuron"), these medications revolutionized the treat-ment of schizophrenia more than 50 years ago and can beregarded as one of the major medical advances of thetwentieth century (Bradford et aI., 2002). They are called"first-generation antipsychotics" (or "typical antipsy-chotics") to distinguish them from a new class of anti-psychotics that have been developed much more recently.These are referred to as "second-generation" (or "atypi-cal") "anti psychotics."
There is overwhelming evidence that antipsychoticmedications help patients. Large numbers of clinical trialshave demonstrated the efficacy and effectiveness of thesedrugs (Bradford et aI., 2002). Also, the earlier patientsreceive these medications, the better they tend to do overthe longer term (Marshall et aI., 2005; Perkins et aI., 2004).As we discussed earlier, first-generation antipsychotics arethought to work because they are dopamine antagonists.This means that they block the action of dopamine, pri-marily by blocking the D2 dopamine receptors. Althoughit is generally taught that antipsychotic medications take 1to 3 weeks to work, with most clinical gains being apparent6 to 8 weeks after the start of treatment (Bezchlibnyk-Butler & Jeffries, 2003), new data suggest that clinicalchanges can be seen within the first 24 hours of treatment(Kapur et aI., 2005). This supports the idea that these med-ications work by interfering with dopamine transmission at
the D2 receptors because dopamine blockade begins withinhours after the patient is given antipsychotic medication.
First-generation antipsychotics work best for the pos-itive symptoms of schizophrenia. In quieting the voicesand diminishing delusional beliefs, these medications pro-vide patients with significant clinical improvement (Jibson& Tandon, 1998). This comes at a cost, however. Commonside effects of these medications include drowsiness, drymouth, and weight gain. Many patients on these antipsy-chotics also experience what are known as extrapyramidalside effects (EPS). These are involuntary movement abnor-malities (muscle spasms, rigidity, shaking) that resembleParkinson's disease.
African-Americans and other ethnic minoritiesappear to be at increased risk of extrapyramidal side effects(Lindamer et aI., 1999). Such side effects are usually con-trolled by taking other medications. Some patients whohave been treated with neuroleptics for long periods oftime may also develop tardive dyskinesia. This involvesmarked involuntary movements of the lips and tongue(and sometimes the hands and neck). Rates of tardivedyskinesia are about 56 percent when patients have takenneuroleptics for 10 years or more, with females being espe-cially susceptible (Bezchlibnyk-Butler & Jeffries, 2003).Finally, in very rare cases there is a toxic reaction to themedication that is called neuroleptic malignant syndrome(Viejo et aI., 2003). This condition is characterized by highfever and extreme muscle rigidity and if left untreated, itcan be fatal.
SECOND-GENERATION ANTI PSYCHOTICS In the 1980sa new class of antipsychotic medications began to appear.The first of these to be used clinically was clozapine(Clozaril). This drug was introduced in the United Statesin 1989, although clinicians in Europe had been using itprior to this. Although initially reserved for use withtreatment-refractory patients (those who were not helpedby other medications), clozapine is now used much morewidely.
Other examples of second-generation antipsychoticmedications are risperidone (Risperdal), olanzapine(Zyprexa), quetiapine (Seroquel), and ziprasidone(Geodon). The most recent addition is aripiprazole (Abil-ify). The reason why these medications are called "second-generation antipsychotics" is that they cause far fewerextrapyramidal symptoms than the earlier antipsychoticmedications such as Thorazine and Haldol (Jibson &Tandon, 1998; Stahl, 2002). They are also remarkablyeffective in alleviating both the positive and the negativesymptoms of schizophrenia. Current thinking is thatsecond-generation antipsychotics work by blocking a muchbroader range of receptors than first-generation antipsy-chotics. These include the D4 dopamine receptor (which isfrom the same "family" as the D2 receptor) and possiblyreceptors for other neurotransmitters as well (Bezchlibnyk-Butler & Jeffries, 2003).

The introduction of second-generation neuroleptit;shas been tremendously beneficial to many patients withschizophrenia. As we have just seen, they reduce symptomsand have few motor side effects. Patients taking thesenewer antipsychotics are also less likely to be rehospitalizedthan patients taking conventional first-generation antipsy-chotics (Rabinowitz et al., 2001). However, these medica-tions are not without other side effects. Drowsiness andweight gain are very common. Diabetes is also a concern(Sernyak et al., 2002). In rare cases, clozapine also causes alife-threatening drop in white blood cells known asagranulocytosis. For this reason, patients taking this med-ication must have regular blood tests.
THE PATIENT'S PERSPECTIVE Not all patients willbenefit from these medications. And many who do showclinical improvement will still have problems functioningwithout a great deal of additional help. We must also notlose sight of what it is like for patients with schizophreniato have to take medications every day, often for years or fora lifetime. Side effects that can sound trivial to someone onthe outside can be so bad for patients that they refuse totake their medications, even when those medications givethem relief from their hallucinations and delusions. Thefollowing comes from the mother of a daughter who suf-fers from schizophrenia:
As a parent I also know that medication is not perfectand that the side effects can be distressing. When mydaughter goes back on her medication, I feel bad see-ing her shuffling or experiencing involuntary arm andmouth movements. These symptoms usually subsideover time; but she also gains weight, and she hatesbeing heavy. I think she hates taking medication mostof all because she is, in a sense, admitting she is men-tally ill, something she very much wants to deny.(From Slater, 1986.)
Psychosocial ApproachesMental health professionals have been slow to realize thelimitations of an exclusively pharmacological approachto the treatment of schizophrenia. In fact, so dominantwas this approach that some extremely promising alter-native approaches that originated in the decades priorto the 1990s were simply ignored by the majority ofmental health professionals (e.g., Fairweather, 1980;Fairweather et al., 1969; Karon & Vandenbos, 1981; Paul& Lenz, 1977).
But we are now beginning to learn from our mistakes.Perhaps the most notable indication of a changing per-spective on the treatment of schizophrenia comes from theAmerican Psychiatric Association's (2004) Practice Guide-line for the Treatment of Patients with Schizophrenia. Thisdocument makes recommendations for using medicationsto manage patients in various phases and at differing
severities of disorder. However, it highlights the impor-tance of psychosocial interventions as well. Some of theseapproaches, which are normally used in conjunction withmedication, are briefly described below.
FAMILY THERAPY The literature that links relapse inpatients with schizophrenia to high family levels ofexpressed emotion (EE) inspired several investigators todevelop family intervention programs. The idea was toreduce relapse in schizophrenia by changing those aspectsof the patient-relative relationship that were regarded ascentral to the EE construct. At a practical level, this gener-ally involves working with patients and their families toeducate them about schizophrenia, to help them improvetheir coping and problem-solving skills, and to enhancecommunication skills, especially the clarity of family com-munication.
In general, the results of research studies in this areahave shown that patients do better clinically and relapserates are lower when families receive family treatment (seePitschel-Walz et al., 2001). Studies done in China indicatethat these treatment approaches can also be used in othercultures (Xiong et al., 1994). Despite this, family treatmentis still not a routine element in the accepted standard ofcare for patients with schizophrenia (Lehman et al., 1998).Given its clear benefits to patients and its considerablecost-effectiveness [Tarrier et al. (1991) calculated that fam-ily treatment results in an average cost savings of 27 per-cent per patient], this seems very unfortunate.
CASE MANAGEMENT Case managers are people whohelp patients find the services they need in order to func-tion in the community. Essentially, the case manager actsas a broker, referring the patient to the people who willprovide the needed service (e.g., help with housing, treat-ment, employment, and the like). Assertive communitytreatment programs are a specialized form of case manage-ment. Typically, they involve multidisciplinary teams withlimited caseloads to ensure that discharged patients don'tget overlooked and "lost in the system." The multidiscipli-nary team delivers all the services the patient needs (seeStein & Test, 1980; Mueser, 1998).
Assertive community treatment programs reduce thetime that patients spend in the hospital. They also enhancethe stability of patients' housing arrangements. Theseapproaches seem to be especially beneficial for patientswho are already high utilizers of psychiatric and commu-nity services (see Bustillo et al., 2001).
SOCIAL-SKILLS TRAINING Patients with schizophre-nia often have very poor interpersonal skills (for a review,see Hooley & Candela, 1999). Their social functioning isalso hampered by deficits in their abilities to recognizebasic facial emotions such as happiness and anger and bydeficits in making social judgments from faces compared

to control subjects (Hall et al., 2004). Social-skills trainingis designed to help patients acquire the skills they need tofunction better on a day-to-day basis. These skills includeemployment skills, relationship skills, self-care skills, andskills in managing medication or symptoms. Social rou-tines are broken down into smaller, more manageablecomponents. For conversational skills, these elementsmight include learning to make eye contact, speaking at anormal and moderate volume, taking one's turn in a con-versation, and so on. Patients learn these skills, get correc-tive feedback, practice their new skills using role-playing,and then use what they have learned in natural settings(Bellack & Mueser, 1993).As Green (2001, p.139) has cor-rectly noted, engaging in social-skills training is a bit liketaking dance lessons. It does not resemble traditional "talktherapy" in any obvious manner.
The results of social-skills treatments are mixed (seePilling et al., 2002). In some cases, treatment approachessuch as this have been found to improve the specific skillsthat patients have and help them function better (seeKopelowicz et al., 2002). Other research studies have failedto find any significant improvements in patients' socialfunctioning, even when very intensive social-skills traininghas been provided (Hogarty et al., 1991). One problem isthat competent social functioning requires a broad rangeof skills. Social-skills training tends to target specific areas(e.g., conversational skills, managing finances, cooking ameal) that are domain-specific and do not always leadpatients to be more generally competent in the world atlarge. Another problem is that many of the new skills thatpatients learn do not seem to generalize to everyday set-tings. Because of this, researchers are now trying to teachpatients skills that transfer better to real-life situations.
Instead of teaching specific skills, the new emphasis ison helping patients deal with their neurocognitive deficitsthrough cognitive remediation training. New researchefforts are now trying to help patients improve some oftheir neurocognitive deficits (e.g., verbal memory, vigi-lance, and performance on card-sorting tasks) in the hopethat these improvements will translate into better overallfunctioning (e.g., conversational skills, self-care, job skills,and so on). Unfortunately, although some of the earlyresults looked promising (Spaulding, 1999; Wykes et al.,1999), a recent meta-analysis suggests that cognitiveremediation efforts may not be particularly beneficial topatients (Pilling et al., 2002).
COGNITIVE-BEHAVIORAL THERAPY As you havealready learned, cognitive-behavioral therapy (CBT)approaches are widely used in the treatment of mood andanxiety disorders as well as many other conditions (Beck,2005). Until fairly recently, however, researchers did notconsider using them for patients with schizophrenia, nodoubt because patients with schizophrenia were consid-ered too impaired. Pioneered by researchers and clinicians
in the United Kingdom, cognitive-behavioral approachesare now gaining momentum in the treatment of schizo-phrenia. The goal of these treatments is to decrease theintensity of positive symptoms, reduce relapse, anddecrease social disability. Working together, therapist andpatient explore the subjective nature of the patient's delu-sions and hallucinations, examine evidence for and againsttheir veracity or veridicality, and subject delusional beliefsto reality testing.
In general, the results are promising. Tarrier and hiscolleagues (1998, 1999) found that patients who receivedCBT showed decreases in their hallucinations and delu-sions, compared to patients who received either support-ive counseling or routine care. These treatment gains weremaintained a year later. Another study by Sensky and col-leagues also showed that patients who received CBT hada decrease in their levels of psychosis, compared to aroutine-care control group, both after 9 months of treat-ment and also after a 9-month follow-up (2000). But bothof these studies also revealed something quite surprising.In the study by Sensky and colleagues, patients who weretreated with a "befriending" intervention also did unex-pectedly well. And in the other study, by the time of the2-year follow-up, the patients who were doing the bestwere those who had received supporting counseling(Tarrier et al., 2000). Both of these "treatments" had ini-tially been designed to be placebo conditions. The factthat patients who received them did so well raises someimportant questions. Far from being placebo treatments,individual meetings with patients that develop rapport,contain unconditional positive regard, provide socialinteraction, and give patients an opportunity to discusstheir problems may actually produce real clinical benefitsof their own.
INDIVIDUAL TREATMENT Before 1960 the optimaltreatment for patients with schizophrenia was psychoan-alytically oriented therapy based on a Freudian type ofapproach. This is what Nobel Prize-winning mathemati-cian John Nash received when he was a patient at McLeanHospital in Massachusetts in 1958 (Nash's story is toldin The World Around Us 14.5 on p. 526). By 1980, how-ever, things had changed. Research began to suggest thatin some cases, psychodynamic treatments made patientsworse (see Mueser & Berenbaum, 1990). This form ofindividual treatment thus fell out of favor.
Individual treatment for schizophrenia now takes adifferent form. Hogarty and colleagues (1997 a, 1997b)report on a controlled 3-year trial of what they call "per-sonal therapy." Personal therapy is a nonpsychodynamicapproach that equips patients with a broad range of copingtechniques and skills. The therapy is staged, which meansthat it comprises different components that are adminis-tered at different points in the patient's recovery. For exam-ple, in the early stages, patients examine the relationship

14.5The film A Beautiful Mind
(based on the book ofthe same name by SylviaNasar, 1998) vividlydepicts the descent of
Princeton mathematician john Nashinto schizophrenia, his subsequentrecovery, and his winning of theNobel Prize in economics. By anymeasure the film is engaging, dis-turbing, and wonderfully uplifting.But how accurate is it? What is thereal story of john Nash?
john Forbes Nash was born inWest Virginia. Even in grade schoolhe stood out, and then he won ascholarship in high school and laterattended the Carnegie Institute ofTechnology in 1945. He then went onto complete a Ph.D. in mathematicsat Princeton, the most elite mathe-matics department in the world. AtPrinceton Nash rarely went toclasses, and he alienated some people with his odd behav-ior, his arrogance, and his eccentricities. Although wemight now regard these as early warning signs of schizo-phrenia, he did not develop schizophrenia at this time.Rather, he impressed his peers and colleagues by inventinga new board game and developing his ideas about theequilibrium point (the Nash equilibrium), for which hewould later win the Nobel Prize.
After graduating from Princeton, Nash took a job atM.LT., where he was regarded as shamelessly elitist, brash,boastful, and egocentric. His brilliant mind, however, meantthat people tolerated his abrasive interpersonal style.Although there is no mention of this in the movie, he dateda nurse, Eleanor Stier, and fathered a son named johnDavid. The affair was kept secret, and after the baby wasborn, Nash abandoned Eleanor and John David, with theresult that his young son had to be placed in foster care.
Shortly after his son's birth in 1953, Nash met AliciaLarde, a talented physics major who was a student in oneof his classes. They married in 1957 and all seemed to bewell. However, a year later, when Alicia was pregnant, Nashwent rapidly downhill. He told colleagues that he was get-ting coded messages from the New York Times, that he haddelusions about men in red ties at M.LT., and that heturned down a job at the University of Chicago because hewas scheduled to become Emperor of Antarctica. Hepainted black spots on his bedroom wall, and in February
Princeton mathematician John Nashwon the 1994 Nobel Prize for hismathematical contributions to gametheory. Nash's struggle withschizophrenia is depicted in themovie A Beautiful Mind.
1958, he was hospitalized at McLeanHospital in Belmont, Massachusetts,just a few miles from M.LT. AtMcLean he was diagnosed with para-noid schizophrenia, given Thorazine,and called "Professor" by the staff.Contrary to the account in the movie,Nash did not experience visual hallu-cinations. And even when people doexperience visual hallucinations, thehallucinations rarely seem like realpeople. More typically, they are fleet-ing visual "fragments." No doubt thehallucinated roommate and his niecein the movie were a creative deviceto sidestep the fact that delusions(i.e., beliefs) do not play well in avisual medium.
After 50 days in McLean, Nashwas released with assistance fromhis lawyer. He resigned from M.LT.,withdrew all the money from his pen-sion fund, and left for Europe. Fear-
ing for his welfare, Alicia went with him, leaving their baby,Johnny, with Alicia's mother. Nash disappeared while theywere in Paris and then spent the next 9 months wanderingEurope trying to renounce his U.S. citizenship. He waseventually deported.
When Nash returned to the United States, he and Ali-cia moved back to Princeton, and Alicia worked to supportthe family. Nash was offered a job at Princeton but was sodelusional that he refused to sign the necessary tax formsand so could not be hired. Within 2 years of leaving McLeanhe was hospitalized again, this time at Trenton State Hospi-tal in New jersey. Trenton State was a very different envi-ronment from the country club setting of McLean. It wascrowded and full of poorly treated patients. As is accuratelydepicted in the movie, Nash was treated with insulin comatherapy. This treatment (which had already been phasedout in most other hospitals) involved an injection of insulinthat led to a rapid decrease in blood sugar, coma, and con-vulsions. Nash received this therapy 5 days a week for 6weeks. He was discharged 6 months later with someimprovement in his symptoms.
The following year, when he was 34, Nash disap-peared to Europe again. He regularly sent friends andfamily members postcards that were both bizarre andfrightening. Later that same year, Alicia filed for divorce.
For the next several years Nash wandered around,sometimes living in Boston, spending time with his older

son and Eleanor Stier, and then abruptly leaving. He beganto take antipsychotics and showed some improvement.Then, like many patients, he would abruptly stop takingthe medications and his symptoms would come backagain. Around this time, Nash also began to hear voices.
By 1970 Nash was essentially indigent. Alicia tookpity on him and took him in. She promised not to rehospi-talize him and provided him with a supportive home envi-ronment. Nash became a regular visitor to Princeton,roaming the campus for a decade and leaving mathemati-cal scribblings on blackboards and windows. He was try-ing to prove the existence of God through mathematics.
The Princeton community was extremely tolerant of him,and slowly, perhaps because he was able to remain in alow-stress environment, Nash began to get better. He latersaid he willed himself to get better, rejecting what thevoices said and deciding not to listen to them. At age 66,remarried to Alicia, he walked in front of the King of Swe-den and received the Nobel Prize, to the delight of his jubi-lant colleagues. His recovery was long in coming, as wasthe formal recognition of his genius. Sadly, however, theNash family is not finished dealing with schizophrenia.Nash's son with Alicia, also a mathematician, suffers fromthe same illness as his father.
between their symptoms and their stress levels. They alsolearn relaxation and some cognitive techniques. Later, thefocus is on social and vocational skills. Overall, this treat-ment appears to be very effective in enhancing the socialadjustment and social role performance of dischargedpatients.
In light of the unexpected findings from some of theCBT studies described above, it is likely that researcherswill have a renewed interest in the elements of individualtreatment for patients with schizophrenia. Although rig-orous psychoanalytic approaches may be too demandingand stressful for patients, supportive forms of therapythat offer an opportunity to learn skills and yet are lowkey and responsive to patients' individual concerns mightwell be very beneficial for patients. Individual reportsfrom patients and therapists attest to the value of suchapproaches (Kendler, 1999b; A Recovering Patient, 1986).Just as progress in research on schizophrenia requires apartnership between molecular biology and the socialsciences, progress in the treatment of schizophreniarequires balancing pharmacology with consideration ofthe specific needs of the patient. For patients who are athigh risk of relapse and who live with families, family-based interventions will be required. If patients have con-tinuing and disturbing hallucinations and delusions,CBT may be appropriate. When patients are clinically sta-
ble, social-skills training and rehabilitation efforts may behelpful. But in all of this, we must not lose sight of theneed of patients (and their families) for support, valida-tion, and respectful care. The treatment of patients withschizophrenia is certainly not easy, and there is no "quickfix." Even with all of the treatment advances that haveoccurred, there is still a need for more high-quality,informed, and clinically sensitive care.
In ReVIew~ What kinds of clinical outcomes are
associated with schizophrenia? Is fullrecovery possible or typical?
~ In what ways are conventional and atypicalneuroleptic medications similar and in whatways are they different? How effective arethese treatments for patients withschizophrenia?
~ Describe the major psychological approachesused in treating schizophrenia.

Schizophrenia is a devastating and costly illness.Successful efforts to prevent it would yield enor-mous humanitarian and financial benefits. But isthis really feasible?
The aim of primary prevention is to preventnew cases of a disorder or condition from ever developing.Primary intervention in schizophrenia would involve improv-ing obstetric care for women with schizophrenia and first-degree relatives of schizophrenia patients (see Warner, 2001).
Good prenatal care is known to result in fewer birth complica-tions and fewer low-weight babies. Although such a programwould not result in a major decline in the incidence of schizo-phrenia, it has no potential for harm. And if it prevented just ahandful of new cases of schizophrenia, the savings in humansuffering and money would be far from trivial.
Another possibility is to try to intervene early with peo-ple who are most at risk of developing schizophrenia. This isknown as secondary prevention. McGorry and his colleaguesin Australia have pioneered this approach, and it is widelyregarded as an important public health priority (see McGorry& Jackson, 1999). One major problem, though, is how to iden-tify people who are at risk. The screening tests that are cur-rently being used, although acceptable in clinical settings(see Klosterkotter et aI., 2001; Warner, 2001; Yung & McGorry,1997), are too flawed to be of use in community settings. This
~ Schizophrenia is the most severe form of mentalillness. It is characterized by impairments in manydomains and affects just under 1percent of the
population.
~ Characteristic symptoms of schizophrenia includehallucinations, delusions, disorganized speech,disorganized and catatonic behavior, and negativesymptoms.
~ Most cases of schizophrenia begin in lateadolescence or early adulthood. The disorder beginsearlier in men than in women. Overall, the clinicalsymptoms of schizophrenia tend to be more severe inmen than in women. Women also have a better long-
term outcome.
~ Genetic factors are clearly implicated in schizophrenia.Having a relative with the disorder significantly raises aperson's risk of developing schizophrenia.
is because they generate far too many "false positives."These are people who the test says are at risk of developingthe disorder but who will not, in fact, develop schizophrenia.
Even if we could identify all of those who are truly at risk,what interventions would be appropriate? McGorry and Jack-son (1999) suggest that low-dose antipsychotic medicationscould be used. But is it really appropriate and ethical to pre-scribe antipsychotic medications to someone who has nopsychotic symptoms? And how harmful might it be to tellsomeone that he or she might develop schizophrenia? Apromising (and less controversial development) is the use ofcognitive therapy to prevent psychosis in people at very highrisk (Morrison et aI., 2004).
Perhaps the most viable form of intervention is tertiaryprevention-early treatment for those who already have thefull illness. Many researchers are now expanding their effortsin this direction. Although we do not yet have direct and com-pelling evidence that intense and early intervention is benefi-cial over the long term, there may be few serious risksassociated with providing short-term inpatient care, medica-tion, vocational rehabilitation, family support, and cognitivetherapy for these patients (McGorry et aI., 1996). Somepatients may certainly be "overtreated." However, comparedto undertreatment, this may be the more desirable choice.
~ Other factors that have been implicated in thedevelopment of schizophrenia include prenatalexposure to the influenza virus, early nutritionaldeficiencies, and perinatal birth complications.
~ Current thinking about schizophrenia emphasizes theinterplay between genetic and environmental factors.
~ Even though schizophrenia begins in early adulthood,researchers believe that it is a neurodevelopmentaldisorder. A "silent lesion" in the brain is thought to liedormant until normal developmental changes occurand expose the problems that result from this brainabnormality.
~ Many brain areas are abnormal in schizophrenia,although abnormalities are not found in all patients.The brain abnormalities that have been found includedecreased brain volume, enlarged ventricles, frontallobe dysfunction, reduced volume of the thalamus,

and abnormalities in temporal lobe areas such as thehippocampus and amygdala.
~ The most important neurotransmitters implicated inschizophrenia are dopamine and glutamate.
~ Patients with schizophrenia have problems in manyaspects of neurocognitive functioning. They show avariety of attentional deficits (e.g., poor P50suppression and deficits on the ContinuousPerformance Test). They also show eye-trackingdysfunctions.
~ Patients with schizophrenia are more likely to relapseif their relatives are high in expressed emotion (EE).High-EE environments may be stressful to patientsand may trigger biological changes that causedysregulations in the dopamine system. This couldlead to a return of symptoms.
~ For many patients, schizophrenia is a chronicdisorder requiring long-term treatment orinstitutionalization. However, with therapy and
medications, around 38 percent of patients can showa reasonable recovery. Only about 16 percent ofpatients recover to the extent that they no longerneed treatment.
~ Patients with schizophrenia are usually treated withfirst- or second-generation antipsychotic (neuroleptic)medications. Second-generation anti psychotics causefewer extrapyramidal (motor abnormality) sideeffects. Antipsychotic drugs work by blockingdopamine receptors. Overall, patients taking second-generation anti psychotics do better than patientstaking first-generation antipsychotic drugs.
~ Psychological treatments for patients withschizophrenia include cognitive-behavioral therapy,social-skills training, and other forms of individualtreatment, as well as case management. Familytherapy provides families with communication skillsand other skills that are helpful in managing theillness. Family therapy also reduces high levels ofexpressed emotion.
anti psychotics (neuroleptics)(P. 523)
brief psychotic disorder (P. 500)
candidate genes (P. 507)
catatonic schizophrenia (P. 497)
cognitive remediation (P. 525)
delusion (P. 493)
delusional disorder (P. 499)
disorganized schizophrenia (P. 497)
dopamine (P. 515)
endophenotypes (P. 510)
expressed emotion (EE) (P. 519)
glutamate (P. 516)
hallucination (P. 493)
linkage analysis (P. 507)
negative symptoms (P. 495)
paranoid schizophrenia (P. 496)
positive symptoms (P. 495)
residual schizophrenia (P. 498)
schizoaffective disorder (P. 499)
schizophreniform disorder (P. 499)
shared psychotic disorder(folie a deux) (P. 500)
undifferentiated schizophrenia(p.498)


Cognitive DisordersBRAIN IMPAIRMENT IN ADULTS
Diagnostic IssuesClinical Signs of Brain DamageDiffuse versus Focal DamageThe Neuropsychology/Psychopathology
Interaction
Dementia from HIV-l InfectionVascular Dementia
DELIRIUM
Clinical PresentationTreatment and Outcome
DISORDERS INVOLVING HEAD INJURY
The Clinical PictureTreatments and Outcomes
DEMENTIA
Alzheimer's Disease
UNRESOLVED ISSUES:Can Dietary Supplements Enhance Brain
Functioning?

he brain is an astonishing organ. Weighing around 3 pounds, it is the most complex structure inthe known universe (Thompson, 2000). It is also the only organ capable of studying and readingabout itself. It is involved in every aspect of our lives from eating and sleeping to falling in love.The brain makes decisions, and it contains all the memories that make us who we are. Whetherwe are physically ill or mentally disturbed, the brain is involved.
Because it is so important, the brain is protected in an enclosed space and covered by a thickouter membrane called the "dura mater" (literally, "hard mother" in Latin). For further protection,the brain is encased by the skull. The skull is so strong that, if it were placed on the ground andweight were applied very slowly, it could support as much as 3 tons (Rolak, 2001, p. 403)! Theseanatomical facts alone indicate just how precious the brain is.
But the brain cannot be protected entirely. Sometimes there is internal damage that occurs early.When structural defects in the brain are present before birth or occur at an early age, mental retar-dation may result (see Chapter 16). In other cases, what was a normally developed brain can sufferfrom internal changes that can lead to destruction of brain tissue. Depending on the nature and siteof the damage, this can result in a movement disorder such as Parkinson's disease or in cognitiveconfusion, referred to as dementia. This dementia could be caused by Alzheimer's disease or by astroke (so named in 1599 because this cerebrovascular event occurs so suddenly that it was likenedto "a stroke of God's hand").
The brain can also be damaged by external influences. A wide variety of injuries and toxicsubstances may result in the death of neurons or their connections. The brain can be damagedby trauma from traffic accidents or from the repeated blows to the head that can occur in boxingor football. In short, even though it is highly protected, the brain is vulnerable to damage frommany sources.
When the brain is damaged or brain functioning is in some way compromised, cognitivechanges result. Although there may be other signs and symptoms (such as mood or personalitychanges), changes in cognitive functioning are the most obvious signs of a damaged brain. In thischapter we will discuss three major types of cognitive disorders that are recognized in DSM-IV-TR:delirium, dementia, and amnestic syndrome.
Why are cognitive disorders discussed at all in a textbook on abnormal psychology? There areseveral reasons. First, as their inclusion in the DSM indicates, these disorders are regarded as psy-chopathological conditions. Second, as you will see from the case study that follows, some braindisorders cause symptoms that look remarkably like other abnormal psychology disorders. Forexample, the American composer George Gershwin died at age 39 because doctors failed to rec-ognize that what they were diagnosing as "hysteria" was really the result of a brain tumor (Jablon-ski, 1987). Third, brain damage can cause changes in behavior, mood, and personality. You willrecognize this more clearly later when we describe the case of Phineas Gage (who survived ametal bar being blown through his head). Understanding what brain areas are involved when
behavior, mood, and personality change after brain damage may helpresearchers better understand the biological underpinnings of manyproblems in abnormal psychology. Fourth, many people who suffer frombrain disorders (for example, people who are diagnosed as havingAlzheimer's disease) react to the news of their diagnosis with depres-sion or anxiety. Prospective studies also suggest that depressive symp-toms may herald the onset of disorders such as Alzheimer's disease(AD) by several years (Devanand et aI., 1996; Wilson et aI., 2002) andthat episodes of depression double the risk for AD even 20 years later(Speck et aI., 1995). Finally, cognitive disorders of the type we describein this chapter take a heavy toll on family members who, for manypatients, must shoulder the burden of care. Again, depression and anx-iety in relatives of the patients themselves are not uncommon.
Case studies are descriptions ofone specific case. Case studies canbe a useful source of informationand can help researchers generatehypotheses. Because of theirhighly selective nature, however,they cannot be used to draw anyscientific conclusions.

A highly successful businessman, age 45, with no previ-ous history of psychiatric disorder began to act differ-ently from his usual self. He seemed driven at work. Hisworking hours gradually increased, until finally he wassleeping only 2 to 3 hours a night; the rest of the time heworked. He became irritable and began to engage inuncharacteristic sprees of spending beyond his means.
Although he felt extremely productive and claimedhe was doing the work of five men, the man's boss feltotherwise. He was worried about the quality of that work,having observed several recent examples of poor busi-ness decisions. Finally, when the man complained ofheadaches, his boss insisted that he seek help. (Adaptedfrom Jamieson & Wells, 1979.)
Clinicians always need to be alert to the possibilitythat brain impairment itself may be directly responsiblefor the clinical phenomena observed. Failure to do socould result in serious diagnostic errors, as when a clini-cian falsely attributes a mood change to psychologicalcauses and fails to consider a neuropsychological originsuch as a brain tumor (Purisch & Sbordone, 1997; Wein-berger, 1984). The case you have just read concerns a manwho, on first glance, looks as if he might be having anepisode of mania. In fact, however, he is suffering fromfour tumorous masses in his brain. Clues that the patienthas a brain disorder rather than a mood disorder comefrom the fact that he is experiencing headaches at the sametime as a major change in behavior. The fact that he has noprior history of psychopathology is also another clue (seeTaylor, 2000).
BRAIN IMPAIRMENTIN ADULTSPrior to the revision of DSM -IV in 1994, most of the dis-orders to be considered in this section were called organicmental disorders. This term was designed to convey thatthere was some kind of identifiable pathology that wascausing the problem (e.g., a brain tumor, stroke, drugintoxication, or the like). Recognizing this, such disorderswere typically treated by neurologists. In contrast,functional mental disorders were brain disorders thatwere considered not to have an organic basis. Such disor-ders were treated by psychiatrists. By the time DSM -IV waspublished, however, it was apparent that it was wrong toassume that psychiatric disorders had no organic (or bio-logical) component. Consider, for example, how impor-
tant problems in brain neuroanatomy and neurochemistryare to our understanding of schizophrenia (see Chapter14). The terms functional and organic were thereforedropped. What was the organic mental disorders section ofthe DSM has been renamed. It is now called "Delirium,Dementia, and Amnestic and other Cognitive Disorders"(see APA, 2000).
Diagnostic IssuesThe DSM-IV- TR presents the diagnostic coding of variousneuropsychological disorders in different and somewhatinconsistent ways. Much depends on what is causing thecognitive problem. For cognitive disorders that have anunderlying medical problem as their cause, both the cogni-tive problem and the medical cause are listed on Axis I.Sometimes the qualifying phrase "Due to [a specified gen-eral medical condition]" is used. Then, in addition, themedical condition that is causing the cognitive problem islisted again on Axis III. Many of the common neuropsy-chological disorders are handled in this manner. For exam-ple, cognitive impairment associated with HIV diseasemight have the following DSM-IV-TR diagnostic code:
Axis I: Dementia due to HIV disease
Axis III: HIV disease
The diagnosis for dementia caused by Alzheimer's dis-ease is managed in a similar way, with Alzheimer's diseasebeing designated on Axis III.
Axis I: Dementia of the Alzheimer's type
Axis III: Alzheimer's disease
On the other hand, pathological brain changes that arerelated to the toxic effects of abusing certain substances,such as long-term, excessive alcohol consumption (seeChapter 12), are handled a little differently. In these cases,a specific etiologic notation is included in the Axis I diag-nosis, as in "Substance-Induced Persisting Amnestic Dis-order" (a circumscribed and characteristic type of memoryimpairment). No diagnosis is given on Axis III.
Axis I: Alcohol-induced persisting amnestic disorder
Axis III: None
Clinical Signs of Brain DamageWith possible minor exceptions, cell bodies and neuralpathways in the brain do not appear to have the power ofregeneration, which means that their destruction is per-manent. When brain injury occurs in an older child oradult, there is a loss in established functioning. Thisloss-this deprivation of already acquired and customaryskills-can be painfully obvious to the victim, adding anoften pronounced psychological burden to the physicalburden of having the lesion. In other cases the impairmentmay extend to the capacity for realistic self-appraisal (acondition called "anosognosia"), leaving these patients

5.5J111of us misplace our keys from time to
time, drive past our intended destinations,or forget something we had planned toremember. Are these signs of cognitiveimpairment? Or are we just too busy and
preoccupied to pay enough attention to what we are doing?Clinicians often use a short screening test called the
Mini-Mental State Examination to examine patients for cog-nitive impairment (see Folstein et aI., 1975). Although thistest is far from new, it is still the most widely used in routineclinical practice. The test has a maximum score of 30 points.A score of less than 25 suggests impairment, and a score of20 or less is indicative of definite impairment.
During the MMSEthe clinician will ask the patient ques-tions that concern orientation (score 1point if correct):
What is the year, season, month, date, day of the week?
Where are we now (country, state, city or town, building,floor of building)?
There will also be questions that assess registration.Here the clinician names three objects (e.g., cat, window,orange) and asks the patient to repeat them. The patientreceives a score of 1point for each object correctlyrepeated.
relatively unaware of their losses and hence poorly moti-vated for rehabilitation.
Damage or destruction of brain tissue may involve onlylimited behavioral deficits or a wide range of psychologicalimpairments, depending on: (1) the nature, location, andextent of neural damage, (2) the premorbid (predisorder)competence and personality of the individual, (3) the indi-vidual's life situation, and (4) the amount of time since thefirst appearance of the condition. Although the degree ofmental impairment is usually directly related to the extentof damage, this is not invariably so. In some cases involvingrelatively severe brain damage, mental change is astonish-ingly slight. In other cases of apparently mild and limiteddamage, there may be profoundly altered functioning.Developments in Practice 15.1 describes a short screeningtest that is widely used to assess patients for possible cogni-tive impairment. A patient with a low score on the testwould be referred for a more extensive evaluation.
Diffuse versus Focal DamageThe fundamental disorders discussed in this section arealways in the strictest sense neuropsychological ones,although psychopathological problems (psychosis, mood
Screening for CognitiveImpairment
Next, the clinician will assess attention andconcentration. The patient is asked to start at 100 andcount backward, subtracting 7 each time until he or shegets to 65. An alternative here is to ask the patient to spella common five-letter word such as world backward. Thispart of the test has a maximum score of 5 points.
Then the clinician will test for recall by asking, "Doyou recall the three objects named before?" One point isgiven for each object correctly recalled.
This is followed by language tests.The clinician will point to two objects such as a watch
and a pen and ask the patient to name them (2 points).The clinician will ask the patient to repeat a phrase
such as "No ifs, ands, or buts" (1 point).Comprehension will be assessed by asking the patient
to comply with a command: "Pick up the paper in your righthand, fold it in half, and set it on the floor" (3 points).
The patient will also be asked to read a command(such as "Close your eyes") off a piece of paper and per-form it (1 point).
The last part of this section requires the patient to writea simple sentence (e.g., subject, verb, object; 1point).
Finally construction ability is tested by asking thepatient to copy a very simple design (1 point).
change, etc.) may be associated with them. Some of thesedisorders are relatively well understood, with symptomsthat have relatively constant features in people whose braininjuries are comparable in location and extent. For exam-ple, attention is often impaired by mild to moderate diffuse(i.e., widespread) damage, such as might occur with mod-erate oxygen deprivation or the ingestion of toxic sub-stances such as mercury. Such a person may complain ofmemory problems due to an inability to sustain focusedretrieval efforts, while his or her ability to store new infor-mation remains intact. As Developments in Research 15.2shows, mild cognitive impairments can also be detected inpeople who have had only low-level exposure to organicsolvents and other neurotoxins.
In contrast to diffuse damage, focal brain lesionsinvolve circumscribed areas of abnormal change in brainstructure. This is the kind of damage that might occurwith a sharply defined traumatic injury or an interrup-tion of blood supply (a stroke) to a specific part of thebrain (see Figure 15.1). The location and extent of thedamage determine what problems the patient will have.As you are aware, the brain is highly specialized (seeFigure 15.2). For instance, the two hemispheres, whileinteracting intimately at many levels, are involved in

:J1 s you will learn inthis chapter, thebrain can be dam-aged by exposure tometals such as lead
and mercury. This places many indus-trial workers at risk. However, thenervous system can also be damagedby exposure to organic solvents thatare neurotoxic. Some of these arefound in a place that most of uswould not immediately think of.
Nail studios routinely use(meth)acrylates and a variety oforganic solvents such as toluene,acetone, and formaldehyde that areknown to be potentially damaging tothe central nervous system. In arecent study, LoSasso et al. (2001)
compared the neuropsychologicalfunctioning of 150 nail salon techni-cians with that of 148 demographi-cally similar controls. All of theparticipants completed a self-reportmeasure that assessed neuropsy-chological impairments in the areas of memory, verballearning, and general cognitive efficiency.
What the researchers found was both interestingand disturbing. The results showed that compared to the
Cognitive Impairments inNail Salon Technicians
controls, the nail salon techniciansreported significantly more cogni-tive and neurological impairments.Many of the impairments were mild.However, the severity of the symp-toms that the nail salon techniciansreported was correlated with howlong they had worked in the indus-try, as well as with such workplacefactors as the size of the salon andthe adequacy of ventilation. In asimilar study that used psychologi-cal, neuropsychological, and sen-sory tests (rather than a mail-inquestionnaire), LoSasso and col-leagues (2002) found that nail salontechnicians performed more poorlythan the controls on tests of atten-tion and information processing.The nail salon technicians alsoscored worse than the controls ontests of olfaction (ability to detectsmells). Taken together, these find-ings highlight the consequences ofeven low-level exposure to neuro-
toxic substances that can be found in places where manypeople work and where many others routinely visit.
The brain can be damaged byexposure to solvents. Nail studiosfrequently use a variety of organicsolvents that are known to be poten-tially damaging to the central ner-vous system.

Corpus callosumCommunicationbetween the brain'sright and lefthemispheres
Motor stripRegulation ofvoluntarymovement
Limbic systemAttention, emotions,"fight or flight,"memory
Discrimination of sounds,verbal and speech behavior
Reticular formationArousal reactions,information screening
somewhat different types of mental processing. At therisk of oversimplifying, it is generally accepted that func-tions that are dependent on serial processing of familiarinformation, such as language and solving mathematicalequations, take place mostly in the left hemisphere fornearly everyone. Conversely, the right hemisphereappears to be generally specialized for grasping overallmeanings in novel situations, reasoning on a nonverbal,intuitive level, and appreciation of spatial relations. Evenwithin hemispheres, the various lobes and regions withinthem mediate specialized functions.
Although none of these relationships between brainlocation and behavior can be considered universally true, itis possible to make broad generalizations about the likelyeffects of damage to particular parts of the brain. Damageto the frontal areas, for example, is associated with either oftwo contrasting clinical pictures: (1) behavioral inertia,passivity, apathy, and perseverative thought, or (2) impul-siveness and distractibility. Damage to specific areas of the
Sensory stripIntegration of sensoryinformation from variousparts of the body
Parietal lobeSomaesthetic and motordiscriminations and functions
ThalamusMajor relay station formessages from all partsof the body, importantin sensations of pain
CerebellumFine motor coordination,posture, and balance
MedullaBreathing, blood pressure,other vital functions
right parietal lobe may produce impairment of visual-motor coordination, and damage to the left parietal areamay impair certain aspects of language function, includingreading and writing, as well as arithmetical abilities. Dam-age to certain structures within the temporal lobes disruptsan early stage of memory storage. Extensive bilateral tem-poral damage can produce a syndrome in which remotememory remains relatively intact but nothing new can bestored for later retrieval. Damage to other structureswithin the temporal lobes is associated with disturbancesof eating, sexuality, and the emotions. Occipital damageproduces a variety of visual impairments and visual associ-ation deficits, the nature of the deficit depending on theparticular site of the lesion. For example, a person may beunable to recognize familiar faces. Unfortunately, manytypes of brain disease are general and therefore diffuse intheir destructive effects, causing multiple and widespreadinterruptions of the brain's circuitry. Some consequencesof brain disorders that have mainly focal origins but com-

1. Impairment of memory. The individual hasnotable trouble remembering recent events andless trouble remembering events of the remotepast, with a tendency in some patients toconfabulate-that is, to invent memories to fillin gaps. In severe instances, no new experiencecan be retained for more than a few minutes.
2. Impairment of orientation. The individual isunable to locate himself or herself accurately,especially in time but also in space or in relationto the personal identities of self or others.
3. Impairment of learning, comprehension, andjudgment. The individual's thinking becomesclouded, sluggish, and/or inaccurate. The personmay lose the ability to plan with foresight or tounderstand abstract concepts and hence toprocess complex information (described as"thought impoverishment").
4. Impairment of emotional control or modulation.The individual manifests emotional overreactivitysuch as easy arousal to laughter, tears, or rage.
5. Apathy or emotional blunting. The individualmanifests emotional underreactivity, especially incases of advanced deterioration.
6. Impairment in the initiation of behavior. Theindividual lacks self-starting capability and mayhave to be reminded repeatedly about what to donext, even when the behavior involved remainswell within the person's range of competence.This is sometimes referred to as "loss of executivefunction."
7. Impairment of controls over matters of proprietyand ethical conduct. The individual may manifesta marked lowering of personal standards in areassuch as appearance, personal hygiene, sexuality,or language.
8. Impairment of receptive and expressivecommunication. The individual may be unable tocomprehend written or spoken language or maybe unable to express his or her own thoughtsorally or in writing.
9. Impaired visuospatial ability. The individual hasdifficulty coordinating motor activity with thecharacteristics of the visual environment, a deficitthat affects graphomotor (handwriting anddrawing) and constructional (e.g., assemblingthings) performance.
monly appear in the context of progressively diffuse dam-age are shown in Table 15.1.
The Neuropsychology/Psychopathology InteractionMost people who have a neuropsychological disorder donot develop psychopathological symptoms such as panicattacks, dissociative episodes, or delusions. However, manyshow at least mild deficits in cognitive processing and self-regulation. Similarly, some people who suffer from psy-chopathological disorders also have cognitive deficits. Forexample, patients with bipolar disorder have persistentcognitive deficits that can be detected even during periodsof illness remission (Cavanagh et aI., 2002; Clark et aI.,2002; Ferrier & Thompson, 2002). This highlights the closelink between psychopathological and neuropsychologicalconditions.
The psychopathological symptoms that do sometimesaccompany brain impairment are not always predictableand can reflect individual nuances consistent with thepatient's age (see Tateno et aI., 2002), her or his prior per-
sonality, and the total psychological situation confrontingthe patient. It is erroneous to assume that a psychologicaldisorder-for example, a serious depression that follows abrain injury-is necessarily and completely explained bythe patient's brain damage. Certainly that could be thecase. However, it is also possible that the depression mightbe better explained by the patient's awareness of dramati-cally lessened competence and the loss of previous skills.After a traumatic brain injury caused by an accident or afall, for example, around 18 percent of patients make a sui-cide attempt (Simpson & Tate, 2002).
People with more favorable life situations tend to farebetter after brain injury than people whose lives are moredisorganized or disadvantaged (Yeates et aI., 1997). Intelli-gent, well-educated, mentally active people have enhancedresistance to mental and behavioral deterioration follow-ing significant brain injury (e.g., see Mori et aI., 1997a;Schmand et aI., 1997). Because the brain is the organresponsible for the integration of behavior, however, thereare limits to the amount of brain damage that anyone cantolerate or compensate for without exhibiting behaviorthat is decidedly abnormal.

In ReVIew~ Describe some of the major ways in which
the brain can become damaged.~ What kinds of clinical symptoms are often
associated with damage to the frontal,parietal, temporal, and occipital lobes ofthe brain?
~ List nine symptoms that are typical of focaland diffuse brain damage.
DELIRIUM
Delirium (see the table on criteria for delirium) is a com-monly occurring syndrome. It is an acute confusionalstate that lies between normal wakefulness and stupor orcoma (see Figure 15.3). It has a sudden onset and involvesa fluctuating state of reduced awareness. Essentially, delir-ium reflects a major change in the way the brain is work-ing. In addition to a disturbance in level of consciousness,delirium also involves cognitive changes. Information-processing capacities are impaired, affecting such basicfunctions as attention, perception, memory, and thinking.Hallucinations and delusions are quite common (seeTrzepacz et aI., 2002). In addition, the syndrome oftenincludes abnormal psychomotor activity such as wildthrashing about and disturbance of the sleep cycle. A deliri-0us person is essentially unable to carry out purposefulmental activity of any kind. The intensity of the symptomsalso fluctuates over the course of a 24-hour period, asdescribed in the following case study.
"I l r
. " DSM-IV-TR:,; "..• 1 ~, t • f' ,
~ Disturbance of consciousness (Le., reduced awareness ofthe environment).
~ A change in cognition (e.g., memory deficit, disorientation)that is not related to dementia.
~ The disturbance develops over a short period of time(usually hours to days) and tends to fluctuate over thecourse of the day.
Source: Adapted with permission from the Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition, Text Revision(Copyright 2000). American Psychiatric Association.
DelirIum FollowIng aRoutine Operation
Mrs. Petersen is a 75-year-old widow. She was admittedto the hospital after breaking her leg. She had a routineoperation, and after this, she began to show signs ofconfusion. Her consciousness became clouded, withreduced attention and awareness. She could not remem-ber what had happened to her or why she was in the hos-pital. During the day, she showed mild and aimlesshyperactive behavior. She was unable to read or watchtelevision and could not always recognize relatives whovisited her. She was seen having conversations withimaginary persons and staring at a point on the ceiling.She was irritable and would burst out in anger. Sheknocked her meals onto the floor and refused to take anymedications. Between outbursts Mrs. Petersen calmeddown and was able to sleep for up to half an hour, but atnight she seemed unable to sleep at all, and the hyper-activity increased. As other patients fell asleep for thenight, Mrs. Petersen started wandering about the wardwaking them up again. She went into other people'srooms and tried to climb into their beds. Several timesshe tried to leave the hospital in her nightdress but wasstopped and brought back to her room. (Adapted fromOstOnet aI., 1996.)
Delirium can occur in a person of any age. However,the elderly are at particularly high risk, perhaps because ofbrain changes caused by normal aging that lead to"reduced brain reserve." As described in the case of Mrs.Petersen, delirium is very common in the elderly after theyhave had surgery, patients over 80 being particularly at risk(Trzepacz et aI., 2002). At the other end of the age spec-trum, children are also at high risk of delirium, perhapsbecause their brains are not yet fully developed. Estimatesof the prevalence of delirium vary widely with the age ofthe population studied but are somewhere in the region of5 to 40 percent of hospitalized patients (Fann, 2000) .
Delirium may result from several conditions includ-ing head injury and infection. However, the most commoncause of delirium is drug intoxication or withdrawal. Toxi-city from medications also causes many cases of delirium.This may explain why delirium is so common in the elderlyafter they have had surgery.
Delirium is a true medical emergency, and its underlyingcause must be identified and managed. Most cases of delir-ium are reversible, except when the delirium is caused by aterminal illness or by severe brain trauma. Treatmentinvolves medication, environmental manipulations, andfamily support (American Psychiatric Association, 1999).

l_Delir_ium ~
The medications that are used for most cases are neurolep-tics (Lee et al., 2004). These are the same drugs that areused to treat schizophrenia. For delirium caused by alcoholor drug withdrawal, benzodiazepines (such as those usedin the treatment of anxiety disorders) are used (Trzepaczet al., 2002). In addition, orienting techniques (such as cal-endars and staff prompting) and environmental modifica-tions (e.g., nightlights) can be helpful. Some patients,however, especially elderly ones, may still have orientationproblems, sleep problems, and other difficulties evenmonths after an episode of delirium.
In ReVIew~ What clinical features characterize the
syndrome of delirium?~ Describe some common causes of delirium.
Who is most at risk of developing this clinicalcondition?
~ How is delirium treated?
DEMENTIAUnlike delirium, dementia is not a rapidly fluctuating con-dition. Dementia implies loss, and it is characterized by adecline from a previously attained level of functioning (seethe table on criteria for dementia). The onset of dementia istypically quite gradual. Early on, the individual is alert andfairly well attuned to events in the environment. Even in theearly stages, however, memory is invariably affected, espe-cially memory for recent events. As time goes on, patientswith dementia show increasingly marked deficits inabstract thinking, the acquisition of new knowledge orskills, visuospatial comprehension, motor control, problemsolving, and judgment. Dementia is often accompanied byan impairment in emotional control and in moral and eth-ical sensibilities; for example, the person may engage in
Continuum of Level ofConsciousness
I_~oma
Source: FromThe American Psychi-atric Publishing Textbook of Neu-ropsychiatry and ClinicalNeurosciences. 4th ed.• p. 526.Reprinted by permission of AmericanPsychiatric Publishing. Inc..www.appLorg.
crude solicitations for sex. Dementia may be progressive(getting worse over time) or static but is more often the for-mer. Occasionally dementia is reversible if it has an under-lying cause that can be removed or treated (such as vitamindeficiency) .
At least 50 different disorders are known to causedementia (Bondi & Lange, 2001). They include degenera-tive diseases such as Huntington's disease and Parkinson'sdisease (which are described in The World Around Us15.3). Other causes are strokes (see Ivan et aI., 2004); cer-tain infectious diseases such as syphilis, meningitis, andAIDS; intracranial tumors and abscesses; certain dietarydeficiencies (especially of the B vitamins); severe or
[
DSM-N-TR
~ The development of multiple cognitive deficits manifestedby both
(1) Memory impairment.
(2) One or more of the following cognitive disturbances:
(a) Aphasia (language disturbance).
(b) Apraxia (impaired ability to carry out motor tasksdespite having the motor ability to do so).
(c) Agnosia (failure to recognize or identify objectsdespite intact sensory function).
(d) Disturbance in executive functioning (Le., planning,organizing, sequencing, abstracting).
~ The cognitive deficits cause significant impairment infunctioning and represent a significant decline from aprevious level of functioning.
~ The onset of the disorder is gradual and there iscontinuing cognitive decline.
Source: Adapted with permission from the Diagnostic andStatistical Manual of Mental Disorders. Fourth Edition, Text Revision(Copyright 2000). American Psychiatric Association.

15.3First described in 1817, Parkinson's disease is a form of"shaking palsy." It is the second most common neurode-generative disorder (after Alzheimer's disease), with aprevalence of 1 per 1,000. The causes of Parkinson's dis-ease are not clear, although both genetic and environmen-tal factors are suspected.
Parkinson's disease is more common in men than inwomen. In general, it develops in people aged 50 to 70
years. However, the actor Michael J. Fox developed Parkin·son's disease when he was only 30 years old. His bookLucky Man (2002) offers a moving personal account of hisstruggle with the illness and well describes some of itsmajor symptoms.
I need to explain the "on-off" phenomenon. This Jekyll-and-Hyde melodrama is a constant vexation for the P.O.patient, especially one as determined as I was toremain closeted. "On" refers to the time when the med-ication is telling my brain everything it wants to hear.I'm relatively loose and fluid, my mind clear and move-ments under control. Only a trained observer coulddetect my Parkinson's. During one of my "off" periods,even the most myopic layperson, while perhaps notable to diagnose P.O.specifically, can recognize that Iam in serious trouble.
When I'm "off," the disease has complete author-ity over my physical being. I'm utterly in its possession.Sometimes there are flashes offunction, and I can beeffective at performing basic physical tasks, certainlyfeeding and dressing myself (though !'lliean towardloafers and pullover sweaters), as well as any chorecalling for more brute force than manual dexterity. In myvery worst "off" times I experience the full panoply ofclassic Parkinsonian symptoms: rigidity, shuffling,tremors, lack of balance, diminished small motor con-trol, and the insidious cluster of symptoms that makescommunication-written as well as spoken-difficultand sometimes impossible.
Huntington's DiseaseHuntington's disease is a rare degenerative disorder of thecentral nervous system that afflicts about 1 in every 10,000
people. It was first described in 1872 by the American neu-rologist George Huntington. The illness begins in mid life (the
repeated head injury; anoxia (oxygen deprivation); and theingestion or inhalation of toxic substances such as lead ormercury. As Figure 15.4 illustrates, the most commoncause of dementia is degenerative brain disease, particu-
Actor Michael]. Fox developed Parkinson's disease when hewas only 30 years old. After the diagnosis, he started afoundation to fund research into a cure for the disorder.
mean age of onset is around 40 years) and it affects menand women in equal numbers. Huntington's disease is char-acterized by a chronic, progressive chorea (involuntary andirregular movements that flow randomly from one area ofthe body to another). Patients eventually develop dementia,and death usually occurs within 10 to 20 years of first devel-oping the illness. Huntington's disease is caused by an auto-somal dominant gene on chromosome 4. This means that aperson who has a parent with the disease has a 50 percentchance of developing the disease himself or herself. Agenetic test can be given to at-risk individuals to determinewhether they will eventually develop the disorder. However,because there is no cure for Huntington's disease, many at-risk people choose not to know what their genetic destiny is.
larly Alzheimer's disease. In this chapter we will focus pri-marily on this greatly feared disorder. We will also brieflydiscuss dementia caused by HIV infection and vasculardementia.

Parkinson'sdisease
7.7%
Brain injury 4.4% /
Other causes 5.5%
MedicationsEmotional depressionVitamin B12 deficiencyChronic alcoholismCertain tumors or infections
of the brain
Blood clots pressingon the brain
Metabolic imbalances(including thyroid,kidney, or liverdisorders)
Distribution of Dementia by Probable Cause*
*Numbers do not add up to 100 percent because ofrounding off.Source: Dennis J. Selkoe. (1993). Aging brain, aging mind. In Mindand Brain: Readings from Scientific American (p. 111).New York: Free·man; and Johnny Johnson, Some treatable causes of dementia,Scientific American (September 2003). Copyright © 2003 by ScientificAmerican, Inc. All rights reserved. Reprinted by permission.
Alzheimer's disease (AD) takes its name from AloisAlzheimer (1864-1915), the German neuropathologistwho first described it in 1907. It is the most common causeof dementia (Askin-Edgar et aI., 2002). In the DSM-IV-TRit is referred to (on Axis 1) as "dementia of the Alzheimer'stype." Alzheimer's disease is associated with a characteris-tic dementia syndrome that has an imperceptible onsetand a usually slow but progressively deteriorating course,terminating in delirium and death. Public awareness of thedisorder has been high since late president Ronald Reaganannounced in November 1994 that he was suffering fromthe disease.
Hans is a 66-year-old man who has become so forgetfulthat his wife is now afraid to leave him alone, even in thehouse. At the age of 60, Hans took early retirement from
Former president Ronald Reagan raised the public's awareness ofAlzheimer's disease after he announced in 1994 that he had beendiagnosed with the illness. He died in 2004.
his job in a government office, because for the previous 5years he had not been able to carry out his duties prop-erly. He constantly made mistakes when delivering themail to different sections of the building. At the sametime, he had gradually given up his hobbies and hadbecome more and more quiet. At first, his growing forget-fulness had not been very noticeable in his home envi-ronment. Then one day, at the age of 62, when leading ahike in an area he knew well, he could not find the wayhome. Since then, his memory failures became ever morepronounced. He mislaid things, forgot appointments, andcould no longer find his way around the area where hehad lived for more than 40 years. He failed to recognizeeven good friends and lost interest in newspapers andtelevision. (Adapted from UstUn et aI., 1996.)
THE CLINICAL PICTURE IN AD The diagnosis of AD ismade on the basis of a thorough clinical assessment of thepatient but cannot be absolutely confirmed until after thepatient's death. This is because an autopsy must be per-formed in order to see the amyloid plaques andneurofibrillary tangles that are such distinctive signs ofAlzheimer neuropathology. In the living patient, the diag-nosis is normally given only after all other potential causesof dementia are ruled out by case and family history,

Some brain diseases, Alzheimer's among them, can bediagnosed with certainty only at autopsy. Amyloid plaques,neurafibrillary tangles, and overall brain atrophy (top) arephysical evidence of Alzheimer's disease. Compare this to ahealthy brain (bottom).
physical examination, and laboratory tests. Neuroimagingtechniques are now being explored as a way to facilitateearly diagnostic assessment of patients suspected to haveAD (e.g., Devanand et al., 2000; D.H.S. Silverman et al.,2001). Although such approaches can aid in the positivediagnosis of AD, the ability of magnetic resonance imag-ing (MRI) to discriminate AD from other dementias isuncertain (Skoog, 2002).
Alzheimer's disease usually begins after about age 45(Malaspina et al., 2002). Contrary to what many peoplebelieve, it is characterized by multiple cognitive deficits,not just problems with memory. There is a gradual declin-ing course that involves slow mental deterioration. In somecases a physical ailment or some other stressful event is amilestone, but most AD victims pass into a demented statealmost imperceptibly, so that it is impossible to date theonset of the disorder precisely. The clinical picture maydiffer markedly from one person to another, depending on
the nature and extent of brain degeneration, the premor-bid personality of the individual, the particular str~ssorspresent, and the degree of environmental support. The fol-lowing case, which involves a man who had retired some7 years prior to his hospitalization, is typical of the deteri-oration resulting from AD.
Duringthe past 5 years, the patient had shown a progres-sive loss of interest in his surroundings and during thelast year had become increasingly "childish." His wifeand eldest son had brought him to the hospital becausethey felt they could no longer care for him in their home,particularly because of the grandchildren. They statedthat he had become careless in his eating and other per·sonal habits and was restless and prone to wanderingabout at night. He could not seem to remember anythingthat had happened during the day but was garrulous con-cerning events of his childhood and middle years.
After admission to the hospital, the patient seemedto deteriorate rapidly. He could rarely remember whathad happened a few minutes before, although his mem-ory for remote events of his childhood remained good.When visited by his wife and children, he mistook themfor old friends, and he could not recall anything about thevisit a few minutes after they had departed. The followingbrief conversation with the patient, which took placeafter he had been in the hospital for 9 months (and about3 months before his death), shows his disorientation fortime and person.
DOCTOR: Howare you today, Mr.__ ?PATIENT: Oh ... hello [looks at doctor in rather puzzled
way as if trying to make out who he is].DOCTOR: Doyou know where you are now?PATIENT: Why yes ... I am at home. I must paint the
house this summer. It has needed painting for a longtime but it seems like Ijust keep putting it off.
DOCTOR: Can you tell me the day today?PATIENT: Isn't today Sunday ... why, yes, the children are
coming over for dinner today. Wealways have dinnerfor the whole family on Sunday. My wife was herejust a minute ago but Iguess she has gone back intothe kitchen.
As is illustrated in this case, AD often begins with theperson's gradual withdrawal from active engagement withlife. There is a narrowing of social activities and interests, alessening of mental alertness and adaptability, and a lower-ing of tolerance to new ideas and changes in routine. Oftenthoughts and activities become self-centered and childlike,

5.1s it possible to detect Alzheimer's disease in its
early stages? Many researchers are now activelyexploring this issue. Todo this, they are using arange of techniques including PET,MRI,andfMRIto study the brain both at rest and at work.
In addition, they are studying not only people who haveAlzheimer's disease, but also those at high risk for devel-oping the disorder.
One high-risk group is people who are experiencingmild cognitive impairment or MCI.MCIis thought to be on acontinuum between healthy aging and the earliest signs ofdementia (Petersen et aI., 2001). People with MCIreportmemory problems and perform less well on tests of mem-ory. However, they are generally functioning at a normallevel. Roughly half of people who currently have MCIwill bediagnosed with ADwithin the next 3 to 5 years (Petersenet aI., 2001). Another high-risk group is people who do nothave any cognitive problems but who are considered to beat high risk for developing AD.This could be either becausethey have a relative with the disorder or because they havethe APOE-E4allele.
The research findings are complex and there are nodefinitive answers yet. However, a central part of the storyinvolves the hippocampus, a brain area that is involved inmemory. Patients with Alzheimer's disease show atrophy ofthe hippocamus (Chetelat et aI., 2003; Kubota et aI., 2005).
This brain area is also less active when ADpatients (ascompared to controls) are engaged in memory tasks (Katoet aI., 2001; Sperling et aI., 2003, 2005).
Interestingly, brain scans of people with MCIalsoshow atrophy in a number of brain areas including thehippocampus (Chetelat et aI., 2002; Du et aI., 2001; Jack
including a preoccupation with the bodily functions ofeating, digestion, and excretion. As these changes becomemore severe, additional symptoms-such as impairedmemory for recent events, "empty" speech (in whichgrammar and syntax remain intact but vague and seem-ingly pointless expressions replace meaningful conversa-tional exchange, for example, "It's a nice day, but it mightrain"), messiness, impaired judgment, agitation, and peri-ods of confusion-make their appearance. The clinicalpicture is by no means uniform until the terminal stages,when the patient is reduced to a vegetative level.
Approximately half of all AD patients display a courseof simple deterioration. That is, they gradually lose variousmental capacities, typically beginning with memory forrecent events and progressing to disorientation, poor judg-ment, neglect of personal hygiene, and loss of contact with
The Early Detection ofAlzheimer's Disease
et aI., 1999; Van Der Flier et aI., 2002; Visser et aI., 1999).
Moreover, when functional imaging techniques are used towatch the brain at work, people with MCI(like those withAlzheimer's disease) also show less activation in the hip-pocampus (Chetelat et aI., 2003; De Santi et aI., 2001).
These findings are in contrast to those found in people whoare cognitively normal but who are at high risk becausethey carry the APOE-E4allele. These people do not show alack of activation in the hippocampus when they areinvolved in memory tasks. Instead, brain-imaging studiesreveal the opposite. Rather than underactivity, people whoare at genetic high risk show increased activity in variousparts of the brain, including the hippocampus, when theyengage in memory tasks (Bookheimer et aI., 2000; Smithet aI., 2002).
How can we explain these rather contradictory find-ings? Current thinking is that the greater degree of brainactivation in people who are cognitively normal but at highrisk for developing ADreflects the greater effort they needto make to manage the task. Simply put, carriers of theAPOE-E4allele may have to work harder. Because theirbrain tissue is still healthy (unlike ADpatients and peoplewith MCt),we see an increase in brain activation inresponse to a cognitive challenge rather than the decreasein activation that is more typical of ADpatients or thosewith mild cognitive impairment.
Does brain-imaging research allow us to identify peo-ple who are going to develop dementia? At present theanswer is no. None of the changes are specific enough yetto be able to be used to make an early diagnosis. This,however, is the goal for the future.
reality to an extent that precludes independent functioningas adults. Perhaps because Alzheimer's disease damages thetemporal lobes of the brain, delusions are also found insome patients (Lyketsos et aL, 2000). Although delusionsof persecution are predominant, delusional jealousy issometimes seen. Here the person persistently accuses his orher partner or spouse-who is often of advanced age andphysically debilitated-of being sexually unfaithful. Fam-ily members may be accused of poisoning the patient'sfood or of plotting to steal the patient's funds. Fortunately,punitive retribution in the form of physical attacks on the"evil-doers" is not especially common, but a combativepattern does occasionally occur, complicating the patient'smanagement. In a study of physically aggressive ADpatients, Gilley and associates (1997) found that 80 percentof them were delusional.

With appropriate treatment, which may include med-ication and the maintenance of a calm, reassuring, andunprovocative social environment, many people withAlzheimer's disease show some alleviation of symptoms.In general, however, deterioration continues its downwardcourse over a period of months or years. Eventually,patients become oblivious to their surroundings, bedrid-den, and reduced to a vegetative state. Resistance to diseaseis lowered, and death usually results from pneumonia orsome other respiratory or cardiac problem. It is typicallytaught that patients with AD live about 7 to 10 years afterthey are diagnosed (Bondi & Lange, 2001). However, datafrom a large Canadian study suggest that the average dura-tion of life after the individual first contacts a doctor formemory problems may be as little as 3.3 years (Wolfsonet aI., 2001).
PREVALENCE OF AD Alzheimer's dementia is fastbecoming a major public health problem, straining soci-etal and family resources. AD accounts for a large propor-tion of all cases of dementia (Lyketsos et aI., 2000).Although AD is not an inevitable consequence of aging(George Bernard Shaw, for example, wrote plays well intohis nineties), age is clearly a major risk factor. For all of us,the brain starts to decrease in size after about age 18. By thetime we reach the age of 80, our brain has lost about 15percent of its original weight (Perl, 1999).
It has been estimated that the rate of AD doublesabout every 5 years after a person reaches the age of 40(Hendrie, 1998). Conservatively, about 1 to 2 percent ofthe population in the age range of 65 to 74 have AD, andabout 25 percent of people older than 85 have the disease(Hendrie, 1998). It is also estimated that approximately360,000 new cases (incidence) will occur each year andthat this number will increase as the population ages(Brookmeyer et aI., 1998). Currently, about 4 million peo-ple in this country have AD. In the next 50 years, this figureis expected to more than triple (Askin-Edgar et aI., 2002).The future prospects regarding the prevalence of AD aretherefore somewhat alarming. If we have not solved theproblem of preventing AD (or arresting it in its earlystages) by around that time, society will be faced with theoverwhelming problem of caring for millions of dementedsenior citizens. The adverse family, social, and economicconsequences, already considerable, could become devas-tating (Fisher & Carstensen, 1990).
For reasons that are not yet clear, women seem to havea slightly higher risk of developing AD than men (Askin-Edgar et aI., 2002). Indeed, Alois Alzheimer's original casewas a 51-year-old woman. Women tend to live longer thanmen, but the increased prevalence of women with AD maynot be entirely explained by this. The prevalence ofAlzheimer's disease is lower in non-Western developedcountries such as Japan, as well as in less industrializedcountries like Nigeria and India (Malaspina et aI., 2002).
Such observations have led researchers to suspect thatenvironmental fadors such as a high-fat, high-cholesteroldiet is implicated in the development of Alzheimer's dis-ease (Sjogren & Blennow, 2005). Also implicating diet,researchers have found that high levels of an amino acidcalled "homocysteine" (which is a risk factor for heart dis-ease) seem to increase a person's risk of developingAlzheimer's disease later in life (Ravaglia et aI., 2005). Lev-els of homocysteine in the blood can be reduced by takingfolic acid and certain B vitamins. Taking statin drugs tolower cholesterol also seems to offer some protectionagainst AD (Sparks et aI., 2005).
GENETIC AND ENVIRONMENTAL ASPECTS OF ADWhen we picture a typical Alzheimer patient, we imagine aperson of very advanced age. Sometimes, however, ADbegins much earlier and affects people in their forties orfifties. In such cases, the progress of the disease and itsassociated dementia is often rapid (Heyman et aI., 1987).Considerable evidence suggests an especially substantialgenetic contribution in early-onset Alzheimer's disease(see Holmes, 2002; Malaspina et aI., 2002, for reviews),although different genes may be involved in different fam-ilies (Breitner et al., 1993). Genes also playa role in late-onset AD.
Cases of early-onset Alzheimer's disease appear to becaused by rare genetic mutations. So far three such muta-tions have been identified. One involves the APP gene,which is located on chromosome 21. The fact that a muta-tion of a gene on chromosome 21 has been found to beimportant in AD is interesting, because it has long beenknown that people with Down syndrome (which is causedby a tripling, or trisomy, of chromosome 21; see Chapter16) who survive beyond about age 40 develop anAlzheimer's-like dementia (Bauer & Shea, 1986; Janicki &Dalton, 1993). They also show similar neuropathologicalchanges (Schapiro & Rapoport, 1987). In addition, cases ofDown syndrome tend to occur more frequently in the fam-ilies of patients with Alzheimer's disease (Heyman et aI.,1984; Schupf et aI., 1994). One study has found thatmothers who gave birth to a child with Down syndromebefore age 35 had a 4.8 times greater risk of developingAlzheimer's disease when they were older, compared tomothers of children with other types of mental retardation(Schupf et al., 2001). Mutations of the APP gene are asso-ciated with an onset of AD somewhere between 55 and 60years of age (Cruts et al., 1998).
Other cases of even earlier onset appear to be associ-ated with mutations of a gene on chromosome 14 calledpresenilin 1 (PSI) and with a mutation of the presenilin 2(PS2) gene on chromosome 1. These genes are associatedwith an onset of AD somewhere between 30 and 50 years ofage (Cruts et aI., 1998). One carrier of the PSI mutation iseven known to have developed the disorder at age 24(Wisniewski et aI., 1998). Remember, however, that these

mutant genes, which are autosomal dominant genes and sonearly always cause AD in anyone who carries them, areextremely rare. The APP, PSI, and PS2 genetic mutationsprobably account, together, for no more than about 5 per-cent of cases of AD.
A gene that may playa greater role in cases of late-onset Alzheimer's disease is the APOE (apolipoprotein)gene on chromosome 19. This gene codes for a blood pro-tein that helps carry cholesterol through the bloodstream.It has been discovered that differing forms (genetic alleles)of APOE differentially predict risk for late-onset AD. Threesuch alleles have been identified, and everyone inherits twoof them, one from each parent. One of these alleles, theAPOE-E4 allele, significantly enhances risk for late-onsetAD. Thus a person may inherit zero, one, or two of theAPOE-E4 forms, and his or her risk for AD increases cor-respondingly. Another such allele, APOE- E2, seems to con-vey protection against late-onset AD. The remaining andmost common allele form, APOE- E3, is of "neutral" signif-icance in predicting AD (e.g., Katzman et al., 1997; Lopezet al., 1997; Martin et al., 1997; Plassman & Breitner, 1997).APOE-E4 has been shown to be a significant predictor ofmemory deterioration in older individuals with or withoutclinical dementia (Hofer et al., 2002). The APOE-E4 alleleis relatively uncommon in Chinese people compared to itsfrequency in people from Europe or North America. Incontrast, people of African descent are especially likely tohave this allele (Waters & Nicoll, 2005).
The APOE- E4 allele (which can be detected by a bloodtest) is overrepresented in all types of AD, including theearly-onset and late-onset forms. Approximately 65 per-cent of patients with AD have at least one copy of theAPOE-E4 allele (see Malaspina et al., 2002). Exciting asthey are, however, these discoveries still do not account forall cases of AD, not even all cases of late-onset AD (e.g.,Bergem et al., 1997). Many people who inherit the mostrisky APOE pattern (two APOE-E4 alleles) do not suc-cumb to AD. One study found that only 55 percent ofpeople who had two APO E-E4 alleles had developed AD byage 80 (Myers et al., 1996). And others with AD have nosuch APOE-E4 risk factor. In addition, substantial num-bers of monozygotic twins are discordant for the disease(Bergem et al., 1997; Breitner et al., 1993).
Why should this be? Current thinking is that ourgenetic susceptibility interacts with other genetic factorsand with environmental factors to determine whether wewill succumb to any particular disorder. Clearly, othergenes involved in the development of AD still remain to befound. However, environmental factors may also playa keyrole. As we have noted, the different prevalences of ADacross different parts of the world suggest that diet may bean important mediating environmental variable. Otherenvironmental factors under consideration include expo-sure to metals such as aluminum, and experiencing headtrauma. One prospective study has found that traumatic
The German neuropathologist Alois Alzheimer was the first torecognize and describe the disease that is now named after him.
brain injury is associated, for up to 5 years after the injury,with a fourfold increase in risk of developing Alzheimer'sdisease (see Malaspina et al., 2002). On the other hand,exposure to nonsteroidal anti-inflammatory drugs such asibuprofen may be protective and lead to a lower risk of AD(Breitner et al., 1994; in't Veld et al., 2001; Weggen et al.,2001). This view leaves open the possibility of reducing ordelaying the occurrence of AD by deliberately limitingexposure to risks and taking other preventive measures.
NEUROPATHOLOGY When Alois Alzheimer performedthe first autopsy on his patient (she was known asAuguste D.), he identified a number of brain abnormalitiesthat are now known to be characteristic of the disease.These are (1) senile plaques, (2) neurofibrillary tangles,and (3) the abnormal appearance of small holes in neu-ronal tissue, called "granulovacuoles;' which derive fromcell degeneration. Although plaques and tangles are alsofound in normal brains, they are present in much greaternumbers in patients with AD.
But what goes wrong first? Senile plaques are made ofdeformed nerve cell terminals. An important observationconcerning the plaques is that at their core, they contain asticky protein substance called beta amyloid. This substance

This photomicrograph of a brain tissue specimen from anAlzheimer's patient shows the characteristic plaques (darkpatches) and neurofibrillary tangles (irregular pattern of strand-like fibers).
(and a chemical precursor to it) also occurs in abnormalabundance in other parts of AD patients' brains (Hardy,2004). It is believed that accumulation of beta amyloid iswhat causes plaques. Having the APOE-E4 form of theAPOE gene may also facilitate the aggregation of amyloidin the brain (Askin-Edgar et aI., 2002). Moreover, betaamyloid has been shown to be neurotoxic. In other words,it causes cell death (Seppa, 1998). Current thinking is thatthe accumulation of beta amyloid plays a primary role inthe development of AD.
Neurofibrillary tangles are webs of abnormal filamentswithin a nerve cell. These filaments are made up of anotherprotein called tau. Researchers now suspect that abnormaltau protein in the neurofibrillary tangles may be caused byan increasing burden of amyloid in the brain. In otherwords, the presence of tau is secondary to the presence ofamyloid and is a sign that the disease is progressing (Hardy,2004). Animal studies of mice that have been geneticallymodified to be highly susceptible to developing AD (so-called "transgenic mice") support this idea (G6tz et aI.,2001; Lewis et aI., 2001). If this idea proves correct, it sug-gests that the most promising drug treatments for
Alzheimer's disease may be those that can target and pre-vent amyloid build-up.
Another notable alteration in AD concerns the neuro-transmitter acetylcholine (ACh). This neurotransmitter isknown to be important in the mediation of memory.Although there is widespread destruction of neurons inAD, particularly in the area of the hippocampus (Adler,1994; Mori et aI., 1997b), evidence suggests that among theearliest and most severely affected structures are a clusterof cell bodies located in the basal forebrain and involved inthe release of ACh (Whitehouse et aI., 1982). The reduc-tion in brain ACh activity in patients with AD is correlatedwith the extent of neuronal damage (i.e., plaques, tangles)that they have sustained (Debettignles et aI., 1997).
The loss of cells that produce ACh makes a bad situa-tion much worse. Because ACh is so important in memory,its depletion contributes greatly to the cognitive andbehavioral deficits that are characteristic of AD. For thisreason, drugs (called "cholinesterase inhibitors") thatinhibit the breakdown of ACh (and so increase the avail-ability of this neurotransmitter) can be clinically beneficialfor patients (Whitehouse, 1993; Winblad et aI., 2001).
TREATMENTS AND OUTCOMES IN AD We currentlyhave no treatment for AD that will restore functions oncethey have been destroyed or lost. Until something that cando this is discovered, we have only palliative measures thatdiminish patient and caregiver distress and relieve as far aspossible those complications of the disorder such as com-bativeness that increase the difficulties of management.
Some common problematic behaviors associatedwith AD (and with other dementias as well) are wander-ing off, incontinence, inappropriate sexual behavior, andinadequate self-care skills. These can be somewhat con-trolled via behavioral approaches (see Chapter 17).Because behavioral treatments need not be dependent oncomplex cognitive and communication abilities (whichtend to be lacking in AD patients), they may be particu-larly well suited for therapeutic intervention with thisgroup. In general, reports of results are moderatelyencouraging in terms of reducing unnecessary frustrationand embarrassment for the patient and difficulty for thecaregiver (Fisher & Carstensen, 1990; Mintzer et aI., 1997;Teri et aI., 1997).
Active treatment research has also focused on theconsistent findings of acetylcholine depletion in AD. Thereasoning here is that it might be possible to improvefunctioning by administering drugs that enhance theavailability of brain ACh. Currently, the most effective wayof doing so is by inhibiting the production of acetyl-cholinesterase, the principal enzyme involved in the meta-bolic breakdown of acetylcholine. This is the rationale foradministering drugs such as tacrine (Cognex) anddonepezil (Aricept). Winblad and colleagues (2001) stud-ied 286 patients who were randomly assigned to receiveeither medication (donepezil) or placebo for a I-year

Alzheimer'saffected cell
Normalcell
Neuriticplaque
FIGURE 15.5Depletion of Acetylcholine in Alzheimer's PatientsAlzheimer's Disease is characterized by nerve cell abnormalities that include the presence of neurofibrillary tangles, neuritic plaques ofbeta amyloid, and decreased levels of the neurotransmitter acetylcholine.
period. Patients' cognitive functioning and ability to per-form daily activities were measured at the start of the studyand again at regular intervals over the study period.Patients who received the medication did better overallthan patients who received the placebo. However, allpatients declined in their functioning over the course ofthe study. Furthermore, although donepezil does helppatients a little, these gains do not mean that patients tak-ing the drug are any less likely to avoid institutionalizationthan those who are not taking the medication (AD2000Collaborative Group, 2004).
The newest medication that has been approved totreat AD is memantine, which is marketed as Namenda.Unlike other approved medications, memantine is not acholinesterase inhibitor. Instead, it appears to regulate theactivity of the neurotransmitter glutamate, perhaps byprotecting cells against excess glutamate by partially block-ing NMDA receptors. Memantine, which can be usedalone or in combination with donepezil, appears to pro-vide patients with some cognitive benefits (Forchetti, 2005;Reisberg et aI., 2003).
Yet another line of treatment research is focused ondeveloping vaccines that might help clear away any accu-mulated amyloid plaques. Although initial findings fromanimal research looked promising (e.g., McLaurin et aI.,
2002), human clinical trials of a vaccine were stoppedabruptly in 2002 because of dangerous side effects.Nonetheless, researchers are continuing to explore noveltreatment approaches (Gestwicki et aI., 2004; Hardy, 2004;Hutter-Paier et aI., 2004). Many drug companies are nowworking on this problem.
Unfortunately, neuronal cells that have died with theadvance of Alzheimer's neuropathology are permanentlylost. This means that even if some new treatment couldhalt a patient's progressive loss of brain tissue, he or shewould still be left seriously impaired. The real key to effec-tive intervention must therefore be seen as preventive, orat least as deployable at the first sign of Alzheimer's (seeSchultz, 2000). For this reason, researchers are nowexploring ways to detect AD in its very early stages (seeDevelopments in Research 15.4 on p. 543).
TREATING CAREGIVERS It is estimated that about 30 to40 percent of nursing home residents are AD patients.Some patients with AD also reside in mental hospitals orother types of institutional settings. Most, however, live inthe community, typically with family members. Thisarrangement is often extremely stressful for caregivers(Fisher & Carstensen, 1990; Intrieri & Rapp, 1994; Shawet aI., 1997).

Patients with Alzheimer's disease slowly lose their mentalcapacities, beginning with memory and progressing todisorientation, poor judgment, and neglect of personal hygiene.
Any comprehensive approach to therapeutic interven-tion must consider the situation of caregivers. As the dis-ease advances, they are confronted not only with manychallenging management problems but also with the"social death" of the patient as a person and their own"anticipatory grief" (Gilhooly et al., 1994). As a group,caregivers are at extraordinarily high risk for developingdepression (Cohen & Eisdorfer, 1988), especially if they arehusbands caring for impaired wives (Robinson-Whelen &Kiecolt-Glaser, 1997; Tower et al., 1997). For example, onestudy showed that in those caregivers who were not clini-cally depressed, cortisol levels were essentially similar tothose in patients with major depression (Da Roza, Davis &Cowen, 2001). Caregivers of patients with AD tend to con-sume high quantities of psychotropic medication them-selves and to report many stress symptoms (Hinrichsen &Niederehe, 1994). Providing caregivers with counselingand supportive therapy is very beneficial and producesmeasurable reductions in their levels of depression (Mit-telman et al., 2004).
Infection with the Human Immunodeficiency Virus (HIV)wreaks havoc on the immune system. Over time, this infec-tion can lead to acquired immune deficiency syndrome orAIDS. Worldwide, the HIV type 1 virus has infected morethan 36 million people and resulted in approximately 20million deaths (Kaul et al., 2005).
In addition to devastating the body, the HIV virus isalso capable of inducing neurological disease that canresult in dementia. This can happen in two ways. First,because the immune system is weakened, people with HIVare more susceptible to rare infections caused by parasitesand fungi (Woodward, 2001). However, the virus alsoappears capable of damaging the brain more directly,resulting in neuronal injury and destruction of brain cells(see Snider et al., 1983; Kaul et al., 2005). Several differentforms of HIV-induced central nervous system pathologyhave been identified, some of which appear to be associ-ated with the emergence of psychotic (e.g., delusional)phenomena (Sewell et al., 1994).
The neuropathology of HIV-associated dementiainvolves various changes in the brain, among them gener-alized atrophy, edema (swelling), inflammation, andpatches of demyelination (Adams & Ferraro, 1997;Gabuzda & Hirsch, 1987; Gray et al., 1988; Price et al.,1988; Sewell et al., 1994). No brain area may be entirelyspared, but the damage appears to be concentrated in sub-cortical regions, notably the central white matter, the tissuesurrounding the ventricles, and deeper gray matter struc-tures such as the basal ganglia and thalamus. Ninety per-cent of AIDS patients show evidence of such changes onautopsy (Adams & Ferraro, 1997).
The neuropsychological features of AIDS, which tendto appear as a late phase of HIV infection (though oftenbefore the full development of AIDS itself), usually beginwith mild memory difficulties, psychomotor slowing, anddiminished attention and concentration (see Fernandezet al., 2002, for a review). Progression is typically rapidafter this point, with clear-cut dementia appearing inmany cases within 1 year, although considerably longerperiods have been reported. In general, and consistent withautopsy findings, the neuropsychological evidence pointsprimarily to a disruption of brain function at the subcorti-cal level; the most reliably reported finding is that ofnotably delayed reaction time (Law & Mapou, 1997). Thelater phases of AIDS dementia include behavioral regres-sion, confusion, psychotic thinking, apathy, and markedwithdrawal.
Estimates from the early 1990s suggested HIV-related dementia was present in 20-30% of people withadvanced HIV disease. Fortunately, the arrival of highlyactive antiretroviral therapy has not only resulted ininfected people living longer but it has also reduced theprevalence of HIV-related dementia to around 10.5%(Kaul et al., 2005). However, although rates of frank

dementia have decreased, around 30% of people who areinfected with the HIV virus show some signs of mild cogni-tive impairment (McArthur, 2004). Moreover, for reasonsthat are not yet clear, women may be at especially high riskof HIV-related cognitive impairment (McArthur, 2004).
Treatment with antiretroviral therapy does not fullyprevent the HIV virus from damaging the brain (Kaulet al., 2005). This may be because HIV penetrates into thenervous system soon after a person becomes infected.What this means is that, even though the new therapieshave made HIV/ AIDS a chronic but manageable condition(at least for those who have access to the necessary medica-tions) prevention of infection remains the only certainstrategy for avoiding the cognitive impairments associatedwith this disease.
Vascular dementia (VAD), formerly called "multi-infarctdementia," is frequently confused with AD because of itssimilar clinical picture of progressive dementia and itsincreasing incidence and prevalence rates with advancingage. It is actually an entirely different disease in terms of itsunderlying neuropathology. In this disorder, a series of cir-cumscribed cerebral infarcts-interruptions of the bloodsupply to minute areas of the brain because of arterialdisease, commonly known as "small strokes"-cumula-tively destroy neurons over expanding brain regions. Theaffected regions become soft and may degenerate overtime, leaving only cavities. Although this disorder tends tohave a more varied early clinical picture than AD (Wallin &Blennow, 1993), the progressive loss of cells leads to brainatrophy and behavioral impairments that ultimatelymimic those of AD (Bowler et al., 1997).
VAD tends to occur after the age of 50 and affectsmore men than women (Askin-Edgar et al., 2002). Abnor-malities of gait (e.g., being unsteady on one's feet) may bean early predictor of this condition (Verghese et al., 2002).Vascular dementia is less common than AD, accounting foronly some 19 percent of dementia cases in a communitysample aged 65 years or older (Lyketsos et al., 2000). Onereason for this is that VAD has a much shorter averagecourse because of a patient's vulnerability to sudden deathfrom stroke or cardiovascular disease (Askin-Edgar et al.,2002). Accompanying mood disorders are also more com-mon in vascular dementia than in Alzheimer's disease, per-haps because subcortical areas of the brain are moreaffected (Lyketsos et al., 2000). Occasionally, an unfortu-nate patient will be discovered to have both AD and VAD, acondition commonly referred to as "mixed" dementia(Cohen et aI., 1997).
The medical treatment ofVAD, though complicated,offers slightly more hope than that of Alzheimer's disease.Unlike AD, the basic problem of cerebral arteriosclerosis(decreased elasticity of brain arteries) can be medicallymanaged to some extent, perhaps decreasing the likeli-
hood of further strokes. The daunting problems that care-givers face, however, are much the same in the two condi-tions, indicating the appropriateness of support groups,stress reduction techniques, and the like.
In ReVIew~ What is dementia? How is it different from
delirium?~ List five diseases or clinical disorders that
can cause dementia.~ Describe some of the major risk factors for
Alzheimer's disease.~ What kinds of neuropathological
abnormalities are typical of theAlzheimer's brain?
AMNESTIC SYNDROME _~_.Amnestic is just another way of saying "amnesia," and thecharacteristic feature of amnestic syndrome is strikinglydisturbed memory. Immediate recall (that is, the ability torepeat what has just been heard) is not usually affected.Memory for remote past events is also usually relativelypreserved. However, short-term memory is typically soimpaired that the person is unable to recall events thattook place only a few minutes previously. To compensate,patients sometimes confabulate, apparently making upevents to fill in the void that they have in their memories.
In contrast to the dementia syndrome, overall cogni-tive functioning in the amnestic syndrome may remain rel-atively intact. The affected person may thus be able toexecute a complex task if it provides its own distinctivecues for each stage of the task. This is well illustrated in thefilm Memento, where the main character, Leonard, has anamnestic disorder caused by a traumatic head injury.Although he has severe anterograde amnesia and is unableto hold anything in his short-term memory for more thana minute or so, he uses polaroid photographs, notes, andtattoos on his body to retain the information he needs tosearch for his wife's killer.
Brain damage is the root cause of amnestic disorders.Most commonly, amnestic syndrome is caused by chronicalcohol use and associated deficiency in vitamin B1 (thi-amine). This was the cause of the memory loss of thepatient whose case is described below. Another commoncause is head trauma. Stroke, surgery in the temporal lobearea of the brain, hypoxia (oxygen deprivation), and someforms of brain infections (such as encephalitis) can also

~ The development of memory impairment (i.e., inability tolearn new information or to recall previously learnedinformation).
~ The memory disturbance causes significant impairment infunctioning and represents a decline from a previous levelof functioning.
~ The memory disturbance does not occur exclusively duringthe course of a delirium or a dementia.
Source: Adapted with permission from the Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition, Text Revision(Copyright 2000). American Psychiatric Association.
lead to amnestic disorder. In these cases, depending on thenature and extent of damage to the affected neural struc-tures and on the treatment undertaken, the syndrome mayin time abate wholly or partially. A wide range of tech-niques has been developed to assist the good-prognosisamnestic patient in remembering recent events (e.g., Gou-vier et aI., 1997).
Moreover, because procedural memory (i.e., the abil-ity to learn routines, skills, and actions) is often preservedin patients with amnesia, even patients without memoryfor specific personal experiences can still can be taught toperform tasks that might help them reenter the workforce(Cavaco et aI., 2004).
He Forgot the Name ofHis Daughter
Apowerfully built six·footer, Charles Jackson still showedtraces of a military bearing. Before he left the army a yearbefore, he had been demoted to buck private; this wasthe culmination of a string of disciplinary actions fordrunkenness.
For over a year he had had monthly consultationswith the current interviewer. On this occasion, the inter-viewer asked when they had last met. Charles replied,"Well, I just don't know. What do you think?" Tothe fol-low-up question, he said he guessed he had seen theinterviewer before. "Maybe it was last week."
Asking him to remain seated, the interviewer wentinto the waiting room to ask Mrs. Jackson how shethought her husband was doing. She said, "Oh, he'sabout the same as before. He sketches some. But mostlyhe just sits around the house and watches TV. I come
home and ask him what he's watching, but he can't eventell me."
Atany rate, Charles was no longer drinking, not sincethey had moved to the country. It was at least 2 miles tothe nearest convenience store, and he didn't walk verywell anymore. "But he still talks about drinking. Some-times he seems to think he's still in the army. He ordersme to go buy him a quart of gin."
Charles remembered quite a few things, if theyhappened long enough ago-the gin, for example, andgetting drunk with his father when he was a boy. But hecouldn't remember the name of his daughter, who wastwo and a half. Most of the time, he just called her "thegirl."
The interviewer walked back into the inner office.Charles looked up and smiled.
"Have Iseen you before?" asked the interviewer."Well, I'm pretty sure.""When was it?""It might have been last week."(Adapted from Morrison, 1995, pp. 50-51.)
In ReVIew~ What are the most striking clinical features of
amnestic syndrome?~ What are some of the major causes of
amnestic syndrome?
DISORDERS INVOLVINGHEAD INJURYTraumatic brain injury (TBI) occurs frequently, affectingmore than 2 million people each year in the United States.The most common cause of TBI is motor vehicle acci-dents. Other causes include falls, violent assaults, andsports injuries (although it is likely that the vast majorityof these are never even reported). Men aged 15 to 24 are atthe highest risk for brain injury. Stated simply, disordersthat result from traumatic injuries to the brain are morecommon than any other forms of neurological diseaseexcept headache (see Silver et aI., 2002, for a review). InDSM-IV- TR, brain injuries that have notable, long-stand-ing effects on adaptive functioning are coded on Axis Iusing the appropriate syndromal descriptive phrase, withthe qualifier "due to head trauma." (Examples include"dementia due to head trauma;"'amnestic disorder due tohead trauma;' and the like.)

Clinicians distinguish three general types ofTBI because theclinical pictures and residual problems vary somewhatamong them: (1) closed-head injury, in which the craniumremains intact; (2) penetrating head injury, in which thecranium, as well as the underlying brain, are penetrated bysome object such as a bullet; and (3) skull fracture, with orwithout compression of the brain by fragmented bone con-cavity. Post-trauma epilepsy, for example, is unusual inclosed-head injury but a rather common outcome of theother two forms of head injury. In closed-head injury, the
15.51n 1999 a 24-year-old Japanese woman devel-
oped a headache after spending the day atthe Fujikyu Highland Park in Japan. Duringthat time, she had ridden twice on each ofthree different roller coasters, including the
Fujiyama. At 259 feet, this is the fifth tallest rollercoaster in the world. It reaches speeds of over 81 milesper hour and it has a 229-foot drop. The young woman'sheadache lasted 4 days and was initially diagnosed asa tension headache. It was only 4 months later, aftershe had received an MRIscan, that it became clear thatthis young woman had something much more serious:She had subdural hematomas (areas of bleeding) onboth sides of her brain (see Fukutake et aI., 2000).
The thrill-ride-seeking public is always hungry fornew and more extreme rides, and the amusement parkindustry has responded accordingly. In 2001, the fastestroller coaster rides were the Tower ofTerror in Queens-land, Australia, and Superman, The Escape at Six FlagsMagic Mountain in Los Angeles, California. Both ridesalso have the greatest drops in the world 828 feet). More-over, technological advances are now allowing more andmore extreme rides to be developed. Some people worry,however, that such rides expose the body to dangerouslyhigh g-forces.
G-force is a measure of the acceleration of an objectdivided by the acceleration caused by gravity. In the UnitedStates, there are now at least 18 roller coasters that produceg-forces above 4.0 Gs. Taz's Tornado at Six Flags AstroWorldin Houston, Texas, is the most extreme at 6.5 Gs. Manyothers, including the Rock 'n' RollCoaster at Disney MGMStudios in Orlando, Florida, register 5.0 Gs.
The U.s. military has studied g-forces and found thatsustained (i.e., 4.2 seconds or longer) exposure to highg-forces leads to a loss of consciousness. Because peopledo not routinely black out when they ride roller coasters,
damage to the brain is indirect because it is produced eitherby inertial forces that cause the brain to come into violentcontact with the interior skull wall or by rotational forcesthat twist the brain mass relative to the brain stem. Notuncommonly, closed-head injury also causes diffuse neurondamage because of the inertial force. In other words, therapid movement of the rigid cranium is stopped on contactwith an unyielding object. However, the softer brain tissuewithin keeps moving, and this has a shearing effect on nervefibers and their synaptic interconnections. As The WorldAround Us 15.5 indicates, riding roller coasters that generatehigh g-forces may also cause brain injury.
Can Thrill Rides CauseBrain Damage?
Exposure to high g-forces, such as those experienced on sometheme park rides, can cause neurological injury in someindividuals by creating small tears in delicate blood vessels inthe brain.
we can assume that most of the applied g-forces thatimpact riders occur for less time than this. Nonetheless,the g-forces created by extreme rides may cause more thanjust thrills. A review of the literature (see Braksiek &Roberts, 2002) suggests that a tiny minority of riders mayexperience neurological injury as a consequence of ridingroller coasters. Although the individual risk is slight, therotational and positional changes that the body experi-ences may create small tears in delicate blood vessels. Todate, there are 58 known cases of brain injuries from rollercoasters, nearly all of which have occurred since 1990(Markey, 2002). Although this risk may not be enough todissuade you from heading to a theme park the next timeyou want to have some fun, it is already prompting calls forgreater oversight of the industry and demands for enforce-able g-force standards.

Neuropsychologically significant head injuries usuallygive rise to immediate acute reactions such as uncon-sciousness and disruption of circulatory, metabolic, andneurotransmitter regulation. Normally, if a head injury issevere enough to result in unconsciousness, the personexperiences retrograde amnesia, or inability to recallevents immediately preceding the injury. Apparently, suchtrauma interferes with the brain's capacity to consolidateinto long-term storage the events that were still beingprocessed at the time of the trauma. As you learned earlier,anterograde amnesia (also called "post-traumatic amne-sia") is the inability to store effectively in memory eventsthat happen during variable periods of time after thetrauma. It is also frequently observed and is regarded bymany as a negative prognostic sign.
A person rendered unconscious by a head injury usu-ally passes through stages of stupor and confusion on theway to recovering clear consciousness. This recovery ofconsciousness may be complete in the course of minutes,or it may take hours or days. Following a severe injury andloss of consciousness, a person's pulse, temperature, bloodpressure, and important aspects of brain metabolism areall affected, and survival may be uncertain. In rare cases anindividual may live for extended periods of time withoutregaining consciousness in a condition known as coma.The duration of the coma is generally related to the sever-ity of the injury. If the patient survives, coma may be fol-lowed by delirium, marked by acute excitement anddisorientation and hallucinations. Gradually the confu-sion may clear up and the individual may regain contactwith reality. Individual courses of recovery are highly vari-able (Crepeau & Scherzer, 1993; Powell & Wilson, 1994).
Even when a TBI seems relatively mild and there is agood recovery, careful neuropsychological assessment mayreveal subtle residual impairment. This is well illustrated inthe following case.
A17-year-old girl was referred by her father for neuropsy-chiatric evaluation because of the many changes that hadbeen observed in her personality during the past 2 years.She had been an Astudent and had been involved in manyextracurricular activities during her sophomore year inhigh school. But now, as a senior, she was barely able tomaintain a Caverage, was "hanging around with the badkids," and was frequently using marijuana and alcohol. Acareful history revealed that 2 years before, her olderbrother had hit her in the forehead with a rake, whichstunned her but did not cause her to lose consciousness.Although she had a headache after the accident, no psy-chiatric or neurological follow-upwas pursued.
Neuropsychological testing at the time of evaluationrevealed a significant decline in intellectual functioningfrom her "preinjury" state. Testing revealed poor concen-tration, attention, memory, and reasoning abilities. Acad-emically, she was unable to "keep up" with the friendsshe had had before her injury.She began to socialize witha group of students who had little interest in academics,and she began to see herself as a rebel. When the neu-ropsychological test results were explained to the patientand her family as a consequence of the brain injury, sheand her family were able to understand the "defensive"reaction to her changed social behavior. (Adapted fromSilver et aI., 2002.)
Large numbers of relatively mild closed-head brainconcussions and contusions (bruises) occur every year as aresult of auto collisions, athletic injuries, falls, and othermishaps. Temporary loss of consciousness and postimpactconfusion are the most common and salient immediatesymptoms. Although there is controversy about whetherthese mild brain injuries produce significant long-standingsymptoms or impairments (Dikmen & Levin, 1993; Zasler,1993), a recent study has shown that older individuals andindividuals who have TEl share several changes in informa-tion-processing speed (Bashore & Ridderinkhof, 2002).
We are also learning something about the factors thatmay increase a person's susceptibility to having problemsafter a brain injury. One important risk factor appears tobe the presence of the APOE-E4 allele that we discussedearlier (Waters & Nicoll, 2005). In one study of boxers, thepresence of the APOE-E4 genetic risk factor was associatedwith more chronic neurological deficits (Jordan et aI.,1997). A study of patients being treated in a neurosurgicalunit found that APOE-E4 predicted patients doing morepoorly at 6-month follow-up. This was true even after con-trolling for such factors as severity of the initial injury(Teasdale et aI., 1997).
Perhaps the most famous historical example of trau-matic brain injury is the case of Phineas Gage, reported byDr. J. M. Harlow in 1868 (here reprinted from History ofPsychiatry, 1993, Vol. 4, pp. 271-281). Because it is of bothhistorical and descriptive significance, it merits our atten-tion. Incidentally, Gage's skull and the tamping iron thatdamaged it are on display at Harvard Medical School.
The accident occurred in Cavendish, Vermont, on the lineof the Rutland and Burlington Railroad, at that time beingbuilt, on the 13th of September, 1848, and was occa-

sioned by the premature explosion of a blast, when thisiron, known to blasters as a tamping iron, and which I nowshow you, was shot through the face and head.
The subject of it was Phineas P. Gage, a perfectlyhealthy, strong, and active young man, twenty-five yearsof age .... Gage was foreman of a gang of men employedin excavating rock, for the road way....
The missile entered by its pointed end, the left sideofthe face, immediately anterior to the angle of the lowerjaw, and passing obliquely upwards, and obliquely back-wards, emerged in the median line, at the back part of thefrontal bone, near the coronal suture ....
The iron which thus traversed the head, is round andrendered comparatively smooth by use, and is three feetseven inches in length, one and one fourth inches in itslargest diameter, and weighs thirteen and one fourthpounds ....
The patient was thrown upon his back by the explo-sion, and gave a few convulsive motions of the extremi-ties, but spoke in a few minutes. His men (with whom hewas a great favorite) took him in their arms and carriedhim to the road, only a few rods distant, and put him intoan ox cart, in which he rode, supported in a sitting pos-ture, fully three quarters of a mile to his hotel. He gotout of the cart himself, with a little assistance from hismen, and an hour afterwards (with what I could aid himby taking hold of his left arm) walked up a long flight ofstairs, and got upon the bed in the room where he wasdressed. He seemed perfectly conscious, but wasbecoming exhausted from the hemorrhage, which by
As Stuss and colleagues (1992) havenoted, Gage's persistent post-trauma difficul-ties are fairly characteristic for severe frontallobe damage; emotional dyscontrol and per-sonality alterations, including impairmentof self-reflective awareness, are often promi-nent features of behavior change due to thistype of injury. In general, however, personal-ity disturbances secondary to traumaticbrain injury are somewhat unpredictableowing to the varied structural pathology thatis usually involved in such injuries (Pri-gatano, 1992).
Prompt treatment of brain injury may pre-vent further damage, for example, whenpooled blood under pressure is removedfrom the skull. In many instances, includingsome that may initially be considered mild,immediate medical treatment may have to besupplemented by a long-range program ofreeducation and rehabilitation.
this time was quite profuse, the blood pouring from thelacerated sinus in the top of his head, and also findingits way into the stomach, which ejected it as often asevery fifteen or twenty minutes. He bore his sufferingswith firmness, and directed my attention to the hole inhis cheek, saying, "the iron entered there and passedthrough my head."
Some time later Dr. Harlow made the followingreport:
His physical health is good, and I am inclined to say thathe has recovered. Has no pain in head, but says it has aqueer feeling which he is not able to describe. Appliedfor his situation as foreman, but is undecided whetherto work or travel. His contractors, who regarded him asthe most efficient and capable foreman in their employprevious to his injury, considered the change in hismind so marked that they could not give him his placeagain. The equilibrium or balance, so to speak, betweenhis intellectual faculties and animal propensities,seems to have been destroyed. He is fitful, irreverent,indulging at times in the grossest profanity (which wasnot previously his custom), manifesting but little defer-ence for his fellows, impatient of restraint or advicewhen it conflicts with his desires, at times pertina-ciously obstinate, yet capricious and vacillating, devis-ing many plans of future operations, which are nosooner arranged than they are abandoned in turn forothers ... his mind is radically changed, so decidedlythat his friends and acquaintances said he was "nolonger Gage."
Though Phineas Gage survived when a tamping iron entered his face and shotthrough his head, his personality was altered such that his friends found that he was"no longer Gage."

This police officer received a gunshot head wound in the line ofduty and is participating in physical therapy to improve muscletone and function in his left arm.
Although many TBI patients show few residual effectsfrom their injury, particularly if they have experiencedonly a brief loss of consciousness, other patients sustaindefinite and long-lasting impairment. Common after-effects of moderate brain injury include chronicheadaches, anxiety, irritability, dizziness, easy fatigability,and impaired memory and concentration. Where the braindamage is extensive, a patient's general intellectual levelmay be markedly reduced, especially if he or she has suf-fered severe temporal lobe or parietal lobe lesions. Mostvictims have significant delays in returning to their occu-pations, and many are unable to return at all (Bennettet aI., 1997; Dikmen et aI., 1994; Goran et aI., 1997). Otherlosses of adult social role functioning are also common(Hallett et aI., 1994). Some 24 percent ofTBI cases, overall,develop post-traumatic epilepsy, presumably because ofthe growth of scar tissue in the brain. Seizures usuallydevelop within 2 years of the head injury. For decades aftera head injury, there is also an elevated risk of depression aswell as other disorders such as substance abuse, anxietydisorders, and personality disorders (Holsinger et a!., 2002;Koponen et aI., 2002).
In a minority of brain injury cases, dramatic personal-ity changes occur such as those described in the case of
Phineas Gage. Other kinds of personality changes includepassivity, loss of drive and spontaneity, agitation, anxiety,depression, and paranoid suspiciousness. Like cognitivechanges, the kinds of personality changes that emerge inseverely damaged people depend, in large measure, on thesite and extent of their injury (Prigatano, 1992). However,even though more than half the people who sustain TBIdevelop psychological symptoms, and even though allevi-ation of such symptoms can improve rehabilitation out-come, there are currently few studies of risk factors,pathogenesis, and treatment of these disturbances (Rao &Lyketsos,2002).
Children who undergo significant traumatic braininjury are more likely to be adversely affected the youngerthey are at the time of injury and the less language, fine-motor, and other competencies they have. This is becausebrain damage makes it harder to learn new skills andbecause young children have fewer developed skills to beginwith. The severity of their injury and the degree to whichtheir environment is accommodating also affect children'srecovery (Anderson et al., 1997; Taylor & Alden, 1997;Yeates et aI., 1997). When the injury is mild, most childrenemerge without lasting negative effects (Satz et al., 1997).
Treatment of traumatic brain injury beyond thepurely medical phase is often long, difficult, and expensive.It requires careful and continuing assessment of neuropsy-chological functioning and the design of interventionsintended to overcome the deficits that remain. Not surpris-ingly, people from many disciplines may become involved
;:.:"~Preci'ictors~f'?" ,':', "~./~ tlinical Outcome ',";,0, :after Traumatic:' ,';'. 'Prain Injury" '. ~., 'I <bi~~ A, q I'" ~'fd' ~ :-... '. ,
~ only a short period of unconsciousness orpost-traumatic anterograde amnesia,
~ minimal cognitive impairment,
~ a well-functioning preinjury personality,
~ higher educational attainment,
~ a stable preinjury work history,
~ motivation to recover or make the most ofresidual capacities,
~ a favorable life situation to which toreturn,
~ early intervention,
~ an appropriate program of rehabilitationand retraining.
Sources: Bennett et aI., 1997; Dikmen et aI., 1994; Diller &
Gordon, 1981; Mackay, 1994; MacMillan et aI., 2002,

including neurologists; psychologists and neuropsycholo-gists; occupational, physical, and speechllanguage thera-pists; cognitive rehabilitation specialists; and vocationaland recreational therapists. Often, a treatment goal is toprovide patients with new techniques to compensate forlosses that may be permanent (Bennett et a1., 1997). How-ever, research is now showing that patients with TBl mayalso benefit from treatment with donepezil, an acetyl-cholinesterase inhibitor widely used in the treatment ofAlzheimer's disease (Zhang et a1., 2004). Table 15.2 showssome of the variables that are associated with patients hav-ing a more favorable outcome after a traumatic brainInJury.
In ReVIew~ What is the link between the APOE-E4allele
and problems after head injury?~ What kinds of clinical problems are
associated with head injury in the short andlonger term?
~ What factors are associated with the degreeof disability after head injury?
Can Dietary Supplements EnhanceBrain Functioning?
7 t is an unfortunate fact that our memories getworse as we get older. In an effort to slow thisdecline (which may begin as young as age 30),many people are turning to dietary supplementsand herbal preparations. Herbs such as Ginkgo
biloba (which is derived from the leaves of the ginkgo tree)are widely used and have been part of traditional Chinesemedicine for centuries. Ginkgo is now approved as a treat-ment for dementia in Germany. But is there any scientificvalidity to the claims that are made?
Using meta-analysis to examine the results of over 50studies, Oken and colleagues (1998) concluded that patientswith Alzheimer's disease who received ginkgo performed bet-ter cognitively than patients who took placebo. In fact, themagnitude of the differences was comparable to that foundwhen patients take donepezil, a drug that is widely used totreat Alzheimer's disease. However, a more recent study thatwas both large and methodologically sound found thatpatients with mild to moderate dementia did not derive anyclinically meaningful benefits from taking ginkgo (van Dongenet al., 2000).
The most recent statement on this issue is a thoroughreview of the literature by Gold and his colleagues (2002).
They note that patients who have mild to moderate cognitiveimpairment and who take ginkgo tend to show modest butsignificant improvement in cognitive functioning when com-
pared to patients who take placebo. They also caution, how-ever, that very few animal studies have been conducted andthat the effects of ginkgo in younger people are still littleexplored. They conclude that ginkgo warrants further atten-tion from researchers but that it is not yet possible to say con-clusively whether ginkgo is helpful or not.
What about other supposed cognitive enhancers? Phos-phatatidylserine (PS) is getting a great deal of attention inItaly as a treatment for dementia and age-related memorydecline. One popular book even recommends it as a cure forpoor memory (Crook & Adderly, 1998). Reviewing the evi-dence, however, McDaniel et al. (2002) conclude that suchenthusiasm may be a little premature. Overall, the findingsare inconsistent, and the increases in cognitive functioning(to the extent that they exist) may be so slight that they mightnot even be noticeable to the people taking the supplement.The same caution is extended to claims made for the benefitsof choline, which is found in foods containing lethicin and isimportant for the production of the neurotransmitter acetyl-choline. Although they call for more rigorous research on theissue of these and other "brain-specific nutrients," McDanieland colleagues (2002) are not willing to conclude categori-cally that such supplements have no clinical value. As withGinkgo biloba, the positive findings that exist in the literatureare suggestive enough to encourage researchers to keepexploring this issue.

~ The DSM-IV-TR recognizes various cognitive ~ Genes playa major role in susceptibility to and riskdisorders including delirium, dementia, and for Alzheimer's disease. Genetic mutations of theamnestic disorder. Typically these disorders result APP,presenilin 1, and presenilin 2 genes arefrom transient or permanent damage to the brain. implicated in early-onset AD. The APOE-E4allele ofChronic neuropsychological disorders involve the the APOEgene is also a risk factor for AD.permanent loss of neural cells. ~ The characteristic neuropathology of Alzheimer's
~ There is no simple relationship between extent of disease involves cell loss, plaques, and neurofibrillary
brain damage and degree of impaired functioning. tangles. Plaques contain a sticky protein called "beta
Some people who have severe damage develop no amyloid." Neurofibrillary tangles contain abnormal
severe symptoms, whereas some with slight damage tau protein.
have extreme reactions. ~ Alzheimer's disease causes the destruction of cells
~ Although such inconsistencies are not completely that make acetylcholine, a neurotransmitter important
understood, it appears that an individual's premorbid for memory. Drug treatments for AD include
personality and life situation are important in cholinesterase inhibitors such as donepezil (Aricept).
determining his or her reactions to brain damage. The These drugs help stop ACh from being broken down
APOE-E4genetic allele is also important. and so make more of it available to the brain.
~ Amnestic disorders involve severe memory loss. The~ Delirium is a fluctuating condition common among most common cause of amnestic disorders is chronic
the elderly. It involves a state of awareness between alcohol abuse.wakefulness and stupor or coma. It is treated with
~ Head injuries can cause amnesia as well as otherneuroleptic medications and also withbenzodiazepines. cognitive impairments. Retrograde amnesia is
inability to recall events that preceded the trauma.~ Dementia involves a loss of function and of previously Anterograde amnesia is inability to remember things
acquired skills. It has a slow onset and a deteriorating that follow it.course. The most common cause of dementia is ~ Any comprehensive treatment approach for cognitiveAlzheimer's disease.
disorders should also involve caregivers, who are~ Age is a major risk factor for Alzheimer's disease as often under a great deal of stress and have difficulty
well as for other forms of dementia such as vascular coping. They may benefit from medications as well asdementia. from support groups.
amnestic syndrome (P. 549)
amyloid plaques (P. 541)
anterograde amnesia (P. 552)
APOE-E4allele (P. 545)
delirium (P. 538)
dementia (P. 539)
early-onset Alzheimer's disease(P. 544)
functional mental disorders (P. 533)
HIV-associated dementia (P. 548)
late-onset Alzheimer's disease(P. 545)
neurofibrillary tangles (P. 541)
organic mental disorders (P. 533)
retrograde amnesia (P. 552)
traumatic brain injury (TBI) (P. 550)
vascular dementia (VAD) (P. 549)