Embed Size (px)
Citation preview
Sports Med 2005; 35 (8): 685-715REVIEW ARTICLE 0112-1642/05/0008-0685/$34.95/0
2005 Adis Data Information BV. All rights reserved.
Central Nervous System Injuries inSport and RecreationA Systematic Review
Cory Toth,1 Stephen McNeil1 and Thomas Feasby2
1 Department of Clinical Neurosciences, University of Calgary, Calgary, Alberta, Canada2 Department of Medicine, University of Alberta and Capital Health, Edmonton,
Alberta, Canada
ContentsAbstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 686
1. Auto Racing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6872. Baseball . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 689
2.1 Head Injuries in Baseball . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6902.2 Spinal Cord Injuries in Baseball . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 691
3. Basketball . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6914. Bicycling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6925. Boxing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 693
5.1 Acute Neurological Injury in Boxing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6935.2 Chronic Neurological Injury in Boxing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6945.3 Spinal Cord Injuries in Boxing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 695
6. Cheerleading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6957. Cricket . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6958. Darts and Lawn Darts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6969. Diving . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 696
10. Equestrian and Horse Racing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69610.1 Head Injuries in Equestrian Sports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69610.2 Spinal Injuries in Equestrian Participants and Jockeys . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 697
11. Field Hockey and Lacrosse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69712. Football . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 697
12.1 Concussion in Football . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69712.2 Second Impact Syndrome in Football . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69912.3 Severe Head Injuries in Football . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69912.4 Spinal Injuries in Football . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 700
13. Golf . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70014. Gymnastics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 700
14.1 The Trampoline in Gymnastics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70115. Hang-Gliding and Paragliding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70116. Hockey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 701
16.1 Head Injuries in Hockey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70216.2 Spinal Injuries in Hockey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 702
17. In-Line Skating, Roller Hockey and Skateboarding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70318. Judo, Karate, Kickboxing and Related Sports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70319. Motorcycling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70320. Mountain Climbing and Hiking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70421. Rodeo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 704

686 Toth et al.
22. Rugby and Australian Rules Football . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70422.1 Head Injuries in Rugby and Australian Rules Football . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70422.2 Spinal Injuries in Rugby and Australian Rules Football . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 705
23. Scuba Diving . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70524. Skiing, Snowboarding, Snowblading, Sledding, Skating and Ski Jumping . . . . . . . . . . . . . . . . . . . . . . 705
24.1 Spinal Injuries in Winter Sports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70524.2 Head Injuries in Winter Sports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70624.3 Injuries in Other Winter Sports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 707
25. Snowmobiling and All-Terrain Vehicle Riding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70726. Soccer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 708
26.1 Head Injuries in Soccer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70827. Volleyball . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70928. Wrestling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70929. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 709
Many sports have been associated with a variety of neurological injuriesAbstractaffecting the central nervous system (CNS), with some injuries specific to thatsport. A systematic review of sport-specific CNS injuries has not been attemptedpreviously, and could assist in the understanding of morbidity and mortalityassociated with particular sporting activities, either professional or amateur. Asystematic review of the literature was performed using PubMed (1965–2003)examining all known sports and a range of possible CNS injuries attributable tothat sport. Numerous sporting activities (45) have associated CNS injuries asreported within the literature. The sports most commonly associated with CNSinjuries are: football, boxing, hockey, use of a trampoline, and various winteractivities. A number of sporting activities are associated with unique CNS injuriesor injury-related diseases such as heat stroke in auto racing, vertebral arterydissection in the martial arts, and dementia pugilistica in boxing. Neurologicalinjuries of the CNS due to sport comprise a wide collection of maladies that areimportant for the neurologist, neurosurgeon, orthopaedic surgeon, physiatrist,sports medicine doctor, athletic trainer and general physician to recognise.
Neurological injuries of either the peripheral or We have performed a systematic review of thescientific peer-reviewed literature in order to obtaincentral nervous system (CNS) are varied and numer-an exhaustive description of injuries to the CNSous depending on the nature of the sporting activity,associated with specific sporting activities. Cat-age of the participants and intensity of play. Theegorisation has been performed by sorting injuriestype of sport may vary from recreational games suchby sporting type. Whenever possible, commentsas lawn darts, individual sports such as skiing orabout pathogenesis and prognosis have been includ-
snowboarding, and team sports such as professional ed, as well as recommendations for diagnostic andfootball. The physician may be confronted with therapeutic interventions for specific sports-relatedsymptoms and signs reflecting injury to the brain injury. Categorisation has also been performed us-and spinal cord. Recognition of specific injuries and ing specific injuries and their relationship to multi-their relationship to specific sporting activities may ple forms of sporting events.assist physicians with the rapidity of diagnosis and A MEDLINE search was performed using thepossible therapy. website of the National Library of Medicine
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

CNS Injuries in Sport and Recreation 687
Table I. List of MeSH and non-MeSH terms used
MeSH terms
Athletic injuries; badminton; baseball; baseballs; basketball; boxing; brachial plexus; brain concussion; brain injuries; brain injury,ischaemic; central cord injury syndrome; cerebral concussion; chronic brain injury; coma, post-head injury; compression neuropathy;concussion, intermediate; concussion, mild; concussion, severe; post-concussion syndrome; crushing skull injury; dancing; diving;entrapment neuropathy; epidural haematoma; equestrian; facial nerve injuries; facial neuropathy, traumatic; football; footballs; golf; headinjuries, closed; head injuries, penetrating; head injury, blunt; head injury, minor; head injury, nonpenetrating; head injury, open; headinjury, penetrating; head injury, superficial; hockey; field hockey; ice hockey; injuries, sports; injury, brain, chronic; brain ischaemia;injury, brain, traumatic; intracranial haemorrhage; ischaemic brain injury; central cord syndrome; lacrosse; lumbar plexus; marathon;mononeuropathies; open head injury; post-concussion symptoms; post-head injury coma; craniocerebral trauma; racquet sports; racketsports; snow sports; sports; sports equipment; sports medicine; medicine, sports; racquetball; rugby; skating; skiing; snowblading;snowboarding; soccer; spinal cord injuries; sports injuries; squash; subdural haematoma; superficial head injury; TBI (traumatic braininjury); brain injury, chronic; tennis; traumatic brain injury; wounds and injuries; wounds and injury; wounds, injury; wrestling
Non-MeSH terms
Anterior interosseus nerve; archery; auto racing; axillary nerve; ballet dancing; cheerleading; common peroneal nerve; femoral nerve;figure skating; gluteal nerve; median nerve; musculocutaneous nerve; nerve injury; neurological injury; paraplegia; peroneal nerve;plexopathy; plexus injury; posterior interosseus nerve; quadriplegia; radial nerve; radiculopathy; sciatic nerve; speed skating; spinal cordcontusion; superficial peroneal nerve; sural nerve; tibial nerve; ulnar nerve
(‘PubMed’) to examine the literature for all possible anatomical levels associated with neurological inju-scientific papers discussing sports and neurological ry due to individual sports. Definitions of medicalinjuries published between the years of 1966–2003. terms used in this review are listed in table VI.MeSH search terms and non-MeSH terms used in- A total of 462 abstracts were found using thecluded all combinations as listed in table I. All defined search criteria. Examination of referencesabstracts found using these MeSH terms were ex- within the initially found manuscripts revealed anamined. Articles were included for consideration in additional 198 articles to be obtained. The finalthis review if they met the following criteria: (i) reference list consisted of 253 papers or books.papers describing a series of injuries, including References were obtained in full in 68% of cases,those of a neurological basis, within one sport or and abstracts were used in remaining cases whereactivity (those sources reporting injury to the CNS the journal could not be located or was in a foreignwere recorded); and (ii) papers describing one par- language, resulting in the abstract being used forticular form of neurological injury of the CNS with- information. Sporting activities associated with neu-in a group of sports. rological injury are listed in alphabetical order, spe-
cific by sport, within this article. The majority of theWhenever possible, full publications were ob-references located were of individual case reports,tained in place of abstracts. References found withinor of a small series of similar injuries within onethe obtained papers, which met the above criteria,sporting activity.were also used to obtain further relevant papers,
textbooks, or scientific presentations for data to be1. Auto Racingused within this review. In situations where the
association between a sporting activity and injurywas questionable, the article was not included with- Although frequently noted to be a dangerousin this review. Categorisation was performed by sporting event, auto racing is conspicuous by theeach individual sport or activity. Injuries of the CNS paucity of reports in the medical literature as a causeare organised by sport within table II, and are or- of neurological injury. However, at the Indianapolisganised anatomically in table III. The prevalence Raceway Park, a retrospective study over six sea-rates of all injuries by sport when available is pro- sons identified neurological injuries to drivers dur-vided in table IV. Table V provides estimated inci- ing 61 open-wheel racing events, with four driversdence rates for concussion within individual sports. requiring admission to hospital and two to intensiveFigure 1 and figure 2 present a pictorial display of care for head injuries.[1] One report noted head trau-
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
688 Toth et al.
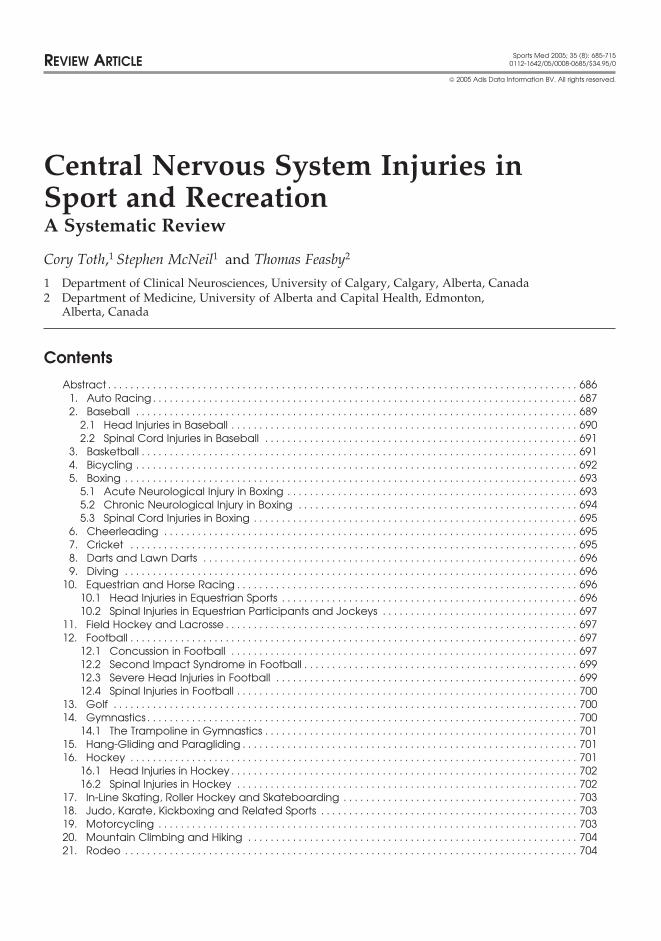
Table II. Locations of neurological injuries by sport
Sport Neurological injuries
Auto racing Closed head injuries; open head injuries; intracranial haemorrhage; diffuse axonalbrain injury; heat stroke; spinal cord injuries; cervical cord injury
Baseball Mild traumatic brain injury; epidural haematoma; cervical spinal cord injury;concussion
Bicycling Concussion
Bodybuilding/weightlifting Benign exertional headache
Boxing Concussion; acute subdural haematoma; chronic traumatic brain injury; dementiapugilistica; cervical spinal cord injury
Cheerleading Concussion; closed head injury; cervical spinal cord injury
Cricket Intracranial haemorrhage; closed head injury
Darts Open head injury
Diving/scuba diving Cervical spinal cord injury; carotid artery dissection with stroke; cerebral arterialoxygen bubble emboli with stroke and encephalopathy; cerebral infarction related tocardiopulmonary shunt and paradoxical thromboembolism; skip breathing headache;‘goggles headache’
Equestrian/horse racing Closed head injury; concussion; intracerebral haemorrhage; cervical spinal cordinjury
Field hockey/lacrosse Closed head injury; concussion; epidural haematoma
Figure skating Concussion
Football Concussion; closed head injury; post-traumatic headache; chronic traumatic braininjury; subdural haematoma; cervical spinal cord injury; transient quadriparesis
Golf Vertebral artery dissection with stroke; ‘yips’; closed head injury (due to golf carts,golf club or golf ball); spinal cord injury (due to golf cart accidents); thoracic spinalcord injury due to osteoporotic fracture of vertebra or thoracic disc prolapse
Gymnastics Cervical spinal cord injury; spinal cord injury (trampoline and aeroball); vertebralartery dissection with stroke (trampoline)
Hang-gliding/paragliding Spinal cord injury
Hockey Concussion; epidural haematoma; subdural haematoma; subarachnoid haemorrhage;spinal cord injury
In-line skating, rollerskating and skateboarding Closed head injury
Judo, karate and kickboxing Vertebral artery, carotid artery dissection with stroke; cervical spinal cord injury dueto disc herniation; closed head injury; subdural haematoma; intracranialhaemorrhages
Motorcycling Closed head injury; intracranial haemorrhages; spinal cord injury
Mountain climbing, hiking Acute mountain sickness with headache; cerebral oedema syndrome due to highelevation
Rodeo Concussion; closed head injury
Rubgy Cervical spinal mild traumatic brain injury cord injury; transient quadriparesis;concussion
Skiing, snowboarding, snowblading, sledding Spinal cord injury – thoracolumbar (skiing); cervical (snowboarding); cervical spinaland ski jumping epidural haematoma; closed head injury; concussion; intracranial haemorrhages
Snowmobiling and all-terrain vehicle riding Closed head injury; spinal cord injury
Soccer Concussion; closed head injury; intracranial haemorrhages – epidural haematoma;acute subdural haematoma; chronic subdural haematoma; basal skull fracture withmeningitis development; mild traumatic brain injury
Speed skating Concussion
Volleyball Concussion
Wrestling Mild traumatic brain injury; concussion; closed head injury; spinal cord injury;transient quadriparesis; vertebral artery territory stroke due to prolonged wrestlinghold
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
CNS Injuries in Sport and Recreation 689
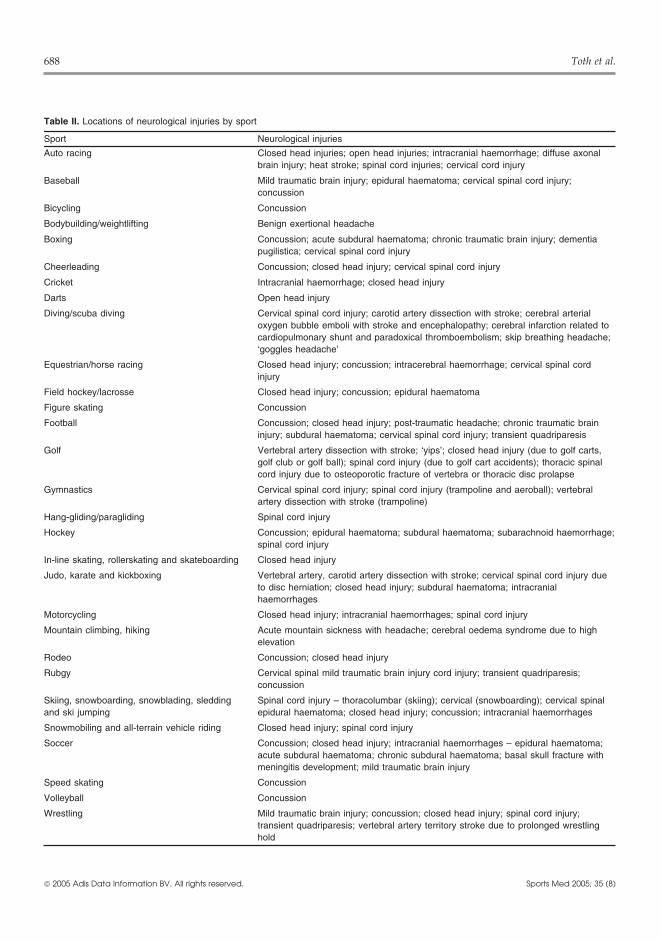
Table III. Neurological injuries of the central nervous system as a result of sport. Classified by anatomical location and injury type
Injury type Sports
Spinal cord
Any location Auto racing; golf; gymnastics; hang-gliding/paragliding; hockey; snowmobiling; all-terrain vehicle riding; wrestling
Cervical Auto racing; baseball; boxing; cheerleading; diving; equestrian; football; gymnastics;rubgy; snowboarding
Thoracic Skiing
Lumbar Skiing
Transient quadriparesis Football; rubgy; wrestling
Epidural haematoma Snowboarding
Brainstem
Stroke Golf; gymnastics; judo, karate and kickboxing; wrestling
Cerebrum
Concussion Auto racing; baseball; bicycling; boxing; cheerleading; equestrian; field hockey/lacrosse; figure skating; football; hockey; rodeo; rubgy; skiing; snowblading;snowboarding; soccer; speed skating; volleyball; wrestling
Closed head injury Auto racing; boxing; cheerleading; cricket; equestrian; field hockey/lacrosse; football;golf; in-line skating, rollerskating and skateboarding; judo, karate and kickboxing;motorcycling; rodeo; rubgy; skiing; snowboarding; snowmobiling; all-terrain vehicleriding; soccer; wrestling
Open head injury Auto racing; darts
Stroke Diving; scuba diving; judo, karate and kickboxing
Subdural haematoma Auto racing; boxing; equestrian; football; hockey; judo, karate and kickboxing;motorcycling; skiing; snowboarding; soccer
Epidural haematoma Auto racing; baseball; cricket; equestrian; field hockey/lacrosse; hockey; soccer
Subarachnoid haemorrhage Hockey; judo, karate and kickboxing; motorcycling; skiing; snowboarding
Diffuse axonal injury Auto racing
Cerebral oedema Mountain climbing
Chronic traumatic brain injury Boxing; football
Dementia pugilistica Boxing
Heat stroke Auto racing
Headache Bodybuilding/weightlifting; scuba diving; football; mountain climbing
Movement disorder Golf
ma in 29% of all injuries in professional auto racing, drivers, most commonly occurring with a vehicularrollover and usually leading lead to cervical spine orwith open head injuries comprising only 5%.[2,3]
spinal cord injury (SCI).[3]Closed head injuries have rarely included intracrani-al haemorrhages, and more commonly were de-
2. Baseballscribed as diffuse axonal injury.[2] Exposure to emis-sions of carbon monoxide and vehicle fires were Most CNS injuries in baseball are acute, notstudied in race-car drivers using a breath analyser; chronic. Acute injury rates and frequency of injuryan increase in carboxyhaemoglobin concentrations per team per season (FITS) are reported in tableduring the competition event was identified in all IV.[6,7] In children aged 7–13 years, more injuriesrace-car drivers, although no correlation with carbon occur during baseball games rather than during prac-monoxide level and driver symptomatology was tice.[7] Little-league player injuries are ball-relateddemonstrated.[4] Heat stroke has been rarely associ- in 46% and collision-related in 27%.[6] The mostated with auto racing.[5] Spinal injuries comprise frequent mechanism in little-league players was be-20% of injuries experienced by professional auto ing hit by the ball, representing 62% of acute inju-
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
690 Toth et al.
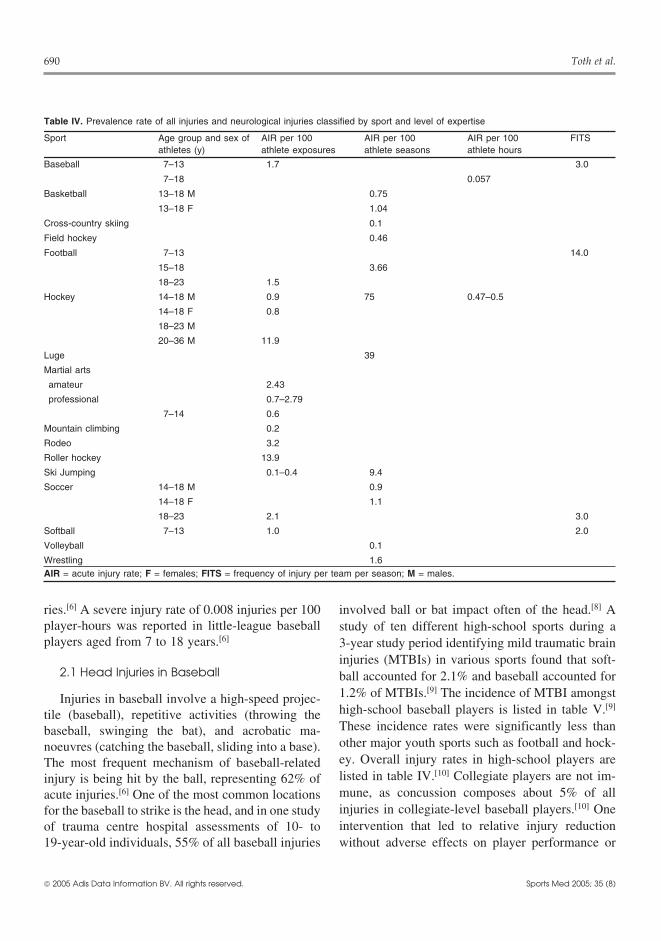
Table IV. Prevalence rate of all injuries and neurological injuries classified by sport and level of expertise
Sport Age group and sex of AIR per 100 AIR per 100 AIR per 100 FITSathletes (y) athlete exposures athlete seasons athlete hours
Baseball 7–13 1.7 3.0
7–18 0.057
Basketball 13–18 M 0.75
13–18 F 1.04
Cross-country skiing 0.1
Field hockey 0.46
Football 7–13 14.0
15–18 3.66
18–23 1.5
Hockey 14–18 M 0.9 75 0.47–0.5
14–18 F 0.8
18–23 M
20–36 M 11.9
Luge 39
Martial arts
amateur 2.43
professional 0.7–2.79
7–14 0.6
Mountain climbing 0.2
Rodeo 3.2
Roller hockey 13.9
Ski Jumping 0.1–0.4 9.4
Soccer 14–18 M 0.9
14–18 F 1.1
18–23 2.1 3.0
Softball 7–13 1.0 2.0
Volleyball 0.1
Wrestling 1.6AIR = acute injury rate; F = females; FITS = frequency of injury per team per season; M = males.
ries.[6] A severe injury rate of 0.008 injuries per 100 involved ball or bat impact often of the head.[8] Aplayer-hours was reported in little-league baseball study of ten different high-school sports during aplayers aged from 7 to 18 years.[6] 3-year study period identifying mild traumatic brain
injuries (MTBIs) in various sports found that soft-2.1 Head Injuries in Baseball ball accounted for 2.1% and baseball accounted for
1.2% of MTBIs.[9] The incidence of MTBI amongstInjuries in baseball involve a high-speed projec-high-school baseball players is listed in table V.[9]
tile (baseball), repetitive activities (throwing theThese incidence rates were significantly less thanbaseball, swinging the bat), and acrobatic ma-other major youth sports such as football and hock-noeuvres (catching the baseball, sliding into a base).ey. Overall injury rates in high-school players areThe most frequent mechanism of baseball-relatedlisted in table IV.[10] Collegiate players are not im-injury is being hit by the ball, representing 62% ofmune, as concussion composes about 5% of allacute injuries.[6] One of the most common locationsinjuries in collegiate-level baseball players.[10] Onefor the baseball to strike is the head, and in one studyintervention that led to relative injury reductionof trauma centre hospital assessments of 10- to
19-year-old individuals, 55% of all baseball injuries without adverse effects on player performance or
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
CNS Injuries in Sport and Recreation 691
player acceptability was the use of a face guard on old male baseball player after a hyperextension inju-ry.[14]the batter’s helmet in one non-randomised study.[11]
More serious intracranial injuries within the sport 3. Basketballof baseball are rare, with one report of epidural
While basketball injuries are relatively common,haematoma secondary to a baseball bat striking thereports of CNS injuries are conspicuously absenthead.[12] A retrospective study of baseball bat-relat-throughout the medical literature. The incidence ofed injuries revealed craniocerebral injury being theMTBI in high-school basketball players is lowermost frequent form of injury and most frequentthan other organised sports such as football, wres-cause of death. One study of victims struck in thetling and soccer. Acute injury rates are listed in tablehead showed that 26% sustained an intracranialIV.[9] Women collegiate basketball players are sub-haemorrhage.[13]
ject to concussion comprising 9% of all injuriesrelative to only 5% in male collegiate basketball
2.2 Spinal Cord Injuries in Baseball players.[8] In one study of trauma centre hospitals,basketball injuries capable of causing head injuries
Even rarer than severe head injury in baseball is in 10- to 19-year-old individuals were related toSCI in baseball players, with a single report of acute striking the basketball pole or rim, or being struckcentral cervical spinal cord syndrome in a 32-year- by a falling pole or backboard.[10]
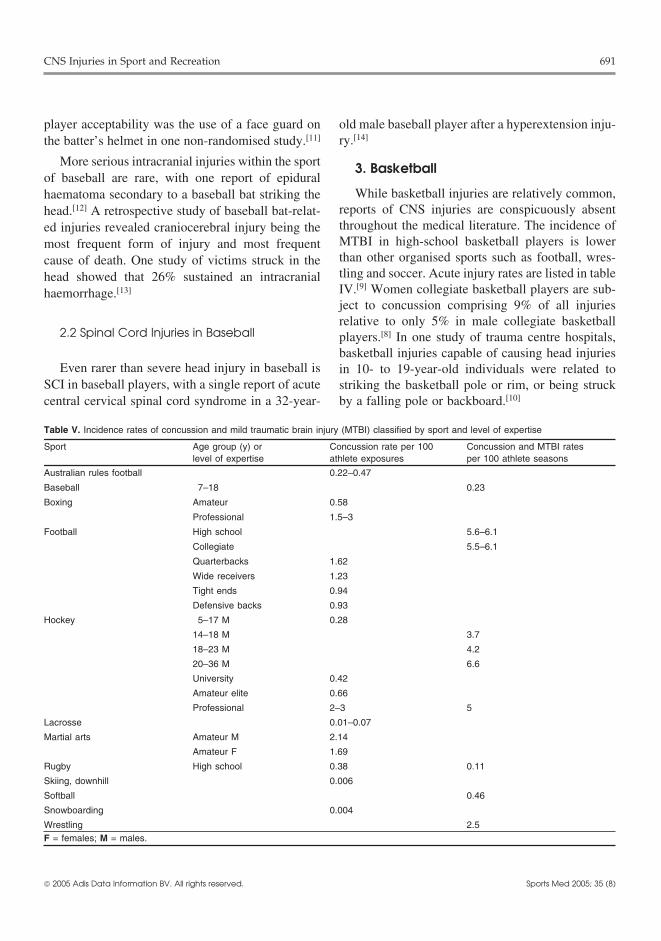
Table V. Incidence rates of concussion and mild traumatic brain injury (MTBI) classified by sport and level of expertise
Sport Age group (y) or Concussion rate per 100 Concussion and MTBI rateslevel of expertise athlete exposures per 100 athlete seasons
Australian rules football 0.22–0.47
Baseball 7–18 0.23
Boxing Amateur 0.58
Professional 1.5–3
Football High school 5.6–6.1
Collegiate 5.5–6.1
Quarterbacks 1.62
Wide receivers 1.23
Tight ends 0.94
Defensive backs 0.93
Hockey 5–17 M 0.28
14–18 M 3.7
18–23 M 4.2
20–36 M 6.6
University 0.42
Amateur elite 0.66
Professional 2–3 5
Lacrosse 0.01–0.07
Martial arts Amateur M 2.14
Amateur F 1.69
Rugby High school 0.38 0.11
Skiing, downhill 0.006
Softball 0.46
Snowboarding 0.004
Wrestling 2.5F = females; M = males.
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

692 Toth et al.
Table VI. Medical terms and definitions used
Medical term Definition
Closed head injury A head injury with continuity of skull and mucous membranes maintained
Concussion Head injury that manifests with impaired consciousness, amnesia, change in mentation, withassociated features of headache, vertigo, nausea, tinnitus, and varying times until resolution ofsymptoms
Decompression illness Known as the ‘bends’, this results from nitrogen bubbles forming within the bloodstream,impairing tissue oxygen supplies, including that of the brain and spinal cord
Dementia pugilistica A chronic form of dementia due to recurrent chronic head trauma as commonly occurs inboxers. In addition to loss of frontal lobe functioning and impaired memory and other higherfunctions, patients often also display problems in motor and coordination functioning. Alsoreferred to as chronic traumatic brain injury
Diffuse axonal injury The shearing (tearing) of the brain’s long connecting nerve fibres (axons) that can occur withsevere brain injury
Epidural haematoma A haemorrhage within the epidural space within the skull, often due to arterial rupture and canbe life threatening
Extradural haematoma A haemorrhage that occurs over the head but outside of the skull
Heat stroke Severe illness due to exposure to high temperature, often during exertion, which can lead tofever, lack of sweating, unconsciousness, headache, and even vascular collapse and coma
Intracranial haemorrhage Bleeding inside the cavity of the skull, including bleeding into epidural, subdural, subarachnoid,intraventricular spaces, as well as within the brain parenchyma itself
L’hermitte’s symptom A sensation similar to an electrical shock radiating from the back of the head down the spineas the neck is bent forward.
Locked-in syndrome A state of wakefulness with paralysis limited to the use of eye movements for communication
Mild traumatic brain injury (MTBI) Traumatic-induced physiological disruption of brain function, manifested by at least one of thefollowing: any disturbed consciousness; amnesia pre- or post-incident; altered mental state;and focal neurological deficit(s) that may or may not be transient. Note that the definition ofMTBI is difficult to discriminate from concussion and many authors see the two entities as one
Myelopathy A disease that affects the spinal cord
Open head injury A head injury with a loss of continuity of scalp and/or mucous membranes, leading tocommunication between the intracranial cavity and the exterior
Paraplegia Paralysis of the lower half of the body
Paraparesis Incomplete paralysis of the lower half of the body
Post-concussion syndrome Disorder that presents after concussion with a variety of symptoms including, but not limited to,headache, dizziness, fatigue and changes in personality
Quadriplegia Paralysis of the majority of the body including all four limbs
Quadriparesis Incomplete paralysis of the majority of the body, including all four limbs
Radicular Referring to the spinal roots leaving the spinal cord, often used to describe a form of lightning-like pains that radiate into a body part, often a limb
Subdural haematoma A haemorrhage that occurs within the subdural space within the skull, often due to venousrupture and less commonly life threatening than epidural haematoma
4. Bicycling Although anecdotal suggestions of bicycle acci-dents being more common with BMX-style bikeshave occurred, the incidence of injuries comparedRecreational and competitive cycling, includingwith non-BMX bikes appears to be similar.[15] InBMX, road and off-road cycling, are associated withfact, BMX riders had a lower proportion of seriousa wide range of neurological injuries affecting theinjuries than bicycle racers, including fewer headperipheral nervous system, and a few injuries of theinjuries. The majority of accidents occurring inCNS. Incidence rates for CNS injuries as a result ofBMX riders are related to performing stunts or tocycling accidents are largely unknown; however,poor cycling technique.[15] The proportion of con-studies involving use of bicycle helmets are plenti-
ful. cussions due to BMX riding is approximately
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
CNS Injuries in Sport and Recreation 693
7%.[16] Although most injuries occurring in off-roadbicycle racing are musculoskeletal, a small inci-dence of concussion (<1%) was reported, about 40%less than other forms of cycling.[17,18] This low inci-dence may relate to a significantly higher rate ofhelmet usage in off-road cyclists.[18] Interestingly,women appeared to be much more likely than mento sustain a serious injury while off-road cycling.[19]
Head injuries as a result of bicycle riding havebecome a hot political topic, with many cities inCanada and selected districts within the US, leadingto the institution of mandatory bicycle helmet laws.In one Canadian study, helmet use was associatedwith less likelihood of hospital admission followinginjury, a lower incidence of head and facial injury,and lower incidence of concussion.[20] An Americanstudy also found that the use of bicycle safety hel-mets for children led to an 88% risk reduction inintracranial injury and prevented occurrence of skullfractures and possibly death due to head injuries,both of which occurred in helmet-less children.[21]
Bicycling accidents have been associated with
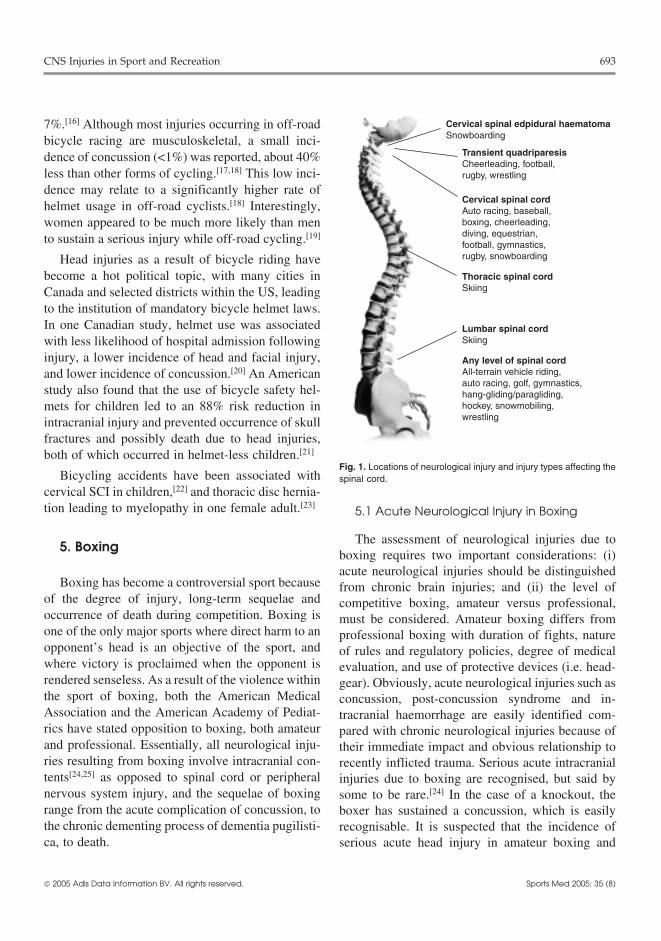
Cervical spinal edpidural haematomaSnowboarding
Cervical spinal cordAuto racing, baseball,boxing, cheerleading,diving, equestrian,football, gymnastics,rugby, snowboarding
Transient quadriparesisCheerleading, football,rugby, wrestling
Thoracic spinal cordSkiing
Lumbar spinal cordSkiing
Any level of spinal cordAll-terrain vehicle riding,auto racing, golf, gymnastics,hang-gliding/paragliding,hockey, snowmobiling,wrestling
Fig. 1. Locations of neurological injury and injury types affecting thespinal cord.
cervical SCI in children,[22] and thoracic disc hernia-tion leading to myelopathy in one female adult.[23]
5.1 Acute Neurological Injury in Boxing
The assessment of neurological injuries due to5. Boxingboxing requires two important considerations: (i)acute neurological injuries should be distinguished
Boxing has become a controversial sport because from chronic brain injuries; and (ii) the level ofof the degree of injury, long-term sequelae and competitive boxing, amateur versus professional,occurrence of death during competition. Boxing is must be considered. Amateur boxing differs fromone of the only major sports where direct harm to an professional boxing with duration of fights, natureopponent’s head is an objective of the sport, and of rules and regulatory policies, degree of medicalwhere victory is proclaimed when the opponent is evaluation, and use of protective devices (i.e. head-rendered senseless. As a result of the violence within gear). Obviously, acute neurological injuries such asthe sport of boxing, both the American Medical concussion, post-concussion syndrome and in-Association and the American Academy of Pediat- tracranial haemorrhage are easily identified com-rics have stated opposition to boxing, both amateur pared with chronic neurological injuries because ofand professional. Essentially, all neurological inju- their immediate impact and obvious relationship tories resulting from boxing involve intracranial con- recently inflicted trauma. Serious acute intracranialtents[24,25] as opposed to spinal cord or peripheral injuries due to boxing are recognised, but said bynervous system injury, and the sequelae of boxing some to be rare.[24] In the case of a knockout, therange from the acute complication of concussion, to boxer has sustained a concussion, which is easilythe chronic dementing process of dementia pugilisti- recognisable. It is suspected that the incidence ofca, to death. serious acute head injury in amateur boxing and
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

694 Toth et al.
StrokeDiving
Scuba divingJudo/karate/kickboxing
Intra-cerebral or sub-arachnoid
haemorrhageHockey
Judo/karate/kickboxingMotorcycling
SkiingSnowboarding
Brainstem strokeGolf
GymnasticsJudo/karate/kickboxing
Wrestling
Open head injuryAuto racing
Darts
Epidural haematomaAuto racingBaseballCricketEquestrianField hockeyHockeyLacrosseSoccer
Subdural haematomaAuto racingBoxingEquestrianFootballHockeyJudo/karate/kickboxingMotorcyclingSkiingSnowboardingSoccer
Concussion/closed head injuryAll terrain vehicle riding, auto racing, baseball, bicycling, boxing,cheerleading, cricket, equestrian, field hockey/lacrosse, figure skating, football, golf, in-line skating, judo/karate/kickboxing, motorcycling, rodeo, rugby, skiing, snowboarding, snowmobiling, soccer, speed skating, wrestling
Fig. 2. Locations of neurological injury and injury types affecting intracranial contents.
noncompetitive boxing is lower than in the profes- 5.2 Chronic Neurological Injury in Boxingsional ranks, perhaps due to more regulation andreporting of injuries.[26] In one study of instructional Chronic neurological injuries from boxing tendboxing in US Marine Corps, only one serious head to have an insidious onset and often present andinjury per 60 000 participants occurred, comprising continue to progress after cessation of boxing.[31] Ofonly 0.3% of all boxing-related injuries during the ex-professional boxers who had participated in thestudy period.[27] Estimated concussion incidence sport for at least 3 years, 17% were found to have
clinical evidence of CNS deficit felt to be attributa-rates in amateur and professional boxing are listed inble to boxing.[32] Measures of more chronic effectstable V.[25,28] Over more recent years, concussionof boxing and neuropsychological and cognitivehas gained more recognition as a medical conditioneffects have been studied many times with varyingrequiring attention following trauma,[29] but at-results. A lack of laboratory abnormalities in boxerstempts to quantify the number of concussions inrelative to other athletes, including testing with elec-boxing have not been published. The incidence oftroencephalography (EEG) and brainstem auditory-
intracranial haemorrhage in boxers is unknown, butevoked responses, has also been noted.[33] In a study
acute subdural haematomas are probably the leading of former Swedish amateur boxers, a single taskcause of boxing-related mortality.[24] One study ex- (finger-tapping) was identified as having inferioramined the acute cognitive effects of concussion in performance relative to other athletes.[34] The mostmilitary cadet boxers compared with baseline test- severe abnormalities of physical examination can being – computerised cognitive assessment demon- seen in the most severe cases of post-boxing en-strated inferior performances on simple reaction cephalopathy, and include cerebellar, extrapyrami-time and continuous performance tests.[30] dal and intellectual impairments – this has been
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

CNS Injuries in Sport and Recreation 695
termed dementia pugilistica.[32] Other clinical fea- Alzheimer’s disease brains. Thus, recurrent braininjury in boxers may activate similar pathologicaltures in patients with dementia pugilistica have in-mechanisms as those in Alzheimer’s disease.[44]cluded tremor, dysarthria, and psychiatric changesMeasurement of the glial protein S-100B in serumsuch as explosive behaviour, and paranoid and jeal-before and after amateur boxing competitions hasous delusions.[35] Risk factors for persistent CNSdemonstrated an increase in S-100B protein afterdeficit after boxing included participation in profes-boxing. The increase in S-100B protein levels,sional boxing as opposed to amateur boxing, thewhich has a postulated relationship to cognitivenumber of punches taken, and a lack of ‘scientificdeficits, correlated significantly with the numberability’.[36] In contrast, a small number of amateurand severity of the strikes to the head.[45]boxers demonstrated no abnormalities on detailed
neurological examinations and magnetic resonance5.3 Spinal Cord Injuries in Boxingimaging (MRI) of the brain.[37] While amateur box-
ers and controls do not demonstrate abnormalities inCervical spine fractures are rare in boxing, yetregional cerebral blood flow (rCBF) with inhalation
potentially catastrophic. A transient SCI occurred inof 133-xenon, professional boxers demonstrate dif-a young male boxer who had an os odontoideum,fuse reductions in rCBF, especially in the frontocen-which may have placed him at risk for such antral regions.[38] Perhaps this reduction in perfusioninjury.[46] Another boxer sustained a C6 vertebralmay relate to chronic brain injury over regions ofbody fracture and quadriplegia during a boxingbrain felt to be affected in dementia pugilistica andmatch.[47]
recurrent concussion.[32]
Pathological findings in former boxers are in- 6. Cheerleadingtriguing. Neuropathological abnormalities docu-mented in ex-professional boxers include scarring of Although cheerleading would not initially be ex-cerebellar folia with loss of cerebellar Purkinje cells, pected to have association with CNS injuries, manydegeneration of the substantia nigra, presence of high risk manoeuvres such as high team throws andneurofibrillary tangles in limbic grey matter and daring aerial drills have led to accidents.[48] Therecavum septum pellucidum.[39,40] In contrast, a study are no estimates for incidence of injuries in cheer-of CT scans in amateur boxers did not identify an leaders. Major injuries have included cervical frac-increased incidence of cavum septum pel- tures or cervical ligament injuries that have led tolucidum.[41] Neurofibrillary tangles in dementia paralysis, as well as spinal cord contusions withpugilistica brains are concentrated in superficial ne- transient or resolving symptoms. Also, severe headocortical layers, in contrast to Alzheimer’s disease, injuries including skull fractures, haematomas orwhere they predominate in deep layers.[42] Possible cerebral oedema have occurred following accidents.markers for neurological deficit in boxers have been Mortality at the time of or within days of a headexamined in recent years. Professional boxers were injury has occurred in two cheerleaders.[48]
scored on the Chronic Brain Injury (CBI) scale, withgreater impairment correlating significantly with a 7. Cricketgreater number of bouts. However, those boxerswith an apolipoprotein E e4 allele present also Cricket is another sport without critical scientificdemonstrated a significantly greater tendency to- evaluation regarding injuries to the nervous system.wards a CNS deficit.[43] Studies into the molecular Injuries to the head, hands and forearms appear to beprofile of tau pathology in patients with chronic the most common, with most injuries secondary totraumatic injury, including boxers, with dementia being struck by a ball in children playing cricket.[49]
pugilistica have demonstrated the same tau epitopes Uncommonly, head injuries can be severe with pres-as found in filamentous tau inclusions in ence of intracranial haemorrhage.[49]
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

696 Toth et al.
8. Darts and Lawn Darts risk of injury, as dives with a maximised flightdistance and low entry angle appear to be safest.[59]
The sharp point on the dart used in indoor recrea-In older adults, rare reports of internal carotid
tional games as well as the lawn dart used outdoorsartery occlusion and carotid dissection have oc-
can sometimes be associated with neurological inju-curred following a sports dive.[60]
ry. The head is the most common body part to beinjured by the dart, and nearly all such patients are
10. Equestrian and Horse Racingchildren.[50] In particular, lawn darts have been asso-ciated with penetrating skull injuries including de- The union of two species in one sport is uncom-velopment of a polymicrobial brain abscess in one mon, and can lead to injuries due to a lack ofcase.[50] Neurological impairment may occur in up to ‘teamwork’, as well as the high speeds achieved and50% of lawn dart-associated head injuries.[50,51]
heights from which to fall. Surprisingly, injuries inequestrian sports are reported to be very common,9. Divingperhaps 20 times more common than motorcy-
The predominant mechanism of injury associated cling.[61]
with water activities is diving, with cervical SCIcomprising 4.9% of all water-related accidents in 10.1 Head Injuries in Equestrian Sportschildren.[52] Amongst all sports, diving is the mostcommon cause of SCI (21.6%), and most commonly Closed head injuries are a common occurrence inaffects males (88%) of young age (mean of 28.5 riders due to falls from the horse. In one Canadianyears).[53] Patients sustaining a cervical SCI are retrospective study, closed head injury was the mostmore likely to be in the early to mid teenage years common cause of admission to hospital after eques-(10–14 years in one study), and to be experienced trian-related trauma.[62] The majority of equestrian-divers.[52,54] The second most common group to related injuries (60%) are caused by falling from theexperience high cervical SCI due to diving are horse,[63] while a smaller percentage of injury (40%)young adult male divers.[55] The cervical SCI is so is due to being kicked by a horse, even as a bystand-common in divers, that in one large retrospective er.[63] Closed head injuries of varying severity havestudy, all SCI associated with diving were at the been associated with a fourth nerve palsy in 46% ofcervical level.[56] Almost all SCI related to diving patients, and loss of vision in 20% of patients.[64]
(87%) occur in private or residential swimming Intracranial haematomas have been reported withpools.[57] Alcohol and presence of a pool party were equestrian trauma, including paediatric cases, andinvolved in 49% and 46% of cases, respectively, of these may be fatal.[63,65] When compared with otherdiving-associated SCI in a retrospective study.[57] As common mechanisms of paediatric injury, the aver-would be expected, most diving-related SCI (57%) age degree of head injury in riders was only less thanoccur with diving into <1.2m (4 feet) of water.[57] automobile-related accidents.[66] Equestrian-relatedAbsence of a lifeguard on duty was noted in 94% of deaths are secondary to head injury in 57% of casescases in a retrospective study.[57] Non-competitive for riders under 25 years of age, which also accountstandard diving accounts for 70% of SCI cases, with for most hospitalisations in this population.[67,68] Fe-unusual or trick dives less commonly associated.[57] males injured in equestrian injuries outnumber
Once the SCI has occurred, only rehabilitative males, partly due to female predominance in thisprogrammes can be attempted for the SCI patient. activity.[69] However, over the age of 44 years, moreClearly, this is a sport-related neurological injury men are injured than women, and male deaths farthat is best addressed with prevention. An interven- outnumber female deaths above the age of 64tion programme for subjects with low diving skills years.[69] Helmet use reduces the risk and severity ofsuggested improvement and greater safety following head injuries and should be vigorously promoted,[64]
participation.[58] The type of dive also determines as most riders are helmetless.[63] Use of a helmet in
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

CNS Injuries in Sport and Recreation 697
paediatric riders was associated with decreased fre- There has been one reported case of epidural in-quency and severity of CNS injury.[66] tracranial haematoma reported after the player was
hit by a lacrosse stick.[77] These statistics have led to10.2 Spinal Injuries in Equestrian Participants recommendations for the use of protective head/faceand Jockeys gear.[74]
An entirely different sport from equestrian, pro- 12. Footballfessional horse racing is a fast sport with high injuryrates.[70] There are surprisingly few epidemiological American and Canadian football are aggressivereports on the subject, and only one report of cervi- sports with significant physical contact and high riskcal SCI in two German jockeys.[71] The long-term of injuries, both neurological and otherwise. In mosteffects of horse riding upon the cervical and lumbar studies, football is reported as the sport most likelyspine of jockeys may be deleterious as well because to be associated with injury, serious injury, andof repetitive trauma. The incidence of degenerative specifically neurological injury. Acute injury rates,changes of both cervical and lumbar spine was FITS, and MTBI for football are listed in tables IIIhigher in jockeys versus age-matched controls in a and IV.[7,9] As would be expected, contact withprospective study with both clinical and radiograph- another player was the most frequent method ofic evaluation of the spine.[72] Although not as com- injury in football.[7] Of all injuries reported, 14%mon as head injuries, spinal injuries causing were considered serious (fracture, dislocation, orquadriplegia or paraplegia make up 30% of severe concussion).[7] The frequency of injuries per or-injuries.[63] Injuries to celebrities such as Christo- ganised team per season is 14, 3-fold greater than allpher Reeve may lead to greater injury prevention in other team sports for children aged 7–13 years (tablehorse riders including helmet use and education.[73] IV).[7]
11. Field Hockey and Lacrosse 12.1 Concussion in Football
Injury rates in lacrosse and field hockey, despite Even with the presence of helmets, the high ve-the use of a hard ball and sticks with aggressive locity and violent nature of football leads to manyplayers, tend to be much less than other major head injuries. Of ten sports investigated, footballsports. Acute injury rates are listed in table IV.[9,74] accounted for 63% of MTBIs.[9] The presence of aLacrosse-related trauma is more common amongst helmet for protection can also lead to injuries, as 7%male players (81% of all cases in a male-dominated of all football injuries involve being struck by ansport), and is most common amongst teenage play- opponent’s helmet.[8] The published incidences ofers (mean age 16.9 years).[74] An estimated head concussion in football have significant variation,injury and concussion incidence rate for lacrosse is partly due to over reporting of recalled episodes ofprovided in table V,[75,76] with most of these injuries concussion in team-mates when compared with self-due to ball contact.[74] In terms of sports leading to reports and videotape analysis.[78] Concussion inci-MTBIs, field hockey was the least likely sport of dence rates for football are provided in table V[79]
those studied to cause head injury (1.1% of all and occur with more than twice the incidence ofMTBIs).[9] Females are more likely to receive head other team sports. High-school football players self-or face injury (30% vs 18% in males), perhaps reported an incidence of concussion of 47% overbecause female lacrosse players are less likely to one season, with 35% of all players reporting multi-wear helmets.[74] Of all major women’s collegiate ple concussions, also over one season.[80] Post-con-sports, lacrosse appears to have the highest percent- cussion headache occurs in 86% of high-school andage of injuries as concussions (14%), higher than collegiate-level football players.[81] Another study ofwith male lacrosse players (10%).[10] Closed head both high-school and college football players report-injuries comprise 6% of all lacrosse-related injuries. ed only 5% of players to sustain one concussion,
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

698 Toth et al.
while 15% of those players sustained a second con- deficit and balance problems compared with con-cussion during the same season.[81] The most com- trols.[91,92] Presence of on-field mental statusmon specific diagnosis in Canadian varsity players changes such as retrograde amnesia and posttrau-was concussion.[82] In Canadian college football matic confusion in high-school football players re-players, incidence of concussion was equally dis- lates to the presence of memory impairment at 36tributed between games and practice,[83] which is hours and up to 4–7 days post-injury, and is alsounique for this sport and injury type as most sports- related to slower resolution of post-concussionrelated injuries have higher incidences during com- symptoms.[93] Over the following 5–7 days, cogni-petitions. A study of Canadian Football League pro- tive functioning returned to baseline while balancefessional players suggested a 45% concussion inci- returned to baseline after 3–5 days, with no measur-dence rate over one season, with a 70% incidence of able differences after 90 days.[91] The mean overallmultiple concussions in players reporting at least duration of concussion-related symptoms in col-one.[84] A slightly increased incidence of concussion legiate football players experiencing concussion iswas noted amongst offensive and defensive line- 82 hours, with further slowing of recovery seen inmen,[83,85] as well as special teams players in two players with multiple concussions.[94] Indeed, a mea-earlier studies.[85] Rates of concussion incidence by sured decline with neurocognitive testing may be theposition are listed in table V.[86] The majority of only objective measure that significantly relates toimpacts (71%) leading to concussion is from an the duration of post-concussion symptoms.[88] De-opponent’s helmet, arm, or shoulder pad to the side spite these findings, it is possible that the effects onof the player’s helmet, and often these impacts are cognition of two concussions may not be dissimilaron the highest portion of the helmet.[87] Blocking from one concussion in collegiate football play-may lead to more concussions than tackling.[85]
ers.[95] Yet, the presence of three or more concus-sions gives a 9.3-fold increased risk of loss of con-The most common symptoms of MTBI in profes-sciousness with subsequent concussion, as well assional football players were headaches (55.0%), diz-other concussion-related symptoms such as anter-ziness (41.8%) and blurred vision (16.3%).[86] A lossograde amnesia and confusion.[96]of consciousness occurs in 8.9–9.3% of cases.[81,86]
Although a loss of consciousness is certainly an A neuropsychological study showed that collegeindicator of greater injury, it fails to correlate with football players with prior concussion demonstrateduration of post-concussion symptoms,[88] but may learning disability for the Trail-Making Test andrelate to the extent of cognitive dysfunction immedi- Symbol Digit Modalities Test compared with play-ately after concussion.[89] Presence of post-concus- ers without prior concussion recorded.[97] Anothersion headache, however, in high-school athletes confounder may be age or educational level, as high-(predominantly football players) may be associated school athletes (predominantly football players)with an incomplete recovery of reaction time and with concussion have more prolonged memory dys-memory function.[90]
function than college athletes with protracted recov-ery of cognitive function still present at 7 days post-The short-term effects of concussion includeinjury in high-school athletes.[98] Another potentialneurocognitive impairment when high-school andconfounder in the assessment of neuropsychologicalcollege football players were assessed immediatelyassessment is the presence of pre-morbid learningand 15 minutes after injury compared with a pre-disability, which has a positive association withseason baseline score.[89] Players with a concussionoccurrence of multiple concussions.[97] A useful tooland loss of consciousness (grade 3 concussion) werein the assessment of post-injury cognition functionfound to be the most severely impaired immediatelyis the Standardized Assessment of Concussionafter injury, giving a gradation for the effects of(SAC), which is highly sensitive in the classificationconcussion on neurocognition.[89] Immediately fol-of concussion injury on the football sideline.[99] Aslowing concussion, players demonstrate cognitive
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

CNS Injuries in Sport and Recreation 699
demonstrated with other tests, the SAC testing also amongst offensive and defensive linemen, and de-fensive backs, and is often unreported to trainers.[106]suggests that most players return to baseline cogni-
tive levels by 48 hours after injury.[65,99] A futuretool in the assessment of concussion-related cogni- 12.2 Second Impact Syndrome in Footballtion deficits is functional magnetic resonance imag-
The presence of an episode of concussion maying (fMRI) using blood oxygen level dependentplace the player at increased risk for recurrence up to(BOLD) signals. Symptomatic concussed athletes3–4 times,[80,107] which also may lead to increasedmay demonstrate task-related activations in somerisk for the recently popularised second impact syn-but not all of the expected brain regions, but maydrome.[78] Although publicised in the past, the prev-also show additional increases in BOLD activityalence of second impact syndrome is difficult tooutside expected regions.[100]
calculate. The second impact syndrome has beenGreater education of football players is obviously defined as a sustained head injury after an initial
required as a recent study suggested that only head injury, usually a concussion, where symptoms18–23% of concussed college and professional foot- associated with the first injury have not fullyball players realised they had experienced a concus- cleared.[78] It has been postulated that this secondsion.[83,84] Fortunately, the majority of concussions impact leads to rapid development of cerebral vas-are mild (88–95%).[80,85] As has been suspected by cular congestion and increased intracranial pressure,many professional players, the use of artificial turf resulting in brainstem herniation and death.[78] Al-may play a role in the high incidence of concussion though some of the first reported patients with sec-in football players,[101] perhaps due to a lack of ond impact syndrome were football players (also iceimpact attenuation demonstrated within a domed hockey and boxing), scepticism about the true na-stadium with artificial turf.[101] The presence of a ture of this entity continues,[108] as this phenomenon
may simply represent diffuse cerebral swelling andcustom-made mouthguard, however, does not seemmay not be due to a true ‘second impact’.to influence the incidence of concussion in col-
legiate level football players.[102] Suspected high12.3 Severe Head Injuries in Footballrates of head injuries in football players during the
1960s and 1970s led to the development of a helmetMore severe brain injuries are less commonlywith improved impact performance, as the result of
reported in the literature concerning football. Initial-an improved headform composed of syntheticly, there were great concerns about second impactmaterials. Significant reductions in youth footballsyndrome, and its possible relationship with diffuseinjuries followed, including a 65% reduction in cra-cerebral swelling with delayed catastrophic neuro-nial fractures, 51% reduction in fatal head injuries,logical deterioration. However, the absence of spe-and 35% reduction in concussions.[103] Video analy-cific risk factors and presence of only scattered casesis of professional football plays resulting in headreports (17) make this syndrome and its postulatedinjuries as well as laboratory reconstructions usingsevere complications controversial and questiona-
helmeted dummies has determined that concussionsble.[78] Similarly, the presence of chronic traumatic
are primarily related to translational acceleration atbrain injury, as seen in boxing, has been postulated
the time of impact as well as a significant velocityin football, but without significant evidence.[109] Oc-
change.[104] Head-to-head collision has been simu- currence of intracranial haemorrhage, particularlylated via a finite element head model, which sug- subdural haematoma, has rarely been reported ingests that shear stress at the brainstem may be an football.[9] Persistent cerebral traumatic injury dueinjury predictor for concussion.[105]
to football has been documented in 66 players overThe presence of post-traumatic headache in foot- the past three decades.[110] Players who tackle with
ball after collisions is common (21%), particularly the head down and use the head as a battering ram
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
700 Toth et al.
may be at increased risk for more severe forms of fracture was found in 4% of injured boys.[116] Thereinjuries to the head and neck.[110] are no reports of adults being injured with golf clubs
or balls. Many of the literature reports regarding12.4 Spinal Injuries in Football golf-related injuries to the CNS are surprisingly due
to golf cart accidents. The use of a golf cart has beenSpinal injuries are some of the most devastating
associated with rare SCI following serious trau-injuries associated with football. Next to diving and
ma.[117] Head injuries including cerebral contusions,skiing, football is the most common cause of sports-
skull fracture and extradural haematoma have eachrelated SCI (13% of all sports-related SCI).[53] A
been reported once as a result of a golf cart-relatedcondition called transient quadriparesis, or cervical
traumatic injury.[118] Golf may have led to vertebraltransient neurapraxia, seems to be most common in
artery dissection and Wallenberg syndrome in onefootball secondary to a blow to the head with sudden
case,[119] perhaps from torsion of the neck.neck flexion or extension. Clinically, the patient
Thoracic spinal injuries including acute thoracicexperiences transient weakness and numbness to thespinal disc prolapse following a golf swing has beenextremities for a period of seconds to a few days.recorded in a male with a decade history ofThe incidence of this condition is between 1–6 perL’hermitte’s symptom,[120] and thoracic spinal oste-10 000 players.[111] In children aged 7–15 years whooporotic fractures in women[121] have been noted.developed cervical cord neurapraxia due to a foot-
A movement disorder called ‘yips’ (not a trueball-related injury, the mobility of the paediatricinjury) has been described in golfers with a jerk,spine rather than congenital cervical spinal stenosisspasm, or other disruption of movement during put-may play a role,[112] although this is controver-ting or chipping; this might be considered a focalsial.[113]
task-specific dystonia.[122]The most common mechanism of SCI is axial
loading of the cervical spine, as opposed to neck14. Gymnasticshyperextension or hyperflexion using film analysis
of plays with injuries.[114] Axial loading due to tack-Gymnastics requires difficult manoeuvres and
ling with the head in moderate flexion actually leadsbody postures that place the body at risk for injury,
to straightening of the cervical spinal curvature, andparticularly with involvement of trampolines. There
has led to sagittal vertebral body fracture as well asare no specific reports of incidence of neurological
fracture of the posterior neural arch with neurologi-injury due to gymnastics. However, the number of
cal sequelae including paralysis.[115] Over recentinjuries to the cervical spine among gymnasts in
decades, a number of changes to the sport includingsome studies is next to only football and wrestling,
changes in penalty systems, emphasis upon tacklingwith the majority of the spinal cord lesions occur-
with shoulders as opposed to using the head as aring at the mid-cervical levels.[123,124] Gymnastics is
spear, and new design of helmets and protectivealso one of the sports where high-school and college
equipment have led to significant reduction of cervi-participants are at greatest risk of death.[125] Specifi-
cal spine injuries associated with quadriplegia incally, the spine and spinal cord appear to be at
football since 1976.[113]substantial risk with gymnastics. Twenty-four for-mer female artistic gymnasts had radiography at the13. Golfend of their athletic careers, still at a young age,
Golf would not be expected to be associated with which demonstrated radiographic changes in >50%a high rate of injury given its ‘relaxing’ nature. Head including spondylolysis, spondylolisthesis, retrolis-injury due to a golf club (91% of all golf-related thesis and scoliosis.[126] Although once hypothesisedhead injuries) or golf ball has been reported in to play a role, the presence of congenital spinalchildren aged 3–13 years, 78% of whom were stenosis in children presenting with cervical cordboys.[116] Evidence of a compound depressed skull neurapraxia resulting from gymnastics and other
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

CNS Injuries in Sport and Recreation 701
sports does not appear to play a role.[112] In young 15. Hang-Gliding and Paraglidingadult gymnasts, the most common mechanism of
Hang-gliding is a sport with obvious risks. Asinjury may be failure to perform a technically ade-with other sports, the majority of injuries reportedquate somersault.[123]
occur in 20–40 year olds.[135] As would be expected,the majority of all injuries (60%) occur at land-
14.1 The Trampoline in Gymnastics ing.[136] In particular, SCI leading to paraplegia orquadriplegia have significantly increased,[56] and
The trampoline has come under attack in recent spinal injuries comprise 36% of all injuries.[136]
years as a cause of injury and SCI in particular. Inmany cases, supervision is present and awareness of 16. Hockeythe danger of the activity is understood, but injuriescontinue to accumulate at an increasing and alarm- Ice hockey is a sport of controlled aggressioning rate. The trampoline is an extremely dangerous where multiple mechanical forces from the player,piece of equipment that can project people up to 9m competitors, the hockey puck, goal posts, ice sur-in the air, resulting in a long fall either back to the face, unyielding boards, and propensity for fightingtrampoline or even to the ground, where the partici- can all contribute to injury. Inherent speeds of thepant is at risk of landing on their head or neck. In puck with a slapshot (190 km/h), as well as theone report, trampolines were deemed responsible for skating speeds (30–45 km/h), and the speed of the>6500 paediatric cervical spine injuries in 1998 in player who is sliding on the ice (25 km/h), all lead tothe US, a 5-fold increase in reported injuries over potential for injury.[137] Despite increasing publicthe past 10 years.[22] This surprisingly high injury concern about the numbers of hockey injuries inrate has been verified in other retrospective studies, both amateur and professional leagues, good epide-also suggesting a dramatic increase in the number of miological studies of injury rates and incidence arerelated SCI over the past decade.[127] Spinal injuries lacking in ice hockey. Acute injury rates, which arecomprise 12% of all trampoline-related injuries, high, are listed in table IV.[138-140] Of these injuries,with the majority of other injuries consisting of 12% were concussions experienced by 9% of thefractures.[127] Neck injuries more commonly occur players.[138] In these adult players, concussions ac-in younger trampoline users,[128] but teenagers and counted for 14% of all injuries.[139]
young adults have also been reported with trampo- Bodychecking remains the most common causeline-related cervical SCI.[129] Trampoline-injured of injury in hockey, as child and teenage players inpatients are both female (53%) and male, with a contact leagues are 4-times more likely to be injuredmedian age of 7 years.[127] Essentially all injuries and 12-times more likely to receive a fracture com-occur on privately owned trampolines (99%).[127] pared with players in non-contact leagues.[141] Fe-Adult supervision is likely to be present at the time male and male hockey players have similar overallof injury (56%) and parents often reported aware- injury rates (9.19 injuries per 1000 male athlete-ness of potential dangers of trampolines before the exposures [A-E] vs 7.77 injuries per 1000 female A-injury (73%).[130] Often, the parent reported that the E) despite the fact that intentional body checking ischild continued to use a trampoline after an injury not allowed in women’s hockey.[142] Women wereoccurred (55%).[130] Many authors have called for a more likely than men to be injured with contact withban on the use of trampolines as a result of these the boards, but women sustain less serious inju-frequent injuries.[128,130-132] As well as SCI, a tram- ries.[142] Injuries to children playing hockey arepoline injury was deemed responsible for a vertebral predominantly due to checking (57%).[143] In con-artery dissection in an 11-year-old boy.[133] trast to adult players, only 4% of children’s injuries
Aeroball, a sport played on a trampoline court occur due to illegal activity;[143] however, in onehas also been associated with rare cervical SCI.[134] survey, 32% of children state that they would check
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

702 Toth et al.
illegally to win, and 6% said that they would pur- player.[148] As with spinal injuries in hockey, theposely injure their opponent to win.[143] frequency of concussion may be increasing, al-
though increased attentiveness and improved diag-Some of the risk factors for injury in ice hockeynostic skills may bias this observation.[149] In con-are distinct from other sports. The more experiencedtrast to other sports again, the incidence of concus-player is significantly more likely to sustain inju-sion increases with higher levels of play andry.[138] The older, taller and heavier a player is, theexperience of the player.[145] Other forms of moregreater the risk of injury as well.[138] Positions mostsevere brain injuries such as epidural and subdurallikely to sustain injury were defencemen andhaematomas are rare, but reported.[145] There arewings.[138] As with other sports, the majority ofrare occurrences of mortality in an observer or par-injuries occur during competition.[138] Particularticipant secondary to their head being struck by aevents associated with injury include forecheckingpuck. In one case, a single patient, struck over theand breakout plays (head injury) and backcheck-left mastoid region by a hockey puck, suffered aing.[138] Illegal activities in hockey such as elbowingfatal rupture of a left vertebral artery berry aneu-and high sticking were responsible for 26% of inju-rysm.[150] The use of face shields was studied inries.[138]
Canadian University hockey players with compari-son of full- and half-face shields. The use of a full16.1 Head Injuries in Hockeyface shield gave a significant decrease in time lost
Most hockey injuries affect the head and neck. from participation because of concussion and noPeak accelerations inside the helmet are significant- difference in the rates of neck injury or concus-ly higher for hockey players than for football play- sion.[151]
ers, which likely contributes to the risk of headinjury.[101] Every season, 10–12% of minor league 16.2 Spinal Injuries in Hockeyhockey players aged 9–17 years experience a headinjury, usually concussive in nature.[144] The inci- Spinal injuries, although less common, are proba-dence rates of concussion are listed in table V.[145,146] bly the most devastating form of ice hockey-relatedIn collegiate male hockey players, concussion com- injury. A Canadian registry of hockey-related spinalprises 10% of all injuries.[10] This strong trend with injuries includes cases from 1966–96[152] of anyage is probably associated with greater rates of fracture or dislocation of the spine with or withoutbodychecking. More concerning is the significant injury to the spinal cord or nerve roots as well asincrease in concussion rates over the recent seasons cases of transient quadriplegia.[152] Since 1981, thereof professional ice hockey.[146] While this increase has been an apparent rise in spinal injuries, althoughmay be due to increased recognition and reporting, reporting bias, increasing populations of hockeyother changes such as larger and faster players, as players, and better diagnostic and reporting skillswell as harder boards and presence of glass over the may play a role.[152] An average of 17 major spinalboards may also be a contributing factor.[146] Head injuries occur annually in Canada,[153] and thereinjuries in ice hockey are most commonly associated have been six deaths in Canada due to SCI over thewith collision with another player (45%), while oth- monitored period.[152] The great majority of maleer causes include hitting the boards (34%) or being athletes experiencing major spinal injuries are agedhit by a stick (22%).[138] Surprisingly, fighting does 16–20 years.[153] The most common level of injurynot appear to be a common cause for concussion.[147] has been at the cervical spinal level (85%),[152] whileIn some studies, concussion is the most common ice another Scandinavian study reported 69% of allhockey-related injury in adults.[145] Rates of MTBI vertebral injuries to occur between C5 and C7are listed in table V.[79,147] levels.[154] Spinal injuries occur most commonly
The annual risk of concussion related to profes- with pushing or checking into the back (40%), whilesional ice hockey is extremely high, about 5% per impact with the boards accounted for 77% of spinal
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
CNS Injuries in Sport and Recreation 703
injuries.[152] The injury experienced at impact with sociated with numerous injuries, neurological inju-the boards is often a burst fracture of the cervical ries, usually involving head and neck, are relativelyspine while the neck is slightly flexed.[155] Approxi- uncommon.[163] The incidence of injuries occurringmately 50% of SCI occur in the 16- to 20-year age amongst each of these disciplines is roughly similar,group, with most occurring in competitive level at least between karate, taekwondo and Muay Thaigames.[152] New rules, such as the introduction of kick boxing.[164] Injury rates are listed in table‘checking from behind’, may be more effective at IV.[164]
decreasing the number of severe spinal injuries in Estimates of total head and concussion incidenceice hockey.[144] However, programmes implemented rates for martial arts are listed in table V.[165,166] Nextin Canada in the past two decades have not de- to contusion, concussion was the most commoncreased the number of injuries reported annually.[156] form of head injury in both sexes.[166] As expected,
the most common head injury mechanism was re-17. In-Line Skating, Roller Hockey ceiving a blow.[166] Male adult full-contactand Skateboarding taekwondo competitors experience slightly higher
rates of head injury (7.04 per 1000 A-E) than childAlthough less common than ice hockey, profes-athletes, but the dominant injury mechanism re-sional roller hockey, or in-line hockey, may actuallymains a blow to the head (6.46 per 1000 A-E).[165]
be associated with more overall injuries than iceThe majority of literature reports of neurologicalhockey, perhaps due to differences in playing sur-
injury in martial arts participants are of single casefaces or with difficulty in stopping on in-linereports. One patient developed a ‘locked-in’ syn-skates.[157] One study found similar total injury ratesdrome following a cervical trauma that occurredbetween roller hockey (139 per 1000 A-E) and iceduring karate training due to vertebral artery dissec-hockey (119 per 1000 A-E), and noted that gamestion.[167] Strokes have been reported in martial artslost because of injuries were greater in ice hockeycompetitors with embolic stroke secondary or possi-(8.3 ice hockey games vs 6.5 in-line hockey games)bly secondary to carotid dissection after neck-hold-[table IV].[158] Roller hockey may have a similaring manoeuvres or blows to the head or neck.[168-171]
incidence of head and neck injuries as ice hock-Kickboxing and French boxing have also been asso-ey.[158]
ciated with intracranial arterial dissection.[172,173] ARecreational in-line skating has become an in-judo participant developed a cervical myelopathycreasingly popular activity for both children andassociated with cervical disc herniation possiblyadults. Injuries related to in-line skating tend toassociated with congenital cervical canal stenosisoccur in boys (61%) with a mean age of 12and judo-related injury.[174]
years.[159,160] Head and neck injuries comprise 16%More serious injuries in judo have includedof all injuries with inexperience with the activity
chronic subdural haematomas[175] and other forms ofappearing to be the most common cause.[161] How-intracranial haemorrhage.[176] The occurrence of de-ever, head injuries due to in-line skating (34%) arementia pugilistica or other chronic cognitivesignificantly less common than with skateboardingchanges in participants of martial arts has not been(51%),[160,162] and severity of injury is significantlyreported.[177]
less than skateboarding.[162] Helmet usage has beenadvocated in all three sports.[160]
19. Motorcycling18. Judo, Karate, Kickboxing and
Injuries to motorcycle racers are quite commonRelated Sportsand are often associated with mortality (9% of all
The martial arts are fighting systems, each em- injuries).[178] Given that racing motorcycles canphasising unique techniques and strategies. Al- reach speeds >306 km/h, this is not surprising.[178]
though these forms of hand-to-hand combat are as- However, the vulnerability of being on a motorcycle
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
704 Toth et al.
does not lead to injury rates higher than that of or from sustaining a blow from the animal.[186,187] Inautomobile racers overall.[179] Of all injuries, contrast to other sporting events, inexperienced10–30% are head injuries, and 25% of these head rough-stock rodeo competitors have a lower overallinjuries are severe with associated intracranial rate of injury and severe injury compared with ex-haemorrhage or mortality.[178,180] Spinal fractures perienced competitors.[188]
are uncommon, representing 4% of all injuries.[180]
22. Rugby and Australian Rules Football20. Mountain Climbing and Hiking
Rugby is an international sport where protectiveMountaineering is a challenging individual sport gear is at a minimum and aggressive tackling is an
where the goal is often to ascend the most difficult integral part of the game. Australian Rules Footballroute with the least amount of necessary equipment. is another aggressive sport that has similarities toInjury rates are listed in table IV.[181] Obviously, rugby and American Football and will be consideredhead and spinal injuries are possible, but no medical here. Epidemiological studies for these sports areliterature information on this is available. Headache, lacking.perhaps due to cerebral oedema, is a prominent
22.1 Head Injuries in Rugby and Australianfeature of acute mountain sickness,[182] as well asRules Footballdyspnoea, weakness, asthenia and nausea. Headache
appears to be secondary to intracranial vascular dila-The majority of rugby-related injuries are to the
tation due to hypercapnoea prior to development ofhead and neck. Cerebral concussion is also a con-
hyperventilation due to hypoxia.[182] The headachecern within both of these sports.[189] As with ice
is often clinically similar to migraine. Cerebral oe-hockey, concussion rates appear to be rising within
dema likely only occurs above 3600m (12 000 feet),Australian rules football (table V).[190] A concerning
and generally requires 2–3 days to develop.[183] Thestatistic is that more junior Australian rules football
incidence of cerebral oedema in all climbers aboveplayers have greater concussion rates than senior
3600m may be as high as 1.8%, and it may occurplayers.[191] Incidence of concussion in high-school
even in experienced climbers.[183] Vasogenic oede-rugby players is listed in table V.[192] In one study of
ma likely predominates early, with development ofprofessional players, 23 concussions were recorded
cytotoxic oedema later, and development of cerebralover a 20-week football season.[193] With video anal-
oedema may be fatal.[183] High altitude cerebral oe-ysis, concussions involved direct head contact most
dema has documented MRI changes with reversiblecommonly, with the majority of impacts to the
white matter oedema, having a predilection for thetemperoparietal region with the striking body seg-
splenium of the corpus callosum.[184]
ment most typically an arm or shoulder/thorax.[194]
As found in American football players, neurocogni-21. Rodeotive difficulties with a digit symbol substitution test
Rodeo injury rates vary by event, but are the correlated with length and number of symptomshighest in bull riding, bareback riding, and saddle post-concussion.[193] Despite the belief of rugbybronc events.[185] Bull riding has a high injury rate of players that headgear offers protection against con-32 injuries per 1000 competitor exposures cussion (62%), only a minority report use of head-(CEs),[185] while the overall injury rate is 2.3 per 100 gear (27%) and only 24% felt that helmet use shouldCEs, lower than most contact sports.[185] Concus- be made mandatory.[195] Interestingly, a study ofsions account for 9% of all reported rodeo inju- childhood and teenage rugby players found thatries,[185] second only to knee injuries. Head and neck currently used headgear does not provide significantinjuries in rodeo most commonly occur during dis- protection against concussion.[196] Although helmetmount due to the violent motions of the animal.[186] use in rugby players has not been validated, a thick-Concussions typically occur from violent dismounts ened polyethylene foam incorporated into headgear
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

CNS Injuries in Sport and Recreation 705
may improve headgear performance.[197] Intake of tentials have demonstrated prolonged cochleopon-glucose in University rugby players with prior con- tine and cochleomesencephalic transmission timescussion led to enhanced performances on neurop- after diving in patients with clinical symptoms andsychological testing including declarative memory signs of vertigo, postural and intentional hand trem-during tests where pre-glucose testing showed defi- or, ataxia and opsoclonus. These features have alsocit.[198] This may suggest that glucose consumption been referred to as otic barotrauma.[201,206] A rela-after concussion may influence cerebral neurotrans- tionship between neurological decompression ill-mitter levels affected by concussion and alleviate ness, of both cerebral and spinal dysfunction, andconcussion-induced memory dysfunction. presence of cardiopulmonary shunt was demonstrat-
ed in a blinded, controlled study. Larger shunts,22.2 Spinal Injuries in Rugby and Australian which are present without a Valsalva manoeuvre,Rules Football were significantly more common in divers affected
by neurological decompression illness.[207] Paradox-Although perhaps not as common, injuries to the
ical thromboembolism and neurological decompres-cervical spine can be amongst the most serious
sion illness in divers has been associated with largeinjuries. The most common mechanism of injury
sizes of patent foramen ovale,[208] which may beappears to be cervical spine hyperflexion, often dur-
amenable to septal occlusion.[208]
ing scrimmaging or tackling, producing fracture dis-Decompression illness of the spinal cord is an-locations of C4-C5 or C5-C6.[199] The number of
other potential complication, although incidence ofserious spinal injuries has increased over the pastthis condition is also unknown. MRI of the spinaldecade despite changes in rules to prevent injury.[200]
cord is less sensitive in divers with decompressionThe phenomenon of transient quadriparesis, mostillness, with focal hyperintensities identified in onlycommon in American football, has also been ob-14% of patients.[205] Somatosensory evoked poten-served in rugby.[200]
tials has identified latency abnormalities in 81% ofpatients with decompression illness.[209]
23. Scuba DivingHeadaches reported in divers include ‘skip
Scuba diving places the participant at unique risk breathing’ headache, with migraine-like features,for ischaemic infarction and decompression illness. possibly associated with carbon dioxide accumula-The incidence of injuries associated with scuba div- tion.[210] Another headache presenting with faci-ing is uncertain. Cerebral arterial oxygen gas bubble otemporal steady discomfort in divers is a headacheemboli have been clinically associated with altera- from an excessively tight face mask or goggles,tions of consciousness, seizures and focal neurologi- perhaps due to pressure on superficial cutaneouscal deficits.[201] Cerebral infarction has been report- nerves or the supraorbital nerve.[211]
ed in professional breath-hold divers during repeti-24. Skiing, Snowboarding, Snowblading,tive dives, with MRI demonstrating multipleSledding, Skating and Ski JumpingT2-weighted hyperintensities corresponding to their
neurological deficit.[202] The most sensitive, but non-specific, diagnostic testing procedures for patients 24.1 Spinal Injuries in Winter Sportswith neurological decompression illness are EEGand MRI, although there is controversy regarding Winter sports are some of the most popular recre-presence of significant differences from con- ational activities. Although many injuries aretrols.[203,204] In divers with arterial gas emboli, MRI orthopaedic in nature, head and spinal injuries areof the brain identified ischaemic cerebrovascular the most commonly occurring serious mala-lesions in 75% of patients, compared with focal dies.[53,212-214] Estimated incidences of SCI due tohyperintensities in 25% of divers with decompres- downhill skiing and snowboarding are 0.01 per 1000sion illness only.[205] Brainstem auditory evoked po- skier-days and 0.04 per 1000 snowboarder-days,
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

706 Toth et al.
respectively.[215] Of sports-related SCI in Germany, associated with flexion-distraction type fractures atvertebral junctions, all of which were due to a back-25% of injuries were due to downhill skiing acci-ward fall from an intentional jump.[218] The presencedents.[53] Of all winter sport-related injuries, spinalof a SCI with winter sport activity is often a harbin-trauma comprises about 5%,[212] with 82% of theseger of another second serious injury, such as crani-due to skiing accidents. Of all skiing-related inju-ocerebral trauma (36%).[212]ries, 1.4% are spinal in nature.[214] The age group
most affected by spinal trauma in winter sports is the24.2 Head Injuries in Winter Sportsgroup aged 15–25 years (40%).[212] In contrast to the
level of SCI in other sports and recreational activi-Head injuries, although not as publicised as SCI,ties, most skiing-related spinal traumas occur in the
are common in downhill skiing. Estimated incidencethoracolumbar region (47%), followed by the cervi-of head injury and concussion for snowboarders andcal region (39%).[212] The most commonly associat-skiers are listed in table V.[219] Head and face inju-ed fracture type with skiing-related SCI is compres-ries comprise 17–22% of injuries in recreationalsion in nature (38%).[216] Although the thoracolum-skiers reporting injuries.[220] Approximately 22% ofbar region is affected most commonly, the mostthese injuries were related to concussion and thisserious injuries to the spinal canal in snowboarding-was the body region injured most frequently in malerelated injuries tend to occur at the cervical level.[212]
skiers.[220] In one Canadian study, 60% of skiersBesides the acute presentation of injury, the rarepresenting after trauma had experienced a head inju-occurrence of a delayed presentation of cervicalry.[213] Approximately 69% of these injuries arespinal epidural haematoma 1 month after aconcussive in nature.[221] However, 14% of thesesnowboarding injury has occurred in a young malepatients received severe brain injuries, with an over-snowboarder after striking his occiput and com-all mortality rate of 4% with a severe head inju-plaining of immediate neck pain and radicularry.[221] As opposed to other forms of skiing-relatedsymptoms.[217] The majority of spinal injuries (70%)injury, collision with a tree or another skier is thecaused by downhill skiing result from a simple fall,mechanism of injury in 47% of skiing-related headfollowed by striking a tree.[213,214]
injuries.[221] Collisions with trees are more likely toSnowboard-related spinal injuries also differ produce severe head injury and mortality.[221] The
from skiing-related injuries with a significantly risk of head injury from skiing is greatest in maleshigher incidence of transverse process fractures.[214]
and those aged <35 years.[221]
The initial period of learning snowboarding appears Snowboarders appear to have even higher ratesto be difficult, as beginner snowboarders are signifi- of head injury, up to 3-fold higher, compared withcantly more subject to SCI than beginner skiers.[214]
skiers.[221,222] In fact, snowboarders are more likelyIn contrast, intermediate or expert snowboarders are to experience intracranial haemorrhage with headmore likely to be injured because of jumping than injury (71%) compared with skiers (28%).[222] Asbeginners (p < 0.001), whereas about 70% of spinal occurs with respect to spinal injuries,[214] beginninginjuries from skiing resulted from a simple fall.[214] snowboarders are significantly more likely to expe-Intentional jumping is the cause of injury in 77% of rience a head injury compared with beginning ski-snowboarders, compared with 20% of skiers.[215] Of ers.[219,223] Risk factors for snowboarding-relatedall snowboard-related injuries, 3% are spinal in na- major head injuries include falling backward (68%),ture.[214] More than half (53%) of all surgically occipital impact (66%), a gentle-moderate ski slopetreated spinal injuries of winter sports-related inju- (76%) and inertia (76%).[219,224] Of cases involvingries showed some neurological impairment, while inertia, contrecoup injury was present in 8% of17% had evidence of a complete transverse lesion of patients.[224] Risk factors for acute subduralthe spinal cord.[212] In one study, young males aged haematoma as a snowboarding-related injury in-23–25 years experienced SCI, which in all cases was clude falling backward and occipital impact.[224]
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

CNS Injuries in Sport and Recreation 707
Subcortical haemorrhagic contusion risk factors in- rates in luge are listed in table IV.[232] Concussionsclude falling during a jump, a temporal impact, or comprise 2% of all injuries, most of which are fromfalling on a jump platform.[224] In particular, jump- crashes.[232] Recreational sledding has similar de-ing is a much more frequent cause of head injury in grees of overall injury compared with skiing, but hassnowboarders (30%) than skiers (2.5%).[224,225] a significantly higher incidence of head injuries,[233]
These snowboarding-related injuries related to the as high as 34% in one study where 3% of injuriesopposite-edge phenomenon, when the opposite edge were to the spinal column in children aged ≤18of the snowboard portion carving touches an uneven years.[234] Skeleton, an emerging extreme wintersnow surface leading to instability and resulting in a sport, is likely too new a sport to have associatedfall on a gentle or moderate slope leading to occipi- literature reports of injuries. No CNS injuries aretal impact.[224] Rarely, skiers and snowboarders can reported with cross-country skiing.be trapped in an avalanche, which may be associatedwith closed head injury.[226] Suggestions have been
25. Snowmobiling and All-Terrainmade for snowboarders to wear protective gear overVehicle Ridingthe occipital region, and for beginners to refrain
from jumping.[219,224,225]
Snowmobiling is a popular recreational activityas well as a form of competitive racing. High speeds24.3 Injuries in Other Winter Sports(75 km/h) and dangerous riding habits contribute to
Snowblading is a relatively new sport that uses injuries associated with snowmobile use.[235] Partici-short, manoeuvrable skis. Head injury, including pants injured using snowmobiles are malesconcussion, comprises 11% of all injuries in snow- (85–90%), and have an average age of 25–29bladers; it remains unclear if helmet use affects years.[235,236] Helmets are used sparingly (35%) andconcussion rate or rates of neck injury.[227]
alcohol intake is present in 44% of cases.[235] SeriousAlthough ski jumping would be expected to have head injuries comprise 34% of all injuries, while
high injury rates given jumps close to 100m high, spinal injuries comprise 18%.[235] Snowmobilingreports of injury are uncommon. Injury rate esti- can be associated with a risk of avalanche dependingmates are provided in table IV.[228,229] Neurological upon the setting, and closed head injuries have beeninjuries are uncommon, with four patients reported reported as a result.[226]
to have closed head injuries, including concus-All terrain vehicles (ATVs) have become moresions.[230] Freestyle skiing is an evolving sport in-
popular, and injuries due to ATVs have becomevolving high-speed jumps, summersaults and twists.more common, especially in paediatric populations,We have seen one patient with multiple concussionswhich comprise 65% of injured riders.[234] Patientsfrom a manoeuvre called a ‘snap back’, where theas young as 2–4 years of age have been reported toparticipant’s head snaps forward after landing withreceive injury from ATV riding.[234,235] As withthe body backward extended at least 45 degrees,snowmobiling, the minority of injured riders did notleading to recurrent occiput head pain.wear a helmet.[235,236] The most common mecha-Injury in short-track speed skating is seldom re-nisms of injury were falling of the ATV to theported, but 6% of elite level speed skaters are sub-ground, striking a tree, or flipping backward.[237]ject to concussions due to accidents during competi-Next to orthopaedic injuries, closed head injuries aretion.[216] Likewise, junior figure skaters can also bethe most commonly reported injury.[238] In terms ofsubject to head injuries, which comprise about 10%neurological injuries, cranial injury comprised 64%of injuries occurring within pairs skating, but has notof the total, and spinal injuries comprised 36%.[237]been reported to occur in single figure skaters.[231]
Avocation for helmet use has been suggested forLuge is a winter sport where an individual orATV users.[237]team rides a sled down a winding ice track. Injury
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

708 Toth et al.
26. Soccer head injuries are less commonly reported in soccer.Occurrence of chronic-subacute subdural
Soccer, the most international sport, has expand- haematomas with an associated arachnoid cyst anded tremendously over the past few decades, and is
presentation after being struck on the head by theplayed on the local, regional, national and interna-
soccer ball have been reported.[241,242] A delayedtional levels. Unintentional collisions with other
presentation of epidural haematoma after beingplayers or goal posts, or mishaps attempting to strike
struck by the soccer ball has been noted in oneor head the ball have all led to injuries within soccer.
report.[243] The lead author (CT) has seen one femaleMany of the injuries experienced by soccer players
patient who experienced a concussion and basalare of a musculoskeletal nature affecting the lower
skull fracture after being struck by a soccer ball,extremities, but head and neck injuries can occur.followed by bacterial meningitis and subsequentInjury rates and FITS in soccer are provided in tablefatality.IV.[7,9]
Although the force and repetitive nature of head-26.1 Head Injuries in Soccer ing the soccer ball and collisions with other players
might suggest the possibility of long-term neurop-Given the fast nature of the sport, and the ability
sychological dysfunction, this association is contro-to ‘head’ the ball, head injuries are the most com-
versial. One study of former soccer players foundmon form of neurological injury in soccer. Head
81% to have mild to moderate neuropsychologicalinjuries have been shown to account for between 4%
impairment.[240] In a study of professional activeand 22% of soccer injuries.[239,240] Of all injuries
soccer players, the number of headers occurring inover a 3-year period, MTBIs in soccer accounted for
one season was related to poorer results on atten-6.2% in both boys’ and girls’ soccer at the childhood
tional and visual/verbal memory tests, while occur-and high-school levels.[9] Canadian University soc-
rence of soccer-related concussions was related tocer players self-reported symptoms of a concussion
poorer results on attention and visuoperceptualduring the previous year in 63% of soccer players,
processing tests.[244] In another study, comparison ofwhile only 20% of the concussed soccer playerssoccer players with control athletes revealed thatrealised that they had experienced a concussion.[84]
amateur soccer players exhibited impaired perform-Of those soccer players experiencing concussion,ance on tests of planning and memory, with themultiple concussions were experienced by 82%,number of concussions incurred inversely related tosuggesting that particular players are more suscepti-the neuropsychological performance.[245] However,ble to head injury.[84] Recognised risk factors forneither participation in soccer nor a history of soc-concussion include female sex.[84] Next to lacrosse,cer-related concussions was found to be associatedwomen’s soccer has the highest percentage of inju-with impaired performance of neurocognitive func-ries as concussion (11%), a higher percentage thantion in high-level soccer players or teenage playersseen with male soccer players (7%).[10] Of all soccerin other studies.[81,239]
positions, goalies were the players most commonlyAnother study examined neuropsychologicalaffected by concussion, even though they rarely
functioning in soccer versus non-soccer collegiatehead the ball.[83] The action of heading the ball leadsathletes (where head injuries would be unusual), andto high accelerational forces to the head; in soccerfailed to demonstrate any change in neurocognitiveplayers at high-school level, heading of the ball wasfunction nor scholastic aptitude despite an averagemeasured with a triaxial accelerometer and identi-of >15 seasons of soccer.[97] Thus, it appears doubt-fied significantly higher (160–180%) peak accelera-ful that the subconcussive impact of purposefultions when compared with impacts occurring inheading is responsible for neurocognitive changes.football or hockey.[101] Although heading the ball isHowever, the question still remains as to whether orcausative for most reported concussions, goal-post
injuries have also been reported.[240] Serious acute not multiple subconcussive impacts may have some
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)

CNS Injuries in Sport and Recreation 709
lingering effects.[246] Electrophysiological evidence and acute lumbar disc herniation (3%), resulting inof abnormalities due to heading are improbable – quadriplegia (33%), residual neurological deficitsnon-specific abnormalities on EEG were found in (20%), paraplegia (3%), and death due to head inju-about 33% of former and active soccer players, ry (3%).[247] Reports of SCI are not unusual in wres-although EEG changes seemed to be more prevalent tling competitions.[248] The majority of severe headamongst players who considered themselves ‘non- injuries are secondary to head-to-head collision dur-headers’ compared with ‘headers’.[240] A non-con- ing takedown attempts, but slams to the mat can alsotrolled study suggested that of former soccer play- result in head injury.[249] A unique wrestling-relateders, 33% were described as having mild central injury occurred with a vertebral artery territorycerebral atrophy identified with CT scan of the stroke due to a prolonged half-Nelson as reported inhead.[240] a single 17-year-old.[250]
27. Volleyball 29. Conclusions
Although volleyball-related injuries primarily af- This article has been extremely broad in terms offect the nerves of the brachial plexus, concussion sporting disciplines and range of injuries affectingcomposes about 4% of all injuries in collegiate-level the CNS. Although we have attempted to provide anfemale volleyball players.[10]
overview of sporting-related injuries, identificationof rarely occurring sport-specific injuries has also
28. Wrestling been attempted. The unique nature of particularinjuries, such as transient quadriparesis in footballAmateur wrestling is an aggressive sport with aplayers, hockey players and rugby players, provide afrequent number of head and neck injuries. Neuro-contrast to common injuries such as concussion andlogical levels affected include the brain, spinal cordmajor SCI within this article.and brachial plexus, with many injuries occurring
This article indicates that injury to the nervouseither due to wrestling holds or takedown ma-system can occur with almost any sport. Even seem-noeuvres. Injury rates in wrestling, which are high,ingly benign sporting activities such as darts andare listed in table IV.[9] Wrestling also accounts fordriving a golf cart have been associated with neuro-the second highest rate (10.5%) of MTBIs in col-logical injury. Particular sports are associated withlegiate athletes, only second to football again.[9]
alarming rates of injury. In particular, trampolineSevere injuries consisting of CNS trauma leading touse, boxing, football and hockey are associated withdisability within wrestlers have been estimated toeither very high CNS injury rates or unacceptableoccur with a rate of 1 per 100 000 participants, withseverity of injury rates.the majority of severe injuries occurring during
competitions (80%).[247] An interesting trend of a This article was limited to reports found withinhigher rate of injuries in low- and middle-weight the PubMed search of medical literature and refer-classes was noted.[247] The rate of concussion in ences found within those articles initially found.wrestling has been estimated at 2.5 per athlete- Obtainable abstracts within PubMed go back to theseason in one study, and seems to comprise about mid-1960s in most cases. Obviously, many injuries6% of all injuries in collegiate male wrestlers.[10,79] must have occurred outside of this review, eitherCertain positions within wrestling have been more because of lack of reporting, or publication outsidefrequently associated with injury including the de- of the PubMed date range. In some cases, neurologi-fensive position during takedown manoeuvres cal abnormalities have been reported in the literature(74%), the down position (23%), and lying position in a patient involved within a sporting activity,(3%). Severe injuries included cervical spinal frac- which may or may not have played a role. Futuretures (77%), spinal cord contusions with transient studies of nervous system injuries in sports could bequadriparesis (12%), severe closed head injury (8%) strengthened by using a case-control design. The use
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
710 Toth et al.
9. Powell JW, Barber-Foss KD. Traumatic brain injury in highof abstention from the offending sporting activityschool athletes. JAMA 1999 Sep 8; 282 (10): 958-63
has been used in some reports as proof of cause and 10. Covassin T, Swanik CB, Sachs ML. Epidemiological considera-tions of concussions among intercollegiate athletes. Appleffect, and this diagnostic and therapeutic methodNeuropsychol 2003; 10 (1): 12-22may be useful in other studies. Also, longer follow-
11. Danis RP, Hu K, Bell M. Acceptability of baseball face guardsup periods of athletes suspected to have MTBI or and reduction of oculofacial injury in receptive youth league
players. Inj Prev 2000 Sep; 6 (3): 232-4degenerative conditions would be valuable assess-12. Rice JO, Walters C, Olson RE, et al. Epidural hematoma afterments. In the cases of sports where possibilities of
minor oral trauma. J Oral Surg 1976 Jul; 34 (7): 639-41long-term effects are considered, such as in football 13. Groleau GA, Tso EL, Olshaker JS, et al. Baseball bat assault
injuries. J Trauma 1993 Mar; 34 (3): 366-72or soccer, improved long-term studies are necessary14. Morse SD. Acute central cervical spinal cord syndrome. Annin order to determine a causal relationship.
Emerg Med 1982 Aug; 11 (8): 436-9This article was intended to assist healthcare 15. Worrell J. BMX bicycles: accident comparison with other mod-
els. Arch Emerg Med 1985 Dec; 2 (4): 209-13professionals in the recognition and assessment of16. Illingworth CM. BMX compared with ordinary bicycle acci-sport-specific CNS injuries. It may serve as a refer-
dents. Arch Dis Child 1985 May; 60 (5): 461-4ence for the physician who encounters athletes with 17. Kronisch RL, Chow TK, Simon LM, et al. Acute injuries in off-
road bicycle racing. Am J Sports Med 1996 Jan-Feb; 24 (1):unique or difficult problems. For physicians not88-93faced with sports-related injuries on a regular basis,
18. Rivara FP, Thompson DC, Thompson RS, et al. Injuries involv-and sports medicine physicians who do not see ing off-road cycling. J Fam Pract 1997 May; 44 (5): 481-5
19. Kronisch RL, Pfeiffer RP, Chow TK, et al. Gender differencesneurological lesions on a regular basis, this articlein acute mountain bike racing injuries. Clin J Sport Med 2002may provide a guide for these mutually distinct May; 12 (3): 158-64
subspecialties. 20. Linn S, Smith D, Sheps S. Epidemiology of bicycle injury, headinjury, and helmet use among children in British Columbia: afive year descriptive study. Canadian Hospitals Injury, Report-Acknowledgements ing and Prevention Program (CHIRPP). Inj Prev 1998 Jun; 4(2): 122-5
No sources of funding were used to assist in the prepara- 21. Shafi S, Gilbert JC, Loghmanee F, et al. Impact of bicycletion of this review. The authors have no conflicts of interest helmet safety legislation on children admitted to a regionalthat are directly relevant to the content of this review. pediatric trauma center. J Pediatr Surg 1998 Feb; 33 (2):
317-2122. Brown PG, Lee M. Trampoline injuries of the cervical spine.
References Pediatr Neurosurg 2000 Apr; 32 (4): 170-51. Steele AG. Emergency medical care for open wheel racing 23. Bradshaw C, McCrory P. Obturator nerve entrapment. Clin J
events at Indianapolis Raceway Park. Ann Emerg Med 1994 Sport Med 1997 Jul; 7 (3): 217-9Aug; 24 (2): 264-8 24. Unterharnscheidt F. About boxing: review of historical and
2. Gennarelli TA. Cerebral concussions and diffuse brain injuries. medical aspects. Tex Rep Biol Med 1970; 28: 421-295In: Cooper PR, editor. Head injury. 2nd ed. Baltimore (MD): 25. Blonstein JL, Clarke E. Further observations on the medicalWilkins and Wilkins, 1987: 108-24 aspects of amateur boxing. BMJ 1957; 1: 362-4
3. Trammell TR, Olivary SE. Crash and injury statistics from Indy-26. Unterharnscheidt F. A neurologist’s reflections on boxing. V.car racing 1985-1989. In: Association for Advancement of
Conclude remarks. Rev Neurol 1995 Sep-Oct; 23 (123):Automotive Medicine. Proceedings of the 34th Annual Con-1027-32ference; 1990 Oct 1-3; Scottsdale (AZ). The Association,
27. Ross RT, Ochsner Jr MG. Acute intracranial boxing-related1991: 329-35injuries in US Marine Corps recruits: report of two cases. Mil4. Holley JE, Butler JW, Mahoney JM. Carbon monoxide poison-Med 1999 Jan; 164 (1): 68-70ing in racing car drivers. J Sports Med Phys Fitness 1999 Mar;
28. Jordan BD, Campbell E. Acute boxing injuries among profes-39 (1): 20-3sional boxers in New York State: a two year survey. Phys5. Jareno A, de la Serna JL, Cercas A, et al. Heat stroke in motorSports Med 1988; 12: 53-67car racing drivers [letter]. Br J Sports Med 1987 Mar; 21 (1):
29. Kelly JP, Nichols JS, Filley CM, et al. Concussion in sports:48guidelines for the prevention of catastrophic outcome. JAMA6. Pasternack JS, Veenema KR, Callahan CM. Baseball injuries: a1991 Nov 27; 266 (20): 2867-9Little League survey. Pediatrics 1996 Sep; 98 (3 Pt 1): 445-8
30. Warden DL, Bleiberg J, Cameron KL, et al. Persistent prolonga-7. Radelet MA, Lephart SM, Rubinstein EN, et al. Survey of thetion of simple reaction time in sports concussion. Neurologyinjury rate for children in community sports. Pediatrics 20022001 Aug 14; 57 (3): 524-6Sep; 110 (3): e28
31. Jordan BD. Neurologic aspects of boxing. Arch Neurol 19878. Cheng TL, Fields CB, Brenner RA, et al. Sports injuries: anApr; 44 (4): 453-9important cause of morbidity in urban youth. District of Co-
lumbia Child/Adolescent Injury Research Network. Pediatrics 32. Roberts AH. Brain damage in boxers. London: Pittman Medical2000 Mar; 105 (3): e32 Scientific Publishing, 1969
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
CNS Injuries in Sport and Recreation 711
33. Haglund Y, Persson HE. Does Swedish amateur boxing lead to 56. Schmitt H, Gerner HJ. Paralysis from sport and diving acci-chronic brain damage? 3. A retrospective clinical neurophysio- dents. Clin J Sport Med 2001 Jan; 11 (1): 17-22logical study. Acta Neurol Scand 1990 Dec; 82 (6): 353-60 57. DeVivo MJ, Sekar P. Prevention of spinal cord injuries that
34. Murelius O, Haglund Y. Does Swedish amateur boxing lead to occur in swimming pools. Spinal Cord 1997 Aug; 35 (8):chronic brain damage? 4. A retrospective neuropsychological 509-15study. Acta Neurol Scand 1991 Jan; 83 (1): 9-13 58. Blitvich JD, McElroy GK, Blanksby BA. Risk reduction in
35. Mendez MF. The neuropsychiatric aspects of boxing. Int J diving spinal cord injury: teaching safe diving skills. J Sci MedPsychiatry Med 1995; 25 (3): 249-62 Sport 2000 Jun; 3 (2): 120-31
36. Critchley M. Medical aspects of boxing, particularly from a 59. Blitvich JD, McElroy GK, Blanksby BA, et al. Characteristicsneurological standpoint. BMJ 1957; 1: 357-62 of ‘low risk’ and ‘high risk’ dives by young adults: risk
reduction in spinal cord injury. Spinal Cord 1999 Aug; 37 (8):37. Jordan BD, Zimmerman RD. Magnetic resonance imaging in553-9amateur boxers. Arch Neurol 1988 Nov; 45 (11): 1207-8
60. Hughes PJ. Internal carotid artery occlusion following sports38. Rodriguez G, Vitali P, Nobili F. Long-term effects of boxingdiving. J R Nav Med Serv 2000; 86 (3): 120-2and judo-choking techniques on brain function. Ital J Neurol
Sci 1998 Dec; 19 (6): 367-72 61. Gierup J, Larsson M, Lennquist S. Incidence and nature ofhorse-riding injuries. Acta Chir Scand 1976; 142: 57-6139. Bodensteiner JB, Schaefer GB. Dementia pugilistica and cavum
septi pellucidi: born to box? Sports Med 1997 Dec; 24 (6): 62. Sorli JM. Equestrian injuries: a five year review of hospital361-5 admissions in British Columbia, Canada. Inj Prev 2000 Mar; 6
(1): 59-6140. Corsellis JAN, Bruton CJ, Freeman-Browne D. The aftermathof boxing. Psychol Med 1973; 3: 270-303 63. Kriss TC, Kriss VM. Equine-related neurosurgical trauma: a
prospective series of 30 patients. J Trauma 1997 Jul; 43 (1):41. Haglund Y, Bergstrand G. Does Swedish amateur boxing lead to97-9chronic brain damage? 2. A retrospective study with CT and
MRI. Acta Neurol Scand 1990 Nov; 82 (5): 297-302 64. Fleming PR, Crompton JL, Simpson DA. Neuro-ophthalmolog-ical sequelae of horse-related accidents. Clin Exp Ophthalmol42. Hof PR, Bouras C, Buee L, et al. Differential distribution of2001 Aug; 29 (4): 208-12neurofibrillary tangles in the cerebral cortex of dementia
pugilistica and Alzheimer’s disease cases. Acta Neuropathol 65. McAbee GN, Ciminera PF. Intracranial hematoma in exper-(Berl) 1992; 85 (1): 23-30 ienced teenage equestrians. Pediatr Neurol 1996 Oct; 15 (3):
235-643. Jordan BD, Relkin NR, Ravdin LD, et al. Apolipoprotein Eepsilon4 associated with chronic traumatic brain injury in 66. Bond GR, Christoph RA, Rodgers BM. Pediatric equestrianboxing. JAMA 1997 Jul 9; 278 (2): 136-40 injuries: assessing the impact of helmet use. Pediatrics 1995
Apr; 95 (4): 487-944. Schmidt ML, Zhukareva V, Newell KL, et al. Tau isoformprofile and phosphorylation state in dementia pugilistica reca- 67. Bixby-Hammett DM. Pediatric equestrian injuries. Pediatricspitulate Alzheimer’s disease. Acta Neuropathol (Berl) 2001 1992 Jun; 89 (6 Pt 2): 1173-6May; 101 (5): 518-24 68. Nelson DE, Bixby-Hammett D. Equestrian injuries in children
45. Otto M, Holthusen S, Bahn E, et al. Boxing and running lead to a and young adults. Am J Dis Child 1992 May; 146 (5): 611-4rise in serum levels of S-100B protein. Int J Sports Med 2000 69. Bixby-Hammett D, Brooks WH. Common injuries in horsebackNov; 21 (8): 551-5 riding: a review. Sports Med 1990 Jan; 9 (1): 36-47
46. Place HM, Ecklund JM, Enzenauer RJ. Cervical spine injury in 70. Turner M, McCrory P, Halley W. Injuries in professional horsea boxer: should mandatory screening be instituted? J Spinal racing in Great Britain and the Republic of Ireland duringDisord 1996 Feb; 9 (1): 64-7 1992-2000. Br J Sports Med 2002 Dec; 36 (6): 403-9
47. Kewalramani LS, Krauss JF. Cervical spine injuries resulting 71. Andermahr J, Schiffer G, Burger C, et al. Spinal injuries infrom collision sports. Int Med Soc Paraplegia 1981; 19: 303-12 jockeys. 2 case reports and review of the literature [in Ger-
48. Boden BP, Tacchetti R, Mueller FO. Catastrophic cheerleading man]. Unfallchirurg 2000 Aug; 103 (8): 688-92injuries. Am J Sports Med 2003; 31: 881-9 72. Tsirikos A, Papagelopoulos PJ, Giannakopoulos PN, et al. De-
49. Upadhyay V, Tan A. Cricketing injuries in children: from the generative spondyloarthropathy of the cervical and lumbartrivial to the severe. N Z Med J 2000 Mar 10; 113 (1105): 81-3 spine in jockeys. Orthopedics 2001 Jun; 24 (6): 561-4
50. Sotiropoulos SV, Jackson MA, Tremblay GF, et al. Childhood 73. Shute N. A super feeling: are there signs of hope in Christopherlawn dart injuries: summary of 75 patients and patient report. Reeve’s modest recovery? US News World Rep 2002 Sep 23;Am J Dis Child 1990 Sep; 144 (9): 980-2 133 (11): 58
51. Tay JS, Garland JS. Serious head injuries from lawn darts. 74. Diamond PT, Gale SD. Head injuries in men’s and women’sPediatrics 1987 Feb; 79 (2): 261-3 lacrosse: a 10 year analysis of the NEISS database. National
Electronic Injury Surveillance System. Brain Inj 2001 Jun; 1552. Hwang V, Shofer FS, Durbin DR, et al. Prevalence of traumatic(6): 537-44injuries in drowning and near drowning in children and adoles-
cents. Arch Pediatr Adolesc Med 2003 Jan; 157 (1): 50-3 75. Webster DA, Bayliss GV, Spadaro JA. Head and face injuries inscholastic women’s lacrosse with and without eyewear. Med53. Katoh S, Shingu H, Ikata T, et al. Sports-related spinal cordSci Sports Exerc 1999 Jul; 31 (7): 938-41injury in Japan (from the nationwide spinal cord injury registry
between 1990 and 1992). Spinal Cord 1996 Jul; 34 (7): 416-21 76. Mueller FO, Blyth CS. A survey of 1981 college lacrosseinjuries. Phys Sports Med 1982; 10: 87-9354. Blanksby BA, Wearne FK, Elliott BC, et al. Aetiology and
occurrence of diving injuries: a review of diving safety. Sports 77. Rimel RW, Nelson WE, Persing JA, et al. Epidural hematoma inMed 1997 Apr; 23 (4): 228-46 lacrosse. Phys Sports Med 1983; 11: 140-4
55. Guiot B, Fessler RG. Complex atlantoaxial fractures. J 78. McCrory PR, Berkovic SF. Second impact syndrome. Neurolo-Neurosurg 1999 Oct; 91 (2 Suppl.): 139-43 gy 1998 Mar; 50 (3): 677-83
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
712 Toth et al.
79. Clarke KS. Prevention: an epidemiologic view. In: Torg JS, high school and collegiate athletes. J Pediatr 2003 May; 142editor. Athletic injuries to the head, neck and face. Philadel- (5): 546-53phia (PA): Lea and Febiger, 1982: 15-26 99. McCrea M. Standardized mental status testing on the sideline
80. Langburt W, Cohen B, Akhthar N, et al. Incidence of concus- after sport-related concussion. J Athl Train 2001 Sep; 36 (3):sion in high school football players of Ohio and Pennsylvania. 274-9J Child Neurol 2001 Feb; 16 (2): 83-5 100. Chen JK, Johnston KM, Frey S, et al. Functional abnormalities
81. Guskiewicz KM, Weaver NL, Padua DA, et al. Epidemiology of in symptomatic concussed athletes: an fMRI study.concussion in collegiate and high school football players. Am J Neuroimage 2004 May; 22 (1): 68-82Sports Med 2000 Sep-Oct; 28 (5): 643-50 101. Naunheim R, McGurren M, Standeven J, et al. Does the use of
82. Meeuwisse WH, Hagel BE, Mohtadi NG, et al. The distribution artificial turf contribute to head injuries? J Trauma 2002 Oct;of injuries in men’s Canada West university football: a 5-year 53 (4): 691-4analysis. Am J Sports Med 2000 Jul-Aug; 28 (4): 516-23 102. Wisniewski JF, Guskiewicz K, Trope M, et al. Incidence of
83. Delaney JS, Lacroix VJ, Leclerc S, et al. Concussions among cerebral concussions associated with type of mouthguard useduniversity football and soccer players. Clin J Sport Med 2002 in college football. Dent Traumatol 2004 Jun; 20 (3): 143-9Nov; 12 (6): 331-8 103. Hodgson VR. Reducing serious injury in sports. Intrascholastic
84. Delaney JS, Lacroix VJ, Leclerc S, et al. Concussions during the Athletic Association, 1980; 7 (2)1997 Canadian Football League season. Clin J Sport Med 2000 104. Pellman EJ, Viano DC, Tucker AM, et al. Concussion in profes-Jan; 10 (1): 9-14 sional football: reconstruction of game impacts and injuries.
85. Alves WM, Rimel RW, Nelson WE. University of Virginia Neurosurgery 2003 Oct; 53 (4): 799-812prospective study of football-induced minor head injuries: 105. Zhang L, Yang KH, King AI. A proposed injury threshold forstatus report. Clin Sports Med 1987; 6: 211-8 mild traumatic brain injury. J Biomech Eng 2004 Apr; 126 (2):
86. Pellman EJ, Powell JW, Viano DC, et al. Concussion in profes- 226-36sional football: epidemiological features of game injuries and 106. Sallis RE, Jones K. Prevalence of headaches in football players.review of the literature: part 3. Neurosurgery 2004 Jan; 54 (1): Med Sci Sports Exerc 2000 Nov; 32 (11): 1820-481-94
107. Gerberich SG, Priest SD, Boen JR, et al. Concussion incidence87. Pellman EJ, Viano DC, Tucker AM, et al. Concussion in profes- and severity in secondary school varsity football players. Am J
sional football: location and direction of helmet impacts: part Public Health 1983; 73: 1370-52. Neurosurgery 2003 Dec; 53 (6): 1328-40
108. McCrory P. Does second impact syndrome exist? Clin J Sport88. Erlanger D, Kaushik T, Cantu R, et al. Symptom-based assess- Med 2001 Jul; 11 (3): 144-9
ment of the severity of a concussion. J Neurosurg 2003 Mar;109. Rabadi MH, Jordan BD. The cumulative effect of repetitive98 (3): 477-84
concussion in sports. Clin J Sport Med 2001 Jul; 11 (3): 194-889. McCrea M, Kelly JP, Randolph C, et al. Immediate neurocogni-
110. Cantu RC, Mueller FO. Catastrophic football injuries:tive effects of concussion. Neurosurgery 2002 May; 50 (5):1977-1998. Neurosurgery 2000 Sep; 47 (3): 673-51032-40
111. Torg JS, Pavlov H, Genuario SE, et al. Neurapraxia of the90. Collins MW, Field M, Lovell MR, et al. Relationship betweencervical spinal cord with transient quadriplegia. J Bone Jointpostconcussion headache and neuropsychological test per-Surg Am 1986; 68: 1354-70formance in high school athletes. Am J Sports Med 2003 Mar-
112. Boockvar JA, Durham SR, Sun PP. Cervical spinal stenosis andApr; 31 (2): 168-73sports-related cervical cord neurapraxia in children. Spine91. McCrea M, Guskiewicz KM, Marshall SW, et al. Acute effects2001 Dec 15; 26 (24): 2709-12and recovery time following concussion in collegiate football
113. Torg JS, Vegso JJ, Sennett B. The National Football Head andplayers: the NCAA Concussion Study. JAMA 2003 Nov 19;Neck Injury Registry: 14-year report on cervical quadriplegia290 (19): 2556-63(1971-1984). Clin Sports Med 1987 Jan; 6 (1): 61-7292. Guskiewicz KM, Ross SE, Marshall SW. Postural stability and
114. Burstein AA, Otis JC, Torg JS. Mechanisms and pathomechan-neuropsychological deficits after concussion in collegiate ath-ics of athletic injuries to the cervical spine. In: Torg JS, editor.letes. J Athl Train 2001 Sep; 36 (3): 263-73Athletic Injuries to the head, neck and face. Philadelphia (PA):93. Lovell MR, Collins MW, Iverson GL, et al. Recovery from mildLea and Febiger, 1982: 139-42concussion in high school athletes. J Neurosurg 2003 Feb; 98
115. Torg JS, Pavlov H, O’Neill MJ, et al. The axial load teardrop(2): 296-301fracture: a biomechanical, clinical and roentgenographic anal-94. Guskiewicz KM, McCrea M, Marshall SW, et al. Cumulativeysis. Am J Sports Med 1991 Jul-Aug; 19 (4): 355-64effects associated with recurrent concussion in collegiate foot-
116. Macgregor DM. Golf related head injuries in children. Emergball players: the NCAA Concussion Study. JAMA 2003 NovMed J 2002 Nov; 19 (6): 576-719; 290 (19): 2549-55
117. Kelly EG. Major injuries occurring during use of a golf cart.95. Macciocchi SN, Barth JT, Littlefield L, et al. Multiple concus-Orthopedics 1996 Jun; 19 (6): 519-21sions and neuropsychological functioning in collegiate football
players. J Athl Train 2001 Sep; 36 (3): 303-6 118. Tung MY, Hong A, Chan C. Golf buggy related head injuries.Singapore Med J 2000 Oct; 41 (10): 504-596. Collins MW, Lovell MR, Iverson GL, et al. Cumulative effects
of concussion in high school athletes. Neurosurgery 2002 Nov; 119. Taniguchi A, Wako K, Naito Y, et al. Wallenberg syndrome and51 (5): 1175-9 vertebral artery dissection probably due to trivial trauma dur-
ing golf exercise [in Japanese]. Rinsho Shinkeigaku 1993 Mar;97. Collins MW, Grindel SH, Lovell MR, et al. Relationship be-33 (3): 338-40tween concussion and neuropsychological performance in col-
lege football players. JAMA 1999 Sep 8; 282 (10): 964-70 120. Jamieson DR, Ballantyne JP. Unique presentation of a prolapsed98. Field M, Collins MW, Lovell MR, et al. Does age play a role in thoracic disk: Lhermitte’s symptom in a golf player. Neurolo-
recovery from sports-related concussion? A comparison of gy 1995 Jun; 45 (6): 1219-21
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
CNS Injuries in Sport and Recreation 713
121. Ekin JA, Sinaki M. Vertebral compression fractures sustained 145. Honey CR. Brain injury in ice hockey. Clin J Sport Med 1998during golfing. Mayo Clin Proc 1993; 68: 566-70 Jan; 8 (1): 43-6
122. Sachdev P. Golfers’ cramp: clinical characteristics and evidence 146. Wennberg RA, Tator CH. National Hockey League reportedagainst it being an anxiety disorder. Mov Disord 1992 Oct; 7 concussions, 1986-87 to 2001-02. Can J Neurol Sci 2003; 30:(4): 326-32 206-9
123. Noguchi T. A survey of spinal cord injuries resulting from sport. 147. Goodman D, Gaetz M, Meichenbaum D. Concussions in hock-Paraplegia 1994 Mar; 32 (3): 170-3 ey: there is cause for concern. Med Sci Sports Exerc 2001 Dec;
33 (12): 2004-9124. Bailes JE, Hadley MN, Quigley MR, et al. Management ofathletic injuries of the cervical spine and spinal cord. Neuro- 148. Tegner Y, Lorentzon R. Concussion among Swedish elite icesurgery 1991 Oct; 29 (4): 491-7 hockey players. Br J Sports Med 1996 Sep; 30 (3): 251-5
125. Mueller FO, Cantu RC. Catastrophic injuries and fatalities in 149. Biasca N, Simmen HP, Bartolozzi AR, et al. Review of typicalhigh school and college sports, fall 1982-spring 1988. Med Sci ice hockey injuries. Survey of the North American NHL andSports Exerc 1990 Dec; 22 (6): 737-41 Hockey Canada versus European leagues. Unfallchirurg 1995
May; 98 (5): 283-8126. Konermann W, Sell S. The spine: a problem area in highperformance artistic gymnastics: a retrospective analysis of 24 150. Sahjpaul RL, Abdulhak MM, Drake CG, et al. Fatal traumaticformer artistic gymnasts of the German A team [in German]. vertebral artery aneurysm rupture: case report. J NeurosurgSportverletz Sportschaden 1992 Dec; 6 (4): 156-60 1998 Nov; 89 (5): 822-4
127. Furnival RA, Street KA, Schunk JE. Too many pediatric tram- 151. Benson BW, Mohtadi NG, Rose MS, et al. Head and neckpoline injuries. Pediatrics 1999 May; 103 (5): E57 injuries among ice hockey players wearing full face shields vs
half face shields. JAMA 1999 Dec 22-29; 282 (24): 2328-32128. Smith GA. Injuries to children in the United States related totrampolines, 1990-1995: a national epidemic. Pediatrics 1998 152. Tator CH, Carson JD, Cushman R. Hockey injuries of the spineMar; 101 (3 Pt 1): 406-12 in Canada, 1966-1996. CMAJ 2000 Mar 21; 162 (6): 787-8
129. Silver JR, Silver DD, Godfrey JJ. Trampolining injuries of the 153. Tator CH, Carson JD, Edmonds VE. New spinal injuries inspine. Injury 1986 Mar; 17 (2): 117-24 hockey. Clin J Sport Med 1997 Jan; 7 (1): 17-21
130. Smith GA, Shields BJ. Trampoline-related injuries to children. 154. Molsa JJ, Tegner Y, Alaranta H, et al. Spinal cord injuries in iceArch Pediatr Adolesc Med 1998 Jul; 152 (7): 694-9 hockey in Finland and Sweden from 1980 to 1996. Int J Sports
Med 1999 Jan; 20 (1): 64-7131. Torg JS, Das M. Trampoline and minitrampoline injuries to thecervical spine. Clin Sports Med 1985 Jan; 4 (1): 45-60 155. Tator CH, Edmonds VE. National survey of spinal injuries in
hockey players. CMAJ 1984 Apr 1; 130 (7): 875-80132. Torg JS. Trampoline-induced quadriplegia. Clin Sports Med1987 Jan; 6 (1): 73-85 156. Tator CH, Edmonds VE, Lapczak L, et al. Spinal injuries in ice
133. Wechsler B, Kim H, Hunter J. Trampolines, children, and hockey players, 1966-1987. Can J Surg 1991 Feb; 34 (1): 63-9strokes. Am J Phys Med Rehabil 2001 Aug; 80 (8): 608-13 157. Varlotta GP, Lager SL, Nicholas S, et al. Professional roller
134. Sinha A, McGlone RG, Montgomery K. Study of aeroball hockey injuries. Clin J Sport Med 2000 Jan; 10 (1): 29-33injuries. Br J Sports Med 1997 Sep; 31 (3): 200-4 158. Hutchinson MR, Milhouse C, Gapski M. Comparison of injury
135. Foray J, Abrassart S, Femmy T, et al. Hang-gliding accidents in patterns in elite hockey players using ice versus in-line skates.high mountains. Apropos of 200 cases [in French]. Chirurgie Med Sci Sports Exerc 1998 Sep; 30 (9): 1371-31991; 117 (8): 613-7 159. Naunheim RS, Standeven J, Richter C, et al. Comparison of
136. Lautenschlager S, Karli U, Matter P. Paragliding accidents: a impact data in hockey, football, and soccer. J Trauma 2000prospective analysis in Swiss mountain regions [in German]. Z May; 48 (5): 938-41Unfallchir Versicherungsmed 1993; Suppl. 1: 55-65 160. Schieber RA, Branche-Dorsey CM, Ryan GW. Comparison of
137. Sim FH, Chao EY. Injury potential in modern ice hockey. Am J in-line skating injuries with rollerskating and skateboardingSports Med 1978; 6: 378-84 injuries. JAMA 1994 Jun 15; 271 (23): 1856-8
138. Gerberich SG, Finke R, Madden M, et al. An epidemiologic 161. Nguyen D, Letts M. In-line skating injuries in children: astudy of high school ice hockey injuries. Child Nerv Syst 1987; 10-year review. J Pediatr Orthop 2001 Sep-Oct; 21 (5): 613-83: 59-64 162. Osberg JS, Schneps SE, Di Scala C, et al. Skateboarding: more
139. Jorgensen V, Schmidt-Olsen S. The epidemiology of ice hockey dangerous than roller skating or in-line skating. Arch Pediatrinjuries. Br J Sports Med 1986; 20: 7-9 Adolesc Med 1998 Oct; 152 (10): 985-91
140. Molsa J, Airaksinen O, Nasman O, et al. Ice hockey injuries in 163. United States Consumer Product Safety Commission. NEISSFinland: a prospective epidemiologic study. Am J Sports Med data highlights. Washington, DC: United States Consumer1997 Jul-Aug; 25 (4): 495-9 Product Safety Commission, 1985; 12: 1-4
141. Juhn MS, Brolinson PG, Duffey T, et al. American Osteopathic 164. Gartland S, Malik MH, Lovell ME. Injury and injury rates inAcademy of Sports Medicine (AOASM) position statement. Muay Thai kick boxing. Br J Sports Med 2001 Oct; 35 (5):Violence and injury in ice hockey. Clin J Sport Med 2002; 12 308-13(1): 46-51 165. Pieter W, Zemper ED. Incidence of reported cerebral concus-
142. Schick DM, Meeuwisse WH. Injury rates and profiles in female sion in adult taekwondo athletes. J R Soc Health 1998 Oct; 118ice hockey players. Am J Sports Med 2003 Jan-Feb; 31 (1): (5): 272-947-52 166. Pieter W, Zemper ED. Head and neck injuries in young
143. Reid SR, Losek JD. Factors associated with significant injuries taekwondo athletes. J Sports Med Phys Fitness 1999 Jun; 39in youth ice hockey players. Pediatr Emerg Care 1999 Oct; 15 (2): 147-53(5): 310-3 167. Pentore R, Nichelli P. De-afferented state syndrome (locked-in
144. Biasca N, Wirth S, Tegner Y. The avoidability of head and neck syndrome) following sudden cervical sprain trauma during ainjuries in ice hockey: an historical review. Br J Sports Med karate training session [in Italian]. Riv Neurol 1991 Mar-Apr;2002 Dec; 36 (6): 410-27 61 (2): 66-70
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
714 Toth et al.
168. Lannuzel A, Moulin T, Amsallem D, et al. Vertebral-artery 191. Seward H, Orchard J, Hazard H, et al. Football injuries indissection following a judo session: a case report. Neuropedia- Australia at the elite level. Med J Aust 1993; 159: 298-301trics 1994 Apr; 25 (2): 106-8 192. Marshall SW, Spencer RJ. Concussion in rugby: the hidden
169. McCarron MO, Patterson J, Duncan R. Stroke without dissec- epidemic. J Athl Train 2001 Sep; 36 (3): 334-8tion from a neck holding manoeuvre in martial arts. Br J Sports 193. McCrory PR, Ariens T, Berkovic SF. The nature and duration ofMed 1997 Dec; 31 (4): 346-7 acute concussive symptoms in Australian football. Clin J Sport
170. Meairs S, Timpe L, Beyer J, et al. Acute aphasia and hemiplegia Med 2000 Oct; 10 (4): 235-8during karate training. Lancet 2000 Jul 1; 356 (9223): 40 194. McIntosh AS, McCrory P, Comerford J. The dynamics of con-
171. Pary LF, Rodnitzky RL. Traumatic internal carotid artery dis- cussive head impacts in rugby and Australian rules football.section associated with taekwondo. Neurology 2003; 60: Med Sci Sports Exerc 2000 Dec; 32 (12): 1980-41392-3
195. Pettersen JA. Does rugby headgear prevent concussion? Atti-172. Echaniz-Laguna A, Fleury MC, Petrow P, et al. Internal carotid tudes of Canadian players and coaches. Br J Sports Med 2002
artery dissection caused by a kick during French boxing [in Feb; 36 (1): 19-22French]. Presse Med 2001; 30: 683
196. McIntosh AS, McCrory P. Effectiveness of headgear in a pilot173. Malek AM, Halbach VV, Phatouros CC, et al. Endovascularstudy of under 15 rugby union football. Br J Sports Med 2001treatment of a ruptured intracranial dissecting vertebral aneu-Jun; 35 (3): 167-9rysm in a kickboxer. J Trauma 2000; 48: 143-5
197. McIntosh A, McCrory P, Finch CF. Performance enhanced174. Godt P, Vogelsang H. Uncommon judo injuries: cervical discheadgear: a scientific approach to the development of protec-herniation and acute high cervical cord damage associated withtive headgear. Br J Sports Med 2004 Feb; 38 (1): 46-9congenital stenosis of the cervical spinal canal (author’s transl)
198. Pettersen JA, Skelton RW. Glucose enhances long-term declara-[in German]. Unfallheilkunde 1979 May; 82 (5): 215-8tive memory in mildly head-injured varsity rugby players.175. DeVera-Reyes JA. Three cases of chronic subdural hematomaPsychobiology 2000; 28: 81-9caused by the practice of judo. Acta Luso Esp Neurol Psiquiatr
199. Quarrie KL, Cantu RC, Chalmers DJ. Rugby union injuries to1970; 29: 53-6the cervical spine and spinal cord. Sports Med 2002; 32 (10):176. Koiwai EK. Fatalities associated with judo. Phys Sportsmed633-531981; 9: 61-6
200. Scher AT. Rugby injuries to the cervical spine and spinal cord: a177. Stiller JW, Weinberger BR. Boxing and chronic brain damage.10-year review. Clin Sports Med 1998 Jan; 17 (1): 195-206Psychiatr Clin North Am 1985; 8: 339-56
178. Varley GW, Spencer-Jones R, Thomas P, et al. Injury patterns in 201. Newton HB. Neurologic complications of scuba diving. Ammotorcycle road racers: experience on the Isle of Man Fam Physician 2001 Jun 1; 63 (11): 2211-81989-1991. Injury 1993 Aug; 24 (7): 443-6 202. Kohshi K, Katoh T, Abe H, et al. Neurological accidents caused
179. Chapman MA, Oni J. Motor racing accidents at Brands Hatch, by repetitive breath-hold dives: two case reports. J Neurol Sci1988/9. Br J Sports Med 1991 Sep; 25 (3): 121-3 2000 Sep 1; 178 (1): 66-9
180. Horner CH, O’Brien AA. Motorcycle racing injuries on track 203. Murrison AW, Glasspool E, Pethybridge RJ, et al. Elec-and road circuits in Ireland. Br J Sports Med 1986 Dec; 20 (4): troencephalographic study of divers with histories of neurolog-157-8 ical decompression illness. Occup Environ Med 1995 Jul; 52
181. Schusman LC, Lutz LJ. Mountaineering and rock climbing (7): 451-3accidents. Phys Sports Med 1982; 10: 52-61 204. Sipinen SA, Ahovuo J, Halonen JP. Electroencephalography
182. Foulke G. Altitude related illness. Am J Emerg Med 1985; 3: and magnetic resonance imaging after diving and decompres-217-26 sion incidents: a controlled study. Undersea Hyperb Med 1999
183. Hackett PH. High altitude cerebral edema and acute mountain Summer; 26 (2): 61-5sickness: a pathophysiology update. Adv Exp Med Biol 1999; 205. Reuter M, Tetzlaff K, Hutzelmann A, et al. MR imaging of the474: 23-45 central nervous system in diving-related decompression ill-
184. Hackett PH, Yarnell PR, Hill R, et al. High-altitude cerebral ness. Acta Radiol 1997 Nov; 38 (6): 940-4edema evaluated with magnetic resonance imaging: clinical
206. Lorenz J, Brooke ST, Petersen R, et al. Brainstem auditorycorrelation and pathophysiology. JAMA 1998 Dec 9; 280 (22):evoked potentials during a helium-oxygen saturation dive to1920-5450 meters of seawater. Undersea Hyperb Med 1995 Sep; 22
185. Butterwick DJ, Hagel B, Nelson DS, et al. Epidemiologic analy- (3): 229-40sis of injury in five years of Canadian professional rodeo. Am J
207. Wilmshurst P, Bryson P. Relationship between the clinicalSports Med 2002 Mar-Apr; 30 (2): 193-8features of neurological decompression illness and its causes.186. Nebergall R. Rodeo. In: Calne PJ, Caine CG, Lindner KJ,Clin Sci (Lond) 2000 Jul; 99 (1): 65-75editors. Epidemiology of sports injuries. Champaign (IL):
208. Walsh KP, Wilmshurst PT, Morrison WL. Transcatheter closureHuman Kinetics, 1996: 350-6of patent foramen ovale using the Amplatzer septal occluder to187. Butterwick DJ, Nelson DS, LaFave MR, et al. Epidemiologicalprevent recurrence of neurological decompression illness inanalysis of injury in one year of Canadian professional rodeo.divers. Heart 1999 Mar; 81 (3): 257-61Clin J Sport Med 1996 Jul; 6 (3): 171-7
209. Murrison A, Glasspool E, Francis J, et al. Somatosensory188. Butterwick DJ, Meeuwisse WH. Effect of experience on rodeoevoked potentials in acute neurological decompression illness.injury. Clin J Sport Med 2002 Jan; 12 (1): 30-5J Neurol 1995 Oct; 242 (10): 669-76189. Orchard J, Wood T, Seward H, et al. Comparison of injuries in
210. Appenzeller O. Sportsman’s headache. Migraine Matters 1985;elite senior and junior Australian football. J Sci Med Sport3: 33-51998 Jun; 1 (2): 83-8
190. Orchard J. AFL 1996 injury report. Melbourne: Australian 211. Pestronk A, Pestronk S. Goggle migraine. N Engl J Med 1983;Football League Medical Officers Association, 1995: 7-8 308: 226-7
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)
CNS Injuries in Sport and Recreation 715
212. Genelin A, Kathrein A, Daniaux A, et al. Current status of spinal 233. Federiuk CS, Schlueter JL, Adams AL. Skiing, snowboarding,injuries in winter sports [in German]. Schweiz Z Med Trau- and sledding injuries in a northwestern state. Wilderness Envi-matol 1994; (1): 17-20 ron Med 2002 Winter; 13 (4): 245-9
213. Myles ST, Mohtadi NG, Schnittker J. Injuries to the nervous 234. Shorter NA, Mooney DP, Harmon BJ. Childhood sleddingsystem and spine in downhill skiing. Can J Surg 1992 Dec; 35 injuries. Am J Emerg Med 1999 Jan; 17 (1): 32-4(6): 643-8
235. Beilman GJ, Brasel KJ, Dittrich K, et al. Risk factors and214. Yamakawa H, Murase S, Sakai H, et al. Spinal injuries in patterns of injury in snowmobile crashes. Wilderness Environ
snowboarders: risk of jumping as an integral part of Med 1999 Winter; 10 (4): 226-32snowboarding. J Trauma 2001 Jun; 50 (6): 1101-5
236. Farley DR, Orchard TF, Bannon MP, et al. The care and cost of215. Tarazi F, Dvorak MF, Wing PC. Spinal injuries in skiers and
snowmobile-related injuries. Minn Med 1996 Dec; 79 (12):snowboarders. Am J Sports Med 1999 Mar-Apr; 27 (2):
21-5177-80
237. Russell A, Boop FA, Cherny WB, et al. Neurologic injuries216. Prall JA, Winston KR, Brennan R. Spine and spinal cord injuriesassociated with all-terrain vehicles and recommendations forin downhill skiers. J Trauma 1995 Dec; 39 (6): 1115-8protective measures for the pediatric population. Pediatr
217. Kondoh T, Kurihara E, Kohmura E. Cervical epidural hemato- Emerg Care 1998 Feb; 14 (1): 31-5ma after snowboarding injury: case report. Neurol Med Chir
238. Lister DG, Carl III J, Morgan III JH, Denning DA, et al.(Tokyo) 2002 Dec; 42 (12): 550-3Pediatric all-terrain vehicle trauma: a 5-year statewide experi-218. Seino H, Kawaguchi S, Sekine M, et al. Traumatic paraplegia inence. J Pediatr Surg 1998 Jul; 33 (7): 1081-3snowboarders. Spine 2001 Jun 1; 26 (11): 1294-7
239. Janda DH, Bir CA, Cheney AL. An evaluation of the cumulative219. Nakaguchi H, Fujimaki T, Ueki K, et al. Snowboard headconcussive effect of soccer heading in the youth population. Injinjury: prospective study in Chino, Nagano, for two seasonsControl Saf Promot 2002 Mar; 9 (1): 25-31from 1995 to 1997. J Trauma 1999 Jun; 46 (6): 1066-9
240. Tysvaer AT. Head and neck injuries in soccer: impact of minor220. Macnab AJ, Cadman R. Demographics of alpine skiing andtrauma. Sports Med 1992 Sep; 14 (3): 200-13snowboarding injury: lessons for prevention programs. Inj
Prev 1996 Dec; 2 (4): 286-9 241. Kawanishi A, Nakayama M, Kadota K. Heading injury precipi-221. Levy AS, Hawkes AP, Hemminger LM, et al. An analysis of tating subdural hematoma associated with arachnoid cysts: two
head injuries among skiers and snowboarders. J Trauma 2002 case reports. Neurol Med Chir (Tokyo) 1999 Mar; 39 (3):Oct; 53 (4): 695-704 231-3
222. Hentschel S, Hader W, Boyd M. Head injuries in skiers and 242. Prabhu VC, Bailes JE. Chronic subdural hematoma complicat-snowboarders in British Columbia. Can J Neurol Sci 2001 Feb; ing arachnoid cyst secondary to soccer-related head injury:28 (1): 42-6 case report. Neurosurgery 2002 Jan; 50 (1): 195-7
223. O’Neill DF, McGlone MR. Injury risk in first-time 243. Bruzzone E, Cocito L, Pisani R. Intracranial delayed epiduralsnowboarders versus first-time skiers. Am J Sports Med 1999 hematoma in a soccer player: a case report. Am J Sports MedJan-Feb; 27 (1): 94-7 2000 Nov-Dec; 28 (6): 901-3
224. Nakaguchi H, Tsutsumi K. Mechanisms of snowboarding-relat-244. Matser JT, Kessels AG, Lezak MD, et al. A dose-responseed severe head injury: shear strain induced by the opposite-
relation of headers and concussions with cognitive impairmentedge phenomenon. J Neurosurg 2002 Sep; 97 (3): 542-8in professional soccer players. J Clin Exp Neuropsychol 2001
225. Fukuda O, Takaba M, Saito T, et al. Head injuries in Dec; 23 (6): 770-4snowboarders compared with head injuries in skiers: a pro-
245. Matser EJ, Kessels AG, Lezak MD, et al. Neuropsychologicalspective analysis of 1076 patients from 1994 to 1999 in Niiga-impairment in amateur soccer players. JAMA 1999 Sep 8; 282ta, Japan. Am J Sports Med 2001 Jul-Aug; 29 (4): 437-40(10): 971-3226. Johnson SM, Johnson AC, Barton RG. Avalanche trauma and
246. Kirkendall DT, Jordan SE, Garrett WE. Heading and headclosed head injury: adding insult to injury. Wilderness Environinjuries in soccer. Sports Med 2001; 31 (5): 369-86Med 2001 Winter; 12 (4): 244-7
227. Bridges EJ, Rouah F, Johnston KM. Snowblading injuries in 247. Boden BP, Lin W, Young M, Mueller FO. Catastrophic injuriesEastern Canada. Br J Sports Med 2003 Dec; 37 (6): 511-5 in wrestlers. Am J Sports Med 2002 Nov-Dec; 30 (6): 791-5
228. Wright Jr JR, McIntyre L, Rand JJ, Hixson EG. Nordic ski 248. Acikgoz B, Ozgen T, Erbengi A, et al. Wrestling causingjumping injuries: a survey of active American jumpers. Am J paraplegia. Paraplegia 1990 May; 28 (4): 265-8Sports Med 1991 Nov-Dec; 19 (6): 615-9
249. Snook GA. A survey of wrestling injuries. Am J Sports Med229. Wright Jr JR, Hixson EG, Rand JJ. Injury patterns in nordic ski 1980; 8: 450-3
jumpers: a retrospective analysis of injuries occurring at the250. Rogers L, Sweeney PJ. Stroke: a neurological complication ofIntervale Ski Jump Complex from 1980 to 1985. Am J Sports
wrestling: a case of brainstem stroke in a 17-year-old athlete.Med 1986 Sep-Oct; 14 (5): 393-7Am J Sports Med 1979; 7: 352-4230. Wester K. Serious ski jumping injuries in Norway. Am J Sports
Med 1985 Mar-Apr; 13 (2): 124-7231. Dubravcic-Simunjak S, Pecina M, Kuipers H, et al. The inci- Correspondence and offprints: Dr Cory Toth, Department of
dence of injuries in elite junior figure skaters. Am J SportsClinical Neurosciences, University of Calgary, Room 128,Med 2003; 31: 511-8Heritage Medical Research Building, 3330 Hospital Drive232. Cummings Jr RS, Shurland AT, Prodoehl JA, et al. Injuries inNW, Calgary, AB T2N 4N1, Canada.the sport of luge: epidemiology and analysis. Am J Sports Med
1997 Jul-Aug; 25 (4): 508-13 E-mail: [email protected]
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (8)