Embed Size (px)
Citation preview

Case Presentations
Anamika B. Mukherjee, MD
September 13, 2017

Disclosures
• Nothing to disclose

Learning Objectives
• Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening HIE infants for therapeutic hypothermia
• Understand which newborns should receive therapeutic hypothermia and when
• Review the process for stabilizing infants with asphyxia

Case
• Baby girl F, born to a 35 year old G5P4 mother with good antenatal care. This pregnancy complicated by GDM, diet control
• Blood group O positive; Hep B neg: HIV neg: RPR neg: Rubella immune: GBS negative
• Mom admitted at 37+2 weeks with active vaginal bleeding
• US showed placental abruption

NICU Team attends the delivery . . .
• Infant was delivered via emergency C-section
• the baby was floppy with no respiratory effort, cyanotic and had no detectable heart rate
• Bag and mask ventilation started immediately, HR > 100 bpm at 5 min, and intermittent spontaneous breathes noted at 5 min. She was intubated at 7 min of life for poor sustained respiration. Color improved, HR 110 bpm but baby remained floppy at 10 min. Apgar score 0@1 min; 4@ 5 min; 5@ 10 min.
What should you ask OB/L&D staff in the DR?

Get cord blood gas
Answer: ask OB/L&D staff to send cord blood gas
Cord arterial gas: pH 6.8, PCO2 103, Bicarb 15 and BD19.7
• Cord blood gas provides critical information regarding the severity and/or duration of hypoxic ischemic insults prior to delivery
• Cord arterial gas (from UA) is a part of the criteria for assessment for hypothermia treatment
• If cord blood gas is not available, get infant ABG within first hour of life.

Physical examination
• Weight 3720gms (>90%), OFC 35.5 cm (90%), Length 54.4 (>90%)
• Temperature 36.5oC
• HR 170 bpm, BP 37/23 mmHg.
• Pale and poor perfusion
• Intubated on mechanical SIMV with periodic respiratory effort
• No significant dysmorphic features
What is your assessment and what should be done next?

Goals of Resuscitation
• Avoid hypoxia and hyperoxia
– Initiate low concentration FiO2 and increase FiO2 to 1.0 if chest compressions required; wean FiO2 as soon as HR recovers
• Avoid hyperthermia in the delivery room
– in moderate – severe HIE; hyperthermia is associated with adverse neurologic outcomes
• Avoid hypoglycemia and hyperglycemia
• Recognize and treat seizures

Lab tests
Your initial lab work should include following:
A. Check blood glucose
B. CBC
C. Blood Culture
D. Basic metabolic panel
E. LFTs
F. Coagulation tests

Lab tests
Answer: All above
• Correcting hypoglycemia is critical for brain protection
• Mom had placenta abruption, HCT and platelet count will help to determine if blood product transfusion is indicated
• Increase in creatinine indicates kidney injury, and elevation of LFTs and coagulopathy indicates liver damage

Lab results
• Cord arterial gas: pH 6.8, PCO2 103, Bicarb 15 and BD 19.7.
• Blood glucose 15
• CBC: WBC 17.7k, HCT 30%, platelet count 141K
• Creatinine 1.3
• AST 945, ALT 220
• PT/PTT/INR significant prolonged

One hour later, fluid boluses were given, blood pressure improved, hypoglycemia was corrected. Infant started to have spontaneous respiration effort and movements and her tone improved.
Your next treatment plan include:
A. Start hypothermia treatment ASAP
B. Obtain brain imaging to confirm hypoxic-ischemic brain injury before starting hypothermia treatment
C. Continue monitoring. Hypothermia will not be indicated if infant’s condition significantly improved at 6hr of life.

Early Screening and Identification of
Candidates for Neonatal Therapeutic
Hypothermia Toolkit Released February 2015
Priya Jegatheesan, MD, Anna Morgan, MD, Thomas Shimotake, MD, Dongli
Song, MD, PhD and Krisa Van Meurs, MD on behalf of the Perinatal Quality
Improvement Panel (PQIP), California Perinatal Quality Care Collaborative
(CPQCC)
download \Toolkit @ www.cpqcc.org


Neurological examination
Does this infant display encephalopathy?
How should the neurological examination be done/documented to show this?

Diagnosis of Neonatal
Encephalopathy is Clinical
• Careful history and neurological exam
• Laboratory studies to exclude “mimics” of hypoxia-ischemia
– Metabolic abnormalities
• including inborn errors of metabolism
– Infection
– Acute bilirubin encephalopathy
– Stroke

Neonatal Neurologic Exam
• Most challenging aspect for community providers
• Experience helps – signs of neonatal encephalopathy and/or asphyxia can be subtle/subclinical
• Observation over time, NE may be progressive – Serial exams are necessary
– Document accurate timing of exam
– “Non-focal” or “normal” inadequate
• Staging system (modified Sarnat) – Important in deciding course of management
– Sarnat stage correlates with childhood outcomes

NE Staging predicts outcomes
Table showing degree of encephalopathy to establish the pretest probability of poor outcome
• Presence of moderate to severe NE best predictor of death/severe handicap at 2.5 years (sensitivity=96%) Levene MI, Lancet 1986
• Severity of NE and the presence of seizures can predict 30 month neurodevelopmental outcome, as early as DOL#1. Miller SP, AJOG 2004

Modified Sarnat Exam
Level of consciousness Hyperalert Lethargic stuporous
Tone Normal Hypotonia Flaccid
Posture Mild distal flexion Strong distal flexion decerebrate
Activity Normal Decreased none
Primitive reflexes suck Moro
weak strong
weak or absent Incomplete
absent absent
Autonomic function pupils heart rate respiration
dilated Tachycardia Normal
constricted Bradycardia periodic
variable Variable apnea
Modified from Sarnat and Sarnat, Arch Neurol, 1976

Management of babies who qualify for possible cooling
• Identify patients to discuss with regional cooling center within 1 hour of birth – After initial resuscitation and stabilization, perform screening evaluation – If screening criteria are met, call the regional cooling center – Discuss if the patient is appropriate to remain for observation vs. transport
for cooling – If determined to be a candidate for cooling by regional cooling center,
begin passive cooling
• Turn down/off external heat sources and avoid hyperthermia – Document the time and do not actively cool patients
• Monitor core (rectal) temp closely – Target rectal temp= 33-34⁰C or axillary temp=32-33⁰C – Check temp continuously/frequently (q 15 minutes) Use flow sheet
(appendix H) – Core temp may still fall <33.5⁰C with passive cooling. Be prepared to
respond – Maintain adequate sedation

Management of babies who qualify for possible cooling (cont)
• Secure vascular access – Before peripheral vasoconstriction occurs with cooling – Umbilical venous and arterial access preferred – Periph IV at a minimum
• Maintain adequate sedation – Keep comfortable/minimize cold stress and avoid shivering during passive
cooling – i.v. morphine
• Treat only clinical seizures – no prophylactic antiepileptic drugs – Lorazepam (Ativan): 0.1 mg/kg/dose IV, repeat 1X prn for suspected
seizures – Phenobarbital: 20 mg/kg/ IV load, for obvious seizures
• Monitor electrolytes closely – fluctuations often seen in CA, K, Mg levels with cooling

Exclusion Criteria
• Infants ≤ 36 weeks gestation (based > 34 weeks considered for cooling at the discretion of the cooling center)
• Infants without evidence or clinical history of HIE
• Inability to initiate cooling by 6 hours of age
• Congenital or chromosomal anomaly
• Refusal of consent by parent or physician
• Severe intrauterine growth restriction (weight ≤ 1800 grams)
• Infants in extremis for which no additional intensive therapy will be offered by attending neonatologist

Decision to Initiate hypothermia
• Evidence of moderate or severe encephalopathy (abnormalities in ≥ 3 categories) on Sarnat exam
• Laboratory/historical criteria for HIE are met
– Add LLUCH blood gas and historical date
• Newborns with laboratory or historical data making them potentially eligible with a normal initial Sarnat exam should be examined hourly for changes in the Sarnat exam

NICHD Trial Protocol for Whole-Body Hypothermia and Re-Warming
Inclusion Criteria: • Infants will be evaluated using two steps
– Biochemical criteria (Step 1A), Clinical (Step 1B), – Neurological (Step 2)
• Infants must meet BOTH Steps (1 and 2) and not meet any exclusion criteria to be eligible for therapeutic hypothermia
• Clinical and Biochemical criteria
– History of an acute perinatal event – Apgar score ≤ 5 at 10 minutes of life – Cord pH or any postnatal blood gas pH of ≤7.0 at ≤1 hour – Base deficit on cord gas or any postnatal blood gas of ≥16 mEq/L at ≤ 1
hour – Continued need for mechanical ventilation imitated at birth and
continued for at least 10 minutes
Shankaran S et al., NICHD Trial, NEJM 2005

STEP 1B: IF BLOOD GAS IS NOT AVAILABLE (Or pH 7.01-7.15 or Base Deficit 10 - 15 mEq/L)
• Acute perinatal event (i.e. abruptio placenta, cord prolapse, severe fetal heart rate abnormalities such as variable or late decelerations),
• Moderate to severe encephalopathy (one or more at any time) within 6 hours of birth): – lethargy or obtundation, stupor or coma (not due to anti-epileptic medications
and maternal magnesium sulfate exposure) – hypotonia or hypertonia (not due to anti-epileptic medications and maternal
magnesium sulfate exposure) – Increased, decreased or absent reflexes (e.g. DTR, gag, grasp, absent or weak
suck) – Autonomic dysfunction (decreased or absent respirations, low resting HR <
100 bpm with rare accelerations to 120 bpm, pupillary constriction (even in dim light, fixed and dilated pupils
– clinical seizures – abnormal aEEG background and/or electrographic seizures
• AND – Apgar score ≤5 at 10 minutes of life
• OR – Continued need for ventilation initiated at birth and continued for at least 10
minutes

4 hours after hypothermia initiated. . .
• Infant develops bradycardia HR 70s
• What should you do?
• What are the most common side effects of hypothermia?

Adverse effects
• Bradycardia • Prolonged QT • Thrombocytopenia • Skin breakdown • Hypocalcemia • Hypokalemia • Metabolic acidosis • Coagulopathy • Clotting • PPHN • Hypotension

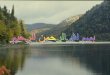
aEEG at 4 hours of life

After 72 hours of hypothermia, rewarming has started the aEEG shows

Neonatal Seizures are Common
• Neonatal seizures are common
and often suggest underlying brain injury or dysfunction
• 50-60% of patients in RCTs • Seen commonly during the first 12 hours of
life and during the rewarming phase of cooling • Birth is most common time of life to
have seizures – 0.95/1000 term births in California
(OSWHPD database) Glass HC, et al J Peds, 2008
• Other estimates – 0.7 - 2.7 / 1000 live births at term – 57.5 -132 / 1000 live birth in preterms

Detecting Seizures by Exam
• Neonatal seizures are often subtle or subclinical
• Only 21% of neonatal seizures on EEG had clinical signs
– Electrographic only events are common
– More in babies with frequent seizures, especially after anti-seizure treatment
• Average accuracy of seizure detections was 50%
– Doctors no better than bedside nurses
Clancy, Epilepsia 1988 Scher , Pediatr Neurol 2003 Malone, Epilepsia 2009

Hypothermia treatment
• Neonatal encephalopathy is a neurological emergency.
• Brain injury evolves over time.
• Biphasic nature of cell death (Gluckman PD, et al 1992): Primary neuronal death (cell hypoxia/primary energy failure). Latent period – at least 6 hours. Secondary phase - delayed neuronal death begins.

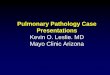
Effect of hypothermia on the hypoxic-ischemic cascade of events
Lina F. Chalak Neoreviews 2016;17:e463-e470

Cooling Trials: Meta-analyses
Control (%) Cooling (%)
Death/moderate-severe disability 62 44
CP 30 19
Visual impairment 14 7
Hearing loss 6 4
11 RCT: n = 1505, combined death/disability at 18 months RRR = 0.75 (95% CI 0.68-0.83) NNTB7= 7 (95% CI 5 – 10)
Jacobs, Cochrane Reviews 2013

Best patient care depends on
• Close communication with family
• Multidisciplinary care
• Neurology– neurological examination (structured /routine), diagnosis, prognosis, follow up
• Radiology – timing and interpretation
• Physical and occupational therapy – evaluation, pre-discharge examination

Alternative Approaches: What about longer cooling and / or deeper cooling?
• NICHD optimizing cooling trial: to determine whether longer cooling (120 hours) or deeper cooling (32.0C) or both is superior to cooling at 33.5C for 72 hours in babies with HIE
Results – Deeper cooling or longer cooling compared with
hypothermia at 33.5C for 72 hours did not further reduce NICU deaths
– Cooling at 32C was associated with more inhaled nitric oxide use and ECMO therapy, and associated with higher incidence arrhythmia and anuria

Recognizing Neonatal Encephalopathy (NE)
• Not always obvious – index of suspicion based on risk factors
• Expect 4:1 ratio of babies with acidosis/acute events to NE
• Send cord gases after every high risk delivery or NE case
– Obs as likely to be sued for not checking cord gases as for having bad ones
– Sometimes the gases indicate non-HI cause of NE exonerating OB

Case • 38-weeks gestation male infant is delivered by emergency C-section
for recurrent late decelerations and moderate variability. • Infant is born apneic, floppy and cyanotic, HR 70 bpm • Apgars are 2,3,8 at 1, 5 and 10 minutes • Infant is intubated and placed on mechanical ventilation. Initial
arterial blood gas obtained at 15 minutes of age: pH 6.8, PCO2 55, PO2 90, base excess -20.
• Baby has seizure-like activity with lip smacking and decorticate posturing.
• Neurologic exam: flaccid infant with absent deep tendon reflexes, absent suck and absent gag, The aEEG prior to any sedation or antiepileptic medication is severely suppressed. Would you cool this baby?

Case 2
You attend the delivery of a 34 weeks gestational age infant with history of fetal distress (poor variability and late decelerations) Apgar scores: 3/4/7 at 1/5/10 minutes The baby has minimal response to PPV via bag mask. The baby is then intubated FiO2 35% and transferred to the NICU. Initial ABG at 30 minutes of life; pH 6.9, PCO2 66, PO2 80, base excess -18. At 1 hour of life, the infant develops repetitive jerking of the right upper extremity. Infant is lethargic with mild hypotonia and a weak suck, consistent with Sarnat stage II. The aEEG demonstrates low voltage and seizure activity. How would you proceed with the management of this infant?

Case 3
You are about to receive a 39 week gestational age male infant born at a community hospital for evaluation for therapeutic hypothermia. Birth history: Emergency C-section 2nd to maternal seizures with preeclampsia. APGARs: 0, 3, and 3 at 1, 5 and 10 minutes with a cord gas pH<7 and BE -16. Infant was intubated in the DR and initial gas at 1hr of life was pH 6.76/pCO2 112/pO2 93 and BE -17. Follow-up ABG 45 minutes later was 7.32/38/81/-6. aEEG showed continuous background and no seizures clinically or on aEEG. Neurologic exam: hyperalert infant with normal to increased tone, normal to increased reflexes, active suck and exaggerated Moro, consistent with Sarnat stage 1. How would you proceed in the management of this infant?

Questions?