Embed Size (px)
Citation preview

Pulmonary Pathology Case
Presentations
Kevin O. Leslie. MD
Mayo Clinic Arizona

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
PulmCase 1

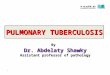
Clinical history
A 65-year-old woman presents with a one year history of bilateral lung lesions. The lesions are said to wax and wane in size and distribution. There is mild hilar and mediastinal adenopathy. Chest imaging reveals multiple lung nodules of variable size, the largest measures 1.5 cm.
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease


Case 1-1

Case 1-2

Case 1-3

Case 1-4

Case 1-5

Case 1-6

Case 1-7

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
What is the pattern?
1. Acute injury
2. Fibrosis
3. Cellular infiltrates
4. Alveolar filling
5. Nodules
6. Minimal changes

What is your “favored” diagnosis?
1. Lymphoid interstitial pneumonia (LIP)
2. Wegener granulomatosis
3. Intraparenchymal lymph node
4. Lymphomatoid granulomatosis (LYG)
5. Focal lymphoid hyperplasia
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
PulmCase 2

Clinical history
A 18-year-old high school student, captain of the
junior varsity track and field team, presents with one
week of rapidly progressive shortness of breath
accompanied by night sweats and fever. She is
hospitalized and requires intubation.
Chest imaging shows bilateral asymmetrical
ground-glass opacities.
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease





A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
What is the pattern?
1. Acute injury
2. Fibrosis
3. Cellular infiltrates
4. Alveolar filling
5. Nodules
6. Minimal changes

What is your “favored” diagnosis?
1. Acute granulomatous infection
2. Bronchiolitis obliterans organising pneumonia (BOOP)
3. Eosinophilic pneumonia
4. Acute viral pneumonitis
5. Cryptogenic organizing pneumonia
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
PulmCase 3

A Pattern-Based Approach to Diffuse Parenchymal Lung
Disease
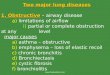
Clinical history
A 47-year-old man presents with unexplained
persistent cough. Constitutional symptoms
are mild, with minimal shortness of breath on
exertion. Chest imaging shows sharply
defined areas of ground-glass attenuation.


Case 4-1

Case 4-4

Case 4-7

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
What is the pattern?
1. Acute injury
2. Fibrosis
3. Cellular infiltrates
4. Alveolar filling
5. Nodules
6. Minimal changes

What is your “favored”
diagnosis?
1. Pulmonary oedema
2. Pneumocystis pneumonia
3. Alveolar proteinosis
4. Pneumoconiosis (Aluminosis)
5. Drug toxicity
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
PulmCase 4

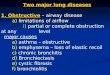
Clinical history
A 52-year-old woman presents with progressive shortness of breath accompanied by non-productive cough. The patient feels her pulmonary problems began following a bout of apparent community acquired pneumonia 1 year earlier.
Chest imaging reveals patchy ground-glass opacities alternating with zones of normal appearing lung. Expiratory views appear to enhance infiltrates.
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease

Inspiratory CT
Expiratory CT

Case 5-1

Case 5-3

Case 5-4

Case 5-5

Case 5-7

Case 5-6

Case 5-8

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
What is the pattern?
1. Acute injury
2. Fibrosis
3. Cellular infiltrates
4. Alveolar filling
5. Nodules
6. Minimal changes

What is your “favored”
diagnosis?
1. Pulmonary hypertension
2. Chronic small airways disease
3. Lymphangitic carcinoma
4. Lymphangioleiomyomatosis (LAM)
5. Sampling error
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
PulmCase 5

Clinical history
A 44-year-old woman presents with a four
month history of cough accompanied by
shortness of breath on exertion.
Chest imaging shows miliary small
centrolobular nodules involving the mid and
upper lung zones, bilaterally.
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease


Case 6-1

Case 6-10

Case 6-3

Case 6-11

Case 6-4

Case 6-5

Case 6-6

Case 6-7

Case 6-9

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
What is the pattern?
1. Acute injury
2. Fibrosis
3. Cellular infiltrates
4. Alveolar filling
5. Nodules
6. Minimal changes

What is your “favored”
diagnosis?
1. Sarcoidosis
2. Atypical mycobacterial infection
3. Hypersensitivity pneumonia
4. IV drug abuse
5. Cryptogenic organising pneumonia (COP)
A Pattern-Based Approach to Diffuse Parenchymal Lung
Disease

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
PulmCase 6

Clinical history
A 36-year-old woman presents for follow-up
screening one year after being diagnosed and
treated for invasive ductal adenocarcinoma of the
right breast.
Imaging reveals miliary bilateral nodules involving
the mid and upper lung zones.
A Pattern-Based Approach to Diffuse Parenchymal Lung
Disease


Case 8-2

Case 8-3

Case 8-4

Case 8-5

Case 8-6

A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
What is the pattern?
1. Acute injury
2. Fibrosis
3. Cellular infiltrates
4. Alveolar filling
5. Nodules
6. Minimal changes

What is your “favored” diagnosis
1. Metastatic carcinoma
2. Mixed dust pneumoconiosis
3. Langerhans cell histiocytosis
4. Sarcoidosis
5. Capillary hemangiomatosis
A Pattern-Based Approach to Diffuse Parenchymal Lung
Disease


A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
PulmCase 8

Clinical history
A 49-year-old woman with inflammatory bowel disease presents with progressive shortness of breath accompanied by fatigue. Four weeks before admission to the hospital she had begun a new regimen for treatment of her inflammatory bowel disease.
Chest imaging shows bilateral asymmetrical ground-glass infiltrates involving all lung zones. The patient's respiratory condition deteriorates and she requires mechanical ventilation.
A Pattern-Based Approach to Diffuse Parenchymal Lung
Disease
PulmCase 8






A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease
What is the pattern?
1. Acute injury
2. Fibrosis
3. Cellular infiltrates
4. Alveolar filling
5. Nodules
6. Minimal changes

What is your “favored” diagnosis?
1. Diffuse alveolar damage (DAD)
2. Organising pneumonia (OP)
3. Cryptogenic organising pneumonia (COP)
4. Nonspecific interstitial pneumonia (NSIP)
5. Usual interstitial pneumonia (UIP)
A Pattern-Based Approach to Diffuse Parenchymal
Lung Disease