Embed Size (px)
Citation preview
© 2018 Cascade Dafo, Inc. All rights reserved. 27
NOTE: If you don’t choose an option, you will receive the Standard.
PosteriorHeight: c ⅔ to ¾ of leg length
Standard c Specify:
Plastic: c Polyethylene (Transfer Pattern is not an option) (Standard to 8” foot length)
c Co-poly (Transfer Pattern is not an option) (Standard above 8” foot length)
c Polypro
Inner Liner: c Softy foam Standard
(white only) c Polyethylene
c Add extra navicular padding
Straps: c Elastic removable d-ring strap Standardc Non-stretch removable d-ring strapc Non-stretch d-ring strap riveted to medial/lateral sides
c Add toe abduction strapStrapColor: c White
Standard c Other:
InstepPattern: c
No pattern Standard c Other:
Special Instructions
Thank you!
Shi
ppin
g
c Shipping info is the same as practitioner facility. –OR–
Shipping contact name:
Street address:
City: State: Zip:
c Rush order (adds $25)
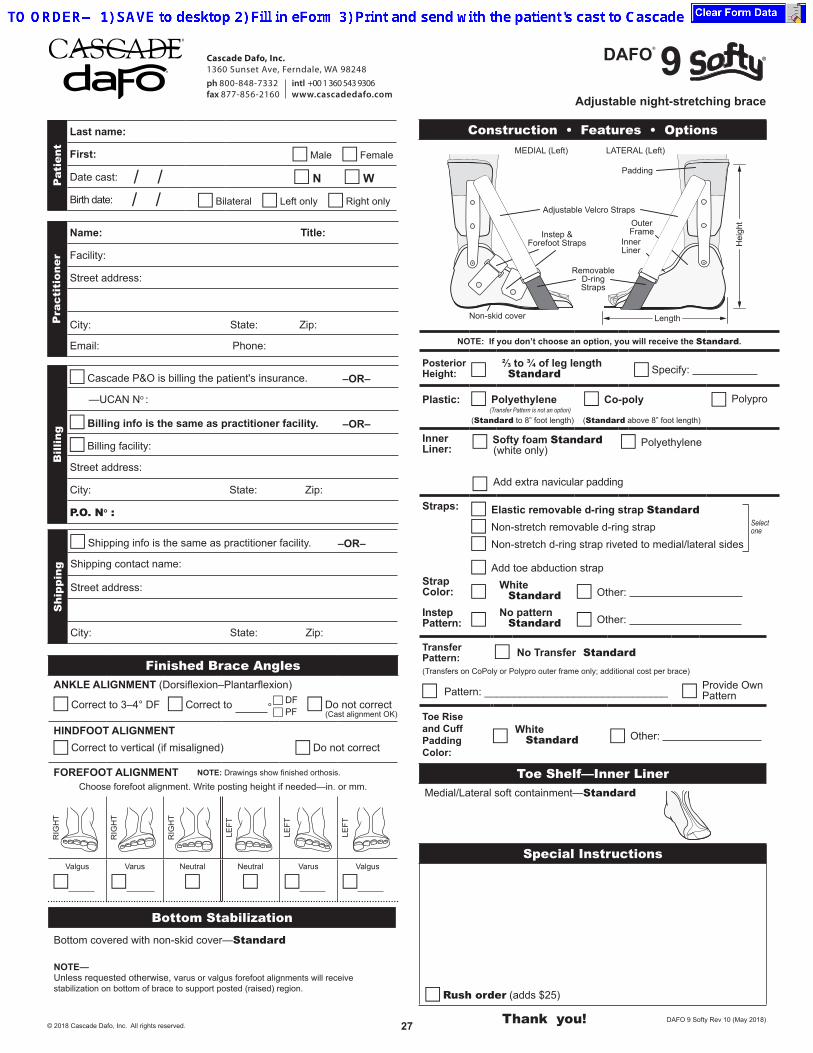
Construction • Features • Options
Pat
ient
Last name:
First: c Male c Female
Date cast: / / c N c W
Birth date: / / c Bilateral c Left only c Right only
Pra
ctit
ione
r
Name: Title:
Facility:
Street address:
City: State: Zip: Email: Phone:
Bill
ing
c Cascade P&O is billing the patient's insurance. –OR–
—UCAN No :
c Billing info is the same as practitioner facility. –OR–
c Billing facility:
Street address:
City: State: Zip:
P.O. No :
Toe Shelf—Inner LinerMedial/Lateral soft containment—Standard
DAFO 9 Softy Rev 10 (May 2018)
Adjustable night-stretching brace
Bottom StabilizationBottom covered with non-skid cover—Standard
NOTE— Unless requested otherwise, varus or valgus forefoot alignments will receive stabilization on bottom of brace to support posted (raised) region.
MEDIAL (Left) LATERAL (Left)
Hei
ght
Length
Adjustable Velcro Straps
InnerLiner
OuterFrame
Non-skid cover
Padding
Instep &Forefoot Straps
RemovableD-ringStraps
DAFO® 9
Select one
Finished Brace AnglesANKLE ALIGNMENT (Dorsiflexion–Plantarflexion)
c Correct to 3–4° DF c Correct to ° c Do not correct
HINDFOOT ALIGNMENTc Correct to vertical (if misaligned) c Do not correct
FOREFOOT ALIGNMENT NOTE: Drawings show finished orthosis.
Choose forefoot alignment. Write posting height if needed—in. or mm.
RIG
HT
RIG
HT
RIG
HT
LEFT
LEFT
LEFT
Valgus
c
Varus
c
Neutral
cNeutral
cVarus
c
Valgus
c
(Cast alignment OK)
c DFc PF
Cascade Dafo, Inc.1360 Sunset Ave, Ferndale, WA 98248ph 800-848-7332 intl +00 1 360 543 9306fax 877-856-2160 www.cascadedafo.com
TransferPattern: c No Transfer Standard (Transfers on CoPoly or Polypro outer frame only; additional cost per brace)
c Pattern: _______________________________ c Provide Own Pattern
Toe Rise and Cuff Padding Color:
c White Standard c Other: