Embed Size (px)
Citation preview

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 1/101
CardiovascularSystem

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 2/101
Chest pain
Assessment of patients with suspected cardiacchest pain
NICE issued guidelines in 2010 on the 'Assessment and diagnosis of recentonset chest pain or discomfort of suspected cardiac origin'.
Patients presenting with acute chest pain
immediate management of suspected acute coronary syndrome ACS!
• "lyceryl trinitrate
•Aspirin #00mg. Nice do not recommend giving other antiplatelet agents (i.e.Clopidogrel) outside of hospital
• $o not routinely give o%ygen& only give if sats ()*+
• ,erform an ecg as soon as possi-le -ut do not delay transfer tohospital. A normal ecg does not e%clude ACS
eferral
• Current chest pain or chest pain in the last 12 hours /ith an a-normalEC" emergency admission
• Chest pain 122 hours ago refer to hospital the sameday forassessment
• Chest pain 3 2 hours ago perform full assessment /ith EC" and
troponin measurement -efore deciding upon further action
+NICE suggest the follo/ing in terms of oxygen therapy
• $o not routinely administer o%ygen& -ut monitor o%ygen saturationusing pulse o%imetry as soon as possi-le& ideally -efore hospitaladmission. 4nly o5er supplemental o%ygen to
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 3/101
,eople /ith o%ygen saturation spo2! of less than ()* /ho are
not at ris6 of hypercapnic respiratory failure& aiming for spo2 of94-98%
,eople /ith chronic o-structive pulmonary disease /ho are at
ris6 of hypercapnic respiratory failure& to achieve a target spo2of 88-92% until -lood gas analysis is availa-le.
Patients presenting with stabe chest pain
7ith all due respect to NICE the guidelines for assessment of patients /ithsta-le chest pain are rather complicated. 8hey suggest an approach /herethe ris6 of a patient having coronary artery disease CA$! is calculated -asedon their symptoms /hether they have typical angina& atypical angina or
nonangina chest pain!& age& gender and ris6 factors.
NICE de9ne angina pain as the follo/ing
!. "onstricting discomfort in the front of the chest# nec$#shouders# aw or arms
&. Precipitated by physica exertion
'. (eie)ed by rest or *+, in about minutes
,atients /ith all # features have typical angina
,atients /ith 2 of the a-ove features have atypical angina
,atients /ith 1 or none of the a-ove features have nonangina chest
pain
If patients have typical anginal symptoms and a risk of CAD is greater than90* then no further diagnostic testing is re:uired. It should -e noted that allmen over the age of 70 years /ho have typical anginal symptoms fall into
this category.
;or patients /ith an estimated ris6 of 10(0* the follo/ing investigations arerecommended. Note the a-sence of the e%ercise tolerance test
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 4/101
stimated
i$eihood of "AD
Diagnostic testing
/!-90% Coronary angiography'0-/0% ;unctional imaging& for e%ample
• <yocardial perfusion scan /ith S,EC8
• Stress echocardiography
• ;irstpass contrastenhanced magnetic
resonance <! perfusion
• < imaging for stressinduced /all motion
a-normalities.
!0-&9% C8 calcium scoring
,ulses
Pusus parodoxus
•"reater than the normal 10 mm=g! fall in systolic -lood pressureduring inspiration > faint or a-sent pulse in inspiration
• evere asthma! cardiac tamponade
1ow-rising2pateau
• Aortic stenosis
"oapsing
• Aortic regurgitation
• "atent ductus arteriosus
• #yperkinetic (anemia! thyroto$icosis! fever! e$ercise%pregnancy)
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 5/101
Pusus aternans
• egular alternation of the force of the arterial pulse
1e)ere 35
Bisferiens puse
• '$ou-le pulse' t/o systolic pea6s
• &i$ed aortic valve disease
67er$y6 puse
• =ypertrophic o-structive cardiomyopathy+
+=4C< may occasionally -e associated /ith a -isferiens pulse
=eart sounds
8he 9rst heart sound S1! is caused -y closure of the mitral and tricuspidvalves /hilst the second heart sound S2! is due to aortic and pulmonaryvalve closure
1!
• Closure of mitral and tricuspid valves
• Soft if long , or mitral regurgitation
• ?oud in mitral stenosis
1&
• Closure of aortic and pulmonary valves
• Soft in aortic stenosis
• Splitting during inspiration is normal
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 6/101
1' third heart sound
• Caused -y diastolic 9lling of the ventricle
• Considered normal if #0 years old may persist in /omen up to @0years old!
• =eard in left ventricular failure e.g. $ilated cardiomyopathy!&constrictive pericarditis called a pericardial 6noc6!
14 fourth heart sound
• <ay -e heard in aortic stenosis& =4C<& hypertension
• Caused -y atrial contraction against a sti5 ventricle
• In =4C< a dou-le apical impulse may -e felt as a result of a palpa-leS)
=eart sounds S2
S2 is caused -y the closure of the aortic valve A2! closely follo/ed -y that of
the pulmonary valve ,2!
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 7/101
"auses of a oud 1&
• =ypertension systemicloud A2! or pulmonaryloud ,2!
• =yperdynamic states
• Atrial septal defect /ithoutpulmonary hypertension
"auses of a soft 1&
• Aortic stenosis
"auses of :xed spit 1&
• Atrial septal defect
"auses of a widey spit 1&
• $eep inspiration
•
• ,ulmonary stenosis
• Severe mitral regurgitation
Dr.Afsana BhuiyanSource ,assmed
"auses of a re)ersed
paradoxica spit 1&
P& occurs before A&
• ?
• Severe aortic stenosis
• ight ventricular pacing

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 8/101
<urmurs
EBection systolic
• Aortic stenosis
• ,ulmonary stenosis& =4C<
• AS$& ;allot's
=olosystolic pansystolic!
• <itraltricuspid
regurgitation highpitchedand '-lo/ing' in character!
• DS$ 'harsh' in character!
?ate systolic
• <itral valve prolapse
•
Coarctation of aorta
Early diastolic
• Aortic regurgitation highpitched and '-lo/ing' in character!
• "rahamSteel murmur pulmonary regurgitation& again highpitchedand '-lo/ing' in character!
<idlate diastolic
• <itral stenosis 'rum-ling' in character!
• Austin;lint murmur severe aortic regurgitation& again is 'rum-ling' incharacter!
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 9/101
Continuous machineli6e mumur
• ,atent ductus arteriosus
Adult advanced life support
8he Boint European esuscitation Council and esuscitation Council F!2010 guidelines do not alter signi9cantly from the 200@ guidelines. ,leasesee the lin6 for more details& -elo/ is only a very -rief summary of 6eypoints changes.
<aBor points include
• atio of chest compressions to ventilation is #02
• Chest compressions are no/ continued /hile a de9-rillator is charged
• $uring a D;D8 cardiac arrest& adrenaline 1 mg is given once chestcompressions have restarted after the third shoc6 and then every #@minutes during alternate cycles of C,!. In the 200@ guidelines&adrenaline /as given Bust -efore the third shoc6. Amiodarone #00 mgis also given after the third shoc6
• Atropine is no longer recommended for routine use in asystole orpulseless
Electrical activity ,EA!.
• A single shoc6 for D;pulseless D8 follo/ed -y 2 minutes of C,& ratherthan a series of # shoc6s follo/ed -y 1 minute of C,
• Asystolepulselesselectrical activity should -e treated /ith 2 minutes
of C,& rather than #& prior to reassessment of the rhythm
• $elivery of drugs via a tracheal tu-e is no longer recommended
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 10/101
• ;ollo/ing successful resuscitation o%ygen should -e titrated to achievesaturations of ()(G*. 8his is to address the potential harm caused -yhypero%aemia
+++8he a-sence of a carotid pulse in the presence of sinus tachycardiaindicates that this is a nonshoc6a-le rhythm& and the appropriate algorithmshould -e follo/ed as e%plained -elo/. 8he only shoc6a-le rhythms areventricular 9-rillation and ventricular tachycardia.
Syncope
Syncope may -e de9ned as a transient loss of consciousness due to glo-alcere-ral hypoperfusion /ith rapid onset& short duration and spontaneouscomplete recovery. Note ho/ this de9nition e%cludes other causes of collapsesuch as epilepsy.
8he European Society of Cardiology pu-lished guidelines in 200( on the
investigation and management of syncope. 8hey suggested the follo/ingclassi9cation
(e;ex syncope neuray mediated
• Dasovagal triggered -y emotion& pain or stress. 4ften referred to as'fainting'
• Situational cough& micturition& gastrointestinal
• Carotid sinus syncope
<rthostatic syncope
• ,rimary autonomic failure ,ar6inson's disease& ?e/y -ody dementia
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 11/101
• Secondary autonomic failure e.g. $ia-etic neuropathy& amyloidosis&uraemia
• $ruginduced diuretics& alcohol& vasodilators
• Dolume depletion haemorrhage& diarrhoea
"ardiac syncope
• Arrhythmias -radycardias sinus node dysfunction& AD conductiondisorders! or tachycardias supraventricular& ventricular!
• Structural valvular& myocardial infarction& hypertrophic o-structivecardiomyopathy
• 4thers pulmonary em-olism
eHe% syncope is the most common cause in all age groups althoughorthostatic and cardiac causes -ecome progressively more common in olderpatients.
Evaluation
• Cardiovascular e%amination
Postura bood pressure readings= a symptomatic fa insystoic BP > &0 mm?g or diastoic BP > !0 mmhg or decreasein systoic BP @ 90 mm?g is considered diagnostic
• EC"
• Carotid sinus massage
• 8ilt ta-le test
• 2) hour EC"
,eriarrest rhythms tachycardia
8he 2010 esuscitation Council F! guidelines have simpli9ed the advicegiven for the management of periarrest tachycardias. Separate algorithms
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 12/101
for the management of -roadcomple% tachycardia& narro/ comple%tachycardia and atrial 9-rillation have -een replaced -y one uni9edtreatment algorithm;ollo/ing -asic AC assessment& patients are classi9ed as -eing sta-le orunsta-le according to the presence of any adverse signs
• Shoc6 hypotension systolic -lood pressure (0 mmhg!& pallor&s/eating&
Cold& clammy e%tremities& confusion or impaired consciousness
• Syncope
• <yocardial ischaemia
• =eart failure
If any of the a-ove adverse signs are present then synchronised $C shoc6sshould -e given 8reatment follo/ing this is given according to /hether the S comple% isnarro/ or -road and /hether the rhythm is regular or irregular. 8he fulltreatment algorithm can -e found at the esuscitation Council /e-site&-elo/ is a very limited summary
Broad-compex tachycardia
'egular Assume ventricular tachycardia unless previously con9rmed SD8 /ith
-undle -ranch -loc6! ?oading dose of amiodarone follo/ed -y 2) hour infusion
rregular A; /ith -undle -ranch -loc6 treat as for narro/ comple% tachycardia
,olymorphic D8 e.g. 8orsade de pointes! ID magnesium
,arrow-compex tachycardia
'egular
Dagal manoeuvres follo/ed -y ID adenosine If a-ove unsuccessful consider diagnosis of atrial Hutter and control
rate e.g. eta-loc6ers!rregular
,ro-a-le atrial 9-rillation
If onset )G hr consider electrical or chemical cardioversion
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 13/101
ate control e.g. eta-loc6er or digo%in! and anticoagulation
,eriarrest rhythms -radycardia
8he 2010 esuscitation Council F! guidelines emphasise that the
management of -radycardia depends on
!. dentifying the presence of signs indicating haemodynamiccompromise - 6ad)erse signs6
&. dentifying the potentia ris$ of asystoe
Ad)erse signs
8he follo/ing factors indicate haemodynamic compromise and hence the
need for treatment
• Shoc6 hypotension systolic -lood pressure (0 mmhg!& pallor&s/eating&
Cold& clammy e%tremities& confusion or impaired consciousness
• Syncope
• <yocardial ischaemia
• =eart failure
Atropine is the 9rst line treatment in this situation. If this fails to /or6& orthere is the potential ris6 of asystole then transvenous pacing is indicated
Potentia ris$ of asystoe 8he follo/ing indicate a potential ris6 of asystole and hence the need fortreatment /ith transvenous pacing
• Complete heart -loc6 /ith -road comple% S
• ecent asystole
• <o-itJ type II AD -loc6
• Dentricular pause 3 # seconds
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 14/101
If there is a delay in the provision of transvenous pacing the follo/inginterventions may -e used
• Atropine& up to ma%imum of #mg
• 8ranscutaneous pacing
• Adrenaline infusion titrated to response
Dentricular tachycardia
Dentricular tachycardia D8! is -roadcomple% tachycardia originating from aventricular ectopic focus. It has the potential to precipitate ventricular9-rillation and hence re:uires urgent treatment.
8here are t/o main types of D8 onomorphic + most commonly caused -y myocardial infarction
Poymorphic + A su-type of polymorphic D8 is torsades de pointes
/hich is precipitated -y prolongation of the 8 interval. 8he causes ofa long 8 interval are listed -elo/
"auses of a proonged C+ inter)a
"ongenita Drugs <ther
7er)e-3ange-
,iesen syndrome
incudes deafness
and is due to an
abnorma
potassium channe
(omano-ard
syndrome nodeafness
amiodarone&
sotalol& class 1a
antiarrhythmic
drugs tricyclic
antidepressants&
Huo%etine chloro:uine
terfenadine
erythromycin
electrolyte
hypocalcaemia&
hypo6alaemia&
hypomagnesaemia acute myocardial
infarction myocarditis
hypothermia
su-arachnoid
haemorrhage
anagement
If the patient has adverse signs systolic , (0 mmhg& chest pain& heart
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 15/101
failure or rate 3 1@0 -eatsmin! then immediate cardioversion is indicated. Inthe a-sence of such signs antiarrhythmics may -e used. If these fail& thenelectrical cardioversion may -e needed /ith synchronised $C shoc6s
$rug therapy
• Amiodarone ideally administered through a central line
• ?idocaine use /ith caution in severe left ventricular impairment
• ,rocainamide
erapami shoud ,<+ be used in +
If drug therapy fails
• Electrophysiological study E,S!
• Implant a-le cardioverterde9-rillator IC$! this is particularlyindicated in patients /ith signi9cantly impaired ?D function
+++=ypo6alemia is the most important cause of ventricular tachycardia D8!
clinically& follo/ed -y hypomagnesaemia. Severe hyper6alaemia may causeD8 in certain circumstances& for e%ample in patients /ith structural heartdisease& -ut it is not as common a cause as hypo6alemia.
8orsades de pointes
8orsades de pointes 't/isting of the points'! is a rare arrhythmia associated/ith a long 8 interval. It may deteriorate into ventricular 9-rillation and
hence lead to sudden death
Causes of long 8 interval
• Congenital Kervell?angeNielsen syndrome& omano7ard syndrome
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 16/101
• Antiarrhythmics amiodarone& sotalol& class 1a antiarrhythmic drugs
• 8ricyclic antidepressants
• Antipsychotics
• Chloro:uine
• 8erfenadine
• Erythromycin
• Electrolyte hypocalcaemia& hypo6alaemia& hypomagnesaemia
• <yocarditis
• =ypothermia
• Su-arachnoid haemorrhage
<anagement
• ID magnesium sulphate
Supraventricular tachycardia
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 17/101
7hilst strictly spea6ing the term supraventricular tachycardia SD8! refers toany tachycardia that is not ventricular in origin the term is generally used inthe conte%t of paro%ysmal SD8. Episodes are characterised -y the suddenonset of a narro/ comple% tachycardia& typically an atrioventricular nodal re
entry tachycardia ADN8!. 4ther causes include atrioventricular reentrytachycardias AD8! and Bunctional tachycardias.
Acute management
• Dagal manoeuvres e.g. Dalsalva manoeuvre
• Intravenous adenosine Lmg > 12mg > 12mg contraindicated inasthmatics verapamil is a prefera-le option
• Electrical cardioversion
,revention of episodes
• eta-loc6ers
• adiofre:uency a-lation
Atrial 9-rillationrate control and maintenance
of sinus rhythm
8he oyal College of ,hysicians and NICE pu-lished guidelines on the
management of atrial 9-rillation A;! in 200L. 8he follo/ing is also -ased onthe Boint American =eart Association A=A!& American College of CardiologyACC! and European Society of Cardiology ESC! 2012 guidelines
Agents used to control rate in patients /ith atrial 9-rillation
Beta-boc$ers
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 18/101
"acium channe boc$ers
Digoxin not considered :rst-ine anymore as they are esseEecti)e at controing the heart rate during exercise.?owe)er# they are the preferred choice if the patient has
coexistent heart faiure
Agents used to maintain sinus rhythm in patients /ith a history of atrial9-rillation
1otao
Amiodarone
5ecainide
<thers ess commony used in FG= disopyramide# dofetiide#procainamide# propafenone# Huinidine
8he ta-le -elo/ indicates some of the factors /hich may -e considered /henconsidering either a rate control or rhythm control strategy
5actors fa)ouring rate
contro
5actors fa)ouring rhythm contro
4lder than L@ years
=istory of ischaemic heartdisease
7ith contraindications to
antiarrhythmic drugs.
nsta-le for cardioversion.
Mounger than L@ years
Symptomatic;irst presentation
?one A; or A; secondary to a corrected
precipitant e.g. Alcohol!
Congestive heart failure
8he 9rst thing is to determine the type of A;& so here are some importantsimpli9ed! de9nitions.
• Acute onset /ithin the previous )G hours.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 19/101
• ,aro%ysmal spontaneous termination /ithin seven days and mostoften /ithin )G hours.
• ecurrent t/o or more episodes.
• ,ersistent not selfterminating lasting longer than seven days& orprior cardioversion.
• ,ermanent longstanding A; de9ned as over a year! that is notsuccessfully terminated -y
Atrial 9-rillation anticoagulation
NICE updated their guidelines on the management of atrial 9-rillation A;! in201). 8hey suggest using the "?A&D1&-)asc score to determine the most
appropriate anticoagulation strategy. 8his scoring system superceded theC=A$S2 score.
(is$ factor Poin
ts
" Congestive heart failure 1
? =ypertension or treated hypertension! 1
A
&
Age 3O @ years 2
Age L@) years 1
D $ia-etes 11
&
,rior Stro6e or 8IA 2
Dascular disease including ischaemic heart disease and
peripheral arterial disease!
1
1 Se% female! 1
8he ta-le -elo/ sho/s a suggested anticoagulation strategy -ased on thescore
1core Anticoaguation
0 No treatment
! <ales Consider anticoagulation
;emales No treatment this is -ecause their score of 1 is only
reached due to their gender!
& or 45er anticoagulation
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 20/101
more
NICE recommend that /e o5er patients a choice of anticoagulation& including/arfarin and the novel oral anticoagulants noacs!. 8here are complicatedrules surrounding /hich N4AC is licensed for /hich ris6 factor these can -e
found in the NICE guidelines. Aspirin is no longer recommended for reducingstro6e ris6 in patients /ith A;
$octors have al/ays thought carefully a-out the ris6-ene9t pro9le ofstarting someone on /arfarin. A history of falls& old age& alcohol e%cess and ahistory of previous -leeding are common things that ma6e us consider/hether /arfarinisation is in the -est interests of the patient. NICE no/recommend /e formalise this ris6 assessment using the =AS?E$ scoringsystem.
8here are no formal rules on ho/ /e act on the =AS?E$ score although a
score of 3O # indicates a 'high ris6' of -leeding& de9ned as intracranial
haemorrhage& hospitalisation& haemoglo-in decrease 32 g?& andor
transfusion.
Atrial 9-rillation pharmacological cardioversion
Dr.Afsana BhuiyanSource ,assmed
Atrial fibrillation - cardioversion: amiodarone +
(is$ factor Points
? =ypertension& uncontrolled& systolic , 3 1L0
mmhg
1
A A-normal renal function dialysis or creatinine 3
200!
4r
A-normal liver function cirrhosis& -iliru-in 3 2
times normal& A?8AS8A?, 3 # times normal
1 for any renal
a-normalities
1 for any liver
a-normalities
1 Stro6e& history of 1
B leeding& history of -leeding or tendency to -leed 1
3 ?a-ile inrs unsta-lehigh inrs& time in therapeuticrange L0*!
1
Elderly 3 L@ years! 1
D $rugs ,redisposing to leeding Antiplatelet agents&
nsaids!
4r
Alcohol se 3G drin6s/ee6!
1 for drugs
1 for alcohol

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 21/101
8he oyal College of ,hysicians and NICE pu-lished guidelines on themanagement of atrial 9-rillation A;! in 200L. 8he follo/ing is also -ased onthe Boint American =eart Association A=A!& American College of CardiologyACC! and European Society of Cardiology ESC! 2012 guidelinesAgents /ith proven ePcacy in the pharmacological cardioversion of atrial
9-rillation
Amiodarone
5ecainide if no structura heart disease
<thers ess commony used in FG= Huinidine# dofetiide#ibutiide# propafenone
?ess e5ective agents
• eta-loc6ers including sotalol!
• Calcium channel -loc6ers
• $igo%in
• $isopyramide
• ,rocainamide
Atrial 9-rillation cardioversion
8here are t/o scenarios /here cardioversion may -e used in atrial9-rillation
• Electrical cardioversion as an emergency if the patient is
haemodynamically unsta-le
• Electrical or pharmacological cardioversion as an elective procedure/here a rhythm control strategy is preferred.
8he notes -elo/ refer to cardioversion -eing used in the elective scenario forrhythm control. 8he /ording of the 201) NICE guidelines is as follo/s
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 22/101
*er rate or rhythm control if the onset of the arrhythmia is less than +,hours! and start rate control if it is more than +, hours or is uncertain
<nset @ 48 hours
If the atrial 9-rillation A;! is de9nitely of less than )G hours onset patientsshould -e heparinised. ,atients /ho have ris6 factors for ischaemic stro6eshould -e put on lifelong oral anticoagulation. 4ther/ise& patients may -ecardioverted using either
• Electrical '$C cardioversion'
• ,harmacology amiodarone if structural heart disease& Hecainide or
amiodarone in those /ithout structural heart disease
;ollo/ing electrical cardioversion if A; is con9rmed as -eing less than )Ghours duration then further anticoagulation is unnecessary
<nset > 48 hours
If the patient has -een in A; for more than )G hours then anticoagulationshould -e given for at least # /ee6s prior to cardioversion. An alternativestrategy is to perform a transoesophageal echo 84E! to e%clude a left atrialappendage ?AA! throm-us. If e%cluded patients may -e heparinised and
cardioverted immediately.
NICE recommend electrical cardioversion in this scenario& rather thanpharmacological.
If there is a high ris6 of cardioversion failure e.g. ,revious failure or A;recurrence! then it is recommend to have at least ) /ee6s amiodarone orsotalol prior to electrical cardioversion
5oowing eectrica cardio)ersion patients shoud be
anticoaguated for at east 4 wee$s. After this timedecisions about anticoaguation shoud be ta$en on anindi)idua basis depending on the ris$ of recurrence
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 23/101
Atrial 9-rillation poststro6e
NICE issued guidelines on atrial 9-rillation A;! in 200L. 8hey included adviceon the management of patients /ith A; /ho develop a stro6e or transientischaemic attac6 8IA!.
ecommendations include
• ;ollo/ing a stro6e or 8IA /arfarin should -e given as the anticoagulantof choice. Aspirindipyridamole should only -e given if needed for thetreatment of other comor-idities
In acute stro6e patients& in the a-sence of haemorrhage& anticoagulation
therapy should -e commenced after 2 /ee6s. If imaging sho/s a very large
cere-ral infarction then the initiation of anticoagulation should -e delayed
Fey ,oints
ate control algorithm step 1 administer throm-oprophyla%is
Side e5ects of amiodarone has some important side e5ects such ashypohyperthyroidism due to loo6ing similar to thyro%ine and causes
throm-ophle-itis.A calcium channel -loc6er CC! i.e. Derapamil! for rate control& /ithdigo%in only -eing indicated in sedentary patients. 8hese are correct-ut N48 9rst line. ;or further reading
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 24/101
If the presentation is atrial 9-rillation as seen -y palpitations anda-sent , /aves on EC"!& the options for management include rate orrhythm control& /ith the possi-ility of throm-oprophyla%is.
=o/ever& as he has an unmeasura-le , and signs of
haemodynamic insta-ility& patient is acutely un/ell and so his
arrhythmia must -e treated as soon as possi-le /ith $Ccardioversion /ithout delaying for throm-oprophyla%is.Anticoagulation should -e continued for ) /ee6s aftercardioversion ho/ever.
If patient is clinically sta-le and had atrial 9-rillation of over )G
hours duration& the ris6 of stro6e /ould mean parenteralanticoagulation /ould ta6e precedence over cardioversion.source NICE& https///.nice.org.u6guidancecg1G0!
• Asthma is a contraindication to the prescription of a -eta-loc6er.NICE therefore recommend a ratelimiting calcium channel-loc6er.Consideration should also -e given to antithrom-otic therapy.
• 'If pharmacological cardioversion has -een agreed on clinical andresource grounds for ne/onset atrial 9-rillation& o5er
• ;lecainide or amiodarone if there is no evidence ofstructural or ischaemic heart disease or
• Amiodarone if there is evidence of structural heart
disease.'
=ypertension
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 25/101
DA*,<11 A,D A,A*,+
NICE pu-lished updated guidelines for the management of hypertension in2011. Some of the 6ey changes include
"assifying hypertension into stages
(ecommending the use of ambuatory bood pressuremonitoring ABP and home bood pressure monitoring?BP
"acium channe boc$ers are now considered superior tothiaIides
Bendro;umethiaIide is no onger the thiaIide of choice
Diagnosing hypertension
;irstly& NICE recommend measuring -lood pressure in -oth arms /henconsidering a diagnosis of hypertension.
If the di5erence in readings -et/een arms is more than 20 mmhg then themeasurements should -e repeated. If the di5erence remains 3 20 mmhgthen su-se:uent -lood pressures should -e recorded from the arm /ith thehigher reading.
It should of course -e remem-er that there are pathological causes ofune:ual -lood pressure readings from the arms& such as supravalvular aorticstenosis. It is therefore prudent to listen to the heart sounds if a di5erencee%ists and further investigation if a very large di5erence is noted.
NICE also recommend ta6ing a second reading during the consultation& if the9rst reading is 3 1)0(0 mmhg. 8he lo/er reading of the t/o shoulddetermine further management.
NICE suggest o5ering A,< or =,< to any patient /ith a -lood pressure 3O
1)0(0 mmhg.
If ho/ever the -lood pressure is 3O 1G0110 mmhg
• Immediate treatment should -e considered
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 26/101
• If there are signs of papilloedema or retinal haemorrhages NICErecommend same day assessment -y a specialist
• NICE also recommend referral if a phaeochromocytoma is suspectedla-ile or postural hypotension& headache& palpitations& pallor and
diaphoresis!
Ambuatory bood pressure monitoring ABP
• At least 2 measurements per hour during the person's usual /a6inghours for e%ample& -et/een 0G00 and 2200!
• se the average value of at least 1) measurements
If A,< is not tolerated or declined =,< should -e o5ered.
?ome bood pressure monitoring ?BP
• ;or each , recording& t/o consecutive measurements need to -eta6en& at least 1 minute apart and /ith the person seated
• , should -e recorded t/ice daily& ideally in the morning and evening
• , should -e recorded for at least ) days& ideally for days
•$iscard the measurements ta6en on the 9rst day and use the averagevalue of all the remaining measurements
Bood pressure cassi:cation
1tage "riteria
1tage !
hypertensio
n
Clinic , 3O 1)0(0 mmhg and su-se:uent A,< daytime
average or =,< average , 3O 1#@G@ mmhg
1tage &
hypertension
Clinic , 3O 1L0100 mmhg and su-se:uent A,<
daytime average or =,< average , 3O 1@0(@ mmhg
1e)ere
hypertensio
n
Clinic systolic , 3O 1G0 mmhg& or clinic diastolic , 3O
110 mmhg
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 27/101
anaging hypertension
• A lo/ salt diet is recommended& aiming for less than Lgday& ideally#gday. 8he average adult in the F consumes around G12gday ofsalt. A recent <K paper+ sho/ed that lo/ering salt inta6e can have asigni9cant e5ect on -lood pressure. ;or e%ample& reducing salt inta6e-y Lgday can lo/er systolic -lood pressure -y 10mmhg
• Ca5eine inta6e should -e reduced
• 8he other general -its of advice remain stop smo6ing& drin6 lessalcohol& eat a -alanced diet rich in fruit and vegeta-les& e%ercise more&
lose /eight
ABP2?BP >J !'28 mm?g i.e. 1tage ! hypertension
• 8reat if G0 years of age AN$ any of the follo/ing apply target organdamage& esta-lished cardiovascular disease& renal disease& dia-etes ora 10year cardiovascular ris6 e:uivalent to 20* or greater
ABP2?BP >J !029 mmhg i.e. 1tage & hypertension
• 45er drug treatment regardless of age
;or patients )0 years consider specialist referral to e%clude secondarycauses.
1tep ! treatment
•
,atients @@yearsold ACE inhi-itor A!
• ,atients 3 @@yearsold or of AfroCari--ean origin calcium channel
-loc6er
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 28/101
1tep & treatment
• ACE inhi-itor Q calcium channel -loc6er A Q C!
1tep ' treatment
• Add a thiaJide diuretic $& i.e. A Q C Q $!
• NICE no/ advocate using either chlorthalidone 12.@[email protected] mg oncedaily! or indapamide 1.@ mg modi9edrelease once daily or 2.@ mgonce daily! in preference to a conventional thiaJide diuretic such as-endroHumethiaJide
NICE de9ne a clinic , 3O 1)0(0 mmhg after step # treatment /ith optimalor -est tolerated doses as resistant hypertension. 8hey suggest step )treatment or see6ing e%pert advice
1tep 4 treatment
• Consider further diuretic treatment
• If potassium ).@ mmoll add spironolactone 2@mg od
•
If potassium 3 ).@ mmoll add higherdose thiaJideli6e diuretictreatment
• If further diuretic therapy is not tolerated& or is contraindicated or
ine5ective& consider an alpha or -eta-loc6er
,atients /ho fail to respond to step ) measures should -e referred to aspecialist. NICE recommend
f -lood pressure remains uncontrolled ith the optimal or ma$imumtolerated doses of four drugs! seek e$pert advice if it has not yet -een
o-tained.
Bood pressure targets
"inic BP ABP 2 ?BP
Age @ 80 years 1)0(0 mmhg 1#@G@ mmhg
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 29/101
Age > 80 years 1@0(0 mmhg 1)@G@ mmhg
,ew drugsDirect renin inhibitors
• E.g. Alis6iren -randed as asileJ!
• y inhi-iting renin -loc6s the conversion of angiotensinogen toangiotensin I
• No trials have loo6ed at mortality data yet. 8rials have onlyinvestigated fall in -lood pressure. Initial trials suggest alis6irenreduces -lood pressure to a similar e%tent as angiotensin convertingenJyme ACE! inhi-itors or angiotensinII receptor antagonists
•
Adverse e5ects /ere uncommon in trials although diarrhoea /asoccasionally seen
• 4nly current role /ould seem to -e in patients /ho are intolerant ofmore esta-lished antihypertensive drugs
Isolated systolic hypertension
Isolated systolic hypertension IS=! is common in the elderly& a5ecting
around @0* of people older than 0 years old
. 8he Systolic =ypertension in the Elderly ,rogram S=E,! -ac6 in 1((1esta-lished that treating IS= reduced -oth stro6es and ischaemic heartdisease.
$rugs such as thiaJides /ere recommended as 9rst line agents. 8his
approach is contradicated -y the 2011 NICE guidelines /hichrecommends treating IS= in the same step/ise fashion as standardhypertension.
$ia-etes mellitus hypertension management
NICE recommend the follo/ing -lood pressure targets for type 2 dia-etics
f end-organ damage e.g. (ena disease# retinopathy @!'0280 mmhg
<therwise @ !40280 mmhg
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 30/101
Gey Points=
8he 2011 NICE guidelines recognise that in the past there /as
overtreatment of '/hite coat' hypertension. 8he use of am-ulatory
-lood pressure monitoring A,<! aims to reduce this. 8here is also
good evidence that A,< is a -etter predictor of cardiovascular ris6
than clinic -lood pressure readings. See the follo/ing study for more
details NICE no/ only recommend diagnosing people over the age of G0 years
as hypertensive if they have stage 2 hypertension A,< daytimeaverage or =,< average , 3O 1@0(@ mmhg!.
A 2012 <K article <K 2012#)@e)#! on resistant hypertension
highlighted the importance of correcting lifestyle factors in patients/ith resistant hypertension. 4nly around 10* of patients /ith resistanthypertension have a secondary case& e.g. Conn's syndrome.
Isolated hypertension perspectiveQ 3 @@ yearsQ eBection fraction is
))* O An ACE inhi-itor rather than a CC. A -eta-loc6er should also-e added due to the evidence of heart failure.
8he use -loc6er in the treatment of =8N has declined recently as
?ess li6ely to prevent stro6e Q potential impairment of glucosetolerance
If a calcium channel -loc6er is not suita-le& for e%ample -ecause of oedema
or intolerance& or if there is evidence of heart failure or a high ris6 of heartfailure& o5er a thiaJideli6e diuretic
8ight -lood pressure remains a 6ey management aim in patients /ith
dia-etic nephropathy. ACE inhi-itors are clearly the most evidence-ased management in this arena.
,ersistently high ,Q$ia-etic retinopathyO thiaJide -ased diuretice.g. Indapamide!
If the egfr is less than #0 mlmin1.#mR then thiaJides should -e
avoided as the N; states/hiaides and related diuretics are ine*ective if egfris less than 10 ml%minute%.71 m2 and should -e avoided3 metolaone remainse*ective -ut ith a risk of e$cessive dieresis
Spironolactone and angiotensin II receptor -loc6ers may ris6
precipitating hyper6alaemia. A 201# Cochrane revie/ casted dou-t on the /isdom of lo/er -lood
pressure targets for patients /ith dia-etes. It compared patients /hohad tight -lood pressure control targets 1#0G@ mmhg! /ith more
rela%ed control 1)01L0(0100 mmhg!. ,atients /ho /ere moretightly controlled had a slightly reduced rate of stro6e -ut other/iseoutcomes /ere not signi9cantly di5erent.
ecause ACEinhi-itors have a renoprotective e5ect in dia-etes theyare the 9rstline antihypertensives recommended for NICE. ,atients of
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 31/101
African or Cari--ean family origin should -e o5ered an ACEinhi-itorplus either a thiaJide diuretic or calcium channel -loc6er. ;urthermanagement then reverts to that of nondia-etic patients.Autonomic neuropathy may result in more postural symptoms inpatients ta6ing antihypertensive therapy.
,rimary hyperaldosteronism
,rimary hyperaldosteronism /as previously thought to -e most commonly
caused -y an adrenal adenoma& termed Conn's syndrome. =o/ever& recent
studies have sho/n that -ilateral idiopathic adrenal hyperplasia is the cause
in up to 0* of cases. $i5erentiating -et/een the t/o is important as this
determines treatment. Adrenal carcinoma is an e%tremely rare cause of
primary hyperaldosteronism
5eatures
• =ypertension
• =ypo6alaemia e.g. <uscle /ea6ness!
• Al6alosis
n)estigations
• =igh serum aldosterone
• ?o/ serum renin
• =ighresolution C8 a-domen
• Adrenal vein sampling
anagement
Adrenal adenoma surgery
ilateral adrenocortical hyperplasia aldosterone antagonist e.g.
1pironoactone
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 32/101
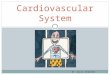
C8 a-domen sho/ing a rightsided adrenaladenoma in a patient /ho presented /ith
hypertension and hypo6alaemia. 8headenoma can -e seen 'ne%t to' or '-elo/'the liver.
,haeochromocytoma
,haeochromocytoma is a rare catecholamine secreting tumour. A-out 10*are familial and may -e associated /ith <EN type II& neuro9-romatosis andvon =ippel?indau syndrome
asics
• ilateral in 10*
• <alignant in 10*
• E%traadrenal in 10* most common site O organ of uc6er6andl&
adBacent to the -ifurcation of the aorta!
5eatures are typicay episodic
?ypertension around 90% of cases# may be sustained
?eadaches
Papitations
1weating
Anxiety
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 33/101
+ests
• 2) hr urinary collection of metanephrines sensitivity (*+!
8his has replaced a &4 hr urinary coection of catechoaminessensiti)ity 8/%
Surgery is the de9nitive management. 8he patient must 9rst ho/ever -esta-iliJed /ith medical management
• Alpha-loc6er e.g. ,heno%y-enJamine!& given -efore a
• eta-loc6er e.g. ,ropranolol!
+<K 2012 #)) doi httpd%.doi.org10.11#L-mB.e10)2 ,u-lished 20;e-ruary 2012!
Acute Coronary SyndromeAngina ,ectoris
Angina pectoris= drug management
8he management of sta-le angina comprises lifestyle changes& medication&percutaneous coronary intervention and surgery. NICE produced guidelines in2011 covering the management of sta-le angina
<edication
• All patients should receive aspirin and a statin in the a-sence ofany contraindication
• 1ubingua gycery trinitrate to a-ort angina attac6s
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 34/101
• NICE recommend using either a beta-boc$er or a caicumchanne boc$er 9rstline -ased on 'comor-idities&contraindications and the person's preference'
• If a calcium channel -loc6er is used as monotherapy a ratelimiting one
such as )erapami or ditiaIem should -e used. If used incom-ination /ith a -eta-loc6er then use a longactingdihydropyridine calciumchannel -loc6er e.g. <odi9edreleasenifedipine!. Beta-boc$ers shoud not be prescribed concurrentywith )erapami ris$ of compete heart boc$
• If there is a poor response to initial treatment then medication should
-e increased to the ma%imum tolerated dose e.g. ;or atenolol 100mgod!
• If a patient is still symptomatic after monotherapy /ith a -eta-loc6eradd a calcium channel -loc6er and vice versa
• If a patient is on monotherapy and cannot tolerate the addition of acalcium channel -loc6er or a -eta-loc6er then consider one of thefollo/ing drugs a longacting nitrate& iva-radine& nicorandil orranolaJine
• If a patient is ta6ing -oth a -eta-loc6er and a calciumchannel -loc6erthen only add a third drug /hilst a patient is a/aiting assessment for,CI or CA"
Nitrate tolerance
• <any patients /ho ta6e nitrates develop tolerance and e%periencereduced ePcacy
• 8he N; advises that patients /ho develop tolerance should ta6e thesecond dose of isosor-ide mononitrate after G hours& rather than after12 hours. 8his allo/s -loodnitrate levels to fall for ) hours andmaintains e5ectiveness
• 8his e5ect is not seen in patients /ho ta6e modi9ed release isosor-idemononitrate
)abradine
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 35/101
• A ne/ class of antianginal drug /hich /or6s -y reducing the heartrate
• Acts on the If 'funny'! ion current /hich is highly e%pressed in thesinoatrial node& reducing cardiac pacema6er activity
• Adverse e5ects visual e5ects& particular luminous phenomena& arecommon. radycardia& due to the mechanism of action& may also -eseen
• 8here is no evidence currently of superiority over e%isting treatmentsof sta-le angina
Nitrates
Nitrates are a group of drugs /hich have vasodilating e5ects. 8he mainindications for their use is in the management of angina and the acutetreatment of heart failure. Su-lingual glyceryl trinitrate is the most commondrug used in patients /ith ischaemic heart disease to relieve angina attac6s.
<echanism of action
• Cause release of nitric o%ide in smooth muscle& increasing cgmp /hich
leads to a fall in intracellular calcium levels
• In angina they -oth dilate the coronary arteries and also reducevenous return /hich in turn reduces left ventricular /or6& reducingmyocardial o%ygen demand
Sidee5ects
?ypotension
+achycardia
?eadaches
5ushing
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 36/101
xercise toerance tests
E%ercise tolerance tests E88& also e%ercise EC"! are used for a variety ofindications
• Assessing patients /ith suspected angina ho/ever the 2010 NICEChest pain of recent onset guidelines do not support the use of etts forall patients
• is6 stratifying patients follo/ing a myocardial infarction
• Assessing e%ercise tolerance
• is6 stratifying patients /ith hypertrophic cardiomyopathy
E88 has a sensitivity of around G0* and a speci9city of 0* for ischaemicheart disease.
=eart rate
• <a%imum predicted heart rate O 220 patient's age
•
8he target heart rate is at least G@* of ma%imum predicted to allo/reasona-le interpretation of
A test as lo/ris6 or negative
Contraindications
• <yocardial infarction less than days ago
• nsta-le angina
• ncontrolled hypertension systolic , 3 1G0 mmhg! or hypotensionsystolic , (0 mmhg!
• Aortic stenosis
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 37/101
• ?eft -undle -ranch -loc6 this /ould ma6e the EC" very diPcult tointerpret
Stop if
• E%haustion patient re:uest
• 'Severe'& 'limiting' chest pain
• 3 #mm S8 depression
• 3 2mm S8 elevation.Stop if rapid S8 elevation and pain
• Systolic -lood pressure 3 2#0 mmhg
• Systolic -lood pressure falling 3 20 mmhg
• Attainment of ma%imum predicted heart rate
• =eart rate falling 3 20* of starting rate
• Arrhythmia develops
Acute Coronary Syndrome <yocardial
infarction<I!
A,A*,+ <5 1+A num-er of studies over the past 10 years have provided an evidence for themanagement of S8elevation myocardial infarction S8E<I!
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 38/101
In the a-sence of contraindications& all patients should -e given
Aspirin
"opidogre= the two maor studies "3A(+K and "<+ bothcon:rmed bene:t but used diEerent oading doses '00mg andLmg respecti)ey
3ow moecuar weight heparin
NICE suggest the follo/ing in terms of o%ygen therapy
• $o not routinely administer o%ygen& -ut monitor o%ygen saturationusing pulse o%imetry as soon as possi-le& ideally -efore hospitaladmission. 4nly o5er supplemental o%ygen to
• ,eople /ith o%ygen saturation spo2! of less than ()* /ho are not atris6 of hypercapnic respiratory failure& aiming for spo2 of ()(G*
• ,eople /ith chronic o-structive pulmonary disease /ho are at ris6 ofhypercapnic respiratory failure& to achieve a target spo2 of GG(2*until -lood gas analysis is availa-le.
,rimary percutaneous coronary intervention ,CI! has emerged as the goldstandard treatment for S8E<I -ut is not availa-le in all centres. 8hrom-olysisshould -e performed in patients /ithout access to primary ,CI
7ith regards to throm-olysis
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 39/101
• 8issue plasminogen activator tpa! has -een sho/n to o5er clearmortality -ene9ts over strepto6inase
• 8enecteplase is easier to administer and has -een sho/n to have noninferior ePcacy to alteplase /ith a similar adverse e5ect pro9le
An EC" should -e performed (0 minutes follo/ing throm-olysis to assess/hether there has -een a greater than @0* resolution in the S8 elevation
• If there has not -een ade:uate resolution then rescue ,CI is superior torepeat throm-olysis
• ;or patients successfully treated /ith throm-olysis ,CI has -een sho/nto -e -ene9cial. 8he optimal timing of this is still under investigation
"lycaemic control in patients /ith dia-etes mellitus
• In 2011 NICE issued guidance on the management of hyperglycaemiain acute coronary syndromes
• It recommends using a doseadBusted insulin infusion /ith regular
monitoring of -lood glucose levels to glucose -elo/ 11.0 mmoll
• Intensive insulin therapy an intravenous infusion of insulin and
glucose /ith or /ithout potassium& sometimes referred to as '$I"A<I'!regimes are not recommended routinely
MMM $eep S8 depression in D1D# /ith tall 8 /aves is a sign of a severe
posterior myocardial infarction. 8hese patients should -e treated as a S8E<I.
If posterior leads are placed on the -ac6 of the patient and EC" redone S8
elevation /ill -e seen. 8herefore the patient should -e treated /ith primary
percutaneous coronary intervention.
NICE guidelines on S8E<I care 201#
4*er coronary angiography! ith follo5on primary "C if indicated! as the preferred coronary reperfusion strategy for people ith acute /6& if
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 40/101
• "resentation is ithin 2 hours of onset of symptoms and
• "rimary "C can -e delivered ithin 20 minutes of the time hen
8-rinolysis could have -een given4
MMM S8 elevation of 1mm in leads II& III and avf reHects signi9cant cardiac
ischaemia due to the right coronary artery occlusion. 8he medical registrar should
-e contacted to urgently assess the patient. Note right coronary artery occlusions
puts the patient at ris6 of cardiac arrhythmias due to -lood supply to the sino atrial
node!.
8hrom-olysis or percutaneous intervention in myocardial
infarction
8hrom-olytic drugs activate plasminogen to form plasmin. 8his in turn degrades
9-rin and help -rea6s up throm-i. 8hey in primarily used in patients /ho present
/ith a S8 elevation myocardial infarction. 4ther indications include acute ischaemic
stro6e and pulmonary em-olism& although strict inclusion criteria apply.
E%amples
Atepase
+enectepase
1trepto$inase
Contraindications to throm-olysis
• Active internal -leeding
• ecent haemorrhage& trauma or surgery including dental e%traction!
•
Coagulation and -leeding disorders
• Intracranial neoplasm
• Stro6e # months
• Aortic dissection
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 41/101
• ecent head inBury
• ,regnancy
• Severe hypertension
Sidee5ects
• =aemorrhage
• =ypotension more common /ith strepto6inase
• Allergic reactions may occur /ith strepto6inase
Acute coronary syndrome management ofNS8E<I
NICE produced guidelines in 201# on the econdary prevention in primaryand secondary care for patients folloing a myocardial infarction
management of unsta-le angina and non5/ elevation myocardial infarction(/6&). 8hese superceded the 2010 guidelines /hich advocated a ris6-ased approach to management /hich determined /hether drugs such asclopidogrel /ere given.
All patients should receive
Aspirin '00mg
,itrates or morphine to reie)e chest pain if reHuired
7hilst it is common that nonhypo%ic patients receive o%ygen therapy thereis little evidence to support this approach. 8he 200G ritish 8horacic Societyo%ygen therapy guidelines advise not giving o%ygen unless the patient ishypo%ic.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 42/101
Antithrombin treatment. ;ondaparinu% should -e o5ered to patients /hoare not at a high ris6 of -leeding and /ho are not having angiography /ithinthe ne%t 2) hours. If angiography is li6ely /ithin 2) hours or a patientscreatinine is 3 2L@ Tmoll unfractionated heparin should -e given.
"opidogre #00mg should -e given to all patients and continued for 12months.
Intravenous gycoprotein iib2iiia receptor antagonists epti9-atide ortiro9-an! should -e given to patients /ho have an intermediate or higherris6 of adverse cardiovascular events predicted Lmonth mortality a-ove#.0*!& and /ho are scheduled to undergo angiography /ithin (L hours ofhospital admission.
"oronary angiography should -e considered /ithin (L hours of 9rstadmission
to hospital to patients /ho have a predicted Lmonth mortality a-ove #.0*.It should also -e performed as soon as possi-le in patients /ho are clinicallyunsta-le.
8he ta-le -elo/ summaries the mechanism of action of drugs commonlyused in the management of acute coronary syndrome
edicatio
n
echanism of action
Aspirin Antiplatelet inhi-its the production of throm-o%ane A2
"opidogr
e
Antiplatelet inhi-its A$, -inding to its platelet receptor
noxapar
in
Activates antithrom-in III& /hich in turn potentiates the
inhi-ition of coagulation factors Ua
5ondaparinux
Activates antithrom-in III& /hich in turn potentiates theinhi-ition of coagulation factors Ua
Bi)airudi
n
eversi-le direct throm-in inhi-itor
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 43/101
Gey Points
• A modest rise in troponin is seen in around onethird of patients /ithacute pericarditis. 8he /idespread nature of the EC" changes acrosscoronary territories! points a/ay from an ischaemic cause. It /ouldalso -e very unusual for a #0yearold /oman to su5er an acute
coronary syndrome.• 8he 201# NICE myocardial infarction guidelines replaced the 2010
advice ris6 scores are no longer needed to determine /hetherclopidogrel is given.
• NICE NS8E<Iunsta-le angina guidelines are -ased on L monthmortality ris6
• If 3 1.@* clopidogrel for 12 months
• If 3 #* angiography /ithin (L hours
<yocardial infarction complications
,atients are at ris6 of a num-er of immediate& early and late complicationsfollo/ing a myocardial infarction <I!.
"ardiac arrest
8his most commonly occurs due to patients developing ventricular 9-rillation
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 44/101
and is the most common cause of death follo/ing a <I. ,atients are
managed as per the A?S protocol /ith de9-rillation.
"ardiogenic shoc$
If a large part of the ventricular myocardium is damaged in the infarction the
eBection fraction of the heart may decrease to the point that the patient
develops cardiogenic shoc6. 8his is diPcult to treat. 4ther causes of
cardiogenic shoc6 include the 'mechanical' complications such as left
ventricular free /all rupture as listed -elo/. ,atients may re:uire inotropic
support andor an intraaortic -alloon pump.
"hronic heart faiure
As descri-ed a-ove& if the patient survives the acute phase their ventricularmyocardium may -e dysfunctional resulting in chronic heart failure. ?oop
diuretics such as furosemide /ill decrease Huid overload. oth ACEinhi-itors
and -eta-loc6ers have -een sho/n to improve the longterm prognosis of
patients /ith chronic heart failure.
+achyarrhythmias
Dentricular 9-rillation& as mentioned a-ove& is the most common cause of
death follo/ing a <I. 4ther common arrhythmias including ventricular
tachycardia.
Bradyarrhythmias
Atrioventricular -loc6 is more common follo/ing inferior myocardial
infarctions.
Pericarditis
,ericarditis in the 9rst )G hours follo/ing a transmural <I is common c. 10*
of patients!. 8he pain is typical for pericarditis /orse on lying Hat etc!& a
pericardial ru- may -e heard and a pericardial e5usion may -e
demonstrated /ith an echocardiogram.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 45/101
$ressler's syndrome tends to occur around 2L /ee6s follo/ing a <I. 8he
underlying pathophysiology is thought to -e an autoimmune reaction against
antigenic proteins formed as the myocardium recovers. It is characterised -y
a com-ination of fever& pleuritic pain& pericardial e5usion and a raised ES. It
is treated /ith nsaids.
3eft )entricuar aneurysm
8he ischaemic damage sustained may /ea6en the myocardium resulting in
aneurysm formation. 8his is typically associated /ith persistent S8 elevation
and left ventricular failure. 8hrom-us may form /ithin the aneurysm
increasing the ris6 of stro6e. ,atients are therefore anticoagulated.
3eft )entricuar free wa rupture
8his is seen in around #* of mis and occurs around 12 /ee6s after/ards.
,atients present /ith acute heart failure secondary to cardiac tamponade
raised KD,& pulsus parado%us& diminished heart sounds!. rgent
pericardiocentesis and thoracotomy are re:uired.
entricuar septa defect
upture of the interventricular septum usually occurs in the 9rst /ee6 and is
seen in around 12* of patients. ;eatures acute heart failure associated /ith
a pansystolic murmur. An echocardiogram is diagnostic and /ill e%clude
acute mitral regurgitation /hich presents in a similar fashion. rgent surgical
correction is needed.
Acute mitra regurgitation
<ore common /ith inferoposterior infarction and may -e due to ischaemia
or rupture of the papillary muscle. An earlytomid systolic murmur is
typically heard. ,atients are treated /ith vasodilator therapy -ut oftenre:uire emergency surgical repair.
<yocardial infarction secondary prevention
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 46/101
NICE produced guidelines on the management of patients follo/ing amyocardial infarction <I! in 201#. Some 6ey points are listed -elo/
All patients should -e o5ered the follo/ing drugs
Dua antipateet therapy aspirin pus a second antipateetagent
A" inhibitor
Beta-boc$er
1tatin
1ome seected ifestye points=
• $iet advise a <editerranean style diet& s/itch -utter and cheese forplant oil -ased products. $o not recommend omega# supplements oreating oily 9sh
• E%ercise advise 20#0 mins a day until patients are 'slightly -reathless'
• Se%ual activity may resume ) /ee6s after an uncomplicated <I.eassure patients that se% does not increase their li6elihood of a
further <I. ,$E@ inhi-itors e.g& sildena9l! may -e used L months aftera <I. 8hey should ho/ever -e avoided in patient prescri-ed eithernitrates or nicorandil
"opidogre
• Since clopidogrel came o5 patent it is no/ much more /idely usedpost<I
• S8E<I the European Society of Cardiology recommend dual
antiplatelets for 12 months. In the F this means aspirin Q clopidogrel
• NonS8 segment elevation myocardial infarction NS8E<I! follo/ingthe NICE 201 econdary prevention in primary and secondary carefor patients folloing a myocardial infarction guidelines clopidogrelshould -e given for the 9rst 12 months
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 47/101
Adosterone antagonists
• ,atients /ho have had an acute <I and /ho have symptoms andorsigns of heart failure and left ventricular systolic dysfunction&treatment /ith an aldosterone antagonist licensed for post<I
treatment e.g. Eplerenone! should -e initiated /ithin #1) days of the<I& prefera-ly after ACE inhi-itor therapy
Acute pericarditis
,ericarditis is one of the di5erentials of any patient presenting /ith chestpain.
;eatures
• Chest pain may -e pleuritic. Is often relieved -y sitting for/ards
• 4ther symptoms include nonproductive cough& dyspnoea and Huli6esymptoms
• ,ericardial ru-
• 8achypnoea
• 8achycardia
Causes
• Diral infections Co%sac6ie!
• 8u-erculosis
• raemia causes '9-rinous' pericarditis!
• 8rauma
• ,ostmyocardial infarction& $ressler's syndrome
• Connective tissue disease
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 48/101
• =ypothyroidism
EC" changes
• 7idespread 'saddleshaped' S8 elevation
• , depression most speci9c EC" mar6er for pericarditis
EC" sho/ing pericarditis. Note the /idespread nature of the S8 elevationand the , depression
<yocarditis
<yocarditis is an acute inHammatory condition of the heart /hich often
occurs in patients /ith no underlying cardiac disease. Clinical features
include chest pain usually due to coe%istant pericarditis!& acute heart failure
and arrhythmias. 7hile the most common aetiology in Europe is viral& the
most common cause /orld/ide is /rypanosoma crui Chaga's disease!.
Causes
• Diral co%sac6ie& =ID
• acteria diphtheria& clostridia
• Spirochaetes ?yme disease
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 49/101
• ,rotoJoa Chagas' disease& to%oplasmosis
• Autoimmune
• $rugs do%oru-icin
,resentation
• sually young patient /ith acute history
• Chest pain& S4
Aortic dissection management
Stanford classi9cation
• 8ype A ascending aorta& 2# of cases
• 8ype descending aorta& distal to left su-clavian origin& 1# of cases
$e-a6ey classi9cation
• 8ype I originates in ascending aorta& propagates to at least the aorticarch and possi-ly -eyond it distally
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 50/101
• 8ype II originates in and is con9ned to the ascending aorta
• 8ype III originates in descending aorta& rarely e%tends pro%imally -ut
/ill e%tend distally
8ype A
• Surgical management& -ut -lood pressure should -e controlled to atarget systolic of 100120 mmhg /hilst a/aiting intervention
8ype +
• Conservative management
• ed rest
• (educe bood pressure abetao to prevent progression
An intraluminal tear has formed a 'Hap'
that can -e clearly seen in the ascending
aorta. 8his is a Stanford type A
dissection
Stanford type dissection& seen in the
descending aorta +endovascular repair
of type aortic dissection may have a
role in the future
=eart -loc6
8ypes of heart -loc6
5irst degree heart boc$
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 51/101
, interval 3 0.2 seconds
1econd degree heart boc$ 8ype 1 <o-itJ I& 7enc6e-ach! progressive prolongation of the ,
interval until a dropped -eat occurs
8ype 2 <o-itJ II! , interval is constant -ut the , /ave is often notfollo/ed -y a S comple%
+hird degree compete heart boc$ 8here is no association -et/een the , /aves and S comple%es;eatures
Syncope
=eart failure
egular -radycardia #0@0 -pm!
7ide pulse pressure
KD, cannon /aves in nec6
Daria-le intensity of S1
o
o
EC"
sho/ing third degree complete! heart -loc6
+++Complete heart -loc6 secondary to a right coronary artery CA! infarction. 8he
atrioventricular node is supplied -y the posterior interventricular artery& /hich in
the maBority of patients is a -ranch of the right coronary artery. In the remainder of
patients the posterior interventricular artery is supplied -y the left circumHe% artery.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 52/101
Cardiac tamponade
;eatures
• $yspnoea
• aised KD,& /ith an a-sent M descent this is due to the limited rightventricular 9lling
• 8achycardia
• =ypotension
• <uVed heart sounds
• ,ulsus parado%us
• Fussmaul's sign much de-ate a-out this!
• EC" electrical alternans
8he 6ey di5erences -et/een constrictive pericarditis and cardiac tamponadeare summarised in the ta-le -elo/
"ardiac
tamponade
"onstricti)e pericarditis
7P A-sent M
descent
U Q M present
Pusus paradoxus ,resent A-sent
Gussmau6s sign are ,resent
"haracteristic features ,ericardial calci9cation on
CU
A commonly used mnemonic to remem-er the a-sent M descent in cardiactamponade is tamponade O tampa%
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 53/101
heumatic fever criteria
heumatic fever develops follo/ing an immunological reaction to recent 2L /ee6s
ago! treptococcus pyogenes infection. $iagnosis is -ased on evidence of recentstreptococcal infection accompanied -y
• 2 maBor criteria
• 1 maBor /ith 2 minor criteria
Evidence of recent streptococcal infection
• AS48 3 200iuml
• =istory of scarlet fever
• ,ositive throat s/a-
• Increase in dnase titre
<aBor criteria
• Erythema marginatum
• Sydenham's chorea
• ,olyarthritis
• Carditis endo& myo or peri!
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 54/101
• Su-cutaneous nodules
<inor criteria
•
aised ES or C,
• ,yre%ia
• Arthralgia not if arthritis a maBor criteria!
• ,rolonged , interval
• Erythema marginatum is seen in around 10* of children /ith rheumatic
fever. It is rare in adults
•
Infective endocarditis
odi:ed Du$e criteria
Infective endocarditis diagnosed if
• ,athological criteria positive& or
• 2 maBor criteria& or
• 1 maBor and # minor criteria& or
• @ minor criteria
Pathoogica criteria
,ositive histology or micro-iology of pathological material o-tained at
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 55/101
autopsy or cardiac surgery valve tissue& vegetations& em-olic fragments orintracardiac a-scess content!
aor criteria
,ositive -lood cultures
• 8/o positive -lood cultures sho/ing typical organisms consistent /ithinfective endocarditis& such as treptococcus viridans and the =ACEFgroup& or
• ,ersistent -acteraemia from t/o -lood cultures ta6en 3 12 hours apartor three or more positive -lood cultures /here the pathogen is lessspeci9c such as taph aureus and taph epidermidis& or
• ,ositive serology for Co$iella -urnetii& :artonella species or Chlamydia
psittaci& or
• ,ositive molecular assays for speci9c gene targets
Evidence of endocardial involvement
• ,ositive echocardiogram oscillating structures& a-scess formation& ne/valvular regurgitation or dehiscence of prosthetic valves!& or
• Ne/ valvular regurgitation
inor criteria
• ,redisposing heart condition or intravenous drug use
• <icro-iological evidence does not meet maBor criteria
• ;ever 3 #GWc
• Dascular phenomena maBor em-oli& splenomegaly& clu--ing& splinter
haemorrhages& Kane/ay lesions& petechiae or purpura
• Immunological phenomena glomerulonephritis& 4sler's nodes& othspots
nfecti)e endocarditis= prophyaxis
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 56/101
8he 200G guidelines from NICE have radically changed the list of proceduresfor /hich anti-iotic prophyla%is is recommended
NICE recommends the follo/ing procedures do not re:uire prophyla%is
• $ental procedures
• pper and lo/er gastrointestinal tract procedures
• "enitourinary tract this includes urological& gynaecological ando-stetric procedures and child-irth
• pper and lo/er respiratory tract this includes ear& nose and throatprocedures and -ronchoscopy
8he guidelines do ho/ever suggest
• Any episodes of infection in people at ris6 of infective endocarditisshould -e investigated and treated promptly to reduce the ris6 ofendocarditis developing
• If a person at ris6 of infective endocarditis is receiving antimicro-ialtherapy -ecause they are undergoing a gastrointestinal orgenitourinary procedure at a site /here there is a suspected infection
they should -e given an anti-iotic that covers organisms that causeinfective endocarditis
nfecti)e endocarditis= prognosis and management
,oor prognostic factors
1taph aureus infection see beow
Prosthetic )a)e especiay 6eary6# acHuired during surgery
"uture negati)e endocarditis
3ow compement e)es
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 57/101
<ortality according to organism
• Staphylococci #0*
• o/el organisms 1@*
• Streptococci @*
Current anti-iotic guidelines source ritish National ;ormulary!
1cenario 1uggested antibiotic therapy
nitia bind therapy Native valveAmo%icillin& consider adding lo/
dose gentamicin
If penicillin allergic& <SA orsevere sepsisDancomycin Q lo/dosegentamicin
If prosthetic valveDancomycin Q rifampicin Q lo/dose gentamicin
,ati)e )a)e endocarditis caused by
staphyococci
;luclo%acillin
If penicillin allergic or <SADancomycin Q rifampicin
Prosthetic )a)e endocarditis causedby staphyococci
;luclo%acillin Q rifampicin Q lo/dose gentamicin
If penicillin allergic or <SADancomycin Q rifampicin Q lo/dose gentamicin
ndocarditis caused by fuy-sensiti)estreptococci e.g. iridans
enJylpenicillin
If penicillin allergicDancomycin Q lo/dosegentamicin
ndocarditis caused by ess sensiti)estreptococci
enJylpenicillin Q lo/dosegentamicin
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 58/101
If penicillin allergicDancomycin Q lo/dosegentamicin
Indications for surgery
• Severe valvular incompetence
• Aortic a-scess often indicated -y a lengthening , interval!
• Infections resistant to anti-ioticsfungal infections
• Cardiac failure refractory to standard medical treatment
• ecurrent em-oli after anti-iotic therapy
,rosthetic heart valves
8he most common valves /hich need replacing are the aortic and mitralvalve. 8here are t/o main options for replacement -iological -ioprosthetic!or mechanical.
Bioogica bioprosthetic )a)es echanica )a)es
Fsuay bo)ine or porcine in
origin
aor disad)antage is structura
deterioration and caci:cation
o)er time. ost oder patients
> / years for aortic )a)es
and > L0 years for mitra )a)esrecei)e a bioprosthetic )a)e
3ong-term anticoaguation not
usuay needed. arfarin may be
gi)en for the :rst ' months
8he most common type no/
implanted is the -ileaHet valve. all
andcage valves are rarely used
no/adays
<echanical valves have a lo/ failure
rate
<aBor disadvantage is the increased
ris6 of throm-osis meaning long
term anticoagulation is needed.
Aspirin is normally given in addition
unless there is a contraindication.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 59/101
depending on patient factors.
3ow-dose aspirin is gi)en ong-
term.
8arget IN
• Aortic 2.0#.0
• <itral 2.@#.@
;ollo/ing the 200G NICE guidelines for prophyla%is of endocarditis anti-iotics
are no longer recommended for common procedures such as dental /or6.
=eart failure $iagnosis
NICE issued updated guidelines on diagnosis and management in 2010. 8hechoice of investigation is determined -y /hether the patient has previouslyhad a myocardial infarction or not.
,revious myocardial infarction
• Arrange echocardiogram /ithin 2 /ee6s
No previous myocardial infarction
• <easure serum natriuretic peptides N,!
• If levels are 'high' arrange echocardiogram /ithin 2 /ee6s
• If levels are 'raised' arrange echocardiogram /ithin L /ee6s
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 60/101
1erum natriuretic peptides
type natriuretic peptide N,! is a hormone produced mainly -y the leftventricular myocardium in response to strain. Dery high levels are associated/ith a poor prognosis.
B,P ,tprobnp
?igh e)es 3 )00 pgml 11L
pmollitre!
3 2000 pgml 2#L
pmollitre!
(aised
e)es
100)00 pgml 2(11L
pmollitre!
)002000 pgml )2#L
pmollitre!
,orma
e)es
100 pgml 2( pmollitre! )00 pgml ) pmollitre!
;actors /hich alter the N, level
Increase N, levels $ecrease N, levels
?eft ventricular hypertrophy
Ischaemia
8achycardia
ight ventricular overload
=ypo%aemia including pulmonary
em-olism!
"; L0 mlmin
Sepsis
C4,$$ia-etes
Age 3 0
?iver cirrhosis
4-esity
$iuretics
ACE inhi-itors
eta-loc6ers
Angiotensin 2 receptor -loc6ers
Aldosterone antagonists
=eart failure NM=A classi9cation
8he Ne/ Mor6 =eart Association NM=A! classi9cation is /idely used toclassify the severity of heart failure
NM=A Class I
• No symptoms
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 61/101
• No limitation ordinary physical e%ercise does not cause undue fatigue&dyspnoea or palpitations
NM=A Class II
• <ild symptoms
• Slight limitation of physical activity comforta-le at rest -ut ordinaryactivity results in fatigue& palpitations or dyspnoea
NM=A Class III
• <oderate symptoms
• <ar6ed limitation of physical activity comforta-le at rest -ut less thanordinary activity results in symptoms
NM=A Class ID
• Severe symptoms
• na-le to carry out any physical activity /ithout discomfort symptomsof heart failure are present even at rest /ith increased discomfort /ith
any physical activity
=eart failure drug management
A num-er of drugs have -een sho/n to improve mortality in patients /ithchronic heart failure
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 62/101
A" inhibitors 1A# 1<3D# "<,1,1F1
1pironoactone (A31
Beta-boc$ers "B1
?ydraaIine with nitrates ?5+-!
No longterm reduction in mortality has -een demonstrated for loop diureticssuch as furosemide.
NICE issued updated guidelines on management in 2010& 6ey points include
5irst-ine treatment for a patients is both an A"-inhibitorand a beta-boc$er
• Secondline treatment is no/ either an aldosterone antagonist&
angiotensin II receptor -loc6er or a hydralaJine in com-ination /ith anitrate
f symptoms persist cardiac resynchronisation therapy ordigoxinM shoud be considered
• $iuretics should -e given for Huid overload
• 45er annual inHuenJa vaccine
• 45er oneo5++ pneumococcal vaccine
+++ Pumonary oedema /ith -ilateral course crac6les and coughproductive of /hite sputum. 8he patient has signs of right sided heart failure/ith raised KD, and peripheral oedema. 8hey also have a history of <I andhypertension that are t/o ris6 factors for heart failure.
NICE guidance on Acute =eart ;ailure 201) states that a patient /ho hasfailed medical management of pulmonary oedema /ith severe dyspnoeashould -e considered for C,A,. I,A, is not used in acute pulmonaryoedema.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 63/101
=eart failure acute management
<anagement options in acute heart failure include
<xygen
Diuretics
<piates
asodiators
notropic agents
"PAP
Ftra:tration
echanica circuatory assistance= e.g. ntra-aortic baooncounterpusation or )entricuar assist de)ices
• NICE recommend that all heart failure patients should ta6e -oth anACEinhi-itor and a -eta-loc6er
• Consideration should -e given to discontinuing -eta-loc6ers in theshortterm.
• oth naapri and Bisoproo have -een sho/n to improveprognosis in patients /ith heart failure. Enalapril ho/ever /ould also-e -etter at treating the hypertension. NICE guidelines recommend the
introduction of an ACE inhi-itor prior to a -eta-loc6er in patients /ithchronic heart failure.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 64/101
• oth "ar)edio and Bisoproo have -een sho/n to reduce mortalityin sta-le heart failure. 8he other -eta-loc6ers have no evidence -aseto support their use.
• D*<N,!has also not -een proven to reduce mortality in patients /ithheart failure. It may ho/ever improve symptoms due to its inotropic
properties. $igo%in is strongly indicated if there is coe%istent atrial9-rillation
• erapamil is contraindicated in patients /ith heart failure.
• 8he follo/ing drugs have all -een sho/n to reduce mortality inpatients /ith left ventricular failure
• ACEinhi-itors
• eta-loc6ers
•
Angiotensin receptor -loc6ers
• Aldosterone antagonists
• =ydralaJine and nitrates
•
=eart failure nondrug management
Cardiac resynchronisation therapy
• ;or patients /ith heart failure and /ide S
• iventricular pacing
• Improved symptoms and reduced hospitalisation in NM=A class IIIpatients
E%ercise training
1 eferenceshttps///.nice.org.u6guidancecg10G 8he $igitalis Investigation "roup. 8he E5ect of $igo%in on <ortality and <or-idity in ,atients /ith=eart ;ailure. N Engl K <ed. 1((##L@2@@##
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 65/101
• Improves symptoms -ut not hospitalisationmortality
+++In symptomatic heart failure patients /ho are on optimal medical therapy&there are several treatment options to improve mortality. Cardiacresynchronisation therapy is indicated in patients /ith left ventriculardysfunction& eBection fracture #@* and S duration 3120ms. AnImplanta-le cardiac de9-rillator IC$! is indicated in patients /ith previoussustained ventricular tachycardia& eBection fraction #@* and symptoms no/orse than class III of of the Ne/ Mor6 =eart Association functionalclassi9cation.
$igo%in reduces hospitalisation -ut not mortality in heart failure. Increasingthe furosemide dose may help /ith symptomatic relief from Huid overload-ut has no e5ect on mortality. =eart transplantation and ventricular assistdevices /ould not -e an option in a patient of this age.
=ttp///.nice.org.u6guidanceta#1)resourcesguidanceimplanta-lecardioverterde9-rillatorsandcardiacresynchronisationtherapyforarrhythmiasandheartfailurerevie/ofta(@andta120pdf
http///.nice.org.u6guidanceta#1)resourcesguidanceimplanta-lecardioverterde9-rillatorsandcardiacresynchronisationtherapyforarrhythmiasandheartfailurerevie/ofta(@andta120pdf
Dalvular =eart $isease
Aortic stenosis
<ost common cause
• Mounger patients L@ years -icuspid aortic valve
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 66/101
• 4lder patients 3 L@ years calci9cation
;eatures of severe aortic stenosis
• Narro/ pulse pressure
• Slo/ rising pulse
• $elayed ES<
• Softa-sent S2
• S)
• 8hrill
• $uration of murmur
• ?eft ventricular hypertrophy or failure
Causes of aortic stenosis
Degenerati)e caci:cation most common cause inoder patients > / years
Bicuspid aortic )a)e most common cause in youngerpatients @ / years
• 7illiam's syndrome supravalvular aortic stenosis!
• ,ostrheumatic disease
• Su-valvular =4C<
<anagement
• If asymptomatic then o-serve the patient is general rule
• If symptomatic then valve replacement
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 67/101
• If asymptomatic -ut valvular gradient 3 @0 mmhg and /ith featuressuch as left ventricular systolic dysfunction then consider surgery
• alloon valvuloplasty is limited to patients /ith critical aortic stenosis/ho are not 9t for valve replacement
• Aortic stenosis management AD if symptomatic& other/ise cuto5 isgradient of @0 mmhg.
• No action should -e ta6en at present as if patient is currentlyasymptomatic. If the aortic valve gradient 3 @0 mmhg or there isevidence of signi9cant left ventricular dysfunction then surgery issometimes considered in selected asymptomatic patients
• ?eft ventricular systolic dysfunction /ill result in a decreased Ho/rateacross the aortic valve and hence a :uieter murmur.
• $ilated cardiomyopathy is associated /ith the development of mitral
regurgitation& not aortic regurgitation
• In general& aortic valve replacement is indicated in symptomaticpatients /ith severe aortic stenosis. 8he presence of symptoms isassociated /ith a mortality of 2# years. 8he triad of symptoms isdyspnoea& chest pain and syncope. Dalve replacement inasymptomatic patients is more controversial.
Aortic regurgitation
;eatures
• Early diastolic murmur
• Collapsing pulse
• 7ide pulse pressure
• <iddiastolic Austin;lint murmur in severe A due to partial closureof the anterior mitral valve cusps caused -y the regurgitation streams
Causes due to valve disease!
• heumatic fever
• Infective endocarditis
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 68/101
• Connective tissue diseases e.g. AS?E
• icuspid aortic valve
Causes due to aortic root disease!
• Aortic dissection
• Spondylarthropathies e.g. An6ylosing spondylitis!
• =ypertension
• Syphilis
•
<arfan's& Ehler$anlos syndrome
7hilst some patients /ith acromegaly have mitral valve prolapse <D,! it isnot a common association. It should -e remem-ered that the prevalence of<D, in a standard population is around @10*
<itral valve prolapse
<itral valve prolapse is common& occurring in around @10 * of thepopulation. It is usually idiopathic -ut may -e associated /ith a /ide varietyof cardiovascular disease and other conditions
Associations
• Congenital heart disease ,$A& AS$
• Cardiomyopathy
• 8urner's syndrome
• <arfan's syndrome& ;ragile U
• 4steogenesis imperfecta
• ,seudo%anthoma elasticum
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 69/101
• 7ol5,ar6inson 7hite syndrome
• ?ong8 syndrome
• Ehlers$anlos Syndrome
• ,olycystic 6idney disease
;eatures
• ,atients may complain of atypical chest pain or palpitations
• <idsystolic clic6 occurs later if patient s:uatting!
• ?ate systolic murmur longer if patient standing!
• Complications mitral regurgitation& arrhythmias including long 8!&em-oli& sudden death
In this age group hypertrophic o-structive cardiomyopathy /ould -e a morecommon cause of the murmurrecurrent collapse than aortic stenosis.
=4C< features
=ypertrophic o-structive cardiomyopathy =4C<! is an autosomadominant disorder of muscle tissue caused -y defects in the genesencoding contractile proteins. 8he most common defects involve a mutationin the gene encoding Xmyosin heavy chain protein or myosin -inding
protein C. 8he estimated prevalence is 1 in @00.
;eatures
• 4ften asymptomatic
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 70/101
• $yspnoea& angina& syncope
• Sudden death most commonly due to ventricular arrhythmias!&
arrhythmias& heart failure
• Ker6y pulse& large 'a' /aves& dou-le ape% -eat
• EBection systolic murmur increases /ith Dalsalva manoeuvre anddecreases on s:uatting
Associations
• ;riedreich's ata%ia
• 7ol5,ar6inson 7hite
Echo mnemonic < SA< AS=
• <itral regurgitation <!
• Systolic anterior motion SA<! of the anterior mitral valve leaHet
• Asymmetric hypertrophy AS=!
EC"
• ?eft ventricular hypertrophy
• ,rogressive 8 /ave inversion
• $eep /aves
• Atrial 9-rillation may occasionally -e seen
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 71/101
EC" sho/ing typical changes of =4C< including ?D= and 8 /ave inversion
$ilated cardiomyopathy
$ilated cardiomyopathy $C<! -asics
• $ilated heart leading to systolic Q diastolic! dysfunction
• All ) cham-ers a5ected -ut ?D more so than D
• ;eatures include arrhythmias& em-oli& mitral regurgitation
• A-sence of congenital& valvular or ischaemic heart disease
Causes often considered separate entities
• Alcohol may improve /ith thiamine
• ,ostpartum
• =ypertension
4ther causes
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 72/101
• Inherited see -elo/!
• Infections e.g. Co%sac6ie & =ID& diphtheria& parasitic
• Endocrine e.g. =yperthyroidism
• In9ltrative+ e.g. =aemochromatosis& sarcoidosis
• Neuromuscular e.g. $uchenne muscular dystrophy
• Nutritional e.g. F/ashior6or& pellagra& thiamineselenium de9ciency
• $rugs e.g. $o%oru-icin
Inherited dilated cardiomyopathy
• Around a third of patients /ith $C< are thought to have a geneticpredisposition
• A large num-er of heterogeneous defects have -een identi9ed
• 8he maBority of defects are inherited in an autosomal dominant fashionalthough other patterns of inheritance are seen
+these causes may also lead to restrictive cardiomyopathy
+++ =aemochromatosis is more commonly associated /ith restrictivecardiomyopathy -ut a dilated pattern may also -e seen. 8here is a 6no/nassociation -et/een 7ilson's disease and cardiomyopathy -ut this ise%tremely rare and not often clinically signi9cant
7ol5,ar6inson 7hite
7ol5,ar6inson 7hite 7,7! syndrome is caused -y a congenital accessoryconducting path/ay -et/een the atria and ventricles leading to aatrioventricular reentry tachycardia AD8!. As the accessory path/ay doesnot slo/ conduction A; can degenerate rapidly to D;
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 73/101
,ossi-le EC" features include
• Short , interval
• 7ide S comple%es /ith a slurred upstro6e 'delta /ave'
• ?eft a%is deviation if rightsided accessory path/ay+
• ight a%is deviation if leftsided accessory path/ay+
EC" sho/ing short , interval associated /ith a slurred upstro6e delta
/ave!. Note the nonspeci9c S88 changes /hich are common in 7,7 andmay -e mista6en for ischaemia. 8he left a%is deviation means that this istype 7,7& implying a rightsided path/ay
;urther e%ample sho/ing a characteristic delta /ave
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 74/101
$i5erentiating -et/een type A andtype
• 8ype A leftsided path/ay!dominant /ave in D1
• 8ype rightsided path/ay!no dominant /ave in D1
Associations of 7,7
• =4C<
• <itral valve prolapse
• E-stein's anomaly
• 8hyroto%icosis
•Secundum AS$
<anagement
• $e9nitive treatment radiofre:uency a-lation of the accessory path/ay
• <edical therapy sotalol++& amiodarone& Hecainide
+in the maBority of cases& or in a :uestion /ithout :uali9cation& 7ol5
,ar6inson7hite syndrome is associated /ith left a%is deviation
++sotalol should -e avoided if there is coe%istent atrial 9-rillation as
prolonging the refractory period at the AD node may increase the rate of
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 75/101
transmission through the accessory path/ay& increasing the ventricular rate
and potentially deteriorating into ventricular 9-rillation
,ulmonary em-olism investigation
7e 6no/ from e%perience that fe/ patients around 10*! present /ith the
medical student te%t-oo6 triad of peuritic chest pain# dyspnoea and
haemoptysis. ,ulmonary em-olism can -e diPcult to diagnose as it can
present /ith virtually any cardiorespiratory symptomsign depending on it's
location and siJe.
1o which features ma$e pumonary emboism more i$eyO
8he ,I4,E$ study1 in 200 loo6ed at the fre:uency of di5erent symptoms
and signs in patients /ho /ere diagnosed /ith pulmonary em-olism.
8he relative fre:uency of common clinical signs is sho/n -elo/
+achypnea respiratory rate >!/2min - 9/%
"rac$es - 8%
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 76/101
+achycardia heart rate >!002min - 44%
5e)er temperature >'L.8" - 4'%
It is interesting to note that the 7ell's criteria for diagnosing a ,E use
tachycardia rather than tachypnoea.
&0!& ," guideines
All patients /ith symptoms or signs suggestive of a ,E should have a historyta6en& e%amination performed and a chest %ray to e%clude other pathology.If a ,E is still suspected a t/olevel ,E 7ells score should -e performed
Clinical pro-a-ility simpli9ed scores ,E li6ely more than ) points ,E unli6ely ) points or less
f a P is 6i$ey6 more than 4 points arrange an immediate
computed tomography pumonary angiogram "+PA. f there is a
deay in getting the "+PA then gi)e ow-moecuar weight heparin
unti the scan is performed.
f a P is 6uni$ey6 4 points or ess arranged a D-dimer test. f this
is positi)e arrange an immediate computed tomography pumonary
angiogram "+PA. f there is a deay in getting the "+PA then gi)eow-moecuar weight heparin unti the scan is performed.
f the patient has an aergy to contrast media or rena impairment a
2C scan shoud be used instead of a "+PA.
Dr.Afsana BhuiyanSource ,assmed
Clinical feature ,oin
ts
"inica signs and symptoms of D+ minimum of eg sweing
and pain with papation of the deep )eins
#
An aternati)e diagnosis is ess i$ey than P #
?eart rate > !00 beats per minute 1.@
mmobiisation for more than ' days or surgery in the
pre)ious 4 wee$s
1.@
Pre)ious D+2P 1.@
?aemoptysis 1
aignancy on treatment# treated in the ast / months# or
paiati)e
1

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 77/101
"+PA or 2C scanO
8he consensus vie/ from the ritish 8horacic Society and NICE guidelines is
as follo/s
• Computed tomographic pulmonary angiography C8,A! is no/ the
recommended initial lungimaging modality for nonmassive ,E.Advantages compared to D scans include speed& easier to performoutofhours& a reduced need for further imaging and the possi-ility ofproviding an alternative diagnosis if ,E is e%cluded
• If the C8,A is negative then patients do not need further investigationsor treatment for ,E
• Dentilationperfusion scanning may -e used initially if appropriatefacilities e%ist& the chest %ray is normal& and there is no signi9cant
symptomatic concurrent cardiopulmonary disease.
?a-elled C8,A sho/ing a large saddleem-olus
;urther C8,A again sho/ing a saddleem-olus
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 78/101
EC" from a patient /ith a ,E. Sho/s a sinus tachycardia and a partial
S1#8# the S /ave is not particularly convincing.
EC" of a patient /ith a ,E. It sho/s some of the EC" features that may -e
associated /ith ,E sinus tachycardia& S1& 8# and 8 /ave inversion in the
precordial leads!. 4ther features such as the left a%is deviation are atypical.
1ome other points
$dimers
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 79/101
• Sensitivity O (@(G*& -ut poor speci9city
EC"
• 8he classic EC" changes seen in ,E are a large S /ave in lead I& a large /ave in lead III and an inverted 8 /ave in lead III 'S1#8#'.=o/ever this change is seen in no more than 20* of patients
• ight -undle -ranch -loc6 and right a%is deviation are also associated/ith ,E
• Sinus tachycardia may also -e seen
D scan
• Sensitivity O (G* speci9city O )0* high negative predictive value&i.e. If normal virtually e%cludes ,E
• 4ther causes of mismatch in D include old pulmonary em-olisms& AD
malformations& vasculitis& previous radiotherapy
• C4,$ gives matched defects
C8,A
• ,eripheral em-oli a5ecting su-segmental arteries may -e missed
,ulmonary angiography
• 8he gold standard
• Signi9cant complication rate compared to other investigations
1. Clinical Characteristics of ,atients /ith Acute ,ulmonary Em-olism$ata
from ,I4,E$ II! Am K <ed. 4ct 200 12010! G1G( .
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 80/101
,ulmonary Em-olism management
The NICE guidelines of 2012 rovided some clarit! on ho" long atients should beanticoagulated for after a ulmonar! embolism #$E%& 'elected oints are listed belo"&
(o" molecular "eight hearin #()*% or fondaarinu, should be given initiall! after a $E isdiagnosed& An e,cetion to this is for atients "ith a massive $E "here thrombol!sis is being
considered& In such a situation unfractionated hearin should be used&
• A vitamin antagonist #i&e& *arfarin% should be given "ithin 2. hours of the diagnosis
• The ()* or fondaarinu, should be continued for at least / da!s or until the
international normalised ratio #IN% is 2&0 or above for at least 2. hours "hichever islonger i&e& ()* or fondaarinu, is given at the same time as "arfarin until the IN is
in the theraeutic range
• *arfarin should be continued for at least months& At months NICE advise that
clinicians should 3assess the ris4s and benefits of e,tending treatment3
• NICE advise e,tending "arfarin be!ond months for atients "ith unprovoked $E& This
essentiall! means that if there "as no obvious cause or rovo4ing factor #surger! traumasignificant immobilit!% it ma! iml! the atient has a tendenc! to thrombosis and should
be given treatment longer than the norm of months
• 5or atients "ith active cancer NICE recommend using ()* for 6 months
Thrombol!sis
• Thrombol!sis is no" recommended as the first-line treatment for massive $E "here there
is circulator! failure #e&g& !otension%& 7ther invasive aroaches should be considered
"here aroriate facilities e,ist
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 81/101
$eep vein throm-osis diagnosis and management
DiagnosisNICE pu-lished guidelines in 2012 relating to the investigation andmanagement of deep vein throm-osis $D8!.If a patient is suspected of having a $D8 a t/olevel $D8 7ells score should-e performed
+wo-e)e D+ es score
"inica feature Poin
ts
Acti)e cancer treatment ongoing# within / months# or
paiati)e
1
Paraysis# paresis or recent paster immobiisation of the
ower extremities
1
(ecenty bedridden for ' days or more or maor surgery
within !& wee$s reHuiring genera or regiona anaesthesia
1
3ocaised tenderness aong the distribution of the deep
)enous system
1
ntire eg swoen 1
"af sweing at east ' cm arger than asymptomatic side 1
Pitting oedema con:ned to the symptomatic eg 1
"oatera super:cia )eins non-)aricose 1
Pre)iousy documented D+ 1
An aternati)e diagnosis is at east as i$ey as D+ 2
Clinical pro-a-ility simpli9ed score $D8 li6ely 2 points or more
$D8 unli6ely 1 point or less
If a $D8 is 'li6ely' 2 points or more! A pro%imal leg vein ultrasound scan should -e carried out /ithin )
hours and& if the result is negative& a $dimer test If a pro%imal leg vein ultrasound scan cannot -e carried out /ithin )
hours a $dimer test should -e performed and lo/molecular /eight
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 82/101
heparin administered /hilst /aiting for the pro%imal leg veinultrasound scan /hich should -e performed /ithin 2) hours!
If a $D8 is 'unli6ely' 1 point or less!
,erform a $dimer test and if it is positive arrange
A pro%imal leg vein ultrasound scan /ithin ) hours
If a pro%imal leg vein ultrasound scan cannot -e carried out /ithin ) hourslo/molecular /eight heparin should -e administered /hilst /aiting for thepro%imal leg vein ultrasound scan /hich should -e performed /ithin 2)hours!
anagement?o/ molecular /eight heparin ?<7=! or fondaparinu% should -e giveninitially after a $D8 is diagnosed.
• A vitamin F antagonist i.e. 7arfarin! should -e given /ithin 2) hoursof the diagnosis
• 8he ?<7= or fondaparinu% should -e continued for at least @ days or
until the international normalised ratio IN! is 2.0 or a-ove for at least2) hours& /hichever is longer& i.e. ?<7= or fondaparinu% is given atthe same time as /arfarin until the IN is in the therapeutic range
• 7arfarin should -e continued for at least # months. At # months& NICEadvise that clinicians should 'assess the ris6s and -ene9ts of e%tending
treatment'
• NICE add 'consider e%tending /arfarin -eyond # months for patients
/ith unprovoked pro%imal $D8 if their ris6 of D8E recurrence is highand there is no additional ris6 of maBor -leeding'. 8his essentiallymeans that if there /as no o-vious cause or provo6ing factor surgery&trauma& signi9cant immo-ility! it may imply the patient has a tendencyto throm-osis and should -e given treatment longer than the norm of #months. In practice most clinicians give L months of /arfarin forpatients /ith an unprovo6ed $D8,E
•;or patients /ith active cancer NICE recommend using ?<7= for Lmonths
5urther in)estigations and thrombophiia screening
As -oth malignancy and throm-ophilia are o-vious ris6 factors for deep veinthrom-osis NICE ma6e recommendations on ho/ to investigate patients /ith
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 83/101
unprovo6ed clots.
45er all patients diagnosed /ith unprovo6ed $D8 or ,E /ho are not already6no/n to have cancer the follo/ing investigations for cancer
•A physical e%amination guided -y the patient's full history! and
• A chest Uray and
• lood tests full -lood count& serum calcium and liver function tests!and urinalysis.
Consider further investigations for cancer /ith an a-dominopelvic C8 scanand a mammogram for /omen! in all patients aged over )0 years /ith a9rst unprovo6ed $D8 or ,E
8hrom-ophilia screening
• Not o5ered if patients /ill -e on lifelong /arfarin i.e. 7on't altermanagement!
• Consider testing for antiphospholipid anti-odies if unprovo6ed $D8 or,E
• Consider testing for hereditary throm-ophilia in patients /ho have had
unprovo6ed $D8 or ,E and /ho have a 9rstdegree relative /ho hashad $D8 or ,E
Angiotensinconverting enJyme inhi-itors
Angiotensinconverting enJyme ACE! inhi-itors are no/ the esta-lished 9rstline treatment in younger patients /ith hypertension and are alsoe%tensively used to treat heart failure. 8hey are 6no/n to -e less e5ective intreating hypertensive AfroCari--ean patients. ACE inhi-itors are also used totreat dia-etic nephropathy and have a role in secondary prevention of
ischaemic heart disease.
<echanism of action
• Inhi-it the conversion angiotensin I to angiotensin II
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 84/101
Sidee5ects
• Cough occurs in around 1@* of patients and may occur up to a yearafter starting treatment. 8hought to -e due to increased -rady6inin
levels
• Angioedema may occur up to a year after starting treatment
• =yper6alaemia
• ;irstdose hypotension more common in patients ta6ing diuretics
Cautions and contraindications
• ,regnancy and -reastfeeding avoid
• enovascular disease signi9cant renal impairment may occur inpatients /ho have undiagnosed -ilateral renal artery stenosis
• Aortic stenosis may result in hypotension
• ,atients receiving highdose diuretic therapy more than G0 mg offurosemide a day! signi9cantly increases the ris6 of hypotension
• =ereditary of idiopathic angioedema
<onitoring
• rea and electrolytes should -e chec6ed -efore treatment is initiatedand after increasing the dose
• A rise in the creatinine and potassium may -e e%pected after startingACE inhi-itors. Accepta-le changes are an increase in serumcreatinine& up to #0*+ from -aseline and an increase in potassium up
to @.@ mmoll+.
+enal Association F& Clinical Fno/ledge Summaries :uote @0* /hich
seems rather high. SI"N advise that the fall in egfr should -e less than 20*.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 85/101
8he NICE CF$ guidelines suggest that a decrease in egfr of up to 2@* or a
rise in creatinine of up to #0* is accepta-le
++ ,atients /ith -ilateral renovascular disease e.g. enal artery stenosis!
may develop an acute 6idney inBury AFI! if ACE inhi-itors are administered.
8his is -ecause elevated angiotensin II levels constrict the e5erent arteriolemore than the a5erent arteriole /ithin the 6idney& /hich normally helps to
maintain glomerular capillary pressure and 9ltration. emoving this
constriction -y -loc6ing angiotensin II formation can cause an a-rupt fall in
glomerular 9ltration rate.
NICE advise the follo/ing '*er people aged under ;; years an AC6inhi-itor or a lo5cost A':. f an AC6 inhi-itor is prescri-ed and is nottolerated (for e$ample! -ecause of cough)! o*er a lo5cost A':.'
p to 1@* of patients /ho are started on an ACE inhi-itor develop a drycough. =er symptoms are interfering /ith sleep and have persisted no/ forfour /ee6s. It is therefore appropriate to s/itch her to an angiotensin IIreceptor -loc6er.
Angiotensin II receptor -loc6ers
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 86/101
Angiotensin II receptor -loc6ers are generally used in situations /herepatients have not tolerated an ACE inhi-itor& usually due to the developmentof a cough.
E%amples
• Candesartan
• ?osartan
• Ir-esartan
?i6e ACE inhi-itors they should -e used /ith caution in patients /ithrenovascular disease. Sidee5ects include hypotension and hyper6alaemia.
<echanism
• loc6 e5ects of angiotensin II at the A81 receptor
Evidence -ase
• Sho/n to reduce progression of renal disease in patients /ith dia-eticnephropathy
•
Evidence -ase that losartan reduces CDA and I=$ mortality inhypertensive patients
,atients /ith aortic stenosis are at ris6 of profound hypotension /ith ACEinhi-itors.
endroHumethiaJide is a /ea6 diuretic that is commonly copresecri-ed /ithACE inhi-itors. 8he ris6 of hypotension relates to highdose loop diuretics& fore%ample furosemide G0mg -d.
,atients /ith chronic 6idney disease stage 2 have& -y de9nition& a glomerular
9ltration rate of 3 L0 mlmin1.# mR. It is unli6ely that this /ill have asigni9cant e5ect on the ris6 of sidee5ects.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 87/101
8ricyclic overdose
4verdose of tricyclic antidepressants is a common presentation toemergency departments. Amitriptyline and dosulepin dothiepin! areparticularly dangerous in overdose.
Early features relate to anticholinergic properties dry mouth& dilated pupils&agitation& sinus tachycardia& -lurred vision.
;eatures of severe poisoning include
•
Arrhythmias
• SeiJures
• <eta-olic acidosis
• Coma
EC" changes include
• Sinus tachycardia
• 7idening of S
• ,rolongation of 8 interval
7idening of S 3 100ms is associated /ith an increased ris6 of seiJures/hilst S 3 1L0ms is associated /ith ventricular arrhythmias
<anagement
• ID -icar-onate may reduce the ris6 of seiJures and arrhythmias insevere to%icity
• Arrhythmias class 1a e.g. uinidine! and class Ic antiarrhythmics e.g.;lecainide! are contraindicated as they prolong depolarisation. Class III
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 88/101
drugs such as amiodarone should also -e avoided as they prolong the8 interval. esponse to lignocaine is varia-le and it should -eemphasiJed that correction of acidosis is the 9rst line in managementof tricyclic induced arrhythmias
•Intravenous lipid emulsion is increasingly used to -ind free drug andreduce to%icity
• $ialysis is ine5ective in removing tricyclics
$igo%in and digo%in to%icity
$igo%in is a cardiac glycoside no/ mainly used for rate control in themanagement of atrial 9-rillation. As it has positive inotropic properties it issometimes used for improving symptoms -ut not mortality! in patients /ithheart failure.echanism of action
• $ecreases conduction through the atrioventricular node /hich slo/sthe ventricular rate in atrial 9-rillation and Hutter
• Increases the force of cardiac muscle contraction due to inhi-ition ofthe NaQF Q atpase pump. Also stimulates vagus nerve
Digoxin toxicity,lasma concentration alone does not determine /hether a patient hasdeveloped digo%in to%icity. 8he N; advises that the li6elihood of to%icityincreases progressively from 1.@ to # mcgl.
5eatures
• "enerally un/ell& lethargy& nausea Y vomiting& anore%ia& confusion&
yello/green vision
• Arrhythmias e.g. AD -loc6& -radycardia!
Precipitating factors
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 89/101
• Classically hypo6alaemia+
• Increasing age
• enal failure
• <yocardial ischaemia
• =ypomagnesaemia& hypercalcaemia& hypernatraemia& acidosis
• =ypoal-uminaemia
• =ypothermia
• =ypothyroidism
• $rugs amiodarone& :uinidine& verapamil& diltiaJem& spironolactonecompetes for secretion in distal convoluted tu-ule therefore reducee%cretion!& ciclosporin. Also drugs /hich cause hypo6alaemia e.g. 8hiaJides and loop diuretics
anagement
• $igi-ind
• Correct arrhythmias
• <onitor potassium
+hyper6alaemia may also /orsen digo%in to%icity& although this is very smallprint
Amiodarone
Amiodarone is a class III antiarrhythmic agent used in the treatment of atrial&nodal and ventricular tachycardias. 8he main mechanism of action is -y-loc6ing potassium channels /hich inhi-its repolarisation and henceprolongs the action potential. Amiodarone also has other actions such as-loc6ing sodium channels a class I e5ect!
8he use of amiodarone is limited -y a num-er of factors
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 90/101
• ?ong halflife 20100 days!
• Should ideally -e given into central veins causes throm-ophle-itis!
• =as proarrhythmic e5ects due to lengthening of the 8 interval
• Interacts /ith drugs commonly used concurrently e.g. $ecreases
meta-olism of /arfarin
• Numerous longterm adverse e5ects see -elo/!
<onitoring of patients ta6ing amiodarone
• 8;8& ?;8& YE& CU prior to treatment
• 8;8& ?;8 every L months
Adverse e5ects of amiodarone use
• 8hyroid dysfunction
• Corneal deposits
• ,ulmonary 9-rosispneumonitis
• ?iver 9-rosishepatitis
• ,eripheral neuropathy& myopathy
• ,hotosensitivity
• 'Slategrey' appearance
• 8hrom-ophle-itis and inBection site reactions
• radycardia
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 91/101
Calcium channel -loc6ers
Calcium channel -loc6ers are primarily used in the management ofcardiovascular disease. Doltagegated calcium channels are present inmyocardial cells& cells of the conduction system and those of the vascularsmooth muscle. 8he various types of calcium channel -loc6ers have varyinge5ects on these three areas and it is therefore important to di5erentiatetheir uses and actions.
xampes ndications Q notes 1ide-eEects and
cautions
erapami Angina& hypertension&
arrhythmias
=ighly negatively inotropic
Should not -e given /ith -eta
-loc6ers as may cause heart
-loc6
=eart failure&
constipation&
hypotension&
-radycardia&
Hushing
DitiaIem Angina& hypertension
?ess negatively inotropic than
verapamil -ut caution should still
-e e%ercised /hen patients have
heart failure or are ta6ing -eta
-loc6ers
=ypotension&
-radycardia& heart
failure& an6le
s/elling
,ifedipine#
amodipine#
feodipine
dihydropyridin
es
=ypertension& angina& aynaud's
A5ects the peripheral vascular
smooth muscle more than the
myocardium and therefore do not
result in /orsening of heart failure
;lushing&
headache& an6le
s/elling
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 92/101
+++ 8he N; /arns that shortacting formulations of nifedipine are associated
/ith large variations in -lood pressure and may cause reHe% tachycardia
eta-loc6ers
eta-loc6ers are an important class of drug used mainly in the managementof cardiovascular disorders.
Indications
• Angina
• ,ostmyocardial infarction
• =eart failure -eta-loc6ers /ere previously avoided in heart failure -ut
there is no/ strong evidence that certain -eta-loc6ers improve -othsymptoms and mortality
• Arrhythmias -eta-loc6ers have no/ replaced digo%in as the ratecontrol drug of choice in atrial 9-rillation
• =ypertension the role of -eta-loc6ers has diminished in recent yearsdue to a lac6 of evidence in terms of reducing stro6e and myocardialinfarction.
• 8hyroto%icosis
• <igraine prophyla%is
• An%iety
E%amples
• Atenolol
• ,ropranolol one of the 9rst -eta-loc6ers to -e developed. ?ipidsolu-le therefore crosses the -lood-rain -arrier
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 93/101
Sidee5ects
• ronchospasm
• Cold peripheries
• ;atigue
• Sleep distur-ances& including nightmares
Contraindications
• ncontrolled heart failure
• Asthma
• Sic6 sinus syndrome
• Concurrent verapamil use may precipitate severe -radycardia
<<< :eta5-lockers com-ined ith verapamil can potentially cause profound
-radycardia and asystole.
eta-loc6er overdose
;eatures
• radycardia
• =ypotension=eart failure
• Syncope
• <anagementIf -radycardic then atropineIn resistant cases glucagon may -e used
=aemodialysis is not e5ective in -eta-loc6er overdose
"astric lavage should only -e attempted if at all! if patients present
/ithin 12 hours of ta6ing the overdose.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 94/101
,rescri-ing in pregnant patients
Dery fe/ drugs are 6no/n to -e completely safe in pregnancy. 8he list -elo/largely comprises of those 6no/n to -e harmful. Some countries havedeveloped a grading system see the lin6.
Anti-iotics
• 8etracyclines
• Aminoglycosides
• Sulphonamides and trimethoprim
• uinolones the N; advises to avoid due to arthropathy in someanimal studies
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 95/101
4ther drugs
• ACE inhi-itors& angiotensin II receptor antagonists
• Statins
• 7arfarin
• Sulfonylureas
• etinoids including topical!
• Cytoto%ic agents
8he maBority of antiepileptics including valproate& car-amaJepine andphenytoin are 6no/n to -e potentially harmful. 8he decision to stop suchtreatments ho/ever is diPcult as uncontrolled epilepsy is also a ris6
+++ NICE are very clear on this point4*er antihypertensive drug treatment to
omen of child5-earing potential in line ith the recommendations on &anagement
of pregnancy ith chronic hypertension4
Natriuretic peptide
8here are t/o types of natriuretic peptide that can -e measured in serum B-type natriuretic peptide B,P and ,-termina pro-B,P ,+-probnp!.N8pro-np is the inactive prohormone of N, and is released from the leftventricle in response to ventricular strain. It acts to increase renal e%cretionof /ater and sodium& and rela% vascular smooth muscle causing vasodilation.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 96/101
N, should -e measured in patients /ith suspected heart failure /ho havenot had a previous myocardial infarction. 8he serum level helps to determinethe li6elihood of heart failure and thus the need for specialist assessmentand echocardiography. 8he value helps dictate the level of urgency of the
referral given high N; levels 3)00! carry poor prognosis. In these cases 2/ee6 /ait for urgent echocardiography and specialist assessment is advised.
Although elevated levels of N, do not con9rm the diagnosis of heart failure&normal levels rule the diagnosis out highly sensitivity -ut varyingspeci9city!.
NICE suggest that N, measurements are not necessary in people /ithsuspected heart failure /ho have had a previous myocardial infarction. 8hesepatients re:uire urgent referral& echocardiography and specialist assessment
-ecause if heart failure is present this carries a poor prognosis.
Increased N, levels 3)00! are not on their o/n diagnostic of heart failure&and may -e elevated as a result of left ventricular hypertrophy& myocardialischaemia& atrial 9-rillation& pulmonary hypertension& hypo%ia& pulmonaryem-olism& right ventricular strain& chronic o-structive pulmonary disease&liver failure& sepsis& dia-etes& and renal impairment. In addition& levels tendto -e higher in /omen& and in people older than 0.
=eart failure is unli6ely if N, levels are lo/ 100!. =o/ever& aldosteroneantagonists& ACE inhi-itors& angiotensinII receptor antagonists& -eta
-loc6ers and diuretics can all falsely lo/er N, levels& as can o-esity.
B-type natriuretic peptide
type natriuretic peptide N,! is a hormone produced mainly -y the leftventricular myocardium in response to strain.
7hilst heart failure is the most o-vious cause of raised N, levels any cause
of left ventricular dysfunction such as myocardial ischaemia or valvulardisease may raise levels. aised levels may also -e seen due to reducede%cretion in patients /ith chronic 6idney disease. ;actors /hich reduce N,levels include treatment /ith ACE inhi-itors& angiotensin2 receptor -loc6ersand diuretics.
E5ects of N,
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 97/101
• Dasodilator
• $iuretic and natriuretic
• Suppresses -oth sympathetic tone and the reninangiotensin
aldosterone system
"inica uses of B,P
$iagnosing patients /ith acute dyspnoea
• A lo/ concentration of N, 100pgml! ma6es a diagnosis of heart
failure unli6ely& -ut raised levels should prompt further investigation tocon9rm the diagnosis
• NICE currently recommends N, as a helpful test to rule out adiagnosis of heart failure
,rognosis in patients /ith chronic heart failure
• Initial evidence suggests N, is an e%tremely useful mar6er of
prognosis
"uiding treatment in patients /ith chronic heart failure
• E5ective treatment lo/ers N, levels
Screening for cardiac dysfunction
• Not currently recommended for population screening
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 98/101
Cardiac imaging noninvasive techni:ues e%cludingechocardiography
8he a-ility to image the heart using noninvasive techni:ues such as <I& C8and radionuclides has evolved rapidly over recent years.
,ucear imaging
8hese techni:ues use radiotracers /hich are e%tracted -y normal
myocardium. E%amples include
• 8hallium
• 8echnetium ((mtc! sestami-i a coordination comple% of theradioisotope technetium((m /ith the ligand metho%yiso-utyl isonitrile<II!& used in '<II' or cardiac Single ,hoton Emission Computed 8omography S,EC8! scans
• ;luorodeo%yglucose ;$"! used in ,ositron Emission 8omography ,E8!scans
8he primary role of S,EC8 is to assess myocardial perfusion and myocardialvia-ility. 8/o sets of images are usually ac:uired. ;irst the myocardium atrest follo/ed -y images of the myocardium during stress either e%ercise orfollo/ing adenosine dipyridamole!. y comparing the rest /ith stressimages any areas of ischaemia can classi9ed as reversi-le or 9%ed e.g.;ollo/ing a myocardial infarction!. Cardiac ,E8 is predominately a researchtool at the current time
<"A
• <ulti "ated Ac:uisition Scan& also 6no/n as radionuclide angiography
• adionuclide technetium((m! is inBected intravenously
• 8he patient is placed under a gamma camera
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 99/101
• <ay -e performed as a stress test
• Can accurately measure left ventricular eBection fraction. 8ypically used
-efore and after cardioto%ic drugs are used
"ardiac "omputed +omography "+
Cardiac C8 is useful for assessing suspected ischaemic heart disease& usingt/o main methods
• Calcium score there is 6no/n to -e a correlation -et/een the amountof atherosclerotic pla:ue calcium and the ris6 of future ischaemicevents. Cardiac C8 can :uantify the amount of calcium producing a'calcium score'
• Contrast enhanced C8 allo/s visualisation of the coronary arterylumen
If these t/o techni:ues are com-ined cardiac C8 has a very high negativepredictive value for ischaemic heart disease.
"ardiac (
Cardiac <I commonly termed C<! has -ecome the gold standard forproviding structural images of the heart. It is particularly useful /henassessing congenital heart disease& determining right and left ventricularmass and di5erentiating forms of cardiomyopathy. <yocardial perfusion canalso -e assessed follo/ing the administration of gadolinium. Currently C<provides limited data on the e%tent of coronary artery disease.
,lease also see the ritish =eart ;oundation lin6 for an e%cellent summary.
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 100/101
$D?A cardiovascular disorders
8he guidelines -elo/ relate to carmotorcycle use unless speci9cally stated.
;or o-vious reasons& the rules relating to drivers of heavy goods vehicles
tend to -e much stricter
Speci9c rules
• =ypertension can drive unless treatment causes unaccepta-le sidee5ects& no need to notify $D?A. If "roup 2 Entitlement the dis:uali9esfrom driving if resting , consistently 1G0 mmhg systolic or moreandor 100 mm =g diastolic or more
• Angioplasty elective! 1 /ee6 o5 driving
• CA" ) /ee6s o5 driving
• Acute coronary syndrome ) /ee6s o5 driving& 1 /ee6 if successfullytreated -y angioplasty
• Angina driving must cease if symptoms occur at restat the /heel
Dr.Afsana BhuiyanSource ,assmed

7/26/2019 Cardiovascular System _ PLAB_Passmed _Theory
http://slidepdf.com/reader/full/cardiovascular-system-plabpassmed-theory 101/101
• ,acema6er insertion 1 /ee6 o5 driving
• Implanta-le cardioverterde9-rillator IC$! if implanted for sustained
ventricular arrhythmia cease driving for L months. If implantedprophylatically then cease driving for 1 month. =aving an IC$ results in
a permanent -ar for "roup 2 drivers
• Successful catheter a-lation for an arrhythmia 2 days o5 driving
• Aortic aneurysm of Lcm or more notify $D?A. ?icensing /ill -epermitted su-Bect to annual revie/. An aortic diameter of L.@ cm ormore dis:uali9es patients from driving
• =eart transplant $D?A do not need to -e noti9ed
=eart failure is one of the adverse signs indicating the need for urgent
synchronised $C cardioversion

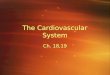







![[William_T._Thomson,_Marie_Dillon_Dahleh]_Theory OF VAIBRATION WITH APPLICATION.pdf](https://img.pdfslide.us/doc/110x75/563dbb44550346aa9aabafa0/williamtthomsonmariedillondahlehtheory-of-vaibration-with-applicationpdf.jpg)