Embed Size (px)
Citation preview
Cardiovascular SystemCardiovascular System
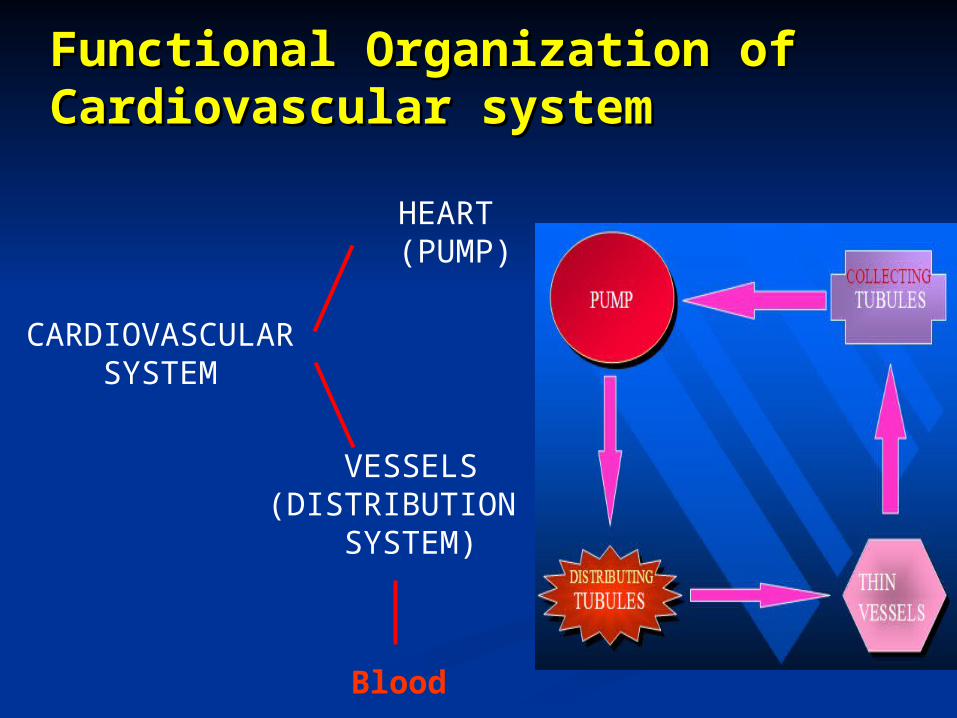
Functional Organization of Functional Organization of Cardiovascular systemCardiovascular system
CARDIOVASCULAR SYSTEM
HEART(PUMP)
VESSELS(DISTRIBUTION
SYSTEM)
Blood
Functions of Cardiovascular Functions of Cardiovascular System:System:
I. Primary (main) function of the heart:I. Primary (main) function of the heart:
♥♥ Acts as a muscular pump:Acts as a muscular pump: in order to maintain adequate level of blood in order to maintain adequate level of blood
flow flow throughout CVS by pumping blood under throughout CVS by pumping blood under
press into press into vascular system.vascular system.
♥♥ Responsible for the mass movement of fluid Responsible for the mass movement of fluid in in
body.body.
Functions of Cardiovascular System Functions of Cardiovascular System (continued)(continued)
II. Secondary functions:II. Secondary functions: 1. Transportation:1. Transportation: delivers Odelivers O22 to tissues, & brings back CO to tissues, & brings back CO22 to lungs. to lungs. carries absorbed digestion products to liver & carries absorbed digestion products to liver &
tissues.tissues. carries metabolic wastes to kidneys to be excreted.carries metabolic wastes to kidneys to be excreted. distribution of body fluids. distribution of body fluids.
2. Regulation:2. Regulation: Hormonal: carries hormones to target tissues to produce Hormonal: carries hormones to target tissues to produce
their effects.their effects. Immune: carries antibodies, leukocytes (WBCs), Immune: carries antibodies, leukocytes (WBCs),
cytokines, & complement cytokines, & complement to aid body defense mechanism against pathogens.to aid body defense mechanism against pathogens. Protection: carries platelets, & clotting factors to aid Protection: carries platelets, & clotting factors to aid
protection of the bodyprotection of the body in blood clotting mechanism.in blood clotting mechanism. Temperature: helps in regulation of body temperature, Temperature: helps in regulation of body temperature,
by diverting blood by diverting blood to cool or warm the body.to cool or warm the body.
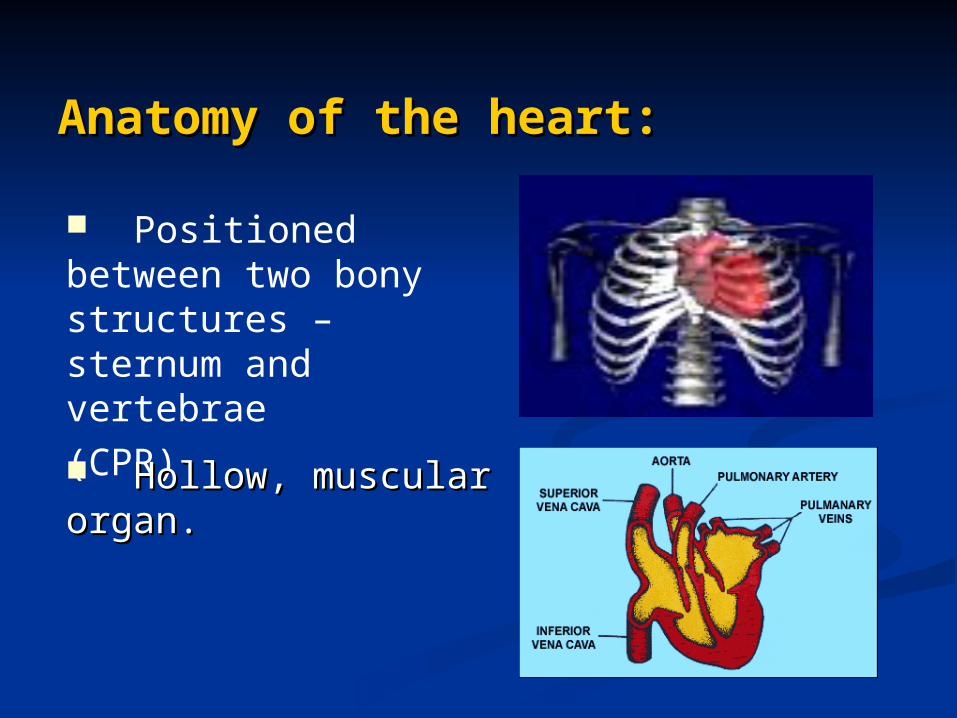
Anatomy of the heart:Anatomy of the heart:
Positioned between two bony structures – sternum and vertebrae
(CPR)
Hollow, muscular organ.Hollow, muscular organ.
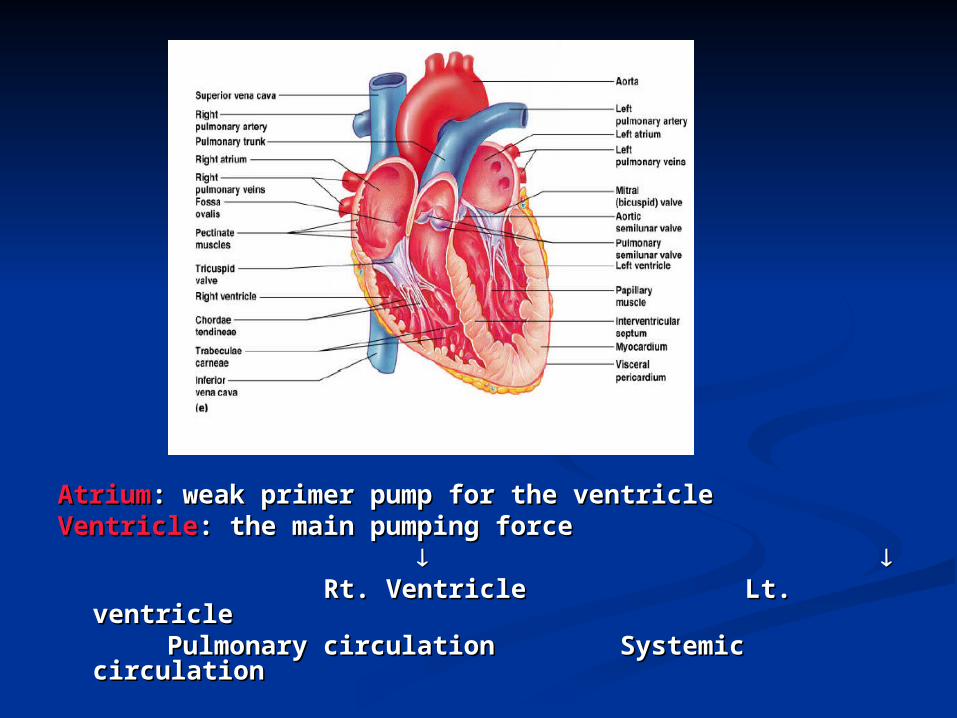
AtriumAtrium: weak primer pump for the ventricle: weak primer pump for the ventricleVentricleVentricle: the main pumping force: the main pumping force Rt. Ventricle Lt. ventricleRt. Ventricle Lt. ventricle Pulmonary circulation Systemic circulationPulmonary circulation Systemic circulation
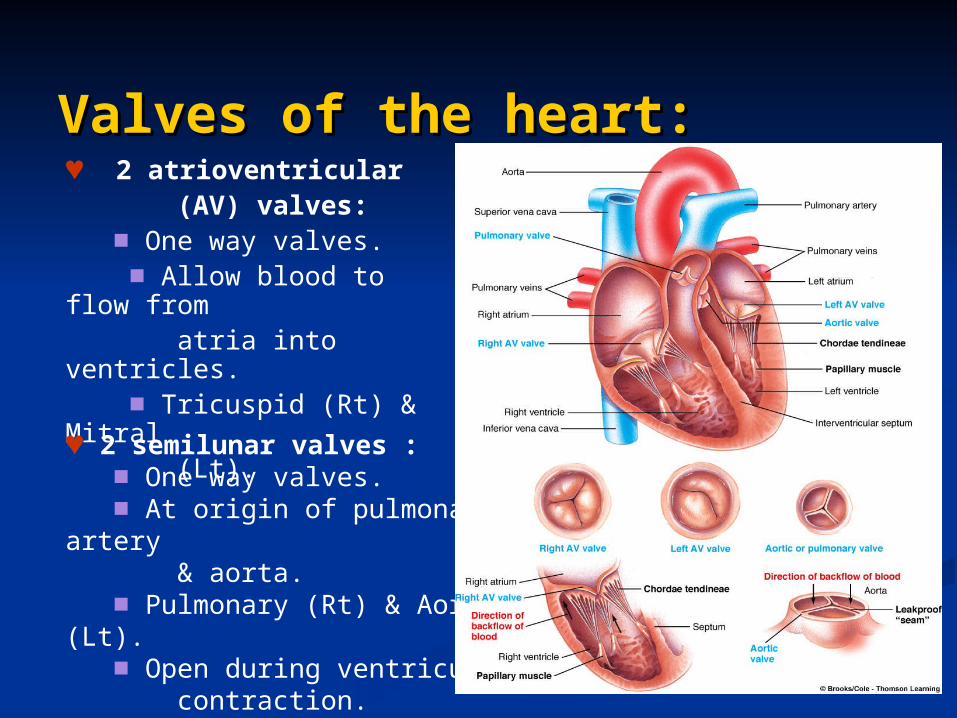
Valves of the heart:Valves of the heart:♥ 2 atrioventricular (AV) valves: ■ One way valves. ■ Allow blood to flow from atria into ventricles. ■ Tricuspid (Rt) & Mitral (Lt).
♥ 2 semilunar valves : ■ One way valves. ■ At origin of pulmonary artery & aorta. ■ Pulmonary (Rt) & Aortic (Lt). ■ Open during ventricular contraction.
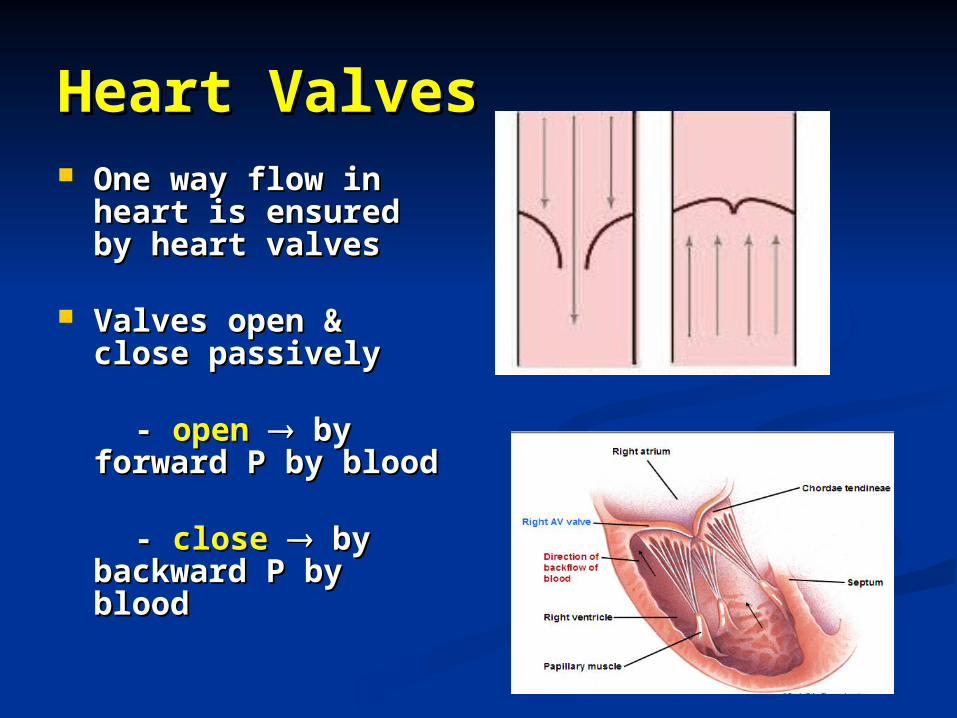
Heart ValvesHeart Valves One way flow in One way flow in
heart is ensured by heart is ensured by heart valvesheart valves
Valves open & Valves open & close passivelyclose passively
-- open open by by forward P by bloodforward P by blood
- - closeclose by by backward P by backward P by bloodblood
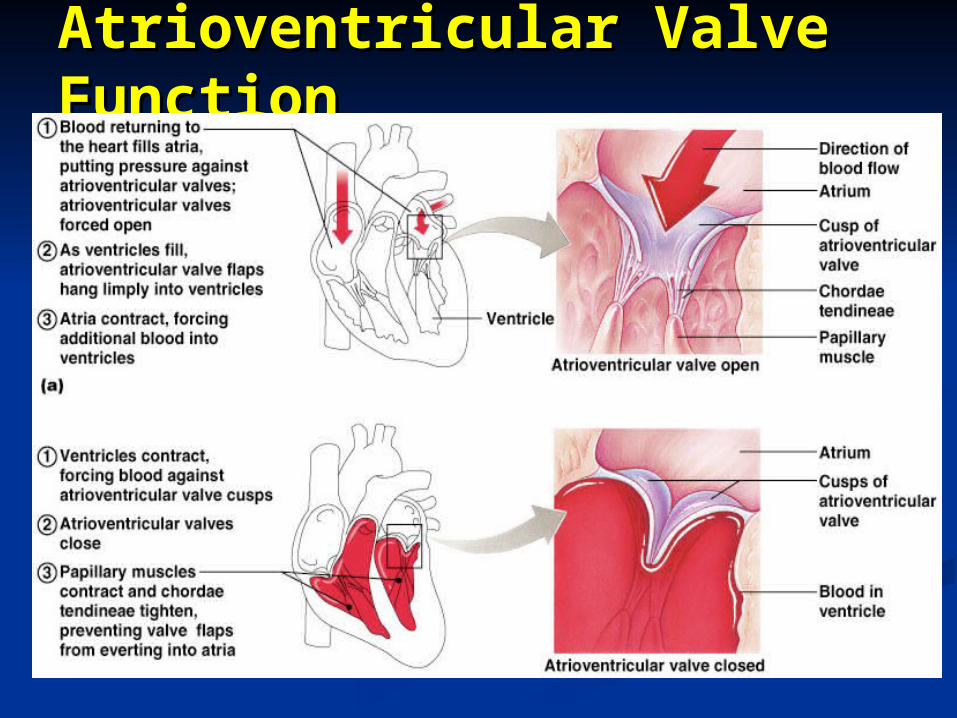
Atrioventricular Valve Atrioventricular Valve FunctionFunction
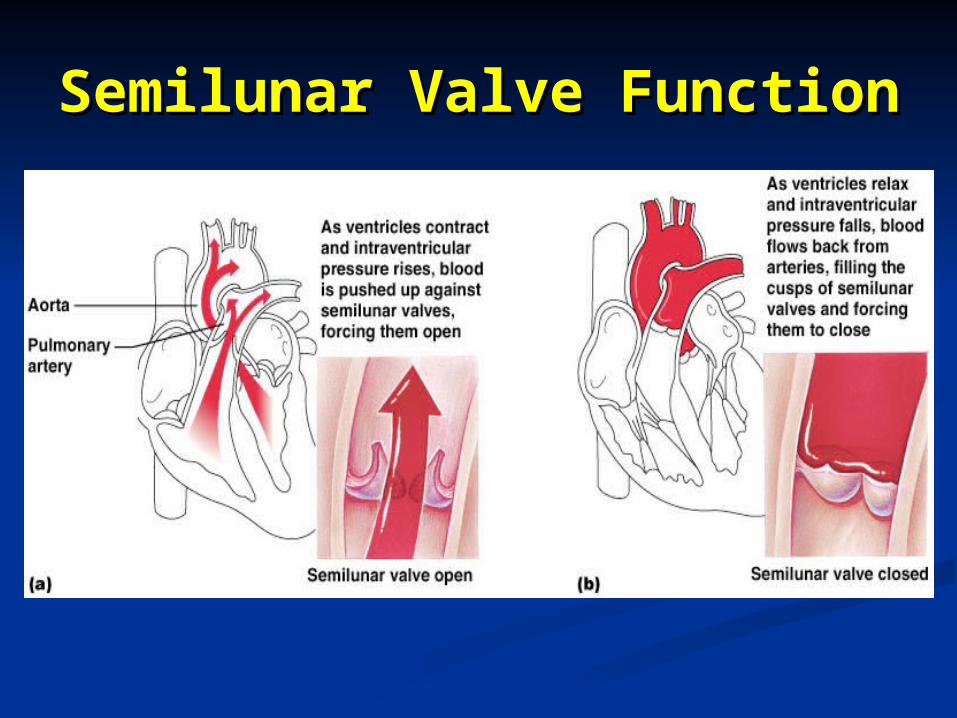
Semilunar Valve Semilunar Valve FunctionFunction
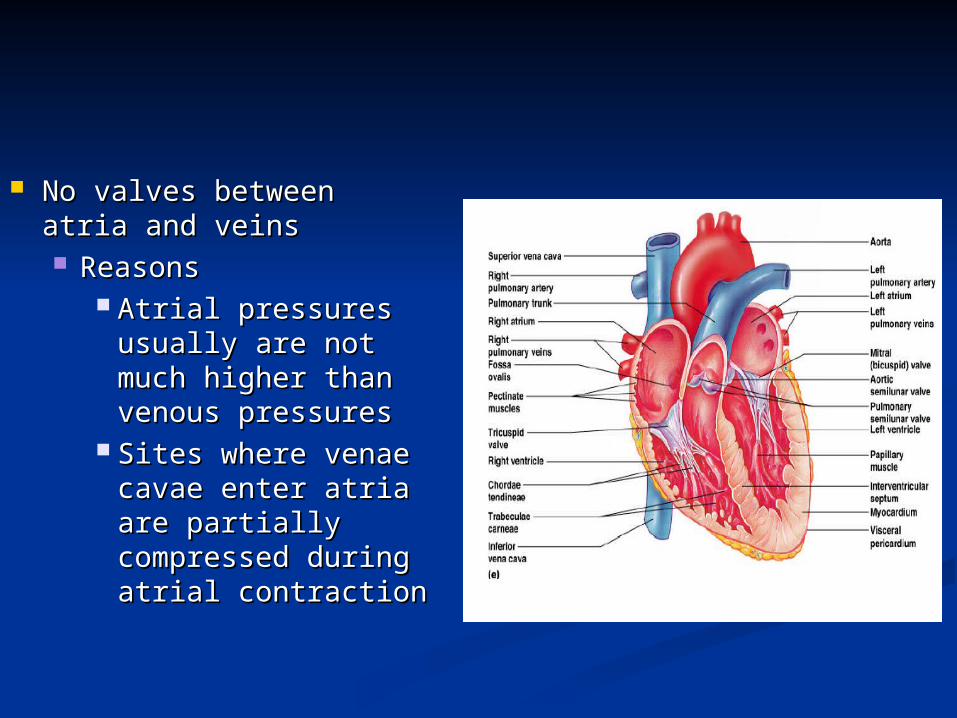
No valves between atria No valves between atria and veinsand veins ReasonsReasons
Atrial pressures Atrial pressures usually are not usually are not much higher than much higher than venous pressuresvenous pressures
Sites where venae Sites where venae cavae enter atria cavae enter atria are partially are partially compressed during compressed during atrial contractionatrial contraction
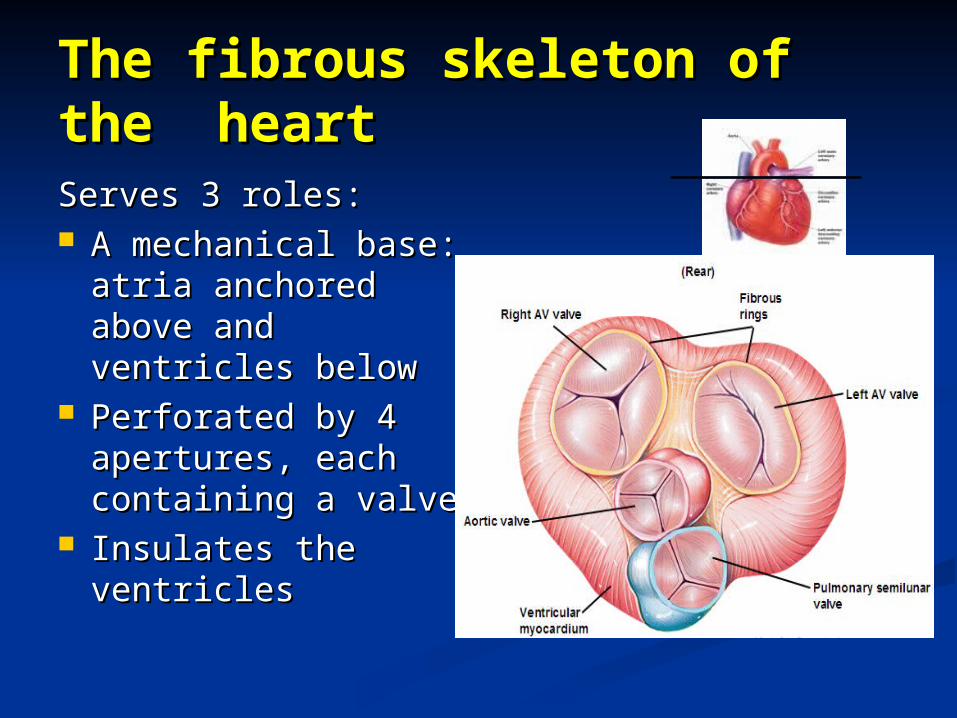
The fibrous skeleton of the The fibrous skeleton of the heartheartServes 3 roles:Serves 3 roles: A mechanical base: A mechanical base:
atria anchored atria anchored above and above and ventricles belowventricles below
Perforated by 4 Perforated by 4 apertures, each apertures, each containing a valvecontaining a valve
Insulates the Insulates the ventriclesventricles
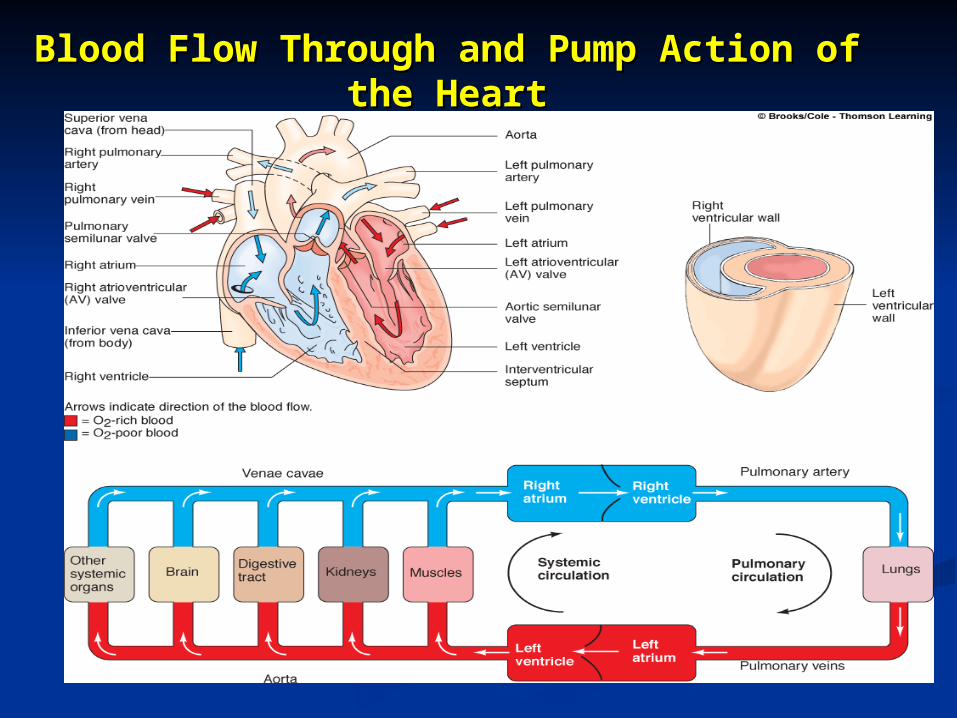
Blood Flow Through and Pump Action Blood Flow Through and Pump Action of the Heartof the Heart
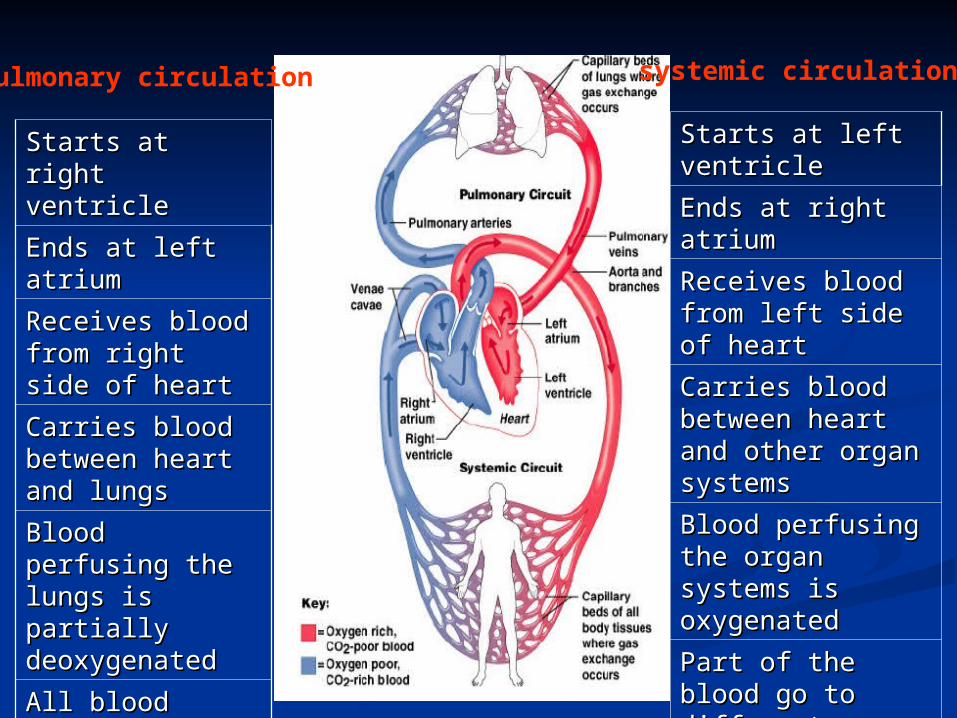
Pulmonary circulation systemic circulation
Starts at right Starts at right ventricleventricle
Ends at left atriumEnds at left atrium
Receives blood Receives blood from right side of from right side of heartheart
Carries blood Carries blood between heart and between heart and lungslungs
Blood perfusing the Blood perfusing the lungs is partially lungs is partially deoxygenateddeoxygenated
All blood flows All blood flows through lungsthrough lungs
Low pressure, low Low pressure, low resistanceresistance
Starts at left ventricleStarts at left ventricle
Ends at right atriumEnds at right atrium
Receives blood from Receives blood from left side of heartleft side of heart
Carries blood Carries blood between heart and between heart and other organ systemsother organ systems
Blood perfusing the Blood perfusing the organ systems is organ systems is oxygenatedoxygenated
Part of the blood go Part of the blood go to different organ to different organ systemssystems
High pressure, high High pressure, high resistanceresistance
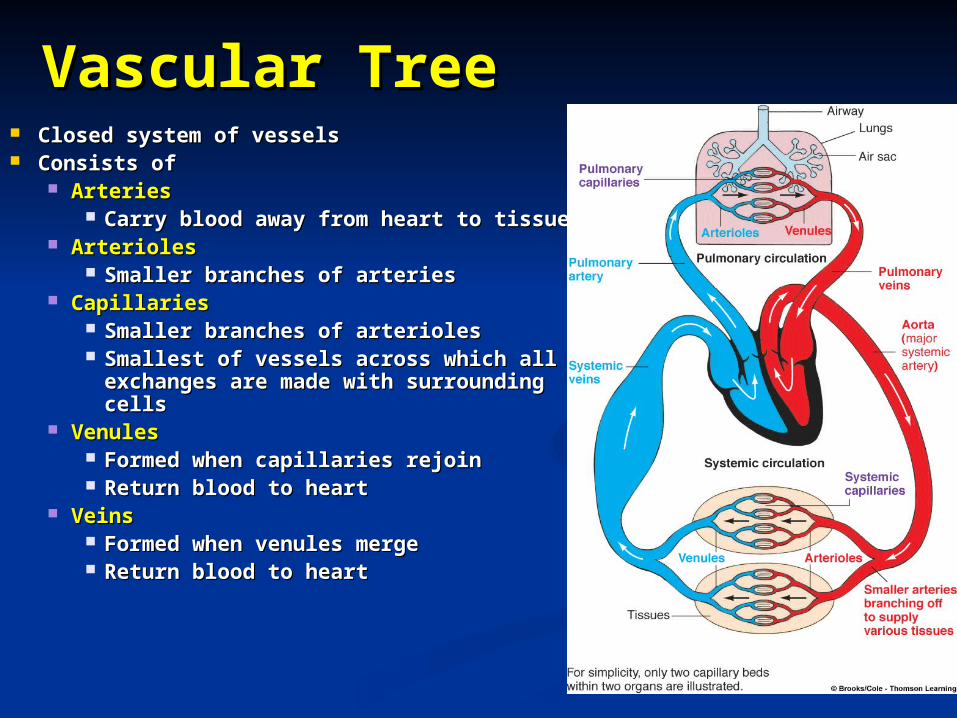
Vascular TreeVascular Tree Closed system of vesselsClosed system of vessels Consists of Consists of
ArteriesArteries Carry blood away from heart to tissuesCarry blood away from heart to tissues
ArteriolesArterioles Smaller branches of arteriesSmaller branches of arteries
CapillariesCapillaries Smaller branches of arteriolesSmaller branches of arterioles Smallest of vessels across which all exchanges Smallest of vessels across which all exchanges
are made with surrounding cellsare made with surrounding cells VenulesVenules
Formed when capillaries rejoinFormed when capillaries rejoin Return blood to heartReturn blood to heart
Veins Veins Formed when venules mergeFormed when venules merge Return blood to heartReturn blood to heart
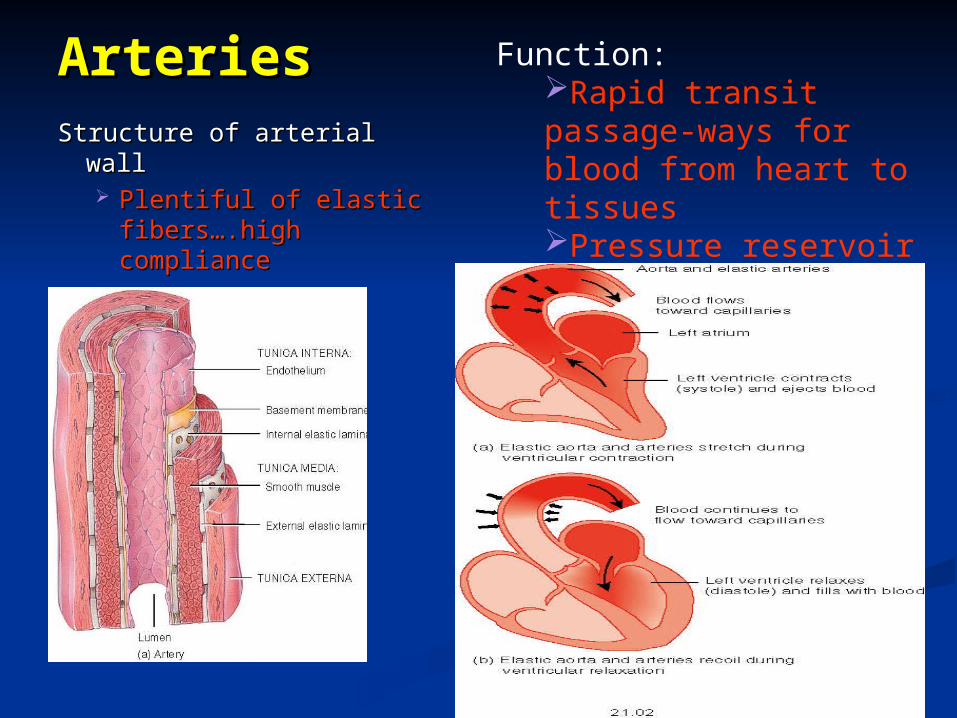
ArteriesArteries
Structure of arterial wallStructure of arterial wall Plentiful of elastic Plentiful of elastic
fibers….high fibers….high compliancecompliance
Function: Rapid transit passage-ways for blood from heart to tissuesPressure reservoir
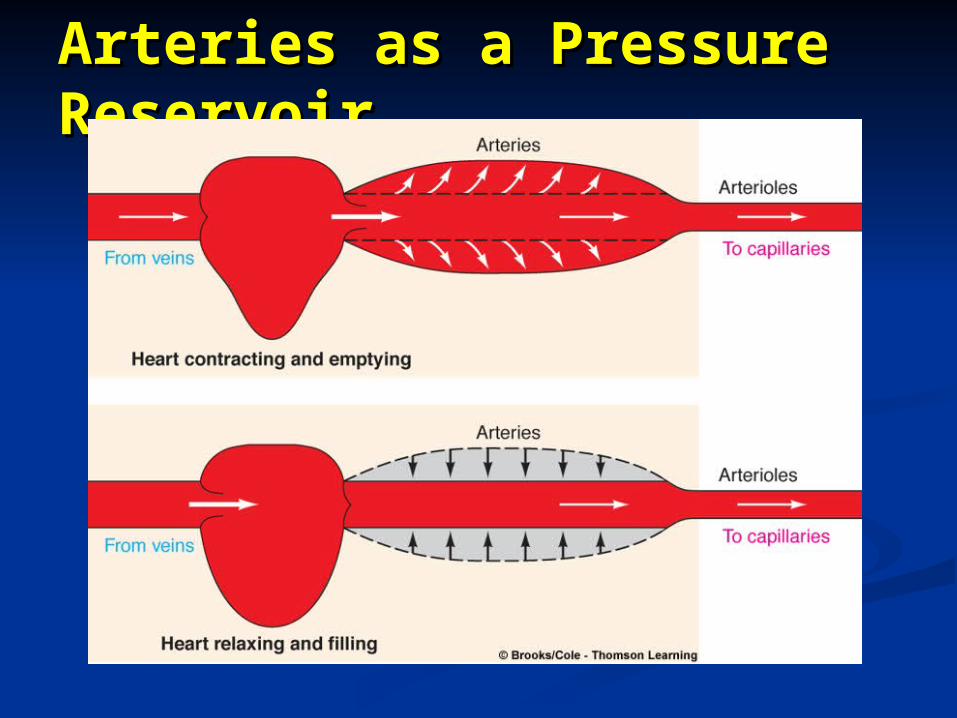
Arteries as a Pressure Arteries as a Pressure ReservoirReservoir
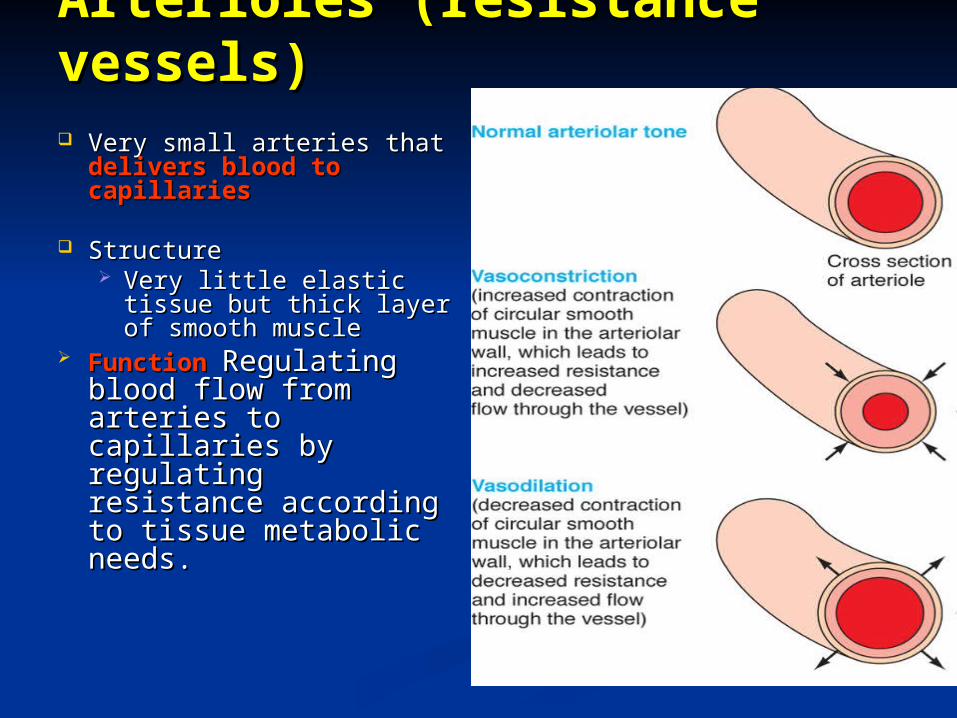
Arterioles (resistance vessels)Arterioles (resistance vessels) Very small arteries that Very small arteries that
delivers blood to delivers blood to capillariescapillaries
StructureStructure Very little elastic tissue Very little elastic tissue
but thick layer of smooth but thick layer of smooth musclemuscle
Function Function Regulating Regulating blood flow from arteries blood flow from arteries to capillaries by to capillaries by regulating resistance regulating resistance according to tissue according to tissue metabolic needs.metabolic needs.
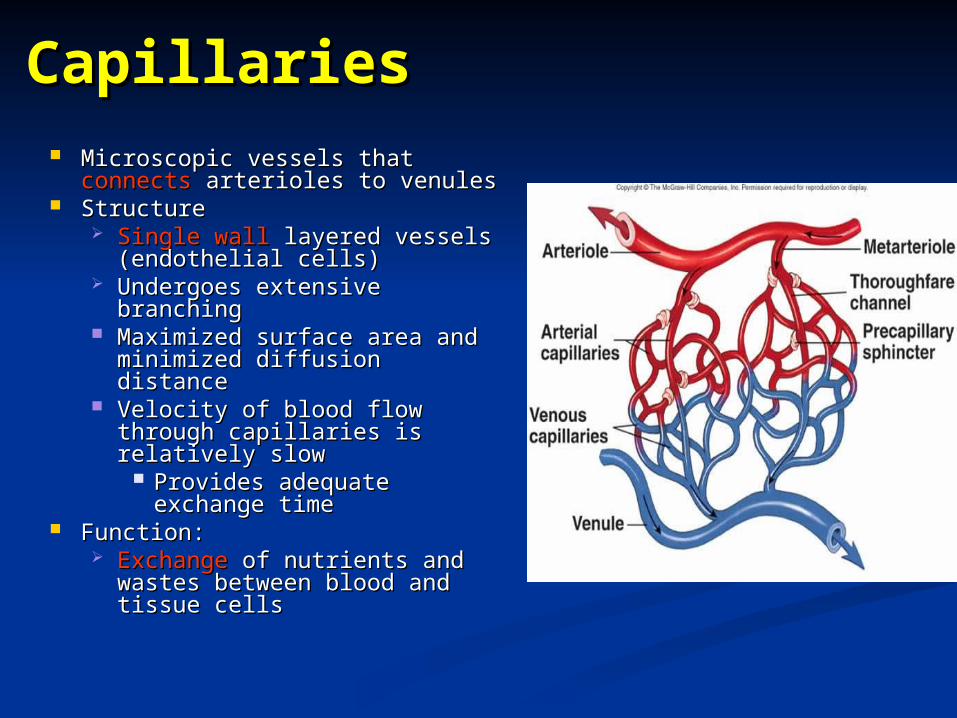
CapillariesCapillaries Microscopic vessels that Microscopic vessels that connectsconnects
arterioles to venulesarterioles to venules StructureStructure
Single wallSingle wall layered vessels layered vessels (endothelial cells)(endothelial cells)
Undergoes extensive branchingUndergoes extensive branching Maximized surface area and Maximized surface area and
minimized diffusion distanceminimized diffusion distance Velocity of blood flow through Velocity of blood flow through
capillaries is relatively slowcapillaries is relatively slow Provides adequate exchange Provides adequate exchange
timetime Function:Function:
Exchange Exchange of nutrients and wastes of nutrients and wastes between blood and tissue cellsbetween blood and tissue cells
Capillaries cont.Capillaries cont.
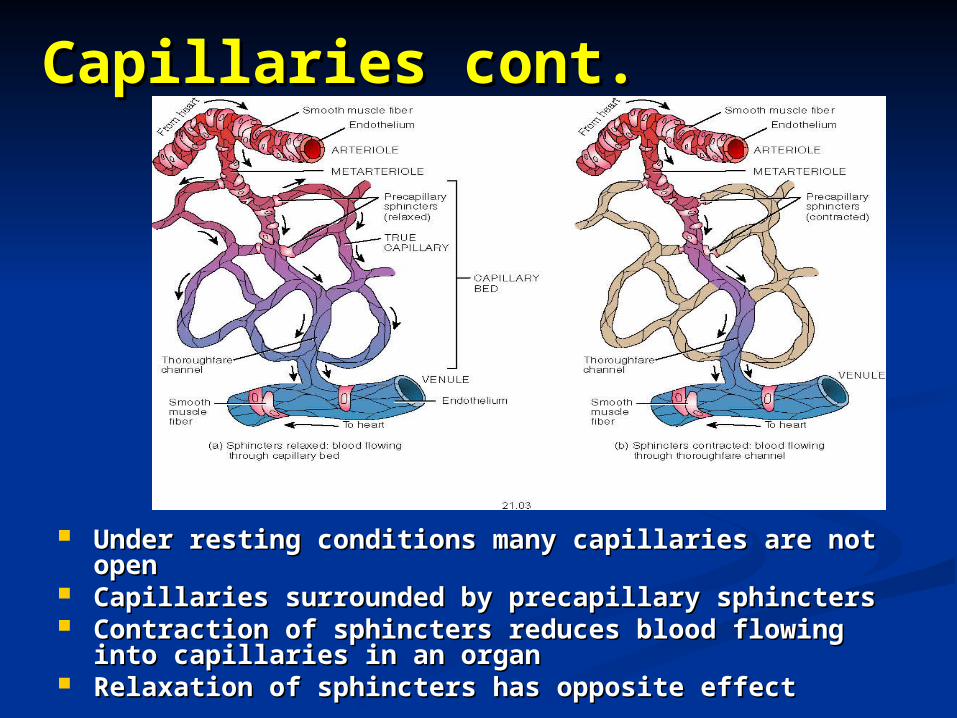
Under resting conditions many capillaries are not Under resting conditions many capillaries are not openopen
Capillaries surrounded by precapillary sphinctersCapillaries surrounded by precapillary sphincters Contraction of sphincters reduces blood flowing into Contraction of sphincters reduces blood flowing into
capillaries in an organcapillaries in an organ Relaxation of sphincters has opposite effectRelaxation of sphincters has opposite effect
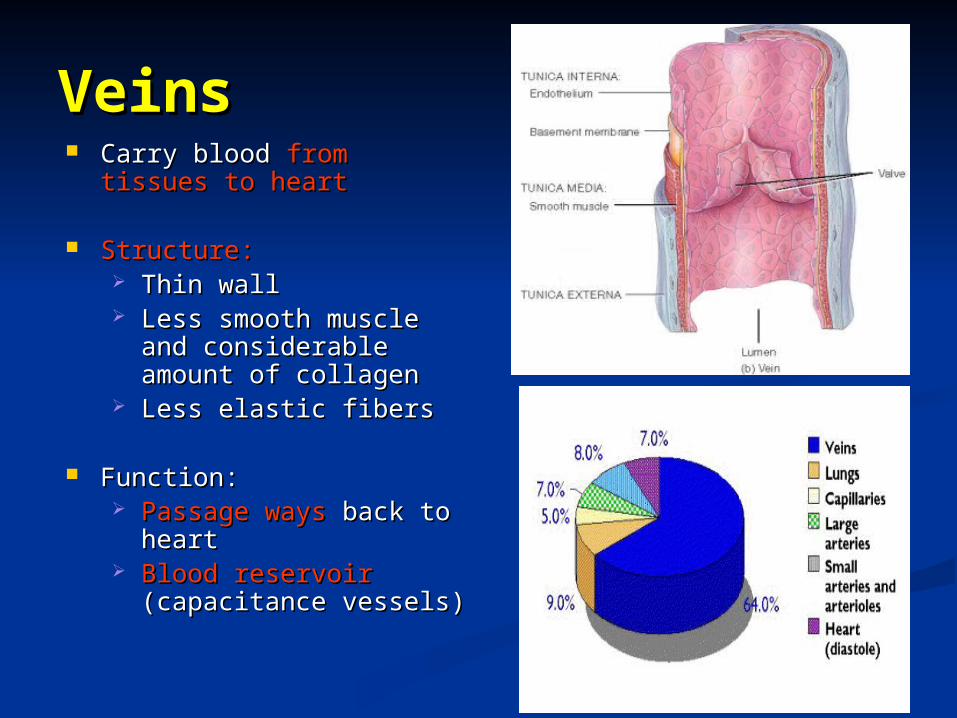
VeinsVeins Carry blood Carry blood from tissues to from tissues to
heartheart
Structure:Structure: Thin wallThin wall Less smooth muscle and Less smooth muscle and
considerable amount of considerable amount of collagencollagen
Less elastic fibersLess elastic fibers
Function:Function: Passage waysPassage ways back to back to
heartheart Blood reservoir Blood reservoir
(capacitance vessels)(capacitance vessels)
Properties of Properties of Cardiac Cardiac MuscleMuscle
22
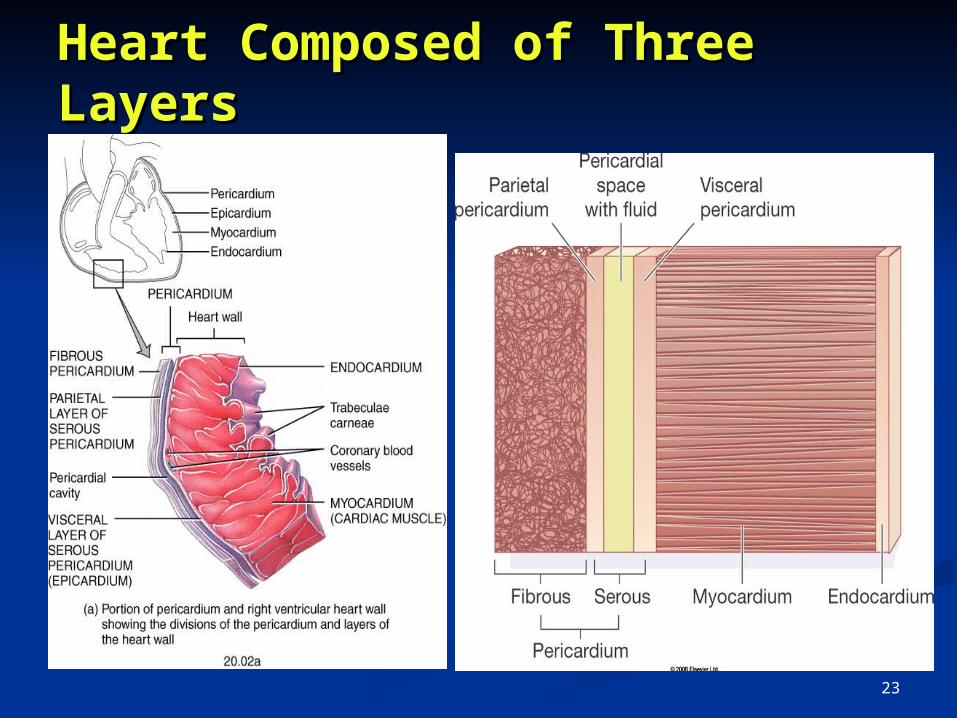
Heart Composed of Three Heart Composed of Three LayersLayers
23
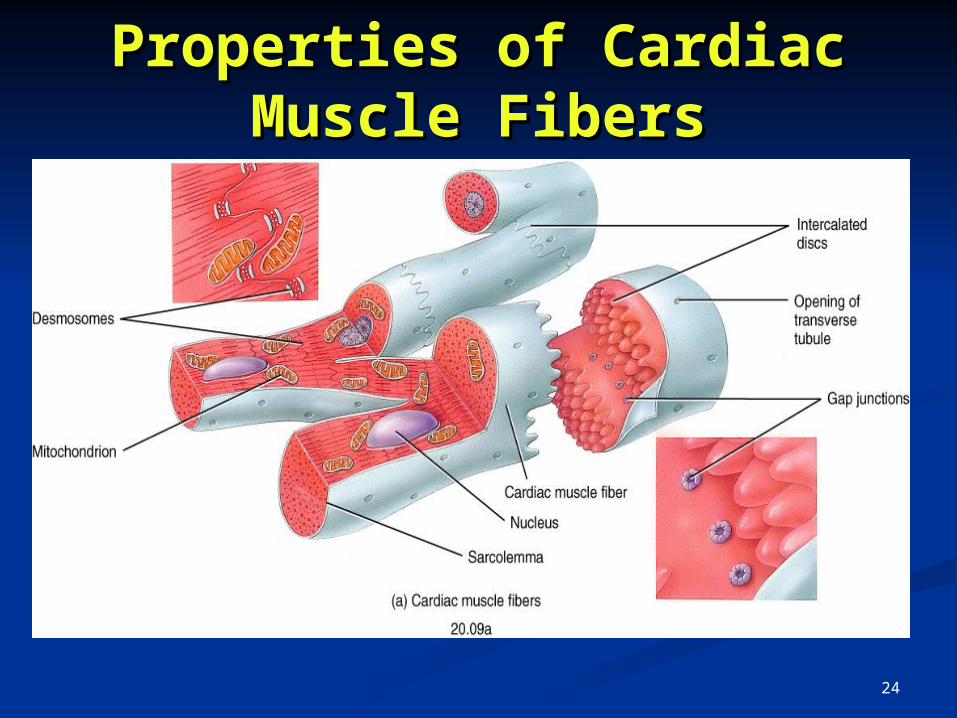
Properties of Cardiac Properties of Cardiac Muscle FibersMuscle Fibers
24
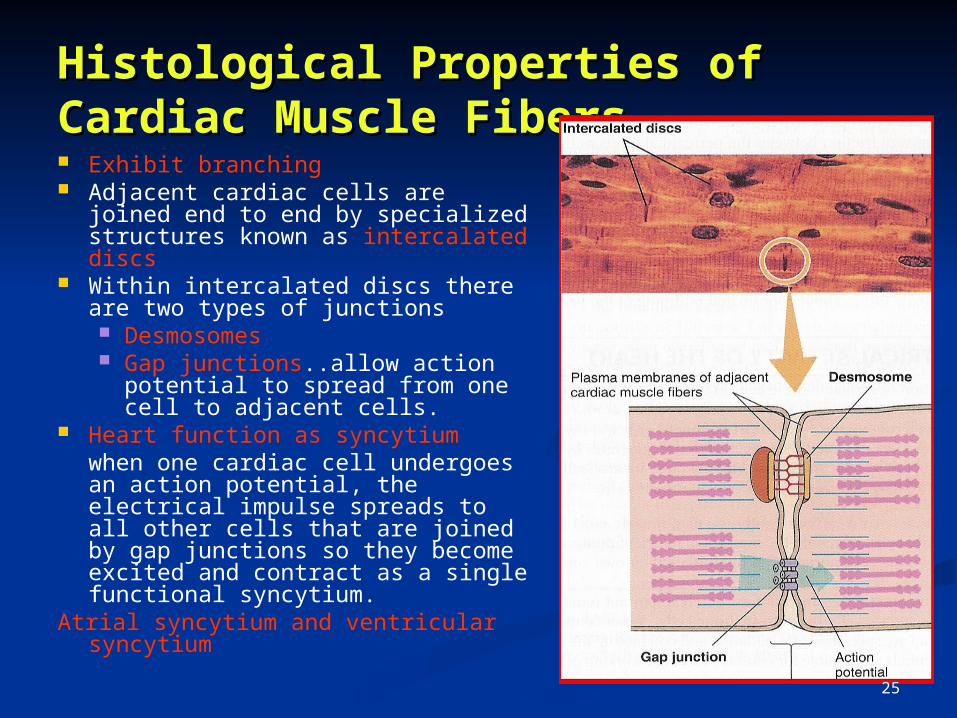
Exhibit branching Adjacent cardiac cells are joined end
to end by specialized structures known as intercalated discs
Within intercalated discs there are two types of junctions Desmosomes Gap junctions..allow action
potential to spread from one cell to adjacent cells.
Heart function as syncytiumwhen one cardiac cell undergoes an action potential, the electrical impulse spreads to all other cells that are joined by gap junctions so they become excited and contract as a single functional syncytium.
Atrial syncytium and ventricular syncytium
Histological Properties of Histological Properties of Cardiac Muscle FibersCardiac Muscle Fibers
25
THE CARDIAC MUSCLETHE CARDIAC MUSCLE
Contractile muscle fibres (myocardium 99%) Atrial muscle fibres & Ventricular muscle fibres
- Both contract same as in sk. Muscle - Duration of contraction much longer Excitatory & conductive muscle fibres (autorhythmic
1%) - Few contractile fibrils (v.weak contraction) - Exhibit either automatic rhythmic discharge(AP) OR Conduction of the AP through heart
26
Properties of Cardiac Muscle Properties of Cardiac Muscle FibersFibers1. Autorhythmicity: The ability to initiate a heart
beat continuously and regularly without external stimulation
2. Excitability: The ability to respond to a stimulus of adequate strength and duration (i.e. threshold or more) by generating a propagated action potential
3. Conductivity: The ability to conduct excitation through the cardiac tissue
4. Contractility: The ability to contract in response to stimulation
27
1. Autorhythmicity1. Autorhythmicity
myogenic myogenic (independent of nerve supply)(independent of nerve supply)
due to the due to the specialized excitatory & conductive systemspecialized excitatory & conductive system of the of the heartheart
intrinsic ability of self-excitationintrinsic ability of self-excitation (waves of depolarization)(waves of depolarization) cardiac impulsescardiac impulses
Definition: the ability of the heart to initiate its beat continuously and regularly without external stimulation
28
Have two important functions1. Act as a pacemaker (set the rhythm of electrical excitation)2. Form the conductive system (network of
specialized cardiac muscle fibers that provide a path for each cycle of cardiac excitation to progress through the heart)
Autorythmic fibersAutorythmic fibers
Forms 1% of the cardiac muscle fibers
29
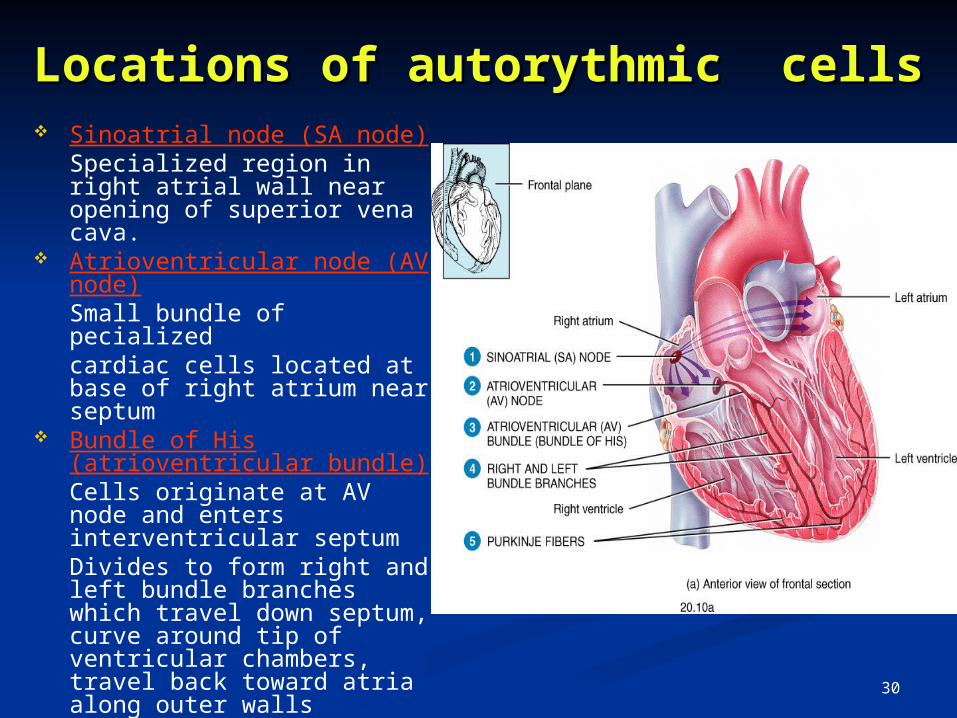
Sinoatrial node (SA node)Specialized region in right atrial wall near opening of superior vena cava.
Atrioventricular node (AV node)Small bundle of pecializedcardiac cells located at base of right atrium near septum
Bundle of His (atrioventricular bundle)Cells originate at AV node and enters interventricular septumDivides to form right and left bundle branches which travel down septum, curve around tip of ventricular chambers, travel back toward atria along outer walls
Purkinje fibersSmall, terminal fibers that extend from bundle of His and spread throughout ventricular myocardium
Locations of autorythmic cellsLocations of autorythmic cells
30
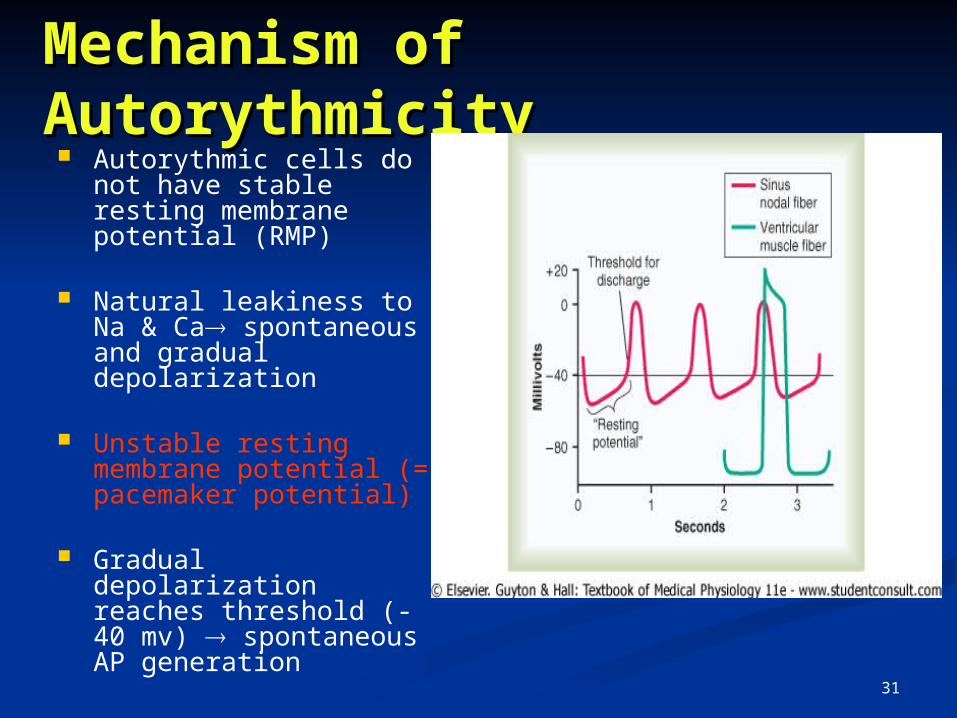
Mechanism of Mechanism of AutorythmicityAutorythmicity Autorythmic cells do not
have stable resting membrane potential (RMP)
Natural leakiness to Na & Ca spontaneous and gradual depolarization
Unstable resting membrane potential (= pacemaker potential)
Gradual depolarization reaches threshold (-40 mv) spontaneous AP generation
31
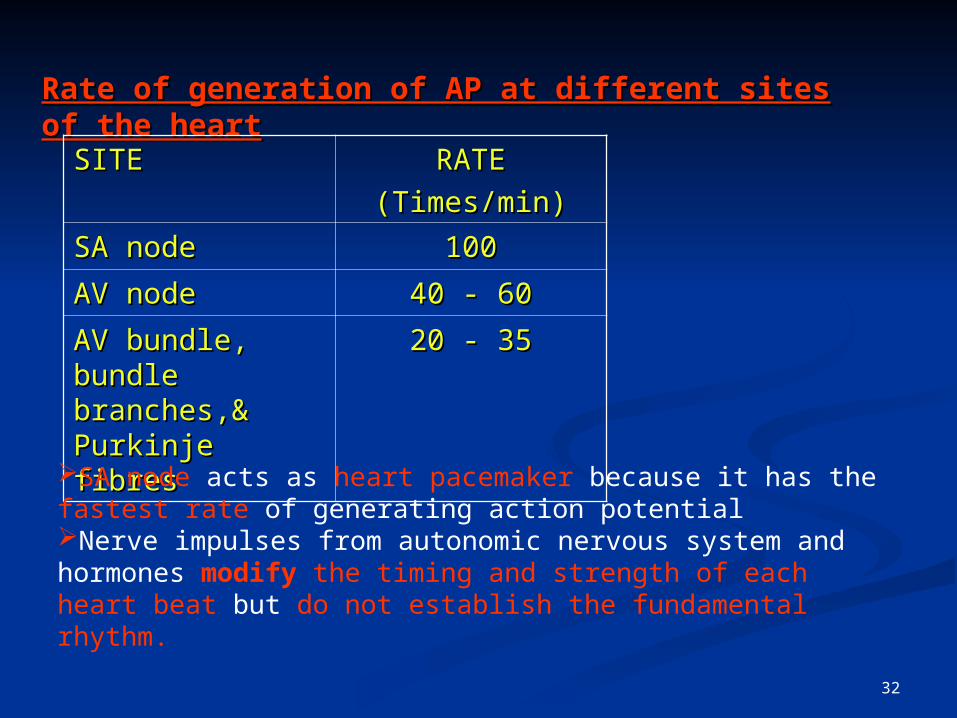
Rate of generation of AP at different sites of the heartRate of generation of AP at different sites of the heart
SITESITE RATERATE
(Times/min)(Times/min)
SA nodeSA node 100100
AV nodeAV node 40 - 6040 - 60
AV bundle, bundle AV bundle, bundle branches,& Purkinje branches,& Purkinje fibresfibres
20 - 3520 - 35
SA node acts as heart pacemaker because it has the fastest rate of generating action potentialNerve impulses from autonomic nervous system and hormones modify the timing and strength of each heart beat but do not establish the fundamental rhythm.
32
2. Excitability2. Excitability
Definition: The ability of cardiac muscle to respond to a stimulus of adequate strength & duration by generating an AP
AP initiated by SA nodetravels along conductive
pathway excites atrial & ventricular muscle fibres
34
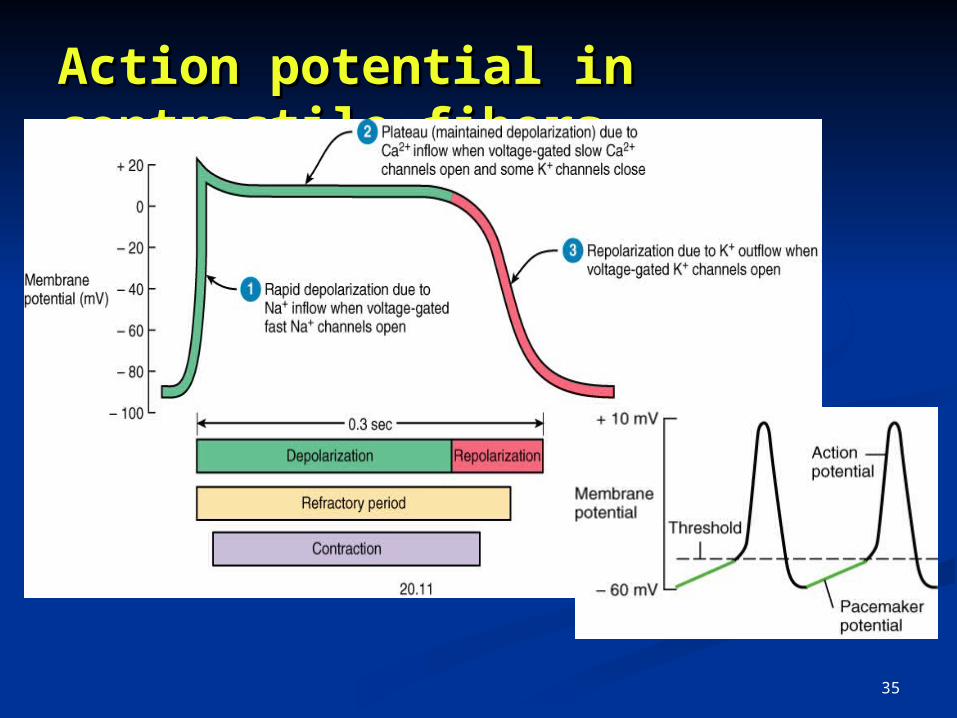
Action potential in Action potential in contractile fiberscontractile fibers
35
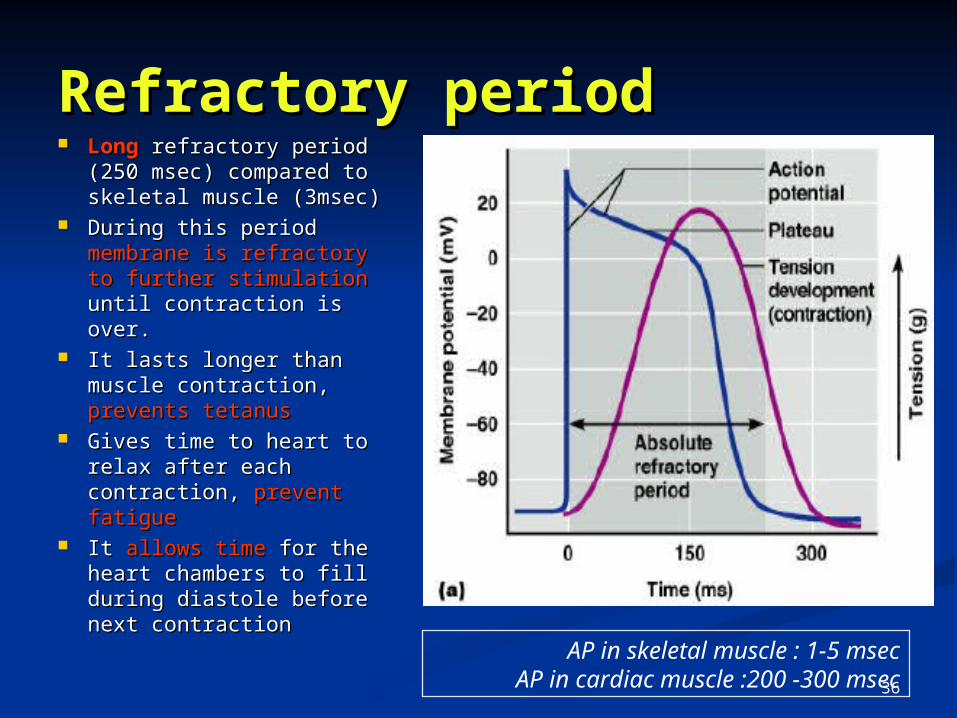
Refractory periodRefractory period LongLong refractory period (250 refractory period (250
msec) compared to skeletal msec) compared to skeletal muscle (3msec)muscle (3msec)
During this period During this period membrane membrane is refractory to further is refractory to further stimulationstimulation until contraction until contraction is over.is over.
It lasts longer than muscle It lasts longer than muscle contraction, contraction, prevents tetanusprevents tetanus
Gives time to heart to relax Gives time to heart to relax after each contraction, after each contraction, prevent fatigueprevent fatigue
It It allows timeallows time for the heart for the heart chambers to fill during chambers to fill during diastole before next diastole before next contractioncontraction
AP in skeletal muscle : 1-5 msecAP in cardiac muscle :200 -300 msec36
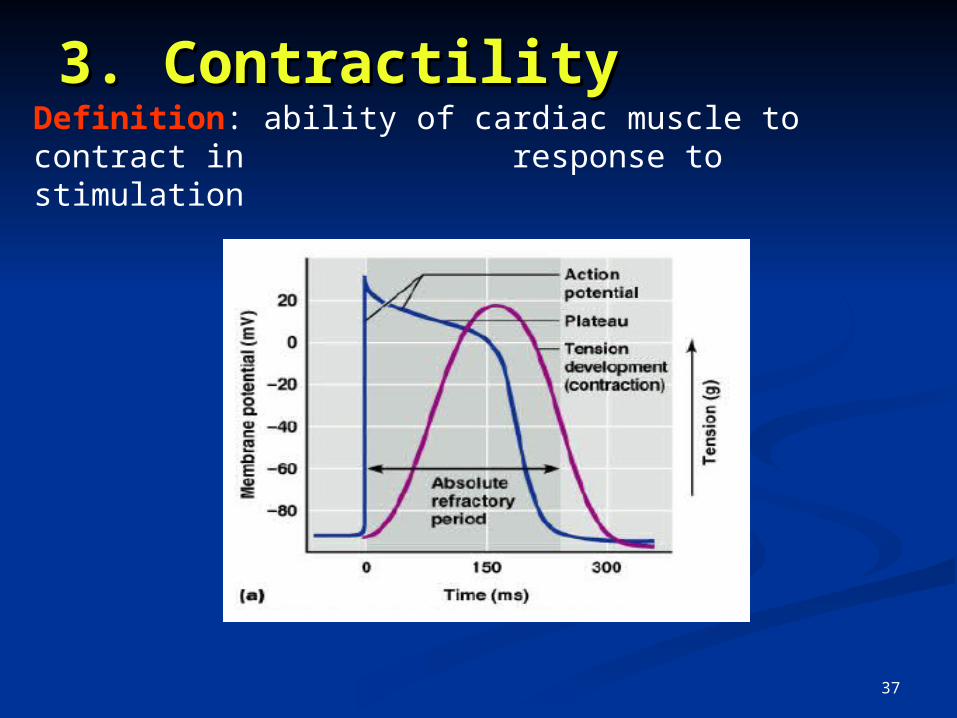
3. Contractility3. ContractilityDefinition: ability of cardiac muscle to contract in
response to stimulation
37
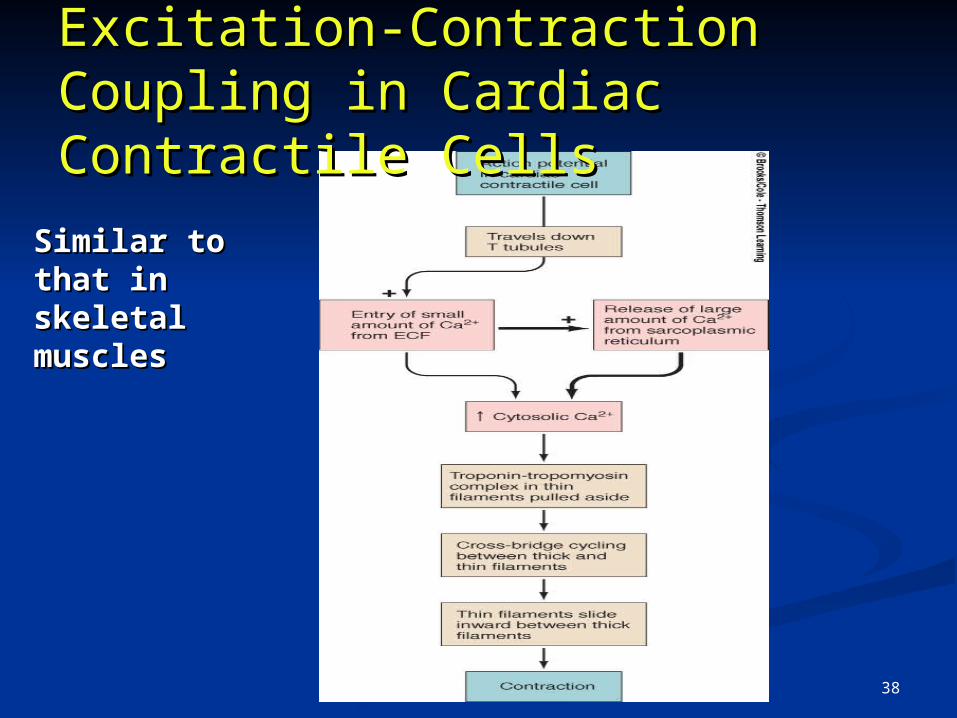
Excitation-Contraction Excitation-Contraction Coupling in Cardiac Coupling in Cardiac Contractile CellsContractile Cells
Similar to that in Similar to that in skeletal musclesskeletal muscles
38
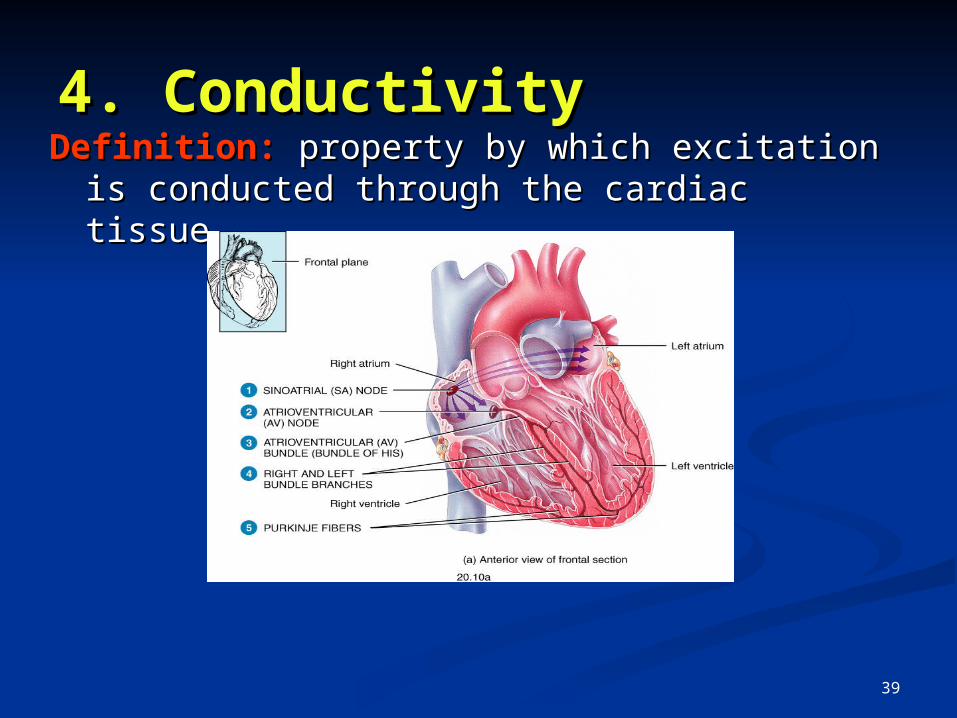
4. Conductivity4. ConductivityDefinition:Definition: property by which excitation is conducted property by which excitation is conducted
through the cardiac tissuethrough the cardiac tissue
39
Criteria for spread of excitation & Criteria for spread of excitation & efficient cardiac functionefficient cardiac function
1. Atrial excitation and contraction should be complete before onset of ventricular contraction
- ensures complete filling of the ventricles during diastole
2. Excitation of cardiac muscle fibres should be coordinated ensure each heart chamber contracts as a unit accomplish efficient pumping
- smooth uniform contraction essential to squeeze out blood
3. Pair of atria & pair of ventricles should be functionally co-ordinated both members contract simultaneously
- permits synchronized pumping of blood into pulmonary & systemic circulation
40
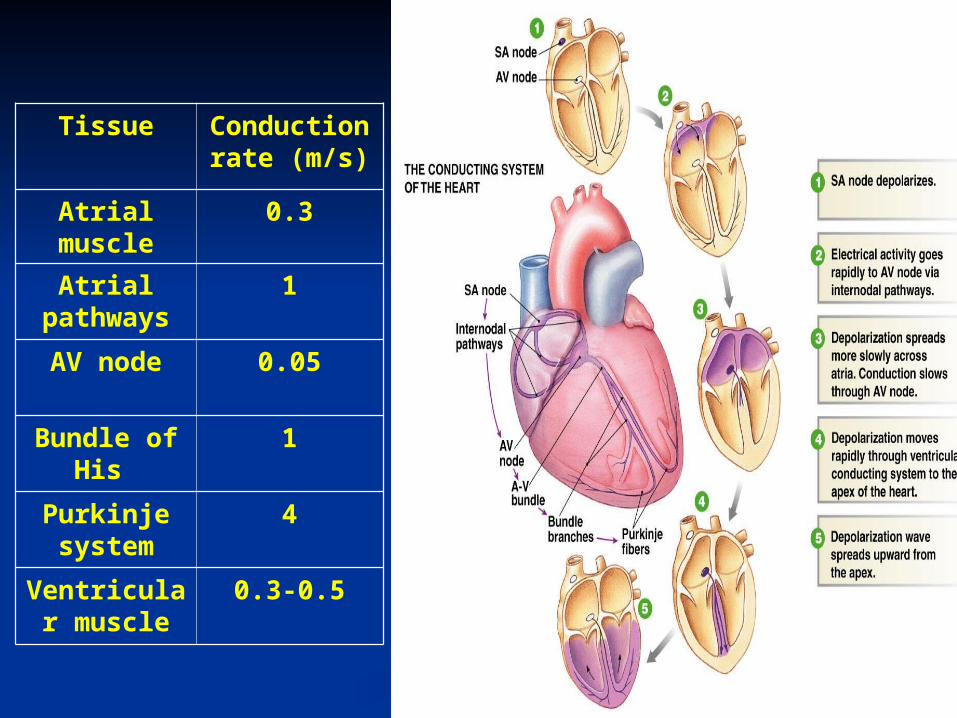
Tissue Conduction rate (m/s)
Atrial muscle
0.3
Atrial pathways
1
AV node 0.05
Bundle of His
1
Purkinje system
4
Ventricular muscle
0.3-0.5
41
Cardiac impulse originates at SA nodeCardiac impulse originates at SA node Action potential spreads throughout right and left atriaAction potential spreads throughout right and left atria Impulse passes from atria into ventricles through AV Impulse passes from atria into ventricles through AV
node (only point of electrical contact between chambers)node (only point of electrical contact between chambers) Action potential briefly delayed at AV node (ensures Action potential briefly delayed at AV node (ensures
atrial contraction precedes ventricular contraction to atrial contraction precedes ventricular contraction to allow complete ventricular filling)allow complete ventricular filling)
Impulse travels rapidly down interventricular septum by Impulse travels rapidly down interventricular septum by means of bundle of Hismeans of bundle of His
Impulse rapidly disperses throughout myocardium by Impulse rapidly disperses throughout myocardium by means of Purkinje fibersmeans of Purkinje fibers
Rest of ventricular cells activated by cell-to-cell spread of Rest of ventricular cells activated by cell-to-cell spread of impulse through gap junctionsimpulse through gap junctions
Spread of Cardiac ExcitationSpread of Cardiac Excitation
42
Normal conduction pathway:
SA node -> atrial muscle -> AV node -> bundle of His -> Left and Right Bundle Branches -> Ventricular muscle
Electrocardiography
• A recording of the electrical activity of the heart over time
• Gold standard for diagnosis of cardiac arrhythmias
• Helps detect electrolyte disturbances (hyper- & hypokalemia)
• Allows for detection of conduction abnormalities
• Screening tool for ischemic heart disease during stress tests
• Helpful with non-cardiac diseases (e.g. pulmonary embolism or hypothermia
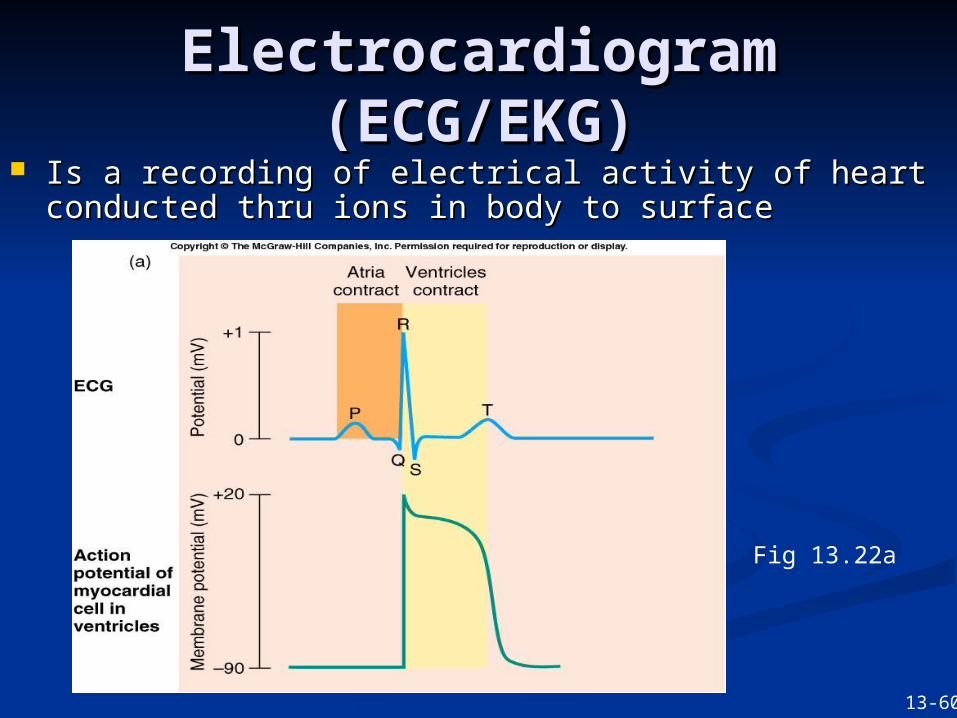
Electrocardiogram Electrocardiogram (ECG/EKG)(ECG/EKG)
Is a recording of electrical activity of heart conducted Is a recording of electrical activity of heart conducted thru ions in body to surfacethru ions in body to surface
Fig 13.22a
13-60
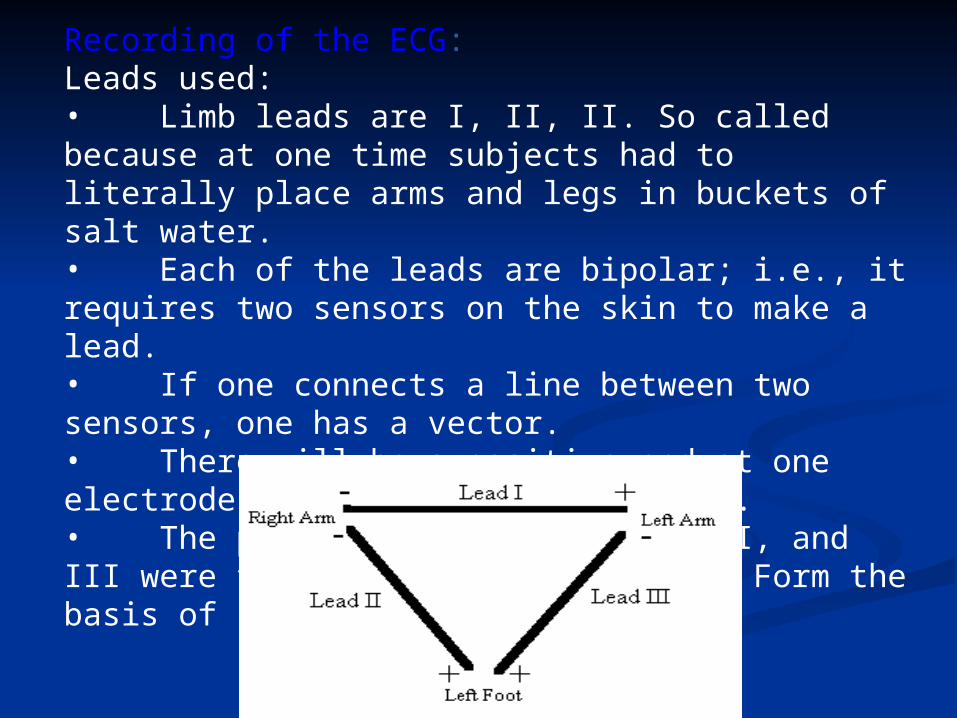
Recording of the ECG:Leads used:• Limb leads are I, II, II. So called because at one time subjects had to literally place arms and legs in buckets of salt water.• Each of the leads are bipolar; i.e., it requires two sensors on the skin to make a lead.• If one connects a line between two sensors, one has a vector.• There will be a positive end at one electrode and negative at the other.• The positioning for leads I, II, and III were first given by Einthoven. Form the basis of Einthoven’s triangle.
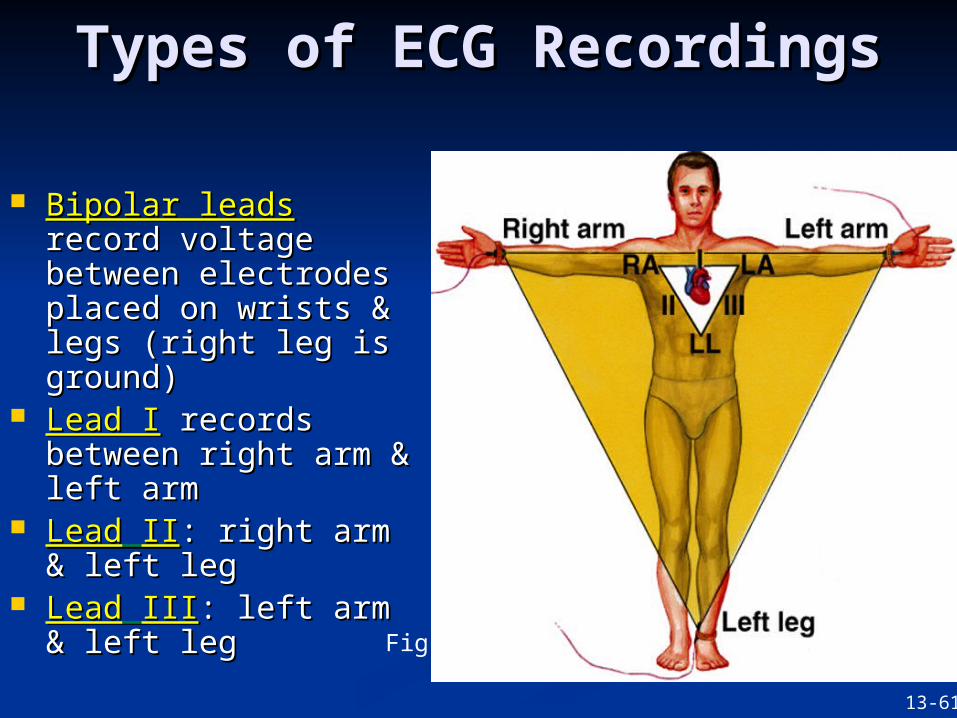
Types of ECG RecordingsTypes of ECG Recordings
Bipolar leadsBipolar leads record record voltage between voltage between electrodes placed on electrodes placed on wrists & legs (right leg wrists & legs (right leg is ground)is ground)
Lead ILead I records records between right arm & between right arm & left armleft arm
LeadLead IIII: right arm & : right arm & left legleft leg
LeadLead IIIIII: left arm & : left arm & left legleft leg
Fig 13.23
13-61
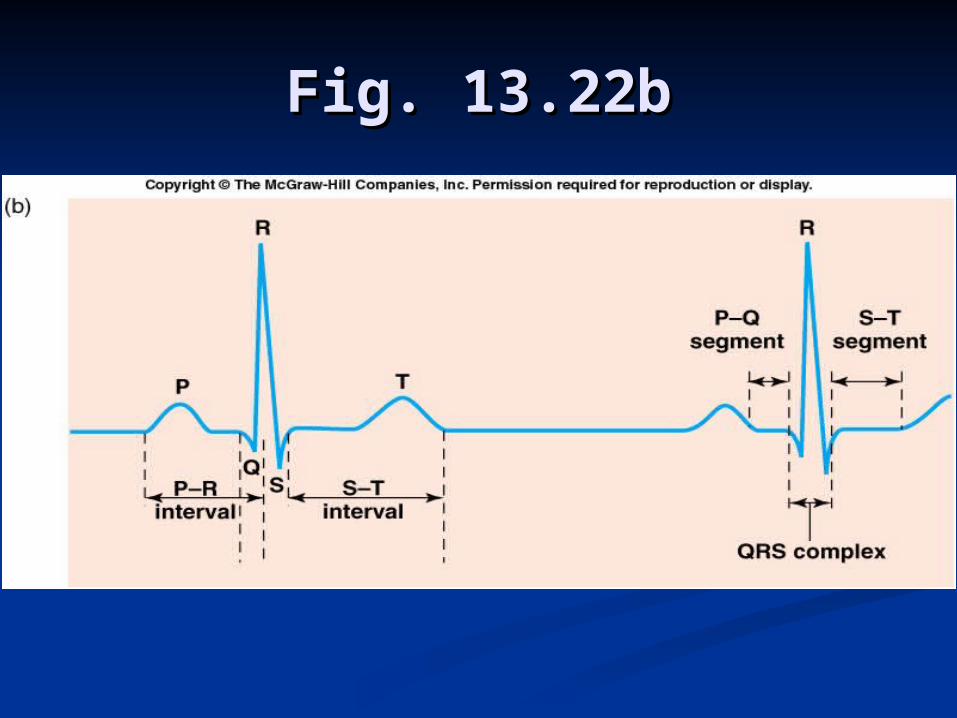
Fig. 13.22bFig. 13.22b
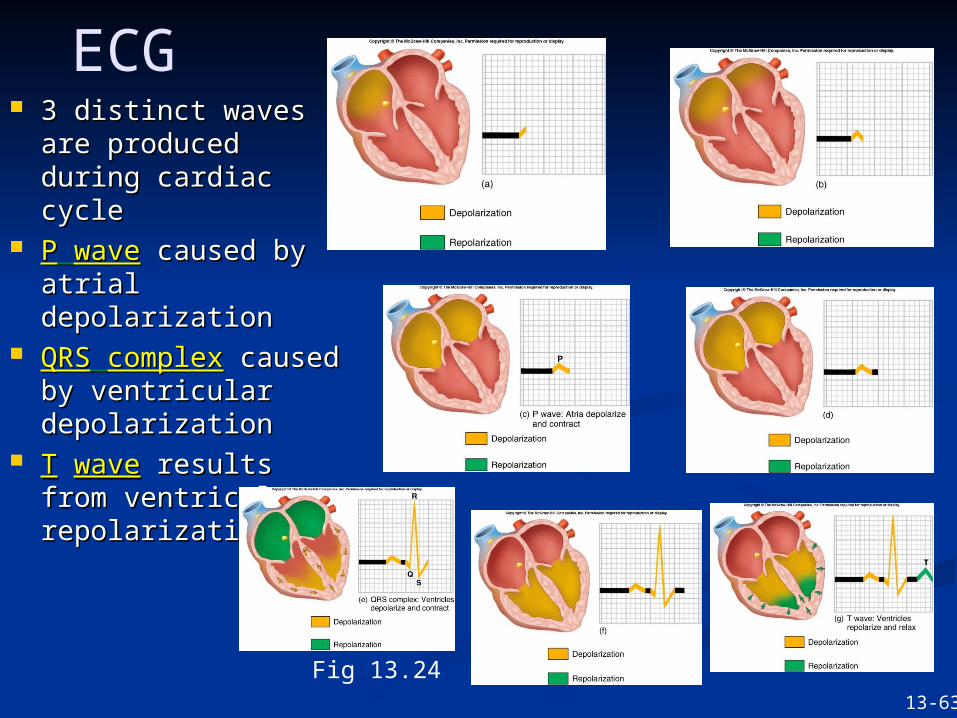
3 distinct waves are 3 distinct waves are produced during produced during cardiac cyclecardiac cycle
PP wavewave caused by caused by atrial atrial depolarizationdepolarization
QRSQRS complexcomplex caused by caused by ventricular ventricular depolarizationdepolarization
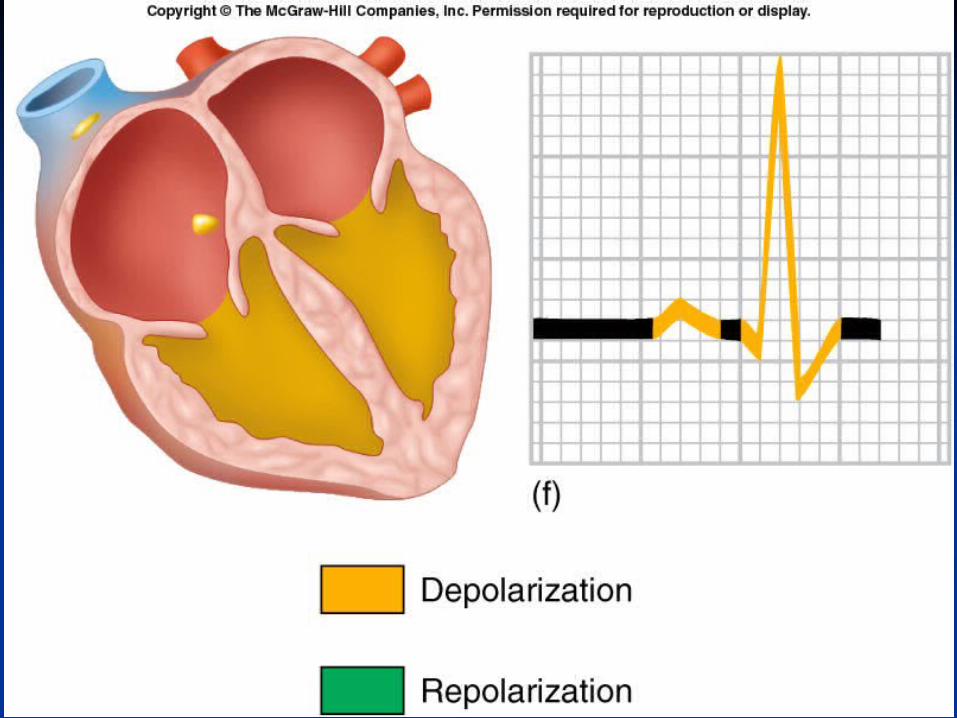
TT wavewave results from results from ventricular ventricular repolarizationrepolarization
ECG
Fig 13.2413-63
Elements of the ECG
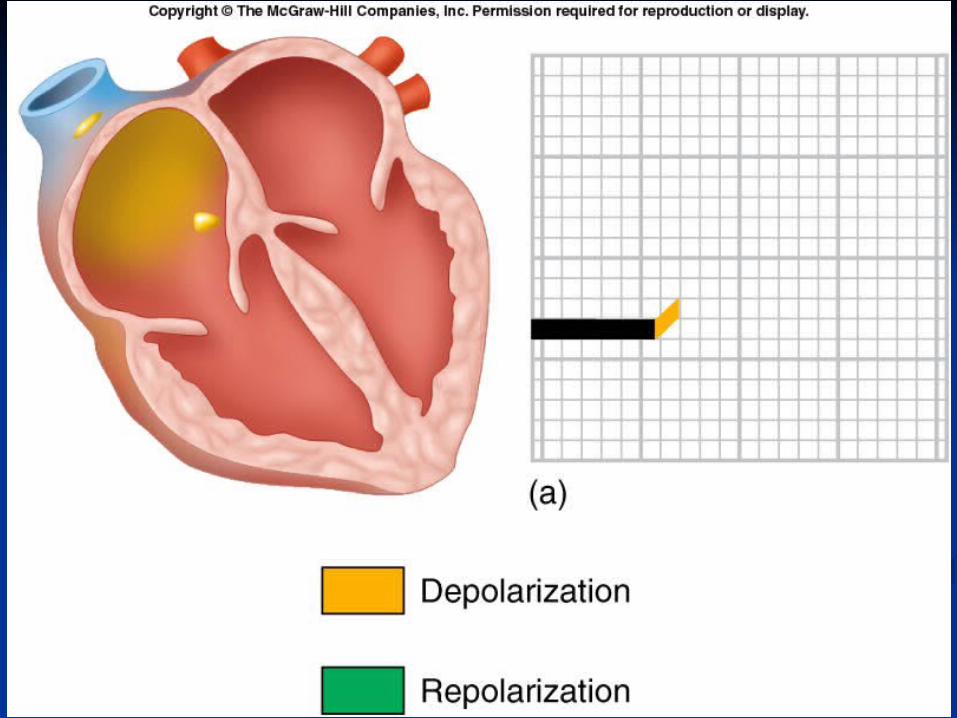
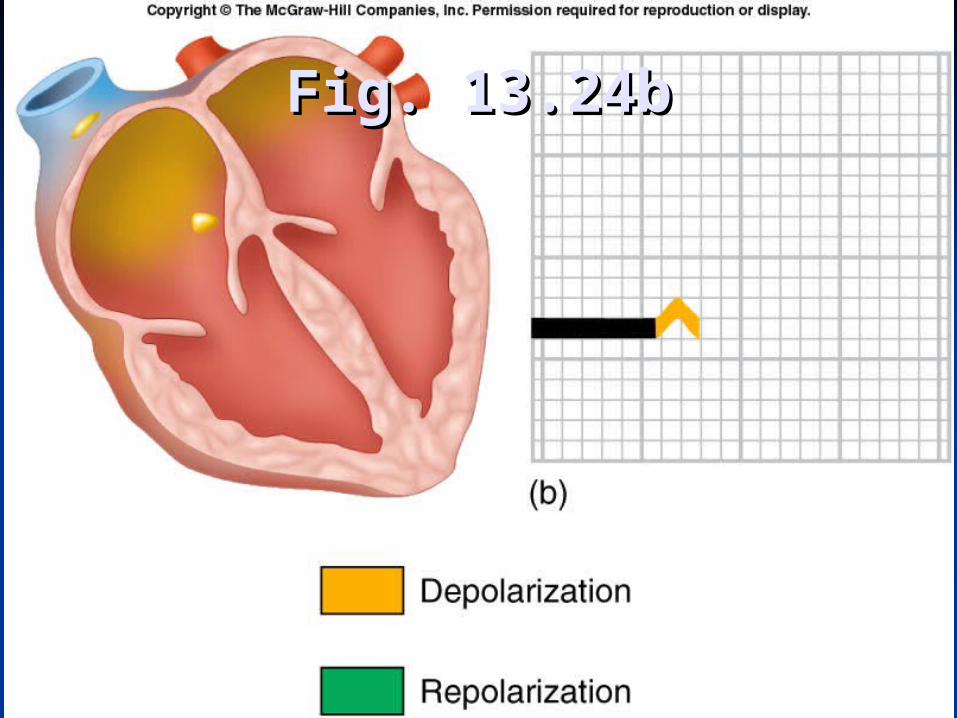
Fig. 13.24bFig. 13.24b
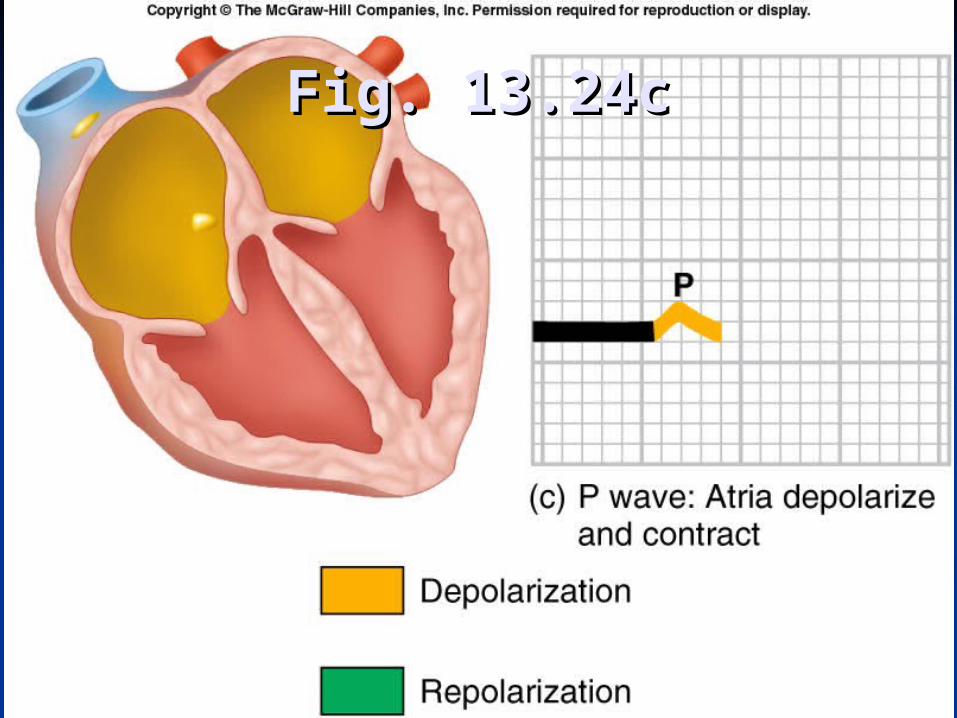
Fig. 13.24cFig. 13.24c
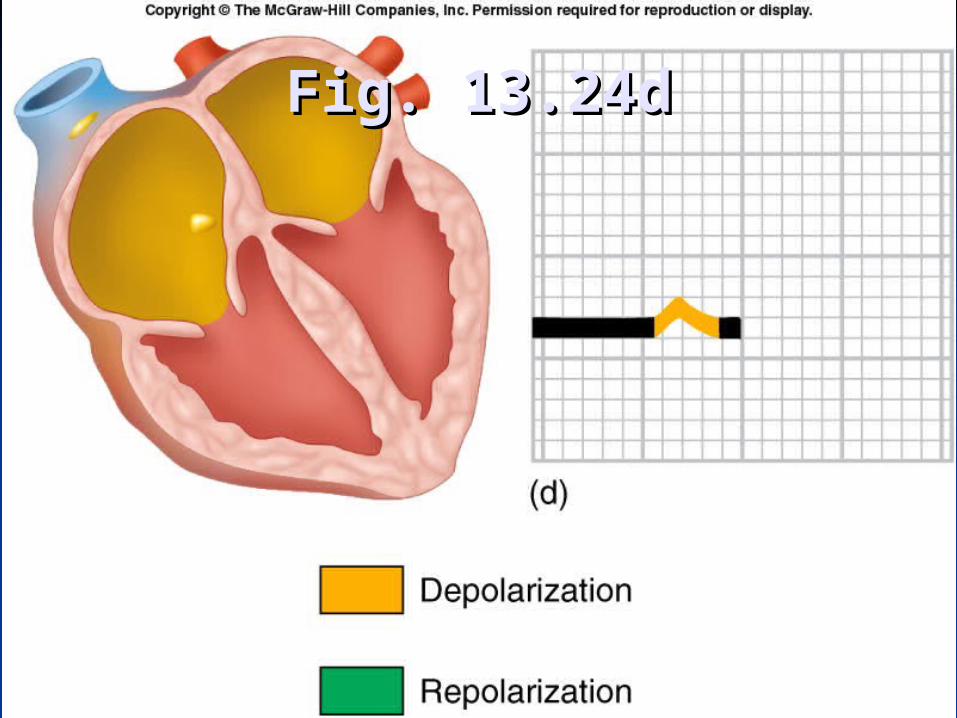
Fig. 13.24dFig. 13.24d
Elements of the ECG:
• P wave• Depolarization of both atria;• Relationship between P and QRS helps distinguish various cardiac arrhythmias• Shape and duration of P may indicate atrial enlargement
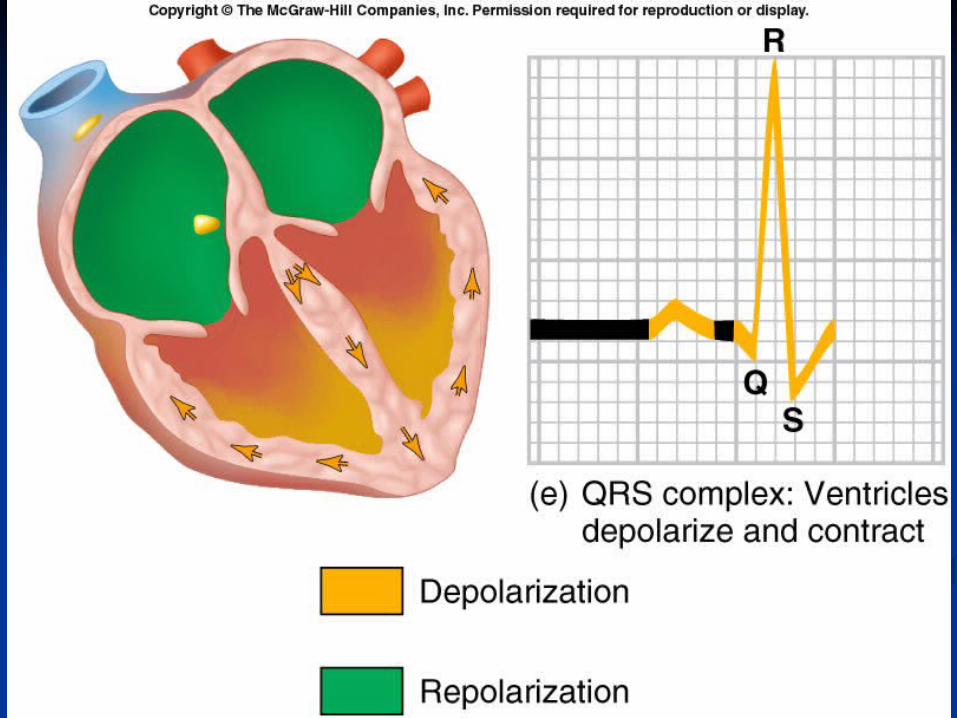
•QRS complex: • Represents ventricular depolarization
• Larger than P wave because of greater muscle mass of ventricles
• Normal duration = 0.08-0.12 seconds
• Its duration, amplitude, and morphology are useful in diagnosing cardiac arrhythmias, ventricular hypertrophy, MI, electrolyte derangement, etc.
• Q wave greater than 1/3 the height of the R wave, greater than 0.04 sec are abnormal and may represent MI
• PR interval: • From onset of P wave to onset of QRS
• Normal duration = 0.12-2.0 sec (120-200 ms) (3-4 horizontal boxes)
• Represents atria to ventricular conduction time (through His bundle)
• Prolonged PR interval may indicate a 1st degree heart block
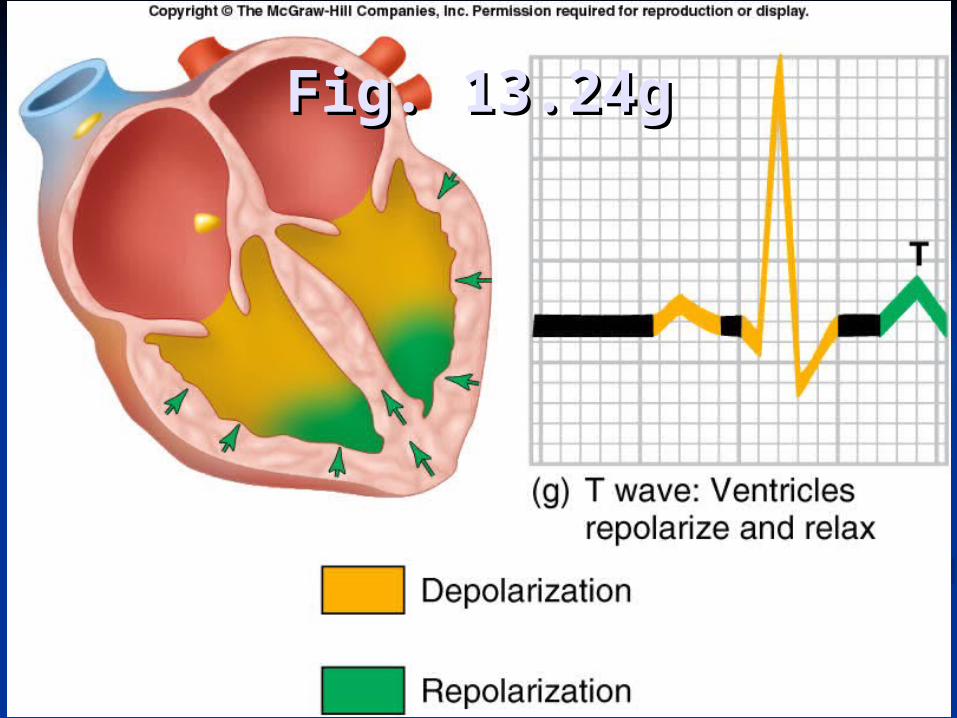
Fig. 13.24gFig. 13.24g
T wave: • Represents repolarization or recovery of ventricles• Interval from beginning of QRS to apex of T is referred to as the absolute refractory period
ST segment:• Connects the QRS complex and T wave• Duration of 0.08-0.12 sec (80-120 msec
QT Interval• Measured from beginning of QRS to the end of the T wave• Normal QT is usually about 0.40 sec• QT interval varies based on heart rate
Ischemic Heart DiseaseIschemic Heart Disease
Is most commonly due to atherosclerosis Is most commonly due to atherosclerosis in coronary arteriesin coronary arteries
IschemiaIschemia occurs when blood supply to occurs when blood supply to tissue is deficienttissue is deficient Causes increased lactic acid from anaerobic Causes increased lactic acid from anaerobic
metabolismmetabolism Often accompanied by Often accompanied by angina pectoris angina pectoris
(chest pain)(chest pain)
13-78
Ischemic Heart DiseaseIschemic Heart Disease
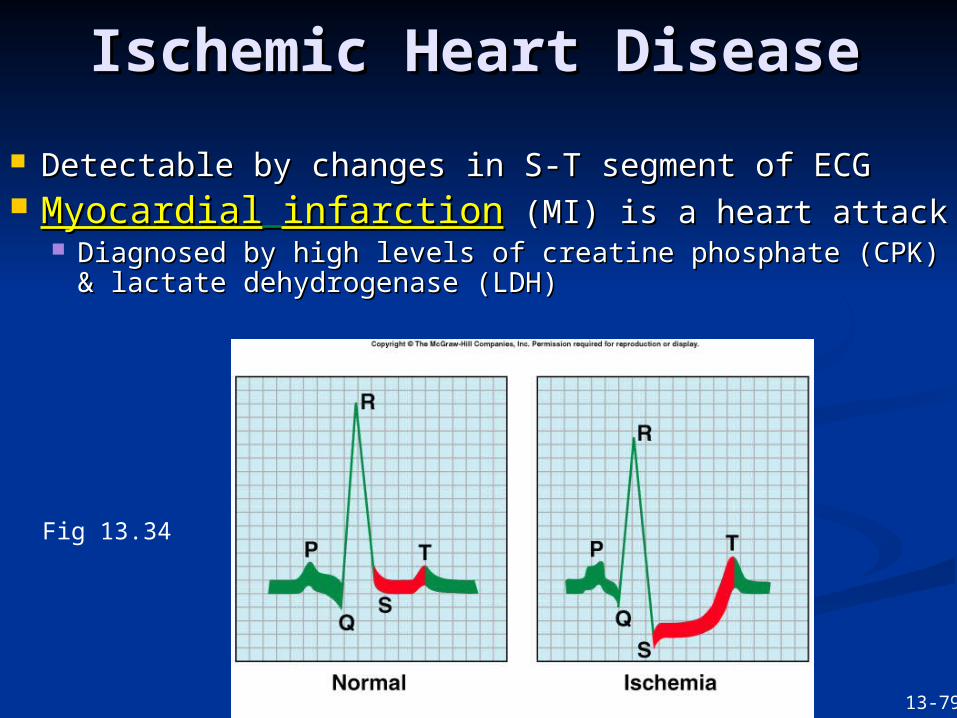
Detectable by changes in S-T segment of ECG Detectable by changes in S-T segment of ECG MyocardialMyocardial infarctioninfarction (MI) is a heart attack (MI) is a heart attack
Diagnosed by high levels of creatine phosphate Diagnosed by high levels of creatine phosphate (CPK) & lactate dehydrogenase (LDH)(CPK) & lactate dehydrogenase (LDH)
Fig 13.34
13-79
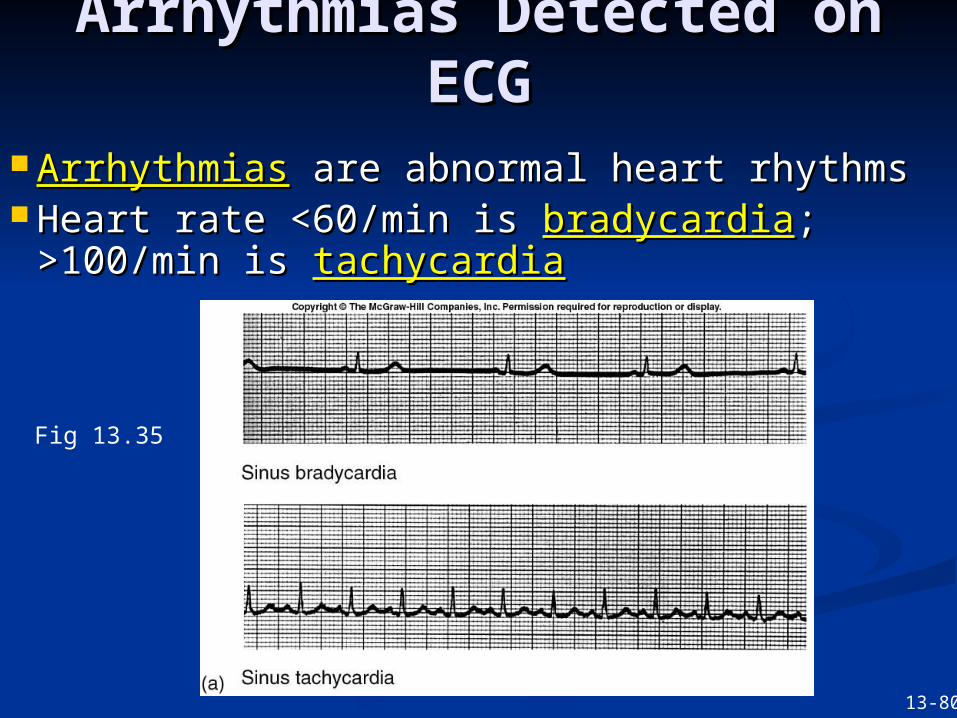
Arrhythmias Detected on Arrhythmias Detected on ECGECG
ArrhythmiasArrhythmias are abnormal heart rhythms are abnormal heart rhythms Heart rate <60/min is Heart rate <60/min is bradycardiabradycardia; ;
>100/min is >100/min is tachycardiatachycardia
Fig 13.35
13-80
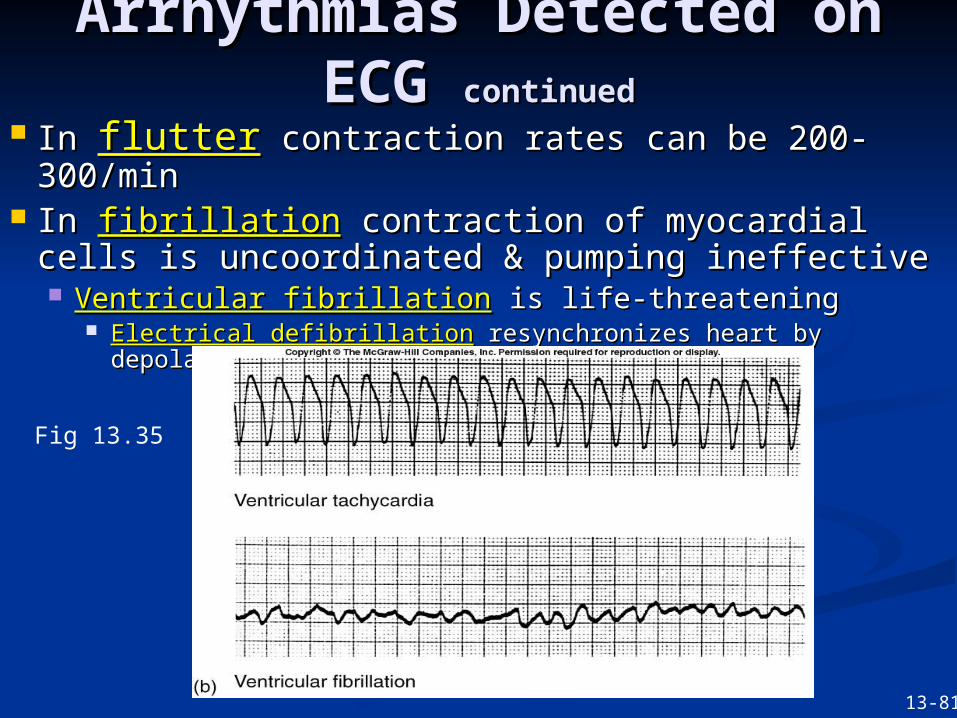
Arrhythmias Detected on Arrhythmias Detected on ECG ECG continuedcontinued
In In flutterflutter contraction rates can be 200-300/min contraction rates can be 200-300/min In In fibrillationfibrillation contraction of myocardial cells is contraction of myocardial cells is
uncoordinated & pumping ineffectiveuncoordinated & pumping ineffective Ventricular fibrillationVentricular fibrillation is life-threateningis life-threatening
Electrical defibrillationElectrical defibrillation resynchronizes heart by depolarizing resynchronizes heart by depolarizing all cells at same time all cells at same time
Fig 13.35
13-81
AV node blockAV node block occur when node is damagedoccur when node is damaged First–degree AV node blockFirst–degree AV node block is when conduction is when conduction
through AV node > 0.2 secthrough AV node > 0.2 sec Causes long P-R intervalCauses long P-R interval
Second-degree AV node blockSecond-degree AV node block is when only 1 out of 2-4 is when only 1 out of 2-4 atrial APs can pass to ventriclesatrial APs can pass to ventricles Causes P waves with no QRSCauses P waves with no QRS
In In third-degree or complete AV node blockthird-degree or complete AV node block no atrial no atrial activity passes to ventriclesactivity passes to ventricles Ventricles driven slowly by bundle of His or PurkinjesVentricles driven slowly by bundle of His or Purkinjes
Arrhythmias Detected on Arrhythmias Detected on ECG ECG continuedcontinued
13-82
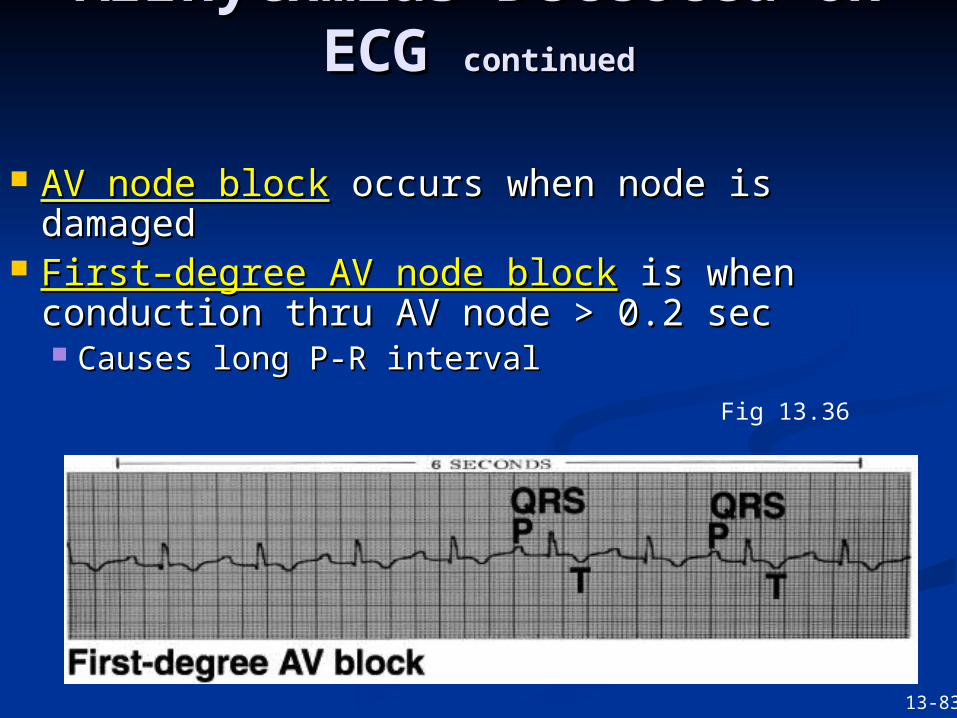
AV node blockAV node block occurs when node is damagedoccurs when node is damaged First–degree AV node blockFirst–degree AV node block is when is when
conduction thru AV node > 0.2 secconduction thru AV node > 0.2 sec Causes long P-R intervalCauses long P-R interval
Arrhythmias Detected on Arrhythmias Detected on ECG ECG continuedcontinued
Fig 13.36
13-83
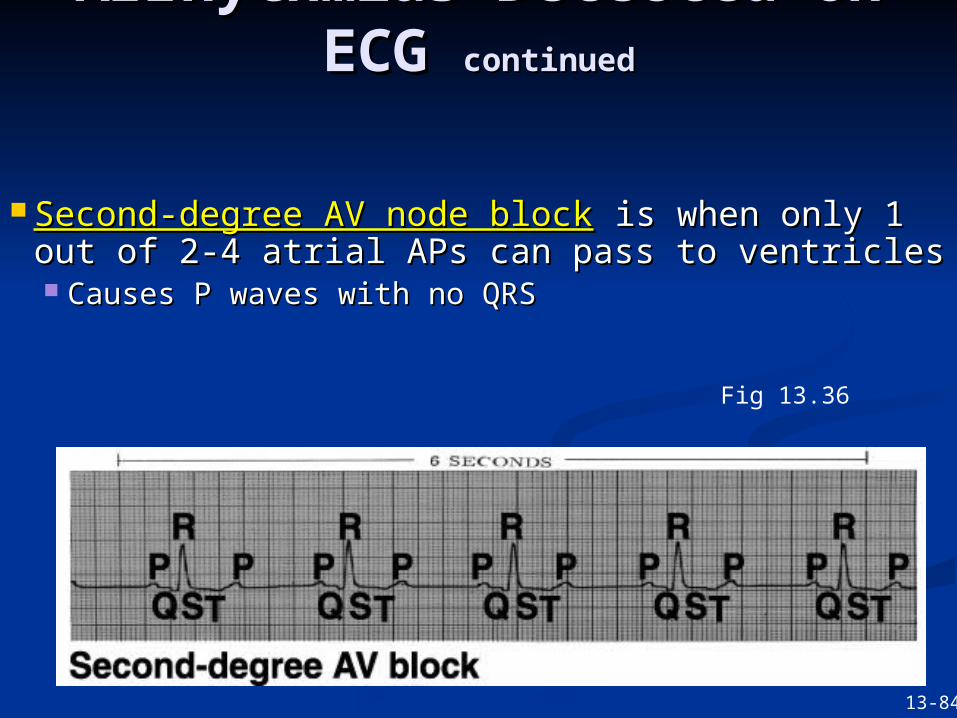
Second-degree AV node blockSecond-degree AV node block is when only 1 is when only 1 out of 2-4 atrial APs can pass to ventriclesout of 2-4 atrial APs can pass to ventricles Causes P waves with no QRSCauses P waves with no QRS
Arrhythmias Detected on Arrhythmias Detected on ECG ECG continuedcontinued
Fig 13.36
13-84
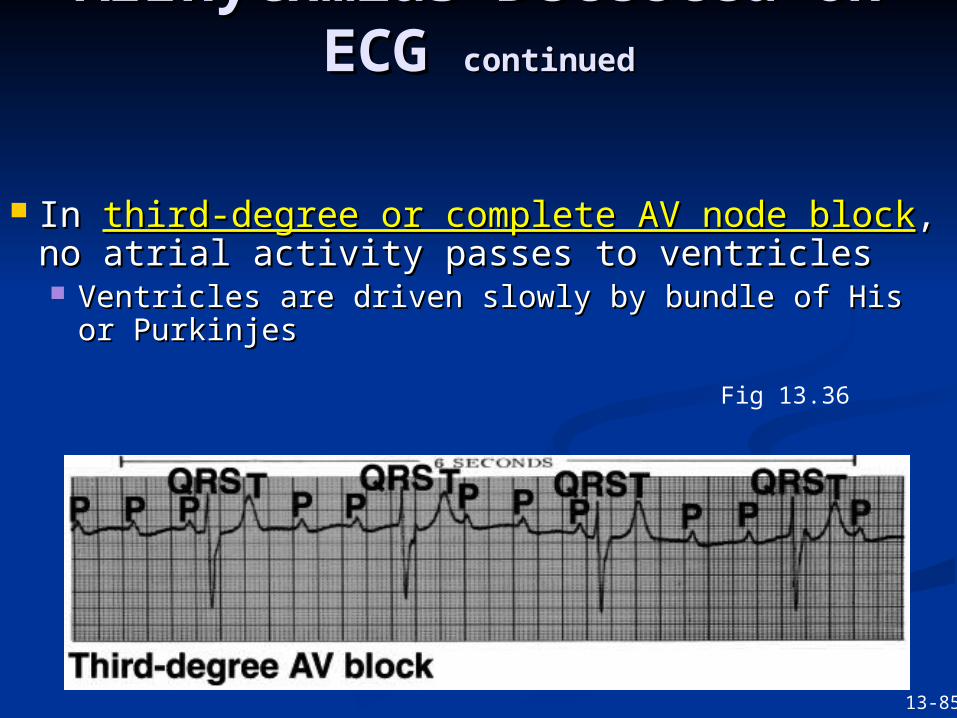
In In third-degree or complete AV node blockthird-degree or complete AV node block, no , no atrial activity passes to ventriclesatrial activity passes to ventricles Ventricles are driven slowly by bundle of His or Ventricles are driven slowly by bundle of His or
PurkinjesPurkinjes
Arrhythmias Detected on Arrhythmias Detected on ECG ECG continuedcontinued
Fig 13.36
13-85
THE CARDIAC THE CARDIAC CYCLECYCLE
ISOVOLUMETRIC ISOVOLUMETRIC CONTRACTIONCONTRACTION
The The
Beginning of systoleBeginning of systole
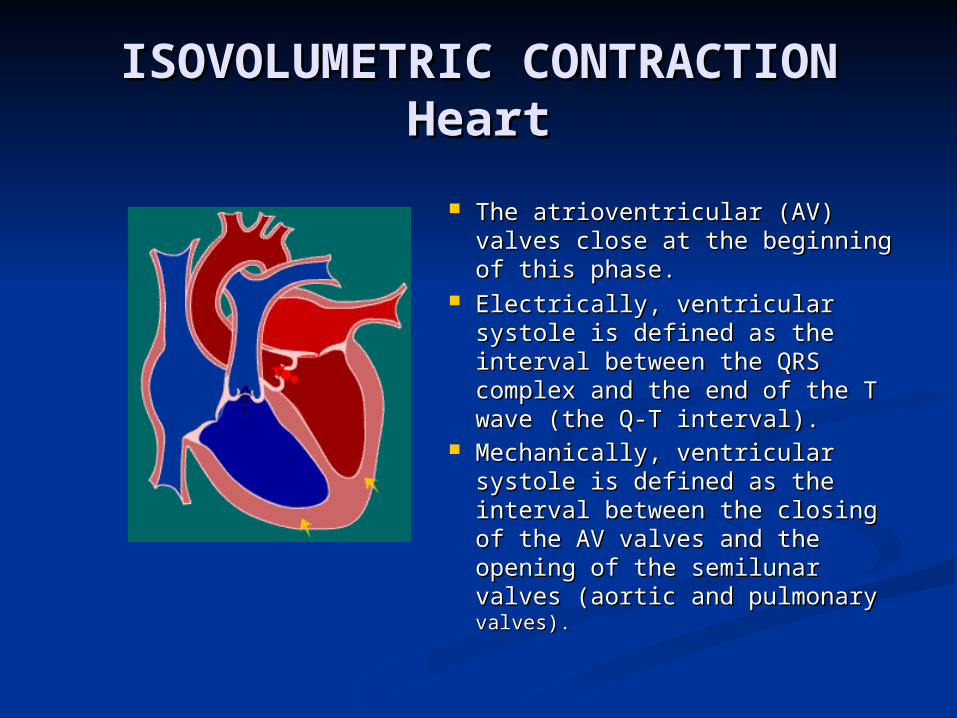
ISOVOLUMETRIC ISOVOLUMETRIC CONTRACTIONCONTRACTION
HeartHeart The atrioventricular (AV) valves The atrioventricular (AV) valves
close at the beginning of this close at the beginning of this phase.phase.
Electrically, ventricular systole Electrically, ventricular systole is defined as the interval is defined as the interval between the QRS complex and between the QRS complex and the end of the T wave (the Q-T the end of the T wave (the Q-T interval).interval).
Mechanically, ventricular Mechanically, ventricular systole is defined as the systole is defined as the interval between the closing of interval between the closing of the AV valves and the opening the AV valves and the opening of the semilunar valves (aortic of the semilunar valves (aortic and pulmonary and pulmonary valves). valves).
RAPID EJECTIONRAPID EJECTION
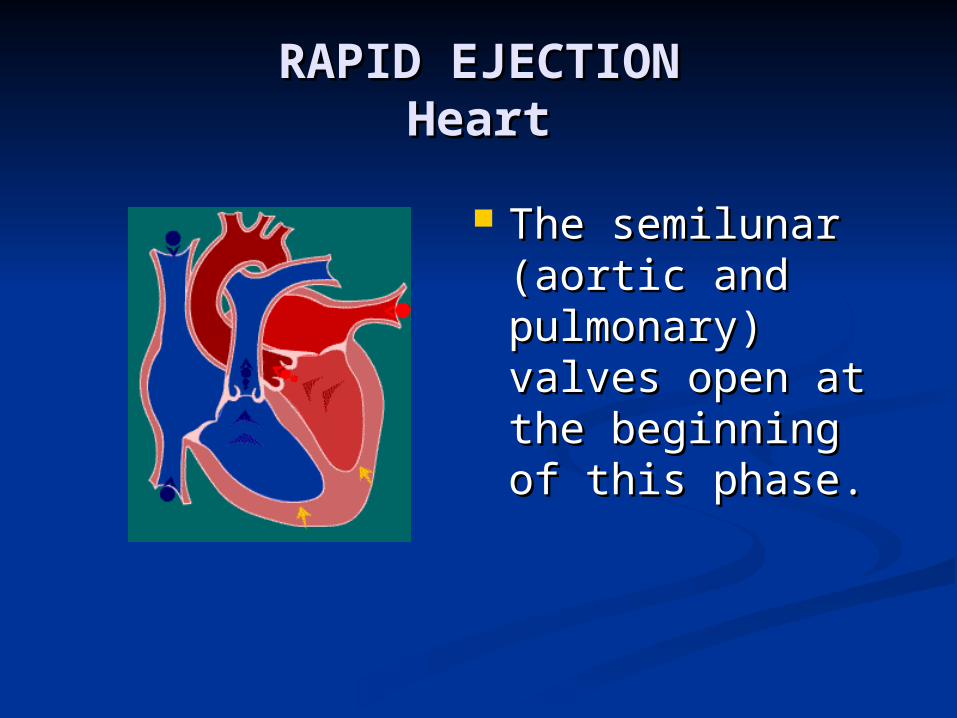
RAPID EJECTIONRAPID EJECTIONHeartHeart
The semilunar The semilunar (aortic and (aortic and pulmonary) valves pulmonary) valves open at the open at the beginning of this beginning of this phase. phase.
REDUCED EJECTIONREDUCED EJECTION
The end of The end of
systolesystole
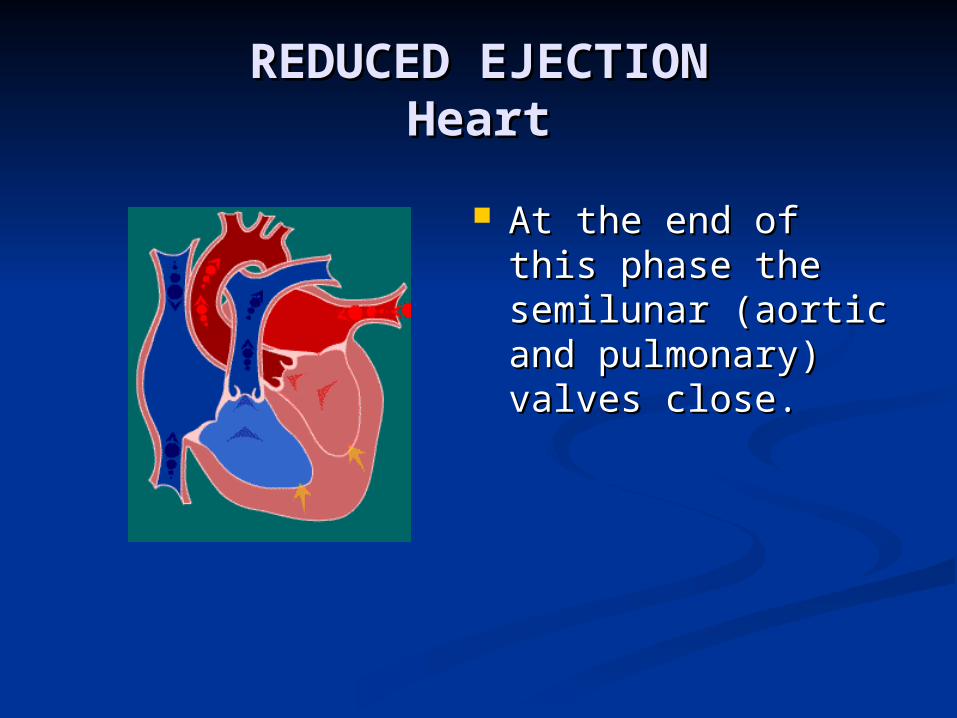
REDUCED EJECTIONREDUCED EJECTIONHeartHeart
At the end of this At the end of this phase the semilunar phase the semilunar (aortic and (aortic and pulmonary) valves pulmonary) valves close.close.
ISOVOLUMETRIC ISOVOLUMETRIC RELAXATIONRELAXATION
The The
beginning of Diastolebeginning of Diastole
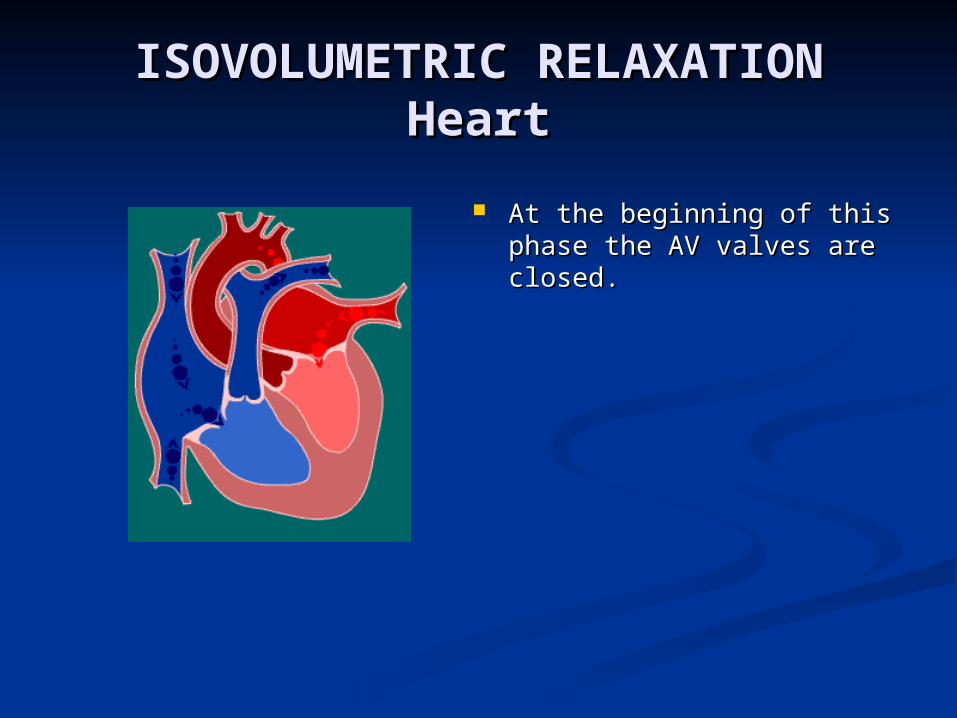
ISOVOLUMETRIC ISOVOLUMETRIC RELAXATIONRELAXATION
HeartHeart At the beginning of this At the beginning of this
phase the AV valves are phase the AV valves are closed. closed.
RAPID VENTRICULAR RAPID VENTRICULAR FILLINGFILLING
REDUCED REDUCED VENTRICULAR VENTRICULAR
FILLINGFILLING (Diastasis) (Diastasis)
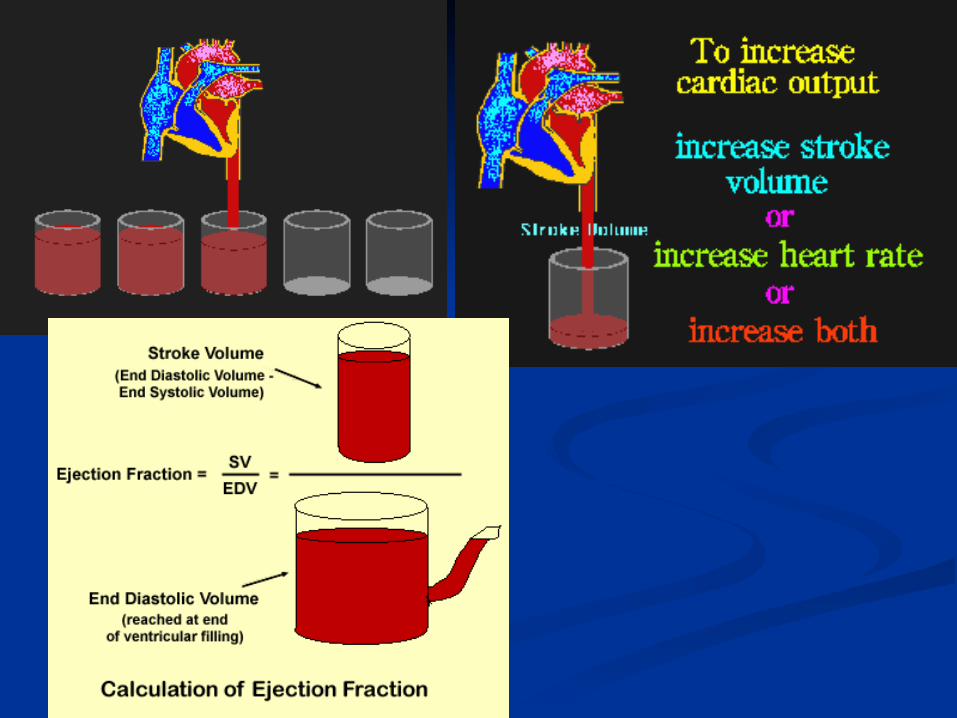
Cardiac Cardiac OutputOutput
When the heart contractsWhen the heart contracts
Cardiac OutputCardiac Output
Cardiac OutputCardiac Output is the volume of blood is the volume of blood pumped each minute, and is expressed by pumped each minute, and is expressed by the following equation:the following equation:
CO = SV x HRCO = SV x HR Where:Where:
COCO is cardiac output expressed in L/min is cardiac output expressed in L/min (normal ~5 L/min)(normal ~5 L/min)
SVSV is stroke volume per beat is stroke volume per beat HRHR is the number of beats per minute is the number of beats per minute
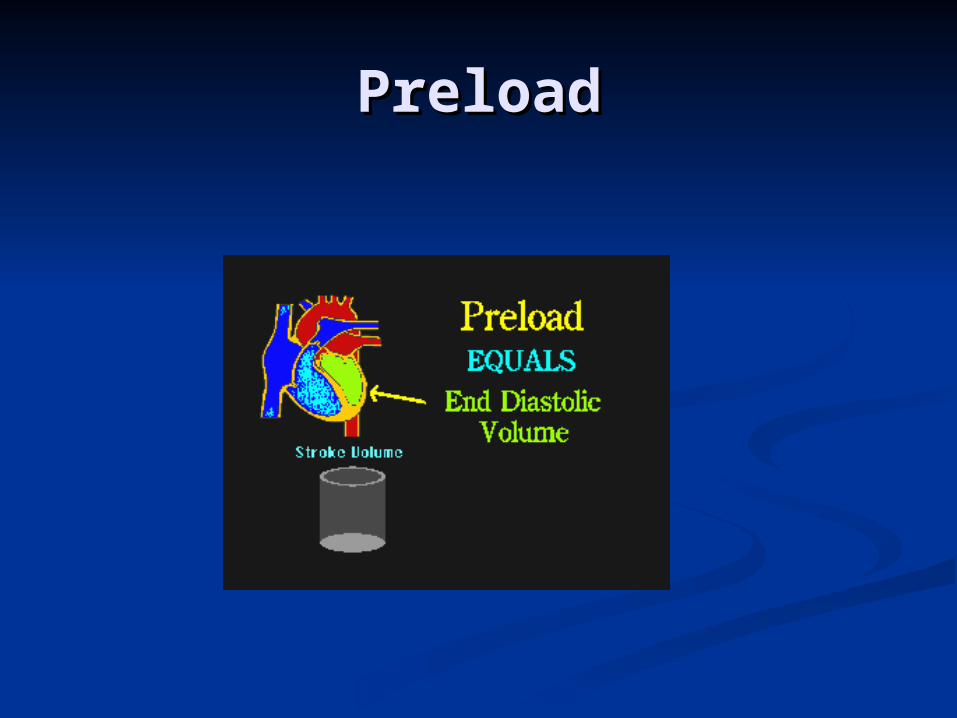
PreloadPreload

PreloadPreload: Preload is the muscle length prior to : Preload is the muscle length prior to contractility, and it is dependent of ventricular contractility, and it is dependent of ventricular filling (or filling (or end diastolic volumeend diastolic volume…EDV) …EDV)
This value is related to right atrial pressure.This value is related to right atrial pressure.
The most important determining factor for The most important determining factor for
preload is preload is venous returnvenous return..
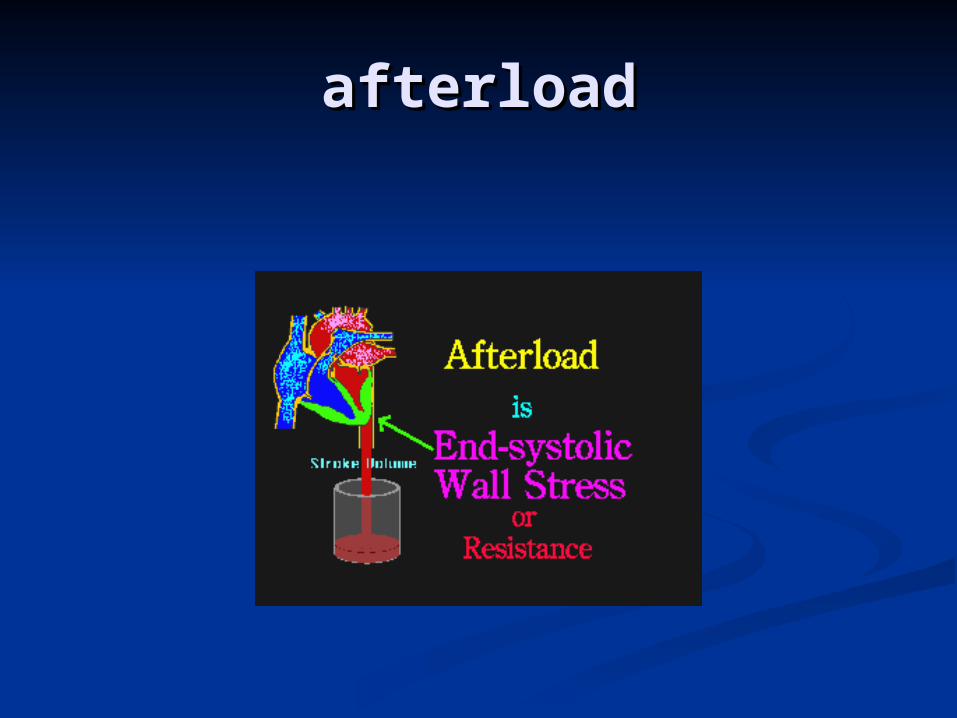
afterloadafterload
AfterloadAfterload: Afterload is the tension (or the : Afterload is the tension (or the arterial arterial pressurepressure) against which the ventricle must contract. ) against which the ventricle must contract.
If arterial pressure increases, afterload also increases. If arterial pressure increases, afterload also increases.
Afterload for the left ventricle is determined by aortic Afterload for the left ventricle is determined by aortic pressurepressure
Afterload for the right ventricle is determined by Afterload for the right ventricle is determined by pulmonary artery pressure.pulmonary artery pressure.
Inotropic and Inotropic and chronotropicchronotropic
Homometric regulationHomometric regulation
Regulation of heart and Regulation of heart and blood vesselsblood vessels
SignificanceSignificance::
To maintain normal blood To maintain normal blood pressure, pressure,
blood flow to be relativity blood flow to be relativity constant.constant.
To redistribute blood supply to To redistribute blood supply to
different tissue and organs.different tissue and organs.
To redistribute blood supply to To redistribute blood supply to
different tissue and organs.different tissue and organs.
Copyright 2009, John Wiley & Sons, Inc.
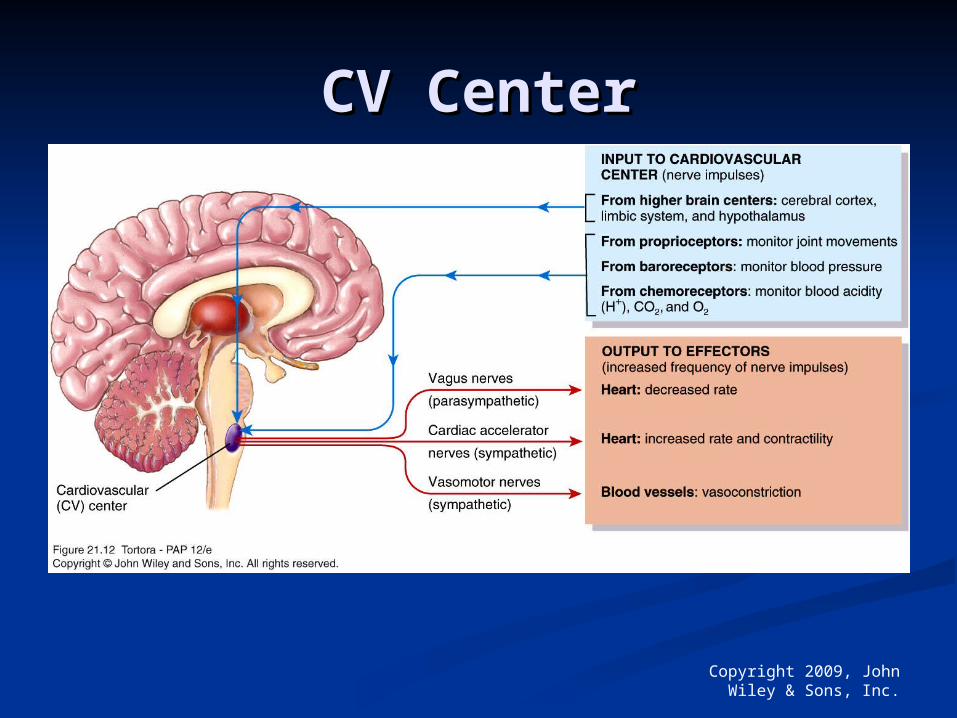
CV CenterCV Center
A. Neural regulation A. Neural regulation
1. Innervation of the 1. Innervation of the
heart heart
dual innervationdual innervation
(1) cardiac sympathetic (1) cardiac sympathetic
nervenerve
(2) cardiac (2) cardiac
parasympathetic nerveparasympathetic nerve
Cardiac Symp nCardiac Symp n Cardiac Cardiac
Vagal nVagal n IML1-5 Amgiguus IML1-5 Amgiguus N, Dorsal N, Dorsal motor N motor N
of vagusof vagus Preganglionic fPreganglionic f Preganglionic fPreganglionic f ACh ACh ACh ACh
Postganglionic N Postganglionic N N receptorN receptor Postganglionic f Postganglionic f Postganglionic fPostganglionic f NE NE Effects Effects AchAch inotropic inotropic receptor receptor chronotropic chronotropic M M receptorreceptor dromotropic dromotropic propranolol propranolol Blocker Blocker atropineatropine
(1) (1) Effects of vagal nerveEffects of vagal nerve
Vagal nerve ending → Vagal nerve ending → ACh.ACh.
→ binds to M cholinergic → binds to M cholinergic
receptor →receptor →↑permeability ↑permeability
to Kto K++ results results
in:in:
↓↓automaticity of S-A nodeautomaticity of S-A node::
↓↓contractilitycontractility due to : due to :
↑↑KK++ efflux at phase 3 efflux at phase 3 repolarizationrepolarization
→↓ →↓AP duration → CaAP duration → Ca2+2+ influx ↓ influx ↓
→ → [Ca[Ca2+2+]]ii↓;↓;
ACh inhibits CaACh inhibits Ca2+2+ influx influx → [Ca → [Ca2+2+]]i i
↓→ ↓↓→ ↓contractility.contractility.
↓ ↓conductivityconductivity
TheThe left left Vagus Vagus
n:↓conductivity in n:↓conductivity in
A-V node A-V node
The The rightright Vagus n: Vagus n:
↓automaticity ↓automaticity
in S-A node. in S-A node.
(2) (2) Effects of cardiac sympathetic Effects of cardiac sympathetic nerve: nerve:
Cardiac sympathetic nerve ending Cardiac sympathetic nerve ending
→ → noradrenaline → binds to noradrenaline → binds to ββ--
adrenergic adrenergic receptor→↑permeabilityreceptor→↑permeability
to Cato Ca2+2+ leads to:leads to:
↑ ↑AutomaticityAutomaticity
↑↑ConductivityConductivity
↑↑ContractilityContractility
The The leftleft Symp n Symp n::↑↑ contractility.contractility.
The The rightright Symp n Symp n ↑:↑: HR.HR.
Sympathetic input - HEARTSympathetic input - HEART
ACTIONSACTIONS Nerve fibers Nerve fibers
release NE release NE SA, atria, and SA, atria, and
ventriclesventricles ↑ ↑ HR and HR and
contractilitycontractility R side SA nodeR side SA node L side contractilityL side contractility
MECHANISMMECHANISM ß1 receptors – ß1 receptors –
pacemaker activitypacemaker activity ß1 myocardium ß1 myocardium
contractioncontraction
Parasympathetic input - Parasympathetic input - HEARTHEART
ACTIONSACTIONS Vagus nerve Vagus nerve
releases ACHreleases ACH SA and myocardiumSA and myocardium HR and conduction HR and conduction
velocityvelocity R side SA node (HR)R side SA node (HR) L side contractility L side contractility
(slight)(slight)
MECHANISMMECHANISM Muscarinic Muscarinic
receptors (M2)receptors (M2) ßßγγ subunit (HR) subunit (HR) Nitric oxide (weak Nitric oxide (weak
inotropic effect) inotropic effect)
Cardiac reflexesCardiac reflexes
Bainbridge ReflexBainbridge Reflex
Infusion of volume causes an Infusion of volume causes an increase in heart rate due to increase in heart rate due to activation of atrial stretch activation of atrial stretch receptors which causes receptors which causes medullary center activation medullary center activation of sympathetic output to the of sympathetic output to the SA nodeSA node
Reflex from atria Reflex from atria Type AType A Type BType B
Reflex from left ventricleReflex from left ventricle Coronary chemo reflex Coronary chemo reflex Sino Aortic reflex Sino Aortic reflex Reflex from peripheryReflex from periphery Reflex from higher centersReflex from higher centers
Arterial blood pressure Arterial blood pressure
Systolic pressureSystolic pressure
Diastolic pressureDiastolic pressure
Mean pressureMean pressure
MAP = DP + 1/3 (SP-DP)
REGULATION OF ARTERIAL REGULATION OF ARTERIAL BLOOD PRESSUREBLOOD PRESSURE
Regulation of Blood Pressure
NervousMechanis
m
Renal Mechanis
m
HormonalMechanis
m
LocalMechanis
m
By Vasomotor Center
and Impulses
from Periphery
By Regulation of ECF Volume
and renin –
angiotensin
mechanism
By Vasocons-
-trictor and
Vasodilator
Hormones
By Local Vasocons--trictors
and Vasodilato
rs
REGULATION OF ARTERIAL REGULATION OF ARTERIAL BLOOD PRESSUREBLOOD PRESSURE
SHORT-TERM CONTROLSHORT-TERM CONTROL
(IN SEC – MIN)(IN SEC – MIN)
INTERMEDIATE-TERM INTERMEDIATE-TERM CONTROLCONTROL
(30 MIN – HOURS)(30 MIN – HOURS)
LONG – TERM CONTROLLONG – TERM CONTROL
SHORT-TERM CONTROL OF SHORT-TERM CONTROL OF APAP
CNS ISCHAEMIC RESPONSECNS ISCHAEMIC RESPONSE
BARORECEPTOR REFLEXBARORECEPTOR REFLEX
CHEMORECEPTOR REFLEXCHEMORECEPTOR REFLEX
INTERMEDIATE CONTROL INTERMEDIATE CONTROL OF APOF AP
RENIN - ANGIOTENSIN – RENIN - ANGIOTENSIN – VASOCONSTRICTOR MECH.VASOCONSTRICTOR MECH.
STRESS RELAXATION OF STRESS RELAXATION OF VASCULATUREVASCULATURE
FLUID – SHIFT THROUGH FLUID – SHIFT THROUGH THE CAPILLARY WALLTHE CAPILLARY WALL
LONG – TERM CONTROL OF LONG – TERM CONTROL OF APAP
RENAL FLUID SHIFT RENAL FLUID SHIFT (THROUGH ADH / VOLUME (THROUGH ADH / VOLUME RECEPTORS)RECEPTORS)
RENIN – ANGIOTENSIN – RENIN – ANGIOTENSIN – ALDOSTERONE MECH.ALDOSTERONE MECH.
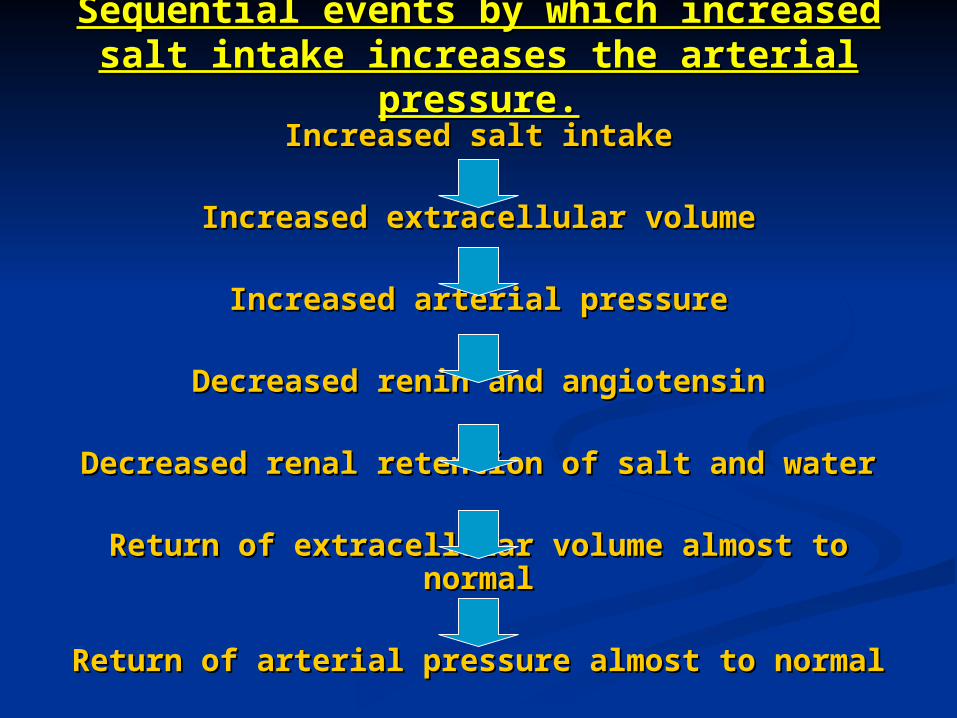
Sequential events by which increased Sequential events by which increased salt intake increases the arterial salt intake increases the arterial
pressure.pressure.Increased salt intakeIncreased salt intake
Increased extracellular volumeIncreased extracellular volume
Increased arterial pressureIncreased arterial pressure
Decreased renin and angiotensinDecreased renin and angiotensin
Decreased renal retention of salt and waterDecreased renal retention of salt and water
Return of extracellular volume almost to Return of extracellular volume almost to normalnormal
Return of arterial pressure almost to normalReturn of arterial pressure almost to normal
LOCAL MECH. FOR CONTROL LOCAL MECH. FOR CONTROL OF APOF AP
A.A. VasodilatosVasodilatos
1. 1. EDRFEDRF
2.2. Bradykinin Bradykinin
3.3. Histamine Histamine
4.4. ANP ANP
5.5. VIP VIP
6.6. Substance Substance PP
7. Prostacyclin8. Adenosine
9. K+
10. Acidosis [ CO2]
11. Hypercapnia12. Hypoxia13. Temperature
B.B. Vasoconstrictors Vasoconstrictors
1.1. Endothelin-1Endothelin-1
2.2. Angiotensin IIAngiotensin II
3.3. NorepinephrineNorepinephrine
4.4. ADHADH
5.5. SerotoninSerotonin
6.6. Thromboxane A2Thromboxane A2
7.7. Neuropeptide-YNeuropeptide-Y
8.8. ColdCold
HORMONAL MECH. FOR HORMONAL MECH. FOR CONTROL OF APCONTROL OF AP
HORMONES RAISING APHORMONES RAISING AP ADRENALINEADRENALINE NORADRENALINENORADRENALINE THYROXINETHYROXINE ALDOSTERONEALDOSTERONE VASOPRESSINVASOPRESSIN ANGIOTENSINANGIOTENSIN SEROTONINSEROTONIN
HORMONAL MECH. FOR HORMONAL MECH. FOR CONTROL OF APCONTROL OF AP
HORMONES DECREASING APHORMONES DECREASING APVIPVIPBRADY KININBRADY KININPROSTAGLANDINPROSTAGLANDINHISTAMINEHISTAMINEACETYLCHOLINEACETYLCHOLINEANPANP