Embed Size (px)
Citation preview

BIOMECHANICS OF PATELLOFEMORAL INSTABILITY
C. C U R T I S E L L I O T T , MD, and D A V I D R. D I D U C H , MS, M D
The patellofemoral joint functions as a complex extensor apparatus with important biomechanical contributions provided by both articular contact and the surrounding soft tissues. The patella must remain relatively stable while tracking along the anterior and distal surfaces of the femur. If there is instability in the coronal plane (subluxation or dislocation) or around the caudocranial axis (tilt), then pain may result. Stability is maintained through the precise interaction of the patellofemoral articulating surfaces, passive and active soft-tissue restraints, and the alignment of the lower extremity. The purpose of this article is to review these biomechanical variables and how they relate to the treatment of patellofemoral instability. KEY WORDS: biomechanics, patellofemoral, instability, subluxation, dislocation Copyright © 2001 by W.B. Saunders Company
The articular surface of the patella is divided into medial and lateral facets by a central ridge. A second vertical ridge near the medial border isolates a narrow articulating strip known as the odd facet. Wiberg 1 classified patellae into 3 types based on the position of the major vertical ridge. Baumgartl 2 added a fourth type. When progressing from a type I to a type IV, there is a gradual increase in the size of the lateral facet. Reider et al 3 found a high correla- tion between the Wiberg type and the width of the lateral patellofemoral ligament. The larger the lateral facet, or greater the Wiberg type, the broader its lateral patel- lofemoral ligament tended to be. This does not suggest that a thick, broad lateral patellofemoral ligament causes lateral patellar tracking, but it appears to be associated with it.
The medial and lateral facets of the femoral trochlea are asymmetrical. In a normal knee, the patella enters the trochlear sulcus from the lateral side, causing the lateral facet to extend proximally more than the medial. The lateral facet is also a few millimeters more prominent than the medial. The greater height or thickness of the lateral trochlear facet contributes to the osseous stability of the joint. The trochlear sulcus averages 7.8 mm in depth. 4 A shallow trochlea may be insufficient to prevent the patella from dislocating laterally even if it engages properly at the beginning of flexion, s A shallow trochlear sulcus is com- mon in knees with lateral patellar instability. 6
Although orthopedists traditionally rely on axial radio- graphs of the knee to evaluate the patellofemoral articu- lation, magnetic resonance arthrotomography has now proven that there are substantial differences in the geom-
From the Department of Orthopaedic Surgery, University of Virginia, Charlottesville, VA.
Address reprint requests to David R. Diduch, MD, UVA Department of Orthopaedics, University of Virginia, PO Box 800159, Charlottesville, VA 229O8-0159.
Copyright © 2001 by W.B. Saunders Company 1060-1872/01/0903-0001 $35.00/0 doi:10.1053/otsm.2001.25157
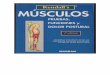
etry and anatomy of the surface of the articular cartilage and the corresponding subchondral osseous contours of the patellofemoral joint 7 (Fig 1). Before decisions are made concerning the diagnosis and management of patellar and /o r trochlear dysplasias, the geometry of the opposing articular surfaces may need to be considered by way of magnetic resonance arthrogram.
THE P A T E L L O F E M O R A L PASSIVE SOFT-T ISSUE R E S T R A I N T S
During knee flexion and extension, the patella is guided by both passive and active soft-tissue restraints. These structures anchor the patella by forming a cruciform ar- rangement 6 (Fig 2). The passive restraints consist of the patella tendon, the quadriceps tendon, and those struc- tures combining to form the medial and lateral retinacu- lum. The average length of the patellar tendon 3 is 4.6 cm. It runs from the inferior margin of the patella to the tibial tubercle in an oblique, lateral direction. This contributes to the normal valgus alignment of the extensor apparatus, which adds to the tendency toward lateral displacement of the patella. 6 There is a negative correlation between the length of the patellar tendon and the width of the medial patellofemoral ligament (MPFL). 3 Longer patellar tendons (patella alta) are associated with smaller or absent MPFL 3 as well as lateral instability of the patella. 8
Regarding the medial retinaculum, anatomic studies have identified at least 4 distinct soft-tissue structures along the medial side of the knee that may play a role in maintaining patellar stability 9 (Fig 3). (1) The MPFL runs from the adductor tubercle to the proximal two thirds of the medial border of the patella. 1° It also has insertions on the deep surface of the vastus medialis and the vastus intermedius. (2) The medial parapatellar retinaculum is formed from a condensation of 2 fascial planes on the medial aspect of the knee and has a broad insertion on the medial patella. 1° (3) The medial patellomeniscal ligament originates from the anterior portion of the medial menis- cus and inserts onto the inferior one third of the patella. 1~
112 Operative Techniques in Sports Medicine, Vol 9, No 3 (July), 2001: pp 112-121

Fig 1. Imaging modalities and diagrams of the same right knee in extension, axial plane. Note the error in the radiologic appearance of the osseous contours (A and C) and the per- fect matching of articular cartilage surfaces in the axial plane of the same right knee on double-contrast magnetic reso- nance arthrotomography (B and D). (Reprinted with permis- sionF)
and patellotibial ligaments were shown to be important secondary stabilizers. Additional release of these liga- ments after release of the MPFL resulted in considerably greater lateral patellar displacement. In addition, repair of these 2 ligaments restored medial-lateral balance to near normal levels. The medial retinaculum, as shown by other investigators played only a minor role in providing medial stability.
In a cadaver study by Reider et al, 18 a medial parapa- tellar soft-tissue release resulted in decreased medial pa- tellar shift and a switch to lateral tilting in a significant portion of the specimens. They concluded that weakening or disruption of these static medial soft-tissue restraints leads to abnormal tracking. A finding in their study was that the MPFL was present in only 7 of 20 (31%) knees that they dissected. When present, the breadth of the ligament ranged from 5 to 12 mm. The lack of a clearly identifiable MPFL in 69% of their specimens, as opposed to others in which it was present in 90% to 100% of dissected knees, 9,11 suggests that this structure may not be a constant entity in normal knees. This is an important issue because several new surgical strategies aimed at patellar instability (espe- cially acute dislocations) are based on repairing or aug- menting this structure.
The third passive, or static, soft-tissue restraint is pro- vided by the lateral retinaculum. Fulkerson and Grossling ~4 described the anatomic details of the lateral retinaculum in 24 dissected knees (Fig 4). The most super-
(4) The medial patellotibial ligament is a thickening of the anterior capsule and runs from the anteromedial aspect of the tibia to the inferior aspect of the patella. 12
There have been several investigations to evaluate the relative contributions of the various medial structures that act to resist a laterally directed force. By sectioning differ- ent structures along the medial aspect of knee specimens, Conlan et a111 found that the MPFL is the major soft-tissue static restraint that resists lateral patellar displacement, contributing an average of 53% of the total medial, static restraining force. The medial patellomeniscal ligament was also found to be a significant medial stabilizer, con- tributing 22% of this total force. The medial retinaculum and the patellotibial ligaments made minimum contribu- tions of 11% and 5%, respectively.
Desio et a113 also studied the medial soft-tissue struc- tures in 9 fresh-frozen cadaveric knees. They found the MPFL to be the primary static restraint to lateral patellar translation at 20 ° of flexion, contributing 60% of the total restraining force. The medial patellomeniscal ligament contributed 13% of the restraining force. The medial reti- naculum and the medial patellotibial ligament were not found to be functionally important.
Hautamaa et al 9 studied 17 fresh-frozen anatomic knee specimens. They also sequentially sectioned different parts of the medial soft-tissue stabilizers. The MPFL, which they identified in every specimen, was found to be the major static restraint. Isolated release resulted in a 50% increase in lateral patellar displacement, and isolated repair re- stored balance to the patella. The medial patellomeniscal
lateral r vastus If iliotibiat
,,dial retinaculum d vastus medialis
Fig 2. The patella is anchored and stabilized to the knee by 4 structures in a cruciform fashion: the patellar tendon infe- riorly, the quadriceps tendon superiorly, and the retinacula medially and laterally. (Reprinted with permission. 6)
BIOMECHANICS OF PATELLOFEMORAL INSTABILITY 113

~ductor agnus ~don
:Ulum aiscal
Fig 3. Anatomy of the medial patellofemoral passive soft- tissue restraints.
Fig 6. The Q angle.
angle
s
f
i' J
Vastus medialis Iongus
Vastus medialis obliquus
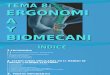
Fig 5. The vastus medialis complex is composed of the vastus medialis Iongus and VMO muscles.

,Vastus. \
ylopatellar
lnsverse Suoerfic rum oblique (reflecte ~ial band
Fig 4. Anatomy of the lateral patellofemoral passive soft- tissue restraints. (Reprinted with permission, s )
ficial layer, the superficial oblique retinaculum, is com- posed of fibers running distally and anteriorly from the anterior border of the iliotibial band to the lateral margin of the patella and patellar tendon. They described a deep layer consisting of 3 bands including an epicondylopatel- lar band, a transverse band from the deep surface of the iliotibial band to the lateral border of the patella, and a patellotibial band. Kaplan 15 also described the lateral epi- condylopatellar ligament, which is the most proximal of these 3 condensations. However , Reider et al 3 was only able to find the epicondylopatellar ligament, which they called the lateral patellofemoraI ligament, in 13 of 20 (65%) fresh knee specimens.
Luo et al ~6 examined 7 cadaveric specimens and found that the tensile stress in the lateral patellofemoral ligament increased significantly around 30 ° of knee flexion. They believed that this increase in the lateral restraining force contributed to the lateral subluxation that occurs at 20 ° to 30 ° of knee flexion in a patient who has patellar instability. It has also been postulated that the portion of the lateral retinaculum connecting the patella to the iliotibial band may cause a laterally directed force with knee flexion. 6 However, other investigators have shown that the lateral retinaculum plays only a passive role; in other words, there is no active pull on the patella. Heegaard et a117 found that the lateral retinaculum contributed very little to patellar tracking in knee specimens which were ex- amined before and after a dissection which left only the bony elements, the cruciate and collateral ligaments, the patella tendon, and the rectus femoris tendon. In another cadaver study, Reider et a118 illustrated that release of the lateral retinaculum had no effect on the tracking of most of the 20 specimens they examined. They concluded that the indiscriminate use of isolated lateral release would not be beneficial in knees in which the lateral retinaculum is normal.
T H E P A T E L L O F E M O R A L A C T I V E S O F T - T I S S U E R E S T R A I N T S
The active restraints on medial-lateral patellar motion con- sist mainly of the quadriceps apparatus. Because of their obliquity in relation to the long axis of the femur, the vastus medialis and the vastus lateralis are the most im- portant contributors in preventing and causing instability, respectively.
In 1968, Lieb and Perry 19 described the anatomy and function of the quadriceps mechanism. After dissecting 6 cadaver specimens, they considered the vastus medialis to be composed of 2 parts because of the marked and abrupt change in fiber alignment between its proximal and distal portions. The upper fibers, which they named the vastus medialis longus, angled 15 ° to 18 ° medially in relation to the long axis of the femur. The lower fibers, they called the vastus medialis obliquus (VMO), angled 50 ° to 55 ° medially, and their insertion is close to the superomedial margin of the patella (Fig 5). The VMO has been found to contribute approximately 30% of the physiologic cross-sectional area of the vastus medialis complex. Lieb and Perry 19 examined the function of the separate heads of the quadriceps in an additional 22 specimens. By altering the applied forces of cables connected with the different muscles, they con- cluded that the only selective function attributable to the VMO is patellar alignment.
Goh et al 2° examined the function of the VMO in 6 normal cadaver limbs. They found that absent VMO ten- sion caused the patella to displace laterally and increased the load on the lateral patellar facet throughout the range of knee motion. A 40% reduction of the lateral vector was required to counterbalance the lateral displacement of the patella caused by the absent VMO. The VMO is thought to be the main active medial patellar stabilizer. In a study by Henry and Craven, 2I 91% of 557 knees with patellar sub- luxation showed signs of a dysplastic VMO. Dysplasia of the VMO has been defined clinically as a large concavity medial to the patella that correlates with muscle atrophy. 22 Other investigators believe that VMO dysplasia refers to an insertion angle less oblique than normal, decreasing its mechanical advantage and its ability to act as a medial stabilizer. 23
There is a notable relationship between the static re- straint mechanism, the MPFL, and the active restraint mechanism, the VMO. Conlan et a111 performed an ana- tomic dissection of the medial soft tissues in 25 fresh- frozen knee specimens. They noted that the MPFL, present in more than 90% of dissected knees, had insertions on the deep surface of the distal aspect of the VMO and vastus intermedius, as well as on the superomedial aspect of the patella. By originating from the adductor tubercle and having insertions on the deep surface of the distal anterior fibers of the VMO, it acts as a checkrein, preventing ex- cessive elongation of the fibers of the VMO and lateral subluxation of the anterior portion of the VMO over the medial femoral condyle. They believed that disruption of the MPFL origin from the femur might have led other investigators to conclude that the VMO had avulsed from the adductor tubercle. 24 Conlan et al ~ found that the ori- gin of the VMO was actually 0.5 to 6.0 cm (average of 3.3 cm) proximal to the adductor tubercle, at the medial
BIOMECHANICS OF PATELLOFEMORAL INSTABILITY 1 15

intermuscular septum and the adductor magnus tendon. Bose et a125 also showed that the VMO arises primarily from the adductor magnus tendon, not from the adductor tubercle. In their study, the origin of the VMO ranged from 1.5 to 7.5 cm (average 3.5 cm) proximal to the adduc- tor tubercle. It was believed that injury to the VMO origin and its checkrein, the MPFL, changed its normal oblique orientation to a more vertical orientation, impairing the ability to offer medial stability to the patella.
The muscle fibers of the vastus lateralis approach the patella at an angle to the rectus tendon averaging 31 ° . The fibers terminate more proximally than those of the VMO (average of 2.8 cm from the superolateral corner of the patella). 3 Similar to the VMO configuration, the most distal part of the muscle has been shown to be anatomically distinct and was named the vastus lateralis obliquus. 26 These fibers originate from the lateral intermuscular septum and appear to function as a lateral displacing force on the patella.
BIOMECHANICAL INFLUENCES ON PATELLAR TRACKING
In full extension, the screw-home mechanism of the tibia, rotating externally in the terminal 30 ° of extension, dis- places the tibial tubercle laterally. 27 The angle formed between the direction of the quadriceps force and the direction of the patellar tendon is called the Q angle (Fig 6). It is measured clinically by the intersection of the line connecting the anterior superior iliac spine to the center of the patella (rectus femoris vector), and the line between the center of the patella and the tibial tubercle. Aglietti et a128 reported a normal Q angle of 14 ° in males and 17 ° in females, with both genders having a standard deviation of 3 °. Post and Fulkerson 29 noted that an angle of greater than 10 ° in males and 15 ° in females is considered poten- tially abnormal. The Q angle is a useful dynamic concept, but can be an unreliable measurement, because an unsta- ble patella lies more lateral than normal in full extension, decreasing the angle. This may produce a "J sign," which can be appreciated when observing active patellar track- ing through a range of motion, indicating subluxation in full extension. In this case, slight flexion of the knee to about 15 ° will engage the patella within the trochlear groove to allow a more accurate measurement of the Q angle.
Tension on the quadriceps, specifically the rectus fem- oris and the vastus lateralis, tends to produce a lateral displacement vector on the patella. As noted, this lateral or "valgus vector" is resisted by the distal muscle fibers of the VMO. By evaluating the normal torque equilibrium about the knee, 3° one can see the importance of the VMO's action (]qM)" The sum of the forces of the rectus femoris (FM), vastus lateralis (FL), and the patella tendon (};T1) is equal to the resultant lateral force created by the Q angle (RL). The sum of the normal quadriceps mechanism (F M + F R + FL) is equal to the counterforce at the tibia (FT2). Therefore, the potential lateral vector (RL) is equal to zero when the quadriceps, including the VMO, is functioning normally (Fig 7). The static medial soft-tissue restraints (MPFL) and the prominent lateral trochlear facet also help resist this laterally directed force. 27
F[.* FR"* #M
\ \ \
, FT 1 ~\
\
\
\ \
\, \
\
\
FT 2
Fig 7. Vector diagram of the quadriceps muscle. FL, force exerted by the vastus iateralis; FR, force exerted by the rectus femoris; FM, force exerted by the vastus medialis; RL, resulting lateral force as the sum of FL + FR -I- FT1 , FT1 = force at the tibia = the counter act force of F L -F FR, FT2 = force at the tibia = the counter act force of F L + F R 4- F M. (Reprinted with permission. 3o)
With the knee in full extension and the quadriceps contracted, the patella lies proximal to the trochlea, resting against the supratrochlear fat pad. Heegaard et a117 showed that the tibia internally rotates during the first 15 ° of flexion. This derotation decreases the Q angle, decreas- ing the lateral vector. As flexion proceeds, the patella is drawn into the entrance of the trochlea. Because of the Q angle, the patella enters the troclea from the lateral side. 27 The degree of knee flexion required for the patella to reach the trochlea depends on the patellar tendon l eng thy When a long patella tendon is present, a high patella, or patella alta, is the result. Normally, patellofemoral contact is made between 10 ° to 20 ° of flexion along the inferior margin of the patella in a broad, continuous band across both medial and lateral facets. With patella alta, the patella will not engage the trochlea until the knee is flexed more, so there is a greater range in which instability may occur. As flexion proceeds, the contact area moves proximally on the patella, extending from the ridge separating the medial from the odd facet to the lateral border of the lateral facet. 27 As flexion continues, patellar contact shifts proxi- mally. The odd facet does not come into contact with the
116 ELLIOTT AND DIDUCH

femur until significant flexion is obtained and the patella sinks into the intercondylar notch. Before about 30 ° of flexion, the soft-tissue restraints, both active and static, are the most important factors in preventing patellar tilt a n d
subluxation. 17 After firm patella-trochlea contact is made, the resultant flexion compresses the patella against the femur. The congruence of the patellofemoral joint and this force provide considerable stability irrespective of the re- straining soft tissuesY ,27
PREDISPOSING RISK FACTORS FOR PATELLOFEMORAL INSTABILITY
Before beginning a course of treatment, the surgeon should pay careful attention to all potential contributions to patellar instability. Failure to correct an anatomic con- tributor such as a high Q angle may predispose to treat- ment failure. The biomechanical factors described that influence patellar tracking are affected by the anatomy a n d c a n be seen on physical examination (Table 1). Normal overall alignment of the lower extremity is important for a proper functioning patellofemoral joint. Limb alignment that includes increased anteversion of the femoral neck, internal femoral rotation, external tibial rotation, genu valgum, and lateral insertion of the patellar tendon c a n
singly or collectively increase the Q angle, assuming that the patella remains in the femoral sulcus. 31 Larson has shown that the effects of limb alignment on patellar track- ing may be exaggerated during functional activities. 32 Genu recurvatum is also a potential contributor to lateral patellar instability. 33 The position of the foot may be im- portant as well, because excessive pronation at the subta- lar joint is accompanied by external tibial torsion and compensatory valgus positioning of the knee, which can increase the Q angle. 6
Abnormalities of the patellofemoral articulation may affect tracking, is The patella may fail to engage and re- main in the trochlea if there is patella alta, 34-36 patellar dysplasia, 37-42 or a poorly developed trochlea. 5,24,33,34,37-49
The importance of the supporting soft-tissue structures in maintaining medial and lateral stability has been dis- cussed. Abnormalities of these structures include VMO dysplasia, laxity of the medial static restraints (MPFL, patellomeniscal ligament, patellotibial ligament) 9,11,1s ei- ther secondary to injury or as a part of a generalized joint laxity, and tightness of the lateral restraints, including the vastus lateralis, lateral retinaculum, and lateral patel- lofemoral l igamentY s,31 Other soft tissues that may be tight with patellar malalignment are the hamstrings, the
T A B L E 1. Anatomic Contributors to Increased Lateral Displacement Forces on the Patella and Patellar Instability
increased Q angle Soft-Tissue Contributors Bony Contributors
Femoral anteversion Tibial torsion Valgus knee alignment Excessive foot
pronation Wide pelvis (females)
Dysplasic VMO Tight lateral retinaculum Patella alta Generalized ligamentous
laxity Torn or attenuated MPFL
Patellar dysplasia Trochlear dysplasia
iliotibial band, the quadriceps, the hip rotators, and the Achilles tendon. 5°
BIOMECHANICAL CONSIDERATIONS IN THE TREATMENT OF PATELLOFEMORAL INSTABILITY
N o n o p e r a t i v e T r e a t m e n t
Historically, nonoperative treatment has been the hall- mark of therapy for all patellofemoral instability. Patients with patellar malalignment and pain should receive a well-structured program of rehabilitation that consists of stretching the tight soft tissues which affect patellar track- ing, strengthening exercises for the quadriceps (especially the VMO), and modification of activity. 5°,5~ Strengthening of the quadriceps is usually beneficial as long as it does n o t
cause pain. 5° Coordination of VMO and vastus lateralis muscle activity is as important as strength training. Biofeedback from surface electrodes has been used to help facilitate this therapy. 52,53
Simple bracing with an elastic patellar cutout brace may be helpful to some patients. 54 Their mode of action is speculative, but it is felt that the brace provides relief by stabilizing the patella during early flexion. This may help to overcome lateral forces, which cause subluxation or dislocation. McConnel155 recommended a patellar taping method that helps to pull the patella medially, controlling tilt and subluxation. Going back to the torque equilibrium, it is believed that the taping contributes to the medial stabilizing vector. This may be especially beneficial in a patient who has VMO weakness or dysplasia. Initial re- sults of a rehabilitation program using McConnell's patel- lar taping protocol had a success rate of 92%. However, in a prospective, randomized study, Kowall et a156 suggested that there was no benefit of adding a patellar taping pro- gram to a standard physical therapy protocol. Finally, orthotic devices may help alleviate lower extremity mal- alignment caused by excessive foot pronation. 57,58
Opera t ive T r e a t m e n t
Surgical intervention is usually considered when symp- toms from patetlar instability persist for longer than 6 months despite undergoing an individualized therapy program. If an episode of subluxation or dislocation oc- curred primarily because of a direct traumatic force, the patient is more likely to respond to conservative manage- ment. The indirect mechanism is more common, and in- volves the combination of a strong quadriceps contraction, a slightly flexed and valgus knee position, and an inter- nally rotated femur on an externally rotated tibia. 59 Pa- tients with an indirect mechanism typically have predis- posing risk factors, such as malalignment. When there is significant malalignment, there is a greater tendency for dislocation to recur. 6° Younger patients with partially de- veloped quadriceps musculature are also more prone to have problems with recurrent patellofemoral instability. 61
There has been an abundant number of surgical proce- dures put forth to address patellofemoral instability. Al- though the list seems endless, the procedures can be grouped into 2 main types based on how the biomechanics
BIOMECHANICS OF PATELLOFEMORAL INSTABILITY 1 1 7

of the patellofemoral joint are affected. The first type, proximal realignment, includes procedures that release tight lateral structures and /o r repair, reinforce, or transfer medial stabilizing structures. This category includes lat- eral retinacular release, 47,62-66 medial plication, 67-69 VMO advancement, 7° and MPFL repair or reconstruction. 9,71-77 By enhancing the action of the VMO, the active, medial stabilizing force is increased. The balance between the static restraints may be shifted medially by restoring the MPFL and/or releasing a tight lateral retinaculum. Most of these procedures not only stabilize the patella, but also medialize it. This fact must be appreciated because the Q angle can actually increase after performing a proximal realignment procedure.
The next category, distal realignment, improves the Q angle by reorienting the insertion of the patellar tendon. 7s This effectively decreases the lateral vector acting on the patella. These include medial transfer of the patellar ten- don, 79 medial transfer of the lateral portion of the patellar tendon, s° medial displacement of the tibial tubercle, s1 an- teromedial displacement of the tibial tubercle, s2-s4 and dis- tal and medial transfer of the tibial tubercle. 44 A lateral release is usually added to the distal realignment proce- dures to remove the tethering effect of the static lateral restraints. 29
An operation that has fallen out of favor is the Hauser procedure, in which the tibial tubercle is transferred dis- tally and medially. 44 The distal advancement is beneficial when the patient has instability resulting from patella alta. The medial displacement improves the Q angle. However, the downward slope of the medial, proximal tibia causes a posterior displacement of the tibial tubercle. This has been associated with a high rate of patellofemoral arthritis, presumably because of its tightening effect on the extensor mechanism and the resultant increase in joint reactive force. 85
The Roux-Emslie-Trillat procedure is usually the pre- ferred technique for a direct medial transfer of the tibial tubercle, s~ This osteotomy is made in the true coronal plane of the body, therefore there is no posterior displace- ment along the slope of the proximal tibia. A lateral release and medial capsular reefing are usually performed in ad- dition to the osteotomy.
When there are articular cartilage lesions at the distal, lateral aspects of the patella in addition to a laterally positioned tibial tubercle, a Fulkerson osteotomy is the more likely successful procedure. 29,54,s3 An anteromedial tibial tubercle transfer is created by an oblique osteotomy. Depending on the obliquity of the osteotomy, the amount of anterior or medial displacement can be varied. A steeper cut allows more anterior displacement of the tu- bercle, which increases the moment arm of the patella tendon. Patellofemoral joint reactive forces are transferred from the distal, lateral patella to the articular surface at the proximal, medial patella. This procedure will not be ben- eficial to a patient who also has chondral defects on the proximal, medial patella. When malalignment from an increased Q angle is more of a concern, the obliquity of the osteotomy is decreased, resulting in more medial displace- ment of the tibial tubercle.
When treating patellofemoral instability, a lateral reti- nacular release is used as an adjunct to a proximal and /o r
distal realignment. When used alone to treat lateral patel- lar instability, lateral retinacular release will give poor results. 86 Huberti and Hayes s7 showed that there is little redistribution of stress after lateral release of a normally aligned patella. Release of this static restraint does not significantly reduce the active lateral vector, s6 It also does not affect predisposing factors for instability, such as an increased Q angle. However, patients who have excessive tilt to their patella radiographically, and on physical ex- amination display painful signs resulting from lateral pa- tellar compression syndrome, may do well with an iso- lated lateral retinacular release, s6
Before selecting a procedure to treat patellofemoral in- stability, the orthopaedist must identify any pathologic anatomy the patient may have. Injured soft-tissue struc- tures that stabilize the patella, such as the MPFL, may need to be addressed. The surgeon must also consider the patient's age, level of activity, causative factors, and the condition of the articular surfaces, ss By customizing the treatment to each individual patient, optimum results will be obtained.
Treatment of Acute Patellofemoral Dislocations
The treatment of acute, primary patellar dislocations has recently become somewhat controversial. Natural history studies of the nonoperative management of these injuries have shown mixed and poor results. Cofield and Bryan 1° noted a 44% redislocation rate in 48 patients with conser- vatively treated patellar dislocations. Hawkins et al, 6° re- ported a 15% redislocation rate in patients who were im- mobilized for 3 weeks after the injury. Hughston and Deese s9 had a 20% to 43% redislocation rate in their pa- tients. Maenpaa and Lehto 90 reported on 100 patients treated nonoperatively for first-time dislocators. They re- ported a 44% redislocation rate and an additional 19% of patients had patellofemoral pain or subluxation. Cash and Hughston 61 noted a 43% redislocation rate in a group of 69 patients with acute patellar dislocation and prior evidence of extensor mechanism abnormalities. In a sec- ond group of patients with acute dislocations, without predisposing patellofemoral problems, the redislocation rate was only 20%.
Many orthopedists are rethinking the traditional treat- ment for these patients. An emerging trend, similar to one used in those treating patients with first-time shoulder dislocations, is the decision to operatively stabilize acute, primary patellar dislocations. The recent biomechanical studies that highlighted the importance of the medial sta- bilizers, especially the MPFL, have directed attention to the repair of this structure.
In a study by Sanders et al, 91 which examined 14 pa- tients with transient acute patellar dislocations, findings at surgery showed disruption of the MPFL in 7 of 14 patients (50%), with stretching or partial tearing of the MPFL in the remaining 50%. Sargent and Teipner 73 reported no redis- locations in 11 patients with acute first-time dislocation who underwent primary repair of the medial patellar ret- inaculum to the medial margin of the patella. Boring and O'Donoghue 92 treated a similar pool of 17 patients with acute dislocation. No redislocations occurred after imme- diate medial retinacular reefing in 8 patients or after a
1 1 8 ELLIOTT AND DIDUCH

,a B
jY
~7~-- Medial
Fig 8. (A) The VMO muscle places a medially directed force on the patella because of its attachment location. (B) When the muscle is torn, its medial stabilizing force on the patella is disrupted.
distal realignment in 9 patients. These investigators be- lieved that a distal realignment procedure was more ap- propriate if the patient had an increased Q angle, patella alta, a shallow trochlear groove, or a history of patellar subluxation. Avikainen et al TM reported on 14 patients, 10 with primary dislocation and 4 with recurrent instability who underwent repair of the MPFL and augmentation with the adductor magnus tendon. A constant surgical finding in the patients with acute dislocation was detach- ment of the MPFL from the medial femoral epicondyle. Postoperatively, 12 of the 14 patients regarded their knees as good and 2 as fair. Sallay et a175 noted that 15 of 16 patients (94%) had tears of the MPFL off of the femur at surgical exploration after acute dislocation. After repair of the MPFL, none of the patients experienced redislocation. Ahmad et a176 reviewed 8 cases of acute patellofemoral dislocation treated surgically. All patients were noted to have a tear of the MPFL off the adductor tubercle as well as injury to the VMO origin from the adductor magnus tendon. The VMO muscle was retracted in an anterior and superior direction (Fig 8). All patients underwent arthro- scopic lateral release, then repair of the torn MPFL to the adductor tubercle and the VMO to the adductor magnus tendon. They addressed injuries to both the static (MPFL) and dyanamic (VMO) medial restraints. No patients expe- rienced a recurrent dislocation and the average patient satisfaction with the operation was 97%.
Nikku et a193 found less satisfying results with primary operative treatment. They performed a prospective, ran- domized study on 125 patients with primary patellofemo- ral dislocation. Fifty-five patients had closed treatment and 70 patients underwent surgery. Sixty-three of the patients had repair of the medial retinaculum, by suturing in 39 patients, by duplication in 18 patients and by addi- tional augmentation of the MPFL with the adductor mag- nus tendon in 6 patients. Of these 63 patients, 54 had a lateral release. Seven patients were treated only with lat- eral release. After a 2-year follow-up, the subjective results and function were better in the nonoperative group. Re-
current instability occurred in 20 patients treated nonop- eratively and in 18 treated operatively. The various patient profiles and techniques in these studies make a direct comparison between them difficult. In a patient who sus- tains an acute, first-time patellofemoral dislocation, treat- ment of the injured static (MPFL), and possibly dynamic (VMO) restraints appears promising. If predisposing patellofemoral risk factors are present, these need to be addressed as well to optimize the surgical results.
C O N C L U S I O N
There is no consensus as to the best method to treat the spectrum of patellofemoral instability. As a result, the literature is full of various nonoperative protocols and surgical procedures. It appears that most of these treat- ment methods are anecdotal, usually based on surgeon preference. Surgeons are now discovering more informa- tion about the pathoanatomy of patellofemoral instability. Injury to the medial static restraints, specifically the MPFL, may prove to be the "essential lesion" leading to recurrent patellofemoral instability, similar to the Bankart lesion seen in anterior shoulder instability. 94 As in the shoulder, other anatomic predisposing factors must be considered. By understanding the biomechanics of patellofemoral in- stability, the treating physician can develop a more scien- tific-based treatment algorithm that is specifically targeted to correct a patient's anatomy, including traumatic injury and predisposing malalignment.
R E F E R E N C E S
1. Wiberg G: Roentgenographic and anatomic studies on the patel- lofemoral joint. With special reference to chondromalacia patella. Acta Orthop Scand 12:319-410, 1941
2. Baumgartl F: Das Kniegetenk. Berlin, Germany, Springer-Verlag, 1944 3. Reider B, Marshall JL, Koslin B, et al: The anterior aspect of the knee
joint an anatomical study. J Bone Joint Surg Am 63:351-356, 1981 4. Dejour H, Walch G, Nove-Josserand L, et al: Factors of patellar
instability: An anatomic radiologic study. Knee Surg Sports Trauma- tol Arthrosc 2:19-26, 1994
BIOMECHANICS OF PATELLOFEMORAL INSTABILITY "1 1 9

5. Dandy DJ: Chronic patellofemoral instability. J Bone Joint Surg Br 78:328-335, 1996
6. Aglietti P, Buzzi R, Insall JN: Disorders of the patellofemoral joint, in Insall JN (ed): Surgery of the Knee (ed 2). New York, NY, Churchill Livingstone, 1993, pp 241-385
7. Staubli HU, Durrenmatt U, Porcellini B, et al: Anatomy and surface geometry of the patellofemoral joint in the axial plane. J Bone Joint Surg Br 81:452-458, 1999
8. Lancourt JE, Christini JA: Patella alta and patella infera. Their etio- logical role in patellar dislocation, chondromalacia, and apophysitis of the tibial tubercle. J Bone Joint Surg Am 57:1112-1115, 1975
9. Hautamaa PV, Fithian DC, Kaufman KR, et ah Medial soft tissue restraints in lateral patellar instability and repair. Clin Orthop 349: 174-182, 1998
10. Cofield RH, Bryan RS: Acute dislocation of the patella: Results of conservative treatment. J Trauma 17:526-531, 1977
11. Conlan T, Garth WP, Lemons JE: Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am 75:682-693, 1993
12. Insall JN, Aglietti P, Tria AJ: Patellar pain and incongruence. II: Clinical application. Clin Orthop 176:225-232, 1983
13. Desio SM, Burks RT, Bachus KN: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 26:59-65, 1998
14. Fulkerson JP, Grossling HR: Anatomy of the knee joint lateral reti- naculum. Clin Orthop 153:183-188, 1980
15. Kaplan EB: Some aspects of the functional anatomy of the human knee joint. Clin Orthop 23:18-29, 1962
16. Luo ZP, Sakai N, Rand JA, et ah Tensile stress of the lateral patel- lofemoral ligament during knee motion. Am J Knee Surg 10:139-144, 1997
17. Heegaard J, Leyvraz P, Kampen AV, et ah Influence of soft structures on patellar three-dimensional tracking. Clin Orthop 299:235-243, 1994
18. Reider B, Marshall JL, Ring B: Patellar tracking. Clin Orthop 157:143- 148, 1981
19. Lieb FJ, Perry J: Quadriceps function: An anatomical and mechanical study using amputated limbs. J Bone Joint Surg Am 50:1535-1548, 1968
20. Goh JC, Lee PY, Bose K: A cadaver study of the function of the oblique part of vastus medialis. J Bone Joint Surg Br 77:225-231, 1995
21. Henry JH, Craven PR: Surgical treatment of patellar instability: In- dications and results. Am J Sports Med 9:82-85, 1981
22. Hughston JC (ed): Knee Ligaments Injury and Repair. St Louis, MO, Mosby Year Book, 1993, pp 81-119
23. Raimondo RA, Ahmad CS, Blankevoort LB, et ah Patellar stabiliza- tion: A quantitative evaluation of the vastus medialis obliquus mus- cle. Orthopedics 21:791-795, 1998
24. Bassett FH: Acute dislocation of the patella, osteochondral fractures, and injuries to the extensor mechanism of the knee, in The American Academy of Orthopaedic Surgeons (eds): Instructional Course Lec- tures. St Louis, MO, Mosby, 1976, pp 40-49
25. Bose K, Kanagasuntheram R, Osman MB: Vastus medialis oblique: An anatomic and physiologic study. Orthopedics 3:880-883, 1980
26. Hallisey M, Doherty N, Bennet W, et ah Anatomy of the junction of the vastus lateralis tendon and the patella. J Bone Joint Surg Am 69:545-549, 1987
27. Hungerford DS, Barry M: Biomechanics of the patellofemoral joint. Clin Orthop 144:9-15, 1979
28. Aglietti P, Insall JN, Cerulli G: Patellar pain and incongruence. I. Measurements of incongruence. Clin Orthop 176:217-224, 1983
29. Post WR, Fulkerson JP: Distal realignment of the patellofemoral joint. Indications, effects, results, and recommendations. Orthop Clin North Am 23:631-643, 1992
30. Hehne H: Biomechanics of the patellofemoral joint and its clinical relevance. Clin Orthop 258:73-85, 1990
31. Kettelkamp DB: Management of patellar malalignment J Bone Joint Surg Am 63:1344-1348, 1981
32. Larson RL: Subluxation-dislocation of the patella, In the injured ado- lescent knee. Baltimore, MD, Lippincott, 1979, pp 161-204
33. Baker RH, Carroll N, Dewar FP, et ah The semitendinosus tenodesis for recurrent dislocation of the patella. J Bone Joint Surg Br 54:103- 109, 1972
54. Hughston JC: Subluxation of the patella. J Bone Joint Surg Am 50:1003-1026, 1968
35. Smillie IS (ed): Injuries of the Knee Joint. Edinburgh, UK, Living- stone, 1970, pp 182-223
36. Hughston JC, Walsh WM: Proximal and distal reconstruction of the extensor mechanism for patellar subluxation. Clin Orthop 144:36-42, 1979
37, Anderson PT: Congenital deformities of the knee joint in dislocation of the patella and achondroplasia. Acta Orthop Scand 28:27, 1958
38. Harrison MHM: The results of a realignment operation for recurrent dislocation of the patella. Clin Orthop 18:96, 1960
39. Jones JB, Francis KC, Mahoney JR: Recurrent dislocating patella. Clin Orthop 20:230, 1961
40. Leach R: Malalignment syndromes of the patella. Surgery of the Patellofemoral Joint. American Academy of Orthopaedic Surgeons, Instr Course Lect 26:49, 1976
41. West FE, Soto-Hall R: Recurrent dislocation of the patella in the adult. J Bone Joint Surg Am 40:386, 1958
42. Wiberg G: Roentgenographic and anatomic studies on the patel- lofemoral joint. With special reference to chondromalacia patella. Acta Orthop Scand 12:319-410, 1941
43. Brattstrom H: Shape of the intercondylar groove normally and in recurrent dislocation of the patella. Acta Orthop Scand 1964 (suppl 68)
44. Hauser EDW: Total tendon transplant for slipping patella. Surg Gynecol Obstet 66:199-214, 1938
45. Hughston JC, Stone MM: Recurrent dislocation of the patella in athletes. South Med J 57:623-628, 1964
46. McKeever D: Recurrent dislocation of the patella. Clin Orthop 3:55, 1954
47. Merchant AC, Mercer RL: Lateral release of the patella. A prelimi- nary report. Clin Orthop 103:40-45, 1974
48. Southwick WO, Becker GE, Albright JA: Dovetail patellar tendon transfer for recurrent dislocating patella. JAMA 203:665-669, 1968
49. Teal F: Treatment of dislocation of the patella. Clin Orthop 3:61, 1954 50. Grelsamer RP: Patellar malalignment. J Bone Joint Surg Am 82:1639-
1650, 2000 51. Fulkerson JP, Shea KP: Disorders of patellofemoral alignment. J Bone
Joint Surg Am 72:1424-1429, 1990 52. Kasman GS, Cram JR, Wolf SL (eds): Clinical applications in surface
electromyography: Chronic musculoskeletal pain. Gaithersburg, MD, Aspen, 1998, p 347
53. Witvrouw E, Sneyers C, Lysens R, et ah Reflex response times of vastus medialis oblique and vastus lateralis in normal subjects and subjects with patellofemoral pain syndrome. J Orthop and Sports Phys Ther 24:160-165, 1996
54. Fulkerson JP: Patellofemoral pain disorders: Evaluation and manage- ment. J Acad Orthop Surg 2:124-132, 1994
55. McConnell JS: The management of chondromalacia patellae. A long term solution. Austr J Physiother 32:215-223, 1986
56. Kowall MG, Kolk G, Nuber GW, et ah Patellar taping in the treatment of patellofemoral pain. Am J Sports Med 24:61-66, 1996
57. Grelsamer RP, McConnell J (eds): The patella: A team approach. Gaithersburg, MD, Aspen, 1998
58. Pedowitz WJ, Kovatis P: Flatfoot in the adult. J Am Acad Orthop Surg 3:293-302, 1995
59. Boden BP, Pearsall AW, Garrett WE, et ah Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 5:47-57, 1997
60. Hawkins RJ, Bell RH, Anisette G: Acute patellar dislocations. The natural history. Am J Sports Med 14:117-120, 1986
61. Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 16:244-249, 1988
62. Dandy DJ, Griffiths D: Lateral release for recurrent dislocation of the patella. J Bone Joint Surg Br 71:121-125, 1989
63. Henry JH, Goletz TH, Wllliamson B: Lateral retinacular release in patellofemoral subluxation. Indications, results, and comparison to open patellofemoral reconstruction. Am J Sports Med 14:121-129, 1986
64. Kolowich PA, Paulos LE, Rosenberg TD, et ah Lateral release of the patella: Indications and contraindications. Am J Sports Med 18:359- 365, 1990
65. Marumoto JM, Jordan C, Akins R: A biomechanical comparison of lateral retinacular releases. Am J Sports Med 23:151-155, 1995
66. O'Neill DB: Open lateral retinacular lengthening compared with arthroscopic release. A prospective, randomized outcome study. J Bone Joint Surg Am 79:1759-1769, 1997
120 ELLIOTT AND DIDUCH

67. Hughston JC, Walsh WM, Puddu G: Patellar subluxation and dislo- cation. Saunders Monographs in Clinical Orthopaedics (vol 5). Phil- adelphia, PA, Saunders, 1984, pp 84-128
68. Insall J, Bullough PG, Burstein AH: Proximal "tube" realignment of the patella for chondromalacia patellae. Clin Orthop 144:63-69, 1979
69. Zeichen J, Lobenhoffer P, Gerich T, et al: Medium-term results of the operative treatment of recurrent patellar dislocation by Insall proxi- mal realignment. Knee Surg Sports Traumatol Arthrosc 7:173-176, 1999
70. McCauley TR, Kier R, Lynch KJ, et al: Chondromalacia patellae: Diagnosis with MR imaging. Am J Roentgenol 158:101-105, 1992
71. Gomes JL: Medial patellofemoral ligament reconstruction for recur- rent dislocation of the patella: A preliminary report. Arthroscopy 8:335-340, 1992
72. Fithian DC, Meier SW: The case for advancement and repair of the medial patellofemoral ligament in patients with recurrent patellar instability. Op Tech Sports Med 7:81-89, 1999
73. Sargent J, Teipner WA: Medial patellar retinacular repair for acute and recurrent dislocation of the patella. A preliminary report, J Bone Joint Surg Am 53:386, 1971
74. Avikainen VJ, Nikku K, Seppanen-Lehmonen TK: Adductor magnus tenodesis for patellar dislocation. Clin Orthop 297:12-16, 1993
75. Sallay PI, Poggi J, Speer KP, et ah Acute dislocation of the patella. A correlative pathoanatomic study. Am J Sports Med 24:52-60, 1996
76. Ahmad CS, Stein BES, Matuz D, et al: Immediate surgical repair of the medial patelIar stabilizers for acute patellar dislocation. Am J Sports Med 28:804-810, 2000
77. Muneta T, Sekiya I, Tsuchiya M, et al: A technique for reconstruction of the medial patellofemoral ligament. Clin Orthop 359:151-155, 1999
78. Scuderi GR: Surgical treatment for patellar instability. Clin Orthop 23:619-630, 1992
79. Roux C: The classic. Recurrent dislocation of the patella: Operative treatment. Clin Orthop 144:4-8, 1979
80. Goldthwait JE: Slipping or recurrent dislocation of the patella. With the report of eleven cases. Boston Med Surg J 150:169-174, 1904
81. Cox JS: Evaluation of the Roux-Elmslie-Trillat procedure for knee extensor realignment. Am J Sports Med 10:303-310, 1982
82. Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a
subluxation-type patellar malalignment. Am J Sports Med 25:375- 381, 1997
83. Eulkerson JP: Anterornedialization of the tibial tuberosity for patel- lofemoral malalignment. Clin Orthop 177:176-181, 1983
84. Stetson WB, Friedman MJ, Fulkerson JP, et al: Fracture of the prox- imal tibia with immediate weightbearing after a Fulkerson osteot- omy. Am J Sports Med 25:570-574, 1997
85. Hampson WGJ, Hill P: Late results of transfer of the tibial tubercle for recurrent dislocation of the patella. J Bone Joint Surg Br 57:209-213, 1975
86. Kolowich PA, Paulos LE, Rosenberg TD, et al: Lateral release of the patella: Indications and contraindications. Am J Sports Med 18:359- 365, 1990
87. Huberti HH, Hayes WC: Contact pressures in chondromalacia patel- lae and the effects of capsular reconstructive procedures. J Orthop Res 6:499-508, 1988
88. Scuderi GR: Extensor mechanism injuries: Treatment, in Scott WiN (ed): Ligament and Extensor Mechanism Injuries of the Knee: Diag- nosis and Treatment. St Louis, MO, Mosby Year Book, 1991, pp 183-193
89. Hughston JC, Deese M: Medial subluxation of the patella as a com- plication of lateral retinacular release. Am J Sports Med 16:383-388, 1988
90. Maenpaa H, Lehto MUK: Patellar dislocation. The long-term results of nonoperative management in 100 patients. Am J Sports Med 25:213-217, 1997
91. Sanders TG, Morrison WB, Singleton BA, et al: Medial patellofemoral ligament injury following acute transient dislocation of the patella: MR findings with surgical correlation in 14 patients. Original work out of Wilford Hall Medical Center, presented at RSNA 1999 (un- published material)
92. Boring TH, O'Donoghue DH: Acute patellar dislocation: Results of immediate surgical repair. Clin Orthop 136:182-185, 1978
93. Nikku R, Nietosvaara Y, Kallio PE, et al: Operative versus closed treatment of primary dislocation of the patella. Similar 2-year results in 125 randomized patients. Acta Orthop Scand 68:419-423, 1997
94. Bankart A: The pathology and treatment of recurrent dislcation of the shoulder-joint. Br 26:23-29, 1938
BIOMECHANICS OF PATELLOFEMORAL INSTABILITY 121