Embed Size (px)
DESCRIPTION
Back to Basics, 2012 POPULATION HEALTH : Health Care Organization. Presented by Doug Coyle Epidemiology & Community Medicine. MCC Objectives: Population health 78-4 Administration of effective health programs at the population level. Rationale: - PowerPoint PPT Presentation
Citation preview

March 23rd 2012 1
Back to Basics, 2012POPULATION HEALTH : Health Care Organization
Presented by Doug Coyle
Epidemiology & Community Medicine

2
MCC Objectives: Population health 78-4 Administration of effective
health programs at the population levelRationale: • Knowing the organization of the health care
and public health systems in Canada as well as how to determine the most cost-effective interventions are becoming key elements of clinical practice. Physicians also must work well in multidisciplinary teams within the current system in order to achieve the maximum health benefit for all patients and residents.

3
MCC Objectives: Population health 78-4 Administration of effective
health programs at the population levelTerminal objectives: • Know and understand the pertinent history,
structure and operations of the Canadian health care system.
• Be familiar with economic evaluations such as cost-benefit / cost effectiveness analyses as well as issues involved with resource allocation.
• Describe the approaches to assessing quality of care and methods of quality improvement.

4
MCC Objectives: Population health 78-4 Administration of effective
health programs at the population levelEnabling objectives (1)• Describe at a basic level:
– methods of regulation of the health professions and health care institutions;– supply, distribution and projections of health human resources; – health resource allocation; – organization of the Public Health system; and – the role of complementary delivery systems such as voluntary organizations
and community health centres.• Describe the role of regulated and non-regulated health care providers and
demonstrate how to work effectively with them. • Outline the principles of and approaches to cost containment and economic
evaluation.• Describe the main functions of public health related to population health
assessment, health surveillance, disease and injury prevention, health promotion and health protection.
• Demonstrate an understanding of ethical issues involved in resource allocation.

5
MCC Objectives: Population health 78-4 Administration of effective
health programs at the population levelEnabling objectives (2)• Define the concepts of efficacy, effectiveness, efficiency,
coverage and compliance and discuss their relationship to the overall effectiveness of a population health program.
• Be able to recognize the need to adjust programs in order to meet the needs of special populations such as new immigrants or persons at increased risk.
• Participate effectively in and with health organizations, ranging from individual clinical practices to provincial organizations, exerting a positive influence on clinical practice and policy-making.
• Define quality improvement and related terms: quality assurance, quality control, continuous quality improvement, quality management, total quality management; audit.
• Describe and understand the multiple dimensions of quality in health care, i.e. what can and should be improved.

6
What Will We Cover?
• Organization of Health Care Delivery in Canada
• Elements of Health Economics

1867 British North America Act Provincial gov. given regulatory power over hospitals, asylums etc.
1914-1917 Saskatchewan Moves towards paying retainers for physicians and the right to collect taxes to finance health care
1920 Creation of Federal Department of Health • Response to Spanish flu epidemic • Focus on public health, child health food and drug standards
1935 Provinces stop Federal gov. plan to provide social and health benefits
1947 Saskatchewan Introduces public insurance for hospital services
1957 Federal Hospital Insurance and Diagnostic Services Act (HIDS)
Provinces given 50% of funding from Federal gov to provide a service which is:
Publicly administered, comprehensive, universal, portable and accessible.
1961 All provinces participate in HIDS
1966 Medical Care Act Universal coverage for physician services
1977 Federal-Provincial Fiscal Arrangements and Established Programs Financing Act (EPFA)
Reduced requirements of federal government to match funding
1984 Canada Health Act
7
Historical Progression in the Organization of Health Care

April 11, 2011 8
Events Post 1984
• 2001: Kirby & Romanow commissions– Attempts to reform the health care system– Focus on long term sustainability
• 2005: Chaoulli decision (Quebec)– Controversial interpretation of the CHA in regards to banning of
private clinics.
• 2012 Drummond report (Ontario)– Emphasis on home care

9
Canada Health Act PrinciplesPublic administration Administered for non profit and
accountable to a provincial government
Comprehensive All medical necessary services provided by hospitals, medical practitioners
Universal All insured persons have equal coverage
Accessible Reasonable access without financial and other barriers
Portable Coverage between provinces

10
Problems with the Canada Health Act
• Only partial coverage– Physician services in and out of hospital only– What is “medically necessary”– Only those “provided by hospitals”– Not all hospitals must provide all services
• Does not legislate which services must be provided– Only that federal government will not provide funding
if conditions not met• Impact of other legislation
– Canadian Charter of Rights and Freedom

11
Ways of organizing a system
• Publicly financed and provided– UK (?), Scandinavia
• Insurance based system for all– Tax based - Canada – Compulsory premiums - Japan
• Insurance based system for some– US– Wouldn’t meet requirements of Canada Health Act
• Purely private– Mainly underdeveloped countries– Wouldn’t meet requirements of Canada Health Act

12
Some Data
• 2010: total health care expenditures were $5,614/person or about $192billion, 11.7% of GDP down from 2009 (SIM web link)
• 70% from public sector (45% in the USA)• 29% spent on hospitals, 18% on drugs, 14%
on MDs• Research shows that private-for-profit care
is more expensive (and potentially less effective)

13
Methods of paying doctors (SIM web link)
• Fee-for-service: unit is services. Incentive to provide many services, especially procedures.
• Capitation: unit is patient. Fixed payment per patient. Incentive to keep people healthy, but not to make yourself accessible.
• Salary: unit is time. Productivity depends on professionalism and institutional controls– Practice plans
• Combinations of above, e.g., "blended funding“– Family health networks (Ontario)

14
Methods for paying hospitals
• Line-by-line: separate payments for staff, supplies, etc. Cumbersome, rigid.
• Global budget: fixed payment to be used as hospital sees fit. Fails to recognize differences in case mix.
• Case-Mix weighted: payment for total cost of episode, greater for more complicated cases. Now used in Canada.
• New technology: OHTAC reviews requests. If approved, government pays. If declined, hospitals can pay for it from core budget.

ORGANIZATIONS
15

April 11, 2011 16
CMPA
• “The role of the CMPA as a medical defence association representing the interests of individual physicians.”
• Canadian Medical Protective Association is a co-operative, replacing commercial malpractice insurance. It advises physicians on threatened litigation (talk to them early), and pays legal fees and court settlements. Fees vary by region and specialty ($792-$39,828/year).

Local Health Integration Networks (LHINs)
• Champlain LHIN– Covers Renfrew, Lanark, Ottawa, Eastern Ontario – Funds 21 hospitals, 7 community health centres, 61
long-term care homes, the Champlain Community Care Access Centre, and more than 100 Community Support Services including mental health and addictions agencies
– Covers approximately 1.1 million people or 9 per cent the population of Ontario
April 11, 2011 17

18
Physician Organizations (1)
• Medical Council of Canada– Maintains the Canadian Medical Registry– Does not grant licence to practice medicine
• College of Physicians and Surgeons of Ontario– Responsible for issuing license to practice medicine– Handles public complaints, professional discipline, etc.– Does not engage in lobbying on matters such as
salaries, working conditions.

19
Physician Organizations (2)
• Royal College of Physicians and Surgeons of Canada.– Maintains standards for post-graduate training through-
out Canada.– Sets exams and issues fellowships for specialty training
• Ontario Medical Association– Professional association; lobbies on behalf of
physicians re: fees, working conditions, etc.
• College of Family Physicians of Canada– Organization certifying/promoting family practice

20
Public Health Units/Medical Officer of Health
• Reports to municipal government.• Responsible for:
– Food/lodging sanitation– Infectious disease control and immunization– Health promotion, etc.– Family health programmes
• E.g. family planning, pre-natal and pre-school care, tobacco prevention, nutrition
– Occupational and environmental health surveillance.

21
Public Health Units/Medical Officer of Health (2)
• Powers include ordering people, due to a public health hazard, to take any of these actions:– Vacate home or close business– Regulate or prohibit sale, manufacture, etc. of
any item– Isolate people with communicable disease– Require people to be treated by MD– Require people to give blood samples

22
Coroner
• Notify coroner of deaths in the following cases:– Due to violence, negligence, misconduct, etc.– During work at a construction or mining site.– During pregnancy– Sudden/unexpected– Due to disease not treated by qualified MD– Any cause other than disease– Under suspicious circumstance or by ‘unfair means’– Deaths in jails, foster homes, nursing homes, etc.

DECISION MAKING
23

24
Role of Federal Government
• General responsibility for international health, public health, aboriginal health, etc.
• Funding: has the greatest taxing power• Its provision of funding allows it to enforce
the Canada Health Act, despite its lack of constitutional authority...
• Reductions in federal contributions have reduced its influence

25
Role of Provincial Governments
• Responsibility for health (and most other expensive services) lies with the provinces
• Provinces provide most of the funding for health services
• Therefore, they are the main decision-makers: hospitals, public health, etc.

26
Decision Making in Ontario (1)
• Province decides– Which drugs funded through ODB– Block budgets to LHINs– Special payments for technologies– Physician fees– Other services covered

27
Decision Making in Ontario (2)
• Drugs – Ontario covers prescriptions for approx 20% of
population• Welfare recipients• Over 65
– Decision on what drugs to fund influenced by Committee to Evaluate Drugs• Based on level of evidence• Cost effectiveness

28
Major Decision Making Committees (Ontario)
• Ontario Health Technology Advisory Committee– Health technology funding to hospitals etc.
• Committee to Evaluate Drugs/ Canadian Expert Drug Advisory Committee– Drug funding through OPDP
• Joint Oncology Drug Review– Cancer drug funding

29
Decision Making in Ontario (3)
• Role of LHINs• 14 in number, replacing DHCs, regional
offices of Ministry of Health & Long-term Care
• Plan, coordinate, integrate and partially manage care at the local level
• Members are appointed

30
Decision Making in Ontario (4)
• Politics– Many decisions are politically motivated not
necessarily evidence based or efficient• HPV vaccine• Newborn screening• Preoperative use of EPO

31
78.1: MEDICAL ECONOMICS (1)
• Define the socio-economic rationales, implications and consequences of medical care– Medical care has impact on costs to society;
both financial and other (non monetary) resources.
– This objective aims to raise awareness of these types of issues.

32
MEDICAL ECONOMICS (2)
• Does effective medical care reduce health care spending?
• How do we value non-fiscal benefits such as quality of life, ‘health’, not being dead?
• Should resources be spent on health or other societal objectives?
• How do we value non-traditional expenditures, etc which impact on health (Healthy Public Policy).


34
Year

35

36
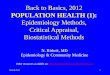
Source: CIHI, National Health Expenditure Trends, 1975 to 2009
19751977
19791981
19831985
19871989
19911993
19951997
19992001
20032005
20072009
0
10
20
30
40
50
60
70
80
90
100
Distribution of Total Health Expenditure by Use of Funds,Canada, 1975 to 2009
Prescribed DrugsOtherPublic HealthOther professionalsAdministrationCapitalNon-prescribed drugsOther institutionsPhysiciansHospitals*
Perc
ent o
f tot
al e
xpen
ditu
re
* Hospital spending includes salaries of professionals other than physicians

37
Source: CIHI 2010

38
Principles of cost-containment
• Three approaches to improve cost effectiveness of health care delivery– Eliminate ineffective care– Reduce costs of effective care
• Substitute cheaper but equally effective care,– day surgery for hospital admission, – nurse practitioners for some primary care, – generic drugs
• Reduce unit costs– reduce salaries (risk of reduced effectiveness) or fees (but quantity
provided may increase)
– Adopt only new interventions that are cost effective

Assessing Cost Effectiveness
39

40
Types of economic analysis (SIM web link)
Form of Analysis Measurement of Costs
Measurement of Benefit
Synthesis of Costs and Benefits
Cost Minimization Analysis
Dollars None Incremental cost
Cost Effectiveness Analysis
Dollars Single dimension of effectiveness (e.g. life years gained)
Incremental cost effectiveness : incremental cost per unit gained
Cost Utility Analysis
Dollars Utility gained (e.g. QALYs - quality adjusted life years)
Incremental cost-effectiveness: incremental cost per QALY gained
Cost Benefit Analysis
Dollars Monetary value of benefits gained
Net benefit gained

Economic Evaluation Example
Coyle D, Coyle K, Bettinger JS, Halperin SA, Vaudry W, Scheifele DW, Le Saux N. Cost effectiveness of infant vaccination for rotavirus in Canada. CJIDDM (In press)

Acknowledgements
• The economic analysis was funded by a grant from the Public Health Agency of Canada to the Canadian Paediatric Society.

Methods• Analysis was conducted through a Markov model which
follows a cohort of children each month from birth to 5 years.
• Analysis uses pertinent data on the natural history of rotavirus and the effects of vaccination.
• Estimates of heath care costs for children requiring hospitalizations and Emergency Department visits were derived from the IMPACT surveillance and emergency department studies and other Canadian studies.
• The model estimates the effect of vaccination on costs and quality adjusted life years (QALYs).

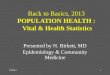
Schematic of Model
No infection
Infection Previous infection
Dead

Data Inputs (1)• Monthly probability of primary RV infection
• Probability of death from RV per case of RV
• Relative risk reduction for secondary infection versus primary infection
• Monthly probability of death from other causes
• Distribution of RV infections without vaccination– Not requiring medical management, GP visit, ED visit,
Hospitalization

Data Inputs (2)• Vaccine Efficacy
– Meta analysis
• Vaccine uptake
• Utility Values– Child and caregiver with and without rotavirus
• Vaccine Costs
• Costs of Rotavirus cases– Hospitalization, Emergency dept. visit, GP visit

Unvaccinated Population

Vaccinated Population

Cost Effectiveness of Infant Vaccination for Rotavirus
No vaccination
Vaccination with Rotateq
Vaccination with Rotarix
Costs
Health Care System $69.29 $206.85 $199.41
Societal Perspective $351.89 $321.99 $304.28
QALYs 4.352 4.353 4.353
Incremental cost per QALY gained versus no vaccination
Health Care System $122,000 $108,000
Societal Perspective Dominant Dominant

Conclusions
• From a societal perspective, a universal vaccination program against rotavirus will be both cost saving and more effective than no vaccination assuming there are limited additional costs of administration.
• From a health care system perspective, a program would not be considered cost effective at current vaccine costs– Reducing the costs of the vaccine by 50% would make
vaccination cost effective

Impact
• Based on the results of the analysis and a negotiated lower price:– Ontario MOHLTC covers RotarixTM
• Publicly Funded Immunization Schedules for Ontario to protect infants against diarrhea and vomiting caused by rotavirus infection.
– BC covers Rotarix

52
Health System
Multiple Choice Questions
For discussion

53
In 2006, which country spent the least on health care as a percentage of GDP (gross domestic product):a) Canada
b) France
c) Sweden
d) UK
e) USA


55
The component of Canada's health care system that receives the highest percentage of the health care budget is:a) hospitals
b) physician fees
c) pharmaceuticals
d) laboratory services
e) administration


57
Regarding health expenditure and health outcomes:a) the U.S. has the greatest health expenditure and
the lowest infant mortality rates
b) there is a positive association between national expenditure on health and GDP
c) increased national health expenditure always increases health status of a country
d) all of the above
e) none of the above

58

59
Deaths/1000 live births1 Singapore 2.312 Bermuda 2.463 Sweden 2.754 Japan 2.795 Hong Kong 2.926 Macau 3.227 Iceland 3.238 France 3.339 Finland 3.47
10 Anguilla 3.5211 Norway 3.5815 Germany 3.9922 Denmark 4.3432 United Kingdom 4.8533 New Zealand 4.9236 Canada 5.0442 Italy 5.5145 United States 6.26

60
All of the following are responsibilities of local public health units in Canada EXCEPT:a) communicable disease control
b) health education
c) investigation of sudden death
d) immunization
e) health promotion

61
Which of the following is not one of the five Terms and Conditions of Medicare?a) portability
b) flexibility
c) universality
d) comprehensive coverage
e) accessibility

62
More MCQs
• Here are some more questions that students can use to test their own knowledge:
http://www.medicine.uottawa.ca/sim/data/Self-test_Qs_HC_System_e.htm
• (The questions contain comments on the
answers, to illustrate why a given response is not correct)