Embed Size (px)
DESCRIPTION
78-6 ENVIRONMENT (1) Objectives: - Identify common environmental hazards and be able to classify them into the appropriate category of chemical, biological, physical and radiation. - Identify the common hazards that are found in air, water, soil and foods. 3Mach 2012
Citation preview

Back to Basics, 2012 POPULATION HEALTH:
Environmental & Occupational Health
B. Pinard, MD (PGY5)G. Dunkley, MD
Epidemiology & Community Medicine
Based on slides prepared by Dr. R. Spasoff and Dr. N. Birkett
1March 2012

MCC Objectives: Population health 78-6 Environment
Rationale: • Environmental issues are important in medical practice because exposures may be causally linked to a patient's clinical
presentation and the health of the exposed population. A physician is expected to work with regulatory agencies to help implement the necessary interventions to prevent future illness. Physician involvement is important in the promotion of global environmental health.
Terminal Objectives: • Recognize the implications of environmental hazards at both the individual and population level. • Respond to the patients concerns through appropriate information gathering and treatment. • Work collaboratively with local, provincial and national agencies/governments as appropriate to address the concerns
at a population level. • Make appropriate recommendations for patients and exposed populations so as to minimize their health risks and
maximize their overall function. Enabling objectives• Identify common environmental hazards and be able to classify them into the appropriate category of chemical,
biological, physical and radiation.• Identify the common hazards that are found in air, water, soil and foods. • Describe the steps in an environmental risk assessment and be able to critically review a simple risk assessment for a
community.• Conduct a focussed clinical assessment of exposed persons in order to determine the causal linkage between exposure
and the clinical condition. • Be aware of local, regional, provincial and national regulatory agencies that can assist in the investigation of
environmental concerns. • Describe simple interventions that will be effective in reducing environmental exposures and risk of disease (e.g.
sunscreen for sunburns, bug spray for prevention of West Nile Virus infection). • Communicate simple environmental risk assessment information to both patients and the community.
April 2011 2March 2012

78-6 ENVIRONMENT (1)
• Objectives: - Identify common environmental hazards and
be able to classify them into the appropriate category of chemical, biological, physical and radiation.
- Identify the common hazards that are found in air, water, soil and foods.
3Mach 2012

78-6 ENVIRONMENT (2)
• Environmental exposure: – Natural and human-made environment– Reservoirs: air, water, soil, food – Route: inhalation, ingestion, absorption– Exposure setting: • Workplace: occupational health (high level exposure,
acute or chronic)• Outside workplace : environmental health (low level
exposure, chronic)
April 2011 4March 2012

78-6 ENVIRONMENT (3)• AIR– Physical contaminants• Radiation: Radon (lung cancer), UV (skin cancer)• Sound waves (hearing loss)
– Chemical contaminants• Ozone at ground level (worsens asthma)• Carbon monoxide (asphyxiation)• Sulphur dioxide; nitrogen oxides (exacerbation of
breathing problems)• Organic compounds: Benzene (carcinogen – leukemia)• Second hand tobacco smoke (lung cancer)• Heavy metals; industrial emissions (specific syndromes)
April 2011 5March 2012

78-6 ENVIRONMENT (4)
• AIR:– Biological contaminants: • Bacteria: Legionella (pneumonia)• Dust mites (upper and lower-airway sx)• Pollen (upper and lower-airway sx)• Moulds (allergies)• Particulates (pollen, spores, aerosols) (asthma)
– Global warming: • Extreme weather (heat waves), change in distribution
of vectors of disease, crop failures, etc.
April 2011 6March 2012

78-6 ENVIRONMENT (5)• WATER
– Biological agents:• Bacteria : E. coli, Salmonella, Pseudomonas• Protozoa (cysts): Giardia, Cryptosporidium (GI symtoms mainly)• Blue green algae (skin irritation, GI symptoms)• Higher risk: aboriginal Canadians, rural population
– Chemical agents:• Volatile organic compounds (VOC), pesticides, heavy metals, other
waste from industries (effects depend on contaminant)• Chlorination by-products - trihalomethanes (THM) (cancer)
• SOIL– Chemical agents:
• Pesticides, petroleum hydrocarbons, solvents, motor oil, lead (effects depend on contaminant)
• Higher risk: infants/toddlers– Biological agents:
• Bacteria (tetanus)
April 2011 7March 2012

78-6 ENVIRONMENT (6)• FOOD
– Biological Contaminants• Salmonella- raw eggs, poultry, meat (GI sx)• Campylobacter - raw poultry and milk (GI sx, joint pain)• E. Coli - hamburger meat (diarrhea, HUS)• Listeria monocytogenes (listeriosis)• Clostridium botulinum (botulism)• Mould toxin (aflatoxin), BSE, virus, parasites
– Chemical Contaminants• PCBs, dioxins/furans, pesticide residues (DDT), mercury• Food additives: nitrites, sulfites (allergy) • Drugs given to livestock: antibiotics, hormones
April 2011 8March 2012

78-6 ENVIRONMENT (7)• Objective: - Describe the steps in an environmental risk
assessment and be able to critically review a simple risk assessment for a community.
• Risk assessment: – Process of evaluating the likelihood of occurrence and
probable severity of health effects due to a hazard– Done by: Occupational health agencies,
Environmental protection agencies , Public health authorities, Clinicians
April 2011 9March 2012

78-6 ENVIRONMENT (8)
• Steps in risk assessment: 1. Hazard identification: Is an environmental hazard
involved? What is it?2. Risk characterization: Is the hazard likely to cause
these types of symptoms in this type of patient?3. Exposure assessment: Is the patient’s exposure
enough to cause these symptoms?4. Risk estimation: How much has the hazard
contributed to the patient’s condition?Source: Primer in Population Health
April 2011 10March 2012

78-6 ENVIRONMENT (9)
• Hazard Identification: – Agent (based on clinical history – see later on)– Adverse effect– Target population– Condition of exposure
• Risk characterisation: – Describe the potential health effects of hazard – Sources of info: scientific literature, toxicology or
poison center, public health department
April 2011 11March 2012

78-6 ENVIRONMENT (10)
• Workplace Hazardous Material Information System (WHMIS):– Labeling requirements for hazards – Indicates availability of Materials Safety Data
Sheets (MSDS): more details on hazard, how to handle it, what to do if emergency
– MSDS are available on the web – should find one site and bookmark it (Health Canada: http://www.hc-sc.gc.ca/ewh-semt/occup-travail/whmis-simdut/index-eng.php)
April 2011 12March 2012

78-6 ENVIRONMENT (11)
• Exposure assessment: – Characterize exposure of individual or population– Can be measured directly at times in people (ex:
blood lead level) or in environment– Estimated most of the time (from history or
inspection of environment)– Consultants: environmental medicine specialists,
toxicologists, industrial/occupational hygienists• Risk estimation– Probability of being affected and severity of effect
April 2011 13March 2012

78-6 ENVIRONMENT (12)
• Objective: - Conduct a focussed clinical assessment of
exposed persons in order to determine the causal linkage between exposure and the clinical condition.
• Clues to environmental causes• Detailed environmental history
April 2011 14March 2012

78-6 ENVIRONMENT (13)
• Clues that illness is caused by environmental factors: – Patient suspects it– Pattern of illness atypical (absence of usual risk
factors, unusual age group, course of illness unusual, no response to tx)
– Temporal pattern of illness (weekends/weekdays, holidays/home)
– No obvious other cause– Signs/symptoms suggest specific toxins
April 2011 15March 2012

78-6 ENVIRONMENT (14)Environmental history - CH20PD2: • Community: neighborhood sources of hazard; industry, waste
storage• Home: year of construction, renovations; materials used in
construction and decoration; moulds; garden and house plants; use of cleaning products, pesticides, herbicides
• Hobbies and leisure: exposure to chemicals, dusts, or micro-organisms
• Occupation: current and previous occupations; work with known hazards; air quality
• Personal habits: hygiene products; smoking• Diet: sources of food and water; cooking methods; food fads• Drugs: prescription, non-prescription, and alternative medications;
health practices
April 2011 16
Source: Primer in Population Health
March 2012

78-6 ENVIRONMENT (15)• If a scanning question reveals a possible hazard, ask detailed
questions to find out as much as possible about the nature and level of the hazard and then check Time, Place and Person:
• Time: When did symptoms begin? When did exposure begin? When do symptoms get worse? When do they improve?
• Place: Where is the patient when symptoms get worse? Where is the likely hazard? What is the channel through which the hazard reaches the patient?
• Person: Does anyone else have similar symptoms? Who? When? Where?
April 2011 17
Source: Primer in Population Health
March 2012

78-6 ENVIRONMENT (16)• Objective: - Be aware of local, regional, provincial and national
regulatory agencies that can assist in the investigation of environmental concerns
• If evidence supports, or a strong suspicion exists for, a causal connection between exposure and the clinical presentation, notify the appropriate authorities to inspect the site and thereafter to decrease and eliminate exposure.
April 2011 18March 2012

78-6 ENVIRONMENT (17)• Environmental Health Jurisdiction– Public Health Unit
• Enforcement of water and food safety regulations, sanitation, local hazard assessment, reportable diseases
– Municipal• Garbage disposal, recycling
– Province/territory• Toxic waste disposal, air/water standards
– Federal• Food regulations (Health Canada), designating and
regulating toxic substances– International
• Multilateral agreement (Kyoto Protocol)
April 2011 19March 2012

78-6 ENVIRONMENT (18)• Objective: - Describe simple interventions that will be effective in reducing
environmental exposures and risk of disease.• Examples: – Carbon monoxide: CO home detector– Salmonella: well cooked poultry and eggs, safe food
handling– Listeria: avoidance of unpasteurized cheese for pregnant
women– West Nile Virus: bug spray – UV light: sunscreen, sunglasses, shade– Radon: ventilation, air exchanger
April 2011 20March 2012

78-6 ENVIRONMENT (20)
• Objective: - Communicate simple environmental risk
assessment information to both patients and the community.
• Important to allow people to understand the risk and take action to avoid it
• Elements of communication: message, messenger (meaning), encoding, channel, decoding, recipient (understanding)
April 2011 21March 2012

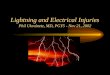
78-6 ENVIRONMENT (19)
April 2011 22
WHO, 2002, Global Solar UV IndexMarch 2012

Air Quality Health Index
• New public health information tool developed by Health Canada and Environment Canada
• Support decision-making about activity levels during increased levels of air pollution.
• Calculated based on:• Ozone (O3) at ground level,
• Particulate Matter (PM2.5/PM10)
• Nitrogen Dioxide (NO2)
March 2012 23

March 2012 24
Health Risk Air Quality Health Index
At Risk Population General Population
Low Risk 1-3Enjoy your usual outdoor activities.
Ideal air quality for outdoor activities.
Moderate Risk
4-6
Consider reducing or rescheduling strenuous activities outdoors if you are experiencing symptoms.
No need to modify your usual outdoor activities unless you experience symptoms such as coughing and throat irritation.
High Risk 7-10
Reduce or reschedule strenuous activities outdoors. Children and the elderly should also take it easy.
Consider reducing or rescheduling strenuous activities outdoors if you experience symptoms such as coughing and throat irritation.
Very High Risk
Above 10Avoid strenuous activities outdoors. Children and the elderly should also avoid outdoor physical exertion.
Reduce or reschedule strenuous activities outdoors, especially if you experience symptoms such as coughing and throat irritation.

78-6 ENVIRONMENT (21)
• Factors increasing perception of danger: – Characteristics of exposure:
• Involuntary; not under personal control• Unnatural; unfamiliar• No trust in institution involved; media attention
– Characteristics of outcome: • Catastrophic (not chronic); immediate; irreversible• Unknown, uncertain outcome, dreaded outcome• Affect children or identifiable people
Source: Primer in Population HealthApril 2011 25March 2012

74-4 WORK-RELATED HEALTH ISSUES
• Key Objective: - Determine whether the work place or
environmental conditions are potentially hazardous, the impact on the health of the workers, and recommend preventive strategies.
• Importance in Canada: – 920 work place deaths in 2001– 373,216 lost-time injuries in 2001
April 2011 26March 2012

Work-related Health Issues (2) • Selected Specific Objectives: - Elicit history of occupation, list of current and longest held
jobs, exposure to toxic/hazardous environments and identify potential relationship to patient presentation (temporal relationship to work or home activities)
- Counsel patients about safety issues and report findings to affected patients as well as employers (considering medical confidentiality issues)
• Consider underlying medical conditions and work risk
April 2011 27March 2012

Work-related Health Issues (3)
• Categories of occupational hazards:– Chemical: organic solvents (carbon
tetrachloride), mineral dusts (silica, asbestos), heavy metals, gases, second-hand smoke
– Physical: noise, temperature, air pressure, radiation
– Biological: bacteria, blood– Mechanical: repetitive strain, trauma– Psychosocial stress
April 2011 28March 2012

Work-related Health Issues (4)
• Occupational health history: – Work description and occupational profile– Prior and current exposure to hazards– Review of relevant workplace materials safety
data sheets– Look for sx of disease; job-related injuries– Temporal relationship between sx and exposure– Other environments, hobbies, occupation of
family members (Toronto Notes, 2011)
April 2011 29March 2012

Work-related Health Issues (5)
• Under provincial jurisdiction except for 16 federally regulated industries (e.g. banks, airports, highway transport) – Canada Labour Code– 90% of workers are under provincial jurisdiction
• Ontario: Occupational Health and Safety Act– Defines rights of workers: • participate, know, refuse and stop
– Employers have duties to protect health and safety
– Enforced by Ministry of Labour (inspectors)
April 2011 30March 2012

Work-related Health Issues (6)• Ontario: Workplace Safety and Insurance Act– Establishes WSIB to oversee work-site
injuries/disease– Funded by employers only– Non-fault protection but no right to sue– MD must submit medical report to WSIB; no need
for patient waiver.– MD must report exposure to designated
substances• Asbestos, arsenic, benzene, lead, mercury, vinyl
chloride, etc.
April 2011 31March 2012

Work-related Health Issues (7)Occupational Health Program – Essential responsibilities: •Health evaluation of employees•Diagnosis/treatment of occup. injuries/illnesses•Emergency treatment of other injury/illness•Education of employees re: occupational hazards•Evaluation of programs for the use of indicated personal protective devices•Assist management in providing a safe and healthful work environment. Inspect workplace.April 2011 32March 2012

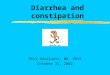
April 2011 33
Source Path Receiver
ModifyRedesign
SubstituteRelocateEnclose
AbsorbBlockDilute
Ventilate
EncloseProtect
Relocate
Potential approaches to risk control
Controlling Occupational Risks
March 2012

Work-related Health Issues (9)
• Work place safety issues can affect family members as well as the workers.
• Asbestos– Causes asbestosis and lung cancer in miners
and other workers– Asbestos in the air adheres to work clothing,
even if the clothes are brushed– Cleaning of clothes at home liberates asbestos
fibers and has been shown to cause cancer in family members.
April 2011 34March 2012

Environmental and occupational health
Multiple Choice Questionsfor discussion
April 2011 35March 2012

1) Which one of the following is not a typical feature of asbestosis?
a) increased risk of cancerb) pleural thickening and calcificationc) interstitial fibrosisd) obstructive pattern on pulmonary function testse) none of the above
April 2011 36March 2012

3) The following statements regarding noise are true EXCEPT:a) temporary threshold shift recovers following
cessation of noise exposureb) permanent threshold shift is characterized by a
progressive pattern of hearing lossc) most cases of permanent threshold shift are
surgically treatabled) higher frequency noise is more damaging than
low frequency noisee) none of the above
April 2011 37March 2012

4) The frequencies most necessary for the understanding of speech extend from about:
a) 20-20 000 Hzb) 400-4 000 Hzc) 250-8 000 Hzd) 100-5 000 Hze) none of the above
April 2011 38March 2012

5) Lead exposure typically results in:
a) chronic dermatitisb) resting and intention tremorc) extensor muscle weaknessd) arrhythmiase) cerebellar ataxia
April 2011 39March 2012

6) Which of the following statements concerning the Worker’s Compensation Act is true?a) the worker reserves the right to sue the
employer for negligenceb) funding is provided by the provincial governmentc) the worker is guaranteed payment from the first
day of injury/illness if it is deemed to be work-related
d) the Worker’s Compensation Board is an independent, private agency
e) none of the above
April 2011 40March 2012

7) Which of following statements regarding radiation is false?a) natural background radiation accounts for about
half of a typical person’s exposureb) ionizing radiation causes intestinal villi to
become denudedc) exposure to non-ionizing radiation may result in
cataractsd) ionizing radiation results in an increased
incidence of neoplasia such as lung and thyroide) none of the above
April 2011 41March 2012

36) All of the following statements concerning occupational health are true EXCEPT:
a) disorders of reproduction are among the top 10 work-related diseases and injuries
b) most workers are covered by both federal and provincial legislation with respect to workplace health and safety
c) skin problems and hearing problems together are responsible for half of WCB claims
d) a complete occupational medical history includes investigation of the temporal relationship between symptoms and exposure
April 2011 42March 2012

37) Which of the following statements concerning exposure to solvents in the workplace is true?
a) each solvent compound has a specific antidote that can be used to treat exposure
b) a prominent symptom of solvent exposure is memory loss
c) some solvents can cause skin dryness and loss of subcutaneous adipose tissue
d) solvents do not affect the bone marrowe) all of the above
April 2011 43March 2012

39) All of the following statements about environmental health are true EXCEPT:
a) levels of toxic agents measured in the environment may not reflect internal organ levels
b) the federal government monitors the quality and types of industrial emissions and toxic waste disposal
c) sick building syndrome is associated with Pontiac fever and Legionnaire’s disease
d) all humans have detectable levels of PCBse) none of the above is true
April 2011 44March 2012

More MCQs
• Here are some more questions that students can use to test their own knowledge:
http://www.medicine.uottawa.ca/sim/data/Self-test_Qs_Environmental_e.htm
• (The questions contain comments on the answers, to illustrate why a given response is not correct)
April 2011 45March 2012

Self-test (1)
• Which one of the following gases is NOT irritating to the respiratory tract?a) ozoneb) sulfur dioxidec) hydrogen chlorided) carbon monoxidee) chlorine
April 2011 46

Self-test (2)• How much radiation is an "average Canadian adult
woman" typically exposed to each year from the following sources: background dose; one screening mammography, and one abdominal CT scan?
a) Background 0.1 Sv; mammography 0.5 Sv; CT 1.0 Sv.b) Background 1.0 Sv; mammography 0.5 Sv; CT 0.1 Sv.c) Background 1.0 mSv; mammography 50.0 mSv; CT 5.0 mSv. d) Background 2.0 mSv; mammography 3.0 mSv; CT 10.0 mSv. e) Background 1.0 mSv; mammography 0.1 mSv; CT 0.1 mSv.
April 2011 47

Self-test (3)
• Toxicokinetics refers to:
a. The speed of distribution of a toxin. b. The biochemical and physiological effects of toxins. c. The diffusion gradient of a toxin. d. The activity or fate of toxins in the body over a
period of time.e. The transport of toxins through cell membranes.
April 2011 48

April 21 March 2012 49