Embed Size (px)
Citation preview

IQ-CSRC Study Results -
Presentation to the CSRC Scientific Oversight Committee
December 4, 2014
Borje Darpo MD, PhD
Co-chair SoC
iCardiac Technologies

• CSRC has entered a collaboration with the IQ-consortium to
prospectively evaluate whether ‘Early QT assessment’ can be
used to generate QT data with the same confidence as the
TQT study
• A prospective study in healthy volunteers has been conducted
in a setting designed to provide similarities with a routine
single ascending dose (SAD) study
• The objective of the study is to evaluate whether ECG
assessment in early phase clinical studies can replace, or
serve as an alternative to the TQT study
Background

History of Project
CSRC Think Tank Meeting (Feb 2012)• https://www.cardiac-safety.org/think-tanks/november-2011/thinktank-
meeting-on-qt-assessment-in-early-clinical-development
FDA-IQ Clinical Pharmacology Leadership Meetings• May 2012. FDA’s retrospective analysis was presented and prospective
study was discussed as a path forward.• Sep 2012. Study design concepts and analyses were discussed. FDA
agreed to select drugs to be tested.
CSRC-IQ Clinical Pharmacology Collaboration (Dec 2012)• September 2013: FTF meeting with FDA at which design and analyses
were agreed.

CSRC-IQ Steering Committee
IQ Consortium Clinical Pharmacology Leadership Group
• Nenad Sarapa (Bayer)
• Venkat Jarugula (Novartis)
• Jim Keirns (Astellas)
• Charles Benson (Lilly)
CSRC
• Christine Garnett (Certara)
• Borje Darpo (iCardiac)
• Catherine Ortemann-Renon (Sanofi)
• Corina Dota (AstraZeneca)
OQT Working Group (SAP)
• Steve Riley (Pfizer)
• Georg Ferber (Consultant)
• DCRI• Cindy Green
FDA
• Kevin Krudys
• Lars Johannesen

• 20 male and female healthy subjects
• 3 treatment periods
• 9 subjects were to receive each drug, 6 on placebo• Target to have at least 6 on active and 5 on placebo
• Study drugs: 5 ‘QT-positive’ drugs, well characterized from previous studies
1 QT negative
Placebo
• Dosing on 2 days: Day 1: Dose intended to give app. 10 to 12 ms QTc effect
Day 2: Dose intended to give app. 15 to 20 ms effect
• ECG methodology as in TQT studies
• Primary analysis: Based on exposure response
IQ-CSRC prospective study - Design

Study treatments (1)
DrugTQT Study Design and
Results
Dose JustificationDay 1 Day 2
ZOFRAN
(ondansetron
HCl)
QTc interval prolongation was studied in a
TQT study. The maximum mean (95%
upper CI) difference in QTcF from placebo
after baseline-correction was 19.5(21.8)
ms and 5.6 (7.4) ms after 15 minute
intravenous infusions of 32 mg and 8 mg
ZOFRAN, respectively.
52 mg oral**
Dose has not been tested in TQT
study. Anticipated effect is 10 to
12 ms.
Expected Cmax: 281 ng/mL
32 mg given by 15
min IV infusionBased on TQT study
results, mean ΔΔQTc=
19.5 ms.
QUALAQUIN
(quinine
sulphate)
QTc interval prolongation was studied in a
double-blind, multiple dose, placebo- and
positive-controlled crossover study in
young (N=13, 20 to 39 years) and elderly
(N=13, 65 to 78 years) subjects. After 7
days of dosing with QUALAQUIN 648 mg
three times daily, the maximum mean
(95% upper confidence bound) differences
in QTcI from placebo after baseline
correction was 27.7 (32.2) ms.
648 mg oral**
In a PK study in HV (n=24) the
mean change from baseline QTc
at Tmax was 12 ms (from old
Qualaquin label).
The Cmax on day 1 is about 3.9
µg/mL with an expected increase
in QTc of 12 ms based on the
PK/PD model.
648 mg q8h x 4
After the 4th dose (75% of
Cmax), the anticipated
concentration is 5.1 µg/mL
and the anticipated QTc is
19 ms.
ANZEMET
(dolasetron)
QTcF interval was evaluated in a TQT
study with IV dolasetron. The maximum
mean (95% upper confidence bound)
differences in QTcF from placebo after
pre-dose baseline-correction were 14.1
(16.1) and 36.6 (38.6) ms for 100 mg and
supratherapeutic 300 mg ANZEMET
administered intravenously, respectively.
100 mg PO**
Target Cmax for hydrodolasetron
~ 278 ng/mL.
150 mg IV by 15
min infusionTarget Cmax ~ 440 ng/mL
**Dose suggested by FDA

Study treatments (2)
DrugTQT Study Design
and Results
Dose JustificationDay 1 Day 2
Moxifloxacin NA 400 mg po**
Mean ΔΔQTc = 10-14 ms
Target Cmax ~ 2.95 µg/mL
800 mg IV given
by 60 min IV
infusion
Mean ΔΔQTc = ~20 ms,
Tikosyn
(dofetilide)
Increase in QT interval is
directly related to dofetilide
dose and plasma
concentration. The
relationship in normal
volunteers between dofetilide
plasma concentrations and
change in QTc is linear, with
a positive slope of
approximately 15-25 ms per
ng/mL after the first dose.
0.125 mg oralΔQTc = 10 to 11 ms
Target Cmax ~ 0.7 ng/mL
0.25 mg oral ΔQTc = 20 ms
Xyzal
(levocetirizine)
(negative drug)
A QT/QTc study using a
single dose of 30 mg of
levocetirizine did not
demonstrate an effect on the
QTc interval.
5 mg(therapeutic dose)
30 mgSupra-therapeutic dose
evaluated in TQT study
Target Cmax ~ 1.3
µg/mL
**Dose suggested by FDA

Randomization and Study treatments
A: Ondansetron
B: Quinine
C: Dolasetron
D: Moxifloxacin
E: Dofetilide
F: Levocetirizine (negative)
P: Placebo
P1, P2, P3: Period 1, 2 and 3
Randomization scheme
2 cohorts; placebo pooled from both.
9 subjects on active and 6 on placeboCohort Subject Period 1 Period 2 Period 3
1 1 A B C
1 2 B C A
1 3 C A B
1 4 C B A
1 5 B A C
1 6 A C B
1 7 P C B
1 8 C P A
1 9 B A P
1 10 A B C
2 11 D E F
2 12 E F D
2 13 F D E
2 14 F E D
2 15 E D F
2 16 D F E
2 17 P F E
2 18 F P D
2 19 E D P
2 20 D E F

Objectives and Endpoints
Primary Objective:
• To study the effect of 6 marketed drugs on the QTc interval using
concentration effect modeling.
Secondary Objectives:
• To evaluate the safety of the two single doses of 6 marketed drugs in
healthy subjects.
• To evaluate the effect of the two single doses of 6 marketed drugs on heart
rate, QTc, PR and QRS intervals using a descriptive statistical analysis by
time point by dose.
• To evaluate the pharmacokinetics of the 6 marketed drugs in healthy
subjects
Primary endpoint:
• Change-from-baseline QTcF (∆QTcF)
Secondary endpoints:
• ∆∆QTcF by time point
• Categorical analysis of the QTc outliers
• Effects on heart rate, PR and QRS intervals.

Criteria for QT Assessment
Positive QT assessment(for the positive drugs in this study):
1. The QT effect is detected:
The upper bound of the 2-sided 90% confidence
interval (CI) of the projected placebo-corrected
∆QTcF is above 10 ms at the observed geometric
mean Cmax of the drug.
2. The slope of the ER relationship is statistically
significant:
The lower bound of the 90% confidence interval
for the slope of ∆∆QTcF vs. concentration is
above zero.
Negative QT assessment (to claim that a drug
is negative, e.g. levocetirizine):
• The upper bound of the confidence interval of
the predicted placebo-corrected ∆QTcF at the
observed geometric mean Cmax of the drug is
below 10 ms.0 2000 4000 6000 8000 10000
-10
-50
51
0
Concentration (ng/mL)
QT
CF
(m
s)
Median concentration quantilesMean (90% CI) predicted QTcF prolongation

Results, evaluable subjects
Number of evaluable subjects
Day 1 Day 2
Ondansetron 9 9
Quinine 8-9 6
Dolasetron 9 9
Moxifloxacin 9 9
Dofetilide 9 9
Levocetirizine 8 8
Placebo 6 6
Discontinuations:• 1 subject prior to Dosing on Day 1 of Period 3 due to unknown criminal record (completed
periods 1 and 2)
• 2 subjects before Day 2 due to prolonged QTc (returned for next period)
• 1 subject withdrew the evening of Day 1 (Period 3) prior to the 16hr PD dose The subject
was experiencing AEs of nausea, vomiting, and dizziness.

Top Line Results
• All 5 positive drugs met the prespecified criteria , i.e.
the study was able to demonstrate a drug-induced QT
effect at the dose identified by FDA
• The negative drug, levocetirizine, also met the
criterion, i.e. a QT effect above 10 ms could be
excluded

Results - Number of evaluable subjects
Day 1 Day 2
Ondansetron 9 9
Quinine 9 6
Dolasetron 9 9
Moxifloxacin 9 9
Dofetilide 9 9
Levocetirizine 8 8
Placebo 6 6

Prespecified criteria for model selection
• Criteria for the absence of hysteresis met for all drugs
• Test for nonlinearity non significant for all drugs except dofetilide For dofetilide, an Emax model provided a better fit to
the data based on AIC

Moxifloxacin – by timepoint analysis
Day Largest mean ∆∆QTc*
(ms)
1 11.9
2 33.4

Moxifloxacin – Exposure response analysis
Slope, mean
ms per ng/mL
LB 90% CI UB 90%
CI
Treatment effect
(intercept) ms
Cmax
Day 1,
ng/mL
Predicted QTc
effect mean,
ms
LB 90% CI UB 90% CI Criteria
0.0065 0.0059* 0.0072 2.3 1862 14.4 10.6 17.9** Met
*: The positive slope is statistically significant
**: QTc effect above 10 ms at the Cmax of Day 1 cannot be excluded
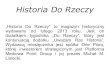
Red bars denote observed median (IQR) ∆∆QTcF within each concentration decile

Levocetirizine – Exposure response analysis
Slope, mean
ms per ng/mL
LB 90% CI UB 90%
CI
Treatment effect
(intercept) ms
Cmax
Day 2,
ng/mL
Predicted QTc
effect mean,
ms
LB 90% CI UB 90% CI Criterion
0.0014 -0.0013 0.0041 0.7 1005 2.1 -2.3 6.1* Met
*: QTc effect above 10 ms can be excluded at the geometric mean Cmax on Day 2

Results – primary and robustness
Drug
Slope,
mean
ms per
ng/mL
LB 90%
CI
UB 90%
CI
Treat-
ment
effect
ms
Cmax
Day 1,
ng/mL
Projected
QTc effect
mean, ms
LB
90%
CI*
UB
90%
CI*
Positive drugs (Day 1)
Ondansetron 0.033 0.025 0.042 0.2284
9.7 6.2 12.8
Day 1 only 0.032 0.022 0.043 0.3 9.5 7.2 13.5
Quinine 0.004 0.0034 0.0047 -3.03623
11.6 6.8 17.1
Day 1 only 0.004 0.0031 0.0051 -4.9 9.8 6.7 17.3
Dolasetron 0.021 0.013 0.028 3.1211
7.4 3.0 11.0
Day 1 only 0.016 0.0008 0.032 3.3 6.8 3.4 11.6
Moxifloxacin 0.0065 0.0059 0.0072 2.31862
14.5 10.5 17.7
Day 1 only 0.0045 0.0024 0.0065 3.4 11.7 10.6 17.9
Dofetilide* 22.2 18.9 25.6 1.10.42
10.5 6.3 14.9
Day 1 only 28.7 20.6 36.7 -0.9 11.3 6.1 14.6
Negative drug (Day 2)
Levocetirizine 0.0014 -0.0013 0.0041 0.71005
2.1 -2.3 6.1
Day 2 only 0.00042 -0.0032 0.0041 1.6 2.0 -2.6 6.0
*: Slope from linear model for comparison.
Predicted effect for dofetilide using Emax model: 11.6 ms; 90% CI 7.0 to 16.0

We propose using the same criteria as in the ICH E14 for QT assessment
adapted to exposure response analysis:
Criteria for negative QT assessment:
The upper bound of the 2-sided 90% confidence interval (CI) of the predicted
placebo-adjusted ∆QTcF is below 10 ms at clinically relevant plasma levels
of the drug.
The definition of clinically relevant plasma levels must be based on
observations in patients, including high plasma levels seen in the 'worst-case
scenario' and considerations are the same as when discussing the choice of the
supratherapeutic dose in a TQT study.
An advantage of QT assessment if performed in FIH studies is that often high
exposure to the drug is achieved, in many cases reaching maximum tolerated
levels and often higher than in any subsequent clinical trial.
Our proposal for QT assessment in early phase clinical studies

Our proposal for QT assessment in early phase clinical studies

We believe that a successful outcome of the study (as defined below for positive QT assessment) would provide evidence in support of a TQT waiver for drugs with a negative outcome in future phase 1 studies conducted in the same robust fashion (e.g. SAD or MAD studies with exposure response analysis)?
Do you agree?
FDA: Yes (with caveats and provisions)
Question asked at our previous FTF meeting with FDA (September/2013)

• Meeting with all key stakeholders at FDA held
October 8 to discuss results and FDA’s independent
analysis
• Results presented to ICH E14 Discussion group
• Results will be discussed on December 12 at a public
meeting at FDA’s White Oak campus Participation from regulators from all regions
Regulatory Activities

Accepted for publication in Clinical Pharmacology & Therapeutics

MY CONCLUSION
-
EXPECT CHANGE

Publications to-date stemming from the IQ-CSRC initiative
1. Darpo, B., Garnett, C. Early QT assessment - how can our confidence in the data be improved? Br J Clin Pharmacol 76, 642-648 (2012)
2. Darpo, B. et al. Cardiac Safety Research Consortium: Can the thorough QT/QTc study be replaced by early QT assessment in routine clinical pharmacology studies? Scientific update and a research proposal for a path forward.Am. Heart J 168, 262-272 (2014)
3. Darpo, B. et al. The IQ-CSRC prospective clinical Phase 1 study:"Can early QT assessment using exposure response analysis replacethe thorough QT study?“ Ann. Noninvasive Electrocardiol. 19, 70-81 (2014)
4. Ferber, Zhou, Darpo. Detection of QTc effects in small studies - Implications for replacing the thorough QT studyANE 2014; Nov 4. doi: 10.1111/anec.12227. [Epub ahead of print]
5. Darpo, B et al. Results from the IQ-CSRC prospective study support replacement of the thorough QT study by QT assessment in the early clinical phase .Accepted for publication in CPT December, 2014










![arXiv:1702.01866v3 [math.RT] 13 Feb 2020 - arXiv.org e ... · ERIK DARPO AND OSAMU IYAMA¨ ... method is based on an adaptation of Gabriel’s covering theory for k-linear categories](https://img.pdfslide.us/doc/110x75/5f4fa349768b7f613b6d52de/arxiv170201866v3-mathrt-13-feb-2020-arxivorg-e-erik-darpo-and-osamu.jpg)