Embed Size (px)
Citation preview

Assessment of groundwater quality in a region of endemicfluorosis in the northeast of Brazil
Consuelo Fernanda Macedo de Souza &
José Ferreira Lima Jr &
Maria Soraya Pereira Franco Adriano &
Fabíola Galbiatti de Carvalho &
Franklin Delano Soares Forte &
Rosimere de Farias Oliveira &
Alexandre Pessoa Silva & Fábio Correia Sampaio
Received: 25 November 2011 /Accepted: 24 September 2012 /Published online: 12 October 2012# Springer Science+Business Media Dordrecht 2012
Abstract The aim of this study was to estimate therisk for caries and fluorosis in a desertification area,applying the calcium/fluoride concentration ratio ofunderground water and the quality of water in a se-lected geographical region. This study was performedin the municipality of São João do Rio do Peixe,located in the tropical semiarid lands of Brazil. A totalof 111 groundwater samples were collected. Fluorideconcentration varied from 0.11 to 9.33 mg/L. Thirtypercent of all samples analyzed showed values above1.5 mg/L, while 64 % were above the ideal limit of0.7 mg/L. Mean calcium concentration was 47.6 mg/L, and 14.4 % of all samples presented values above
the WHO acceptable limits. The proportional value ofcalcium/fluoride in water showed that only 12 % ofthe samples were suitable for dental caries preventionwith minimal risk for dental fluorosis. Mapping of thefluoride distribution indicated that approximately2,465 people could be affected by dental fluorosisand 1,057 people might be affected by skeletal fluo-rosis. It can be concluded that, in addition to fluoride,many water parameters were not suitable for the drink-ing water. Mapping out calcium/fluoride ratio mayindicate areas of water suitability for caries control,whereas the fluoride concentration solely can indicatethe areas with the risk for fluorosis. This approach can
Environ Monit Assess (2013) 185:4735–4743DOI 10.1007/s10661-012-2900-x
C. F. M. de Souza : F. D. S. Forte : F. C. SampaioDepartment of Clinical and Social Dentistry, FederalUniversity of Paraíba,João Pessoa 58051-900, Brazil
J. F. Lima Jr :M. S. P. F. AdrianoSchool of Health of Cajazeiras, Federal University ofCampina Grande,Cajazeiras 58900-000, Brazil
F. G. de CarvalhoDentistry Department, UNIPE,João Pessoa 58053-000, Brazil
R. de Farias OliveiraNational Health Foundation,João Pessoa 58015-190, Brazil
A. P. SilvaAmbios Engineering and Processes,São Paulo 04015-011, Brazil
F. C. Sampaio (*)Health Science Center, Post graduation program inPreventive Dentistry and Pedodontics, Laboratory of OralBiology, Federal University of Paraíba,Campus I,João Pessoa, PB, Brazil 58051-900e-mail: [email protected]

be relevant for health authorities for identifying com-munities where dental caries or dental fluorosis isprevalent.
Keywords Fluoride . Calcium . Dental caries .
Fluorosis .Water quality
Introduction
Fluoride occurs naturally in soils and natural waterdue to chemical weathering of minerals that containthis element. Drinking water containing optimal con-centration of fluoride (0.7 mg/L) can lead to the pre-vention of dental caries (Galagan and Vermillion1957; Fejerskov and Kidd 2007). However, in a con-centration above 1.5 mg/L, prolonged intake of fluo-ride can cause dental fluorosis, and values above3 mg/L may lead to skeletal fluorosis (WHO 2000).For the sake of caries prevention, the calcium ion isrelevant because it may diffuse into plaque and pro-vide extra binding sites for fluoride, acting as deposits(Bruvo et al. 2008; Vogel et al. 2006). Thus, theconcentration of free calcium has to be higher in thedrinking water than in saliva in order to have thepreventive effect (Bruvo et al. 2008).
It has been estimated that only 0.6 % of the totalwater resources on Earth come from groundwater(Karthikeyan et al. 2010). However, an increase onhuman exposure to fluoride may have occurred, since300 million wells were probably perforated in the lastdecades (Bruvo et al. 2008; UNESCO 2001). Nowa-days, the problem of high concentration of fluoride ingroundwater has become an important toxicologicaland environmental issue in many parts of the world.More than 200 million people from around the worldsuffer from dental fluorosis caused especially by anexcess of fluoride in the drinking water (Brindha et al.2011; Heikens et al. 2005; Pauwels and Ahmed 2007;Yadav et al. 2009).
In the northeast region of Brazil, a semiarid region,characterized by scanty superficial hydrological resour-ces, due to very low annual rainfall precipitation, ground-water is considered a strategic water source. In São Joãodo Rio do Peixe (PB, Brazil), drinking water sources arescarce, and high fluoride concentration in the wells hasled to endemic fluorosis observations. Consequently,fluorosis has become an increasingly serious publichealth issue for the inhabitants of this area as well as for
neighboring regions. For instance, in the state of Paraíba,dental fluorosis reaches 31, 61, and 71 % of childrenresiding in regions where the fluoride concentration inthe drinking water is below 0.7 mg/L, between 0.71 and1.0 mg/L, and above 1.0 mg/L, respectively (Sampaio etal. 1999). At least three regions of this Brazilian statehave been identified as endemic for fluorosis (Sampaio etal. 1999). In addition to dental fluorosis, the state ofParaíba has also a high prevalence of dental caries amongchildren (Brasil 2004; Carvalho et al. 2007).
Several studies have shown the efficacy of waterfluoridation regarding dental caries prevalence (Burt etal. 2000; Narvai 2000; Bruvo et al. 2008). In general,there is scientific evidence showing that water fluorida-tion can be most advantageous for more deprived com-munities where other health policies are unavailable;however, most of these communities have limitationseven in the access to potable water (CDC 1999). Thereare few researches showing the importance of otherchemical compositions of drinking water to caries pre-vention. Bruvo et al. (2008) studied the chemical com-position of drinking water and its relation to theprevention of dental caries and concluded that the ions,calcium and fluoride, play an important role in theprevention of this disease (Bruvo et al. 2008).
The aim of this study was to estimate the risk forcaries and fluorosis in a desertification area applyingthe calcium/fluoride concentration ratio of under-ground water to assess the quality of water in a select-ed geographical region.
Materials and methods
Study area
The municipality of São João do Rio do Peixe is situatedabout 490 km away from João Pessoa, capital of Para-íba. It lies on latitude 06°43′45″, longitude 38°26′56″,and altitude 245 m. The study region covers an area ofapproximately 473.43 km2, and the estimated total pop-ulation is 18,323, according to the statistics of the Na-tional Institute of Geographic Statistics (Brasil 2009).
The population estimate done by the National In-stitute of Geography and Statistics was not used on theestimation of people affected by fluorosis, as this is amore general number (Table 3). On the other hand, theestimated total population of 11,870 was obtained bythe Official Health System records which is more local
4736 Environ Monit Assess (2013) 185:4735–4743

and specific for that region, leading to a more accurateestimation.
São João do Rio do Peixe is a semiarid region,presenting scanty rainfalls. The annual mean precipi-tation is about 431.8 mm (Brasil 2009). This areapresents an elevated content of fluoride in its ground-water beds, concentrating a major number of cases offluorosis in its severe state (Sampaio et al. 1999).
The municipality presents 400 underground waterpoints, from which 272 are operating, 14 have beenabandoned for being dried out or obstructed, and 114are paralyzed for various reasons. Most of them(85 %) are located in private property. The water isextracted mainly through the use of electrical pump(Beltrão et al. 2005).
Water sample collection and general analysis
A total of 111 groundwater samples, from 68 ruralcommunities, were collected from São João do Riodo Peixe, in precleaned vials. Samples were stored inan icebox and sent to the oral biology laboratory at theFederal University of Paraíba, where they were storedat 10 °C until the moment of analysis of fluoride andcalcium. Hydrochemical parameters, including watertemperature, pH, electrical conductivity, turbidity, to-tal alkalinity, and total hardness, were measured onsite, using colorimetric methods at the facilities of alocal laboratory. The later measurements were carriedout only for 20 water sources, following the criteria ofthe most populated villages (>500 inhabitants).
Fluoride analysis
A fluoride-ion-specific electrode (model 9409 BN,Orion, Cambridge, MA, USA) and a potentiometer(model 720A, Orion) were used for fluoride measure-ments. Calibration curves were made using knownstandard samples, containing between 0.2 and6.4 mg/L of fluoride. Both standard solutions andwater samples were prepared with Total Ionic StrengthAdjusting Buffer II (TISAB II). Millivolt readingswere converted to fluoride ion concentration usingthe standard correlation curve. The readings werecompared to the fluoride standard curve (r2>0.99).
The data were entered into an Excel spreadsheet(Microsoft Excel®) where mean and standard devia-tions were calculated. The correlation curve was used,as well as the correlation coefficient (r2≥0.999).
The number of people in a population affectedby dental fluorosis was based on the World HealthOrganization (WHO) calculation that states that ifthe concentration of fluoride on the drinking wateris of 1 mg/L, 1 to 2 % of the population drinkingthat water may be affected by dental fluorosis. Ifthis concentration rises to 2 mg/L, then 10 % ofthe population may be affected by dental fluorosis.That is, the higher the concentration of fluoride onthe drinking water, the higher the prevalence ofthe disease.
Calcium analysis
For the analysis of calcium, 10-μL aliquots ofwater samples were taken and mixed with 90-μLaliquots of arsenazo III solution in a microplate(Attin et al. 2005). The standard solutions usedwere prepared, mixing 10 μL of standard 25, 50,and 100 mg/L of calcium solutions to 90 μL ofarsenazo III, using pure arsenazo as blank solution.Calcium concentrations were colorimetricallyassessed through absorbance using a flat micro-plate reader at a wavelength of 650 nm (FLUOstarOPTIMA–BMG Labtech, Offenburg, Germany).
Statistical analysis
All data handling was performed using SPSS 13.0,and the significance was set at p<0.05. Confron-tation of population distribution maps and waterparameters were carried out using simple tables inExcel software (Microsoft Excel®). A proportionvalue for calcium and fluoride of 2.0 was attribut-ed as threshold for optimal drinking water for theprevention of dental caries and acceptable frequen-cies for dental fluorosis (Bruvo et al. 2008). Thesevalues were obtained by applying the values offluoride and calcium found on the samples toBruvo's equation, shown below:
DMF�S ¼ exp ½1:05� 0:18 fluoride� 0:33ð Þ= 0:25� 0:11 calcium� 83:5 = 25:63Þð �
ð1Þ
In addition to using Bruvo's model to see theeffect of calcium and fluoride on the decayed,missing, and filled teeth index (DMF-S index), wealso use the values to access the risk of fluorosis(Bruvo et al. 2008).
Environ Monit Assess (2013) 185:4735–4743 4737

Results
Fluoride concentration varied from 0.11 to 9.33 mg/L.Thirty percent of all samples analyzed showed fluorideconcentration above 1.5 mg/L, while 63.9 % were abovethe ideal limit of 0.7 mg/L (Table 1). The mean calciumvalue was 47.6 mg/L, and 14.4 % of all samples pre-sented values above the WHO acceptable limits(Table 1).
Water parameters of 20 samples are presented inTable 2. The pH levels of 20 water samples wereslightly alkaline. The electrical conductivity of thesamples varied from 0.124 to 1.96 μS/cm. Turbid-ity values showed large variation (Table 2). Exceptfor fluoride, the average concentrations of all otherions measured were within WHO acceptable limits(Tables 1 and 2).
The mean (±SD) total groundwater hardness calculat-ed for the area was 246.1 mg/L, with a minimum of 32and maximum of 620 mg/L. Except for five, all othersamples showed alkalinity values higher than total hard-ness. Therefore, the total hardness of the groundwater ofthe study area was related to temporary hardness. Mostof the samples (85 %) showed total hardness valueswithin acceptable WHO standard limits, while only23.8 % of the total samples showed alkalinity valueswithin the acceptable WHO standard limits for (Table 1).
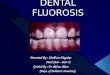
Taking into account the fluoride exposure, an esti-mate of 2,465 people may be affected by dental fluoro-sis, and 1,057 people could be affected by skeletalfluorosis (Table 3). The distribution of fluoride concen-trations is expressed in a map showing varying degrees
of risk as well as marking the spatial variation and thepotential perimeters of impact on the local populationrepresented in Fig. 1.
Applying the calcium/fluoride ratio model, only11.6 % of the total sample was suitable for cariesprevention following Bruvo's suggestion for calcium/fluoride ratio of an optimal drinking water, while37.8 % of the samples stand below caries prevention,and 47.7 % may incur in the risk of developing fluo-rosis (Table 4) (Bruvo et al. 2008; Vikas et al. 2009).
Discussion
There is consensus in the literature regarding the effectsof fluoride concentration in the drinking water on fluo-rosis or dental caries; however, there is little or no datashowing the interaction of fluoride with other ions.Bruvo et al. (2008) tested the effects of all standardchemical characteristics of the drinking water on DMF-S index in schoolchildren, and they found out that calci-um and fluoride were of major importance regardingdental caries prevention (Bruvo et al. 2008). They devel-oped a mathematical model showing how various con-centrations of calcium and fluoride in the drinking wateraffect the DMF-S index. In the present study, wemappedout calcium/fluoride ratio applying the values to Bruvo'smodel. Unlike Bruvo's study, our suggestion for optimaldrinking water is presented as a range (Table 4). Thereason for that modification is that, unlike Denmark, ourresearch found a large range of fluoride concentrationvalues.
Table 1 Comparison ofgroundwater samples at thestudy area with drinking waterstandards (WHO)
All concentrations are expressedin milligrams per liter except pH,temperature (in degrees Celsius),color (true color unit, TCU),turbidity (FTU), and conductivi-ty (in microsiemens)aNo health-based guideline valueis proposed for color in drinkingwater. However, levels of colorbelow 15 TCU are usually ac-ceptable to consumers
Parameters Mean (±SD) Range of values from samples WHO standards
pH 7.77 (±0.5) 7.11–8.84 6.5–8.5
Color (TCU)a 9.62 (±18.3) 1.6–73.5 –
Conductivity (EC) 0.65 (±0.47) 0.12–1.96 –
Total hardness (TH) 246.1 (±168.7) 32–620 500
Total alkalinity (TA) 251.1 (±99.9) 86.6–442.5 –
Turbidity 3.08 (±7.15) 0.02–29.5 –
Fluoride (F−) 1.64 (1.80) 0.11–9.33 1.5
Calcium (Ca2+) 47.6 (11.1) 27.4–82.3 –
Chloride (Cl−) 134.5 (±94.4) 58.3–421.6 –
Magnesium (Mg2+) 36.1 (±23.4) 4.8–92.4 –
Iron (Fe3+) 0.10 (±0.25) 0–1.1 –
Sulfate (SO42−) 27.8 (±45.6) 1–210 –
4738 Environ Monit Assess (2013) 185:4735–4743

Brazil has been regarded as a country of low fluo-ride levels in the drinking water with few reports ofendemic fluorosis regions particularly for urban areas
(Sampaio et al. 1999). Recently, the natural fluoridelevels in drinking water supplies of 223 cities of thestate of Paraíba in the northeast of Brazil were
Table 2 Physicochemical composition of 20 groundwater sam-ples at São João do Rio do Peixe, PB (all concentrations areexpressed in milligrams per liter except pH, temperature (in
degrees Celsius), color (TCU), turbidity (UT), and conductivity(in microsiemens per centimeter))
Sample pH Temperature (°C) Color Turbidity Conductivity Alkalinity TH F− Ca2+ Fe3+ SO42− Mg2+ Cl−
1 7.95 31.2 3.4 0.02 0.872 354.0 300 5.2 56.1 0.01 17 38.91 156.9
2 7.35 31.2 2.0 0.02 1.634 348.2 540 2.6 104.2 0.00 62 68.09 340.9
3 7.44 31.2 2.2 0.18 0.407 134.7 130 1.4 28.1 0.00 15 14.59 103.1
4 7.75 31.2 42.4 12.9 0.144 96.2 70 0.2 20.0 0.11 5 4.86 58.3
5 7.53 31.5 3.6 0.25 0.220 192.4 170 0.7 24.1 0.04 6 26.75 71.8
6 7.11 31.6 2.3 0.02 0.406 230.9 220 0.8 28.1 0.01 7 36.48 80.8
7 7.59 31.4 2.5 0.02 0.402 355.9 210 0.9 36.1 0.00 1 29.18 76.2
8 7.32 31.4 1.6 0.17 0.684 432.9 360 1.6 48.0 0.01 16 58.75 103.1
9 8.01 31.2 1.7 0.17 0.684 442.5 270 1.9 32.1 0.01 32 51.07 80.8
10 7.97 25.7 3.0 0.02 0.630 288.6 260 1.1 48.1 0.01 22 34.05 112.1
11 7.28 25.8 2.3 0.67 0.258 153.9 130 0.7 24.0 0.06 3 17.02 62.8
12 7.66 28.2 3.5 0.36 0.124 86.6 120 0.5 16.0 0.03 25 19.46 80.8
13 8.58 32.1 3.1 0.27 0.728 240.5 200 2.6 0.0 0.02 34 4.86 170.4
14 8.84 32.1 1.8 0.14 0.723 202.0 100 2.4 0.0 0.01 34 24.32 165.9
15 8.75 30.3 1.9 0.02 0.636 211.6 100 2.9 32.1 0.01 1 4.86 134.5
16 7.99 31.3 30.0 9.89 0.359 221.3 260 1.5 28.1 0.12 2 46.21 80.8
17 7.73 30.7 73.5 29.5 0.365 230.9 230 1.4 28.1 1.10 35 38.91 76.2
18 7.28 31.4 4.3 0.07 1.104 221.3 600 1.7 88.2 0.01 15 92.42 206.3
19 7.97 31.5 3.7 2.20 0.620 269.4 32 2.0 56.1 0.08 14 43.77 107.6
20 7.35 31.7 3.5 4.64 1.964 307.8 620 0.6 136.3 0.34 210 68.09 421.6
Mean ± SD 7.77 30.6 9.6 3.08 0.65 251.1 246.1 1.64 41.7 0.01 27.8 36.1 134.5
0.50 1.8 18.3 7.15 0.47 99.9 168.7 1.14 33.8 0.25 45.6 23.4 94.4
Values above accepted limits are in italic
Table 3 Estimate of population affected by dental fluorosis and at risk of developing skeletal fluorosis
Fluoride level (mg/L) Number ofwells
Estimated population(N of regular consumers)
Estimated population affectedby fluorosisa (n)
Estimated population at riskfor developing fluorosisa (%)
Dental fluorosis Skeletal fluorosis Dental fluorosis Skeletal fluorosis
<0.7 39 5,080 0 0 0 0
0.71–1.5 38 3,120 312 0 10 0
1.51–3.0 17 1,500 465 0 31 0
3.1–5.0 11 1,120 683 56–112 61 5–10
>5.1 06 1,050 1,050 735–945 100 70–90
Total 111 11,870 2,465 1,057 – –
a Risk of fluorosis based on expected prevalence according to fluoride levels in the drinking water as reported by the World HealthOrganization (2000), Sampaio et al. (1999), and Ozsvath (2009)
Environ Monit Assess (2013) 185:4735–4743 4739

< 0.7
0.71 - 1.5
1.51 – 3.0
3.1 – 5.0
> 5.1
F mgL-1
Fig. 1 Fluoride distribution in the municipality of São João do Rio do Peixe, PB, Brazil
4740 Environ Monit Assess (2013) 185:4735–4743

evaluated. Three urban areas presented optimal fluoridelevels, while samples from one city presented fluorideconcentrations above the recommended level of 0.7 mg/L but not exceeding 1.5 mg/L (Sampaio et al. 2010).Contrary to these data, the present study does not sup-port the view of general low fluoride levels in mostBrazilian groundwater sources. Actually, this is proba-bly the first report to present data indicating an area ofrisk of skeletal fluorosis in Brazil (Table 3).
The fluoride ion is more effective at inhibiting thehydroxyapatite dissolution when calcium and phosphateions are present in the medium (Hirata 2006). Fluorideand calcium have been shown by several studies to havea negative correlation. Once fluorite (CaF2) reaches alimit of solubility, an inverse relationship will existbetween fluoride and calcium concentrations (Ozsvath2009). By maintaining an optimal level of calcium andphosphate, enamel demineralization can be diminishedand re-mineralization increased enhancing naturaldefenses of saliva (Hirata 2006). Moreover, researchesshow that fluoride retention on the biofilm depends oncalcium concentration once fluoride is attracted to cal-cium ion (Rølla 1977; Schamschula et al. 1978; Vogel etal. 2006; Whitford et al. 2002). According to Bruvo'sstudy, the effects of both ions become less at higherconcentrations, where the effects tend to flatten out(Bruvo et al. 2008). So, an important factor that caninfluence fluoride bioavailability is calcium concentra-tion since it can modulate the adsorption of fluoride bybones and its elimination through urine (Whitford1994). Few studies have attempted to consider the
calcium/fluoride ratio effects on dental caries preventionregarding the drinking water (Bruvo et al. 2008).
Dental fluorosis is an enamel alteration related to achronic ingestion of fluoride during teeth formation. Itis a common misconception that fluorotic enamel isrich on fluoride; however, it actually shows a hypo-mineralization on its surface resulting in a poroustissue (Thylstrup and Fejerskov 1978). Studies haveshown a trade-off between caries and fluorosis whenthe concentration of fluoride is around 0.7 mg/L (Helleret al. 1997). However, an inverse relationship betweenfluoride content of the enamel's surface and dental carieshas not yet been demonstrated (Fejerskov 2004). More-over, it has been shown that there is no relative resis-tance of enamel to dental caries attack (Brudevold et al.1965; Weatherell et al. 1984).
It must be pointed out that dental caries and fluo-rosis are both modulated by calcium/fluoride ions.Nevertheless, these dental conditions have differentmechanisms. Dental caries is a topical localized pro-cess of low pH with a microbial influence, whereasdental fluorosis is a systemic condition that occurswhen fluoride is ingested excessively during the peri-od of dental formation (Kidd and Fejerskov 2004).Hence, dental caries and fluorosis have different etio-logical factors. However, taking into account the fluo-ride exposure, this effect has an inverse influencesince optimal fluoride in the drinking water may resultin low prevalence of caries and a high fluoride expo-sure may result in a high prevalence of dental fluoro-sis. Moreover, in areas with a high prevalence of
Table 4 Estimated DMF-S values at various calcium and fluoride concentrations
<0.25 0.25–0.5 0.51–0.75 0.76–1.0 1.1–1.25 1.26–1.75 1-76–2.0 >2.0
10–20 4–4.6 3.3–4.1 Calcium (mg/L)21–40 3.7–4.4 (1) 3.0–4.0 (5) 2.5–3.3 (6) 2.1–2.7 (3) 1.8–2.1 (1) 1.2–1.9 (3) 1.0–1.3 (1) <1.1 (6)
41–60 3.4–4.0 (5) 2.8–3.6 (8) 2.3–2.8 (5) 2.0–2.5 (18) 1.6–2.0 (2) 1.1–1.8 (5) 0.9–1.2 (1) <1.0 (15)
61–80 2.6–3.3 (2) 2.1–2.8 (4) 1.8–2.3 (2) 1.5–1.8 (1) <0.9 (3)
81–100 2.4–3.1 (1) 2.0–2.5 (1) 1.6–2.1 (1)
101–120 1.8–2.1 (1) <0.8 (1)
121–140 2.0–2.6 (1)
141–160 1.8–2.4 (2) 0.7–1.1 (2)
161–180 1.5–2.0 (2) 0.7–1.0 (1)
>181 0.7–1.0 (1)
Fluoride (mg/L)
A matrix of DMF-S values obtained at various calcium and fluoride concentrations according to the model shown in Eq. 1. Theitalicized values show our suggestion for optimal drinking water, with ranges of concentrations of both ions
Environ Monit Assess (2013) 185:4735–4743 4741

dental fluorosis, the pits of the dental enamel canaggravate caries development. Thus, dental caries datamay be taken with caution due to the influence ofdental fluorosis effect on dental enamel. Therefore,the evaluation of the adapted calcium/fluoride ratiofor the effects on dental caries may not be valid forthe extreme values of the table (>2.0) when dentalfluorosis prevalence may interfere on the dental cariesprocess (Ellwood and Fejerskov 2005; Fejerskov2004; Thylstrup and Fejerskov 1978).
The distribution of fluoride concentrations isexpressed on a map showing varying degrees ofrisk as well as marking the spatial variation andthe potential perimeters of impact on the localpopulation represented on Fig. 1. Our map datasuggest that high water fluoride content coincideswith the most populated rural areas of the munic-ipality. This situation creates the challenge ofimplementing defluoridation systems or findingnew sources of water where fluoride levels arelower than in the original wells. Contrary to den-tal fluorosis, skeletal fluorosis does not show spe-cific periods of susceptibility, and 3.0 mg/L offluoride in the water source is needed for a skel-etal fluorosis situation, making it less prevalentthan dental fluorosis (Aoba and Fejerskov 2002).Our estimates indicated 2,465 people with dentalfluorosis and 1,057 people affected by skeletalfluorosis. Even though these are numbers lowerthan those from India and African countries(Kloos and Haimanot 1999; Vikas et al. 2009),almost 8 % of the total population of this Brazil-ian municipality may be affected by fluorosis.
Although our data on other physical–chemicalcharacteristics are limited to a subsample of themapping study, the values give the trend of someparameters such as alkalinity, turbidity, electricalconductivity, and other ions (Table 2). In ground-water, dissolution activity of fluoride may becomefaster under some physical–chemical conditions. Inacidic conditions, fluoride is absorbed in clays, whereasin alkaline conditions, it is desorbed. So alkaline medi-um is more favorable for fluoride dissolution activity(Rafique et al. 2009; Saxena and Ahmed 2003), which isthe case of the present study as well as other works (Jainet al. 2009; Karthikeyan et al. 2010; Rao 2009; Ravindraand Garg 2007; Vikas et al. 2009). Except for fluoride,the average concentrations of all other ions measuredwere within WHO acceptable limits (Tables 1 and 2).
Conclusions
Apart from the simplicity of obtaining the calcium/fluoride ratio in the drinking water, the true value ofthis parameter needs further investigation taking intoaccount trends in dental caries prevalence. Mappingout fluoride in the drinking water provided enoughdata on fluorosis risk areas guiding health workers inspotting critical areas for defluoridation systems. Thedata generated from the present survey will be in-volved in formulating water policies, planning, andimplementing social and health services to individualsaffected by fluorosis.
Acknowledgments This study was supported by the BrazilianNational Council for Research and Development—CNPq—n.576703/2008-7.
Conflict of interest The authors declare no conflicting issues.
References
Aoba, T., & Fejerskov, O. (2002). Dental fluorosis: chemistryand biology. Critical Reviews in Oral Biology and Medi-cine, 13, 155–170.
Attin, T., Becker, K., Hannig, C., Buchalla, W., & Hilgers, R.(2005). Method to detect minimal amounts of calciumdissolved in acidic solutions. Caries Research, 39, 432–436.
Beltrão, B. A., Morais, F., Mascarenhas, J. C., Miranda, J. L. F.,Junior, L. C. S., & Mendes, V. A. (2005). Projeto decadastro de fontes de abastecimento por água subterrânea.Diagnóstico do município de São João do Rio do Peixe.Ministério de Minas e Energia. Programa de Desenvolvi-mento Energético dos Estados e Municípios—PRODEEM(p. 34). Recife: Serviço Geológico do Brasil—CPRM.
Brasil (2004). Projeto SB Brasil: condições de saúde bucal dapopulação brasileira 2002-2003–resultados principais:Coordenação Nacional de Saúde Bucal. Ministério daSaúde: pp. 52.
Brasil (2009). Contagem Populacional. Ministério do Planeja-mento, Orçamento e Gestão. Instituto Brasileiro de Geo-grafia e Estatística.
Brindha, K., Rajesh, R., Murugan, R., & Elango, L. (2011).Fluoride contamination in groundwater in parts of Nal-gonda District, Andhra Pradesh, India. EnvironmentalMonitoring and Assessment, 172, 481–492.
Brudevold, F. H., Mccann, et al. (1965). Caries resistance asrelated to the chemistry of the enamel. In: G. O. C. M (Ed.).Caries resistant teeth. London: Ciba Found Symp. Cariesresistance as related to the chemistry of the enamel, 121–148
Bruvo, M., Ekstrand, K., Arvin, E., Spliid, H., Moe, D.,Kirkeby, S., et al. (2008). Optimal drinking water
4742 Environ Monit Assess (2013) 185:4735–4743

composition for caries control in populations. Journalof Dental Research, 87, 340–343.
Burt, B. A., Keels, M. A., et al. (2000). The effects of a break inwater fluoridation on the development of dental caries andfluorosis. Journal of Dental Research, 79(2), 761–769.
Carvalho, T. S., Kehrle, H. M., & Sampaio, F. C. (2007). Prevalenceand severity of dental fluorosis among students from JoãoPessoa, PB, Brazil. Brazilian Oral Research, 21, 198–203.
(CDC) Center for Disease Control and Prevention (1999).Achievements in Public Health, 1900-1999. Fluoridationof drinking water to prevent dental caries. Morbidity andMortality Weekly Report (MMWR), 48(41), 933–956.
Ellwood, R., & Fejerskov. O. (2005). Uso clínico do flúor. In:(Ed.). Cárie dentária- a doença e seu tratamento clínico.São Paulo: Santos. Uso clínico do flúor, 189–219
Fejerskov, O. (2004). Changing Paradigms in Concepts onDental Caries: Consequences for Oral Health Care. CariesResearch, 38, 182–191.
Fejerskov, O., & Kidd, E. (2007). Cárie dentária: A doença e seutratamento clínico: Santos. p 352.
Galagan, D. J., & Vermillion, J. R. (1957). Determining opti-mum fluoride concentrations. Public Health Reports, 72(6), 491–493.
Heikens, A., Sumarti, S., Mv, B., Widianarko, B., Fokkert, L.,Kv, L., et al. (2005). The impact of the hyperacid IjenCrater Lake: risks of excess fluoride to human health.Science of the Total Environment, 346, 56–69.
Heller, K. E., Eklund, S. A., et al. (1997). Dental Caries andDental Fluorosis at Varying Water Fluoride Concentrations.Journal of Public Health Dentistry, 57(3)136–143.
Hirata, E. (2006). Potencial de remineralização do cálcio efosfato: revisão de literatura e estudo laboratorial. Facul-dade de Odontologia da Universidade Estadual Paulista,Araçatuba. http://www.athena.biblioteca.unesp.br/exlibris/bd/bfo/33004021073P5/2006/hirata_e_dr_araca.pdf.
Jain, C. K., Bandyopadhyay, A., & Bhadra, A. (2009). Assess-ment of groundwater quality for drinking purpose, DistrictNainital, Uttarakhand, India. Environmental Monitoringand Assessment, 166, 663–676.
Karthikeyan, K., Nanthakumar, K., Velmurugan, P., Tamilarasi,S., & Lakshmanaperumalsamy, P. (2010). Prevalence ofcertain inorganic constituents in groundwater samples ofErode district, Tamilnadu, India, with special emphasis onfluoride, fluorosis and its remedial measures. Environmen-tal Monitoring and Assessment, 160, 141–155.
Kidd, E. A. M., & Fejerskov. O. (2004). What constitutes dentalcaries? Histopathology of carious enamel and dentin relat-ed to the action of cariogenic biofilms. Journal of DentalResearch, 83, 35–38.
Kloos, H., & Haimanot, R. T. (1999). Distribution of fluorideand fluorosis in Ethiopia and prospects for control. Tropi-cal Medicine & International Health, 4, 355–364.
Narvai, P. C. (2000). Cárie dentária e flúor: uma relação doséculo XX. Ciência & Saúde Coletiva, 5(2), 381–392.
Ozsvath, D. L. (2009). Fluoride and environmental health: areview. Reviews in Environmental Science and Biotechnol-ogy, 8, 59–79.
Pauwels, H., & Ahmed, S. (2007). Fluoride in groundwater:origin and health impacts. Géosciences, 5, 68–73.
Rafique, T., Naseem, S., Usmani, T. H., Bashir, E., Khan, F. A.,& Bhanger, M. I. (2009). Geochemical factors controlling
the occurrence of high fluoride groundwater in the NagarParkar area, Sindh, Pakistan. Journal of Hazardous Mate-rials, 171, 424–430.
Rao, N. S. (2009). Fluoride in groundwater, Varaha RiverBasin, Visakhapatnam District, Andhra Pradesh, India.Environmental Monitoring and Assessment, 152, 47–60.
Ravindra, K., & Garg, V. K. (2007). Hydro-chemical survey ofgroundwater of Hisar City and assessment of defluorida-tion methods used in India. Environmental Monitoring andAssessment, 132, 33–43.
Rølla, G. (1977) Effects of fluoride on initiation of plaqueformation. Caries Research, 11(1), 243–261.
Sampaio, F., von der Fehr, F., Arneberg, P., Petrucci Gigante, D.,& Hatloy, A. (1999). Dental fluorosis and nutritional statusof 6 to 11 year old children living in rural areas of Paraíba,Brazil. Caries Research, 33, 66–73.
Sampaio, F. C., Silva, F. D. S. C. M., Silva, A. C. B., Machado,A. T. A. B., Araújo, D. A. M., & Sousa, E. M. (2010).Natural fluoride levels in the drinking water, water fluori-dation and estimated risk for dental fluorosis in a tropicalregion of Brazil. Oral Health & Preventive Dentistry, 8,71–75.
Saxena, V. K., & Ahmed, S. (2003). Inferring the chemicalparameters for the dissolution of fluoride in groundwater.Environmental Geology, 43, 731–736.
Schamschula, R, M., Bunzel, et al. (1978). Plaque minerals andcaries experience: associations and interrelationships. JDent Res, 57, 427–432. .
Thylstrup, A., & Fejerskov. O. (1978). Clinical apearance ofdental fluorosis in permanent teeth in relation to histologicchanges. Community Dental Oral Epidemiology, 6, 315–328. .
UNESCO (2001). Internationally shared (transboundary) aqui-fer resources management. A framework document. IHP-VI Series on Groundwater, Document SC-2001/WS/40,Paris.
Vikas, C., Kushwaha, K., & Pandit, M. K. (2009). Hydrochem-ical status of groundwater in district Ajmer (NW India)with reference to fluoride distribution. Journal GeologicalSociety of India, 73, 773–784.
Vogel, G., Shim, D., Schumacher, G., Carey, C., Chow, L., &Takagi, S. (2006). Salivary fluoride from fluoride dentifri-ces or rinses after use of a calcium pre-rinse or calciumdentifrice. Caries Research, 40, 449–454.
Whitford, G. M. (1994). Intake and metabolism of fluoride.Advances in Dental Research, 8, 5–14.
Whitford, G., Wasdin, J., Schafer, T., & Adair, S. (2002). Plaquefluoride concentrations are dependent on plaque calciumconcentrations. Caries Research, 36, 256–265.
Weatherell, J, C., & Robinson, et al. (1984). The concept of enamelresistance: a critical review. Cariology Today, 223–230.
World Health Organization (WHO) (2000). Air quality guide-lines. World Health Organization (WHO), Regional Publi-cations, European Series, Regional Office for Europe,Copenhagen, Denmark Chapter 6.5.
Yadav, J. P., Lata, S., Kataria, S. K., & Kumar, S. (2009).Fluoride distribution in groundwater and survey of dentalfluorosis among school children in the villages of theJhajjar District of Haryana, India. Environmental Geo-chemistry and Health, 31, 431–438.
Environ Monit Assess (2013) 185:4735–4743 4743