Embed Size (px)
DESCRIPTION
Updating of Primary Health Care Notebook in Oral Health, Ministry of Health, FOUSP, 2012 - Brazil.
Citation preview

U P D A T I N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 1
Fluorosis
1. Conceptual and Epidemiological Aspects
! Dental fluorosis is a development anomaly that occurs by prolonged fluoride intake during the period of tooth formation and enamel maturation. It is characterized by an increase in enamel porosity making it seem opaque.
! In some regions in Brazil, there is an increased number in diagnosis of dental fluorosis. Results from the Survey of the Oral Health Conditions of the Brazilian Population – SB Brasil, finished in 2003 showed around 9% prevalence of dental fluorosis in 12 year-old children and 5% in adolescents from 15 to 19 years of age.
! In 12 year-old children, the highest rates were seen in the Southeast and South regions (around 12%) and the lowest in the Central West and Northeast (about 4%).
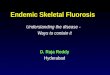
! The mild forms of fluorosis are characterized by thin lines or white chalky spots that appear in the dental enamel or tips of cusps. They are common in places where public water supply is fluoridated.
! Systemic forms and the intake of topical fluoride also contribute to fluorosis. According to various authors, the prevalence of mild fluorosis in the population that has access to fluoridated water is around 15 to 25%.
! In the most severe forms the enamel is completely whitish and it is possible to lose structure. Dark spots are frequent, resulting from food pigments and they are not necessarily related to the degree of severity. Severe fluorosis is generally seen in places where the residual fluoride contents (in natura) are present in high concentrations in consumption water, mainly the rural areas supplied by artesian wells. The concomitant fluoride intake from various sources may also result in severe fluorosis.
Dental fluorosis is a development anomaly that occurs by prolonged fluoride intake during the period of tooth formation and enamel maturation.
1. Conceptual and Epidemiological Aspects
Page 1
2. Main Risk Factors
Page 2
3. Collective Approacha. Organization of
Surveillance Actions in Health emphasizing Prevention and Fluorosis Detection
b. Health Promotion Actions
Page 2
4. Individual Approach a. Diagnosisb. Treatment
Page 3
5. Clinical Cases
Page 3
6. References and Credits
Page 4
Capítulos Atualizado e Ilustrado
Figure 1. Mild dental fluorosis. Note the whitish lines along the enamel.

UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 2
2. Main Risk Factors• Presence of fluoride in contents above the
recommended in public water supply, derived from the fluoridation process or naturally existing in springs (fluoride residual content).
• Concomitant use of two or more forms of fluoride intake (systemic). Example: fluoridated water and fluoride-containing drugs.
• Frequent intake of fluoridated toothpaste in the period of dental formation (up to 6 years of age) in areas with fluoridated water.
• Absence of a surveillance system to monitor fluoride content in public water supply and packaged mineral water.
• Preparation of child’s food with fluoridated water, for example, powdered milk.
• Abusive use of topical fluoride applications (causing swallowing) in places where there is systemic fluoride.
3. Collective ApproachOrganization of Health Surveillance Actions Emphasizing Prevention and Fluorosis Detection
• Surveillance, control and education to the population about the several ways of using fluoride as a necessary measure to control the acute and chronic forms of fluoride intoxication mainly in the ages at risk of dental fluorosis (children up to 6 years of age).
• Implementation of surveillance systems to control fluoride contents in public water supply to improve the quality of water fluoridation, systematic control of contents applied and process continuity.
• Surveillance of fluoride content in food: mineral water, canned drinks, soft drinks, juices and teas should have their maximum allowed fluoride content regulated and exhibited in labels and packaging and be systematically analyzed by the sanitary surveillance.
• Check fluoride content in dentifrices and dental products containing fluoride.
• Include dental fluorosis in the routine epidemiological trials: oral health services should carry on longitudinal epidemiological trials in the population exposed to fluoride sources following the trend of damage prevalence and severity.
• Epidemiological surveillance of dental fluorosis cases: perform epidemiological investigation of fluorosis cases diagnosed in its range with the objective of identifying social, environment, cultural and individual factors that favored the incidence and proposing integral prevention actions.
• Creation of protocols with recommendations about the individual and collective use of fluoridated substances in dental care.
Health Promotion Actions (interdepartmental and educational)
! The Oral Health Team should pay attention to the causes of dental fluorosis in the region in order to plan prevention actions according to the existing problems, including broad communication and information to the population about the risks of swallowing fluoride dentifrice, mainly children in cities supplied with fluoridated water, as well as other preventive procedures.
! In the regions where room temperature is high, water intake is greater and the risk of excessive fluoride ingestion through the water is also high. The ideal fluoride concentration in drinking water in places where the average room temperature is around 30C is 0.7 ppm (mg/L). The fluoride concentration in drinking water should increase according to the drop in room temperature. In regions where the climate is mild (< 25C) and where water consumption is less, the ideal fluoride concentration is 1 ppm (mg/L) and should not exceed 1.2 ppm.
! There should be a joint search for alternative sources of water supply when it is identified the presence of elevated fluoride contents in the water for human consumption. If dental fluorosis is proven in a
U P D A T I N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L

UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 3
community, it is recommended to investigate the degree of esthetic satisfaction
and perception of the problem in the region.
4. Individual Approach
Diagnosis
! Clinically, dental fluorosis presents fine white lines that may become yellowish or brown due to food dye impregnation, as well as various forms of erosion. The severity of fluorosis depends on dosage (contents and amounts), age when ingestion occurred, exposure time. It may lead to loss of enamel parts with anatomic deformity in teeth.
! The individual diagnosis should be done after prophylaxis and drying for 30 seconds (with gauze or air spray) to disclose the enamel pores.
! Fluorosis is always symmetrical; homologous teeth show fluorosis in the same levels. The most important differential diagnosis is the white spot due to caries and other opacities. When evaluating, consider fluoride exposure, its origin and content in water consumption.
Treatment
! Severe forms of dental fluorosis may sometimes be considered an esthetic discomfort to the patient and the indication is to treat the spots. This treatment consists of pumicing the external porous enamel until the spot, caused by the impregnation of food pigments, is removed. After micro abrasion, fluoride application (gel or varnish) is indicated. Enamel with fluorosis stains is more porous and not necessarily richer in fluoride.
Among the products used in the micro abrasion technique there are hydrochloric acid, hydrogen peroxide and phosphoric acid. In severe cases, it is necessary to fabricate crowns or veneers.
5. Clinical Cases
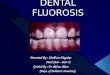
Figure 2. Mild dental fluorosis. See the whitish lines along enamel.
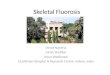
Figure 3. Severe dental fluorosis. See dental enamel loss in the buccal aspect of incisors.
Figure 4. Severe dental fluorosis with great enamel loss and staining
U P D A T I N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L

UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 4
6. CreditsUpdating of Primary Health Care Notebook on Oral Health and images – 2012:
Prof. Fábio Correia Sampaio – Universidade Federal da Paraíba
Layout: Profa. Mary Caroline Skelton-Macedo
Translation: Flávia Egner
U P D A T I N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L