Embed Size (px)
DESCRIPTION
Skeletal Fluorosis, Review of literature, dental fluorosis, diagnosis and management, neurological complications in fluorosis
Citation preview

Skeletal Fluorosis
Vinod NaneriaGirish Yeotikar
Arjun WadhwaniChoithram Hospital & Research Centre, Indore,
India

Fluorine
• Fluorine is the most abundant element in nature, and about 96% of fluoride in the human body is found in bones and teeth.
• Fluorine is essential for the normal mineralisation of bones and formation of dental enamel?????
• The NRC estimates, for instance, that the biological half-life of fluoride in bone (the time for half of it to be removed) is as long as 20 years.
• The principal sources of fluorine was drinking water and food such as sea fish, cheese and tea.
• The recommended level of fluoride in drinking water in India is 0.5 to 0.8 mg/l

Common causes of fluorosis
• Consumption of fluoride from drinking water in India.
• Ingestion of contaminated food grains by burning coal as an indoor fuel source, a common practice in China.
• Consumption of fluoride from the drinking of poor-quality pu-erh tea (brick tea) is reported to cause fluorosis in Tibet and China.
• Inhalation of fluoride dusts/fumes by workers in Aluminium industry.

Fluorosis in China
• In China -burning coal with a non-chimney stove → fluoride released in large quantity → polluting indoor air → polluting stored crop (mainly corn and chili) → ingestion into body → fluorosis.

Fluorosis - World
• Fluorosis is a public health problem in 24 countries, including India, which lies in the geographical fluoride belt that extends from Turkey to China and Japan through Iraq, Iran and Afghanistan.
• Estimated total population consuming drinking water containing elevated levels of fluoride is over 66 million in India.

Five Global Belts• Belt 1: Turkey, Syria, Jordan, Egypt, Sudan, Somali,
Ethiopia Kenya, Tanzania, Mozambique + South Africa.
• Belt 2: Egypt , Libya , Algeria , Morocco , Western Sahara, Mauritania.
• Belt 3: Turkey, Iraq, Iran, Afghanistan, Pakistan, India, North Thailand, (parts of) China.
• Belt 4: Sierra Nevada, USA Rocky Mountain, Central America, Colombia, Peru, Bolivia, Andes Mountains.
• Belt 5: Japan, Philippines, Volcanic Indonesia.


Fluoride levels
• The safe level of fluoride is standardized to 0.5 mg/L and 1.0 mg/L, respectively as the desirable and maximum allowable concentrations in drinking water.
• The literature contains a wide range (0.008–0.045 ppm) of reported normal plasma fluoride concentrations.

Fluoride
• More than 90 % of the ingested fluoride is absorbed from the gut.
• Approximately 50 % of the fluoride absorbed is deposited in the bones and teeth. The remaining is excreted in urine.

Fluoride
• About 99 % of the fluoride retained in the body is stored in the
• mineralized bones and teeth on account of its affinity for calcium phosphate. Its effects on bones and teeth only are of clinical importance influencing their mineralisation, structure, functions and development.
• Fluoride ions are taken up rapidly by bone by replacing hydroxyl ion in bone.

Fluoride
• Fluoride is a bone seeker and its incorporation into hydroxyapatite, i.e. the spot wise production of fluoroapatite, alters the size and the structure of the bone crystals.

Fluoride
• The fluoroapatite crystals are larger in size; offer less surface exchange, less soluble, more stable and less reactive to the actions of parathyroid hormone.
• The toxic effects are more severe in children with growing bones, women with children with their depleted bone and mineral reserves and in labourers with excessive drinking of water that can be up to 6 to 8 litres in summer.

Fluoride
• Continuous daily intake of 2.5 mg of fluoride for more than 6 months deposits 4000-6000 mg/kg of fluoride and causes detectable radiological changes of fluorosis. About 100 million people in India are affected and more than 200 million are exposed to the risk of developing endemic fluorosis.

mechanism of fluorosis
• The fluoride incorporation into the bone hydroxyapatite, altering the size and structure of its crystals.
• The fluoroapatite formed decreases the mechanical competence of the bone, resulting in abnormal structure and poor quality of bone, with increased risks for fractures.
• Rickets, osteomalacia, secondary hyperparathyrodism and regional osteoporosis are often associated with skeletal fluorosis.
• The bone diseases and deformities are more severe and complex in patients with dietary calcium and vitamin-D deficiencies.

Fluorosis – Indian States
• 15 States in India are endemic for fluorosis (fluoride level in drinking water >1.5 mg/l).
• Worst affected – Rajasthan, Gujarat, & Andhra.
• Moderately affected - Punjab, Haryana, Madhya Pradesh and Maharashtra.
• Mildly affected - Tamil Nadu, West Bengal, Uttar Pradesh, Bihar and Assam.

Fluorosis is endemic in 20 states out of the 35 states.
70-100% districts are affected in Andhra Pradesh, Gujarat and Rajasthan.
40-70% districts are affected in Bihar, New Delhi, Haryana, Jharkhand, Karnataka, Maharashtra, Madhya Pradesh, Orissa, Tamil Nadu and Uttar Pradesh
10-40% districts are affected in Assam, Jammu & Kashmir, Kerala, Chhattisgarh and West Bengal.

Radiological features:
• The earliest radiological findings appear within six mouths of continuous exposure to high intakes of fluoride and include periosteal and endosteal reactions, coarse axial trabcculations and osteopenia in the metaphyseal regions, sclerosis, and modelling abnormalities of the epiphyses, carpal and other bones of the hand, more particularly observed in growing children.
• The incidence of spinal osteoporosis is significantly low and of osteomalacia and secondary hyperparathyroid bone disease significantly higher in women residing in endemic fluorosis villages.

Biochemical Markers:
• Plasma calcium, magnesium and phosphorus remain normal,
• Alkaline phosphatase and fluoride levels are elevated.
• Serum parathyroid hormone levels are always raised as a compensatory mechanism to maintain extracellular ionised calcium equilibrium consequent to decreased solubility and reactivity of fluoroapatite crystals, fluoride induced osteomalacia and dietary calcium deficiency.

Biochemical Markers:
• Osteocalcin, Calcitonin and (1,25 (OH)2D3) concentrations are increased or high normal.
• Pituitary, thyroid, adrenal and gonadal functions remain unaltered and serum growth hormone levels are variably increased.
• Twenty-four hour urinary excretions of fluoride and of hydroxyproline are increased and of calcium and magnesium are decreased or low normal. Renal functions remain unaltered.

Bone scanning and densitometry
• 99mTC dl-phosphonate bone scanning revealed nonspecific appearance of generalized increased tracer uptake throughout the skeleton.
• Greater uptake is observed in axial skeleton with tie sternum sign, patella sign and faint kidney images, diagnostic of compensatory secondary hyperparathyrodism with high bone turnover.
• The DXA bone densitometric measurements of lumber spine (L1-L4) showed increased BMD 1.12 ± 0.04 g/cm2 in patients of endemic skeletal fluorosis as compared to matched normal controls 0.78 ± 0.03 g/cm2.

Bone histopathology and histomorphometry:
• Histopathological studies of undecalcified iliac crest biopsies revealed poorly formed haversian systems, disordered lamellar orientation of the bone and the new bone formed is immature, woven, amorphous and hypomineralized.
• There is an increase in bone surfaces lined with wide osteoid seams associated with increased bone re-sorption. These findings suggest occurrence of osteomalacia with secondary Hyperparathyroidism in patients with endemic skeletal fluorosis.

Bone quality
• Bone quantity in skeletal fluorosis is increased at the cost of bone quality, which increases the risk for fracture.
• True fractures are extremely rare and occurred in less 1.5 percent of our cases.
• Pseudo-fractures appeared in more than 35% of the patients with endemic skeletal fluorosis, more particularly in women of child bearing age.
• The rare occurrence of true fractures and of spinal osteoporosis may be due to associated osteomalacia consequent to chronic exposure to fluoride.

Fluorosis, Goiter, & Renal Stones
• In the community with endemic fluorosis, goiter and stone disease were practically non-existent. In the community with endemic goiter, fluorosis was non-existent and the stone disease was sporadic. In the community with endemic renal stone disease, the prevalence of goiter was sporadic and fluorosis was practically non-existent.

Fluorosis, Goiter, & Renal Stones
• A positive correlation existed between the occurrence of stone disease, water hardness and its calcium content. In endemic fluorosis villages water analysis showed higher the fluoride, higher the iodine, higher the alkalinity and softer the water. In the areas endemic for goitre lower the iodine and lower was the fluoride in the drinking water.

Clinical recovery
• Clinical recovery occurred in more than 85% with mild to moderate severity within 1-5 years after the exposure to fluoride is ceased and treated with calcium and vitamin D.
• In severe cases clinical recovery was slow and took 5-15 years for satisfactory clinical and occupational recovery after the exposure to fluoride is ceased and treated with calcium, vitamin D and appropriate physiotherapy.

Clinical recovery
• The radiological reversibility in radiographs of the pelvis, spine, chest and hands showed that the trabecular sclerosis in all the films was slowly reduced.
• The urine showed persistent increase in the excretion of calcium. The cortical thickness and sclerosis, calcifications of ligaments, muscular attachments, tendons, capsules and of interosseous membrane essentially remained unchanged.

Reversibility of ESF in 15 years old girl 9 months after exposure tofluoride is ceased and treated with vit-Dand calcium.

Clinical Reversibility of ESF in a patient aged 65 years 24 months after exposure to fluoride isceased.

Reversibility of ESF in 18 years old boy 8 years after exposure to fluoride is ceased and treated with vit-D and calcium.
(A) Before Treatment (B) After Treatment

Prevention
• The most illustrious and practical example is of Sri Sathya Sai Project for the safe drinking water supply, which has controlled fluorosis from more than 1,000 villages in district Ananthpur of the state of Andhra Pradesh, using deep bore water technology.
• The use of more than 100 m deep bore water supply is able to provide water with fluoride less than 1mg/L, low alkalinity and normal or high normal calcium contents and this could play a master role in the control of endemic fluorosis.

Calcium and vitamin D supplements:
• Calcium is the strongest antagonist of fluoride toxicity. The toxic effects of fluoride on bones and teeth are more severe and complex in dietary calcium deficiency states.
• Calcium deficiency and fluoride interaction syndrome of bone disease and deformities are more severe and complex in growing children, adolescents, pregnant and lactating mothers, because of the greater demands for calcium in these groups.
• Adequate intakes of calcium to maintain the positive calcium balance to counteract the toxic effects of fluoride is therefore essential for the population residing in endemic fluorosis villages.

Dental Fluorosis
• There is no conclusive evidence proving that fluoride is an essential nutrient for human health.
• The widely propagated dental caries protection effect of fluoride is erroneous and has not been supported by long-term control double blind scientific investigations on a large cross-section of population.

Dental Fluorosis
• The decline in the incidence of dental caries in fluoridated areas, in fact has resulted due to simultaneously increased dental health facilities, increasing number of dental clinics and hospitals, besides education and rising community awareness on 1) oral health and hygiene, 2) calcium and vitamin D nutrition, and 3) the deleterious effects of excess consumption of the sugary and starchy foods on dental health.

Dental Fluorosis
• Tooth enamel is principally made up of hydroxyapatite (87%) which is crystalline calcium phosphate.
• Fluoride which is more stable than hydroxyapatite displaces the hydroxide ions from hydroxyapatite to form fluoroapatite.
• Fluorosis of dental enamel occurs when excess Fluoride is ingested during the years of tooth calcification-essentially during the first 7 years of life.

Dental Fluorosis
• 1890 - "Tanagra", first Calcium Fluoride containing toothpaste, sold by Karl F. Toellner Company, of Bremen, Germany.
• Fluoride toothpastes developed in the 1950s received the ADA's approval.
• In 1955, Procter & Gamble's Crest launched its first clinically proven fluoride-containing toothpaste.

Children under 6 years of age should have adult supervision. Use only a pea sized amount.Do not swallow.
Directions for use in children

Dental Fluorosis
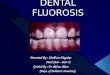
• It is characterised by mottling of dental enamel, which has been reported at levels above 1.5 mg/L intake.
• On prolonged continuation of this process the teeth become hard and brittle.
• Dental fluorosis in the initial stages results in the tooth becoming coloured from yellow to brown to black.
• Depending upon the severity, it may be only discolouration of the teeth or formation of pits in the teeth. The colouration on the teeth may be in the form of spots or as streaks.

Dental Fluorosis in children

Dental Fluorosis in adult

Skeletal Fluorosis
• Exposure to very high fluoride over a prolonged period of time results in acute to chronic skeletal fluorosis.
• Crippling skeletal fluorosis might occur in people who have ingested 10 to 20 mg of fluoride per day for over 10 to 20 years.

Skeletal Fluorosis
• Early stages of skeletal fluorosis start with pain in bones and joints, muscle weakness, sporadic pain, stiffness of joints and chronic fatigue.
• During later stages, calcification of the bones takes place, osteoporosis in long bones, and symptoms of osteosclerosis where the bones become denser and develop abnormal crystalline structure.

Skeletal Fluorosis
• In the advanced stage the bones and joints become completely weak and moving them is difficult.
• The vertebrae in the spine fuse together and the patient is left crippled which is the final stage.
• Neurological symptoms developed in the form of radiculopathy or myelopathy due to mechanical compression of the spinal card any multiple level.

Severity classification of skeletal fluorosis by Teotia et al:Mild: Clinical: Generalised bone and joint pains. Radiology: Only osteosclerosis.Moderate:Clinical: As above + Stiffness, rigidity and restricted movements at spine and joints. Radiology: As above + Periosteal bone formation, dense cortex, loss of trabecular pattern, calcifications of interosseous membrane and ligaments.Severe:Clinical: As above + Flexion deformities at spine and joints (hips, knees, elbows, hands), features of metabolic bone disease. Radilogy: As above + Osteophytosis, exostoses, Calcification of muscular attachments, tenons and capsules.Very Severe:Clinical: As above + Crippling deformities, neurological complications (radicular pains, muscle wasting, compression rediculo-myelopathy at cervical and lumbar regions, paraplegia, quadriplegia) and bed-ridden state. Radiology: As above + Metabolic bone disease (osteomalacia, pseudofractures, osteoporosis, hyperparathyroid bone disease), Calcification of neural arch and narrowing of spinal canal and intervertebral foramina.

Drinking water - fluorination
• More than 150 million people in the U.S. drink fluoridated water.
• 50 cities or towns in USA have withdrawn fluoride from supplies since 1990.
• Their legal limit, of four parts per million - is four times our legal limit.

Drinking Water - Fluorination Banned
• Fewer than 2 per cent of Europe's population have fluoridated water. Last year the Belgian government outlawed the sale of fluoride tablets and chewing gum.
• This was based on fears that it might increase the risk of osteoporosis.
• France, Italy, Germany, Sweden, Denmark and Holland have also rejected mass water fluoridation.
• There has also been mounting opposition to it in Ireland.

Fluoridation Linked To:
• Dental Fluorosis: Almost half of people drinking fluoridated water at permissible levels, one part per million, exhibit dental fluorosis. White and brown spots appear on the enamel of the teeth - causing an unsightly 'mottled' effect.
• This is the first sign that fluoride has poisoned enzymes in the body. Some dentists understandably question the wisdom of preventing dental disease in one in six people, only to cause it in one in two.

Fluoridation Linked To:
• Skeletal Fluorosis: - symptoms include pains in the bones and joints, muscle weakness and gastrointestinal disorders - may occur in people who have ingested 10-20mg of fluoride per day for 10 to 20 years (equivalent to 2.5-5 mg per day for 40-80 years). In the most severe cases, the spine becomes completely rigid.
• Osteoporosis: Although fluoride exposure results in denser bones, the bone appears to be weaker than normal bone. Scientists in America have reported that fluoride in strengths as little as 1 part per million decreases bone strength and elasticity.

Fluoridation Linked To:• 1992, a study of elderly patients in Utah found 'a small but significant
increase' in the risk of hip fracture in both men and women.• 1992, a study by the New Jersey Department of Health in the U.S.
found a strong link between fluoridation and osteosarcoma in young males. They reported that osteosarcoma rates were three to seven times higher in fluoridated areas than non-fluoridated areas.
• This disease is routinely found to be more common in males than in females due to it’s interfere with the testosterone.
• Kidney Stones: 4.6 times more common in an area with high fluoride (3.5 to 4.9 ppm) than in a similar area without high fluoride.
• Moreover, in the high fluoride area, the prevalence of kidney stones 'was almost double in subjects with fluorosis than without fluorosis‘.

Case report
• A 45 female from Kota Rajasthan.• Obese, Peri-menopausal, Hypothyroid, &
Hypertensive.• C/o – chronic backache for last 2 years,
cramps, leg pains, parasthesia Rt > lt.• Claudication distance about 10 meters, can
stand for 5 minutes.• No bladder problem.

Case report – cont….
• On Exam – Spinal movements were limited.• SLRT – negative.• Hips, Knees, and Ankle movements normal.• All deep jerks were brisk.• Planter reflex equivocal.• Can stand and walk on heels and toes.• Referred to Neurologist for possible
myelopathy.

Case report – cont….
• X-ray of Chest.• X- Both fore arms - AP• MRI of Dorsal and Lumbar Spine.• CBC, serum Creatinine, TSH, PTH, Ca, Alk Po4,
Urine routine.











Treatment
• Calcium.• Vitamin D.• Vitamin C.• Use of tape water/ river water, deep well.• Use of water filter.• Physiotherapy• Continuous follow ups.

DISCLAIMER • Information contained and transmitted by this presentation is based on
personal experience and collection of cases at Choithram Hospital & Research centre, Indore, India.
• Some representative x-rays & text have taken from an article “Highlights of Forty Years of Research on Endemic Skeletal Fluorosis in India - S P S Teotia *, M Teotia and K P Singh, India.
• It is intended for use only by the students of orthopaedic surgery. Views and opinion expressed in this presentation are personal opinion. Depending upon the x-rays and clinical presentations viewers can make their own opinion. For any confusion please contact the sole author for clarification. Every body is allowed to copy or download and use the material best suited to him. I am not responsible for any controversies arise out of this presentation. For any correction or suggestion please contact [email protected]