Embed Size (px)
Citation preview

Endoscopic Histologic Mapping of a Mixed Germ Pineal Tumor
Carlos Velasquez1, Monica Rivero-Garvıa2, Eloy Rivas3, Marıa de los Angeles Canizares4, Marıa Jose Mayorga-Buiza5,Javier Marquez-Rivas2
INTRODUCTIONPineal region tumors account for 2.5%e5%of intracranial tumors in children, 50%e70% of which are germ cell tumors(GCTs).1 Their accurate diagnosis isimportant for determining the treatmentstrategy and prognosis2,3 especially in themixed GCT subgroup, in which theidentification of all the tumoral histologiccomponents represents a real challengefor the neuropathologist.4
Despite the technical advances in neu-roimaging techniques, radiologic findingsare not specific enough for differentialdiagnosis.5,6 Current neuroendoscopicapproaches allow for a tumoral biopsy tobe performed, although several technical
questions remain about the procedure anddifferent negative biopsy rates have beendescribed,7,8 most being those with a lownumber of samples and limited to a smalltumoral area.We describe a pineal mixed GCT histo-
logic mapping procedure through anendoscopic supraorbital approach andoutline the technical pitfalls that need to beovercome to obtain an accurate diagnosis.
CASE DESCRIPTION
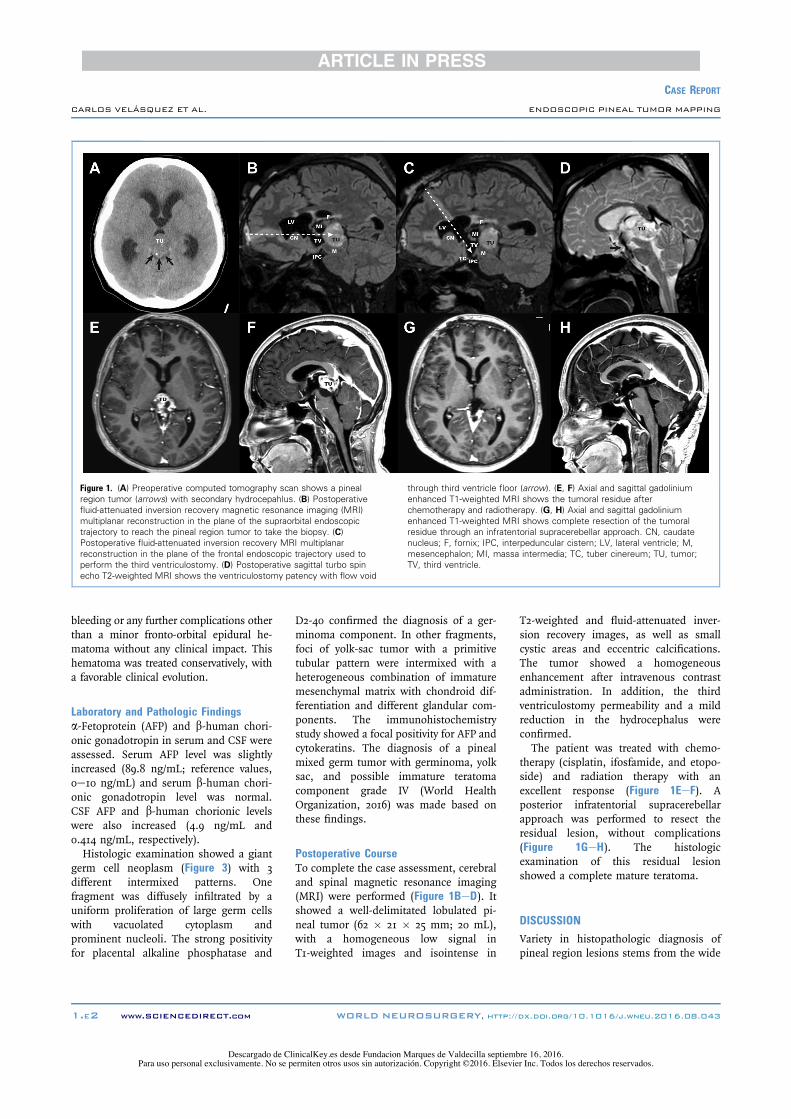
History and ExaminationA 13-year-old male with no previous medi-cal history was admitted to the emergencydepartment with headache and seizures. Inthe previous month, he had had 3 gener-alized, self-limited, tonic episodes withconsciousness impairment, the last onejust before admission. On admission, hehad mild consciousness impairmentwithout any motor or sensory focal signs.Computed tomography (Figure 1A) showeda large pineal tumor with secondarysupratentorial hydrocephalus. Based onhis clinical and radiologic features, thepatient underwent an urgent endoscopicventriculostomy and biopsy.
OperationAn endoscopic echo-guided dual approachwas chosen using a 2 burr-hole strategy with2 different rigid endoscopes. Burr holeswere enlarged to obtain minicraniotomieson both sides. Ventriculostomy was per-formed with a standard procedure4 througha right precoronal frontal minicraniotomyto access the tuber cinereum in the floorof the third ventricle with a 6-mm-diam-eter endoscope and a 0! lens (Minop [Aes-culap, Center Valley, Pennsylvania, USA]).At this stage, cerebrospinal fluid (CSF)samples for microbiology, biochemistry,and tumoral markers were collected. Asecond, more anterior, ipsilateral supraor-bital minicraniotomy was used to reach thepineal tumor through the Monro foraminain the posterior part of the third ventriclewith an 8-mm-diameter endoscope with a30! lens (Minop InVent [Aesculap]).Once the tumor was reached, several
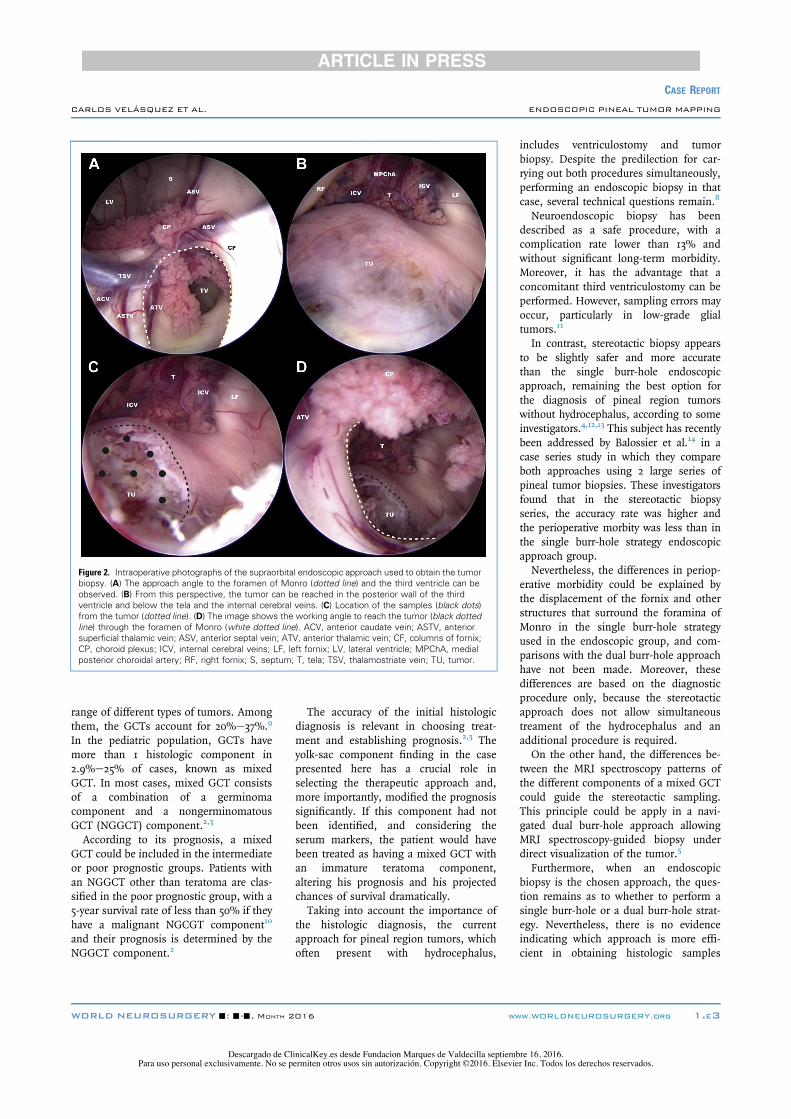
samples were taken using a multibiopsyapproach (Figure 2) to map the tumorhistologically and therefore enhance thepathologic diagnosis.Fifteen small tumor fragments were
extracted, proceeding in a clockwise direc-tion. The postoperative computed tomog-raphy scan did not show intraparenchymal
-BACKGROUND: The accurate histologic diagnosis of germ cell tumors in thepineal region is a keystone for determining the best treatment strategy andprognosis. This situation poses a challenge for the neuropathologist, consideringthe lack of a standarized procedure to obtain biopsy samples, which results infew and small specimens, which are not suitable for diagnosis.
-CASE DESCRIPTION: We report a case in which a pineal region mixed germcell tumor was accurately diagnosed by performing histologic mapping througha dual burr-hole endoscopic approach. The technical pitfalls and other con-siderations necessary for obtaining an accurate diagnosis in this tumor sub-group are specified. In addition, the histologic analysis regarding the samplingtechnique used is described.
-CONCLUSIONS: The supraorbital frontal endoscopic approach enables thesurgeon to perform histologic mapping of pineal region tumors, allowingstandarization of the procedure used to obtain the specimens. This approach couldresult in a more accurate diagnosis, especially in mixed germ cell neoplasms.
Key words- Biopsy- Disgerminoma- Endoscopy- Pineal tumor- Ventriculostomy- Yolk sac
Abbreviations and AcronymsAFP: a-FetoproteinCSF: Cerebrospinal fluidGCT: Germ cell tumorMRI: Magnetic resonance imagingNGGCT: Nongerminomatous germ cell tumor
From the 1Department of Neurological Surgery and SpineUnit, Hospital Universitario Marqués de Valdecilla andFundación Instituto de Investigación Marqués de Valdecilla(IDIVAL), Santander; Departments of 2Neurosurgery,3Pathology, and 4Pediatric Anesthesiology, HospitalesUniversitarios Virgen del Rocio, Seville; and 5Departmentof Neurosurgery, Complejo Hospitalario de Toledo, Toledo,Spain
To whom correspondence should be addressed:Javier Márquez-Rivas, M.D., Ph.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2016).http://dx.doi.org/10.1016/j.wneu.2016.08.043
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2016 Elsevier Inc. Allrights reserved.
WORLD NEUROSURGERY-: ---, MONTH 2016 www.WORLDNEUROSURGERY.org 1.E1
Case Report
Descargado de ClinicalKey.es desde Fundacion Marques de Valdecilla septiembre 16, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.
bleeding or any further complications otherthan a minor fronto-orbital epidural he-matoma without any clinical impact. Thishematoma was treated conservatively, witha favorable clinical evolution.
Laboratory and Pathologic Findingsa-Fetoprotein (AFP) and b-human chori-onic gonadotropin in serum and CSF wereassessed. Serum AFP level was slightlyincreased (89.8 ng/mL; reference values,0e10 ng/mL) and serum b-human chori-onic gonadotropin level was normal.CSF AFP and b-human chorionic levelswere also increased (4.9 ng/mL and0.414 ng/mL, respectively).Histologic examination showed a giant
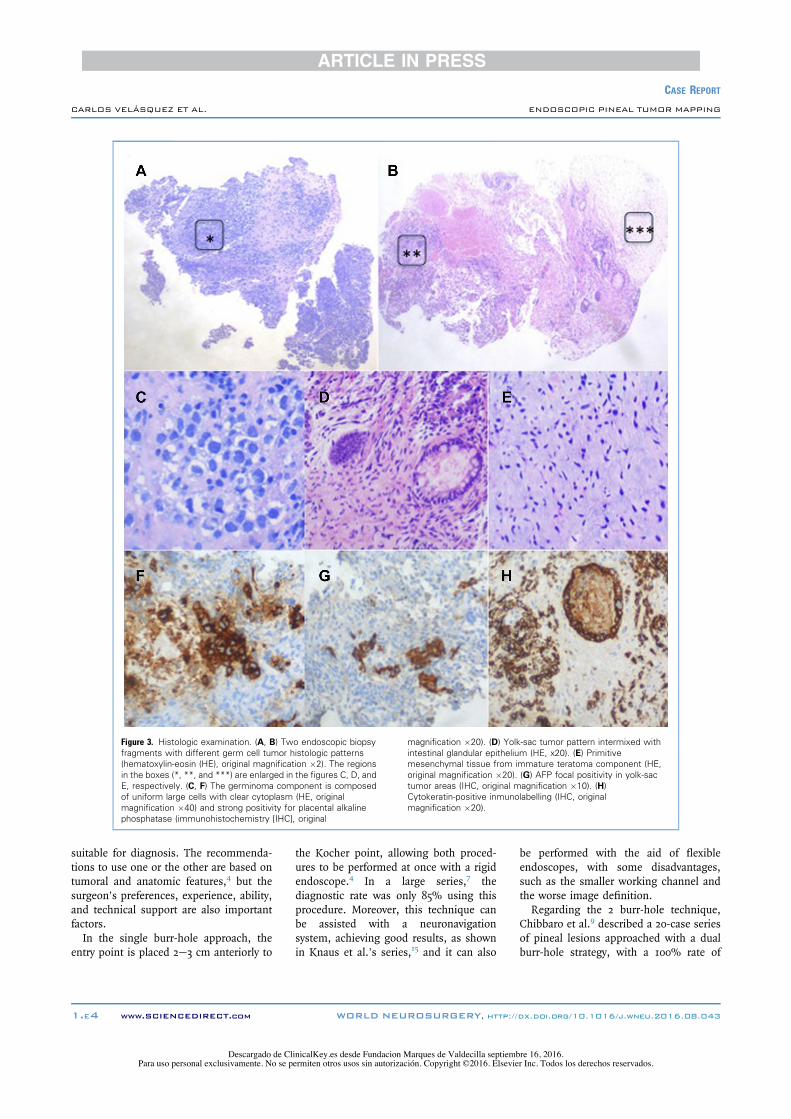
germ cell neoplasm (Figure 3) with 3different intermixed patterns. Onefragment was diffusely infiltrated by auniform proliferation of large germ cellswith vacuolated cytoplasm andprominent nucleoli. The strong positivityfor placental alkaline phosphatase and
D2-40 confirmed the diagnosis of a ger-minoma component. In other fragments,foci of yolk-sac tumor with a primitivetubular pattern were intermixed with aheterogeneous combination of immaturemesenchymal matrix with chondroid dif-ferentiation and different glandular com-ponents. The immunohistochemistrystudy showed a focal positivity for AFP andcytokeratins. The diagnosis of a pinealmixed germ tumor with germinoma, yolksac, and possible immature teratomacomponent grade IV (World HealthOrganization, 2016) was made based onthese findings.
Postoperative CourseTo complete the case assessment, cerebraland spinal magnetic resonance imaging(MRI) were performed (Figure 1BeD). Itshowed a well-delimitated lobulated pi-neal tumor (62 " 21 " 25 mm; 20 mL),with a homogeneous low signal inT1-weighted images and isointense in
T2-weighted and fluid-attenuated inver-sion recovery images, as well as smallcystic areas and eccentric calcifications.The tumor showed a homogeneousenhancement after intravenous contrastadministration. In addition, the thirdventriculostomy permeability and a mildreduction in the hydrocephalus wereconfirmed.The patient was treated with chemo-
therapy (cisplatin, ifosfamide, and etopo-side) and radiation therapy with anexcellent response (Figure 1EeF). Aposterior infratentorial supracerebellarapproach was performed to resect theresidual lesion, without complications(Figure 1GeH). The histologicexamination of this residual lesionshowed a complete mature teratoma.
DISCUSSIONVariety in histopathologic diagnosis ofpineal region lesions stems from the wide
Figure 1. (A) Preoperative computed tomography scan shows a pinealregion tumor (arrows) with secondary hydrocepahlus. (B) Postoperativefluid-attenuated inversion recovery magnetic resonance imaging (MRI)multiplanar reconstruction in the plane of the supraorbital endoscopictrajectory to reach the pineal region tumor to take the biopsy. (C)Postoperative fluid-attenuated inversion recovery MRI multiplanarreconstruction in the plane of the frontal endoscopic trajectory used toperform the third ventriculostomy. (D) Postoperative sagittal turbo spinecho T2-weighted MRI shows the ventriculostomy patency with flow void
through third ventricle floor (arrow). (E, F) Axial and sagittal gadoliniumenhanced T1-weighted MRI shows the tumoral residue afterchemotherapy and radiotherapy. (G, H) Axial and sagittal gadoliniumenhanced T1-weighted MRI shows complete resection of the tumoralresidue through an infratentorial supracerebellar approach. CN, caudatenucleus; F, fornix; IPC, interpeduncular cistern; LV, lateral ventricle; M,mesencephalon; MI, massa intermedia; TC, tuber cinereum; TU, tumor;TV, third ventricle.
1.E2 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, http://dx.doi.org/10.1016/j.wneu.2016.08.043
CASE REPORT
CARLOS VELÁSQUEZ ET AL. ENDOSCOPIC PINEAL TUMOR MAPPING
Descargado de ClinicalKey.es desde Fundacion Marques de Valdecilla septiembre 16, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.
range of different types of tumors. Amongthem, the GCTs account for 20%e37%.9
In the pediatric population, GCTs havemore than 1 histologic component in2.9%e25% of cases, known as mixedGCT. In most cases, mixed GCT consistsof a combination of a germinomacomponent and a nongerminomatousGCT (NGGCT) component.2,3
According to its prognosis, a mixedGCT could be included in the intermediateor poor prognostic groups. Patients withan NGGCT other than teratoma are clas-sified in the poor prognostic group, with a5-year survival rate of less than 50% if theyhave a malignant NGCGT component10
and their prognosis is determined by theNGGCT component.2
The accuracy of the initial histologicdiagnosis is relevant in choosing treat-ment and establishing prognosis.2,3 Theyolk-sac component finding in the casepresented here has a crucial role inselecting the therapeutic approach and,more importantly, modified the prognosissignificantly. If this component had notbeen identified, and considering theserum markers, the patient would havebeen treated as having a mixed GCT withan immature teratoma component,altering his prognosis and his projectedchances of survival dramatically.Taking into account the importance of
the histologic diagnosis, the currentapproach for pineal region tumors, whichoften present with hydrocephalus,
includes ventriculostomy and tumorbiopsy. Despite the predilection for car-rying out both procedures simultaneously,performing an endoscopic biopsy in thatcase, several technical questions remain.8
Neuroendoscopic biopsy has beendescribed as a safe procedure, with acomplication rate lower than 13% andwithout significant long-term morbidity.Moreover, it has the advantage that aconcomitant third ventriculostomy can beperformed. However, sampling errors mayoccur, particularly in low-grade glialtumors.11
In contrast, stereotactic biopsy appearsto be slightly safer and more accuratethan the single burr-hole endoscopicapproach, remaining the best option forthe diagnosis of pineal region tumorswithout hydrocephalus, according to someinvestigators.4,12,13 This subject has recentlybeen addressed by Balossier et al.14 in acase series study in which they compareboth approaches using 2 large series ofpineal tumor biopsies. These investigatorsfound that in the stereotactic biopsyseries, the accuracy rate was higher andthe perioperative morbity was less than inthe single burr-hole strategy endoscopicapproach group.Nevertheless, the differences in periop-
erative morbidity could be explained bythe displacement of the fornix and otherstructures that surround the foramina ofMonro in the single burr-hole strategyused in the endoscopic group, and com-parisons with the dual burr-hole approachhave not been made. Moreover, thesedifferences are based on the diagnosticprocedure only, because the stereotacticapproach does not allow simultaneoustreament of the hydrocephalus and anadditional procedure is required.On the other hand, the differences be-
tween the MRI spectroscopy patterns ofthe different components of a mixed GCTcould guide the stereotactic sampling.This principle could be apply in a navi-gated dual burr-hole approach allowingMRI spectroscopy-guided biopsy underdirect visualization of the tumor.5
Furthermore, when an endoscopicbiopsy is the chosen approach, the ques-tion remains as to whether to perform asingle burr-hole or a dual burr-hole strat-egy. Nevertheless, there is no evidenceindicating which approach is more effi-cient in obtaining histologic samples
Figure 2. Intraoperative photographs of the supraorbital endoscopic approach used to obtain the tumorbiopsy. (A) The approach angle to the foramen of Monro (dotted line) and the third ventricle can beobserved. (B) From this perspective, the tumor can be reached in the posterior wall of the thirdventricle and below the tela and the internal cerebral veins. (C) Location of the samples (black dots)from the tumor (dotted line). (D) The image shows the working angle to reach the tumor (black dottedline) through the foramen of Monro (white dotted line). ACV, anterior caudate vein; ASTV, anteriorsuperficial thalamic vein; ASV, anterior septal vein; ATV, anterior thalamic vein; CF, columns of fornix;CP, choroid plexus; ICV, internal cerebral veins; LF, left fornix; LV, lateral ventricle; MPChA, medialposterior choroidal artery; RF, right fornix; S, septum; T, tela; TSV, thalamostriate vein; TU, tumor.
WORLD NEUROSURGERY-: ---, MONTH 2016 www.WORLDNEUROSURGERY.org 1.E3
CASE REPORT
CARLOS VELÁSQUEZ ET AL. ENDOSCOPIC PINEAL TUMOR MAPPING
Descargado de ClinicalKey.es desde Fundacion Marques de Valdecilla septiembre 16, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.
suitable for diagnosis. The recommenda-tions to use one or the other are based ontumoral and anatomic features,4 but thesurgeon’s preferences, experience, ability,and technical support are also importantfactors.In the single burr-hole approach, the
entry point is placed 2e3 cm anteriorly to
the Kocher point, allowing both proced-ures to be performed at once with a rigidendoscope.4 In a large series,7 thediagnostic rate was only 85% using thisprocedure. Moreover, this technique canbe assisted with a neuronavigationsystem, achieving good results, as shownin Knaus et al.’s series,15 and it can also
be performed with the aid of flexibleendoscopes, with some disadvantages,such as the smaller working channel andthe worse image definition.Regarding the 2 burr-hole technique,
Chibbaro et al.9 described a 20-case seriesof pineal lesions approached with a dualburr-hole strategy, with a 100% rate of
Figure 3. Histologic examination. (A, B) Two endoscopic biopsyfragments with different germ cell tumor histologic patterns(hematoxylin-eosin (HE), original magnification "2). The regionsin the boxes (*, **, and ***) are enlarged in the figures C, D, andE, respectively. (C, F) The germinoma component is composedof uniform large cells with clear cytoplasm (HE, originalmagnification "40) and strong positivity for placental alkalinephosphatase (immunohistochemistry [IHC], original
magnification "20). (D) Yolk-sac tumor pattern intermixed withintestinal glandular epithelium (HE, x20). (E) Primitivemesenchymal tissue from immature teratoma component (HE,original magnification "20). (G) AFP focal positivity in yolk-sactumor areas (IHC, original magnification "10). (H)Cytokeratin-positive inmunolabelling (IHC, originalmagnification "20).
1.E4 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, http://dx.doi.org/10.1016/j.wneu.2016.08.043
CASE REPORT
CARLOS VELÁSQUEZ ET AL. ENDOSCOPIC PINEAL TUMOR MAPPING
Descargado de ClinicalKey.es desde Fundacion Marques de Valdecilla septiembre 16, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

succesful biopsies. The accurate diagnosisin the case presented could be related tothe 2 burr-hole rigid endoscope approachused (Figure 1CeD). The resultingworking angle and a large workingchannel endoscope that allows moreefficient instrument movements enablethe surgeon to perform histologicmapping of the tumor with accuratecontrol of the sample sites (Figure 2C).Among other advantages, it reduces therisk of fornix damage with less tissuedisplacement.16 In addition, it allows afrontal visualization of the tumor,whereas the angle with a single burr-holenecessitates samples to be taken from itsinferior part. Endoscope-assisted naviga-tion over MRI spectroscopy is possible.Considering that the particular hetero-
geneity of mixed GCT makes it difficult toobtain an accurate diagnosis in smallspecimens,4 the number of tissue samplestaken and the strategy for obtaining themare significant technical factors. It is notclear if taking more samples results in amore accurate diagnosis withoutincreasing complications. Besides, thenumber of samples is not standardized,as can be seen from several case series,in which the number of samples rangesfrom 1 to 12 specimens. Furthermore,high variability between patients, withseveral patients with an undeterminednumber of tissue samples, can beobserved.7,9,11
Regarding the number of tissue sam-ples, those series with a high and standardnumber, as in that reported by Chibbaroet al.,9 reached the histologic diagnosis inall cases, and in a large series reported byAhmed et al.,7 with a high variability in thenumber of tissue samples, the negativehistologic diagnosis rate was 16%.Despite the fact that comparison betweenthese studies is impossible because oftheir methodological differences,increasing the number of samples,among other measures, could reducesample error, as Ahmed et al. themselvesproposed.7
The histologic analysis of the samplestaken in this case showed a yolk-sac tumorcomponent in just 2 of 15 specimens, lessthan 15% of the tissue samples, thus
indicating the importance of increasingthe number of samples typically taken.Furthermore, the procedure for obtainingthe samples is not standardized, leadingto difficulties in the consistency of thediagnosis and comparison between series.Standardized histologic mapping of thetumor, as performed in the case pre-sented, could be an effective way ofreducing the impact of these issues.
CONCLUSIONSThe supraorbital frontal endoscopicapproach allows the surgeon to performhistologic mapping of pineal regiontumors. This technique enables standari-zation of the procedure used to obtain thespecimens, resulting in more representa-tive samples. This approach could result ina more accurate diagnosis, especially inmixed germ cell neoplasms.
ACKNOWLEDGMENTSWe would like to thank Lilian Vargas andPhil Woodall for reviewing the manuscriptand for their valuable comments.
REFERENCES1. Villano JL, Propp JM, Porter KR, Stewart AK,
Valyi-Nagy T, Li X, et al. Malignant pineal germ-cell tumors: an analysis of cases from threetumor registries. Neuro Oncol. 2008;10:121-130.
2. Echevarría ME, Fangusaro J, Goldman S. Pediatriccentral nervous system germ cell tumors: a review.Oncologist. 2008;13:690-699.
3. Gao Y, Jiang J, Liu Q. Clinicopathological andimmunohistochemical features of primary centralnervous system germ cell tumors: a 24-yearexperience. Int J Clin Exp Pathol. 2014;7:6965-6972.
4. Azab WA, Nasim K, Salaheddin W. An overviewof the current surgical options for pineal regiontumors. Surg Neurol Int. 2014;5:39.
5. Deiana G, Mottolese C, Hermier M, Louis-Tisserand G, Berthezene Y. Imagery of pinealtumors. Neurochirurgie. 2015;61:113-122.
6. Dumrongpisutikul N, Intrapiromkul J,Yousem DM. Distinguishing between germi-nomas and pineal cell tumors on MR imaging.AJNR Am J Neuroradiol. 2012;33:550-555.
7. Ahmed AI, Zaben MJ, Mathad NV, Sparrow OC.Endoscopic biopsy and third ventriculostomy forthe management of pineal region tumors. WorldNeurosurg. 2015;83:543-547.
8. Morgenstern PF, Osbun N, Schwartz TH,Greenfield JP, Tsiouris AJ, Souweidane MM. Pi-neal region tumors: an optimal approach forsimultaneous endoscopic third ventriculostomyand biopsy. Neurosurg Focus. 2011;30:E3.
9. Chibbaro S, Di Rocco F, Makiese O, Reiss A,Poczos P, Mirone G, et al. Neuroendoscopicmanagement of posterior third ventricle and pi-neal region tumors: technique, limitation, andpossible complication avoidance. Neurosurg Rev.2012;35:331-338.
10. Kamoshima Y, Sawamura Y. Update on currentstandard treatments in central nervous systemgerm cell tumors. Curr Opin Neurol. 2010;23:571-575.
11. Constantini S, Mohanty A, Zymberg S,Cavalheiro S, Mallucci C, Hellwig D, et al. Safetyand diagnostic accuracy of neuroendoscopic bi-opsies: an international multicenter study.J Neurosurg Pediatr. 2013;11:704-709.
12. Balossier A, Blond S, Touzet G, Lefranc M, deSaint-Denis T, Maurage CA, et al. Endoscopicversus stereotactic procedure for pineal tumourbiopsies: Comparative review of the literature andlearning from a 25-year experience. Neurochirurgie.2015;61:146-154.
13. Lefranc M, Touzet G, Caron S, Maurage CA,Assaker R, Blond S. Are stereotactic sample bi-opsies still of value in the modern management ofpineal region tumours? Lessons from a single-department, retrospective series. Acta Neurochir(Wien). 2011;153:1111-1121.
14. Balossier A, Blond S, Reyns N. Endoscopic versusstereotactic procedure for pineal tumor biopsies:focus on overall efficacy. World Neurosurg. 2016;92:223-228.
15. Knaus H, Matthias S, Koch A, Thomale UW.Single burr hole endoscopic biopsy with thirdventriculostomy-measurements and computer-assisted planning. Childs Nerv Syst. 2011;27:1233-1241.
16. Zhu XL, Gao R, Wong GK, Wong HT, Ng RY,Yu Y, et al. Single burr hole rigid endoscopic thirdventriculostomy and endoscopic tumor biopsy:what is the safe displacement range for the fora-men of Monro? Asian J Surg. 2013;36:74-82.
Conflict of interest statement: The authors declare that thearticle content was composed in the absence of anycommercial or financial relationships that could be construedas a potential conflict of interest.
Received 6 July 2016; accepted 10 August 2016
Citation: World Neurosurg. (2016).http://dx.doi.org/10.1016/j.wneu.2016.08.043
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2016 Elsevier Inc. Allrights reserved.
WORLD NEUROSURGERY-: ---, MONTH 2016 www.WORLDNEUROSURGERY.org 1.E5
CASE REPORT
CARLOS VELÁSQUEZ ET AL. ENDOSCOPIC PINEAL TUMOR MAPPING
Descargado de ClinicalKey.es desde Fundacion Marques de Valdecilla septiembre 16, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.