Embed Size (px)
Citation preview

April 2008
MANAGEMENT OF CHRONIC COUGH
HUEH 2011
TERRY FLOTTE, MD
Primary source:Murray and Nadel’sTextbook of Respiratory Medicine 2010

December 2010
ORIGIN OF COUGH REFLEX
• Irritant receptors of the airways via Cranial Nerve 10– Larynx
– Trachea
– Bronchi
• Rarely, referred from external ear due to Vagus innervation– foreign body in external auditory meatus



COMMON DIFFERENTIAL OF COUGH
• Upper airway
– Post-nasal drainage• Viral URI
• Allergic rhinitis
• Sinusitis
– Gastro-esophageal Reflux Disease
– Direct aspiration
• Lower airway
– Infectious• Pneumonia (bacterial, viral, mycoplasma, chlamydia)
• Bronchiolitis (RSV, metapneumovirus)
• Influenza, parainfluenza, Adeno, measles
• TB
• Pertussis
• HIV
– Environmental irritant
• Wood-burning
• Other environmental
– Asthma
– Aspirated foreign body
– Cystic fibrosis or immune defects
– Tumors and malformations

December 2010
MAJOR POINTS FROM HISTORY AND PHYSICAL
• Acute vs. chronic
– Acute: pneumonia, URI, other infections
• Upper vs. lower origin
– Upper: sinusitis, allergy,viral URI, GERD, aspiration
• Systemically ill vs. not systemically ill
– Systemic: TB, HIV, immune defects and CF
• Digital clubbing indicates chronic hypoxemia

December 2010
CASE
• 3 year old child with fever, tachypnea, cough progressing over last 4 days
• Exam RR60, T40.3C, Pulse ox 94%
• Crackles over right axilla, increased whispered pectorloqy, bronchial breath sounds


December 2010
MANAGEMENT OF ACUTELOWER RESPIRATORY TRACT
INFECTION
• Rule-out and treat malnutrition
• Evaluate for signs of sepsis or acute decompensation– In this case, stabilize, give first dose IM and ship to hospital
• Oral therapy with TMP/sulfa or amoxicillin
• Parenteral therapy with Amp/Pen and Gentamicin or Ceftriaxone

CHRONIC COUGH• With Sputum
– Chronic irritants (COPD in adults)
– TB
– Immune Defect, CF, cilia defect
– Bronchiectasis due to any of above, long-term aspirated foreign body
– Untreated pneumonia with abscess
– Rarely asthma
• Without sputum
– Asthma
– Chronic irritants
– Recent foreign body
– TB
– Upper airway sources

December 2010
CASE
• 6 yo with 5 month history of cough, weight loss, some night sweats, swallowing sputum
• Few anterior crackles on exam, very thin
• Tests? Differential?


December 2010
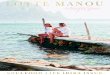
RISK OF PULMONARY AND EXTRAPULMONARY DISEASE IN TB
BY AGERisk of Disease Following Primary Infection Comments
Age Disseminated TB or Meningitis
Pulmonary TB
No Disease
<1 year 10-20% 30-40% 50% High morbidity
1-2 years 2-5% 10-20% 75-80% High morbidity
2-5 years 0-5% 5% 95%
5-10 years <0.5% 2% 98% Safe School years
> 10 years <0.5% 10-20% 80-90% Effusions or adult type pulmonary disease

December 2010
DIAGNOSIS OF TB• Tuberlin Skin Test (PPD) reactivity
– False positives due to BCG (altered criteria)
– False negatives due to anergy
• Acid-fast stain and/or culture (very poor sensitivity, 10 to 15%– Sputum
– Gastric aspirates
• Clinical– Radiographic pattern (hilar adenopathy, disseminated pattern,
effusion)
– Chronic history with fever, cough, weight loss, night sweats
– Exposure history
– Risk factors: HIV, overcrowding, local prevalence

December 2010
TB PREVENTION
• Prophylaxis for children in home of TB-infected adult
• BCG
• ? New vaccines

December 2010
CASE
• 10 year old with history of recurrent cough, dyspnea while playing soccer (?futbol?), nocturnal cough during episodes of rhinorrhea
• Exam normal, no digital clubbing
• Differential diagnosis? Studies? Medication trial?



December 2010
CASE
• 7 year old presents with 3 month history of cough
• History of when it first began reveals sudden onset of severe cough, no rhinorrhea or other prodrome, no fever
• Exam reveals differential wheezing right>left
• Further questions?
• X-ray Exams? Differential?

Ou est l’arachide?

December 2010
SPECIAL CASES
• Recurrent pneumonias, X-ray proven (see following)
• Chronic cough with sputum production
– Chronic irritant
– Immune Defect
– TB
– Less common with asthma
• Digital clubbing

RISK FACTORS FOR PNEUMONIAMORBIDITY AND MORTALITY
(WHO-GAPP)
• Nutritional deficiency– Shortened breast-
feeding time
– Underweight
– Zinc deficiency
• Indoor air pollution– Wood-burning
– Tobacco smoke
– Urban air pollution
• Immunization status (measles, pertussis, Hib, Pneumococcus)
• Case Management– Prompt detection and
Antibiotic therapy
• HIV status

© 2002 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 3
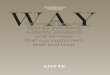
Table 2Evaluation of children with recurrent pneumonia diagnosed by World Health Organization criteria.HEFFELFINGER, JAMES; DAVIS, TIMOTHY; GEBRIAN, BETTE; BORDEAU, ROYNELD; SCHWARTZ, BEN; DOWELL, SCOTT
Pediatric Infectious Disease Journal. 21(2):108-112, February 2002.
Table 2 . Clinical findings* Chest radiographs revealed infiltrates.NS, not significant.

December 2010
EVALUATION OF CHILDREN WITH RECURRENT PNEUMONIA IN HAITI
• Heffelfinger, et al., Peds Inf Dis Journal 2002
– Screened for TB, immune deficiency, HIV
– Most were sporadic
– Only association was with Asthma, but this was a minority of cases

CASE
• 8 year old with history of three distinct episodes of right upper lobe pneumonia

PULMONARY SEQUESTRATION
• One of several congenital malformations that can lead to recurrent pneumonia at a single location– Congenital cystic
adenomatoid malformations
– Bronchogenic cysts
• Abnormal blood supply and lacks normal bronchial connection