Embed Size (px)
Citation preview

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2013) 48, E5–E7
Apple-peel intestinal atresia: Enteroplasty for intestinallengthening and primary anastomosisLuciano Silveira Onofre⁎, Renato Frota de Albuquerque Maranhão,Elaine Cristina Soares Martins, Camila Girardi Fachin, Jose Luiz Martins
Department of Pediatric Surgery, Universidade Federal de São Paulo, Unifesp, Brazil
Received 26 November 2012; revised 29 April 2013; accepted 29 April 2013
C
0h
Key words:Apple-peel intestinalatresia;Intestinal lengtheningprocedure;Tailoring procedure
Abstract Apple-peel atresia (or Type-IIIb intestinal atresia) is an unusual type of jejunoileal atresia.They present with jejunal atresia near the ligament of Treitz and a foreshortened small bowel. Manysurgical options have been used, but the optimal method of repair remains unclear. We present a case ofa newborn with apple-peel intestinal atresia managed by enteroplasty for intestinal lengthening andprimary anastomosis.© 2013 Elsevier Inc. All rights reserved.
Infants born with jejunoileal atresia have considerable Intestinal-lengthening procedures are rarely used as the
dilatation of the intestine proximal to the obstruction, and thedistal segment of intestine is collapsed. When the dilatatedproximal intestine is anastomosed to the distal, persistentfunctional bowel obstruction occurs even though theanastomosis is widely patent [1]. In cases of proximaljejunal atresia with adequate length of intestine, resection ofthe dilatated atretic segment and end-to-end anastomosisobviates these complications. When there is limitated lengthof remaining intestine, an antimesenteric reduction-taperingjejunoplasty has proved useful [2]. Nevertheless some casesof intestinal atresia are associated with a loss of a sizeablesegment of the small bowel, frequently the case in apple-peelatresia (type-IIIb intestinal atresia). The requisite resection toadjust anastomotic openings and avoid the functionalobstruction of the bowel in these patients can compromisethe absorptive area of the intestine and increase the incidenceof short-bowel syndrome.⁎ Corresponding author. Rua Baltazar Lisboa, , São Paulo-SP, BrazilEP 04110–060. Tel.: +55 11 98209 9938; fax: +55 11 5908 1665.E-mail address: [email protected] (L.S. Onofre).
022-3468/$ – see front matter © 2013 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.jpedsurg.2013.04.024
primary correction in these cases. The authors present thecorrection of apple-peel intestinal atresia through entero-plasty using a flap on the antimesenteric border from thedilated blind proximal segment of intestine for intestinallengthening and primary anastomosis. This procedure isbased on application of the technique initially described by J.Ten Kate to correct long gap esophageal atresia [3]. By usingthis technique, we simultaneously managed a tailoringprocedure that promote intestinal lengthening and primaryanastomosis without a significant loss of the absorptive area.
1. Case report
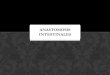
A two-day old female newborn with a gestational age of35 weeks was admitted with a diagnosis compatible withintestinal obstruction. The child's birth weight was 2600 g.The patient underwent a laparotomy, which resulted in adiagnosis of apple-peel intestinal atresia (Fig. 1). The dilatedproximal bowel segment from the duodenal junction to the

Fig. 1 Apple-peel intestinal atresia diagnosed in a newborn withintestinal obstruction.
ig. 2 The line of incision in the dilatated blind proximalegment of intestine is marked, the arrow demonstrating theirection the flap will turn. The proximal segment is tabularizedith a funnel-effect leading down to the anastomotic opening. End--end anastomosis without significant loss of the absorptive area.
E6 L.S. Onofre et al.
site of atresia measured 30 cm in length and 10 cm indiameter. The distal small bowel segment from the ileocecalvalve expressing features of atresia measured approximately20 cm in length.
Due to concern about the length of the intestine, thetechnique used to correct the defect consisted of creating aflap on the antimesenteric border from the dilated blindproximal segment of intestine. This flap of the proximalintestinal segment measured 10 cm in length and had a basemeasuring 5 cm in length. The flap was turned down to thelower segment and tabularized employing a funnel-effectthat lead to the anastomotic opening with a 1.5 cm diameter.An end-to-end anastomosis was performed from thetubularized proximal segment to the distal intestinalsegment, as shown in Fig. 2.
This enteroplasty technique enabled to lengthen thedilatated proximal atretic segment by about a third of itsinitial length, promotes tailoring to avoid functionalobstruction, enabling anastomosis with adequate calibers tothe distal intestinal segment (Fig. 3).
There were no post-operative complications. The patientremained on total parenteral nutrition for a period of3 months until full enteral feeding was achieved. The patientis now a thriving seven year old, weighs 27 kilograms andmeasures 1 meter and 26 centimeters, and has 1–2 well-formed bowel movements a day. She is currently in theweight-for-age chart 73,4 percentile and in the body massindex-for-age chart 76,7 percentile, considered eutrophic(WHO child growth standards, reference 2007). No othersurgical procedures were required and there were noepisodes of bowel obstructions.
ig. 3 Enteroplasty for intestinal lengthening and primarynastomosis.
2. Discussion
When correcting intestinal atresia, we should not use thedilated proximal intestinal segment to reconstruct the
Fsdwto
intestinal tract without first somehow adjusting the caliber.Despite the segment’s producing vigorous peristalsis, itswalls do not adequately coapt, which results in lowintraluminal pressure. The resulting peristalsis is incapableof producing an adequate upstream pressure gradient [4].
Fa

E7Apple-peel intestinal atresia
The use of this segment is associated with an increase in afunctional bowel obstruction [3].
Many approaches can be taken to resolve this problem.Functional anastomosis is obtained through resection of thedilatated atretic proximal intestinal segment and end-to-endanastomosis; however this technique sacrifices an importantsegment of the absorptive intestinal surface [1,3,5]. As analternative, an antimesenteric reduction-tapering jejuono-plasty can be used to perform anastomosis, but this alsonegatively affects the absorptive area [6]. Tapering anti-mesenteric reduction jejuonoplasty of the dilated segmentensures effective anastomosis without the loss of intestinalmucosa, but this technique is more appropriate forobstructions and dehiscience in the suture [7].
Apple-peel atresia (or Type-IIIb intestinal atresia) is anunusual type of jejunoileal atresia. Its etiopathogenesisincludes the occurrence of mesenteric vascular accident afterthe emergence of the middle colic artery. They present withjejunal atresia near the ligament of Treitz, foreshortenedbowel, and a large mesenteric gap. The bowel distal to theatresia is precariously supplied in a retrograde fashion byanastomotic arcades from the ileocolic, right colic or inferiormesentery artery. Most of these children had less than halfof the normal length of the small bowel and had aphysiologically short bowel [7]. Many surgical optionshave been used, but the optimal method of repair remainsunclear. The ideal technique would enable intestinallengthening and primary anastomosis.
In 1952, J. Ten Kate described a technique to correct longgap esophageal atresia using a flap from the anterior wall ofthe esophagus. He showed that it was possible to lengthen thedilated proximal stump and to decrease anastomotic tension[8,9]. In this clinical case, we apply this principle to correct anapple-peel intestinal atresia. The length of the flap we createdmeasured one-third the length of the dilated proximalintestinal segment, and its base measured half the diameterof the dilated segment. It was designed with a funnel-effectleading to the anastomotic opening. The diameter of the distalportion of the flap was made to adjust the anastomoticopenings and ensured anastomosis with adequate diameter tothe distal intestinal segment. There was no impairment ofvascularization of the flap after its confection. However, hadthere been an ischemic segment of flap, this would have beenresected before the tubulization.
Serial transverse enteroplasty procedure (STEP) wasdescribed in 2003 by Kim et al for intestinal lengtheningof patients with short bowel syndrome [10,11]. Theprocedure also promotes intestinal lengthening and tapering
and is another viable option in the management of intestinalatresia [12,13]. STEP involves the use of a stapler, whichmay not be affordable for less affluent countries [14]. Serialtransverse enteroplasty in intestinal atresia management alsorequires an extensive proximal dilated intestinal segment[11]. The proposed technique of enteroplasty with a flapfrom the antimesenteric border is simpler than STEP,particularly when the stapler is simply not available.Furthermore, enteroplasty with a flap from the antimesen-teric border can be performed on any length of proximalintestinal segment, which is not the case for STEP.
The technique of enteroplasty with a flap from the anti-mesenteric border to correct apple-peel intestinal atresiaguarantees functional anastomosis without significant loss ofthe absorptive area. It is a simple operation and can be usedas an alternative in correcting intestinal atresia where othertechniques favor the occurrence of short bowel syndrome.
References
[1] De Lorimier AA, Norman DA, Gooding CA, et al. A model forcinefluoroscopic and manometric study of chronic intestinal obstruc-tion. J Pediatr Surg 1973;8:758-91.
[2] Grosfeld JL. Jejunoileal atresia and stenosis. In: O´Neill Jr JA, RoweMI, Grosfeld JL, Fonkalsrud EW, Coran AG, editors. Pediatricsurgery. 5 th ed. St Louis: Missouri Mosby-Year Book; 1998.p. 1145-58.
[3] Benson CD. Resection and primary anastomosis of the jejunum andileum in the newborn. Ann Surg 1955;142:478-85.
[4] Thomas Jr CD. Jejunoplasty for the correction of jejunal atresia. SurGynecol Obstrect 1969;129:545-6.
[5] De Lorimier AA, Harrison MR. J Intestinal plication in the treatment ofatresia. J Pediatr Surg 1983;18:734-7.
[6] Weitzman JJ, Vanderhoof RS. Jejunal atresia with agenesis of thedorsal mesentery with “Christmas tree” deformity of the smallintestine. Am J Surg 1966;11:443-9.
[7] Waldhausen JHT, Sawain R. Improved long-term outcome for patientswith jejunoileal apple peel atresia. J Pediatr Surg 1997;32:1308-9.
[8] Kate JT. A method of suturing in operations for congenitaloesophageal atresia. Arch Chir Neerl 1952;4:43-7.
[9] Gough MH. Esophageal atresia –Use of an anterior flap in the difficultanastomosis. J Pediatr Surg 1980;15:310-1.
[10] Kim HB, Fauza D, Garza J. Serial transverse enteroplasty (STEP): anovel bowel lenghtening procedure. J Pediatr Surg 2003;38:425-9.
[11] Kim HB, Lee PW, Garza J. Serial transverse enteroplasty for shortbowel syndrome: a case report. J Pediatr Surg 2003;38:881-5.
[12] Wales PW, Dutta S. Serial transverse enteroplasty for neonates withproximal jejuna atresia. J Pediatr Surg 2005;40:E31-4.
[13] Ismael A, Alkadhi A, Alnagaar O, et al. Serial transverse enteroplastyin intestinal atresia management. J Pediatr Surg 2005;40:E5-6.
[14] Sheth NP. Serial transverse enteroplasty.J Pediatr Surg 2005;40:1060[author reply 1060].