Embed Size (px)
Citation preview

8/3/2019 Lambda-Shaped Anastomosis With Intravascular Stenting Method for Safe and Effective Lymphaticovenular Anasto…
http://slidepdf.com/reader/full/lambda-shaped-anastomosis-with-intravascular-stenting-method-for-safe-and-effective 1/6
RECONSTRUCTIVE
Lambda-Shaped Anastomosis with IntravascularStenting Method for Safe and Effective
Lymphaticovenular AnastomosisTakumi Yamamoto, M.D.
Mitsunaga Narushima, M.D.Kazuki Kikuchi, M.D.
Hidehiko Yoshimatsu, M.D.Takeshi Todokoro, M.D.
Makoto Mihara, M.D.Isao Koshima, M.D.
Tokyo, Japan
Background: Lymphaticovenular anastomosis has become an increasingly com-mon treatment for lymphedema. Supermicrosurgical techniques are essentialfor the successful performance of lymphaticovenular anastomosis. A positivecorrelation between the number of lymphaticovenular anastomoses performedand therapeutic efficacy has been reported, and in performing these anasto-moses, the establishment of as many bypasses as possible is important.Methods: Forty limbs of 20 patients with lower extremity lymphedema whounderwent lymphaticovenular anastomosis in our department were assessed. Allcases were performed under local anesthesia using two to four surgical micro-scopes. A new method of anastomosis, lambda-shaped anastomosis assisted by
intravascular stenting, was chosen in required cases.Results: Lymphaticovenular anastomoses resulted in 186 anastomoses on 20 pa-tients with lower extremity lymphedema; the average number of anastomoses percase was 9.3 (range, five to 18). The number of surgical microscopes used rangedfrom two to four (average, 3.3), and the duration of the operation ranged from 3to 5 hours (average, 4.1). In the cases of lambda-shaped anastomosis (n 11), thenumber of anastomoses was significantly greater than in the cases without lambda-shaped anastomosis (n 9; 10.2 2.3 versus 8.2 1.4; p 0.05).Conclusions: Lambda-shaped anastomosis assisted by intravascular stenting is asafe and relatively easy method that can be performed by surgeons with less than1 year of experiencein microsurgery. Thisin turnallows efficient lymphaticovenularanastomoses to be performed simultaneously by a team of surgeons, resulting in anincreased number of bypasses. (Plast. Reconstr. Surg. 127: 1987, 2011.)
Management options for lymphedema in-clude both conservative methods, suchas compression therapy, and surgical
interventions.1– 8 Among the surgical procedures,lymphaticovenular anastomosis can be performedunder local anesthesia, is less invasive than othermethods, and is effective in severe cases refractory to compression therapy.9–15 These advantages havemade lymphaticovenular anastomosis an increasingly
common treatment for lymphedema. Supermicro-surgery, microsurgical techniques that allow
anastomoses of vessels less than 0.5 mm in di-ameter, are essential, however, for the successfulperformance of lymphaticovenular anastomo-sis, as is sufficient experience to identify func-tional lymphatic channels and to decide whichapproach to use.10–12,14,15
A positive correlation between the number of lymphaticovenular anastomoses performed andtherapeutic efficacy has been reported, and in
performing lymphaticovenular anastomoses, theestablishment of as many bypasses as possible isimportant.15 We established a new lymphatico- venular anastomosis technique, lambda-shapedanastomosis with intravascular stenting methods, which can be safely performed by surgeons withless than 1 year of experience in microsurgery. We
From the Department of Plastic and Reconstructive Surgery,Graduate School of Medicine, University of Tokyo.Received for publication September 13, 2010; accepted No- vember 22, 2010.Presented at the First European Conference on Supramicro- surgery, in Barcelona, Spain, March 5, 2010, and at the 10th Korea–Japan Congress of Plastic and Reconstructive Surgery, in Busan, Korea, June 16, 2010.Copyright ©2011 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31820cf5c6
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
www.PRSJournal.com

8/3/2019 Lambda-Shaped Anastomosis With Intravascular Stenting Method for Safe and Effective Lymphaticovenular Anasto…
http://slidepdf.com/reader/full/lambda-shaped-anastomosis-with-intravascular-stenting-method-for-safe-and-effective 2/6
elaborate on these methods and then provide datasupporting their significance for the efficient es-tablishment of lymphaticovenular anastomoses.
PATIENTS AND METHODS
We developed lambda-shaped anastomosis in which, first, the proximal end of the lymphatic chan-nel is anastomosed to the side of a venule, makingan end-to-side anastomosis. Next, an end-to-endanastomosis was made between the distal end of thelymphatic channel and the venule. This lambda-shaped anastomosis was clinically applied to patients with lymphedema of the lower extremities. FromMay to September of 2009 under a University of Tokyo Hospital institutional review boardap-proved protocol, we assessed 40 limbs of 20 patients with lower extremity lymphedema who underwent
lymphaticovenular anastomosis in our department (Table 1). All patients received conservative therapy,such as compression therapy with an elasticstocking,lymph drainage, or elastic bandage compression forat least 3 months, which resulted in no clinical im-provement. All cases were performed under localanesthesia using two to four surgical microscopes.To minimize movement of patients during the pro-cedure, urinary catheters were inserted in all pa-tients during operations, and 5-minute breaks weretaken to allow patients to move their bodies andextremities every 2 hours. Thesurgeonsall had more
than 2 months of experience in microsurgery andhad successfully completed free superficial inferiorepigastric artery flaps in rats.16 Lambda-shaped anas-tomosis was chosen in cases in which only one lym-phatic channel and one venule could be found, re-spectively, andtheintravascularstenting method wasapplied in such cases (Fig. 1).17
Girth measurements were taken before andafter the operations at the following five locationsin the lower extremity: plantar arch, ankle, 10 cm
distal to the knee, horizontal patellar midline, and10 cm proximal to the knee. For patients wearingelastic stockings preoperatively, measurements were taken approximately 10 minutes after re-moval of the stockings. These measurements wereused to evaluate the change in the cross-sectional
area after the operation. We compared patient characteristics, opera-
tional findings, and average percentage of reduc-tion in cross-sectional areas between cases withand without lambda-shaped anastomosis. The oc-currence of venous backflow into lymphatic chan-nels was calculated for three basic anastomoses(end-to-end, side-to-end, and end-to-side). Differ-ences in the means between groups were assessedusing the t test, and statistical significance wasdefined as p 0.05.
Intravascular Stenting Method and MaterialsUsed as Intravascular Stenting
Intravascular stenting is a piece of nylon mono-filament suture specifically prepared for each vessel,used as an intravascular stent.17 The stent is insertedinto a vessel to keep the lumen open, assisting safeanastomosis. The needle is inserted into and out from the space between the vessel wall and the in-travascular stenting, significantly facilitating the pro-cedure. In a basic end-to-end anastomosis, the last one or two stitches are left untied to allow removal
of the nylon stent. The intravascular stenting is then
Table 1. Patient Characteristics (40 Limbs of 20
Lower Extremity Lymphedema Patients)
Values
Age, yr 23–71 (average, 49.5)Sex (male:female) 1:19Campisi clinical stage 1–4 (average, 2.4)Duration of edema, yr 0.8–16 (average, 5.6)Cause of lymphedema
Primary, n 2Secondary, n 18
Uterine cervical cancer 7Uterine corpus cancer 4Ovarian cancer 3Other cancers* 4
*Other cancers include malignant lymphoma (n 2), rectal cancer
(n
1), and bladder cancer (n
1).
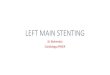
Fig. 1. Graphic representation of intravascular stenting–as-
sistedlambda-shapedanastomosis.First,end-to-sideanastomo-
sis was performed after insertion of an intravascular stent into a
venule. When theanastomosis was completed, thestentwas ex-
tracted fromthe venule. By thismethod,insertionand extraction
oftheintravascularstentwaseasyandfacilitatedtheend-to-side
anastomosis.Greenarrows indicate thelymphflowafterthe lym-
phaticovenular anastomosis.
Plastic and Reconstructive Surgery • May 2011
1988

8/3/2019 Lambda-Shaped Anastomosis With Intravascular Stenting Method for Safe and Effective Lymphaticovenular Anasto…
http://slidepdf.com/reader/full/lambda-shaped-anastomosis-with-intravascular-stenting-method-for-safe-and-effective 3/6
removed from the space between the free vesselends. Diameters of vessels anastomosed in lympha-ticovenular anastomosis are usually around 0.5 mm. According to Narushima’s original method, nylonsutures with size from 3-0 to 7-0 are suitable as in-travascular stenting for lymphaticovenular anasto-mosis (Table 2).
Intravascular Stenting–Assisted Lambda-Shaped Anastomosis
After identification of the lymphatic channelsand venules appropriate for anastomoses, the di-ameters of the vessels were measured. The vessels were then transected, and an intravascular stent-ing of a suitable diameter was inserted into the venule. Next, an incision or excision was made inthe venule using the microscissors to make a win-dow for the end-to-side anastomosis (Fig. 2, above,left ). End-to-side anastomosis was performed be-tween the proximal end of the severed lymphaticchannel and the sidewall of the venule. We startedmaking sutures from the toe and proceeded to theheel side, using 11-0 or 12-0 nylon sutures. For thesafety and facility of the procedure, the needle wasinserted into the venule along the intravascularstenting (Fig. 2, above, right ). The anterior walls of the vessels were sutured likewise. After sutures of the anterior wall were finished, the site of anas-tomosis was turned over using the intravascularstenting, rendering the sutures as easy on the pos-terior wall as on the other side (Fig. 2, below, left ).Finally, an end-to-end anastomosis was made be-tween the distal end of the lymphatic channel andthe venule. The intravascular stenting was pulledout at this point, provided the diameter of the vessel was not too small, rendering the anastomo-sis relatively manageable (Fig. 2, below, right ).
RESULTSThe lymphaticovenular anastomoses resulted in
186 anastomoses in 20 patients with lymphedema of the lower extremities; the average number of anas-
tomoses per case was 9.3 (range, five to 18). The
number of surgical microscope used was two to four(average, 3.3), duration of the operation was 3 to 5hours (average, 4.1 hours), and average percentageof cross-sectional area reduction ranged from 1.9 to11.3 percent (average, 5.9 percent) (Table 3). In thecases of lambda-shaped anastomosis (n 11), thenumber of anastomoses was significantly greaterthan in the cases without lambda-shaped anastomo-sis (n 9; 10.2 2.3 versus 8.2 1.4; p 0.05). Thedifference in average percentage of cross-sectionalarea reduction was not statistically significant be-tween cases with and without lambda-shaped anas-tomosis (6.6 2.1 versus 5.0 1.4 percent; p 0.073) (Table 4). The occurrence of the venousbackflow increased in the following order: end-to-end anastomosis (n 110), side-to-end anas-tomosis (n 27), and end-to-side anastomosis(n 49). The occurrence of venous backflow was
significantly higher in end-to-side anastomosisthan in end-to-end anastomosis (57 versus 24 per-cent; p 0.05) (Fig. 3).
Using intravascular stenting–assisted lambda-shaped anastomosis, surgeons with only 2 months of experience in microsurgery could safely completebidirectional bypasses under conditions in whichonly one lymphatic channel and one venule couldbe found. When the diameter of thelymphaticchan-nel was under 0.3 mm, intravascular stenting–as-sisted end-to-end anastomosis facilitated the anasto-moses, resulting in safe procedures.
DISCUSSION Although various conservative and surgical
therapies are used to treat lymphedema, no ther-apy that is effective in severe cases refractory tocompression therapy has yet been established.1– 8
Lymphaticovenular anastomosis is a process in which anastomosis between a lymphatic channeland a venule of around 0.5 mm in diameter ismade under a microscope.11,12 It is less invasivethan other surgical approaches, can be done un-der local anesthesia, and is postulated to be effec-
tive in lymphedema refractory to compressiontherapy.14,15 Lymphaticovenular anastomoses of vessels this narrow, however, cannot be done suc-cessfully without supermicrosurgical techniquesnor can the best approaches and venules and lym-phatic channels best suited for anastomosis bechosen without sufficient experience. A positivecorrelation between the number of lymphatico- venular anastomoses performed and therapeuticefficacy has been reported. Making as many effi-cient bypasses as possible is also understood to bean important strategy when performing lympha-
ticovenular anastomoses.15
Table 2. Recommended Intravascular Stenting Sizesand Vessel Diameters
Vessel Diameter Size of Nylon Used as IVaS
0.10–0.15 mm 8–00.20 mm 7–00.25–0.35 mm 6–00.40–0.45 mm 5–00.50–0.65 mm 4–00.70–0.85 mm 3–00.90 mm 2–0
IVaS, intravascular stenting.
Volume 127, Number 5 • Lambda-Shaped Anastomosis
1989

8/3/2019 Lambda-Shaped Anastomosis With Intravascular Stenting Method for Safe and Effective Lymphaticovenular Anasto…
http://slidepdf.com/reader/full/lambda-shaped-anastomosis-with-intravascular-stenting-method-for-safe-and-effective 4/6
A variety of lymphaticovenular anastomosismethods exist, and each has its advantages and dis-advantages. Careful selection should be made ac-cording to the circumstances. End-to-end anastomo-sis is the most basic method; it requires fewer
technical skills but is capable of making only one-way
bypasses (Fig. 4, above, left ). In end-to-end flow-through anastomosis, which does not require muchtechnical skill, two anastomoses are made with abranched venule, enabling bidirectional lymphaticbypasses (Fig. 4, above, right ). In side-to-end anasto-
mosis, the end of a venule is anastomosed to the sideof a lymphatic channel, making a bidirectional lym-phatic bypass with each anastomosis; this is techni-cally demanding, however, and the application of intravascular stenting is difficult (Fig. 4, below, left ).Double end-to-side anastomosis, or pi-shaped anas-tomosis, calls for both ends of a lymphatic channelto be anastomosed to a venule, making bidirectionallymphatic bypasses possible; this method is time-con-suming, requiring two anastomoses, and it is tech-nically demanding because the application of intra- vascular stenting is not feasible with this approach
(Fig. 4, below, right ). Lambda-shaped anastomosis is
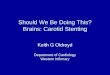
Fig. 2. Images from an actual intravascular stenting–assisted lambda-shaped anastomosis. First, the diameter of the venule
wasmeasuredandanappropriateintravascularstentwasmade.Next,theintravascularstentingwasinsertedtomakeawindowfor end-to-side anastomosis (above, left ). Suturing, which was made easier with the guidance by the intravascular stenting in
the venule, began with the end-to-side anastomosis (above, right ). The posterior wall could be sutured safely by turning over
the site of anastomosis using the intravascular stenting (below, left ). If the diameter of the lymphatic channel was larger than
0.3 mm, the intravascular stenting was extracted before an end-to-end anastomosis (below, right ).
Table 3. Operation Summary (186Lymphaticovenular Anastomoses in 20 LymphedemaPatients)
Values
No. of LVAs per patient 5–18 (average, 9.3)
No. of microscopes usedper patient 2–4 (average, 3.3)Operative time, hr 3–5 (average, 4.1)
Average cross-sectionalarea reduction, % 1.9–11.3 (average, 5.9)
LVAs, lymphaticovenular anastomoses.
Plastic and Reconstructive Surgery • May 2011
1990

8/3/2019 Lambda-Shaped Anastomosis With Intravascular Stenting Method for Safe and Effective Lymphaticovenular Anasto…
http://slidepdf.com/reader/full/lambda-shaped-anastomosis-with-intravascular-stenting-method-for-safe-and-effective 5/6
capable of making bidirectional bypasses even whenthere is only onevenuleavailable; intravascularstent-ing is also possible with this method and is techni-cally less demanding. In lambda-shaped anastomo-sis, intravascular stenting method is applied to
end-to-side anastomosis, so the insertion and extrac-tion of the intravascular stenting is much easier com-pared with conventional intravascular stentingmethods used in end-to-end anastomosis.17,18
When selecting the method of anastomosis inlymphaticovenular anastomoses, it is important tochoose one that enables bidirectional bypasses of the lymphatic channels and allows as many end-to-end anastomoses as possible. In lymphedema,retrograde flow of lymphatic fluid from the prox-imal to the distal part of the vessels makes it nec-essary to make bypasses for both the proximal and
the distal lymphatic channels. This requires that a
method be chosen from among the following:flow-through type anastomosis, side-to-end anas-tomosis, and lambda-shaped anastomosis. In ad-dition, as seen in Figure 3, technically less de-manding end-to-end anastomosis, which has littlebackflow of venous blood into lymphatic channels,should be used, because venous backflow into thelymphatics is considered to be related to the in-effectiveness of lymphovenous bypasses.19 End-to-end anastomosis, end-to-end flow-through typeanastomosis, and lambda-shaped anastomosis willsuffice for this purpose. Therefore, the surgeon
should choose end-to-end flow-through type anas-
Table 4. Comparison between Cases with and without Lambda-Shaped Anastomosis (Mean SD)
With Lambda Anastomosis(n 11)
Without Lambda Anastomosis(n 9) p
Age, yr 48.2 14.2 51.1 11.0 0.619Campisi clinical stage 2.3 0.6 2.6 0.7 0.369Duration of edema, yr 5.3 2.7 6.0 4.2 0.625
No. of LVAs per patient 10.2 2.3 8.2 1.4 0.039*Diameter of lymphatic channel, mm 0.45 0.20 0.44 0.20 0.731Diameter of venule, mm 0.54 0.25 0.53 0.23 0.865No. of microscopes used per patient 3.3 0.5 3.2 0.7 0.844Operative time, hr 4.3 0.6 3.9 0.6 0.159
Average cross-sectional area reduction, % 6.6 2.1 5.0 1.4 0.073
LVAs, lymphaticovenular anastomoses.* p 0.05.
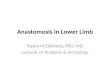
Fig. 3. Three basic anastomoses and frequency of venous back-
flow in 186 lymphaticovenular anastomoses. The occurrence of
the venous backflow increased in the following order: end-to-
end anastomosis (n 110), side-to-end anastomosis (n 27),
and end-to-side anastomosis (n 49). The rate of venous back-
flow was significantly higher in end-to-side anastomosis than in
end-to-end anastomosis (57 versus 24 percent; p 0.05).
Fig. 4. Various methods of lymphaticovenular anastomosis.
( Above,left )End-to-endanastomosisofthedistalendofalymphatic
channel and proximal end of a venule. ( Above, right ) End-to-end
flow-through type anastomosis between a branched venule and
proximal and distal ends of a lymphatic channel. (Below, left ) Side-
to-endanastomosis,inwhichavenulewassuturedtothesidewallof
alymphaticchannel.(Below,right )Doubleend-to-sideanastomosis,
orpi-shapedanastomosis,whichcalledforbothendsofalymphatic
channel to be anastomosed to a venule. Green arrows indicate the
lymph flow after the lymphaticovenular anastomosis.
Volume 127, Number 5 • Lambda-Shaped Anastomosis
1991

8/3/2019 Lambda-Shaped Anastomosis With Intravascular Stenting Method for Safe and Effective Lymphaticovenular Anasto…
http://slidepdf.com/reader/full/lambda-shaped-anastomosis-with-intravascular-stenting-method-for-safe-and-effective 6/6
tomosis or lambda-shaped anastomosis wheneverpossible, but in cases in which only one venule canbe found, lambda-shaped anastomosis is themethod of choice, as end-to-end flow-through typeanastomosis cannot be implemented.
Although this study could not show statistically significant differencesin averagecross-sectional areareduction rates between cases with and without lambda-shaped anastomosis, it showed statistically significant increases in the number of anastomosesin cases with lambda-shaped anastomosis. Based onthe report that the effectiveness of the lymphatico- venular anastomosis correlates with the number of bypasses made, in our department, several surgeonsperformed lymphaticovenular anastomoses usingtwo to four surgical microscopes simultaneously toincrease the number of anastomoses.15 Becausesome surgeons have less than 1 year of experience
with microsurgery, a safe and effective method of anastomosis for beginners is required. Intravascularstenting–assisted lambda-shaped anastomosis is anefficacious method for lymphaticovenular anasto-mosis that fulfills these requirements.
The drawbacks of lambda-shaped anastomosisare that it requires two anastomoses to be madeand that it takes a relatively long time to completebidirectional bypasses. Although microsurgeons with less experience should use lambda-shapedanastomosis in cases in which only one lymphaticchannel and a venule are available, side-to-end
anastomosis is recommended for expert supermi-crosurgeons who can perform side-to-end anasto-moses with ease and safety.
CONCLUSIONSLambda-shaped anastomosis assisted by intra-
vascular stenting, which allows bidirectional lym-phatic bypasses to be made even in cases in whichonly one venule can be found, is a safe and rela-tively easy method that can be performed by sur-geons with less than 1 year of experience in mi-crosurgery. This in turn allows efficient and
effective lymphaticovenular anastomoses to beperformed simultaneously by a team of surgeons,resulting in an increased number of bypasses.
Takumi Yamamoto, M.D.Department of Plastic and Reconstructive Surgery
Graduate School of MedicineUniversity of Tokyo
7-3-1 Hongo, Bunkyo-ku, Tokyo, 113-8655 [email protected]
ACKNOWLEDGMENTSThis study was supported in part by Princess Taka-
matsu Cancer Research Fund grant 09-24120 (to T.Y.).
The authors thank all the members of their department for their kind help in the data collection.
REFERENCES
1. Szuba A, Cooke JP, Yousuf S, et al. Decongestive lymphatic
therapy for patients with cancer-related or primary lymphedema. Am J Med. 2000;109:296–300.
2. Homans J. Treatment of elephantiasis of the legs: A prelim-inary report. N Eng J Med. 1936;215:1099–1104.
3. Sistrunk WE. Modification of the operation for elephantiasis. JAMA. 1918;71:800.
4. Thompson N. The surgical treatment of advanced postmas-tectomy lymphoedema of the upper limb: With the late re-sults of treatment by the buried dermis flap operation. Scand
J Plast Reconstr Surg. 1969;3:54–60.5. Kinmonth JB, Hurst PA, Edwards JM, et al. Relief of lymph
obstruction by use of a bridge of mesentery and ileum. Br J Surg. 1978;65:829–833.
6. Goldsmith HS, De los Santos R, Beattie EJ Jr, et al. Relief of
chronic lymphoedema by omental transportation. Ann Surg.1967;166:573–585.7. O’Brien BM. Microlymphaticovenous surgery for obstructive
lymphoedema. Aust N Z J Surg. 1977;47:284–291.8. Baumeister RG, Siuda S. Treatment of lymphedemas by mi-
crosurgical lymphatic grafting: What is proved? Plast Reconstr Surg. 1990;85:64–76.
9. Campisi C, Boccardo F. Microsurgical technique forlymphedema treatment: Derivative lymphatic-venous micro-surgery. World J Surg. 2004;28:609–613.
10. Yamada Y. Studies on lymphatico-venous anastomoses inlymphedema. Nagoya J Med. 1969;32:1–21.
11. Koshima I, Inagawa K, Urushibara K, et al. Supermicrosur-gical lymphaticovenular anastomosis for the treatment of lymphedema in the upper extremities. J Reconstr Microsurg.
2000;16:432–437.12. Koshima I, Nanba Y, Tsutsui T, et al. Long-term follow-up
after lymphaticovenular anastomosis for lymphedema in theleg. J Reconstr Microsurg. 2003;19:209–215.
13. Yamamoto Y, Sugihara T. Microsurgical lymphaticovenousimplantation forthe treatment of chronic lymphedema. Plast Reconstr Surg. 1998;10:157–161.
14. Koshima I, Nanba Y, Tsutsui T, et al. Minimal invasive lym-phaticovenular anastomosis under local anesthesia for leglymphedema: Is it effective for stage III and IV? Ann Plast Surg. 2004;53:261–266.
15. Narushima M, Mihara M, Yamamoto Y, et al. The intravas-cular stenting method for treatment of extremity lymphedema with multiconfiguration lymphaticovenousanastomoses. Plast Reconstr Surg. 2010;125:935–943.
16. Yamashita S, Sugiyama N, Hasegawa K, et al. A novel model forsupermicrosurgery training: The superficial inferior epigastricartery flap in rats. J Reconstr Microsurg. 2008;24:537–543.
17. Narushima M, Koshima I, Mihara M, et al. Intravascularstenting (IVaS) for safe and precise supermicrosurgery. Ann Plast Surg. 2008;60:41–44.
18. Miyamoto S, Sakuraba M, Asano T, et al. Optimal techniquefor microvascular anastomosis of very small vessels: Compar-ative study of three techniques in a rat superficial inferiorepigastric arterial flap model. J Plast Reconstr Aesthet Surg.2010;63:1196–1201.
19. Nagase T, Gonda K, Inoue K, et al. Treatment of lymphedema with lymphaticovenular anastomoses. Int J Clin Oncol. 2005;10:304–310.
Plastic and Reconstructive Surgery • May 2011
1992