Embed Size (px)
Citation preview

Page 1 of 4
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Case report
For citation purposes: Guida A, Meleti M, Vescovi P, Serpico R, Lucchese A, Lo Muzio L, et al. Anaplastic large cell ana-plastic lymphoma kinase + non-Hodgkin lymphoma in a 10-year-old male discovered during dental visit: a case report. Head Neck Oncol. 2012 Dec 07;4(5):84.
Licensee OA Publishing London 2012. Creative Commons Attribution License (CC-BY)
AbstractNon-Hodgkin lymphoma is rare in children, even though it is the third most frequent type of tumour. Management of a child with non-Hodgkin lymphoma is complex and coordinate presence of haematolo-gists, surgeons, radiotherapists, neu-rologists, psychologists and other expert personnel is required.
Our patient presented with a bulky mass of approximately 5 cm in diam-eter, which grew from his upper-left maxillary bone, thereby causing gum bulge. Thus, the left side of his face from lip to eye appeared swollen. A whole body computed tomography–positron emission tomography exam-ination revealed that the mass was growing in the mouth and maxillary bone and that many bulky nodes were present both in the right and left neck. Histological haematoxylin and eosin assessment revealed an anaplastic large cell proliferation un-derlying the epithelial tissue without epithelial infiltration.
The patient underwent a first cycle of chemotherapy according to the ‘International Protocol of ana-plastic large cell lymphoma’. The Maxillofacial Surgery Unit and the Dentistry Unit of the same hospital took care of his dental situation to
Anaplastic large cell anaplastic lymphoma kinase + non-Hodgkin lymphoma in a 10-year-old male discovered during dental visit:
a case reportA Guida1*, M Meleti2, P Vescovi2, R Serpico1, A Lucchese1, L Lo Muzio3, P Bufo3, G Pannone3
avoid the spread of infective foci to the entire body.
After 1 year and 3 months from the first cycle of chemotherapy, a bulky splenic mass was discovered. Laparoscopic biopsy revealed a re-lapse of the anaplastic lymphoma kinase-positive anaplastic large cell lymphoma in a splenic node. The pa-tient is now alive in good conditions, and continuously followed-up by the Pediatric and Hemato-oncology Operative Unit of University Hospital of Parma.
Rapidity of action and a correct multidisciplinary (oncology-maxillo-facial surgery-dentistry) approach is the key to cure illness, promptly diag-nose relapse and avoid the spread of infective foci from the patient’s teeth during chemotherapy cycles.
IntroductionNon-Hodgkin lymphoma (NHL) is rare in children, even though it is the third most frequent type of tumour. Management of a child with NHL is complex and coordinate presence of haematologists, surgeons, radiother-apists, neurologists, psychologists and others expert personnel is re-quired. Moreover, social workers and nurses are very important in granting the best quality of life to the patient and to fasten rehabilitation. Thus, children with NHL should be treated in reference centres with proper experience.
The dissemination of NHL has been put in correlation with patients’ prognosis1. For this reason, early di-agnosis can lead to a dramatic in-crease in the patient’s probability of disease-free survival. When a patient realises that there is something
unusual orally, he generally visits a dentist. The dentist would carefully inspect oral soft tissues and routine radiographic examination may dem-onstrate an ongoing disease; thus, dentists play a key role in the prelimi-nary detection of NHL.
Histological classification of paediatric NHLHistological classification of paediat-ric NHL is simpler than conventional adult NHL classification. Indeed, almost every case of paediatric NHL belongs to high malignancy grade lymphomas and can be classified into three histological patterns: fol-licular lymphoma, Burkitt’s lym-phoma and anaplastic large cell lymphoma (ALCL).
In each of these histological pat-terns, different subtypes can be recognised. Diagnosis of first two patterns can be difficult if the mar-row is affected; in case neoplastic cells reach ≥25% (30% according to some authors), the disease is classi-fied as lymphoblastic acute leukae-mia. This distinction makes no difference in terms of therapy2.
Staging and presentation modesPaediatric NHL staging procedure is similar to adult NHL staging proce-dure; the sole difference is repre-sented by the role of surgery. Indeed, paediatric NHL presents with bulky abdominal or mediastinal masses; therefore, in many cases, exploratory laparoscopy is used to harvest biop-sies, especially when superficial nodes cannot be harvested for biopsy.
Pathological masses are usually har-vested during abdominal surgery as according to many studies, prognosis
* Corresponding authorEmail: [email protected] Multidisciplinary Department of Medical and
Dental Specialties, Second University of Naples, Naples, Italy
2 Department of ENT, Dental, Ophthalmologic and Head & Neck Sciences, Section of Dentistry, University of Parma, Parma, Italy
3 Department of Clinical and Experimental Medicine. Section of Biomorphological, Stomatological and Reconstructive Sciences. University of Foggia, Foggia, Italy

For citation purposes: Guida A, Meleti M, Vescovi P, Serpico R, Lucchese A, Lo Muzio L, et al. Anaplastic large cell ana-plastic lymphoma kinase + non-Hodgkin lymphoma in a 10-year-old male discovered during dental visit: a case report. Head Neck Oncol. 2012 Dec 07;4(5):84.
Page 2 of 4
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Case report
Licensee OA Publishing London 2012. Creative Commons Attribution License (CC-BY)
is best when each visible mass is harvested.
Many different paediatric NHL staging systems exist. The most com-monly used staging system is the one used at the Saint Jude Children’s Research Hospital.
Two emergency situations occur more often in paediatric NHL cases than in adult NHL cases:
• Obstruction of superior vena cava syndrome, more frequently in lymphoblastic lymphoma, caused by bulky tumour masses com-pressing the airways and other mediastinal structures
• Acute tumour lysis syndrome, more frequently in Burkitt’s lym-phoma, caused by the release of ‘toxic’ molecules from neoplastic cells2.
Paediatric NHL therapyMultidisciplinary approach is neces-sary for paediatric NHL. Chemother-apy is the gold standard approach, as we consider the disease to dissemi-nate from the beginning even in appar-ently localised cases. Many different protocols have been proposed, which are sometimes very complex and rec-ommend up to 4–10 different drugs.
Radiotherapy has a marginal role in paediatric NHL. It is sometimes used before chemotherapy when rapid reduction of mediastinal tu-mour masses is required. In recent studies, radiotherapy was omitted from treatment programs to attempt to reduce the incidence of long-term side effects in patients treated with a combined therapy involving chemo-therapy and radiotherapy.
Since few years, prognosis of chil-dren with NHL has remarkably im-proved. Worldwide, 60%–70% of children with NHL have a 5 year disease-free prognosis; the percent-age has increased to 90% in some subtypes. Recurrences (uncommon, 30%) are treated with a different protocol and often remain sensitive to chemotherapy3. Allogeneic or
autologous bone marrow transplant may be considered, but it is still con-sidered to be an experimental proce-dure, lacking long-term efficacy data2.
Case presentationA 10-year-old boy visited the University of Foggia Dental Clinic as recommended by his dentist. He vis-ited his dentist for check-up of a rap-idly growing intra-oral mass in the upper-left maxilla. The patient came to our observation with a bulky mass, approximately 5 cm in diame-ter, which grew from his upper-left maxillary bone, thereby causing gum bulge. Thus, the left side of his face from lip to eye appeared swollen. A whole body computed tomography–positron emission tomography (CT-PET) examination was required. This revealed that the mass was growing in the mouth and maxillary bone and that there were many bulky nodes both in the right and left neck.
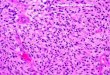
An incisional biopsy of the gum and underlying tissue (approximately 1.5 cm in diameter) was performed. Beneath the gum, instead of bone, surgeons found an amorphous lymphoid-like soft tissue. The sample then underwent histological and immunohistochemical examinations. Histological haematoxylin and eosin (H&E) assessment revealed an anaplastic large cell proliferation
underlying the epithelial tissue without epithelial infiltration. Thus, immunophenotypisation was per-formed for checking positivity for a series of markers (Table 1). Immu-nohisto chemical staining results are shown in Figure 1.
Tumour cells were positive for epi-thelial membrane antigen (EMA), and they stained positively for CD30. They were also positive for Ki-67, showing very high proliferation in-dex (70%). Finally, positivity for ana-plastic lymphoma kinase (ALK) directed us towards a diagnosis of ALK-positive ALCL (ALK+ ALCL). This is a T-cell lymphoma, which is very rare in adults (about 3% of NHLs) but quite frequent in children (10%–20% of all lymphomas). It fre-quently involves extranodal sites such as skin, soft tissues, lung, liver and—as in this case—bone.
The patient was immediately sent to the Department of Mother–Child, Pediatric and Hematology-Oncology Operative Unit, University Hospital of Parma, where he could be treated with the necessary multidisciplinary approach. The patient underwent a first cycle of chemotherapy according to the ‘International Protocol of ALCL’. The Maxillofacial Surgery Unit and the Dentistry Unit of the same hospi-tal took care of his dental situation to avoid the spread of infective foci to
Table 1 Immunohistochemical findings of ALK+ ALCL caseAntibody Immunohistochemical stainingMyeloperoxidase NegativeMyoglobin NegativeCD30 PositiveCD10 Negative in neoplastic cells, positive in surrounding cellsCD3 PositiveCD2 Negative in neoplastic cells, positive in surrounding cellsCD20 NegativeCD79a Negative in neoplastic cells, positive in surrounding cellsTdT NegativeALK-1 PositiveEMA Positive

Page 3 of 4
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Guida A, Meleti M, Vescovi P, Serpico R, Lucchese A, Lo Muzio L, et al. Anaplastic large cell ana-plastic lymphoma kinase + non-Hodgkin lymphoma in a 10-year-old male discovered during dental visit: a case report. Head Neck Oncol. 2012 Dec 07;4(5):84.
Case report
Licensee OA Publishing London 2012. Creative Commons Attribution License (CC-BY)
clinicopathological entity; this was subsequently included in the revised Kiel classification in 1988 as ‘large cell anaplastic lymphoma’11,12. The term ‘anaplastic large cell lymphoma’ ultimately became the preferred des-ignation13. The pathogenesis of ALCL was unravelled in 1994 when Morris and colleagues cloned the genes in-volved in translocation, identifying a newly described tyrosine kinase namely ‘anaplastic large cell lym-phoma kinase’ (ALK)14.
ALCL has been defined as a distinct clinicopathological entity based on its histological, clinical, immunophe-notypical, and molecular features. Molecular analysis has been an im-portant tool in clarifying the border-lands of this and other entities, as most diseases have a distinct molecu-lar fingerprint that relates to under-lying pathogenesis. Moreover, in this paradigm, molecular studies may be used to refine the ultimate morpho-logic definition, leading to improved diagnostic criteria. The accurate di-agnosis of ALCL has important clini-cal implications because it is a highly treatable form of lymphoma and has a much better prognosis than other types of T-cell lymphoma, even in case of relapses as observed in this case, unlike ALK-negative ALCL.
Conclusion• Rapidity of action and a correct
multidisciplinary (oncology-max-illofacial surgery-dentistry) ap-proach is the key to cure illness, promptly diagnose relapse and avoid the spread of infective foci from the patient’s teeth during chemotherapy cycles.
• General practitioners/paediatric dentists and orthodontists have a key role in diagnosing soft tissues/bone neoplasms of the jaw. An accurate inspection of oral soft tissues and radiographic ex-amination can easily lead to the dis covery of abnormal conditions during routine visits to private practices.
under surveillance by the Dentistry and Maxillofacial Surgery Units.
DiscussionThe historical background of ALCL began in 19824 when the monoclonal antibody Ki-1 was raised against a Hodgkin’s disease (HD) cell line5. Ki-1 was subsequently shown to stain the malignant cells of HD in tissue sec-tions as well as a smaller lymphoid cell was found in the parafollicular regions of normal lymph nodes6. The Ki-1 antigen, subsequently assigned to the CD30 cluster, was identified as an activation antigen, which could be expressed on T-cells, B-cells and even activated histiocytes7–9.
In 1985, Stein et al. found that the Ki-1 (CD30) antigen was highly ex-pressed by a group of 45 large cell lymphomas that shared a number of histological characteristics10. These tumours exhibited a morphology which was suggestive of ‘malignant histiocytes’ and also exhibited promi-nent sinusoidal invasion. It was proposed that the anaplastic CD30-positive tumours represent a distinct
the entire body. Two teeth were ex-tracted and professional hygiene was performed every month; antibiotics were prescribed as and when re-quired. RM, CT, PET and eco exams were performed to check the status of primary lesions and detect possi-ble relapses and neck node status, which were found to be mildly posi-tive. After five months, the primary lesion was undetectable, but the right neck node remained mildly positive. A ‘wait and see’ policy was adopted. After 1 year and 3 months from the first cycle of chemotherapy, a bulky splenic mass was discovered. Laparoscopic biopsy revealed a re-lapse of ALK+ ALCL in a splenic node. The patient thus was cured according to the ‘Italian Association of Pediatric Hematology-Oncology ALCL Relapse’ protocol under continuous dental care to prevent the spread of infective foci to the entire body. The patient is now alive in good conditions, continuously followed-up by the Pediatric and Hemato-oncology Operative Unit of University Hospital of Parma. His dental condition is
(a)
(b) (c)
ALKALK
(d)
(e)
ALKEMAALKCD30
Figure 1: Histopathological findings of the reported ALK+ ALCL case. H&E staining showed proliferation of large–medium neoplastic lymphocytes not in-volving the superficial epithelial layer of the gum (a, 40×; b, 200×). The lym-phoma stained positive for ALK (c, 400×), EMA (d, 400×) and CD30 (e, 400×) (LSAB-HRP technique, nuclear counterstaining with type II Gill’s haematoxylin).

For citation purposes: Guida A, Meleti M, Vescovi P, Serpico R, Lucchese A, Lo Muzio L, et al. Anaplastic large cell ana-plastic lymphoma kinase + non-Hodgkin lymphoma in a 10-year-old male discovered during dental visit: a case report. Head Neck Oncol. 2012 Dec 07;4(5):84.
Page 4 of 4
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Case report
Licensee OA Publishing London 2012. Creative Commons Attribution License (CC-BY)
antigen Ki-1 (CD30). Am J Pathol. 1989 Jan;134(1):187–92.9. Abbondanzo SL, Sato N, Straus SE, Jaffe ES. Acute infectious mononucleosis. CD30 (Ki-1) antigen expression and histologic correlations. Am J Clin Pathol. 1990 May; 93(5):698–702.10. Stein H, Mason D, Gerdes J, O’Connor N, Wainscoat J, Pallesen G, et al. The expres-sion of the Hodgkin’s disease associated antigen Ki-1 in reactive and neoplastic lymphoid tissue: evidence that Reed-Sternberg cells and histiocytic malignan-cies are derived from activated lymphoid cells. Blood. 1985 Oct;66(4):848–58.11. Stansfeld AG, Diebold J, Noel H, Kapanci Y, Rilke F, Kelényi G, et al. Updated Kiel classification for lymphomas. Lancet. 1988 Feb;1(8580):292–3.12. Lennert K, Feller A. Histopathology of non-Hodgkin’s lymphomas. 2nd ed. New York: Springer-Verlag; 1992.13. Harris NL, Jaffe ES, Stein H, Banks PM, Chan JK, Cleary ML, et al. A revised European-American classification of lym-phoid neoplasms: a proposal from the International Lymphoma Study Group. Blood. 1994 Sep;84(5):1361–92.14. Morris SW, Kirstein MN, Valentine MB, Dittmer KG, Shapiro DN, Saltman DL, et al. Fusion of a kinase gene, ALK, to a nucleo-lar protein gene, NPM, in non-Hodgkin’s lymphoma. Science. 1994 Mar;263(5151): 1281–4.
of tumours of haematopoietic and lym-phoid tissues. Lyon: IARC Press; 2008, pp. 312–6.3. Liso A, Tiacci E, Binazzi R, Pulford K, Benedetti R, Carotti A, et al. Haploidentical peripheral-blood stem-cell transplanta-tion for ALK-positive anaplastic large-cell lymphoma. Lancet Oncol. 2004 Feb;5(2): 127–8.4. Jaffe ES. Anaplastic large cell lym-phoma: the shifting sands of diagnostic hematopathology. Mod Pathol. 2001 Mar; 14(3):219–28.5. Schwab U, Stein H, Gerdes J, Lemke H, Kirchner H, Schaadt M, et al. Production of a monoclonal antibody specific for Hodgkin and Sternberg-Reed cells of Hodgkin’s disease and a subset of normal lymphoid cells. Nature. 1982 Sep; 299(5878):65–7.6. Stein H, Gerdes J, Schwab U, Lemke H, Mason DY, Ziegler A, et al. Identification of Hodgkin and Sternberg-Reed cells as a unique cell type derived from a newly-detected small-cell popula-tion. Int J Cancer. 1982 Oct;30(4):445–59.7. Andreesen R, Osterholz J, Löhr G, Bross K. A Hodgkin cell-specific antigen is expressed on a subset of auto- and alloac-tivated T (helper) lymphoblasts. Blood. 1984 Jun;63(6):1299–302.8. Andreesen R, Brugger W, Löhr GW, Bross KJ. Human macrophages can express the Hodgkin’s cell-associated
• For these reasons, dentists must not underestimate their impor-tance in early diagnosis of oral and maxillofacial neoplasms.
Abbreviations listALCL, anaplastic large cell lym-phoma; ALK, anaplastic lymphoma kinase; EMA, epithelial membrane antigen; HD, Hodgkin’s disease; NHL, non-Hodgkin lymphoma.
ConsentWritten informed consent was obtained from the patient for publi-cation of this case report and accom-panying images.
References1. Mussolin L, Damm-Welk C, Pillon M, Zimmermann M, Franceschetto G, Pulford K, et al. Use of minimal disseminated dis-ease and immunity to NPM-ALK antigen to stratify ALK-positive ALCL patients with different prognosis. Leukemia. 2012 Jul.2. Delsol G, Falini B, Müller-Hermelink HK, Campo E, Jaffe ES, Gascoyne RD, et al. Anaplastic large cell lymphoma, ALK-positive. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, editors. World Health Organization (WHO) classification