Embed Size (px)
Citation preview

669
Received February 5, 2004; Accepted July 1, 2004
669
Neurol Med Chir (Tokyo) 44, 669¿673, 2004
Long-Term Control of Recurrent Anaplastic EpendymomaWith Extracranial Metastasis: Importance of Multiple
Surgery and Stereotactic Radiosurgery Procedures
—Case Report—
Manabu KINOSHITA, Shuichi IZUMOTO, Naoki KAGAWA, Naoya HASHIMOTO,Motohiko MARUNO, and Toshiki YOSHIMINE
Department of Neurosurgery, Osaka University Medical School, Suita, Osaka
Abstract
An 11-year-old Japanese girl presented with a right frontal lobe anaplastic ependymoma. The tumor wasremoved surgically. However, she developed a secondary lesion and extracranial metastasis in thecervical lymph node. In total, she underwent eight intracranial tumor removal procedures, fivestereotactic radiosurgeries with six targets, and five cervical lymph node removal surgeries during thecourse of 7 years. She is currently alive with a good quality of life, and has no major neurological de-ficits except right facial nerve palsy. The combination of surgery and radiosurgery can achieve localcontrol of anaplastic ependymoma. Multiple surgery or radiosurgery procedures can result in goodoutcome, if the tumor does not involve crucial structures, even if extracranial metastasis occurs.
Key words: anaplastic ependymoma, extracranial metastasis, multiple surgery,stereotactic radiosurgery
Introduction
Ependymoma accounts for 2–5% of all brain tumorsand 5–10% of childhood brain tumors, but progres-sive disease develops within 5 years in 40–70% ofpatients.15) The extent of tumor resection and con-trol of local recurrence are the primary factorsaffecting the treatment outcome.6,14,15) We treated apediatric patient with supratentorial anaplasticependymoma who suffered multiple tumor recur-rences and extracranial metastasis by surgery andradiosurgery, and who continues to live 7 years afterdisease detection without significant deficits.
Case Presentation
An 11-year-old Japanese girl was transferred to ourhospital for the treatment of a cerebral tumor in theright frontal lobe manifesting as headache, nausea,and clumsiness of the left fingers. On admission,magnetic resonance (MR) imaging showed a 5.5-cmring-shaped enhanced mass with a solid nodular
compartment. The tumor was removed surgically.Histological examination established the diagnosisof anaplastic ependymoma (Fig. 1A–C). The Ki-67staining index was 36%. She was given 50 Gy oflocal field radiation. However, 15 months later, sheagain presented with severe headache and a 5-cmmass was identified at the right temporal base.Surgery achieved gross total removal of the tumor.MR imaging identified a small residual tumor, sogamma knife radiosurgery was performed. Thepatient was followed up by MR imaging every 3months to detect tumor recurrence before anyneurological symptom emerged.
Surgery was again necessary 3 years after theinitial treatment due to local recurrence at the tem-poral base and tent. Painless rapid swelling of herright cervical lymph node was observed and fineneedle aspiration cytology revealed the presence ofclass V malignant cells. Head and neck surgery wasperformed to remove the right deep cervical lymphnodes. Tumor metastases to multiple lymph nodes ofthe internal jugular chain of the deep lateral cervicalgroup were confirmed at the operation. As expected,histological examination confirmed metastasis of

670
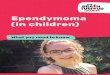
Fig. 1 Photomicrographs of the first lesion showing atypical cells (A: HE stain, ×400) and tumorcells positive for glial fibrillary acidic protein (GFAP) (B:×400), with a Ki-67 staining indexas high as 36% (C: ×400). Photomicrographs of the latest specimen showing no drasticchanges in histological features during the clinical course (D: HE stain, ×400; E: GFAPstain, ×400; F: Ki-67 stain, ×400).
670
Neurol Med Chir (Tokyo) 44, December, 2004
M. Kinoshita et al.
the anaplastic ependymoma to the cervical lymphnode. Although metastasis to other organs wasfeared, investigation of the whole body using Gascintigraphy and computed tomography (CT)revealed no other metastatic sites.
She had suffered three episodes of intracranialand two episodes of neck lymph node recurrence,so chemotherapy with cyclophosphamide, VP-16,CDDP, vincristine, and dexamethasone, withintrathecal injection of methotrexate, was ad-ministered. This therapy resulted in 22 months oftumor remission, but she then developed localrecurrence in the right frontal lobe and consecutiverecurrences in the right cervical lymph node andright temporal base. Each recurrence requiredsurgical removal of the tumor. The high rate of local
recurrence at the right frontal lobe required toofrequent surgical intervention, so we treated therecurrent intracranial lesions with stereotacticradiosurgery using a cyber knife and gamma knife toboth reduce the need for reoperation and reduce therisk of motor deficit due to iatrogenic damage of themotor cortex. Stereotactic radiosurgery controlledthe irradiated lesion for 3 to 15 months, but tumorregrowth was observed and the lesion was againsurgically removed. The most recent surgical sampleof the latest right frontal lesion showed evidenceof both radiation necrosis and tumor recurrence(Fig. 1D–F).
In total, eight intracranial tumor removal opera-tions, five stereotactic radiosurgery procedures withsix targets, and five cervical lymph node removal

671
Fig. 2 Illustration of the entire clinical course. The magnetic resonance images were obtained onthe documented date. Tumor removals of intracranial lesions are recorded as arrows,stereotactic radiosurgeries as broken line arrows, and removals of the cervical lymph node asasterisks. The numbers following the broken arrows are the dose of the radiation (Gy) appliedat each stereotactic radiosurgery.
671
Neurol Med Chir (Tokyo) 44, December, 2004
Control of Recurrent Anaplastic Ependymoma
operations have been required (Fig. 2). Everysurgical procedure, both intracranial and ex-tracranial, achieved gross total removal of thetumor. She continues to survive without neurologi-cal deficits other than right facial nerve palsy due tosacrifice of the right facial nerve in the course ofright cervical lymph node removal. She manifestsno cognitive disorders and maintains a good qualityof life.
Discussion
The grading system proposed by the World HealthOrganization (WHO) classifies subependymoma asgrade I, ependymoma as grade II, and anaplasticependymoma as grade III. Low grade ependymomatends to occur in infratentorial regions whereas highgrade anaplastic ependymoma arises in the cerebralhemisphere.3) There are numerous prognostic
factors such as resection extent, radiation strategy,chemotherapy, histological grade, location, and soon.3–6,10,11,14,15,18) As can be expected, high gradeanaplastic ependymoma carries a poorer prognosisthan low grade.3) The extent of resection is thekey prognostic factor and the location of the tumordetermines the extent to which removal is possi-ble.6,12,14,15) Local field may be more effective thanwhole-brain irradiation.7) However, most studiesquestion the effect of chemotherapy.4,14) Chemother-apy failed to improve the outcome in children withependymoma.4)
In our case, the tumor arose in the supratentorialcerebral hemisphere and was anaplastic ependymo-ma (WHO grade III), which matches the previouslyreported characteristics. The very interestingcharacteristic of our case is that recurrence onlyoccurred in the ipsilateral hemisphere and ex-tracranial metastasis was observed only at the ip-

672672
Neurol Med Chir (Tokyo) 44, December, 2004
M. Kinoshita et al.
silateral side. The secondary lesion at the temporalbase was outside the surgical field of the primarylesion in the frontal lobe, and no multiple intracrani-al metastases were detected, so we think that thesecondary lesion was unlikely to result from tumorcell seeding. CT and Ga scintigraphy detected noother metastatic lesions in other organs in the 4years since the presence of extracranial metastasiswas first detected, although the patient suffered mul-tiple episodes of local recurrence.
Extracranial metastases from primary braintumors are frequently found in the cervical lymphnodes, vertebral bodies, and lungs.9,13,16,19) Ex-tracranial metastasis of gliomas may occur viavascular or lymphatic tumor cell seeding caused bysurgical exposure of the tissues.19) However, twopatients with glioma suffered extracranial metasta-sis despite not undergoing surgery.13) Brain extracel-lular fluid drains into the deep cervical lymphnodes,2) so may be involved in the extracranialmetastasis of primary brain tumors.
Our patient's clinical course confirms the impor-tance of control of local recurrence in patients withependymoma. Surgical and/or stereotactic radiosur-gical control of the tumor is imperative, even inpatients with extracranial metastasis. Surgery canbe expected to provide a good outcome unless thetumor involves crucial structures. Stereotacticradiosurgery may be useful for controlling the lesionif the tumor involves crucial structures such as themotor cortex, and may reduce the number of directsurgical interventions required for controlling thelesion. Recently, stereotactic radiosurgery has beenuseful for treating children with ependymomas.1,8,17)
We suggest that the combination of direct surgeryand stereotactic radiosurgery is very effective forcontrolling recurrent anaplastic ependymoma.
References
1) Aggarwal R, Yeung D, Kumar P, Muhlbauer M, KunLE: Efficacy and feasibility of stereotactic radiosur-gery in the primary management of unfavorablepediatric ependymoma. Radiother Oncol 43: 269–273,1997
2) Cserr HF, Harling-Berg CJ, Knopf PM: Drainage ofbrain extracellular fluid into blood and deep cervicallymph and its immunological significance. BrainPathol 2: 269–276, 1992
3) Ernestus RI, Schroder R, Stutzer H, Klug N: Theclinical and prognostic relevance of grading inintracranial ependymomas. Br J Neurosurg 11:421–428, 1997
4) Evans AE, Anderson JR, Lefkowitz-Boudreaux IB,Finlay JL: Adjuvant chemotherapy of childhoodposterior fossa ependymoma: cranio-spinal irradia-
tion with or without adjuvant CCNU, vincristine,and prednisone: a Childrens Cancer Group study.Med Pediatr Oncol 27: 8–14, 1996
5) Gerszten PC, Pollack IF, Martinez AJ, Lo KH,Janosky J, Albright AL: Intracranial ependymomas ofchildhood. Lack of correlation of histopathology andclinical outcome. Pathol Res Pract 192: 515–522, 1996
6) Healey EA, Barnes PD, Kupsky WJ, Scott RM, SallanSE, Black PM, Tarbell NJ: The prognostic sig-nificance of postoperative residual tumor in ependy-moma. Neurosurgery 28: 666–672, 1991
7) Kovalic JJ, Flaris N, Grigsby PW, Pirkowski M,Simpson JR, Roth KA: Intracranial ependymomalong term outcome, patterns of failure. J Neurooncol15: 125–131, 1993
8) Merchant TE, Zhu Y, Thompson SJ, Sontag MR,Heideman RL, Kun LE: Preliminary results from aPhase II trial of conformal radiation therapy forpediatric patients with localised low-grade astrocyto-ma and ependymoma. Int J Radiat Oncol Biol Phys 52:325–332, 2002
9) Ordonez NG, Ayala AG, Leavens ME: Extracranialmetastases of oligodendroglioma: report of a caseand review of the literature. Neurosurgery 8: 391–396,1981
10) Oya N, Shibamoto Y, Nagata Y, Negoro Y, HiraokaM: Postoperative radiotherapy for intracranialependymoma: analysis of prognostic factors andpatterns of failure. J Neurooncol 56: 87–94, 2002
11) Palma L, Celli P, Cantore G: Supratentorial ependy-momas of the first two decades of life. Long-termfollow-up of 20 cases (including two subependymo-mas). Neurosurgery 32: 169–175, 1993
12) Palma L, Celli P, Mariottini A, Zalaffi A, Schettini G:The importance of surgery in supratentorial ependy-momas. Long-term survival in a series of 23 cases.Childs Nerv Syst 16: 170–175, 2000
13) Pasquier B, Pasquier D, N'Golet A, Panh MH,Couderc P: Extraneural metastases of astrocytomasand glioblastomas: clinicopathological study of twocases and review of literature. Cancer 45: 112–125,1980
14) Perilongo G, Massimino M, Sotti G, Belfontali T,Masiero L, Rigobello L, Garre L, Carli M, LombardiF, Solero C, Sainati L, Canale V, del Prever AB,Giangaspero F, Andreussi L, Mazza C, Madon E:Analyses of prognostic factors in a retrospectivereview of 92 children with ependymoma: ItalianPediatric Neuro-oncology Group. Med Pediatr Oncol29: 79–85, 1997
15) Pollack IF, Gerszten PC, Martinez AJ, Lo KH, ShultzB, Albright AL, Janosky J, Deutsch M: Intracranialependymomas of childhood: long-term outcome andprognostic factors. Neurosurgery 37: 655–667, 1995
16) Sadik AR, Port R, Garfinkel B, Bravo J: Extracranialmetastasis of cerebral glioblastoma multiforme: casereport. Neurosurgery 15: 549–551, 1984
17) Stafford SL, Pollock BE, Foote RL, Gorman DA,Nelson DF, Schomberg PJ: Stereotactic radiosurgeryfor recurrent ependymoma. Cancer 88: 870–875, 2000

673673
Neurol Med Chir (Tokyo) 44, December, 2004
Control of Recurrent Anaplastic Ependymoma
18) Vanuytsel LJ, Bessell EM, Ashley SE, Bloom HJ,Brada M: Intracranial ependymoma: long-termresults of a policy of surgery and radiotherapy. Int JRadiat Oncol Biol Phys 23: 313–319, 1992
19) Wallace CJ, Forsyth PA, Edwards DR: Lymph nodemetastases from glioblastoma multiforme. AJNR AmJ Neuroradiol 17: 1929–1931, 1996
Address reprint requests to: S. Izumoto, M.D., Departmentof Neurosurgery, Osaka University Medical School,2–2 Yamadaoka, Suita, Osaka 565–0871, Japan.e-mail: sizumoto@nsurg.med.osaka-u.ac.jp